Embed Size (px)
Citation preview
Ankita Rathi, et al., BAOJ Dentistry 2017, 3: 12: 027
BAOJ Dentistry
Case Report
BAOJ Dentistry, an open access journal Volume 3; Issue 1; 027
*Corresponding author: Ankita Rathi, Lecturer, Nobel Medical College and Teaching Hospital Dentist, Ganpati Clinic Hospital Chowk Birat-nagar 12Nepal Email: [email protected]
Sub Date: 13 March, 2017, Acc Date: 3 April, 2017, Pub Date: 3 April, 2017.
Citation: Ankita Rathi, Kanchana Shrestha and Suraj Ram Bhakta Math-ema (2017) Prosthetic Management of Patient with Hereditary Ecto-dermal Dysplasia. BAOJ Dentistry 3: 027.
Copyright: © 2017 Ankita Rathi, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution Li-cense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Prosthetic Management of Patient with Hereditary Ectodermal DysplasiaAnkita Rathi1*, Kanchana Shrestha2 and Suraj Ram Bhakta Mathema3
1Lecturer, Department of Prosthodontics, Nobel Medical College and Teaching Hospital2Assistant Professor, Department of Prosthodontics, Peoples Dental College and Teaching Hospital
3Professor and Head of Department, Department of Prosthodontics, Peoples Dental College and Teaching Hospital
AbstractEctodermal dysplasia is a hereditary condition characterized by absence or defect in the structure of ectodermal origin. A 16 year old female presented to our department with some of her teeth missing and desiring of replacement with artificial substitute. Since the patient was young, minimally invasive mode of treatment in the form of flexible denture was opted so that the growth is not interfered and patient can be reviewed and adjustment could be done in follow up till further definitive form of treatment can be rendered.
IntroductionEctodermal dysplasia (ED) represents a large group of inherited disorders characterized by a primary defect in the structures of ectodermal origin [1]. It was first reported in a paper by Thurman in 1848. The term “Ectodermal Dysplasia” was coined by Weech in 1929 [2,3].
ED represents a large and complex group of diseases comprising more than 170 different clinical conditions. Its Prevalence is estimated to be 7 cases in 10000 births [4]. It is a genetic anomaly, which can be inherited through either parents or manifested via gene mutations [5].
Two different entities of hereditary ectodermal dysplasias have been reported; the Hidrotic (Clouston’s syndrome) and Hypohidrotic/ Anhydrotic (Christ-Siemens-Touraine syndrome) forms. The difference between the two is in terms of sweat gland manifestations. Hidrotic ectodermal dysplasia has an autosomal dominant inheritance where sweat glands are normal which are absent in Anhidrotic ectodermal dysplasia [6,7].
An hydrotic ectodermal dysplasia is a rare X-linked condition characterized by the classical triad of hypodontia, hypohidrosis and hypotrichosis. These patients generally have prominent supraorbital ridges, frontal bossing, and a saddle nose. The maxillae may be underdeveloped and the lips thick and prominent. The nose may appear pinched, and the alae nasi hypoplastic. The patient may resemble an edentulous old person. Some patients do not produce tears. The nails are usually normal. The skin of an infant may appear hypo pigmented. Maculopapular eruptions may occur during infancy. The characteristic dental defect in this syndrome is peg-shaped or conical front teeth, which cannot be
distinguished from incisors. Both the deciduous and permanent teeth are affected. Anodontia may occur, but hypodontia with misshapen teeth is common, and these teeth may be hypoplastic [8].
In these patients, the appearance is extremely important since it ultimately affects their self esteem. Therefore prosthetic treatment is of great value for these patients for functional, psychologic as well as psychosocial point of view. The most frequent prosthetic treatment for the dental management of ED is removable prosthodontics.
`This clinical report describes about the non invasive approach for the prosthodontic management of a young patient with an hydrotic ectodermal dysplasia.
Case ReportA 16 year old female presented to department of prosthodontics with the complaint of unaesthetic appearance due to missing teeth. There was no history of extraction of teeth in the past. The patient also gave history of lack of sweating and dryness of skin.
Extra oral Examination revealed sparse hair, frontal bossing, depressed nasal bridge, protuberant lips and loss of facial height.
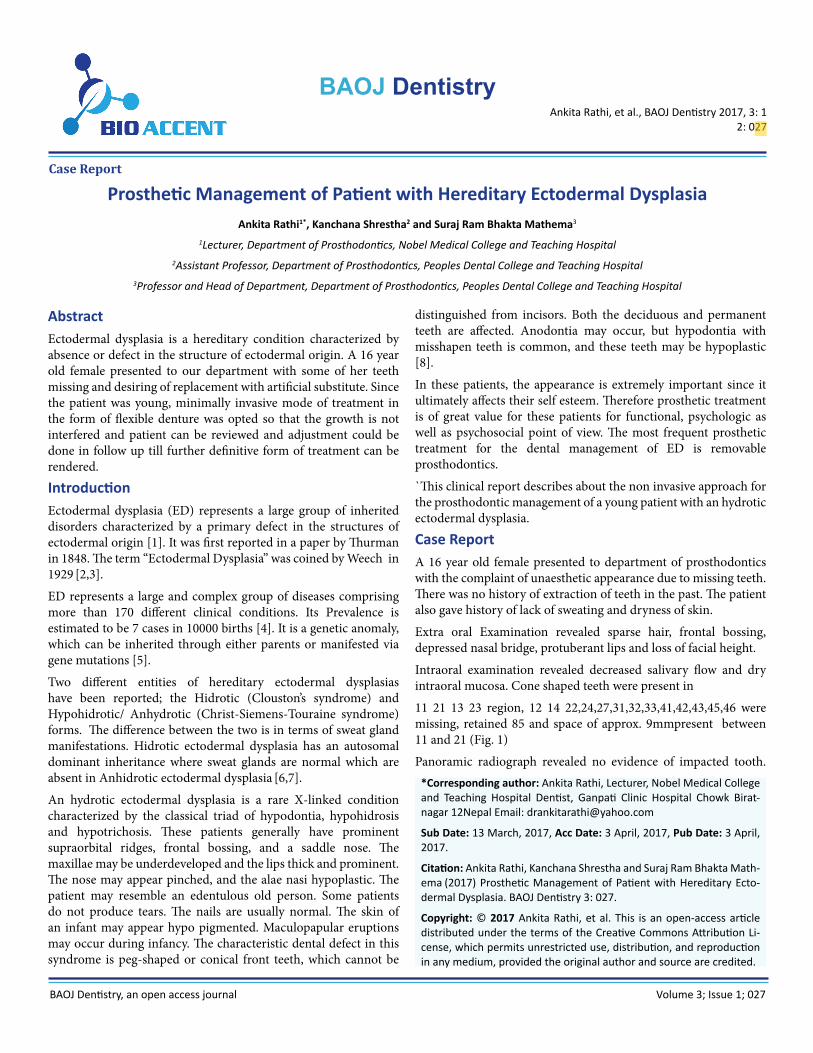
Intraoral examination revealed decreased salivary flow and dry intraoral mucosa. Cone shaped teeth were present in
11 21 13 23 region, 12 14 22,24,27,31,32,33,41,42,43,45,46 were missing, retained 85 and space of approx. 9mmpresent between 11 and 21 (Fig. 1)
Panoramic radiograph revealed no evidence of impacted tooth.
Citation: Ankita Rathi, Kanchana Shrestha and Suraj Ram Bhakta Mathema (2017) Prosthetic Management of Patient with Hereditary Ectodermal Dysplasia. BAOJ Dentistry 3: 027.
Page 2 of 3
BAOJ Dentistry, an open access journal Volume 3; Issue 1; 027
Since the patient was young and not willing for orthodontic treatment, minimal invasive approach was selected for prosthetic rehabilitation. Maxillary left and right
Fig. 1. Pretreatment presentation of the patient
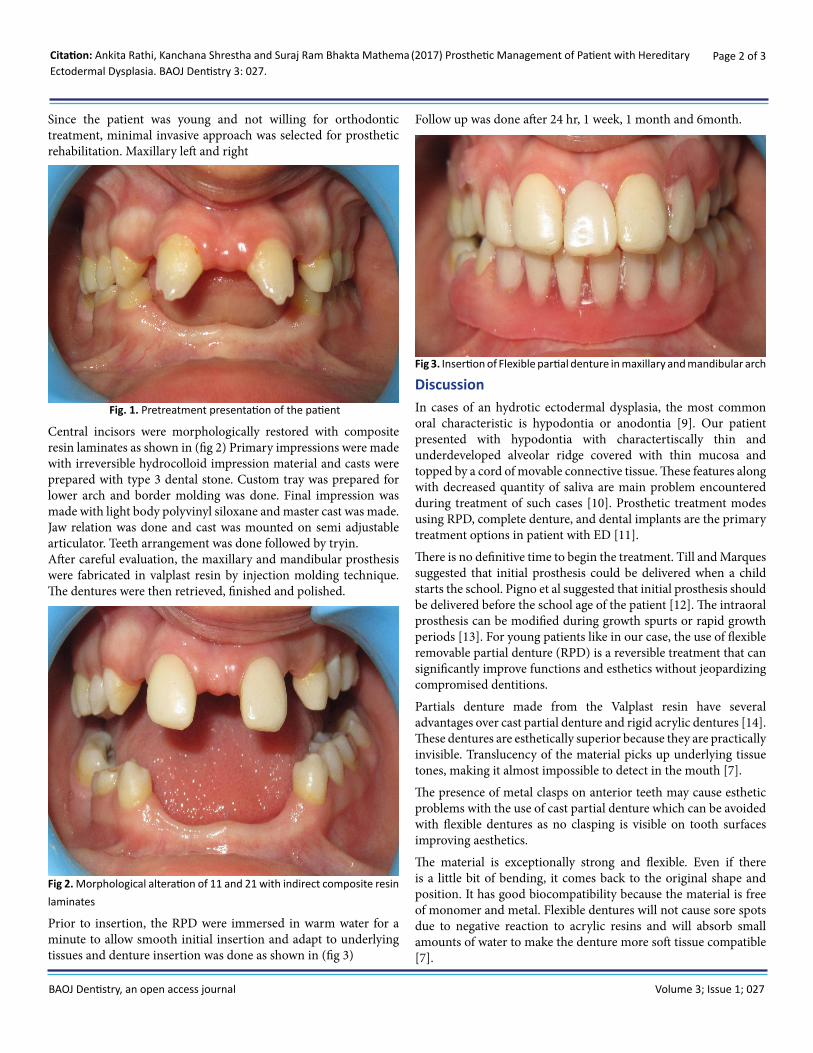
Central incisors were morphologically restored with composite resin laminates as shown in (fig 2) Primary impressions were made with irreversible hydrocolloid impression material and casts were prepared with type 3 dental stone. Custom tray was prepared for lower arch and border molding was done. Final impression was made with light body polyvinyl siloxane and master cast was made. Jaw relation was done and cast was mounted on semi adjustable articulator. Teeth arrangement was done followed by tryin.After careful evaluation, the maxillary and mandibular prosthesis were fabricated in valplast resin by injection molding technique. The dentures were then retrieved, finished and polished.
Fig 2. Morphological alteration of 11 and 21 with indirect composite resin laminates
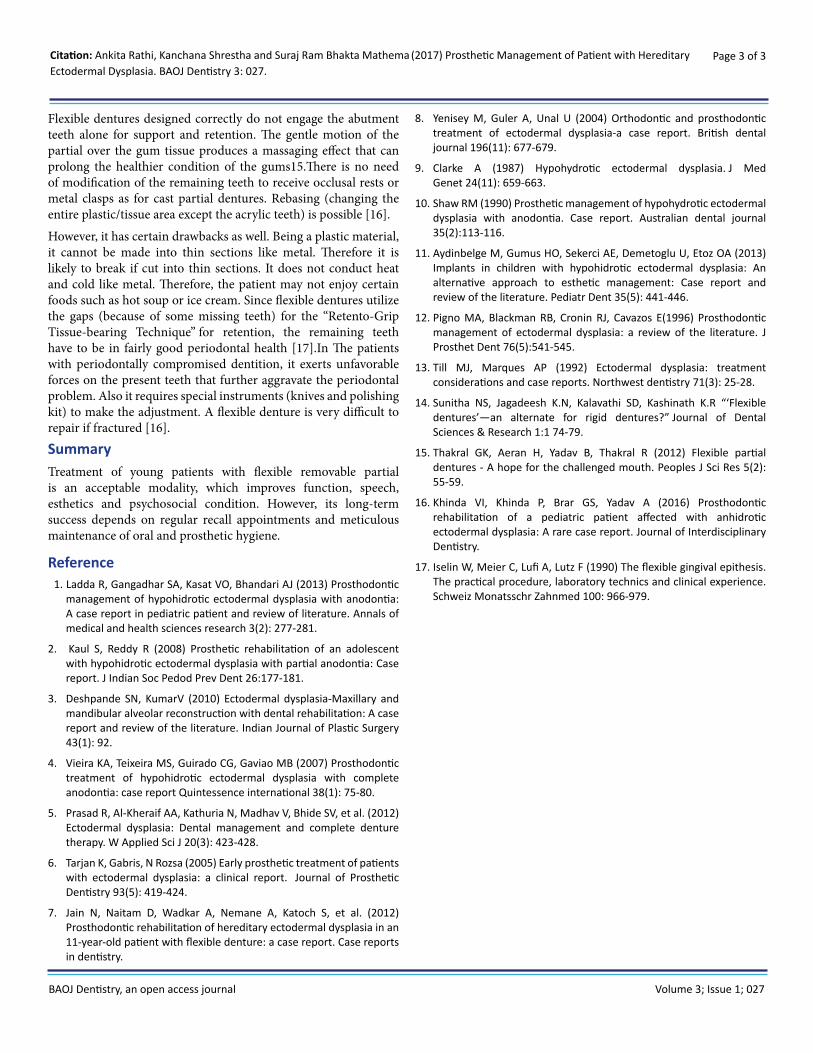
Prior to insertion, the RPD were immersed in warm water for a minute to allow smooth initial insertion and adapt to underlying tissues and denture insertion was done as shown in (fig 3)
Follow up was done after 24 hr, 1 week, 1 month and 6month.
Fig 3. Insertion of Flexible partial denture in maxillary and mandibular arch
DiscussionIn cases of an hydrotic ectodermal dysplasia, the most common oral characteristic is hypodontia or anodontia [9]. Our patient presented with hypodontia with charactertiscally thin and underdeveloped alveolar ridge covered with thin mucosa and topped by a cord of movable connective tissue. These features along with decreased quantity of saliva are main problem encountered during treatment of such cases [10]. Prosthetic treatment modes using RPD, complete denture, and dental implants are the primary treatment options in patient with ED [11].
There is no definitive time to begin the treatment. Till and Marques suggested that initial prosthesis could be delivered when a child starts the school. Pigno et al suggested that initial prosthesis should be delivered before the school age of the patient [12]. The intraoral prosthesis can be modified during growth spurts or rapid growth periods [13]. For young patients like in our case, the use of flexible removable partial denture (RPD) is a reversible treatment that can significantly improve functions and esthetics without jeopardizing compromised dentitions.
Partials denture made from the Valplast resin have several advantages over cast partial denture and rigid acrylic dentures [14].These dentures are esthetically superior because they are practically invisible. Translucency of the material picks up underlying tissue tones, making it almost impossible to detect in the mouth [7].
The presence of metal clasps on anterior teeth may cause esthetic problems with the use of cast partial denture which can be avoided with flexible dentures as no clasping is visible on tooth surfaces improving aesthetics.
The material is exceptionally strong and flexible. Even if there is a little bit of bending, it comes back to the original shape and position. It has good biocompatibility because the material is free of monomer and metal. Flexible dentures will not cause sore spots due to negative reaction to acrylic resins and will absorb small amounts of water to make the denture more soft tissue compatible [7].
Citation: Ankita Rathi, Kanchana Shrestha and Suraj Ram Bhakta Mathema (2017) Prosthetic Management of Patient with Hereditary Ectodermal Dysplasia. BAOJ Dentistry 3: 027.
Page 3 of 3
BAOJ Dentistry, an open access journal Volume 3; Issue 1; 027
Flexible dentures designed correctly do not engage the abutment teeth alone for support and retention. The gentle motion of the partial over the gum tissue produces a massaging effect that can prolong the healthier condition of the gums15.There is no need of modification of the remaining teeth to receive occlusal rests or metal clasps as for cast partial dentures. Rebasing (changing the entire plastic/tissue area except the acrylic teeth) is possible [16].
However, it has certain drawbacks as well. Being a plastic material, it cannot be made into thin sections like metal. Therefore it is likely to break if cut into thin sections. It does not conduct heat and cold like metal. Therefore, the patient may not enjoy certain foods such as hot soup or ice cream. Since flexible dentures utilize the gaps (because of some missing teeth) for the “Retento-Grip Tissue-bearing Technique” for retention, the remaining teeth have to be in fairly good periodontal health [17].In The patients with periodontally compromised dentition, it exerts unfavorable forces on the present teeth that further aggravate the periodontal problem. Also it requires special instruments (knives and polishing kit) to make the adjustment. A flexible denture is very difficult to repair if fractured [16].
SummaryTreatment of young patients with flexible removable partial is an acceptable modality, which improves function, speech, esthetics and psychosocial condition. However, its long-term success depends on regular recall appointments and meticulous maintenance of oral and prosthetic hygiene.
Reference1. Ladda R, Gangadhar SA, Kasat VO, Bhandari AJ (2013) Prosthodontic
management of hypohidrotic ectodermal dysplasia with anodontia: A case report in pediatric patient and review of literature. Annals of medical and health sciences research 3(2): 277-281.
2. Kaul S, Reddy R (2008) Prosthetic rehabilitation of an adolescent with hypohidrotic ectodermal dysplasia with partial anodontia: Case report. J Indian Soc Pedod Prev Dent 26:177-181.
3. Deshpande SN, KumarV (2010) Ectodermal dysplasia-Maxillary and mandibular alveolar reconstruction with dental rehabilitation: A case report and review of the literature. Indian Journal of Plastic Surgery 43(1): 92.
4. Vieira KA, Teixeira MS, Guirado CG, Gaviao MB (2007) Prosthodontic treatment of hypohidrotic ectodermal dysplasia with complete anodontia: case report Quintessence international 38(1): 75-80.
5. Prasad R, Al-Kheraif AA, Kathuria N, Madhav V, Bhide SV, et al. (2012) Ectodermal dysplasia: Dental management and complete denture therapy. W Applied Sci J 20(3): 423-428.
6. Tarjan K, Gabris, N Rozsa (2005) Early prosthetic treatment of patients with ectodermal dysplasia: a clinical report. Journal of Prosthetic Dentistry 93(5): 419-424.
7. Jain N, Naitam D, Wadkar A, Nemane A, Katoch S, et al. (2012) Prosthodontic rehabilitation of hereditary ectodermal dysplasia in an 11-year-old patient with flexible denture: a case report. Case reports in dentistry.
8. Yenisey M, Guler A, Unal U (2004) Orthodontic and prosthodontic treatment of ectodermal dysplasia-a case report. British dental journal 196(11): 677-679.
9. Clarke A (1987) Hypohydrotic ectodermal dysplasia. J Med Genet 24(11): 659-663.
10. Shaw RM (1990) Prosthetic management of hypohydrotic ectodermal dysplasia with anodontia. Case report. Australian dental journal 35(2):113-116.
11. Aydinbelge M, Gumus HO, Sekerci AE, Demetoglu U, Etoz OA (2013) Implants in children with hypohidrotic ectodermal dysplasia: An alternative approach to esthetic management: Case report and review of the literature. Pediatr Dent 35(5): 441-446.
12. Pigno MA, Blackman RB, Cronin RJ, Cavazos E(1996) Prosthodontic management of ectodermal dysplasia: a review of the literature. J Prosthet Dent 76(5):541-545.
13. Till MJ, Marques AP (1992) Ectodermal dysplasia: treatment considerations and case reports. Northwest dentistry 71(3): 25-28.
14. Sunitha NS, Jagadeesh K.N, Kalavathi SD, Kashinath K.R “‘Flexible dentures’—an alternate for rigid dentures?” Journal of Dental Sciences & Research 1:1 74-79.
15. Thakral GK, Aeran H, Yadav B, Thakral R (2012) Flexible partial dentures - A hope for the challenged mouth. Peoples J Sci Res 5(2): 55-59.
16. Khinda VI, Khinda P, Brar GS, Yadav A (2016) Prosthodontic rehabilitation of a pediatric patient affected with anhidrotic ectodermal dysplasia: A rare case report. Journal of Interdisciplinary Dentistry.
17. Iselin W, Meier C, Lufi A, Lutz F (1990) The flexible gingival epithesis. The practical procedure, laboratory technics and clinical experience. Schweiz Monatsschr Zahnmed 100: 966-979.


















![heapofbirds.ou.eduheapofbirds.ou.edu/Websites/heapofbirds/files/Content/… · · 2012-11-04the Lila Wallace/Readers Digest International Artist Fellowship. ... Songs video] Brenda](https://img.pdfslide.us/doc/110x75/5b04704e7f8b9a89208d9e08/2012-11-04the-lila-wallacereaders-digest-international-artist-fellowship-.jpg)









