Embed Size (px)
Citation preview

CLINICAL REPORT
A De Novo Supernumerary Genomic DiscontinuousRing Chromosome 21 in a Child With MildIntellectual DisabilityNicoletta Villa,1 Angela Bentivegna,2 Adam Ertel,3 Serena Redaelli,2 Carla Colombo,4
Renata Nacinovich,5 Fiorenza Broggi,5 Sara Lissoni,1 Silvia Bungaro,6 Sankar Addya,3 Paolo Fortina,3,7
and Leda Dalpr�a1,2*1Medical Genetics Laboratory, S. Gerardo Hospital, Monza, Italy2Department of Neuroscience and Biomedical Technologies, School of Medicine, University of Milano-Bicocca, Monza, Italy3Kimmel Cancer Center, Department of Cancer Biology, Thomas Jefferson University, Jefferson Medical College, Philadelphia, Pennsylvania4Neonatal Intensive Care Unit, S. Gerardo Hospital, Monza, Italy5Department of Child and Adolescent Neuropsychiatry, S. Gerardo Hospital, Monza, Italy6M. Tettamanti Research Center, Pediatric Clinic, University of Milano Bicocca, S. Gerardo Hospital, Monza, Italy7Department of Molecular Medicine, School of Medicine, University ‘‘La Sapienza’’, Rome, Italy
Received 12 November 2010; Accepted 17 February 2011
Small supernumerary marker chromosomes (sSMCs) are struc-
turally abnormal extra chromosomes that cannot be unambigu-
ously identified or characterized by conventional banding
techniques alone, and they are generally equal in size or smaller
than chromosome 20 of the same metaphase spread. Small
supernumerary ring chromosomes (sSRCs), a smaller class of
marker chromosomes, comprise about 10% of the cases. For
various reasons these marker chromosomes have been the most
difficult to characterize; although specific syndromes have not
yet been defined, 60% of cases are associated with an abnormal
phenotype. The chromosomal material involved, the degree and
tissutal distribution of mosaicism, and the possible presence of
uniparental disomy, are the important factors determining
whether or not the ring chromosome will give rise to symptoms.
Using conventional and molecular cytogenetics approaches we
identified a de novo chromosome 21 sSRC in a child with speech
delay and mild intellectual disability. By using aCGH analysis
and SNP arrays, we report the presence of two discontinuous
regions of chromosome 21 and the paternal origin of the sSRC. A
thorough neuropsychiatric evaluation is also provided. Only few
other cases of complex discontinuous ring chromosomes have
been described in detail. � 2011 Wiley-Liss, Inc.
Key words: ring chromosome 21; fluorescence in situ hybridiza-
tion (FISH); array-CGH
INTRODUCTION
Small supernumerary marker chromosomes (sSMCs) are structur-
ally abnormal extra chromosomes that cannot be unambiguously
identified or characterized by conventional banding techniques
and are generally equal in size or smaller than chromosome 20 on
the same metaphase spread [Liehr et al., 2004]. According to the
data reviewed by Liehr and Weise [2007], sSMCs were present in
0.075% of all analyzed prenatal cases but only in 0.044% of
consecutively studied postnatal ones. In infertile subjects,
0.125% were sSMC carriers (male/female rate 7.5:1). In develop-
mentally retarded patients the sSMC rate was elevated to 0.288%
Additional supporting information may be found in the online version of
this article.
Grant sponsor: Fondazione Cariplo; Grant sponsor: AIRC; Grant sponsor:
MIUR.
Nicoletta Villa and Angela Bentivegna contributed equally to this work.
*Correspondence to:
Leda Dalpr�a, M.D., Dipartimento di Neuroscienze e Tecnologie
Biomediche, School of Medicine, Universit�a degli Studi di Milano-
Bicocca, Via Cadore 48, 20052 Monza, MI, Italy.
E-mail: [email protected]
Published online 13 May 2011 in Wiley Online Library
(wileyonlinelibrary.com).
DOI 10.1002/ajmg.a.34010
How to Cite this Article:Villa N, Bentivegna A, Ertel A, Redaelli S,
Colombo C, Nacinovich R, Broggi F, Lissoni
S, Bungaro S, Addya S, Fortina P, Dalpr�a L.
2011. A de novo supernumerary genomic
discontinuous ring chromosome 21 in a child
with mild intellectual disability.
Am J Med Genet Part A 155:1425–1431.
� 2011 Wiley-Liss, Inc. 1425

[Liehr and Weise, 2007]. The small size of sSMCs prohibits
characterization by traditional banding techniques, and instead
requires molecular cytogenetic techniques, such as FISH or array-
based comparative genomic hybridization (aCGH), to determine
the chromosomal origin.
sSMC are scientifically interesting due to an incomplete under-
standing of their formation, karyotypic evolution, and the fact
that their presence may lead to chromatin imbalances (partial
tri-, tetra-, or hexasomies) without detectable clinical consequences
[Liehr et al., 2008]. Subjects with a supernumerary marker
chromosome have duplication and, in some cases, a triplication
of the material comprising the sSMC. The risk of an abnormal
phenotype associated with a randomly ascertained de novo sSMC
derived from acrocentric autosomes (excluding chromosome 15) is
approximately 7%, compared with approximately 28% for sSMC
derived from non-acrocentric autosomes [Crolla, 1998]. A collab-
orative study of 19 Italian laboratories involving 241 sSMCs
[Dalpr�a et al., 2005] has allowed definitive conclusions concerning
karyotype–phenotype correlations. These studies emphasize that
molecular characterization of sSMCs and their associated clinical
phenotypes can provide karyotype–phenotype correlations useful
for genetic counseling.
We report on a de novo small supernumerary ring chromosome
(sSRC) of paternal origin, derived from different regions of chro-
mosome 21, in a child with speech delay and mild intellectual
disability.
MATERIALS AND METHODS
CytogeneticsMetaphase chromosome preparations were obtained from PHA-
stimulated lymphocyte cultures of peripheral blood according to
standard procedures. Chromosome analysis was carried out apply-
ing QFQ banding according to routine procedures, and karyotypes
for the patient (50 metaphases) and for both parents (100 meta-
phases, each) were reconstructed following the guidelines of ISCN
2009 [Shaffer et al., 2009].
Fluorescence In Situ Hybridization (FISH)FISH was performed as previously reported [Lissoni et al., 2009]. To
characterize the sSMC, the following probes were applied: Pan-
centromeric, Pan-telomeric, D13Z1/D21Z1, beta-satellite, and
WCP for chromosome 21 (Oncor, Inc., Gaithersburg, MD). To
define the chromosome 21-derived euchromatic sequences, BAC
probes were applied: RP11-91N21, RP11-106K13, RP11-22D1,
RP11-61A21, RP11-97K13, RP11-78J18, RP11-242C13, RP11-
141K11, and RP11-89M24 (Wellcome Trust Sanger Institute,
Hinxton, Cambridge, UK).
Array-CGHGenomic DNA was extracted from patients’ lymphoblastoid
cultures by phenol–chloroform standard protocols and DNA con-
centration was determined on a NanoDrop ND-1000 spectropho-
tometer (NanoDrop Technologies, Berlin, Germany). Gene copy
number analysis was performed by aCGH using Agilent Human
Genome CGH Microarray 44K kit (Agilent Technologies�, Wall-
dbron, Germany) following manufacturer’s recommendations.
Genomic DNA (Promega�, Mannheim, Germany) was used as
reference in sex-matched hybridizations which were analyzed using
Feature Extraction v10.5 and DNA Analytics v4.0 software (Agilent
Technologies�) applying ADM2 algorithm with a threshold of 5,
minimum absolute average log 2 ratio in called intervals of 0.30 and
a minimum of three probes. Putative chromosome copy number
changes were defined by intervals of three or more adjacent probes
and were considered as duplicated or deleted when results exceeded
the �0.30 range.
High-Resolution Cytogenetics AnalysisDNA samples were hybridized to the Affymetrix Cytogenetics
whole-genome 2.7 M array and processed according to the man-
ufacturer’s recommended protocol (http://www.affymetrix.com).
This platform interrogates approximately 2.7 million markers,
providing high-density coverage across the entire genome. Cyto-
genetics data was processed using Chromosome Analysis Suite
(ChAS) software from Affymetrix (Santa Clara, CA). ChAS soft-
ware was used to process the raw data (.CEL files) and determine
regions of copy number segment gains/losses as well as copy-neutral
loss of heterozygosity (cn-LOH). Copy number segments were
filtered to include only gains represented by at least 250 markers
extending over 500 kb, and losses represented by at least 100
markers over a 200 kb region. Confidence levels were restricted to
at least 85%. Following copy number analysis on the Affymetrix
Cytogenetics platform, the source of the chromosomal duplication
was determined from trisomic genotype calls in the chromosome 21
ring region, which were estimated using the Standardized Centered
Allelic Ratio (SCAR). The SCAR value was computed from
Affymetrix software, where positive values map to the homozygous
‘‘A’’ allele, negative values to the homozygous ‘‘B’’ allele, and values
close to 0 indicate heterozygosity. In duplicated regions, positive
SCAR values indicate duplication of the ‘‘A’’ allele and negative
SCAR values indicate duplication of the ‘‘B’’ allele. Heterozygous
alleles in the proband where one parent carried the homozygous
‘‘A’’ allele and the other parent carried the homozygous ‘‘B’’ allele
provided evidence to determine the source of the extra copy.
Sequence In Silico AnalysisIn silico sequence analysis was performed using the following
database and bioinformatic tools: Entrez Nucleotides Database,
http://www.ncbi.nlm.nih.gov/Entrez/query.fcgi?db¼nucleotide;
NCBI BLAST, http://www.ncbi.nlm.nih.gov/Blast/; UCSC
Genome Bioinformatics, http://www.genome.ucsc.edu/ (for
sequence homology analyses for identification of gene content and
for BAC/PAC clones used as probes in the FISH experiments).
CLINICAL REPORT
The female patient was born at 36 weeks of gestation after an
uneventful pregnancy, as the second child of healthy, unrelated
parents. The mother and father were 17 and 25 years old, respec-
tively, and had a healthy older female child. Birth weight of the
1426 AMERICAN JOURNAL OF MEDICAL GENETICS PART A

patient was 2,370 g with an Apgar score of 7 at 1 min. She was
cytogenetically studied because of mild facial dysmorphisms and
hypotonia. The family pedigree shows a history of Down syndrome
(DS) (Supplemental Fig. 1). At 2 months, she was hospitalized for a
suspected non-febrile seizure; weight was 5,250 g (90th to 97th
centile), length of 55 cm (25th to 50th centile). Clinical evaluation
confirmed a general muscular hypotonia, malformed ears, umbili-
cal hernia, and gastroesophageal reflux, but neuropsychiatric eval-
uation, EEG, and MRI of the brain were normal. At 5 months her
weight was 11,700 g (>97th centile). She was later referred because
of slight delay in psychomotor development, especially speech
delay. She could sit without support at the age of 7 months, and
walk without support at the age of 20 months.
Neuropsychiatric EvaluationThe patient was referred for clinical assessment at the local Child
Neuropsychiatry Service at the age of 29 months. The first psycho-
motor assessment (Brunet Lezine Test) showed a disharmonic
psychomotor retardation: 20.8 months of developmental quotient
(DQ) compared to 29 months of chronological age, with posture
control (DQ 24 months), coordination (DQ 24 months), sociali-
zation (DQ 21 months), and significant impairments in the lan-
guage domain (DQ 10 months). At the time of the psychomotor
development check up at 39 months of chronological age the
disharmonic psychomotor retardation was confirmed (DQ 24.9
months), with small improvement in all developmental domains,
but with an increased retardation compared to the standardized
average development. The differences between chronological and
psychomotor age shifted from 8.4 months at the first psychomotor
assessment (29 months of chronological age) to 14.3 months at the
second check up (39 months of chronological age).
The patient underwent psychomotor therapy from age 4 to
6 years and speech therapy from age 6 to 8 years. When the speech
therapy began, she showed difficulties with attention, language
comprehension, and critical reasoning, and she was able to read by
syllabicating. At the end of the speech therapy, at the age of 8, she
was able to perform syllabic fusion, though decoding was very slow.
The language, which had shown expressive delay, was simply
structured and phonologically adequate, but lexical and semantic
limits were more evident. Comprehension was limited to concrete
contexts or related to personal experiences.
Results of the Leiter-R and speech assessment confirmed a mild
intellectual disability with difficulties with logical, communicative
and language abilities, attention, spatial memory, and short- and
long-term memory (see a full report on Supplemental Material:
Complete Neuropsychiatric Evaluation).
METHODS AND RESULTS
Chromosome analyses from the patient’s blood lymphocyte cul-
tures showed a sSMC, which was DA/DAPI negative, in all 50
metaphases investigated (Fig. 1a), while analysis of both parents
showed normal karyotypes (100 metaphases investigated). FISH
analysis using the Pan-centromeric probe and the Pan-telomeric
probe (Oncor, Inc.) revealed a small monocentric sSRC, positive for
the alphoid probe D13Z1/D21Z1, but negative for the beta-satellite
probe (Fig. 1b–d). Finally, the WCP probe for chromosome 21 was
positive demonstrating chromosome 21 origin and suggesting
additional euchromatic sequences in the r(21) (Fig. 1e). Using
ISCN 2009 recommendation, the aberration was characterized as:
47,XX,þmar de novo.ish r(21) (wcp21þ,D13Z1/D21Z1þ,bsat-).
In order to define the chromosome 21-derived euchromatic
sequences and attempt to identify the breakpoint region, FISH
analysis with a battery of BAC clones was performed on EBV-
transformed lymphoblastoid cell line of the patient (Fig. 1f and
Supplemental Fig. 2). The r(21) showed hybridization signals for
RP11-97K13 and RP11-78J18, but none for RP11-141K11, while for
RP11-242C13 there is no clear interpretation, since it showed a
weak hybridization signal or no signals. From these results we were
able to define a partial trisomy of about 3 Mb extending from cen to
21q21.1, with a breakpoint region of 158 kb by the size of RP11-
242C13 (from nt 15,546,175 to 15,704,232). By aCGH analysis, two
different regions of copy gain on chromosome 21 were evidenced
(all the positions on chromosome 21 were referred to the old
Assembly Mar. 2006 hg18 of UCSC): (a) the proximal one’s, from
21q11.2 to 21q21.1 (nt 13,548,935–15,510,501), extending for
1.96 Mb; (b) the distal one’s, from 21q21.3 to 21q22.11 (nt
29,278,776–31,123,552), extending for 1.84 Mb (Fig. 2). The
two regions of copy gain were confirmed during subsequent
whole genome analysis on the Affymetrix Cytogenetics array
(Supplemental Fig. 3). Copy number segment analysis using the
higher resolution cytogenetics array identified the amplified
regions as 21q11.2–21q21.1 (1,066 markers; nt 13,527,258–15,552, 772) and 21q21.3–21q22.11 (2,613 markers; nt
29,265,617–31,950,671).
Uniparental disomy (UPD) was excluded using microsatellite
analysis (data not shown). These results were confirmed by the
Affymetrix Cytogenetics array, which determined this region was
free from long contiguous stretches of homozygosity (LCSH),
which are characteristic of UPD. The paternal origin of the ring
was assessed using allele signal intensities from the Affymetrix
Cytogenetics Array. Trisomic genotypes were determined for the
proband in regions 21q11.2 and 21q21.3–q22.11 and compared to
the parental genotypes at locations where one parent carried the
homozygous ‘‘A’’ allele and the other parent carried the homo-
zygous ‘‘B’’ allele. The amplified allele in 24 out of 29 valid trisomic
genotypes in this region matched the homozygous allele of the
father (P< 0.001) (Supplementary Table I).
In Silico Sequence AnalysisIn order to clarify the discontinuity of this ring chromosome, an in
silico sequence analysis to delineate the genomic structural features
of the two genomic regions involved was performed. The two
regions of trisomy lie in the same contig (NT_011512: Homo
sapiens chromosome 21 genomic contig, GRCh37.p2 reference
primary assembly). BLAST analysis using the proximal region
(as query) versus the distal one’s (as subject), evidenced more
than 30,000 blast hits on the query sequence, with a query
coverage of 13% (see Supplemental Material: In silico Results,
A). Furthermore, variation and repeats analysis by UCSC
Genome Browser on Human Mar. 2006 (NCBI36/hg18) assembly
was conducted for both regions. In the proximal region
VILLA ET AL. 1427

(chr21:13,548,935–15,510,501) several duplications of >1,000
bases of non-repeatmasked sequence were evidenced; three of them
(chr21:28204081, chr21:28321445, and chr21:28335703) have a
genomic size of 94,550 bases, 9,791 and 20,456 bases, respectively,
and a similarity>96% with sequences belonging to the distal region
of trisomy (chr21:29,278,776–31,123,552) (see Supplemental
Material: In silico Results, B). Finally, again for the proximal region,
The database of chromosomal imbalance and phenotype in humans
using ensembl resources (DECIPHER) ([email protected])
reported one patient (249224) with a deletion of 6.37 Mb
(chr21:14320039–20690911) affected by speech delay.
DISCUSSION
Here we report on the first case of a supernumerary discontinuous
ring chromosome 21. However, this is the first instance where the
sSRC was characterized in detail by FISH, array-CGH and then
confirmed by the Affymetrix Cytogenetics array, as a de novo ring
from chromosome 21. Previously, one case of ring chromosome
originating from three discontinuous regions of chromosome 4
[Fang et al., 1995], and a second from different parts of the q arm of
chromosome 20 [Anderlid et al., 2001] were described. Both
reported the ring chromosomes were formed during repeated
breakage and reunion cycles as a result of the formation of inter-
locked rings during cell division [Fang et al., 1995; Anderlid et al.,
2001]. Two similar cases of r(1)s were identified in the work of
Callen et al. [1999], but the discontinuous regions of chromosome 1
were not well characterized. R€othlisberger et al. [2009], report a
discontinous sSMC(18), while Starke et al. [2001] described an
acquired one from chromosome 11. Similar cases can be found
at http://www.med.uni-jena.de/fish/sSMC/00START.htm, like
08-W-p23.3/1-1 for chromosome 8 and 14-W-q13.3/1-1 for chro-
mosome 14. Although several discontinuous sSMCs have been
reported, few were the sSRCs accurately studied.
In our case, we evidenced two different regions of partial trisomy
on the q arm of chromosome 21 by array-CGH and also confirmed
by the Affymetrix Cytogenetics array. Starting from Affymetrix
Cytogenetics array data and microsatellite analysis it is possible to
postulate a mechanism of formation for r(21) as initiating from
a complete trisomy 21, originated more likely through a non-
disjunction event at the second meiotic paternal division, or, less
likely, at an early post-zygotic division. Then, in early stages of
mitotic division, the supernumerary chromosome was reduced to a
ring. The loss of genomic material from r(21) occurred by the
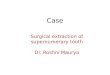
FIG. 1. Results of cytogenetic and molecular-cytogenetic investigations showing a de novo supernumerary ring chromosome 21 in the proband. a: QFQ
banding; (b) alphoid probe D13Z1/D21Z1; (c) beta-satellite probe; (d) Pan-telomeric probe; (e) WCP probe for chromosome 21; (f) RP11-106K13 BAC
clone. The white arrows indicate the r(21) while the red signals indicate presence of the various probes.
1428 AMERICAN JOURNAL OF MEDICAL GENETICS PART A

mechanism proposed by Fang et al. [1995], or through non-
allelic homologous recombination (NAHR), Indeed, NAHR can
be mediated by the presence of low-copy repeats (LCRs, also called
segmental duplications, SD) [Stankiewicz and Lupski, 2002; Shaw
and Lupski, 2004]. LCRs are region-specific DNA blocks usually of
10–300 kb in size and of >95–97% similarity to each other
[Stankiewicz and Lupski, 2002; Bailey and Eichler, 2006]. We
evidenced the presence of at least three SDs in the two regions of
trisomy, that may have triggered the mechanism NAHR, function-
ing as substrates (see Fig. 3).
Finally, as the paternal lineage shows two relatives with DS, one
could assume that there is a tendency to non-disjunction of the two
chromosome 21s at meiosis in this family.
It is the distal trisomy region of r(21), not identified by FISH
analysis and with higher gene content, to fall in the critical area
associated with severe clinical problems (nt 18,100,000-q-tel)
[http://www.med.uni-jena.de/fish/sSMC/21.htm#Start21]; this is
in accordance with the model proposed by Liehr, based on the
interpretation of the presently available data on sSMC and on the
hypothesis that a genetic imbalance induced by sSMC presence, is
the major reason for clinical symptoms in sSMC carriers. Supple-
mentary Table II and Supplemental Figure 6 show an attempt of
genotype–phenotype correlation in sSMC cases derived from chro-
mosome 21 reported in the literature, in addition to the one
presented here.
Our case emphasizes the difficulty of a genotype–phenotype
correlation for cases with partial trisomy 21, as already discussed by
others [Kondo et al., 2006; Lyle et al., 2009]. Kondo and coworkers
reported two cases of partial trisomy 21 (pter-q22.12 and pter-
q22.11) without the major features of DS. Both patients had a
similarly sized extra chromosome 21, lacked all of DS critical region
(DSCR) on 21q22, but they presented with moderate intellectual
disability, delayed motor development, and speech delay, as our
patient. Although the two cases described by Kondo et al. was
associated with a distal partial trisomy 3p and 14q, respectively, the
authors conclude that the moderate intellectual disability most
likely results from partial trisomy 21pter-q22.1. On the other hand,
Lyle and coworkers reported on genotype–phenotype correlations
in DS in 30 cases of partial trisomy 21. Patients with milder
phenotype are those in which the partial trisomy overlaps with
one of the two regions of trisomy identified in our ring. From all this
evidence one might speculate that a critical region, associated with
psychomotor and intellectual disability and speech delay, maps to
21q22.11.
In conclusion, we were able, using aCGH analysis and SNP array,
to identify the real genomic content of the r(21) in our patient, to
determine its paternal origin (with important implications for
counseling), to correlate with the phenotype and to hypothesize
a possible mechanism of formation. It is increasingly evident that,
given the rarity of these partial trisomies of chromosome 21, there is
a need for a web-based collection of cases with both phenotypic and
genotypic characterization, as suggested by Lyle et al.; in addition
the use of oligonucleotide platforms for array-CGH may reveal not
only additional cases that could be undiagnosed or better map the
breakpoints, but also may help to define which regions contribute to
phenotypic features.
FIG. 2. Array-CGH profile of chromosome 21 showing the two regions of trisomy present in r(21): the centromeric region covers 1.96 Mb, encompassing
from 21q11.2 to 21q21.1 (nt 13,548,935–15,510,501) while the distal region covers 1.84 Mb, encompassing from 21q21.3 to 21q22.11 (nt
29,278,776–31,123,552). The colored boxes show magnification of the two regions with their known gene content.
VILLA ET AL. 1429

ACKNOWLEDGMENTS
We are grateful to the family for agreeing to participate in this study.
We wish to thank the Galliera Genetic Bank for EBV-transformed
lymphoblastoid cell line; Galbiati M. and Lettieri A. (M. Tettamanti
Research Center, Pediatric Clinic, University of Milano, Bicocca,
San Gerardo Hospital), Colombo D. (Istituto Auxologico Italiano)
and Surrey S. (Thomas Jefferson University, Philadelphia, PA,
USA) for technical support and editorial assistance. This work was
supported in part by Fondazione Cariplo, AIRC, and MIUR (S.B.,
M. Tettamanti Research Center).
REFERENCES
Anderlid BM, Sahlen S, Schoumans J, Holmberg E, Ahsgren I, Mortier G,Speleman F, Blennow E. 2001. Detailed characterization of 12 supernu-merary ring chromosomes using micro-FISH and search for uniparentaldisomy. Am J Med Genet Part A 99:223–233.
Bailey JA, Eichler EE. 2006. Primate segmental duplications: Crucibles ofevolution, diversity and disease. Nat Rev Genet 7:552–564.
Callen DF, Eyre H, Fang YY, Guan XY, Veleba A, Martin NJ, McGill J, HaanEA. 1999. Origins of accessory small ring marker chromosomes derivedfrom chromosome 1. J Med Genet 36:847–853.
Crolla JA. 1998. FISH and molecular studies of autosomal supernumerarymarker chromosomes excluding those derived from chromosome 15. II.Review of the literature. Am J Med Genet Part A 75:367–381.
Dalpr�a L, Giardino D, Finelli P, Corti C, Valtorta C, Guerneri S, Ilardi P,Fortuna R, Coviello D, Nocera G, Amico FP, Martinoli E, Sala E, Villa N,Crosti F, Chiodo F, di Cantogno LV, Savin E, Croci G, Franchi F, Venti G,Donti E, Migliori V, Pettinari A, Bonifacio S, Centrone C, Torricelli F,Rossi S, Simi P, Granata P, Casalone R, Lenzini E, Artifoni L, Pecile V,Barlati S, Bellotti D, Caufin D, Police A, Cavani S, Piombo G, Pierluigi M,Larizza L. 2005. Cytogenetic and molecular evaluation of 241 smallsupernumerary marker chromosomes: Cooperative study of 19 Italianlaboratories. Genet Med 7:620–625.
Fang YY, Eyre HJ, Bohlander SK, Estop A, McPherson E, Trager T, RiessO, Callen DF. 1995. Mechanisms of small ring formation suggestedby the molecular characterization of two small accessory ring chromo-somes derived from chromosome 4. Am J Hum Genet 57:1137–1142.
Kondo Y, Mizuno S, Ohara K, Nakamura T, Yamada K, Yamamori S,Hayakawa C, Ishii T, Yamada Y, Wakamatsu N. 2006. Two cases of partialtrisomy 21 (pter-q22.1) without the major features of Down syndrome.Am J Med Genet Part A 140A:227–232.
Liehr T, Weise A. 2007. Frequency of small supernumerary markerchromosomes in prenatal, newborn, developmentally retarded andinfertility diagnostics. Int J Mol Med 19:719–731.
Liehr T, Claussen U, Starke H. 2004. Small supernumerary markerchromosomes (sSMC) in humans. Cytogenet Genome Res 107:55–67.
Liehr T, Mrasek K, Kosyakova N, Ogilvie CM, Vermeesch J, Trifonov V,Rubtsov N. 2008. Small supernumerary marker chromosomes (sSMC) inhumans: Are there B chromosomes hidden among them. Mol Cytogenet1:12.
FIG. 3. Proposed mechanism for the formation of the de novo supernumerary discontinuous r(21) from a larger ring. The two regions of trisomy of r(21)
evidenced by array-CGH are highlighted by red rectangles. The red dashed lines represent a likely NAHR event between the two sub-regions with
sequence homology nearly 100% identified by in silico analysis. See also BLAST analysis in Supplemental Material. [Color figure can be viewed in the
online issue, which is available at wileyonlinelibrary.com.]
1430 AMERICAN JOURNAL OF MEDICAL GENETICS PART A

Lissoni S, Baronchelli S, Villa N, Lucchini V, Betri E, Cavalli P, Dalpr�a L.2009. Chromosome territories, X;Y translocation and premature ovarianfailure: Is there a relationship? Mol Cytogenet 27:2–19.
Lyle R, B�ena F, Gagos S, Gehrig C, Lopez G, Schinzel A, Lespinasse J, BottaniA, Dahoun S, Taine L, Doco-Fenzy M, Cornillet-Lef�ebvre P, Pelet A,Lyonnet S, Toutain A, Colleaux L, Horst J, Kennerknecht I, WakamatsuN, Descartes M, Franklin JC, Florentin-Arar L, Kitsiou S, A€ıt Yahya-Graison E, Costantine M, Sinet PM, Delabar JM. Antonarakis SE. 2009.Genotype–phenotype correlations in Down syndrome identified by arrayCGH in 30 cases of partial trisomy and partial monosomy chromosome21. Eur J Hum Genet 17:454–466.
R€othlisberger B, Chrzanowska K, Balmer D, Riegel M, Schinzel A. 2009. Asupernumerary marker chromosome originating from two differentregions of chromosome 18. J Med Genet 37:121–124.
Shaffer L, Slovak ML, Campbell LJ. 2009. ISCN 2009, an internationalsystem for human cytogenetic nomenclature. Basel: S. Karger.
Shaw CJ, Lupski JR. 2004. Implications of human genome architecture forrearrangement-based disorders: The genomic basis of disease. Hum MolGenet 13:R57–R64.
Stankiewicz P, Lupski JR. 2002. Genome architecture, rearrangements andgenomic disorders. Trends Genet 18:74–82.
Starke H, Raida M, Trifonov V, Clement JH, Loncarevic IF, Heller A, BleckC, Nietzel A, Rubtsov N, Claussen U, Liehr T. 2001. Molecular cyto-genetic characterization of an acquired minute supernumerary markerchromosome as the sole abnormality in a case clinically diagnosed asatypical Philadelphia-negative chronic myelogenous leukaemia. Br JHaematol 113:435–438.
VILLA ET AL. 1431







![Brief CV English[1]«Supernumerary marker chromosomes (SMC’s) in Turner syndrome are mostly derived from Y chromosome». Clinical Genetics, 51: 184 - 190, 1997 I.F: 3.276 9. …](https://img.pdfslide.us/doc/110x75/5f03cf897e708231d40ae2a1/brief-cv-english1-supernumerary-marker-chromosomes-smcas-in-turner-syndrome.jpg)