Embed Size (px)
Citation preview

The International Journal of the Addictions, 19(1), 25-44, 1984
A Diagnostic Tool with Important Implications for Treatment of Addiction: Identification of Factors Underlying Relapse and Remission Time Distributions
Nancy R. Mann," PhD
V. Charles Charuvastra, MD
V. K. Murthy, PhD
Abstract
The results of analysis of successive relapse and remission times of many opiate addicts were examined. It is discovered that motivation is the preeminent factor that governs the distribution of lengths of re- mission times (periods of abstinence), differences in types of motiva- tion leading to an underlying mixture of three or fewer Weibull distri- butions. On the other hand, two distinct factors-namely wear-out (dysfunction resulting from exhaustion or tiring out brought on by the addict's enforced life-style) and precipitation of events that may not be beyond the control of the addict-govern the distribution of lengths of relapse times (periods of using opiates), leading, typically, to an underlying competing-risk distribution. Methods for using this informa- tion to aid in treatment and in research are described.
*To whom correspondence should be addressed at BM-82, Department of Biomathematics, School of Medicine, University of California, Los Angeles, California 90024.
25
Copyright 0 1984 by Marcel Dekker, Inc. 0020-773X/84/19014025$3.50/0
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

26 MA”, CHARWASTRA, AND MURTHY
INTRODUCTION
The present study, as well as previous research (Brill, 1972; Waldorf, 1973; Waldorf and Biernacki, 1979), suggests that feelings of dysfunction regarding heroin and the related life-style, “rock bottoms” that precipitate “surrender,” existential c,rises, and other events that change the way in which the addict views his or her use of the drug are among the major contributing factors leading ad- dicts to quit the use of heroin for extended periods of time. Dysfunction is ex- pressed usually in terms of being tired: tired of the life, the “changes,” the “hassles”; tired of the junkies and being in and out of jails (Waldorf and Biernacki, 1979). One might view this as a type of “wearing out.” “Rock bottom” is a subjective state wherein the individual reaches some low point in his or her life and is sometimes motivated to surrender and make a radical change in behavior. On the other hand, existential crisis (Kierkegaard, 1941a, 1941b) is a more profound emotional and psychological state in which the addict questions the very nature and meaning of his or her whole life and being. Other precipitating events may take the form of falling in love, becoming a parent, having a “eureka” (sudden insightful) experience, etc.
The present authors are thus led to the hypothesis that these different types of factors, as well as factors precipitating shorter periods of abstinence, “compete” during periods of use of heroin to motivate the patient to quit the use of the drug. In statistical terminology, the hypothesis states that the distribu- tion of successive intervals of use of heroin by an individual behaves as a random sample from an underlying distribution corresponding to a competing-risk m ode1 .
The question now arises: How does the addict stay successful in maintaining abstinence? For help in answering this question and in validating our hypothesis concerning the distribution of intervals of use, an analysis was made of histories of successive intervals of remission and relapse in addicts from several populations.
DESCRIPTION OF DATA SOURCES AND METHODS
The data for this study were obtained from three different institutions. They are the Maryland Psychiatric Research Center (MPRC), the Brentwood Veterans Administration Hospital Methadone Maintenance Program, and the New Jersey Medical School. The data from the MPRC pertain to a community- wide study, made in Baltimore beginning in 1965 and continuing throughout the decade of the ’7Os, in which detailed use histories of 405 male narcotic abusers were obtained by intensive interviews and validated by follow-up investigations. The initial study involving part of the data is described by Nurco et al. (1975).
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

RELAPSE AND REMISSION TIME 21
The Brentwood Methadone Program, under the direction of Dr. V. C. Charuvastra (Ling and Charuvastra, 1976), began in 1974 as part of the Brent- wood Hospital drug treatment program. The recidivism data from this program were obtained for this study in early 1980 from 88 randomly selected patient records, about a third of the patient population (all males) who were active at the time of selection. Additional data from the methadone clients were obtained by means of an interview program. Informed consent was obtained after the purpose of the research was fully explained. All recidivism data were extracted from the patient records and resulted from randomly performed weekly urinalyses made to determine presence or absence of various drugs, including both heroin and methadone.
Information from the New Jersey Medical School (NJMS) was provided in 1980 by Dr. A. Sheffet (Lavenhar et al., 1975). The data used from the NJMS study pertain to periods of both inpatient and outpatient residency that were terminated prematurely, by Newark residents only among over 5,000 narcotics abusers in the various Newark community treatment programs from 1969 to 1980.
The sequence of consecutive remission times and the sequence of consecu- tive durations of relapse, along with demographic and background profiles of the addict, were available for all of these populations. The methods used in this paper are directed toward characterizing the basic underlying distributions of remission and relapse times.
Earlier analyses (Mann, 1979; Mann and Rothberg, 1980) of the type per- formed in this study were made by one of the authors on data stored at the Walter Reed Research Center, concerning U.S. Army personnel who were re- peatedly hospitalized for alcoholism.
AN A LYS I S
In the present context it has been found that detoxification provides a time that one may fruitfully define as the initiation of a life test which ends in “failure” if and when the subject returns to use of heroin. Thus, a single patient beginning with detoxification may generate successive times to failure, first, second, third, . . ., etc., just as would light bulbs successively tested until failure (burnout) in a single electrical outlet.
“Detoxification” is used in this analysis rather loosely as the time an addict abstains from ingestion of the substance to whch he or she is addicted long enough to eliminate the drug and its immediate toxic effects from his or her body and brain. Detoxification in this sense may result from inpatient or out- patient treatment at a hospital or a treatment center, or it may be self-induced. It may be a result of legal pressure or of social pressure brought to bear by family members, a friend, or an employer, or by temporary unavailability of the
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

28 MANN, CHARUVASTRA, AND MURTHY
substance. Or it may result simply from a decision on the part of the addict or drug abuser to give up the habit because of its deleterious effects on his or her life and the lives of others.
Also, we define “remission time” (number of days to relapse, or failure) as the number of days from detoxification until resumption of use, leading (hope- fully) to a subsequent detoxification. A “relapse time” is defined as the time fol- lowing resumption of use until a subsequent remission. In utilizing historical hospitalization data (treatment program data), one may define “time to relapse” as the number of days between hospitalizations resulting from drug use (number of days from entry until premature termination). However, such measures of time to failure are biased since they often include time of using and, indeed, may be affected by various extraneous factors, including strength of drug.
The methods used in this paper for the analysis of remission and relapse times are survival analysis techniques (Mann, Schafer, and Singpurwalla, 1974). Essentially, this methodology provides a means of characterizing the underlying distributions governing the histories of consecutive relapse and remission times of a patient. Characterization of the distributions gives insight into the mechanics of the phenomena of relapse and remission, and provides an objective tool to aid in prediction of treatment outcome and for detecting treatment ef- fects, spontaneous or otherwise. The tool provided is one that is much more sen- sitive than the usual procedures based solely on an arbitrary time threshold. Also, one can use this type of methodology with “time to first relapse” or “ex- tent of longest period of abstinence” of patients in a treatment program for comparing different treatment modalities. These various issues of prediction and comparison will be, for the most part, addressed in a subsequent paper.
Statistical Models
The three statistical models that have emerged from the analysis are a single Weibull distribution, a mixture of two or more Weibull distributions, and a competing-risk distribution. The Weibull distribution is one in which, for an addict in remission, the logarithm of conditional probability of a relapse is pro- portional to the logarithm of the duration of remission. When the constant of proportionality is 0, the distribution becomes the well-known exponential distri- bution governing relapsed times between Poisson (or purely random) events. The Weibull mixture model is one in which the distribution is a linear combination of two or more Weibull distributions.
Suppose “time to failure” in a random sample of hardware such as, for ex- ample, razor blades, exhibits a frequency distribution that suggests a single Weibull population. Then one would be justified in inferring that failure is pre- cipitated by a single cause (wear-out, e.g.), and that the razor blades are from a single population. If two (three) distinct distributions are indicated, suggestive
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

RELAPSE AND REMISSION TIME 29
of perhaps a bimodal (trimodal) frequency distribution, then one would again hypothesize a single cause of failure, but in this case with two (three) different types of razor blades with very different average failure times.
Finally, the competing-risk distribution is the distribution of “time to event” (relapse, remission) in which two or more forces are competing througb- out the time until the event (relapse, remission) to pressure the addict to give up.
A convenient hardware analogy for competing risk is given by the two processes of wear-out and destruction by vandals of light bulbs in a street lamp post. Each bulb will eventually wear out unless it is prematurely destroyed by a vandal. In this model the vandalism may occur at any time throughout the life of each bulb. In an alternative light bulb model that is seen to be clearly a mix- ture, one would observe a single cause of failure in a sample from two or more populations of light bulbs with very different average failure times.
Graphical Plotting of the Data
Based on a random sample of N times to an event (relapse or remission) from a single individual or a single population, the underlying distribution of duration of a remission or relapse can be estimated as follows: The data are first ordered according to increasing size. Let T(i) be the ith smallest time to the event in a sample history of N observed times. The quantity 1-(i- S) /N is calcu- lated for each i as an estimate of the probability that the event does not occur before time T(i). The graph of ( i -S) /N plotted against T(i) is a graph of the underlying cumulative distribution of time to the event.
To capture any pattern of the type we are after, we plot In-ln[l - (i - . 5 ) / N ] ) versus ln[T(i)J . A straight-line plot (Kao, 1959) suggests that the original (unordered) observations are independent events and that the underlying distribution belongs to the Weibull family. A pattern of two (or three) distinct consecutive straight lines suggests that the underlying distribution is a mixture of two (or three) Weibull distributions. A corresponding frequency distribution for time to failure would be bimodal (or trimodal), unless one or more of the Weibull distributions has no mode.
If, on the other hand, the plot is a curve with several twists and turns, then it indicates an underlying competing-risk model. The competing-risk plot for a large sample of successive intervals of use of heroin looks like a sample random- ly selected from two or more different (possibly Weibull or mixture of Weibull) distributions whch completely overlap. A corresponding frequency function would be the result of two or more unimodal or multimodal frequency distribu- tions (with possibly one or more frequency distributions among these devoid of a mode). As opposed to a unimodal, bimodal, or trimodal mixture model, the competing-risk frequency function could be characterized as a lumpy mass formed by the two or more overlapping modes and/or masses of density.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

30 MA”, CHARUVASTRA, AND MURTHY
Computerized graphical (Versatec) plots of time to relapse were made for each of the subjects who exhibited three or more failure times among all of the methadone clients, all of the Baltimore addicts, and a sample of 200 of the Newark residents with premature terminations. Plots of periods of use (time to remission) were made for eight of the methadone clients who exhibited 20 or more such periods.
DI SCUSSl ON
The authors found, from analysis of the data, that the type of motivation (or “intention”) appears to be the preeminent factor determining length of re- mission times of addicts. From the many sets of longitudinal time-to-relapse data, they identified three different levels (or strengths) of intention, corre- sponding to a mixture of three different failure patterns with different average failure times. These three patterns appeared randomly distributed over time in individual histories and over individual subjects in “time to chronologically first (or kth, 1 < k GAJ, or most recent) failure” in samples o f N cohorts. (It is inter- esting that a study of prison recidivism by Carr-Hill and Carr-Hill [ 19721 , which investigates time to first failure, also finds a mixture of three distributions.) The three levels appear, on the basis of interview results, to be associated with, re- spectively, uninternalized motivation (such as compliance arising in response to coercion), ordinary internalized motivation (somewhat akin to that leading to New Year’s resolutions, going on a diet, and the like), and very profound motiva- tion (such as provided by falling in love, having a spiritual experience, or by an extremely strong feeling of dysfunction).
Thus, an intention (or resolve) to abstain and to make changes in behavior and/or life-style that facilitate abstinence is formed and may or may not be strengthened or changed after the original formation. Meanwhile, the stresses and traumas that the addict experiences, or time itself, will tend to erode away this intention. Making behavior modifications and changes in one’s environment is for an addict analogous to using a beard softener that can to some extent pro- long the life of a razor blade. Only in cases in which there is an ingredient in the beard softener that profoundly strengthens the blade can it be changed from an ordinary one to one designed to last for years.
Thus, the type of intention alone determines whether the period of re- mission will be, for the individual in any particular instance during his or her history of use, of more or less average length, unusually short or unusually long. This leads one to the hypothesis that successive periods of abstinence in an indi- vidual addict behave like a random sample from an underlying distribution corre- sponding to a mixture of three or fewer distributions, each individual distribu- tion corresponding to one of the three possible degrees of motivation.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

RELAPSE AND REMISSION TIME 31
Previous research (Simpson et al., 1977) has shown that background family responsibility and background socioeconomic status are predictors of per- formance following narcotic treatment programs. What is suggested here is that these background variables give a measure of the ability of a subject to be motivated.
CONCLUSIONS
Identification of Failure Patterns
The slopes of the Weibull plots estimate the Weibull shape parameter. If the slope of the true plotted line is greater than unity, then the corresponding distribution has a (single) mode, and the implication is that the hardware is wearing out and that the failure rate is increasing. By “failure rate” we mean the probability of failure in the next instant, given survival until that instant. We therefore conclude or hypothesize that in applications to recidivism in which the Weibull shape parameter is greater than 1, the subject’s intention to abstain (in- volving both physiological and psychological factors) is wearing out. Thus, as time goes on, the impact required to destroy the intention to abstain becomes less and less.
When the Weibull shape parameter is less than 1 (decreasing failure rate), one sees failure times ranging from very early to average combined with ex- tremely long ones. Samples of electronic equipment often exhibit this kind of failure pattern. In a random sample of a dozen television sets, for example, a few may fail early because of loose connections, faulty components, etc., but most will operate for hundreds of hours before exhibiting any kind of failure. This is a type of mixture involving some pieces of equipment with parts that wear out very early, mixed with sample elements that are devoid of such quality defects.
This kind of behavior in an addict sometimes appears to be manifested as a result of a treatment program that occasionally makes a strong impact but some- times fails completely. And, if a subject whose failure data are of this type ab- stains for a rather moderate period of time, one might predict that there is a high probability that he or she will abstain for an extended period.
When the Weibull shape parameter is unity, then failure is purely cata- strophic or random. In this special case, the distribution is exponential and the failure rate is constant. Some electronic systems that have been “burnt in” (i.e., operated long enough to eliminate the early failure modalities) exhibit this type of failure behavior. Exponential failure data for an addict might imply a lack of commitment to abstain. In this case the addict apparently responds with- out resistance to random stresses and traumas that occur as a homogeneous Pois- son process.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

32 MANN, CHARUVASTRA, AND MURTHY
Table 1
Sources of Data ~~
Methadone Baltimore Newark Types of data patients community residents
Periods of abstinence from opiates
Periods of using opiates
Background and demographic in- formation
Information related to motivational levels
Urinalysis records
Urinalysis records
Patient records
Intensive interviews
Records from intensive interview combined with police reports, peer and family follow-up
Same as above
Same as above
Patient records indi- cating treatment periods premature- ly terminated
Patient records indi- cating periods out of treatment fol- lowing premature termination-be fore return for new treatment
Patient records
The three different samples are representative of completely different di- verse populations engaging in three different types of recidivism activities and would ordinarily not be compared (see Table 1). The Brentwood and Baltimore samples include only males, while the Newark patients are of both sexes. Each Brentwood patient is exposed to a single type of treatment (methadone), but for each of a large number of the Baltimore and Newark clients, there are several treatment modalities. Still, all of the various patterns that have been discussed- that is, single distributions, mixtures, and increasing, constant, and decreasing failure rate-were exhibited in all three of the plotted individual time-to-relapse data sets. There is no outstanding feature of the individual failure patterns that characterizes the different populations except that the number of relapse and re- mission periods exhibited per individual tends to be larger for the methadone clients than for the other subjects. The principal cause for this may be the ease with which the methadone client may terminate periods of using, so that fears ordinarily associated with detoxifying do not aid in deterring reinitiation of use.
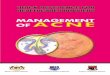
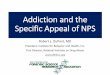
Figures 1 and 2 give the times to relapse and the associated graphical plots for two methadone patients. One sees for each, two different wear-out distribu- tions with distinctly different average failure times. In Fig. 2 there is a single observation significantly longer than the others (suggesting a very much stronger motivation associated with this remission period). Analytical methodologies
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

RELAPSE AND REMISSION TIME 33
3.00
2.00
1.00
h - . 0.00
? .- I - r
r; -1.00 - -c
E -
-2.00
-3.OC
-4.00
J INCREASING
ORDER
/;::OF OBS T DAYS T
1 24 4 2 71 6 3 42 7 4 4 22 5 24 24 6 6 24 7 89 42 8 67 42 9 22 54
10 56 56 1 1 42 67 12 7 71 13 54 89
I I I I I 1 0 1.00 2.00 3.00 4.00 5.00 6.00
In(&
Fig. 1. Subject ME 6 : Weibull probability plot of time until drug relapse.
(Fertig et al., 1980; Mann, 1982) have recently been developed for testing for statistical significance of suspected outliers, such as this single large observation, and for testing whether a next period of remission (after initiation of a new treatment program) is significantly longer than to be expected. Typically, as shown in Figs. 1 and 2, the slope of a second line is smaller than the first when the first is associated with very early failure.
The time-to-failure data from the Baltimore study were stored as numbers of months, so that it is impossible to tell, for these subjects, the type of behavior exhibited for the period extending less than 1 month after detoxification.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

34
4.00.
3.00.
2.00.
- 1.00 - ZI
m =, 0.00
. -
r Y
C - -c
C - -1.00
-4.00
-2.00
-3.00
-r I I I
MANN, CHARUVASTRA, AND MURTHY
NUMBER OF DAYS
ORDER OF INCREASING OCCURRENCE ORDER
085 T T
1 2 3 4 5 6 7 8 9
10 1 1 12 13 14 15
25 1 1 8 21 35 27 28 14 4
42 6 9 15 8
I I6
4 5 6 7 7 7 8 8
NUMBER OF DAYS
ORDER OF INCREASING OCCURRENCE ORDER
OBS T
16 56 15 17 44 18
20 13 25 t 21 5 26 I. 22 49 27
i 23 8 ne 24 21 35 25 7 4 2 26 7 42 27 18 44 28 8 49 29 42 56 30 10 116
Fig 2. Subject ME 18: Weibull probability plot of time until drug relapse.
Figures 3 and 4 give the time-to-relapse data and the associated probability plots of two Baltimore heroin addicts. The subject of Fig. 3 exhibits a decreasing failure rate pattern. For this individual there is a strong probability of a very long current period of remission when the current period has exceeded 2 months. The subject whose data are plotted in Fig. 4 exhibits two inordinately long periods of abstinence.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

RELAPSE AND REMISSION TIME 35
3.00
2.00.
1 .oo,
-L- - ZI . 0.00
LD. - . - I - F
y -1.00, - - t -
-2.00
-3.00
-4.00. 0
NUMBER OF D A Y S
ORDER OF INCREASING OCCURRENCE ORDER
OBS T T
1 I8 I 8 2 74 31 3 76 74 4 31 76 5 91 91
I I 1 10 1.00 2.00 3.00 4.00 5.b0 6.00 7.00
fnfI)o
Fig. 3. Baltimore, subject 27: Weibull probability plot of time until drug relapse.
The successive premature treatment termination times for subject 2870 of the New Jersey Medical School study are shown in Fig. 5. The probability plot indicates that the patient tends to wear out after a treatment period has lasted about 1 to 3 months.
Figure 6 gives data pertaining to periods of relapse (periods of use of heroin) and the resulting plot for a typical methadone client among those who exhibited sufficient recidivism so that the time-to-remission patterns could be identified. Note the several twists and turns.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

36
-2.00-
-3.00-
-4.00-t
MANN, CHARUVASTRA, AND MURTHY
8 8 29 9 57 57
1 I 1 I 1 1 t
'1 1.0
INCREASING ORDER OF OCCURRENCE ORDER
085 T
8 / ; 2: I 6 10 3 10 I 1 4 22 16 5 29 20 6 1 1 22 7 20 23
Fig. 4. Baltimore, subject 104: Weibull probability plot of time until drug relapse.
Characterization of the Recidivism Process
Probably the most important implication of this study results from the fact that when different failure mechanisms operate within a single individual, the time-to-relapse data plot as mixtures of distributions, rather than as competing- risk distributions. The fact that a competing-risk model does not apply to this kind of data suggests that if an addict exhibits, for example, two distinct types of failure patterns with very different average failure times, the resulting patterns are exhibited only because there are two completely different types of motiva- tion, like two different types of hardware. In other words, the intention that is
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

RELAPSE AND REMISSION TIME 37
3.00
2.00
1 .oo
0.00.
- I
c - -c c -
-2.00,
-3.00
-4.00,
-5.00, 0
NUMBER OF D A Y S
ORDER OF INC RE AS1 NG OCCURRENCE ORDER
00s T T
87 36 2 36 47 3 92 8 7 4 47 92
I I I I 10 1.00 2.00 3.00 4.00 5.bO 6.b0
In(L)o
Fig. 5. Newark, subject 2870: Weibull probability plot of time until drug relapse.
creating the abstinence is associated with one of the two patterns of failure: one that is early, on the average, and one that is late, on the average. It is this fact that demonstrates that the most important factor in determining expected length of abstinence of a subject is the type of motivation that is operating.
In the case of wear-out, we draw an analogy between the razor blades, which a subject selects repeatedly and randomly from one or more prescribed
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

38 MANN, CHARUVASTRA, AND MURTHY
t I 1 I I I I I I I I I
/ ' NUMBER OF D A Y S
f' ORDER OF INCREASING OCCURRENCE ORDER
OBS T T
1 21 5 2 9 5 3 1 5 5 4 7 6 5 9 6
L 6 5 6
f ' 7 IS 7 8 1 1 7 9 5 7
1 10 6 8
I1
.. 1 1 17 8 12 16 8
/ I 13 6 9 14 20 9 15 7 1 1 16 20 15 17 19 15 I8 21 16
I 19 6 17
1
20 7 19 21 22 20 22 62 20 23 28 21 24 8 21 25 8 21 26 5 22 27 8 28 28 21 62
In TIME
Fig. 6. Extent of time using heroin: plot of methadone patient 53. Numbers on curve indi- cate the number of observations at the given intersection.
populations after wear-out of a blade used previously, and the intentions of an addict to abstain from use of heroin. (For failure patterns characterized by other than wear-out, another hardware analogy may be more appropriate.) The inten- tions are very often formed repeatedly after extinction of a previous intention and appear, from the data, to be independent of previous responses, long and short periods being apparently randomly intermixed with those of more or less average length. One never sees a clear-cut trend toward either longer or shorter duration of remission periods. (See, e.g., the data in Figs. 1-5.) The fact that data for individual addicts plot as would failure data from random samples from three or fewer specific types of hardware corroborates an assumption of inde- pendence of events.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

RELAPSE AND REMISSION TIME 39
Thus, what is observed here is not a nonhomogeneous Poisson process indi- cating a tendency toward gradual increase or decrease in time to failure through- out the history of the addiction. Such a process would suggest that the recidivism phenomenon involves something like “repair” of the addict before returning to using and continuation of a trend (Crow, 1974). In fact, only in the special case of exponential data resulting from a homogeneous Poisson process (for whch we hypothesize a lack of intention) might one interpret the recidivism phenomenon as one involving repair before return to use. For exponential data, even when conceptualized as resulting from a failure and re- pair process, there is no trend in either direction. Hence, in general, one cannot use a single most recent failure time to predict a next failure time for an indi- vidual, except in a special situation in which an individual exhibits extreme wear- out. (In such a case the addict might always terminate periods of abstinence after some fixed period of time, plus or minus a very small percentage of that period, as long as his or her motivational level was not dramatically changed.)
On the other hand, if one examines results of analysis of the methadone program data set (which has received the most thorough scrutiny in this study to date), one sees that some individuals do improve with respect to length of period of abstinence in an unexpected and subtle way. As noted earlier, failure times for each methadone patient moved more or less randomly within each of the patterns (as many as three) that he or she exhibited, as well as between pat- terns. Nevertheless, there appeared to be a tendency over calendar time for the patient population to experience fewer of the short-term failure times (9 most recent failure times vs 23 times to first failure out of each total sample of 88 that were less than 21 days-significant at the .006 level) and more of the ex- tremely long-term failure times (16 most recent failure times vs 5 first failure times greater than 665 days-significant at the .03 level).
The overall mean time to failure increased from 196 days to 366 days, but the proportion of the sample that experienced failure times that were of moderate average length stayed relatively constant. For the razor blade analogy, one can assume that later deliveries to a retail outlet contain fewer blades with extremely short lives and more that last an extremely long time.
Lengths of periods of using heroin by the methadone patients exhibited the same sort of random variation as did lengths of periods of abstinence. However, the sample median for both time of first use and time of most recent use was 8 days, and the mean times of using were 1 1.3 and 1 1.7 days, respectively. That is, improvement in the recidivism behavior reflected in the increase in number of longer periods of abstinence was not reciprocated by a corresponding improve- ment (decrease) in the duration of periods of use. This gives corroboration to intuitive feelings that lengths of periods of using drugs are not useful in measuring performance since they are often terminated by random events com- pletely out of the control of the addict.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

40 MANN, CHARWASTRA, AND MURTHY
Uninternalized Motivation
Further corroboration (in addition to the interview data) of the interpreta- tion, stated earlier, concerning unintemalized motivation is given by the follow- ing. Probation and other legal restraints on the methadone patients upon entering the program were highly predictive of a time to first failure in the early range, that is, less than 21 days (15 patients out of 39 on probation vs 8 out of 49 not on probation-significant at the .02 level). Presence or absence of these early legal restraints, however, had essentially no effect on the graphical plots (number of early failures, slopes of the three lines, mean, etc.) of time to longest failure or time to most recent failure, both of which sometimes occurred sev- eral years after the patient entered the methadone program. For example, the probation and nonprobation data sets for time to most recent failure both exhibited approximately 10% failure times less than 21 days and had a mean time to failure of 367 and 365 days, respectively.
The implication of legal restraint being often associated with uninternalized motivation is not in conflict with that of earlier research (Desmond and Maddux, 1977; Vaillant and Rasor, 1966) which compared addicts on probation with those that appeared to be unmotivated. What is suggested here is that although law enforcement agencies exacerbate the difficulties of the addict in coping with his or her habit, and thus add pressure for at least temporary wear-out of drug use, their coercion is ineffective in producing internalized motivation for main- taining abstinence (except perhaps in their cumulative effect on feelings of dysfunction).
This phenomenon is in agreement with results of previous research (Zander and Curtis, 1962) which found that, in an experiment, high school boys evi- denced a weaker motivation to do well on a group task when they were sub- jected to the threat of being expelled from the group than when no threats were employed. It has been demonstrated by recent research in the field of personality (Carver and Scheifer, 1981) that excessive coercion may lead to aversion, movement away from the communicator's idea, while gentle persuasion may move one into closer agreement with the communicator. It seems that at- tempted influence causes psychological reactance, a motivational state which oc- curs when an individual's freedom is threatened. Reactance, hence, causes an at- tempt to reassert the threatened freedom.
RECOMMENDATIONS
Motivating the Patient
A rather clear implication of this analysis is that a necessary ingredient of any really successful drug treatment program is a method of strongly motivating
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

RELAPSE AND REMISSION TIME 41
the patient to want to abstain and to want to maintain any modifications of be- havior or changes in environment and life-style that help him or her to abstain. It also suggests that the use of willpower alone (i.e., simply “trying hard”) in fighting return to use of a drug dooms the subject to eventual failure unless he or she is profoundly motivated during the period of abstinence in which the will- power is being exerted.
Obviously, a treatment facility has no control over most of the motivating factors mentioned earlier, such as, for example, parenting. There are some such factors, however, that treatment personnel can conceivably influence. For ex- ample, it may be possible to intensify the patient’s awareness of the dysfunction caused by use of heroin and/or his or her awareness of other behavior options available to him or her besides use of drugs and to demonstrate the incongruence between a patient’s behavior and his or her goals and values. Also, it may be possible to initiate insightful experiences so that use of heroin is then seen to be an undesirable, or at least a less desirable, activity.
Given these goals, one may ask how to go about achieving them. Results of the present study, combined with previous research (Brill, 1977; Simmell, 1948), give us several valuable clues. Interview responses demonstrate that instances in which addicts have had eureka experiences, spiritual experiences, or any other kinds of experiences that have turned their lives around have often been times of withdrawal from drugs. The time of withdrawal and detoxification is usually one during which the addict experiences feelings of hitting bottom and has the po- tential for surrender and a commitment to abstinence. Altered states of consciousness and the physical trauma caused by the chemical detoxification can intensify this potential. This suggests that treatment effects can be enhanced if a significant part of treatment resources are allocated to very early stages of treat- ment, beginning with detox.
Using the Methodology to Predict Behavior
Most recidivism studies measure only time to first failure (e.g., relapse, re- turn to prison) or number of subjects who have failed after some specified period following “treatment.” On the basis of such measurement, some investi- gators have Characterized subjects in terms of their levels of responsiveness. This study makes clear that length of time before relapse to undesirable habitual be- havior does not characterize an individual, but rather temporarily characterizes the motivational level of an individual.
Thus, neither the most recent period of relapse nor, as stated earlier, any other one single previous period of relapse can be used to predict how an indi- vidual will tend to respond following detoxification. An individual’s hstory of time to relapse, however, will allow one to determine (1) how long a next period of remission must be before it can be considered significantly different from
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

42 MA”, CHARUVASTRA, AND MURTHY
previous ordinary behavior and (2) if and under what conditions treatment effects were experienced in the past. The latter can be used to direct treat- ment.
To facilitate this sort of analysis, the senior author (N.R.M.) has developed special graphical plotting papers (each one appropriate for a specified number of times to relapse) for plotting the individual historical time-to-relapse data. Using these plots, one can identify failure patterns, identify instances of treatment ef- fects, and predict future recidivism behavior. The recidivism data can be solicited by means of a questionnaire (which is also available from the senior author, along with suggestions for its administration). The two publications (Fertig et al., 1980; Mann, 1982) give procedures for detecting, respectively, past and present potential treatment effects by means of the probability plots. Use of this methodology requires staff training and/or a good understanding of survival analysis techniques.
Using the Methodology in Selecting Experimental Samples
One important byproduct of this study is the identification of a method for selecting two experimental groups who are to receive treatment for elimination or alleviation of their addictive behavior. This has been a problem in the past be- cause of difficulties involved in making sure that one of the populations does not exhibit an imbalance with respect to some concomitant variable that could possibly influence outcome.
Although extent of “time to most recent relapse” cannot be used to charac- terize an individual, the distribution of such relapse times and the parameters of this distribution can be used to characterize the current motivational level of a population at any given time, such as before treatment. Thus, we saw earlier that the two groups who were identified as being with or without legal restraints upon entry into the methadone program exhibited sample distributions of time to first failure that were significantly different and distributions of time to most recent failure (occurring in general after elimination of the legal restraints) that were without discernible differences. It seems appropriate to conclude (on the basis of comparison of probability plots and sample parameters) that after some initial period of exposure to the program, the distributions of motivational levels of the two groups were identical for all practical purposes. If such a near equiv- alence can be established for two experimental groups in terms of their most recent relapse experience before entry into an experimental program, then it is only necessary to ensure that, aside from experimental parameters that are to be varied, there are no systematic differences in dealing with the two groups by treatment personnel or legal authorities. If the two groups are large enough, ex- ternal motivational factors will tend to balance out within and between the two populations. Thus, a question relating to “length of most recent period of ab-
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

RELAPSE AND REMISSION TIME 43
stinence" should be added to patient intake forms, even when more extensive abstinence histories are not solicited.
ACKNOWLEDGMENT
Financial support was given by grants lH81DA02118-01 and -02 from the National Institute on Drug Abuse.
REFERENCES
BRILL, L. The De-Addiction Process. Springfield, IL: C. C. Thomas, 1972. BRILL, L. The treatment of drug abuse: Evolution of a perspective. A m J. Psychiatry
CARR-HILL, G.A., and CARR-HILL, R.A. Reconviction as a process. Br. J. Criminol.
CARVER, C.S., and SCHEIFER, M.F. Self-consciousness and reactance. J. Res. Pers. 15:
CROW, L.H. Reliability analysis for complex repairable systems. In F. Proschan and R.J. Serfling (eds.), Reliability and Biometry. Philadelphia: Society for Industrial and A p plied Mathematics, 1974.
DESMOND, D.P., and MADDUX, J.F. The effect of probation on behavior of chronic opioid drug users. Contemp. DrugProbl. Spring 1977, pp. 41-58.
FERTIG, K.W., MEYER, M.E., and MANN, N.R. On constructing prediction intervals for samples from a Weibull or extreme-value distribution. Technometrics 22: 567-573, 1980.
KAO, J.H.K. A graphical estimation of mixed Weibull parameters in life testing of electron tubes. Technometrics 1:389-407, 1959.
KIERKEGAARD, S. Fear and Trembling. Princeton, NJ: Princeton University Press, 1941a. KIERKEGAARD, S . The Sickness unto Death. Princeton, NJ: Princeton University Press,
1941b. LAVENHAR, M., SHEFFET, A., DUVAL, H., and LOURIA, D. The New Jersey Medical
School narcotics case register: Methodology and summary of first four years of opera- tion. Addict. Dis. l(4): 513-527, 1975.
LING, W., and CHARUVASTRA, C. Methadyl acetate and methadone as maintenance treatments for heroin addicts. Arch. Gen. Psychiatry 33: 709-720, 1976.
MANN, N.R. Use of life-test data analysis methodology for analyzing undesirable habitual behavior. George Washington University School of Engineering and Applied Science Institute for Management Science and Engineering, Serial T-406, July 1979.
MANN, N.R. Optimal outlier tests for a Weibull model-To identify process changes or to predict failure times. In J.S. Rustagi and S. Zanakis (eds.), Optimization in Statistics. North-Holland, 1982.
M A " , N.R., and ROTHBERG, J. Using life-test data analysis rnethodologv to think about human behavior. Presented at TIMS/ORSA Annual Meeting, Washington, DC, May 5- 7, 1980.
MANN, N.R., SCHAFER, R., and SINGPURWALLA, N. Methods for StatisticalAnalysis o f Reliability and Life Data. New York: Wiley, 1974.
NURCO, D.N., BONITO, A.J., LERNER, M., and BALTER, M.B. Studying addicts over time: Methodology and preliminary findings. Am. J. Drug Alcohol Abuse 2(2): 183- 196, 1975.
134(2): 157-160, 1977.
12: 35-43, 1972.
16-29, 1981.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.

44 MANN, CHARUVASTRA, AND MURTHY
SIMMEL, E. Alcoholism and addiction. Psychoanal. Q. 17: 6-31, 1948. SIMPSON, D.D., SAVAGE, L.J., LLOYD, N.R., and SILLS, S.B. Evaluation ofdrugabuse
treatments bused on the first year after DARP: National followup study of admissions to drug abuse treatments in DARPduring 1969-1 972. Institute of Behavioral Research Report No. 77-1 0, Texas Christian University, 1977.
VAILLANT, G.E., and RASOR, R.W. The role of compulsory supervision in the treatment of addiction. Fed. Probation 30: 53, June 1966.
WALDORF, D. Careers in Dope. Englewood Cliffs, NJ: Prentice-Hall, 1973. WALDORF, D., and BIERNACKI, P. Natural recovery from heroin addiction: A review of
ZANDER, A., and CURTIS, T. Effects of social power on aspiration setting and striving. the incidence literature. J. Drug Issues 9(2), 1979.
J. Abnorm. Soc. Psychol. 64: 63-67, 1962.
Subs
t Use
Mis
use
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f A
uckl
and
on 1
1/02
/14
For
pers
onal
use
onl
y.