Embed Size (px)
Citation preview
227
A CONSIDERATION OF SOME OF THE PROBLEMS PRESENTED BY EPILEPSY.
By ROBERT THOMPSON (Armagh).
T HE appearance of fits in a child, adolescent or adult, is a~ occurrence of very considerable gravity, and one which, as a rule, exerts a profound shock on the immediate relatives. Although the
gravity of the issues at stake is fully realised by most doctors, the correct and essential steps in diagnosis and treatment are, generally speaking, only vaguely comprehended, with the result that vital months and years during which treatment might have been effective are frittered away, and full investigation and correct methods of treatment are instituted only when it is too late. The paper which follows will attempt to cover the usual clinical problems presented by epilepsy, without aspiring to touch upon recent work in the biochemical or encephalographic fields.
Case-Taking. With a history of fits of any kind it is imperative in the first place to
decide whether these are truly epileptiform in nature; this, of course, equally applies to a history of "fainting attacks ", unexplained periodic bed-wetting, unexplained falls, attacks of " weakness " or "giddiness " . I f there is a tendency to a "fal l " or a "faint " of any kind, at any age, epilepsy must be excluded.
Points strongly in favour of epilepsy (as against hysteria) are attacks without any emotional setting, attacks at work, attacks when alone~ attacks during sleep or while in bed, injury during attacks, sleep or confusion following attacks, intense headache associated with attacks, premonitory symptoms of attacks. Careful evaluation of all the points~ of the history, and especially of the observations of a near relative, wilI make the diagnosis clear in the vast majority of cases, but a residue of doubtful eases will still remain in which the only course open is t~ admit the patient to hospital, stop all treatment, and wait for the next attack which you hope will at least be observed by an experienced sister.
Convulsions in Ch~hood. Convulsions in childhood are rarely treated with the skill and care
that such a grave development demands. Apart from the quite con- siderable risk of death during a convulsion, the onset of a fit of any kind in infancy or childhood is a matter which should be regarded witI~ the utmost seriousness, calling for the most skilled investigation an~l treatment. Not infrequently a repetition of convulsions continues without appreciable break into the epilepsy of childhood, with, lmles$ the most prompt measures are taken, an almost certain hnpairment of mental development. More frequently, perhaps, there is a free gap of ten or twelve years before fits reappear. In these cases I think it i~ only fair to assume that the neglected oonvulsions of infancy had fixe~ the neutral pattern for the later development of epilepsy.
The examination of a child who has just had his first convulsion is s vital procedure. Everything must be questioned : food, elotking, general r~,ime, sleep, bowels, intercurrent infections. The most common mis~
228 IRISH JOURNAL OF MEDICAL SCIENCE
take is the too hasty attribution of the convulsion to constipation or teething, and letting the investigation drop at this point. The average healthy child should not react to either constipation or teething in this manner, and even an intercurrent infection should not stop the investigation.
Food is always the first thing to be scrutinised; it may be wholly beyond the powers of digestion of the child, greatly deficient in fluids~, given irregularly, deficient in vitamins, etc. After any convulsive attack the diet should be immediately reduced to glucose and water alone for 24 to 48 hours; afterwards, for the next two to three weeks to a diet several months below the age of the child, and this continued until the danger period appears to have passed.
Clothing is not often mentioned, but I have seen a child suffering from convulsions almost smothered with some eight to ten layers of woollies on top of a binder.
Again, the general r6gime must be analysed in detail. Is the mother competent, and can she handle her child with self-confidence? The anxious, frightened mother who has no self-confidence produces the sleep- tess, irritable baby who ends up in convulsions. Or has the mother some weird plan she religiously follows~. For example, does she allow the child to cry its heart out and refuse to t ry to pacify it ? There arc all sorts of strange rituals followed by some mothers, but surely the most bizarre is the belief that crying does a child no harm or that a child needs no variation in its life beyond its feeding and toilet requirements.
This, of course, by no means ends the investigation. The general nourishment must be observed and signs of dehydration detected. The possibility of a very early stage of rickets or of latent syphilis must be kept in mind. Some twenty years ago I saw a boy of 11 years who had recently developed epilepsy. He had suffered from convulsions in childhood. He was a healthy-looking, well-developed boy, with no stigmata of any kind, but a lucky "hunch" revealed a plus 3 Wassermann. Bismuth treatment completely controlled the fits within a year, and he has kept well since. (Nowadays penicillin would be infinitely more effective.)
When everything has been investigated, the nursing rfigime corrected and an extremely simple dietary instituted, the question of further medicinal treatment must be considered. Here I believe there is still a field--perhaps the only field in which bromide is of value in epilepsy. We have to assume that following the first convulsion the nervous system is in a highly irritable state, and until the new r6gimc has begun to take effect it will be wise to give an appropriate dose of bromide for at least several weeks and to keep the child under close observation.
Idiopathic Epilepsy in Adolescence. The early teens is a favouritc period for the onset of idiopathic
*Experimentally it may be true tha t hydration favours convulsions m o r e t h a n dehydration, but in all childrens' affections, constipation, pyrexia, marasmus, etc., d e h y d r a t i o n is t h e prevailing evil and is often in fact one of the main causes.
SOME PROBLEMS PRESENTED BY EPILEPSY 229
epilepsy, an onset which as a rule comes as a tragic shock to the parents. These cases require preliminary investigation on similar lines to cases of convulsions in childhood. There must be a complete and compre- hensive check-up on the physical health and all sources of irritation (e.g., tonsils, adenoids, carious teeth, refractory errors) eliminated. At the same time the entire r~gime must be overhauled, e.g., amount of sleep, friction in the home, happiness at school, physical or mental over- work. Next to be considered is the diet. Here I always prescribe extremely simple meals, avoiding such things as pastry, suet puddings and rich soups. No heavy meal should ever be taken, and it is often best to avoid anything after 7-8 p.m., but if especially desired a glass of milk and a biscuit could be taken an hour before going to bed. Not more than four hours should elapse between moals.
Having dealt with the diet and general r~gime, the crucial question of the medicinal treatment of epilepsy must now be faced. It can now fairly be stated that except in infants, for whom phenobarbitone would be difficult to prescribe, bromides are no longer of any real value in epilepsy and, if prescribed, usually only lead to bromide rashes and bI~)mide intoxication. In phenobarbitone, however, we have the sheet anchor in the treatment of epilepsy. I t must be stepped up to an effective dose, the doses spaced equally, as far as possible, over the twenty-four hours, and a dose never omitted for any consideration. Relatives should be instructed to make a note in writing of the date, time and nature of every fit.
In epanutin we have another very effective agent. In some cases of epilepsy, in which phenobarbitone is ineffective in safe doses, epauntin will be completely effective, while in others the reverse will be found to be the case. In other cases the best result is obtained by a combination of the two drugs, say phenobarbitone at 8 am. and 8 p.m. and epanutin at 2 p.m., or the reverse. Where there is much restlessness, irritability or sleeplessness, phenobarbitone will usually be found to be essential; its sedative as opposed to its anticonvulsant action is much greater than that of epanutin. The important fact to grasp, however, in the medicinal treatment of epilepsy is that dosages and combinations of phenobarbitone and epanutin must be experimented with until the fits are completely controlled, and thereafter the treatment must be kept up for yeaxa (Tridione, with suitable precautions, has recently been strongly recom- mended for cases of uncomplicated petit real, which in practice are velT rare.)
A moderate " standard " dose of pbenobarbitone for an adult is one and a half grains twice daily, and of epanutin one and a half grains, in capsules, three times a day after food. Children require, as a rule, proportionately much larger doses, which they tolerate excellently. Thus I have one boy of eleven who is just controlled by the above dose of phenobarbitone, which keeps him in robust physical and mental health, and another boy of seven who requires half the adult dose of epanutin. When the dose is just sufficient to control the attacks the patient displays his maximum physical and mental health.
The reappearance of a fit, major or minor, indicates immediately, that the effective dose or combination of drugs has not been reached and no effo~ must be spared to reach this and to reach it quie, kly. Epilepsy
230 IRISH JOURNAL OF MEDICAL SCIENCE
thus controlled gives a very fair hope of complete and lasting cure, but with ineffective control the outlook is one of extreme gravity and a big percentage of such eases either die in status epileptieus or develop psychotic episodes which necessitate their permanent incarceration in a mental hospital.
Epilepsy in Later Life. Epilepsy appearing for the first time in middle life should arouse
the strongest suspicion that it is based upon organic cerebral changes. Brain tumour must be excluded and any possibility of syphilitic infec- tion. I f neither of these conditions is present, the most likely third cause will be arteriosclerotic changes; in the latter case the appearance of fits sometimes seems to be hastened by alcoholism. It will thus be seen that the treatment of this form of epilepsy resolves itself into the treatment of the cause.
Early arteriosclerotic ehanges which give rise to any mental distur- bance, including epilepsy, carry with them a very poor prognosis. (It is essential, of course, to be certain that the disturbance is based upon these ehangos and that the latter are not an accidental accompaniment.) "thus, in the ease of epilepsy arising in middle and later life, the gravity ~)f the outlook depends on the cerebral and general arteriosclerosis and not upon the occurrence of fits which, as a rule, are very infrequent. I t is, therefore, a question to be decided whether in fact any treatment will be directed towards stopping the fits. The whole general picture must be taken into consideration, state of heart and arteries, blood pressure, amount of sleep, restlessness or irritability, degree of memory failure. In the case of poor sleep combined with a good deal of restless- heSS or irritability, phenobarbitone may give considerable relief from its effects upon the fits. In a case in which there is no restlessness or irritability, but considerable somnolence and memory failure, the general l~icture may be made worse by any type of anticonvulsant drug; here it may be wiser completely to ignore the presence of an occasional fit.
In exceptional eases, epilepsy reappears in middle life after a lapse of fifteen to twenty years. In such cases, energetic antieonvulsant treatment, along the lines already indicated, will probably yield the best dividends.
Epilepsy in Old Age. Epileptiform convulsions not infrequently make their first appearance
in the senile and arteriopathie dementias between the ages of sixty-five and eighty-five. (These are frequently referred to as "seizures ", but I think the term should be reserved for the " seizures " which appear ia the course of general paralysis.)
Fits as a rule are very infrequent and anticonvulsant treatment is rarely called for, but the appearance of a fit renders the nursing of these patients more hazardous, and they must thereafter sleep in night observation or, if at home, in a room with a relative or nurse. Other pre- cautions regarding epilepsy must be observed. While it might be thought that there was a special danger to life in fits occurring at advanced ages, my experience has been that fits are tolerated well in old age and are usually mild in character.
SOME PROBLEMS PRESENTED BY EP1LEPSY 23].
Status Epilepticus. In the case of epilepsy of any severe degree, viz., where it is found
next to impossible to control the fits, or where control can only be obtained by maximum doses of anticonvulsant dru~, status epilepticus must always be feared, and it is often wise to convey to the relatives the probability of this complication and the dangers which it may threaten. One attack of status also seems to predispose the patient to others and the successful handling of one attack is no guarantee that treatment will be equally successful in subsequent attacks. In institu- tions, the occurrence of status occasions more anxiety thau almost any other complication. The best way to deal with it is, if at all possible, to prevent its occurrence. This is done as a rule by good nursing, that is, by never omitting a dose of the antieonvulsant drug, attention to the bowels, diet, etc., but even granting all this it is, unfortunately, true that attacks of status will arise. In St. Luke's Hospital we have found the following rules most useful in warding off threatened attacks; many attacks seemed, as it were, nipped in the bud, whereas if staff had to wait for directions, attacks would probably be well under way when the doctor arrived. The rules were drawn up after the death of a strong, healthy man in his sixth fit, one and three-quarter hours from the beginning of status. (He had received an injection of pheno- barbitone (3 grs.) after his second fit.) Death may occur at any stage in status, but is much more usual after a long series of fits which nothing seems to control.
Epil~ic Parietal. Threate.~ 8ta~us £pileptlcus.
The following directions are set out for the guidance of Nursing Staff when dealing with Epileptic Patients : -
In the event of a pa t ient taking two fits in fairly rapid succession an injection of moluble phenobarbi tone (grains 3 in one c.c.) is to be given immediately and the Medical OiBcer notified of such action.
The pa t ien t mus t be careftdiy observed and if the injection is followed by more than one fit the Medical Officer mus t again be informed without delay. I f the Medical Officer is not immediately available and any fur ther fit occurs the patient may receive a n injection of morphia, grain one quarter .
During and after fits the pa t ien t ' s condition, pulse rate and volume, respiratory distress, facial colour, signs of shock, confusion and r~stlessnsss0 must be carefully noted. The general pa t t e rn of the fit, t h a t is, durat ion and whether light or heavy, should also be noted.
Fi ts occurring a t short intervals, t h a t is, under half an hour, must be regarded with the u tmost seriousness and the Medical Officer notified forthwith. I f breathing Stel~ suddenly in the middle of a fit artificial respiration should he immediately performed and one c.c. Coramine injected by another nurse. Care should be taken tha t the tongue has not been swallowed and is obstructing breathing.
No food or fluids should be given by mouth unt i l recovery is complete0 and afterwarda fluid diet only. When recovery is complete an enema should be given.
The foregoing rules are to be carried out in respect of all known adult epileptico, bu t in pat ients from 7 to 14 years of age the injection of soluble phonobarbitono will only be one half c.e. (one and a half grains). Morphia will not be given un leu a u t ~ by a Medical Officer.
In the event of a pa t ient who is not an established epileptic undergoing an epfleptfform fit the Medical Officer mus t be notified immediately.
I t shall be the du ty of Charge and Acting Charge Nurses to m~lre their subordimbte staff thoroughly conversant wi th these rules and they ~mll be r~ponsibJe for tlmir efficient application in their respective wards.
The above rules, of course, only apply to the threatened occurrence of status. I f the condition develops in spite of these precautions the
232 IRISH JOURNAL OF MEDICAL SCIENCE
doctor must use his judgment as to when to give further injections of phenobarbitone, morphia, etc. Paraldehyde by the rectum (three or four drachms in two ounces of olive oil or syrup) is highly recommended by some writers, but my experience of rectal medication in this con- dition has been disappointing. Not infrequently the rectum is loaded with fmces, but even when emptied, there is no guarantee that the drug will be retained and one can often make only the vaguest guess as to the probable amount absorbed.
Both Symonds 1 and Nattras 2 strongly favour the intranmscular injec- tion of paraldehyde, 8 to 10 ml. given forthwith and smaller amounts repeated half-hourly if required. In dangerously exhausted patients S~nonds favours thiopentone intravenously (0.25 g. for an adult) followed by intramuscular paraldehyde if necessary. For patients who are known not to respond well to phenobarbitone, Hill a recommends intravenous sodium amytal (grains 7½ in 10 c.c. water). Hill also recommends the administration of continuous intravenous 5 per cent. glucose saline, a procedure which certainly should be of assistance in combating the rapidly increasing degree of shock.
The " Insane Epileptic ".
There is frequently much misunderstanding about what is meant by the term "insane epileptic ", an ugly and clumsy expression, but one which, unfortunately, has taken root. Perhaps a working definition would be " an epileptic who periodically displays, either in association with fits or apart from them, such states of excitement, threatened violence, impulse, suspicion or confusion, as to render him a danger to the community in which he lives ". It will thus be seen that it is usually a matter of judgment to decide when any of the above conditions has advanced to the degree which would render the patient a menace to those around him. It will also be seen that the condition is usually essentially a periodic one, and that nothing like a continuous psychosis can be expected. The" insane epileptic " is, as a rule, rational, cheerful and co-operative until the psychotic episode sets in; this may be a flect- ing outburst of violence, lasting from ten minutes upwards, or an acute confusional episode of from several days to one or two weeks. In some cases a degree of hostility or suspicion against some particular individual may be the only evidence, or may continue after the acute episode has passed off.
In all cases of severe epilepsy the occurrence of psychotic episodes must be expected sooner or later, and a warning to the relatives will prepal~ them for this contingency, so that they will the more readily agree to allow the patient to be sent to an institution before a tragedy happens. My own experience of such cases forces me to adopt a gloomy prognosis. It is only in rare instances that sufficient adjustment takes place to allow such a patient to be discharged to the care of his relatives; such adjustment can hardly ever be expected unless some change in treatment completely controls the fits. I f fits are occurring, even at long intervals, my experience has been that sooner or later another psychotic episode will make its appearance, usually in association with fits, but sometimes quite apart from them.
SOME PROBLEMS PRESENTED BY EPILEPSY 233
For the " insane epileptic ", occupational therapy in an institution, together with the optimum anticonvulsant therapy, is the treatment of choice. These patients require very tactful handling, but if properly nursed are usually cheerful, helpful patients. Their requests for dis- charge should not be blunt]y turned down, and they thrive on praise and encouragement. Frequently they bring greatly exaggerated or unfounded charges against patients or staff (the established epileptic tends to be an irritable, self-centred and often somewhat self-righteous individual) but patient listening to such charges, with a promise to go into them, is usually all that is required. In a short time the patient is back to his cheerful, useful life. Tactless or ignorant nursing of such patients produces, of course, conditions reminiscent of the " Snake Pit "
General Ma~agement of Epilepsy.
It is illegal for epileptics to be in charge of any mechanically- propelled vehicle. Epileptics should be warned against going into positions of unnecessary danger, such as going to an open well for water, attending to fires, standing on the edge of a railway platform, going up a ladder for any purpose. Labourers should be particularly warned against acting as "hod men ", or ascending scaffolding for any purpose. Such an action inevitably endangers other lives as well as their own. Epileptics should also be instructed never to lock the door of a lavatory or bathroom, and they should never omit to remove false teeth at night. A pillow stuffed tightly with coarse fibre must always be used to obviate the possibility of suffocation by a large mass of material being drawn into the mouth during a fit; a low bed should be used to lessen the risk of falling out. In the actual fit, it is usually only necessary to undo tight clothing around the neck and to place the patient in a comfortable, semi-prone position with the head well turned over to one side. (Experience with E:C.T. indicates that pulmonary abscess from the inhalation of infected saliva is probably the greatest risk of any fit whether spontaneous or electrically induced.) If the fit occurs during a meal, or if it is suspected that the patient has been chewing something, a forefinger should be swept around the mouth and pharynx. This, of course, must be done if there is the slightest sign of respiratory obstruc- tion at the beginning of respiration. Only a small percentage of epilepties tend to bite the tongue in a fit and it is only in thes~ cases that something incapable of being bitten through should be placed between th~ teeth. After the fit, the patient should be left undisturbed as long as possible to "sleep it off "
Epileptics may be allowed to smoke in moderation, but alcohol in any form should be prohibited. The diet has already been referred to. In schools it is not usually thought necessary to prohibit an epileptic from taking part in combined games. For some strange reason, an epileptic fit in such circumstances is extremely rare. Special care must always be taken in swimming baths or when bathing, and an epileptic must never be allowed to bathe alone.
I t must be kept in mind that a history of epilepsy does not preclude the development of anxiety neurosis. I have had three patients, all former epileptics (one had fits as recently as twelve months before and
234 I R I S H J O U R N A L OF M E D I C A L S C I E N C E
was still controlled by phenobarbitone), who displayed the typical symptoms of anxiety neurosis--depression, sleeplessness, weeping-- to which I have referred elsewhere2 All made excellent recoveries with E.C.T. In such cases I do not think there is any real danger of re-establishing the epilepsy ; the fear that epilepsy might follow the usual course of E.C.T. in depressed states has been proved to be quite unfounded.
Conclusion.
I have tr ied t o present some o f the problems with which one is con- f ronted in dealing with eases of epilepsy from childhood upwards and to suggest how, in my opinion, these problems can best be taclded in the light of our present knowledge. I f I would emphasise one point, it is that epilepsy is a condition which must be energetically and scientifically dealt with, and that when this is done one will often be amazed at the response and at the continuous diminution of the gravi ty of the outlook. When this is not done, however, even in the mildest cases, progressively graver problems continue to arise and it is probably t rue to say that in no other disease does one so frequently deplore " t h e years that the locust hath eaten ".
~f~r~8. 1. Symonds (Nov. 4, 1950). " Management of the Epileptic," B.M.J . 2. Nattras (Jan. 8, 1949). " Clinical and Social Problems of Epilepsy," B . M . J . 3. Hill. " Treatment of the Epilepsies," Physical Me~hods of Trea~ne~ in Psychi~y.
(Sargant and Slater). Livingstone. 4. Thompson (March, 1951). " The Diagnosis and Treatment of the N e ~ in
Out-Patient Practice." Practitioner.
THE QUIET ART. In his Gonfceaio~s of ar~ Un.coranum Attoraey. Reginald Hine confessed to having
kept a series of common.place books from his youth up : this "honourable habit " had been practised aforetime by such wise men as Leonardo, Milton and others, such as the gentle Archbishop Parker who admitted to " toying out his time with copying of books." Tnfly, legere et nihil colligere eat negligere. Dr. Robert Coope is clearly of their blood, considering with Samuel Butler that " appropriate passages are to be appropriated." His appropriations from the writings of medical men from Clifford Allbutt to Zachary Cope will bring pleasure and enlightenment to any and every doctor who is wise enough to secure his delightful anthology (The Quiet Art, Living- stone, 1952) for his bedside reading. It belongs distinctly to that class of good books which Dr. Johnson declared should help one to enjoy life rather than to endure it. The collector's pleasure should be matched by his readers' gratitude.
W.D.
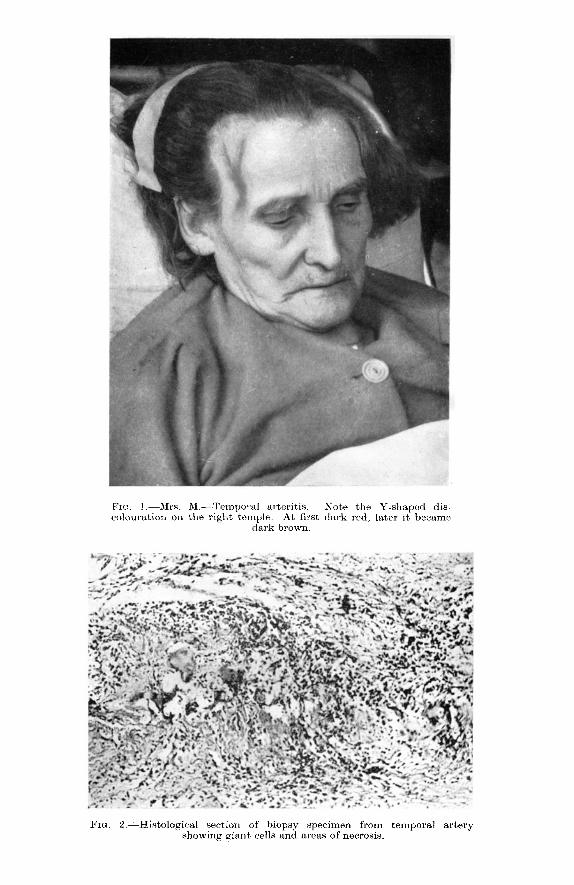
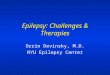
FIG. I.--~.h.s. M.--Temporal arteritis. Note the Y-shaped dis- colouration ol~ the right temple. At first dark red, later it became
dark brown.
FIG. 2.--Histological section of biopsy specimen from temporal artery showing giant cells and areas of necrosis.