-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
1/18
A Critical Examination of the
Homeopathic Treatment of Chronic
Fatigue Syndrome
April 7, 2011 by Gill Graham
-with particular reference to the reliability of the randomised
controlled trial as amethod of measuring its efficacy in practice
-
Abstract
The aim of this study is to evaluate whether or not homeopathy
is an effective treatment
for Chronic Fatigue Syndrome (CFS). Highly complex in its
nature, CFS is a challenge
to physicians of every discipline, thus guidelines as to the
efficacy of treatment are
warranted. Chronic Fatigue Syndrome is a symptom-defined
condition in which
physical and mental fatigue, usually made worse by activity, are
the core symptoms
(Sharpe 2004)
A literature search on the subject of Chronic fatigue/ME was
undertaken, both on-lineand through the Glasgow Homeopathic
Library. An investigation into the allopathic
treatment of the condition has been undertaken, documented and
critically reviewed.
Randomised Control Trials, the function of the placebo effect
and what constitutes
Evidence Based Medicine were discussed to put the research into
context. Homeopathic
treatment and approaches were then evaluated by referring to
published case studies,
whilst analysing the different methodologies of individual
homeopaths. In addition,different concepts and individual schools
of thought were studied to highlight any
particular successes or failures in approaches to their cases.
Two RCTs have beenanalysed (Awdry 1996, Weatherley-Jones 2002) and
other treatment protocols namely,
Peter Chappells CFS trial in Leuven (2004) and Harthoornes in
South Africa (1997).
There is a positive response to homeopathic treatment in most
trials and cases based onobservation and outcome. Howeverthis study
concludes that the focus on current
methods of measuring the efficacy of homeopathy, namely
randomised control trials, isnot an appropriate or balanced
assessment of the evidence. Other methods of measuring
the efficacy of homeopathy such as observational studies
(Rawlins, 2008) are more
suited to adapting to the homeopathic paradigm.
This study suggests that there are many aetiologies for CFS and
it is evident from theliterature that the cure is often dependant
on these facts. Treatment is individualised and
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
2/18
ongoing to match the state of the patient. It is recommended in
this study that research
into CFS should continue to refine the optimum approach. While
statistical analysismay have some value, it is clear that
professional judgement reinforced by longitudinal
observation is a much stronger approach for correctly evaluating
the success oftreatment.
It is the intention of this study to give an in-depth insight
into the homeopathictreatment of Chronic Fatigue Syndrome (CFS),
through the analytical and criticalresearch of published cases and
trials. Because the efficacy of homeopathy is judged
largely on the rigours of the Randomised Controlled Trials
(RCT), a large section of the
research in this study concentrates on the viability of the RCT,
which according toProfessor Sir Michael Rawlins, the Chairman of
National Institute for Health and
Clinical Excellence (NICE), does not deserve its elevated place
in the hierarchy ofevidence (Rawlins, 2008). In the Harveian
Oration of 2008, De Testimonio he cites
Hill, the architect of the RCT in stating Any belief that the
controlled trial is the onlyway to go would mean not that the
pendulum had swung too far, but that it had come
right off the hook. He goes on to say: Hierarchies attempt to
replace judgment with anover simplistic, pseudo-quantitative,
assessment of the quality of available evidence.
Most trials alluded to in this study are double or triple blind
against placebo. For this
reason the placebo concept will be similarly analysed and placed
in appropriate context.
What constitutes Evidence Based Medicine (EBM) is highly
significant to the
credibility of this study, so this too will be discussed. Its
about integrating individual
clinical expertise and the best external evidence (Sackett et
al, 1996). The researcher is
therefore using the study of the homeopathic treatment of CFS as
a framework to
explore these wider issues, whilst endeavouring to present the
optimum approach to the
condition.
To complete this study, a concise allopathic literature review
will link into the
homeopathic perspective on CFS, where homeopathic philosophy
will be seen to relate
to some allopathic concepts including psychoneuroimmunology. An
in-depth analysis
of the homeopathic treatment of CFS, including the rationale
behind various trials and
protocols, methodologies and philosophy will be discussed,
appraised and criticised bythe researcher, the purpose being to
inform the reader at the highest level.
History of Chronic Fatigue Syndrome (CFS) to the present day
Descriptions of a disease not dissimilar to CFS were found on a
piece of Egyptian
papyrus dating back to 1900 B.C. From very early studies, clear
aetiologies for this
condition were evident and will be discussed at length in this
study. Beard, (1869), a
psychiatrist, referred to the condition as neurasthenia, after
treating several young
women for an illness with many similarities to CFS. He defined
this as a condition ofnervous exhaustion, characterised by undue
fatigue on the slightest exertion, both
physical and mental . the chief symptoms are headache,
gastro-intestinal disturbances
and subjective sensations of all kinds. He also referred to
fatigue as The Central Africa
of Medicine, an unexplored territory where few men enter. Deale
and Adams, (1894)concurred with Beard, also describing the
condition as neurasthenia, with enfeeblement
of the nervous force, which may have all degrees of severity.
Almost one hundredyears later, Jay Goldstein MD, a specialist in
CFS, describes it as a neurosomatic
disorder, problems caused by a biochemical neural network
dysfunction which is a
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
3/18
novel paradigm, confounding researchers and physicians alike.
(Goldstein,1996:2).
Clearly, time has not offered the gift of great insight or cure
which is the gold standardin our research that has to be validated
(Rutten et al, 2006), except that what is required
is a multidimensional approach (Wessely, Hotopf and Sharpe
1999:19)
An outbreak of an apparent disease at the The Royal Free
Hospital 1955 was the
defining situation for the beginning of acceptance of CFS. In
this, sufferers presentedsymptoms such as problems with brain
function, headaches, blurred vision and unusualskin sensations. The
Central nervous system had been affected in 74% of cases
(Parish,
1978, Shepherd, 1999). Some of these patients never recovered.
(Chief Medical
Officers Working Group report on CFS/ME, Feb 2002:4). Dr Melvin
Ramsay who wasthe consultant physician at the infectious diseases
unit at the time was compelled to
publish a report in the Lancet (1956) describing the disease as
A New Clinical Entity.He subsequently suggested it should be called
Benign Encephalomyelitis. Two
psychiatrists however, described the situation in the British
Medical Journal in 1970 asbeing caused by mass hysteria (McEvedy
and Beard, 1970). Sadly, this had a
profound effect on the medical community, who in large, remained
cynical. It was onlyin 1998 that the Chief Medical Officer finally
recognised the illness, after years of
controversy and debate. Some remain cynical however, and views
such as those ofShorter (1995) are still frequently voiced:
In every community there will be at least one physician willing
to play up to his
patients need for organicity. Thus do the caregivers themselves
contribute to their
patients somatic fixations, plunging youthful and productive
individuals into careers of
disability.
What is Chronic Fatigue Syndrome?
Chronic Fatigue Syndrome (CFS) is a disorder that presents with
profound,
debilitating fatigue which accompanies normal activities and is
not relieved by bedrest and cannot be explained by another medical
condition . (Afari and Buchwald,
2003:221.) It is also sometimes referred to as ME (Myalgic
Encephalomyelitis), Post
Viral Fatigue Syndrome and Immune Dysfunction Syndrome. It often
comes on
suddenly with no obvious cause. It is a syndrome that affects
twice as many women
than men and can last for months or years and it is envisaged
that even more people will
present with it in the years to come. It is thus an area of
study that will be useful in
practice. Dr Lucinda Bateman who serves on the board of CFIDS
Association of
America opened a fatigue consultation clinic in 2000 and has
since had to evaluate more
than 1000 patients: In my clinical experience, I have found that
CFS is among the most
difficult conditions to improve at all, with either physical or
psychological
interventions. (Bateman, 2003).
According to Shepherd, (1999), it is generally acknowledged that
CFS is a three stage
illness which encompasses:
y1. Predisposing factors which result in people becoming more
susceptible2. Events which subsequently stress the immune system
and thus prompt
the onset
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
4/18
3. Factors that contribute to perpetuating the symptoms and
consequentdisability
Young women (average age 32) are 3 times more likely to get CFS
than men (Dowsett,1990). The reason for this is multifaceted and
Shepherd (1999) suggests that this is
likely to occur for the following reasons:
y Possibly a hormonal link with CFS (Harlow et al. 1996).
Shepherd again statesthat during pregnancy women with CFS often see
an improvement in their
symptoms
y Mothers and women of young children may be more exposed to
infectiony It is harder for mothers and women with domestic and
family commitments to
take time off when they should be resting
y Women are more knowledgeable about CFS thus more likely to get
a diagnosisAllopathic Criteria for diagnosing CFS
The following diagnostic criteria are from Dr Melvin Ramsay who
was The Royal Free
Hospitals infectious diseases specialist during the outbreak in
1955. There have beennumerous other definitions since then (NICE
guidelines run to over 50 pages) but Dr
Ramseys original work remains the best clinical description to
date (Shepherd:1999:
7).
y Muscle Fatigability with tenderness, twitching and spasmsy
Circulatory Impairment encompassing cold extremities, sensitivity
to climatic
change and excessive sweating
y Cerebral dysfunction, including deterioration in memory and
concentration,cognitive difficulties, sleep disturbance and mood
change
The current NHS symptoms are less succinct but essentially
similar. (Appendix 1). It
is clear that the Royal Free Outbreak and the symptoms currently
listed by the NHS are
referring to the same illness thus adding credence to the views
of those who fought for
its recognition as far back as 1955.
Other authors remain as bemused as to the exact origin of the
condition. Mostert
(1999:72) states that there are no tests to confirm or refute a
diagnosis of CFS.
However, recently, an osteopathic doctor, Raymond Perrin has
developed a technique
for diagnosing CFS, based on the theory that different stress
factors whether physical,allergies, emotional or infections lead to
an overstrain of the sympathetic nervous
system. He goes on to suggest that a build up of toxins in the
fluid around the brain and
spinal cord are the result of a nervous system overload. He has
discovered definitephysical signs common to all CFS sufferers and
has developed a physical examinationwith a definite diagnosis at
the end, based on what is found. (Perrin, 2007). It would
appear that this could be revolutionary as regards treatment of
the condition, but thediscovery will take time to be absorbed and
accepted by the medical community as a
whole. In the meantime, diagnostic criteria has been set out by
various bodies including
Centre of Disease Control (CDC, Appendix 2), and the Oxford
Criteria for CFS
(Appendix 3) but as Wessely et al (1999) have discovered, the
current classification for
CFS stands inadequate and unresolved.
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
5/18
Much research has been conducted in terms of conventional
medical treatment for CFS.
Drug therapies have included anti depressants, hormones,
corticosteroids, antiviralmedications as well as immunologically
targeted drug treatments. (Afari & Buchwald,
2003:229). Research has concluded that these approaches have not
been significantlyeffective: There is no pharmacological treatment
or cure for CFS/ME (National
Institute for Health and Clinical Excellence)
Homeopathic Research and the requirement for Evidence Based
Medicine (EBM)
in relation to the credibility of the Randomised Control
Trial
Significantly, much of the recent specific homeopathic
information available on CFS
highlights an RCT carried out by Dr Elaine Weatherley-Jones at
the University of
Sheffield. She used a triple blind design (patient and homeopath
blind to groupassignment and data analyst blind to group until
after initial analyses to reduce the
possibility of bias due to data analyst) in a trial where
patients were randomly assignedto homeopathic medicines or placebo.
One hundred and three patients meeting the
Oxford criteria for CFS were recruited to two specialist
hospital outpatient departmentsin the UK and attended monthly
consultations with professional homeopaths. Outcomes
were assessed at six months using the Multidimensional Fatigue
Inventory (MFI),Fatigue Impact Scale and the Functional Limitations
Profile (FLP). Ninety two patients
completed the trial (47 simillimum treatment and 45 placebo).
The results showed that
47% of the patients in the treatment group showed significant
improvement compared
to only 28% of the placebo group. (Weatherley-Jones, 2004)
The trial was published in of the Journal Psychosomatic Research
(2004) concluding
that There is weak but equivocal evidence that the effects of
homeopathic medicine are
superior to placebo. In response to the same study, the British
Medical Journals
Clinical Evidence (2007) interprets the research differently,
concluding as a clinical
guide That there is insufficient evidence to recommend
homeopathy as a treatment in
chronic fatigue syndrome. Here the different paradigms of
allopathic and homeopathic
medicine are clearly indicated, with the difficulty in
performing homeopathic research
trials under the same conditions as allopathic trials, where the
methods of prescribing
and case analysis are so clearly different. Another author
appraised this trial concluding;
The study certainly hasnt conclusively answered the question of
whether the effects are
purely due to placebo or if there is a specific homeopathic
component in homeopathic
remedies. (Walach, 2004:211).
Similar problems presented with the analysis of a trial
undertaken by Awdry (1996).
Awdrys trial was a randomized double blind trial involving 64
participants each of
whom attended at least 12 clinic visits over a 12 month period.
Awdry considered the
results to be encouraging. The study had two outcome measures: a
daily wellness graphand a self-assessment chart to be completed at
the end of the trial his results are
summarised overleaf. In conducting a statistical analysis of the
data collected in the
study, Wessely, Hotopf and Sharpe (1999:387) were sceptical in
their opinions even
though the study data suggested a 33% improvement in the group
taking homeopathicmedicines as opposed to a 3% improvement in the
placebo group. They stated that the
internal validity was questionable and insufficient to render
reliable results. Afari andBuchwald (2003:228) concurred,
considering Awdrys study to be of poor quality and
stated the outcome as inconclusive This once more demonstrates
the difficulty in
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
6/18
measuring homeopathic success rates by conventional, limited
methods, not suited to
the homeopathic paradigm. Disraeli (1804-1881) was aware of the
dangers of basingjudgement on pure statistics : There are three
kinds of lies: lies, damned lies and
statistics. (Disraeli, cited by Rutten et al, 2006)
Clearly, the results of these trials are sufficient proof to
homeopaths of the success of
the research given that more people in the homeopathic group
showed clinicalimprovement on all primary outcomes. (Awdry, 1996)
An article in The BMJ, statesthat evidence based medicine is about
integrating individual clinical expertise and the
best external evidence Sackett et al (1996). Sir Ian Chalmers,
Director of the UK
Cochrane Centre, suggests that conventional Medicine is biased
against Complementaryand Alternative Medicine (CAM), requiring
lower standards of proof for conventional
medical treatments than they do for CAM. (cited in House of
Lords report on CAM2000). Many researchers a priori see homeopathy
as scientifically implausible, creating
an immediate bias before any research is undertaken. Some of the
theories put forwardto explain the mechanisms of homeopathy can
indeed be confusing to both the
homeopath and allopath. Central to homeopathy is Hahnemanns idea
of The VitalForce, which the researcher sees as a spirit like
essence animating an undefined energy
which is capable of fuelling a living organism; something that
is inherent in all livingthings. When this energy is disrupted by
illness The Vital force is unable to feel, act, or
maintain itself (Hahnemann 2003:15), Aphorism 10, and It is only
the pathological
untuned vital force that causes disease (Hahnemann, 2003:19),
Aphorism 12. Kent
refers to Vital force as simple substance energy is not energy
per se, but it is a
powerful substance, and is endowed with intelligence that is of
itself a substance (Kent,
1990:61). Vithoulkas in the Science of Homeopathy (1980) looks
at the Vital Force in
more scientific terms and suggests that it can be viewed in
terms of the electromagnetic
energy. The advent of Kirlian photography where the
electrodynamic field surrounding
all objects, living or not has added great weight to his ideas,
although this is still
somewhat controversial. He goes on to discuss that should the
vital force be
synonymous with the electrodynamic field in the body, then it
would conform to known
principles in physics.
Homeopathic views such as these may be difficult in concept to
grasp, but this does notmean that the therapy is not effective,
even though a clear understanding or exact
hypothesis as to its mechanism (or that which is adapted to the
scientific paradigm) stilleludes us. A similar example is the
action of aspirin, which took many years to
understand, though was still used and its effectiveness
applauded. (Walach, 2001).
The House of Lords report on Complementary and Alternative
Medicine (2000) statesthat there are several types of evidence that
is required, before a therapy is to be
advocated.
y Evidence that the therapy is efficacious above and beyond the
placebo effecty Evidence that the therapy is safey Evidence that
the therapy is cost effectivey Evidence concerning the mechanism
and action of the therapy
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
7/18
The researcher must affirm that contrary to popular belief,
patients with CFS have a
lower rate of response to placebo than many other illnesses.
Cho, Hotopf and Wessely,(2005) in a recent review and meta-analysis
showed that 19.6 % of CFS patients
improved from placebo, compared to the widely accepted figure of
about 30% for otherillnesses. This could be explained by the
already low expectations of the patient due to
disappointing treatment outcomes in the past.
The following quotation is encouraging to the homeopath;
The finding of significant differences between the effects of
placebo is consistent with
a recent meta-analysis of placebo controlled clinical trials in
homeopathy in which the
authors concluded that their results were incompatible with the
hypotheses that clinical
effects of homeopathy are completely due to placebo. (Linde,
1997).
Linde, here, even though he is allowing allopathic testing to
set the criteria forhomeopathy (albeit incompatible), is clearly
stating that even under these
circumstances, homeopathy is more than just the placebo
effect.
Given that the Power of the Placebo is constantly being used as
a measure againsthomeopathic remedies and in homeopathic RCTs,
accurate definition and research into
this concept is warranted. The word placebo originates from the
Latin I Will Please. It
was originally seen in Latin text in the bible Placebo Domino in
Regione Vivorum
(Psalm114: 1-9). Jerome, the translator, translates this as I
will please the Lord in the
land of the living. Hrobjatsson and Gozsche (2001) state:
Placebo is difficult to definesatisfactorily. In clinical trials
placebos are generally control treatments with a similar
appearance to the study treatments but without their specific
activity. We thereforedefined placebo practically as an
intervention labelled as such in the report of a clinical
trial
Hrobjartsson and Gozsche conducted studies in 2001 and 2004
which analysed clinicaltrials comparing placebo with no treatment.
Two meta-analyses were undertaken
involving all 156 clinical trials in which an experimental drug
or treatment wascompared to a placebo/untreated group. It was found
that in studies with a binary
outcome (ie: improved or not improved) placebo had no
significant effect regardless
of whether these outcomes were subjective or objective. There
was a small
beneficial effect in the treatment of pain however, but the
conclusion of these reviews
clearly stated that we found little evidence that placebo had
powerful clinical
effects. Criticism of their meta-analysis following this
conclusion ensued on the basis
that their control group covered a highly mixed group of
conditions. For instance,
Meissner et al, 2007, stated that the placebo effect does work
in peripheral disease
processes such as asthma, hypertension etc but not for processes
reflecting physical
diseases such as Crohns, urinary tract infections and heart
disease. Similarly Barford(2005) concurs, stating that the placebo
effect can be demonstrated under appropriate
conditions.
It is clear that RCTs will continue to be used in both
homeopathic and allopathic trials,at least in the near future. As
discussed in the introduction to this study, this method of
assessing evidence has huge limitations. One of the most
significant recentdevelopments regarding the thinking as to what is
evidence was delivered by Sir
Michael Rawlins, chairman of NICE On the Evidence for Decisions
about the use of
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
8/18
Therapeutic Interventions. Known as one of the lectures for The
Harvein Oration, this
speech was delivered before the fellows of The Royal College of
Physicians (Rawlins,2008). It is ground breaking and thought
provoking in its delivery, passionate and
erudite in its content. Rawlings cited Jadad 2007 stating that
Hierarchies place RCTson an undeserved pedestal, although the
technique has advantages it also has significant
disadvantages, similarly observational studies have defects but
they also have merits.
This is the fundamental essence of the speech which clearly has
implications for anyphysician, allopathic or homeopathic and for
this reason the key points of his speech aresummarized in order to
contribute to the understanding of trials in relation to
research,
an integral part of this study.
Sir Michael outlined the limitations of RCTs in several key
areas, stating that they are:
Table 1. Limitations of RCTs. ( according to Sir Michael
Rawlins)
Impossible in treatments for very rare diseases where the number
of patients is too
limited
Unnecessary when a treatment produces a dramatic benefit
Often stopped early, which leads to misinterpretation of the
results. Interim
analyses of trials to assess whether the treatment is showing
benefit are nowcommon, but the possibility that an interim analysis
is a random high may be
difficult to avoid, especially as there is no consensus among
statisticians as to howbest to handle this problem
Expensive in terms of money, time and energy. A recent study of
153 trials
completed in 2005 and 2006 showed a median cost of over 3
million with one
trial costing 95 million
Often carried out on specific types of patients for a relatively
short period of time,whereas in clinical practice the treatment
will be used on a much greater variety of
patients and for much longer.
Lionel Milgrom (2009) in alluding to Rawlins speech, became the
collective voice of
the homeopath, when he stated:
No doubt Sir Michaels words will be music to the ears of those
in homeopathy andCAM struggling to get their healing message heard
against the cacophony of sceptical
heavy metal being pumped out by a largely hostile media.
It was clear that Rawlins highly-rated observational studies,
particularly historical
controlled trials and case-control studies, but other forms of
observational data can also
reveal important issues. Contrary to a recent claim, only
observational studies can
realistically offer the evidence required for assessing less
common or latency harms
(Rawlins, 2008:33). It is clear that what he is purporting is
highly significant to thehomeopath, with much of the success of the
therapy being evident through case
studies and observation. He begins his address noting that both
Rene Descartes (1596-1650) and Thomas Hobbes (1588-1679) regarded
observation to be the most appropriate
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
9/18
approach, and ends it stating that Charles Darwin (1809-82)
conceived the theory of
evolution as a result of close observation. The essence of this
speech is summarized inthe following quotation:
For investigators to continue to develop and improve their
methodologies, for decision
makers to avoid adopting entrenched positions about the nature
of evidence and for both
to accept that the interpretation of evidence requires judgment.
(Rawlins 2008)
Homeopathy and the RCT
Homeopath
Given that for now at least, the RCT will continue to be used,
despite the shortcomings
outlined above, it is clear that on analysing the literature
surrounding RCTs, there
appears to be methodological problems in their application to
homeopathy (Kaptchuk
1998, Smallwood 2005, Kaptchuk 2002). The problems of
methodology are complex, as
even if the clinical effect is positive as in the
Weatherley-Jones et al (2004) trial, the
interpretation of actual proof is questionable. RCTs are the
gold standard of medical
research, yet as Rawlins (2008) states the technique has
important limitations andimperfections. They are designed to test
those medications which target specific areas
in the body, therefore having a specific effect. Because
homeopathy stimulates the
bodys healing mechanisms, the focus of the cure does not lie in
one specific organ.
Thus its way of achieving efficacy is non-specific. (Tyler,
2006, Mason et al 2002).
Homeopathically, a remedys action is evident in a more holistic
way, withimprovement seen in mental and emotional symptoms and in
many secondary physical
symptoms. (See Figure 2. Lilley). There is often no way of
measuring this in an RCT,so would be generally attributed to the
placebo effect (Kaptchuk, 1998). Despite the
incompatibility of homeopathy to this method of testing, some
RCTs have nonethelessshown that homeopathy can be efficacious, if
only the mechanism of action were more
plausible (Kleijneet et al 1991). Essentially, research must
focus on whether a
patients symptoms can be controlled by homeopathy, the exact
mechanism of
action could be considered irrelevant. Many researchers concur
that we must redirect
our energies to whole systems healthcare (Long et al, 2008).
Jenkins 1989 concurs,
stating No particular line of treatment seems to be consistently
effective so a broad-
based holistic and multi-disciplinary approach would at present
seem appropriate.
The Multifactored Perspective and the Homeopathic Link:
Psychoneuroimmunology as Scientific Evidence.
Jay Goldstein, MD, Director of the Chronic Fatigue Institute in
Beverley Hills,
California states that there is an increasing consensus that the
illness (CFS) is a virally
induced, cytokine-mediated psychoneuroimmunologic disorder that
occurs ingenetically predisposed individuals. (Goldstein: 1991) It
is significant from an
allopathic perspective that there is a shift from a single-cause
approach, such as a
virus, to a multicausal approach. Goldstein refers to CFS as
neurosomatic disorder.
(Goldstein 1996:2). He cites over 50 conditions that belong to
this same group ofdiseases, Fibromyalgia, Irritable Bowel Syndrome
and Premenstrual Syndrome to
name but a few. He sees four influences which are responsible
for the development ofneurosomatic illness.
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
10/18
y Genetic susceptibility and Expression of the traity
Developmental issues in childhoody Viral encephalopathy and genetic
susceptibilityy An increased susceptibility to environmental
stressors.
(Goldstein 1996)
The summation of the first three points results in impaired
flexibility of the brain
relating to the concept of allostatic load` described as `The
price the body pays for
containing the effects of arousing stimuli and expectation of
negative consequences`
(Goldstein 1996:75). The multi-causal perspective represents a
`historic shift in how the
medical world thinks about what determines health and illness.
(Engel, G.L:1997).
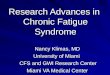
Goldsteins treatment protocol (see fig 3) is shocking to a
homeopath: I administer
multiple medications sequentially in the same office visit until
one has time to exert its
effect before trying the next. Homeopathically, allopathic drugs
are seen as suppressors
of The Vital Force. Hahnemann states in Aphorism 37 that: If the
disease is treated
with violent allopathic drugs, other graver, more life
threatening ailments are created inits place. (Hahnemann S,
2003:34). He calls this method of prescribing contraria
contrariis (Aphorism 57), the opposite of treating like with
like. The fact that using
this protocol most patients are dramatically improved in 1-2
office visits (Goldstein
1996:17) makes one wonder how long this cure lasts; one is
clearly sceptical from a
homeopathic perspective. Goldsteins results are inevitably
disputed for Wessely,Hotopf and Sharpe, (1999:399) disagree stating
that: No pharmacological agent has yet
been shown to be convincingly helpful for CFS. Cont..
Figure 3.
A Typical Neurosomatic New Patient Treatment Protocol
(Goldstein, 1996)
Agents, tried sequentially Onset of action Duration of
action
Naphazoline HCL 0.1 % gtt T OU 2-3 seconds 3-6 hours
Nitroglycerin 0.04 mg sublingual 2 - 3 minutes 3-6 hours
Nimodipine 30 mg po 20-40 minutes 4-8 hours
Gabapentin 100-300 mg 30 minutes 8 hours
Badofen 10 mg 30 minutes 8 hours
Oxytocin 5 -10 UIM QD or BID
or Synlocinon 1 2 pufls TID
15 minutes to 72
hours
12 -24hours
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
11/18
Base
d onGold
steins
publi
cations,there
seem
s to
be a
meet
ing
of
mind
s
amo
ngstthehom
eopaths
andallop
athsregar
dingthe
psyc
hone
uroi
mmu
nolo
gical
basis
of
CFS.
But
howfar
canthis
conv
erge
nce
be
seen
to
com
Pyridostigmine 30 60mgpo 30 minutes 4-6 hours
Hydralazine 10-25 mg po 30-60 minutes 6-12 hours
Mexiletine 150 mgpo 30-45 minutes 6-8 hours
Tacrine 10 mg 30 minutes 4-6 hours
Risperidone 0.25 0.5 mg 45-60 minutes 8 12 hours
Pindolol 5 mg BID 15 minutes to 7days
12 hours
Lamotrigine 25 50 mg QD 30-45 minutes 24 hours
Sumatriptan 3 6 mg SQ 15-30 minutes 16 hours
Ranitidine 150 mg BID 1 hour 1 week
1
12-24 hours
Doxepin HCL elixir 2 - 20 mg HS 1 hour variable
Sertraline 25 50 mg QAM
or Paroxetine 10 20 mg QAM
1 hour- 8 weeks 1- 2 days
Biipropion lOOmgTID 30 minutes 8
weeks
8 24 hours
Nefazodone 100 300 mg BID 2-8 weeks 24 hours
Venlafaxine 37.5 75 mg BID 1-4 weeks 24 hours
Glycine powder 0.4 Gm/Kg/day in
juice
or Cycloserine 15 50 mg QD
1 hour 24 hours
Felbamate 400 mg 30 minutes 6 8 hours
Lidocaine 200 300 mg in 500 ml normal saline
infused over 2 hours
2hours - 2 weeks
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
12/18
ply within the confines of EBM?
Psychoneuroimmunology is described by Rober Ader (2007) as a
convergence of
disciplines, namely the behavioural sciences, the neurosciences,
endocrinology andimmunology. (Ader 2007). The concept has
effectively grown from the realization that
the immune system does not operate autonomously and research in
this field in recent
years has proved that the brain and immune system represent a
single, integrated systemof defence. Indeed numerous studies
conducted over the past 30 or so years havedemonstrated that a wide
variety of stressors can alter many aspects of the immune
response (Maier et al, 1994). Watkins A (2007) and Ader et al
(1995) concur, stating
that there is biochemical, anatomical and physiological evidence
that the bodyssystems as outlined, engage in an interactive
dialogue, to effectively attempt to create
homeostatis. Dr David Felton, who heads up the Department of
Neurobiology andAnatomy at the University of Rochester Medical
Centre in New York, has been
awarded several prestigious grants for his growing work in the
field ofpsychoneuroimmunology (PNI). Similarly, Dr Herbert Benson,
a cardiologist and
associate professor of The Harvard Medical School and Director
Emeritus of TheBenson Henry Institute for Mind Body Medicine at
Massachusetts General Hospital,
received the prestigious Mani Bhaumik award, in March 2009, as a
pioneer in MindBody Medicine. As both are highly trained in
orthodox medicine, this once more
demonstrates a shift in allopathic thinking to a more integrated
approach
Thus, the evidence suggests that those ideas central to
homeopathic philosophy, the
totality of symptoms, the outer image expressing the inner
essence of the disease, ie: of
the disturbed vital force (Hahnemann S, 2003:12) Aphorism 7, are
those which need to
be explored in order to treat a patient successfully. This is
irrefutable and is clearly
demonstrated above.
Many of the diseases Vithoulkas refers to as new diseases (1991)
are ironically seen
by Goldstein to be part of neurosomatic group which would
benefit from his treatment
protocols`. Hahnemann clearly states in Aphorism 74 that Among
chronic disease we
must unfortunately include all those widespread illnesses
artificially created by
allopathic treatments.(Hahnemann, 2003:73)
Vithoulkas groups CFS together with Cancer, Asthma, MS etc as
new diseases, their
cause unknown, puzzling and elusive. How responsible for this
phenomenon were the
chemical drugs we were using? Is it possible that there is a
connection between the
practice of drug overuse and the inability of our immune system
to prevent the
appearance of these alarming new diseases? (Vithoulkas 1991:4).
Herein lies the
ultimate dilemma. Are the so-called medications used to cure
disease by the likes of
Goldstein actually causing them?
PNEI Axis as Evidence
Given that one has established that CFS is a multi-systemic
disease, it important as part
of this study to discuss the way in which the homeopath can
treat the condition based onthe philosophy of those such as
Sankaran (1997), Ullmann (1991), Reichenberg-
Ullmann (1995), Chappell (1997). In homeopathy, the totality of
symptoms deems thatthe mind state is at the top of the hierarchy
and the deepest core of an individuals
health (Ullmann 1991:16). In treating the underlying cause of
illness, the homeopath
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
13/18
will often find that the root of illness, even if the symptoms
are physical, begins with a
mental or emotional trauma. The homeopath then searches for the
state of eachindividual that allows the person to be susceptible to
particular symptoms (Ullmann,
Reichenberg-Ullmann, 1995:16-17). Sankaran sees multi-systemic
disease on a psycho-neuro-endocrine-immunological axis, he refers
to as PNEI (Sankaran 1999:52). In short,
the mind acts on the body through three systems, the nervous,
endocrine and the
immunological system. A remedy will act on the Vital Force
through this axis, targetingthe central disturbance which could
appear anywhere on this axis, depending onsusceptibility. A
delusion is a false perception of a reality, and disease too is a
false
perception of the present. The whole mental state of a person is
an expression of this
false perception. (Sankaran 2005:10). Sankaran considers this
state to be maladaptive
(1999:11-15) and refers to it as delusion. Essentially the PNEI
axis is like an energy
grid, allowing flow of energy between each of the systems. It is
kept in homeostasis by
the Vital Force. Sankaran maintains his belief in this system
but has subsequently
extended the delusion idea, inferring that there is a deeper
underlying state which also
manifests on the physical sphere. He calls this The Vital
Sensation which can be
brought out of the patient through in- depth case taking,
essentially a sensation
connecting mind and body. Given that CFS is multi-systemic,
Sankarans theories sit
very well in unfurling the central disturbance which is often
elusive.
Both Vithoulkas (1991) and Scholten (1993) and Chappells (1997)
views are in
accordance with those of Sankaran in that the mind state is
dominant and intrinsically
linked with the other systems in the body. Each of these three
planes the mental,
emotional and physical though complex in nature, constitute
distinct and separate
entities that differ essentially in their vibrational
frequencies and informational patterns.
These three planes interact with extreme intelligence and react
to any stimulus in a
concerted manner that is always consistent with their own
idiosyncrasies (Vithoulkas
1991:59). Where Sankaran looks as CFS as a multi -systemic
disease on PNEI axis,
Vithoulkas has essentially created a model which recognises the
uniqueness of the
individual and their particular susceptibility. Although
Vithoulkas is one of the most
classical homeopaths and Sankaran of a newer breed, it is
interesting to observe thatfundamentally they agree on the
interaction of all systems in the body. Although vastly
different in their approach to treatment, (as previously shown)
this correlates with JayGoldsteins (1996) thinking of CFS as
psychoneuroimmunologic disorderthe study of
how emotional and other psychological responses influence the
biochemistry of thebrain, hormone production, and the immune
response
Hahnemann and Chronic Disease
With reference to CFS, it is fundamentally essential to consider
how Hahnemann views
chronic diseases. His original and unique work on Chronic
Disease Die Chronischen
Krankheiten, was first published in four volumes (1828-1830) the
second edition offive volumes (1830-1835). Dimitriadis (2005)
analyses this work and explains that
Hahnemann in referring to Chronic Disease is relating to every
disease which is neither
acute, epidemic, sporadic nor chronic venereal disease. These
include neurasthenia,
hysteria, hypochondria, mania, melancholia, idiocy, madness,
epilepsy and all kinds offits, softening of the bones.deficiency of
the senses and every type of pain.
(Hahnemann 2003:78), Aphorism 80. He states also in this
Aphorism that psora is the
true underlying cause. He goes on to say that the homeopathic
physician must still
piece together the perceptible symptoms and peculiarities of the
chronic (psoric) disease
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
14/18
being treated just as carefully as before to form an indicative
picture, because no true
cure of a psoric disease can take place without the strict
individualization of everycase.
According to de Schepper (2004), both Boger and Boennninghausen
base their
repertories on Aphorism 95, which states: patients become so
accustomed to prolonged
suffering that they no longer pay much if any attention to the
many smaller,concomitant symptoms. (Hahnemann 2003:91), Aphorism
95. Sankarans views ofmodalities reflecting the central disturbance
is reflected here also, stating that if the
specific mental state is discovered, it cannot be prescribed
upon unless there is a
concomitant from another sphere (Sankaran, 1999:68). He states
that this is the basisof Boenninghausens doctrine of concomitance
and the concomitant is to the totality
what modality is to the symptom: it is the differentiating
factor. This reflectsHahnemanns fundamental belief and the
challenge that CFS presents to the homeopath,
as so many common symptoms are presented with CFS and one is
searching for thosesymptoms which are striking, strange, unusual or
peculiar (Hahnemann, S. 2003:125),
Aphorism 153.
An evaluation of the evidence of homeopathic treatment as seen
in two RCTS(Weatherley Jones, 2002, Awdry 1996), published case
studies and homeopathic
literature including commonality in remedies, methodologies and
philosophy.
Methodologies
Through the analysis of published cases and trials, it is
essential to discover which
methodologies were used in prescribing, and which had the most
success in treatment inrelation to CFS. Clearly, there are
different approaches as discussed to measuring the
success of treatment, each of which will be explored. Specific
methodologies will behighlighted and critically analysed as to
effectiveness in practice, the success measured
in recovery, with a view to suggesting the optimum approach to a
case. This helps tofurther understand that if homeopathy is
successful in the treatment of CFS, (with
reference to the research question), what makes it so, and what
is the optimum method
of administration? It is hoped that a consistency of approach
can be determined in those
cases that have been successful, to enable future prescribing
and case management to be
more effective.
Classical Method:
The Weatherley-Jones et al trial (2002) and that of Awdry in
1996 are similar in that the
approach to their cases was essentially classical or Kentian
`taking the whole person
into account as far as this is possible and treating the person
simultaneously on all
levels, physical, mental and emotional` (Watson, 2004:12).
Mental and Emotionalsymptoms (including delusions) are given
priority, followed by Physical General
Symptoms and disease symptoms or Physical Particulars (Kramer,
2006). The
homeopath, in using this method of prescribing is searching for
the simillimum. It is
based on the premise of like cures like (Similia Similibus
curanter,). This principlewas first introduced by Paracelcus
(1493-1541) and is outlined in Aphorism 27 in The
Organon The curative virtue of medicine thus depends on their
symptoms being similarto the disease but stronger. It follows that
a particular case of disease can be destroyed
and removed most surely, thoroughly, swiftly and permanently
only by a medicine that
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
15/18
can make a human feel the totality of symptoms most completely
similar to it but
stronger. (Hahnemann 2003: 28), Aphorism 27.
It is important to note that even if the constitutional method
of prescribing is not used, itis still the simillimum that is
sought, regardless of methodology used; this should still
be the focus of the homeopathic enquiry. Both Weatherley-Jones
(2002) and Awdry
(1996) did not, however, use the constitutional method
exclusively in their trials. Aswith other homeopaths, the
constititutional approach was supported by part patient ormiasmatic
prescribing in conjunction with lifestyle changes. De Schepper
(2004)
concurs stating that although often the problem cannot be
rectified by a single
medication, it can be controlled by a total approach. Other
constitutional prescribers areAllen (1993) Hoover (1998) Klein
(1998), Scholten 1998
In the Weatherley-Jones trial, mainly single remedies were
prescribed but where
remedies were prescribed sequentially, more than one was given.
This method is avariation on the aetiological method, where there
is evidence of a sequence of causative
factors (traumas that have systematically contributed to the
patients current state ofdisease (Kramer 2005:58). Case management
predicted when the remedy should be
changed and the most common potency prescribed (to avoid
aggravation) was Lms.17% of the cases required an aetiological
prescription of carcinosin as a specific
antidote to glandular fever, similarly where viruses and
vaccinations were seen as the
cause; the appropriate antidoting remedy was given. These
together with bowel
nosodes added up to 8% of cases. The remaining 75% of cases were
prescribed
polychrest remedies, taking in the totality of symptoms and
applying the constitutional
method.
Dimitriadis (1991), in contrast who has worked with many cases
of CFS, emphasises
that some cases are not suitable for polychrests. Similarly,
Klein (1998) finds that
polychrest prescriptions particularly for CFS, are like trying
to fit a square peg in a
round hole with mediocre results and often chooses remedies on
materia medica
knowledge. In the case he is discussing, he prescribes
scutellaria which is very
specific to the patients symptoms, but probably not a remedy
that would have appeared
on a repertorisation sheet. Hoover (1998), steers clear of the
polychrests, and reaches aconstitutional prescription of onosmodium
a small remedy rarely prescribed by means
of careful repertorisation and materia medica work.
Aetiological prescribing
Awdry (1996b) states that overwork is a strong aetiology, seeing
the virus infection as
merely the final straw which serves to dismantle an already
shaky status quo. De
Schepper (2004) mirrors this theory stating: In every CFS
patient that I have seen in
my practice, stress was the ultimate triggering factor, the
straw that broke the camelsback. And most often, it is the single
cause of relapse. In contrast, Harthoorn (1997)
sees viruses as being a main aetiology and in a trial of 219
case histories, most
responded well to viral therapy. This approach, refined by
Harthoorn was initially used
in relation to a number of hepatitis cases which responded well
to the followingprotocol:
y The virus in question (in this case hepatits A or B) was
administered in highhomeopathic potency.
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
16/18
y Organ therapy (the liver was treated in these cases) to induce
regeneration of thetissues and function
y Immune system boosters giveny Constitutional remedies given in
addition to remedies for hepatitis.
Such was the success of this trial in relation to hepatitis, it
has been used with other
viruses such as herpes zoster and herpes progenitalis amongst
others. Blood tests showthe three most commonly implicated viruses
in CFS/ME to be: Coxsackie, Epstein Barrand Cytomegalo, often seen
in combination. The above protocol, applied as above and
complete recovery occurred in 81.74% of cases treated. This
trial was undertaken in
Africa and it was not possible to conduct double-blind
procedures in the environment ofpractice. Yet again, the results
are based on observation and cure with comments such
as I had been dead for 10 years and now I am alive again, being
muted by gratefulpatients. (Harthoorn, 1997)
Dowson (1993) states: The use of generalized homeopathic
anti-virals may be
beneficial, but if the exact virus present can be identified-by
orthodox orcomplementary methods-high potency preparations of that
virus may be more
successful. Allen (1992) concurs stating: It is thought that
viruses alter our immunesystems, causing our bodies to react to
stress, bacteria toxins, chemicals and the like.
A different approach to aetiological prescribing is taken by
Rudolph Verspoor in his
book Homeopathy Renewed (1995). He suggests an effective
approach to chronic
complex cases (like CFS) that traditional homeopathic methods
have failed to cure,
often because the picture was confused by drugs, vaccinations
and chronic stress. The
method is sequential therapy and is outlined below by Ian
Watson:
It involves taking a detailed case history and determining the
nature and exact sequenceof all shocks and traumas that have
occurred in a persons life, including the gestation
period. Remedies are then given in reverse order which are known
clinically to becapable of neutralising the effects of each. I am
unsure how much time is allowed to
elapse between each prescription, but my impression is that it
ranges from as little as a
day or two up to a month or longer, depending on the severity of
the shock being
treated, and on the potencies being used. (Watson, 1995).
Organ support, Isopathy, Tautopathy
Dowson (1993) discusses that patients with CFS complain of
altered bowel action,
abdominal discomfort and excess flatulence as part of their
condition and he strongly
advocates support of the gastro-intestinal system, particularly
remedies aimed at
supporting the liver and kidneys. Organ support involves
identifying weakened organs
in the system and prescribing remedies that are known to have an
affinity for thoseorgans in order to bring about improved function
(Kramer 2006: 64). Like Awdry
(1996), he suggests an anti-candida diet, anti-fungal
medication. He also recommends
specific nosodes, particularly in bacterial infection, combined
with homeopathic
drainage and renal stimulation. Weatherley-Jones (2004) also
employed the use ofbowel nosodes prepared remedies from non lactose
fermenting bacilli from the
intestinal tract (Kramer 2006:68) in eight percent of her cases
in the trial. Dr JulieAllen (1993) uses Isopathy desensitising her
patient suffering from intolerance to
wheat. Similarly, Jenkins recommends this approach. Watson
defines this as
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
17/18
prescribing a remedy made from the supposed causative agents or
products of a disease
to a patient suffering from that same disease (Watson 2004:34).
Harthoorn (1997) usesorgan therapy, nosodes and tautopathy in his
trial, the differentiating factor from
isopathy being that it focuses on a drug or toxin taken by the
patient that appears to havecaused the symptoms (Kramer, 2006). Due
to the high number of anti biotics given to
many suffering from ME, candida is thought to be a causative
factor by several authors.
(Balch 1993, Chaitow, 1991).
The rationale behind Peter Chappells CFS trial
Sankaran alludes to central disturbance and the connection
between mind and body
and how one vital sensation expresses the fundamental state.
(Sankaran, 2002). This is
mirrored by other homeopaths (Vithoulkas 2004, Scholten1993,
Verspoor 1995).Chappell (1997) refers to a state of stuckness which
has feeling and physical
components acting together synchronously. Chappell is a
controversial figure whowent to Ethiopia in 2001 to help find a
homeopathic solution to AIDS. Realising the
normal homeopathic approach was not viable due to lack of
information in thehomeopathic information set, he developed a
method of reverse engineering a remedy
from the totality and essence of the pathology. His remedy for
AIDS was known asPC1 and he generalized the approach to other
epidemic diseases (malaria, dengue fever,
diphtheria and gonorrhoea), referring to the remedies as the
second simillimum. He
extended his thinking to chronic diseases, which he sees as slow
running epidemics
based on bacteria and viruses. These became known as Genus
chronicus, CFS being
accompanied by remedies for Parkinsons, Alzheimers and MS
amongst others.
Chappell is controversial as he does not reveal the content of
his remedies: I am very
reluctant to explain something fully which would leave the whole
situation open to
ridicule, because it is ahead of the science and because the
terms arent there to explain
it within the science. (Chappell, Aug 07). Chappell refers to
his remedies as
resonances to distinguish them from being exactly homeopathic,
which are made by
imprinting specific information into water, which has the
ability to memorize and store
information, as is the case for all homeopathic remedies diluted
beyond Avogrados
number. Ullman clarifies the idea of resonance with an analogy
to music: It iscommonly known that when one plays a C on the piano,
other C notes reverberate.
Even on a piano at the other end of the room, C notes still have
a hypersensitivity tothe C resonance. In music theory (and
physics), there is a basic principle that two
things resonate if and only if they are similar. (Ullmann
1991:13).
The rationale behind Chappells trial was clearly to find a cure
for CFS, where so many
other methods, (including homeopathic) had failed. It was
another variation away from
constitutional prescribing, another protocol to try and get to
the root of the condition,
similar to those discussed already by the researcher. Like other
approaches (Weatherley-Jones 2002, Awdry, 1996), the trial although
small, did have a level of success. Much
research was done before by the homeopaths involved, who looked
at over 50 casestreated constitutionally, the results discussed
with Chappell to formulate the identity of
the disease. The remedy was designed as discussed with an
emphasis on the pathology,a granule of PC CFS (the remedy name)
dissolved in water and to be taken daily after
vigorously shaking. All the patients suffered immediate
aggravations and were advisedto discontinue the remedy until their
next consultation. Most of the aggravations faded
away and were followed by an amelioration. Individual treatment
ensued with some
-
8/6/2019 A Critical Examination of the Homeopathic Treatment of
Chronic Fatigue Syndrome
18/18
patients after 6 months ameliorating dramatically, better with
the PC remedy than with
any other treatment they had had before (Vervarcke 2005.) This
concurs with Rawlingstheory that case studies and observations
should be given weight as evidence of cure.
Too often homeopaths such as Chappell, who have had real
successes in terms of cure,are denigrated due to lack of
understanding as to the method. After one year, half the
group showed remarkable improvements and the final conclusion
for 50% was that
they were able to be prescribed a constitutional remedy because
the picture had beencleared. Sadly, a small number of the
participants either had no reaction or had anaggravation to the
remedy without subsequent improvement. On balance however PC
CFS could offer a solution in many cases. It could bridge the
state of no reaction on
homeopathic remedies and fill the gap in our therapeutic
approach. In this sense PC
CFS remedy is a solution and success. (Vervarcke 2005.)
CONCLUSIONS AND RECOMMENDATIONS
It is clear from the research involved in this study, that
current methods of ascertaining
the efficacy of homeopathy are inadequate. The RCT has obvious
limitations asdemonstrated by Sir Michael Rawlins (2008) who has
been Chairman of NICE for the
last ten years. Simply, that the hierarchy of evidence as is now
stands for all methods ofassessing the evidence is inappropriate.
Most of the cases analysed in this study have
positive outcomes, based on observation. The results of the
trials (Weatherley-Jones
2002, Awdry, 1996) as demonstrated were open to interpretation,
depending on who
was critiquing them. However, they were an unbiased
cross-section of the available
evidence because not every case was cured, and there were those
highlighted that
seemed, so far, resistant to any cure. Homeopathy is complex and
cannot be assessed in
a simplistic way. Researchers at Sheffield University are
currently developing new and
rigorous research models that will better fit the homeopathic
paradigm in all its aspects.
Dr Elaine Weatherley-Jones, in her paper Placebo Control Trials
in CAM (2004)
concludes that it is time to redirect our energies into a whole
systems healthcare and
design more relevant pragmatic studies of comparative
effectiveness. This appears to
echo the opinion of Rawlins and other experts in the field of
research.
Thus, based on the findings of this study, the researcher would
like to see in practicethat which Rawlins (2008) proposes: that
hierarchies of evidence should be replaced by
accepting, indeed embracing a diversity of approaches. He is
convinced fromexperience that that it is wrong to replace judgement
with more robust approaches
such as the RCT.
As regards research into CFS specifically, it is hoped that more
trials are undertaken in
the form suggested by Dr Elaine Weatherley-Jones (2004). These
will be more suited to
the homeopathic paradigm, thus delivering a fair assessment of
the evidence, based on a
multidimensional, holistic approach. Our mechanistic society
tends to overestimate thevalue of apparatus, but epidemiology
teaches us this is not correct in medicine. (Rutten
et al, 2006).
To conclude, this study has comprehensively demonstrated that
observation andjudgment must consistently take precedence over
statistical analysis alone.