Embed Size (px)
Citation preview

A CRAWLING
SUSPICION… SHIO YEN TIO
WESTERN HEALTH

Mrs AA • 31 year-old Sudanese lady
• No past medical history, no regular medications
• 4/12 history of progressive weakness of lower limbs
• Needing crutches for mobilisation
• Neuropathic pain
• Impaired sensation from hip down
• 7kg weight loss
• No back pain
• Normal cranial nerves, upper limbs, bladder and bowel functions

Mrs AA
• Came to Melbourne from South Sudan in 2004
• Cleaner at school
• No recreational/ intravenous drug/ alcohol use, non smoker
• 2 previous partners – no history of STIs
• No precipitating event she could recall

Physical Examination • Walking with an aid of 2 crutches, slow ataxic gait
• Normal upper limb neurological and cranial nerves examination
Right Left
Tone Normal, no wasting Normal, no wasting
Power
Hip flex/ ext
Hip abd/ add
Knee flex/ ext
Ankle flex/ ext
Ankle inv/ eversion
3+/5
3+/5
3+/5
4/5
4/5
3-/5
3-/5
3-/5
3+/5
3+/5
Reflexes
Knee
Ankle
Plantar
Absent
Absent
Downgoing
Absent
Absent
Downgoing
Coordination Can’t be tested Can’t be tested
Sensation
Joint position
Pinprick
Vibration
Normal
Impaired to knee
Impaired to knee
Normal
Impaired to hip
Impaired to iliac crest
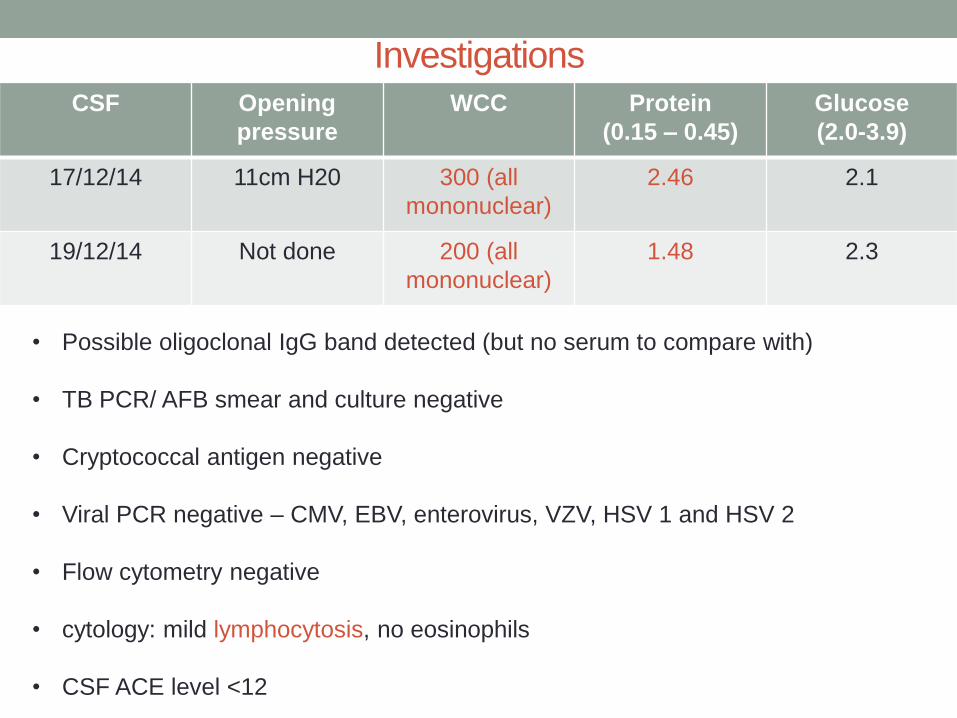
CSF Opening
pressure
WCC Protein
(0.15 – 0.45)
Glucose
(2.0-3.9)
17/12/14 11cm H20 300 (all
mononuclear)
2.46 2.1
19/12/14 Not done 200 (all
mononuclear)
1.48 2.3
Investigations
• Possible oligoclonal IgG band detected (but no serum to compare with)
• TB PCR/ AFB smear and culture negative
• Cryptococcal antigen negative
• Viral PCR negative – CMV, EBV, enterovirus, VZV, HSV 1 and HSV 2
• Flow cytometry negative
• cytology: mild lymphocytosis, no eosinophils
• CSF ACE level <12

Investigations
Negative tests:
• Vasculitic screen
• B12 level
• SPEP
• Serum free light chain
• Urine BJP
• HIV
• Hepatitis B
• Hepatitis C
• HTLV
• Syphilis serology
• Quantiferon gold
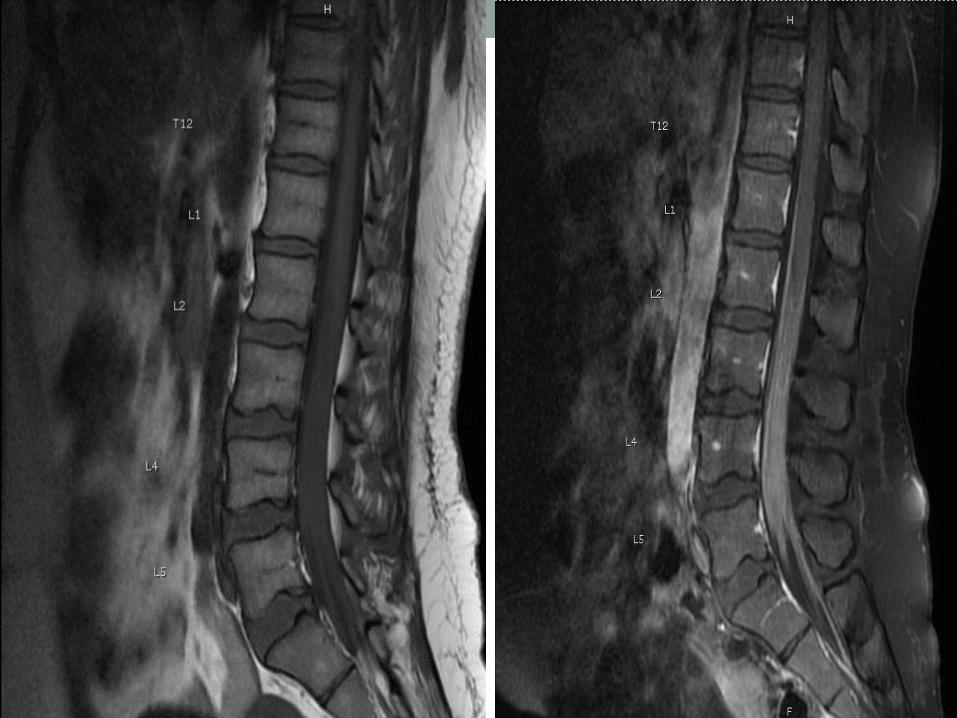


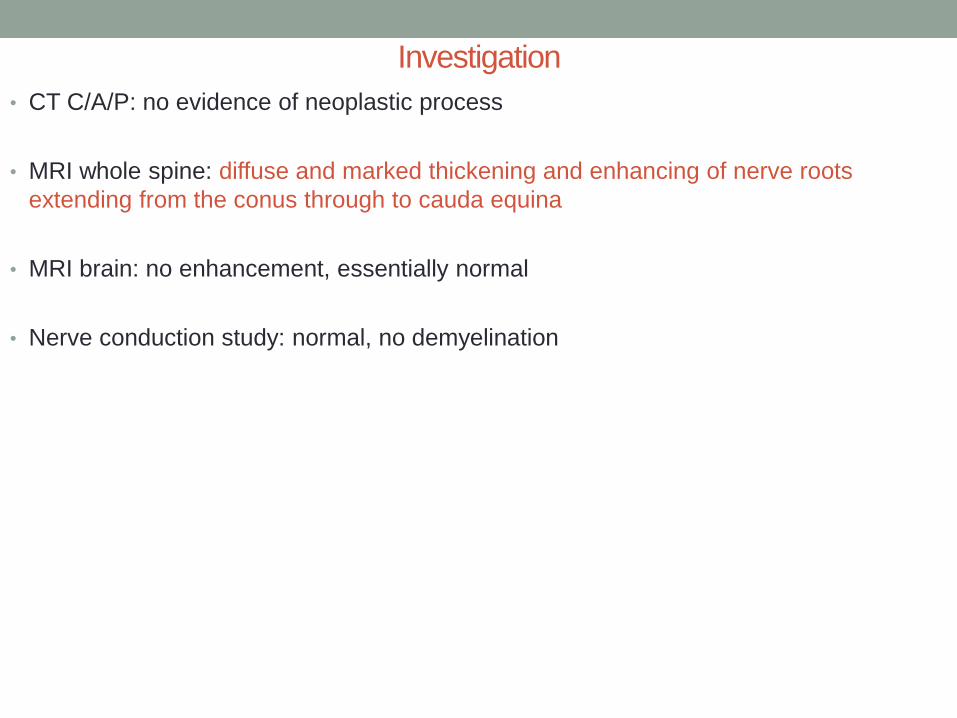
Investigation
• CT C/A/P: no evidence of neoplastic process
• MRI whole spine: diffuse and marked thickening and enhancing of nerve roots
extending from the conus through to cauda equina
• MRI brain: no enhancement, essentially normal
• Nerve conduction study: normal, no demyelination

Progress
• Transferred to RMH for dural, arachnoid and nerve root biopsy
Intra-op finding: swollen cauda equina nerve roots
Dura histology: NAD
Arachnoid: mature T lymphocytes, eosinophils and macrophages, no atypia
Nerve roots: perineural inflammatory infiltrates
No necrotising granulomatous inflammation and tumour

Progress
• Received 3 doses of IV methylprednisolone
• HRZE + dexamethasone started on 12/1/15
Visual disturbance – ethambutol ceased 28/1/15
Steroids induced diabetes started on insulin
Abnormal LFTs improved over time

Progress • Overall slow improvement
• Dexamethasone prednisolone, and Bactrim for PJP prophylaxis
• Schistosoma serology 13.5 (<8.5), strongyloides serology negative
3 x urine and 2 x faecal samples negative for Schistosome ova
Schistosoma serology on CSF (Westmead, unvalidated) – negative
POSSIBLE NEUROSCHISTOSOMIASIS
(SCHISTOSOMAL MYELORADICULOPATHY)

Progress • Praziquantel 40mg/ kg given as a single dose on 18/3/15
Vomited 2nd course given
Increasing early morning headache
Admitted over Easter for meningitis work up:
Raised opening pressure 30cm H20
CSF: WCC 700 (mostly mononuclear), protein 1.47, glucose 3.7
Prednisolone doubled in dose
Headache improved

Outpatient Review (May/ July)
• Marked improvement in lower limbs weakness
• Neuropathic pain resolved
• Ongoing paraesthesia of dorsum of feet
• TB treatment downgraded to Isoniazid and Rifampicin – aim 12-18 months
of treatment
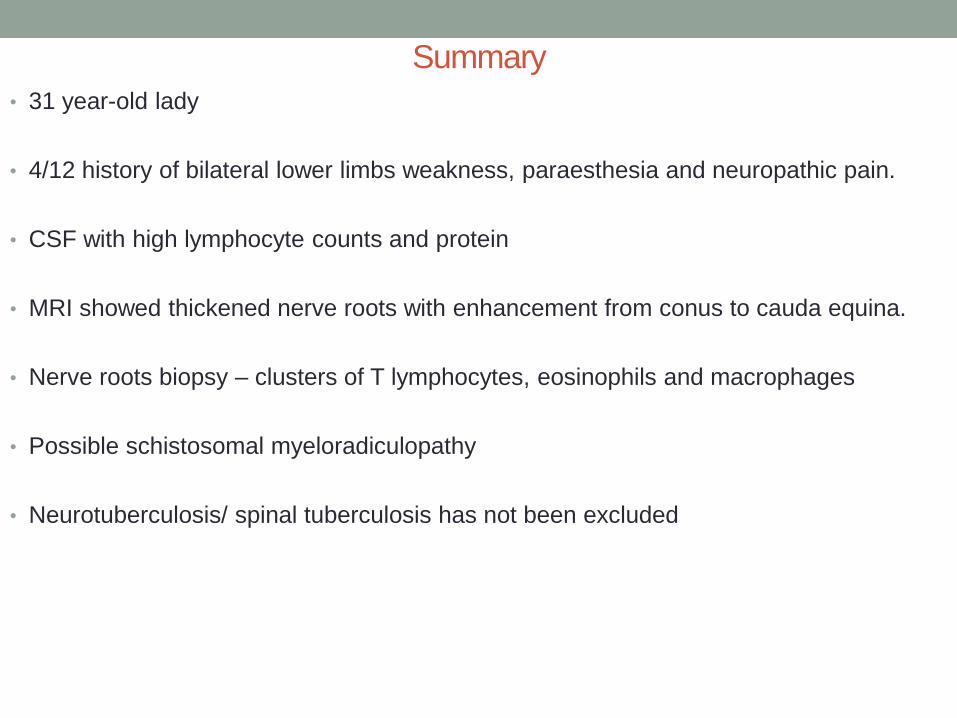
Summary
• 31 year-old lady
• 4/12 history of bilateral lower limbs weakness, paraesthesia and neuropathic pain.
• CSF with high lymphocyte counts and protein
• MRI showed thickened nerve roots with enhancement from conus to cauda equina.
• Nerve roots biopsy – clusters of T lymphocytes, eosinophils and macrophages
• Possible schistosomal myeloradiculopathy
• Neurotuberculosis/ spinal tuberculosis has not been excluded

Neuroschistosomiasis (Schistosomal myeloradiculopathy)
• Introduction & epidemiology
• Pathogenesis
• Clinical features
• Investigations
• Treatment & prognosis

Epidemiology
• World Health Organization (WHO) data 1:
schistosomiasis occurs in 78 countries
100 million with some clinical manifestation
20 million with severe forms of disease
261 million people required preventive treatment in 2013
40 million people were treated for schistosomiasis in 2013
• Annually, over 200,000 people die as a consequence of schistosomiasis. 2
• Schistosomiasis is a Neglected Tropical Disease (NTD). 3

Gryseels et al.
South Sudan, where
Mrs AA is from.


Neuroschistosomiasis
• Neuroschistosomiasis, when symptomatic, is a severe disorder in which prognosis depends
largely on early treatment.
• Not uncommon, under-recognised and morbidity seriously under-estimated. 6
In 1948, Faust published a review on the 82 cases of ectopic schistosomiasis.
8/82 patients presented with signs of spinal cord lesions.
3 of these patients were infected with Schistosoma mansoni.
Conclusion: Be aware of this!!
The American Journal of Tropical Medicine and Hygiene,
28: 175-199, 1948
Author Journal Title Comment
Scrimgeor &
Gajdusek et
al
Brain 1985 Involvement of The Central
Nervous System in
Schistosoma mansoni and S.
haematobium Infection A
Review
Probably contributed to
1% of all non-traumatic
paraplegia in Tanzania,
presumed cause in 5% of
other cases
Carod Artal
et al
Neurology
2004
Schistosoma mansoni
myelopathy
Prevalence:
approximately 5.6%
amongst patients with
inflammatory
myelopathies, Brazil

Spinal Cord Schistosomiasis, 2013, Freitas et al.
The Lancet, 2013, Volume 381 , Issue 9879 , 1788

Spinal Cord Schistosomiasis, 2013, Freitas et al.

Pathogenesis
http://www.yourgenome.org

Neurosciencejournal.org
Pathogenesis

• The host’s cellular inflammatory response to eggs
• Host’s inflammatory response varies in intensity: negligible clinical signs to severe
reaction resulting in space-occupying granulomatous mass and nervous tissue
necrosis
• ?autoimmune process vasculitis and ischemia
Pathogenesis

Clinical Features
NEUROSCHISTOSOMIASIS
Encephalitic or Cerebral
Schistosomiasis/
CNS Pseudotumoral
Schistosomiasis 13, 14
• Encephalopathy with headache
• Nystagmus/ visual impairment
• Delirium & seizures
• Motor deficits
• Ataxia
• Speech disturbances
• Cranial nerves abnormalities
Spinal Cord Schistosomiasis 14
1. Acute transverse myelitis
2. Subacute progressive
myeloradiculopathy
• Lumbar and/or lower limb pain
• Weakness of the lower limbs
• Anaesthesia/hypoesthesia of the lower
limbs
• Paraparesis of the lower limbs
• Bladder dysfunction
• Intestinal dysfunction
• Erectile dysfunction

Diagnosis/ Investigations • Difficult!
Cerebral and spinal schistosomiasis. Carod Artal FJ, 2012

• Spinal cord schistosomiasis (presumptive diagnosis) 15, 16:
a) Typical clinical manifestations (medullar and/ or radicular symptoms) and signs
resulting from lesions of spinal cord
b) Proof of exposure to Schistosoma through parasitological and/ or immunological
methods
c) Exclusion of other possible causes of myelopathy
Spinal Cord Schistosomiasis, Freitas et al, 2013
Diagnosis/ Investigations

Spinal cord MRI at T2
sequence, showing
swelling of conus
medullaris.
Neuroschistosomiasis, Francisco
Javier, Carod-Artal
Expert Rev. Anti Infect. Ther. 8(11),
1307–1318 (2010)

CARVALHO, Gustavo Balthazar da Silveira et al. 2013

1. Medullary schistosomiasis – conus medullaris expansion, linear and nodular
enhancement pattern
2. Tuberculosis – intramedullary tuberculoma is rare (2% of neurotuberculosis
cases); defined granuloma which is hypersignal in T2, peripheral annular
enhancement
3. Neurosarcoidosis – multiple and centrally located, heterogeneously contrast-
enhanced lesions observed with hypersignal on T2 images
4. Neurocysticercosis – intramedullary involvement is rare (2-5%). T2 images
showing multiple hypersignal cyst like nodules
5. Viral transverse myelitis – most frequently affecting thoracic segments and less
frequently conus medullaris. Centrally located hypersignal on T2, with or without
post contrast enhancement, thickening of spinal cord
Radiol Bras, 2013, vol.46, n.1 pp. 51-55

Spinal Tuberculosis
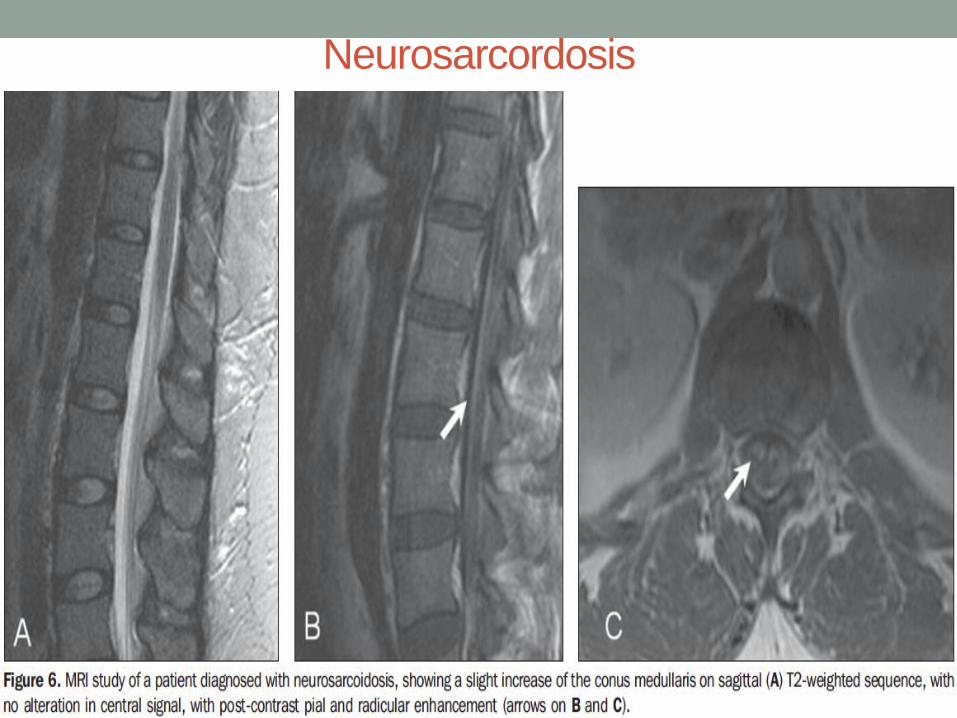
Neurosarcordosis

Neurocysticercosis

Herpes- related myelitis

Sagittal (A) and coronal (B) T2-
weighted MRI of the brain - confluent
high signal in the cerebellum,
especially in the right hemisphere
Coronal
gadolinium-enhanced
T1-weighted
sequence shows
areas of nodular
enhancement in the
cerebellum,
especially in the right
hemisphere.
Neuroschistosomiasis: clinical symptoms and pathogenesis
Ferrari, Teresa Cristina A et al.
The Lancet Neurology, Volume 10, Issue 9, 853 - 864
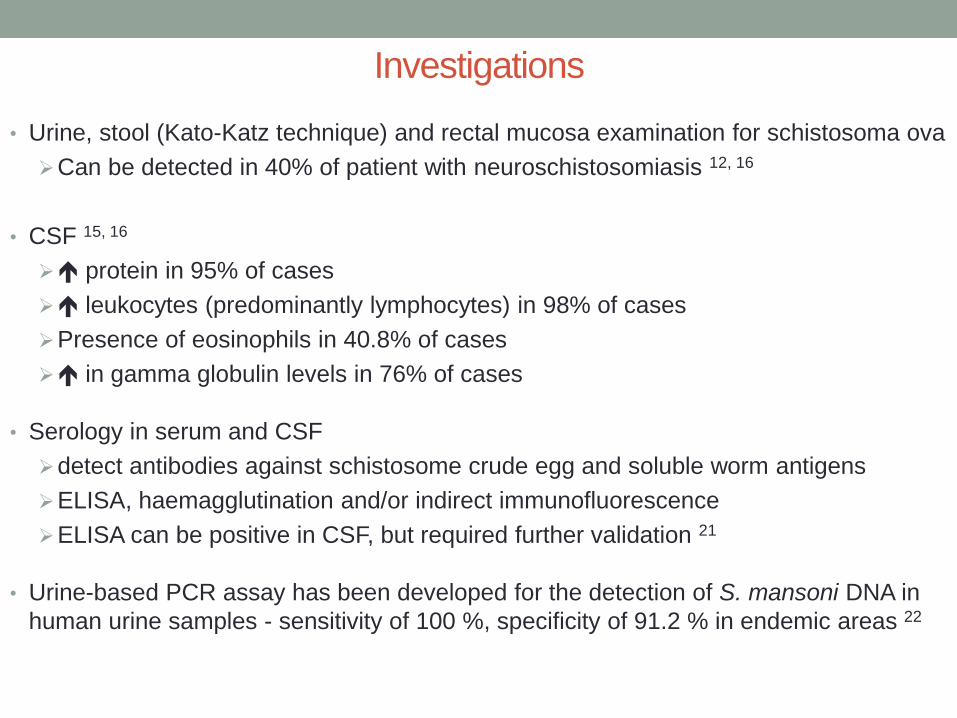
• Urine, stool (Kato-Katz technique) and rectal mucosa examination for schistosoma ova
Can be detected in 40% of patient with neuroschistosomiasis 12, 16
• CSF 15, 16
protein in 95% of cases
leukocytes (predominantly lymphocytes) in 98% of cases
Presence of eosinophils in 40.8% of cases
in gamma globulin levels in 76% of cases
• Serology in serum and CSF
detect antibodies against schistosome crude egg and soluble worm antigens
ELISA, haemagglutination and/or indirect immunofluorescence
ELISA can be positive in CSF, but required further validation 21
• Urine-based PCR assay has been developed for the detection of S. mansoni DNA in
human urine samples - sensitivity of 100 %, specificity of 91.2 % in endemic areas 22
Investigations

• Definitive diagnosis :
Biopsy - may show schistosome ova in various stages of evolution, surrounding
inflammatory reaction
The granuloma around the ova have a necrotic centre that contains schistosome
egg and/or an egg cluster surrounded by epithelioid cells, giant cells and
lymphocytes, and an outer layer of eosinophils, fibroblasts and plasma cells
Freitas et al, 2013 Carod Artal et al, 2012
Diagnosis/ Investigations
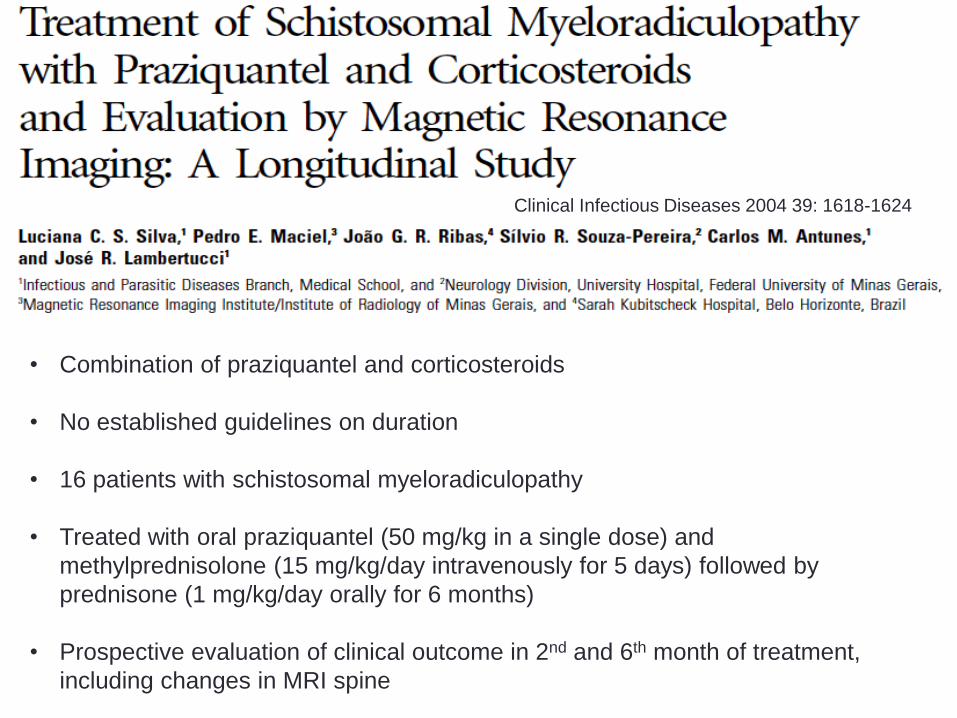
• Combination of praziquantel and corticosteroids
• No established guidelines on duration
• 16 patients with schistosomal myeloradiculopathy
• Treated with oral praziquantel (50 mg/kg in a single dose) and
methylprednisolone (15 mg/kg/day intravenously for 5 days) followed by
prednisone (1 mg/kg/day orally for 6 months)
• Prospective evaluation of clinical outcome in 2nd and 6th month of treatment,
including changes in MRI spine
Clinical Infectious Diseases 2004 39: 1618-1624
• Statistically significant improvement observed in both the 2nd and 6th months
of corticosteroid therapy
• 12 /16 patients had repeat MRI – 3 showed normalisation, 9 showed
improvement in changes
• But this did not necessarily correlate with clinical improvement
• Time to treatment is important – within 30 days
• Steroids > 2 months is associated with better clinical outcome

Conclusion • Neuroschistosomiasis is a severe disorder, often under-recognised.
• Huge migrant population in Victoria.
• Maintain awareness.
• Early diagnosis is essential to reduce severity and disability resulting from it.
• Development and validation of new ELISA and other diagnostic techniques is needed.
• Currently no consensus on duration of schistosomicidal drugs and steroid therapy –
further clinical trials needed.

Thank you!!
• Western Health ID Team
• Western Health Neurology Team
• RMH Neurosurgical Team
• Dorevitch/ Microbiology Department Western Health
• Westmead ICPMR

References
1. http://www.who.int/mediacentre/factsheets/fs115/en/
2. World Health Organization (WHO) http://www.who.int/mediacentre/factsheets/fs115/en/index.html (accessed 7 September 2012)
3. https://www.iamat.org/risks/schistosomiasis
4. Gryseels B, Polman K, Clerinx J et al (2006) Human schistosomiasis. Lancet 368:1106–1118
5. http://www.cdc.gov/parasites/schistosomiasis/biology.html
6. Drummond SC, Silva LC, Amaral RS, Sousa-Pereira SR, Antunes CM, Lambertucci JR. Morbidity of schistosomiasis mansoni in
the state of Minas Gerais, Brazil. Memórias do Instituto Oswaldo Cruz 101: 37-44, 2006.
7. http://www.intechopen.com/books/parasitic-diseases-schistosomiasis/spinal-cord-schistosomiasis
8. Faust EC. An inquiry into the ectopic lesions in schistosomiasis. The American Jounral of Tropical Medicine and Hygiene 28:
175-199, 1948
9. Scrimgeour EM, Gajdusek DC. Involvement of the central nervous system in Schistosoma mansoni and Schistosoma
haematobium infection: a review. Brain 108: 1023-1038, 1985.
10. Carod-Artal FJ, Vargas AP, Horan TA, Marinho PB, Coelho-Costa PH. Schistosoma mansoni myelopathy: clinical and pathologic
findings. Neurology 63: 388-391, 2004.
11. http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(13)60317-7/fulltext?rss%3Dyes
12. Cerebral and Spinal Schistosomiasis, Current Neurology and Neuroscience Reports, December 2012, Volume 12, Issue 6, pp
666-674
13. Ross AG, McManus DP, Farrar J, et al. Neuroschistosomiasis. J Neurol 2012; 259:22.
14. Neuroschistosomiasis, November 2010, Vol. 8, No. 11 , Pages 1307-1318 (doi:10.1586/eri.10.111), Francisco Javier Carod-Artal
15. http://www.intechopen.com/books/parasitic-diseases-schistosomiasis/spinal-cord-schistosomiasis
16. Guidelines for the diagnosis and treatment of schistosomal myeloradiculopathy, Lambertucci JR1, Silva LC, do Amaral RS, Rev
Soc Bras Med Trop. 2007 Sep-Oct;40(5):574-81.
17. Neuroschistosomiasis, Francisco Javier, Carod-Artal, Expert Rev. Anti Infect. Ther. 8(11), 1307–1318 (2010)
18. CARVALHO, Gustavo Balthazar da Silveira et al. Magnetic resonance imaging in the differential diagnosis of infectious and
inflammatory conus medullaris lesions. Radiol Bras [online]. 2013, vol.46, n.1 [cited 2015-07-18], pp. 51-55
19. Neuroschistosomiasis: clinical symptoms and pathogenesis, Ferrari, Teresa Cristina A et al. The Lancet Neurology , Volume 10 ,
Issue 9 , 853 - 864

20. • Zhu H, Yu C, Xia X, et al. Assessing the diagnostic accuracy of immunodiagnostic techniques in the diagnosis of
schistosomiasis japonica: a meta-analysis. Parasitol Res. 2010;5:1067–73. A meta-analysis about the accuracy of
immunodiagnostic techniques in schistosomiasis japonica.
21. Ferrari TC. A laboratory test for the diagnosis of neuroschistosomiasis. Neurol Res. 2010;32:252–62.
22. Enk MJ, Oliveira E, Silva G, Rodrigues NB. Diagnostic accuracy and applicability of a PCR system for the detection of
Schistosoma mansoni DNA in human urine samples froman endemic area. PLoS One. 2012;7:e38947.
23. FREITAS, André Ricardo Ribas; OLIVEIRA, Augusto César Penalva and SILVA, Luiz Jacintho. Schistosomal myeloradiculopathy
in a low-prevalence area: 27 cases (14 autochthonous) in Campinas, São Paulo, Brazil. Mem. Inst. Oswaldo Cruz [online]. 2010,
vol.105, n.4 [cited 2015-07-18], pp. 398-408
24. Luciana C. S. Silva, Pedro E. Maciel, João G. R. Ribas, Sílvio R. Souza-Pereira, Carlos M. Antunes, and José R. Lambertucci
Treatment of Schistosomal Myeloradiculopathy with Praziquantel and Corticosteroids and Evaluation by Magnetic Resonance
Imaging: A Longitudinal Study. Clinical Infectious Diseases 2004 39: 1618-1624.
25. CARVALHO, Gustavo Balthazar da Silveira et al. Magnetic resonance imaging in the differential diagnosis of infectious and
inflammatory conus medullaris lesions. Radiol Bras [online]. 2013, vol.46, n.1 [cited 2015-07-19], pp. 51-55 .





























