Embed Size (px)
Citation preview

FACULTEIT GENEESKUNDE EN
GEZONDHEIDSWETENSCHAPPEN
Academiejaar 2012 - 2013
A comparison of the remineralisation effect of
CPP-ACP, fluoride and a combination on initial
caries lesion
Charlotte VAN ELST
Promotor: Prof. dr. Guy De Pauw
Copromotor: Prof. dr. Ronald Verbeeck
Masterproef voorgedragen in de Master na Master Opleiding Orthodontie


FACULTEIT GENEESKUNDE EN
GEZONDHEIDSWETENSCHAPPEN
Academiejaar 2012 - 2013
A comparison of the remineralisation effect of
CPP-ACP, CPP-ACPF and fluoride
on initial caries lesion
Charlotte VAN ELST
Promotor: Prof. dr. Guy De Pauw
Copromotor: Prof. dr. Ronald Verbeeck
Masterproef voorgedragen in de Master na Master Opleiding Orthodontie

De auteur(s) en de promotor geven de toelating deze Masterproef voor consultatie
beschikbaar te stellen en delen ervan te kopiëren voor persoonlijk gebruik. Elk ander
gebruik valt onder de beperkingen van het auteursrecht, in het bijzonder met betrekking
tot de verplichting uitdrukkelijk de bron te vermelden bij het aanhalen van resultaten uit
deze Masterproef.
Datum 09/08/2013
Charlotte Van Elst Prof. dr. Guy De Pauw

Voorwoord
Deze Master na Masterproef kwam tot stand met behulp van verschillende mensen en deze wens ik hier graag te bedanken.
Speciale dank gaat uit naar Petra Maes, die niet alleen de zware taak had om mij te helpen met het analyseren van de coupes maar wiens steun en begrip eindeloos was.
Mijn oprechte dank gaat ook uit naar Lynn Hauspy voor de talloze uren van hulp en gezelschap.
Chris Vercruysse dank ik graag voor zijn hulp bij het opstellen van de onderzoeksmethode en wiens geduld groot was om mij de nodige technieken in het labo aan te leren.
Mijn copromotor, Prof. dr. R. Verbeeck, wil ik van harte danken voor het verstrekken van onontbeerlijke informatie en het constant kritisch evalueren.
Mijn promotor Prof. dr. G. De Pauw bedank ik graag voor de kritische blik en het coachen van mijn masterproef.
Tenslotte wil ik ook mijn collega’s, mijn familie en Bernard bedanken voor hun niet aflatende morele steun gedurende de voorbije jaren.
“Learn from yesterday, live for today, hope for tomorrow.”
Albert Einstein

Table of contents
Samenvatting .............................................................................................................................. 1
Abstract ...................................................................................................................................... 3
Inleiding ..................................................................................................................................... 5
Study of the literature ................................................................................................................. 6
1. Caries process and white spot lesions .......................................................................... 8
2. Anticariogenetic properties of CPP-ACP (GC Tooth MousseTM) ............................. 19
3. Mechanism of action of fluoride (Elmex Medical Gel®) ......................................... 20
4. Interaction of CPP-ACP and fluoride (MI Paste PlusTM) .......................................... 23
5. Quantifying enamel demineralisation ........................................................................ 24
Aim of this study ...................................................................................................................... 29
Methodology ............................................................................................................................ 30
Results ...................................................................................................................................... 36
Discussion ................................................................................................................................ 44
Critical evaluation .................................................................................................................... 49
Conclusions .............................................................................................................................. 50
References….. .......................................................................................................................... 51
Annexe…………...…..…………………………………………………………….……...….....…63

1
Samenvatting
Introductie: Ondanks preventie, blijft het ontstaan van “white spots” tijdens de
orthodontische behandeling met vaste apparatuur nog steeds een belangrijk klinisch probleem
(prevalentie white spot laesies -WSL- van 2% tot 97%). De verhoogde prevalentie van deze
glazuurontkalking tijdens de behandeling is deels te wijten aan het feit dat brackets voor een
onregelmatig oppervlak zorgen en dat er een beperking is van het zelfreinigend mechanisme
van speeksel en de beweging van de orale spiermassa. Na het verwijderen van de apparatuur
blijven “white spots” zichtbaar door hun opaak, kalkachtig uitzicht op het glazuur en kunnen
ze een esthetisch probleem zijn voor de patiënt. Een goede mondhygiëne tijdens een
orthodontische behandeling is daarom absoluut noodzakelijk. Verschillende producten (zoals
fluoride en meer caseïne fosfopeptide-amorf calciumfosfaat) worden gepromoot voor het
voorkomen en remineralizeren van WSL.
Doel: Het doel van deze studie was het in vitro effect van fluoride, CPP-ACP (caseïne
fosfopeptide-amorf calciumfosfaat) en een combinatie van beide (CPP-ACPF) te vergelijken
met een controlegroep op de remineralisatie van WSL na 6 en 12 weken.
Materiaal en Methoden: 96 premolaren werden in twee gesplitst (buccaal en palataal). WSL
werden gecreëerd met een demineraliserende oplossing gedurende 96 uur, gevolgd door een
pH-cycling regime van 3 dagen. De premolaren werden in vier groepen verdeeld: een fluoride
groep (Elmex Medical Gel®), een CPP-ACP groep (Tooth Mousse TM), CPP-ACPF groep
(Mi Paste Plus TM) en een controle groep. Elke groep werd behandeld volgens de instructies
van de fabrikant (GABA, Lörrach, Duitsland en GAC Europe, Nieuwegein, Nederland). Alle
tanden werden dagelijks gepoetst met een tandpasta (1450 ppm fluoride) behalve de controle
groep. Op drie verschillende plaatsen van de WSL werd met microradiografie na 6 en 12
weken de volgende acht parameters gemeten: diepte van de totale laesie (DTL), de
‘body’laesie (DBL), de diepte van de oppervlaktelaag (DSL), de maximum “mineral content
van de surface layer” (MSL), de minimum “mineral content van de body of the lesion”
(MBL), het demineralisatie volume (VD), de basis minerale hoeveelheid (BMC) en het aantal

2
“body laesies”(NBL). Verschillende statistische tests werden uitgevoerd om de groepen te
vergelijken na 6 en 12 weken. Het significantieniveau werd ingesteld op p <0.05.
Resultaten: De Student’s t-test toonde geen statistisch significant verschil tussen de palatale
en buccale zijden voor de verschillende variabelen. De Wilks' Lambda exact test vertoonde
een sterk significant verschil (p<0.001) voor de testgroepen tussen 6 en 12 weken en geen
verschil voor de controlegroep (p=0.402). Na 6 weken was het punt BMC-DTL significant
verschillend in mineraalgehalte en laesiediepte voor de fluoridegroep versus de controlegroep
(p=0.045) en voor de CPP-ACP groep versus de CPP-ACPF groep (p=0.041). Na 12 weken,
waren de testgroepen zeer sterk verschillend (p<0.001) t.o.v. de controle groep voor de
verschillende parameters. BMC-DTL was statistisch significant lager voor CPP-ACPF versus
de fluoride groep (p=0.025) en versus de CPP-ACP groep (p=0.03). De Friedman test toonde
geen significant verschil aan voor het volume van demineralisatie (VD) van de drie
testgroepen tussen 6 en 12 weken. Er was meer remineralisatie (lagere VD) bij de testgroepen
dan bij de controlegroep (p=0.007). De Pearson Chi-Square test en de Fisher ’s exact test
toonden geen verschil in het aantal NBL na 6 weken, wel na 12 weken (p< 0.001).
Conclusie: De resultaten van deze studie toonden geen significante verschillen tussen de drie
experimentele tandpasta’s voor de regressie van de WSL. Pas na 12 weken was er een
statistisch significante verbetering van de laesiedieptes van de drie experimentele tandpasta in
vergelijking met de controlegroep. De laesiediepte, maar ook het mineraalgehalte, van de
WSL is aanzienlijk lager na 12 weken voor de experimentele tandpasta.

3
Abstract
Introduction: Despite prevention, the development of white spot lesions (WSL) during
orthodontic treatment with fixed appliance still is a significant clinical problem (the overall
prevalence of WSL varies from 2% to 97%). The increased prevalence of enamel
decalcification during fixed appliances therapy is partly due to the irregular surface of
brackets, bands and other attachments and a limitation of the self-cleansing mechanism such
as saliva and the movement of the oral musculature. At the end of orthodontic treatment white
spot lesions might persist as visible damage and can be an aesthetic problem to the patient
because of the chalky, rough opaque appearance of the enamel. Good oral hygiene during
orthodontic treatment is therefore necessary. Different products (such as fluoride and more
recently casein phosphopeptide-amorphous calcium phosphate) are promoted for preventing
and remineralizing WSL.
AIM: The aim of this study was to evaluate the in vitro effects of fluoride, casein
phosphopeptide-amorphous calcium (CPP-ACP) and a combination of both (CPP-ACPF) and
to compare it with a control group on remineralisation of WSL after 6 and 12 weeks.
Materials and Method: 96 premolars were sectioned in two parts (buccal and palatal). WSL
were created with a demineralisation solution during 96h, following a pH-cycling regime
during 3 days. The premolar parts were divided into four groups: a fluoride-group (Elmex
medical gel®), a CPP-ACPF group (Tooth MousseTM), a CPP-ACPF group (Mi Paste PlusTM)
and a control group. Each group of teeth was treated according to the instructions of the
manufacturer (GABA, Lörrach, Germany and GAC Europe, Nieuwegein, the Netherlands).
All teeth were daily brushed with toothpaste (1450 ppm fluoride) except the control group.
Eight different parameters were measured with transverse microradiography after 6 and 12
weeks: the depth of the total lesion (DTL) with the basic mineral content (BMC), the depth of
the body of the lesion (DBL) with the minimum mineral content of the body of the lesion
(MBL) and the depth of the surface layer (DSL) with the maximum mineral content of the

4
surface layer (MSL). The volume of demineralisation (VD) and the amount of body lesions
(NBL) were also measured. Different statistical tests were performed to compare the four
groups after 6 and 12 weeks. The significant level is p<0.05.
Results: The Student’s t-test showed no statistically significant difference between the palatal
and buccal sides for the different measured parameters. The multivariate test, Wilks' Lambda
exact test, showed a strong significant difference (p<0.001) for the experimental groups
between 6 and 12 weeks and no significant difference for the control group (p=0.402). At 6
weeks, only BMC-DTL differed significantly for the mineral content and the lesion depth for
the fluoride group versus the control group (p=0.045) and for CPP-ACP-group versus CPP-
ACPF-group (p=0.041). At 12 weeks, the difference was highly significant (p<0.001) for the
comparison between the three experimental groups and the control group for the different
parameters. BMC-DTL was also statistically significant lower for CPP-ACPF versus the
fluoride group (p=0.025) and the CPP-ACP group (p=0.030). The Friedman test showed no
statistically significant difference for the volume of demineralisation (VD) in the 3
experimental groups between 6 and 12 weeks. The results demonstrated significantly more
remineralisation (lower VD) in the experimental groups than in the control group (p=0.007).
The Pearson Chi-Square test and the Fisher’s exact test showed no significant difference in
NBL after 6 weeks and a highly significant difference after 12 weeks (p< 0.001).
Conclusion: The results of this study revealed no significant differences between the three
different experimental toothpastes in regression of the WSL. Only after 12 weeks, there was a
statistically significant improvement of lesion depths for the three experimental toothpastes
compared with the control group. The lesion depth but also the mineral content of the WSL
decreased significantly after 12 weeks for the experimental toothpastes.

5
Inleiding
Aan de afdeling orthodontie te Gent worden onderzoeken uitgevoerd met betrekking tot de
werking van Casein Phosphopeptide in vergelijking met conventionele tandpasta’s. In een
eerder onderzoek aan onze afdeling onderzocht Veronique Noens het therapeutisch effect van
Casein PhosphoPeptide-Amorphous Calcium Phosphate (CPP-ACP) op ‘white spots’ na een
orthodontische behandeling. Silvia Dauwe spitste zich in een tweede deel toe op het
preventieve aspect van ‘white spots’ tijdens de orthodontische behandeling. In een derde luik
van deze onderzoekslijn wordt het effect van deze tandpasta’s (CPP-ACP en Fluoride) en de
combinatie CPP-ACP/fluoride op ‘white spots laesies’(WSL) in een in-vitro studie verder
onderzocht. In functie van de duurtijd zal de demineralisatie en remineralisatie vergeleken
worden.

6
Study of the literature
The following search terms were used:
- White Spot Lesions (WSL) => “Dental caries” [MeSH], “White Spot Lesions”,
- Casein PhosphoPeptide – Amorphous Calcium Phosphate (CPP-ACP) =>
“caseins”[MeSH], “CPP-ACP”
- Fluoride =>”Fluoride”[MeSH], “Fluor*”,
- Remineralisation => “ Remineralisation”[MeSH], “Reminerali*”
- Demineralisation =>“ Demineralisation”[MeSH], “Deminerali*”
- Microradiography => “Microradiography"[Mesh],”Transverse microradiography”
- Orthodontics=> “Orthodontics” [MeSH], “orthodon*”
The cursive words stand for the combination of the different search terms per term. Different
electronic databases (Medline, Web of science, Cochrane) were used. The search was
restricted to English and Dutch literature only, full texts must been available. If the amount of
selected articles was high, only the articles published in the last 10 years were selected. For
WSL and fluoride only reviews were selected.
Database Search Terms Results Selected
PubMed WSL 49 10
WSL AND Cpp-Acp 98 12
WSL AND Fluoride 871 17
WSL AND Cpp-Acp AND Fluoride 33 /
WSL AND Remineralisation 346 16
WSL AND Demineralisation 420 23
WSL AND Remineralisation AND Demineralisation 147 0
WSL AND Microradiography 86 /
WSL and Orthodontics 415 /

7
CPP-ACP AND Fluoride 221 17
CPP-ACP AND Remineralisation 148 4
CPP-ACP AND Demineralisation 103 1
CPP-ACP AND Remineralisation AND Demineralisation 74 0
CPP-ACP AND Microradiography 10 /
CPP-ACP AND Orthodontics 24 /
Fluoride AND Remineralisation 254 /
Fluoride AND Demineralisation 249 23
Fluoride AND Remineralisation AND Demineralisation 135 /
Fluoride AND Microradiography 183 12
Fluoride AND Orthodontics 310 19
Remineralisation AND Demineralisation 336 /
Remineralisation AND Microradiography 68 1
Remineralisation AND Orthodontics 33 1
Demineralisation AND Microradiography 89 5
Demineralisation AND Orthodontics 136 /
WSL AND Fluoride AND Remineralisation AND Demineralisation 142 12
Web White Spots Lesions 77 7
of CPP-ACP 90 9
Science Fluoride 1148 7
Enamel remineralisation 296 12
Enamel demineralisation 448 10
Transverse microradiography 71 2
WSL AND CPP-ACP 10 2
WSL AND Fluoride 48 8
WSL AND Remineralisation 35 5
WSL AND Demineralisation 61 6
Cochrane White Spots Lesions 3 /
Fluoride 15 3
Remineralisation 4 /
Demineralisation 4 /

8
1. Caries process and white spot lesions
Dental caries is the most prevalent human disease of bacterial origin. It is a major public
health problem for both children and adults. The involvement of microorganisms has been
recognized since the late 1800s. Nowadays, modern management of dental caries is based on
appropriate detection of the disease, diagnosis of pathological changes (including lesion
formation in its earliest stages), prevention, control and treatment (3).
The caries process is initiated by the demineralisation of tooth hard tissue by organic acids.
Dental plaque bacteria like Mutans Streptococci (MS) and Lactobacillus can fermentate
dietary sugar and produce organic acids (4). Granulicatella, Veilloellaceae, Bifidobacteriacea
and Wiggsiae were also associated with the presence of WSL in adolescents undergoing
orthodontic treatment (5). The acids decrease the pH in the biofilm and causing the
dissolution of the calcium phosphate mineral in the tooth enamel or dentin. This leads to
dissolution of the hard tissue (2). At different stages in the caries process, different
combinations of bacteria may interact to produce the overall effect of a plaque with lowered
pH (6). This demineralisation, a dynamic process, is reversible in early stages. The calcium,
phosphate and fluoride in the saliva restore the crystalline structure of the tooth. This process,
known as remineralisation, neutralizes the acids and reverses the diffusion gradient for
calcium and phosphate (2, 7). In a remineralisation process, the pH increases. An imbalance
between demineralisation and remineralisation of dental hard tissues can result in dental
caries. The caries balance is shown in figure 1. A diminution of the salivary flow decreases
the resistance to white spot formation (8).

The use of fixed appliances provides a rough surface that makes tooth cleaning more difficult.
This accelerates the rate of plaque accumulation and plaque maturation. The presence of the
carbohydrates in the plaque in combination with the plaque associated bacter
and the demineralisation starts.
correlation between plaque accumulation and development of carious lesions. The
the local environment by placing an orthodontic
acid uric bacteria. Mutans streptococci
treatment. After the removal of fixed appliances,
significantly to levels comparable with age
phase (5). The reduction in bacterial counts was more pronounced for lactobacilli, which may
indicate that MS levels need mo
these plaque bacteria is shifted during orthodontic treatment
amount of subgingival P. gingivalis remained high for 6 months after appliance removal. This
finding might imply a potential risk to periodontal health in certain patients
Enamel crystal dissolution starts
enamel rods. The early clinical sign of an e
termed white spot lesions because of the resultant
causing scattering of light and giving the enamel a chalky, rough opaque appearance
14).
Figure 1: The caries balance: a diagram of the balance between pathological and protective factors in the caries process, a balance that alternates either way several times a day in most people (2).
of fixed appliances provides a rough surface that makes tooth cleaning more difficult.
This accelerates the rate of plaque accumulation and plaque maturation. The presence of the
in the plaque in combination with the plaque associated bacter
ation starts. According to Zachrisson & Zachrisson (
correlation between plaque accumulation and development of carious lesions. The
by placing an orthodontic appliance appear to favour
streptococci can increase up to fivefold during orthodontic
After the removal of fixed appliances, microbial levels were found to decrease
significantly to levels comparable with age-matched controls, 6 to 15 weeks into retention
he reduction in bacterial counts was more pronounced for lactobacilli, which may
indicate that MS levels need more time to return to normal, or that natural balance between
these plaque bacteria is shifted during orthodontic treatment (10). According to Liu, the
amount of subgingival P. gingivalis remained high for 6 months after appliance removal. This
finding might imply a potential risk to periodontal health in certain patients
starts with subsurface demineralisation, creating pores between th
The early clinical sign of an enamel mineral loss is a white spot lesion. I
because of the resultant change in the refractive index of the enamel,
causing scattering of light and giving the enamel a chalky, rough opaque appearance
The caries balance: a diagram of the balance between pathological and protective factors in the caries process, a balance that alternates either way several times a day in most
9
of fixed appliances provides a rough surface that makes tooth cleaning more difficult.
This accelerates the rate of plaque accumulation and plaque maturation. The presence of the
in the plaque in combination with the plaque associated bacteria lowers the pH
(9) there is a linear
correlation between plaque accumulation and development of carious lesions. The changes in
favour colonization of
can increase up to fivefold during orthodontic
microbial levels were found to decrease
o 15 weeks into retention
he reduction in bacterial counts was more pronounced for lactobacilli, which may
re time to return to normal, or that natural balance between
According to Liu, the
amount of subgingival P. gingivalis remained high for 6 months after appliance removal. This
finding might imply a potential risk to periodontal health in certain patients (11, 12).
ation, creating pores between the
a white spot lesion. It is
in the refractive index of the enamel,
causing scattering of light and giving the enamel a chalky, rough opaque appearance (8, 13,
The caries balance: a diagram of the balance between pathological and protective factors in the caries process, a balance that alternates either way several times a day in most

10
This change in the refractive index of the enamel surface and subsurface are due to the
changes in physical and chemical properties, the spatial configuration of the crystals and the
presence of water (12, 15). When the demineralisation process progress, the full thickness of
the enamel and some of the dentine demineralize before the relatively hypermineralized
surface layer is actually lost (8, 14). WSL, a visual damage, may detract from the beneficial
effect of orthodontic treatment.
There seems to be a difference in progression between traditional caries formation and white
spots lesions. The latter has a rather superficial (75µm) and ‘speedy’ character and can
become apparent within 4 weeks after placement of fixed appliance, which is the average time
between two orthodontic visits (14, 16, 17). The formation of a normal caries lesion is usually
a slower process, which takes at least 6 months (18). The shape of the white-spot lesion is
determined by the distribution of the biofilm and the direction of the enamel prisms. This
emphasizes that the lesion is driven by, and reflects, the specific environmental conditions in
the overlying biofilm (19).
a) Prevalence of white spots
The prevalence of dental caries has drastically decreased the last decades but is far from being
eliminated (20-22). The age group (11-14 years) in which orthodontic treatment is usually
carried out is considered to be at greatest risk of developing caries (23). In 2011, Al Maaitah
et al reported the overall incidence of WSL reported from 2% to 97% (24). According to
Behnan et al, the incidence of WSL during orthodontic treatment with fixed appliances is 73%
to 95% (25). This large variation of prevalence-data could be attributed to the variety of
clinical investigations, registration and the difficulty in standardizing clinical examinations.

11
The increased prevalence of WSL in orthodontic patients can be attributed to the following
factors:
- Fixed orthodontic appliances form a niche for bacterial plaque to inhabit, complicating
a proper oral hygiene practice. Patients with inadequate oral hygiene tend to develop
more WSL affecting more teeth, during orthodontic treatment.
- The newly erupted teeth, seen in typical orthodontic patients, might also be more
susceptible to acid attack (13).
- The fixed appliance makes conventional oral hygiene for plaque removal more
difficult, and increases gingival inflammation. The clearance of plaque by saliva or the
movement of oral musculatures adjacent to the brackets is also reduced.
- Younger patients tend to develop WSL during orthodontic treatment more often than
adult patients.
- Patients with at least 1 decayed, missing due to caries or filled first permanent molar
before orthodontic treatment might develop more WSL after orthodontic treatment
than patients who have 4 healthy first permanent molars.
No significant association between severity of WSL and patient’s age, socio-economic status,
compliance with attendance, treatment duration or treatment type was found. Except that once
WSL have developed in male patients, the lesions have a greater degree of demineralisation
after orthodontic treatment than in female patients (24).
On average, in males 40% and in females 22% of surfaces showed white spots (10).
Zachrisson and Zachrisson (26) reported that higher caries index, recorded for male
orthodontic patients, was a result of a lower standard of oral hygiene (with higher scores for
plaque and gingival index) in male patients as compared to female patients.

12
After orthodontics, the enamel lesions have been reported to develop most frequently on the
cervical and middle third of the buccal surfaces. In the literature, different distribution of
affected teeth is mentioned. Most frequently, lateral maxillary incisors, mandibular canines
and first premolars are affected with enamel lesions, followed by maxillary central incisors
and first molars in the upper and/or the lower arch or both arches. (23, 27, 28). A significant
difference in the number of lesions was found between incisors and canines on the one hand
and molars and premolars on the other hand, indicating more lesions in the molar-premolar
region (10). When the appearance of white spots was evaluated in overall manner, there was
significantly more upper than lower decalcification (29).
The lingual surfaces are less prone to caries in comparison to the buccal surfaces (30). This
may be explained by differences in surface morphology, plaque retention, salivary flow and
mechanical cleaning of surfaces by the tongue. WSL development on buccal surfaces is 4.8
times higher than the number of new WSL developing or progressing on bracketed lingual
surfaces. The caries extent was 10.6 higher for buccal surfaces (31).
b) Prevention of white spot lesions
Many studies have been performed to find the solution to prevent caries lesions during
orthodontic treatment with fixed appliances. Oral hygiene is the most important factor. The
patient’s cooperation can be improved by repeatedly verbally praising and re-education (32).
The orthodontist prevents WSL also by starting fixed appliance treatment only in plaque-free
patients, providing a strict oral hygiene protocol during treatment, placement of the
orthodontic appliance on a less plaque-retentive way and discontinuing orthodontic treatment
as soon as incipient WSL become visible.

13
Patients, parents, orthodontists and general dentists indicate that patients are the most
responsible for the prevention of WSL. Most patients and parents are aware that WSL were
caused by inadequate or improper brushing and flossing during orthodontic treatment (33).
To obtain a good oral hygiene and to prevent WSL, there are several products like fluoride,
CPP-ACP and chlorhexidine to use. Underneath, a short explanation of the different products.
In the following chapters, the mechanism of actions of fluoride and CPP-ACP is explained.
Fluoride
The standard actions used in an orthodontic practice to prevent demineralisation are brushing
with fluoride (1000ppm) toothpaste twice daily (32, 34) combined with 0.05% sodium
fluoride mouth rinse and nutritional counselling (35-37). 0.2 % Sodium fluoride mouth rinse
helps to reduce the severity of enamel decay adjacent to fixed braces, and also inhibits lesion
development by about 60%. Unfortunately the trustworthiness of any home medication
treatment can’t be controlled. Only 42% of patients rinsed with a sodium fluoride mouth rinse
at least every other day (38).
Fluoride administration is possible in various ways and there is a great variability of products
on the market. Many fluoridated materials release large amounts of fluoride initially, but the
level drops rapidly and might not be sufficient to prevent decay over the whole course of
orthodontic treatment. Long duration and low-dose fluoride release appears to increase the
caries-resistant fluorapatite concentration in enamel and to reduce demineralisation during
orthodontic treatment (39). Evidence suggests that the use of extra fluorides during fixed
appliance treatment reduces the occurrence and severity of white spot lesions (16, 40, 41).

14
There are 2 different ways to apply fluoride: a topical way and an adhesive way.
Topical way (toothpaste, mouth rinse, gel, varnish):
- Fluoride varnish during orthodontic treatment resulted in 50% less enamel
demineralisation according to Todd et al., 48% according to Øgaard et al and 44, 3%
less demineralisation according to Vivaldi-Rodrigues et al. (11, 42, 43). Following Du
et al., varnish application should be advocated as a routine caries prevention measure
after orthodontic treatment (6).
- Topical fluoride pastes provide a protective coat which decreases enamel solubility
and an increase of fluoride uptake in enamel (32). After debonding, application of
topical fluoride on WSL remineralizes these lesions (44-46). On the contrary, topical
application of acidulated phosphate fluoride gel immediately after debonding appears
to be of little benefit in reducing the incidence of white spots (36).
- Titanium tetrafluoride (TiF4) is more effective in preventing WSL than other fluoride
agents (47). The mode of action of TiF4 is due to the formation of an acid-resistant
surface layer. This layer provides mechanical protection to the surface, and increases
the fluoride uptake, which might chemically reduce demineralisation of dental hard
tissues. Clinical trials analysing the effect of TiF4 are lacking so the potential of TiF4
to prevent acid demineralisation requires further research to confirm the promising in
vitro results obtained (48).

15
Adhesive way: fluoride releasing cements, elastomeric modules, glass ionomer, etc...
- Elastomeric or modules are used in orthodontics to hold the arch wire in the bracket
slots. Instead of conventional elastomers, there are also fluoride-releasing elastomers.
The overall reduction in score per tooth produced by the fluoride-releasing
elastomerics was 49%. A significant difference was seen in all but the occlusal enamel
zones. Fluoride-releasing elastomers have been shown to reduce significantly the
salivary levels of Mutans Streptococcus MS. However clinically, these elastomers
showed a more rapid deterioration with swelling and apparent loss of elastic properties
2-3 weeks after insertion. Apparently, these modules are less elastic, rendering figure-
of-eight ligating impossible and not available in different colours. The magnitude of
fluoride released by these modules was considerably higher than that reported for
fluoride-releasing chain (49).
- Fluoride-releasing orthodontic bonding adhesives have been available for several
years but long-term clinical trials have shown them to be ineffective in preventing
enamel damage (28, 29). The bond strength is also too weak so it is clinically not
successful for routinely bonding of brackets (29). These composites generally release
fluoride over a short time span, which is insufficient to provide protection throughout
a 2-year treatment period.
- Glass ionomer cements have been suggested as alternative bracket bonding materials.
The cements provides greater fluoride release, but their bond strengths are considered
inadequate for clinical use (49). According to Gjorgievska et al., conventional glass
ionomer has the greatest effect of caries inhibiting and shows the highest level of ion
migration (50).
- Enamel sealants/Resin sealers: An in vitro study found that Pro-seal TM® can resist
acid challenges and toothbrush abrasion in a laboratory environment. In a second in
vitro study, it was found that Pro-Seal TM® (a fluoride containing sealant) provided
significantly more protection than either fluoride varnish or an unfilled resin sealer
with 92% reduction in lesion depth compared with the controls (25).

16
Casein phosphopeptide – Amorphous calcium phosphate
Casein phosphopeptide – Amorphous calcium phosphate (CPP-ACP) would slow down the
demineralisation process and enhance the remineralisation. CPP-ACP can be incorporated
into various products (methacrylate composites, sugar-free gum, mints, topical gels, pastes,
sport drinks, glass ionomer cements) in order to exert a topical effect (51-53).
The daily topical exposure to CPP-ACP in CPP-ACP containing sugar-free chewing gum and
mint in-situ increase enamel remineralisation of artificially demineralized subsurface enamel
lesions, with an increase in enamel mineralisation of 78 to 176% (51-53). In addition, the
consumption of chewing gum and mints results in an increased production of stimulated
saliva (32). Sudjalim et al. recommended the combination of CPP-ACP with fluoride varnish
to enhance the treatment effect (54). The use of CPP-ACP in orthodontic practice has been
proposed for white spots prevention and caries prophylaxis even before bracket placing
procedures (9).
Chlorhexidine
Chlorhexidine applications, such as the chlorhexidine-thymol varnish (Cervitec, Vivadent)
used in conjunction with a fluoride varnish might help to lower the level of Mutans
Streptococci (55). Chlorhexidine inhibits acid production in plaque and thus reduces the pH
decrease during sucrose challenges (56). But the use of antimicrobials, such as chlorhexidine
against the temporary elevations in salivary MS levels may not be warranted in all orthodontic
patients (32). An adverse effect includes a bitter taste and discoloration of the teeth and
tongue (57).

17
Others
Argon lasers are also suggested in this context but there are very few data about this subject
(2, 32).
Excessive surplus orthodontic etching of the complete labial enamel surface, instead of the
bracket bases only, must be avoided to prevent iatrogenic white spot lesions. Etching times
not exceeding 15 seconds are favourable (58).
c) Treatment of white spot lesions
Despite preventive measurements, some patients have unsightly WSL after debonding
presenting a challenge for restorative treatment. While de-bonding eliminates a major
etiological factor, remineralisation of white-spot lesions is not guaranteed. During the first 6
months after de-bonding, the greatest change of the white spot can occur (59). A significant
clinical improvement of about 80% was seen of the sites after 6 months, only 40% became totally
invisible, 22% remained as an aesthetic problem (60-62).
The remineralisation of WSL can be attributed to a reduction of the cariogenic challenge. By
removal of the accumulated plaque and cariogenic microorganisms around the appliances, the
cariogenic challenge is substantially reduced. Other factors of importance in this respect could
be reduced clearance time for cariogenic food items and also more efficient tooth brushing
(63). According to Artun and Thylstrup, the result of surface abrasion with some
predisposition of minerals is to be held responsible for the loss of porous tissue and the
gradual regression of the WSL after debonding (27).
Highly concentrated fluoride solutions hypermineralize the surface of the lesion, leaving them
more resistant to acid attacks and decrease body remineralisation. Unfortunately, since these

18
solutions do not penetrate inside the lesion, they do not eliminate its opaque whitish aspect
which is less aesthetic (64). Low doses of fluoride in mouth rinses do not improve the lesions
either (61).
Allowing remineralisation by saliva and, if necessary, the use of acid microabrasion 10 weeks
after debonding is suggested by Welbury and Carter (62). The hydrochloric acid-pumice
micro-abrasion technique offers a method for improving the appearance of these lesions.
The potential of CPP-ACP to promote lesion remineralisation has been demonstrated (52, 53,
66, 67). According to Bailey et al., there is 31% more regression at 12 weeks for WSL code 2
and 3 (68). In the presence of fluoride, CPP-ACP has been shown to promote the formation of
fluorapatite deep in the subsurface lesion (69). Hence, this ability to promote remineralisation
of enamel subsurface lesions in situ explains the significant regression of WSL by CPP-ACP
in this post-orthodontic population using fluoride toothpaste and receiving supervised fluoride
mouthrinses.
The aesthetic result of bleaching spot- or stripe-shaped local opacities is rather limited
according to Glockner (70). In contrast to Knosel’s study where patients were satisfied with
the outcome (71). The susceptibility to the formation of caries-like lesions after bleaching
increases. Therefore perfect oral health and hygiene is needed. Wiegand et al. suggested
fluoridation after the bleaching therapy to enhance remineralisation of bleached teeth (72).
Featherstone demonstrated that specific pulsed carbon dioxide, or CO2 laser treatment of
dental enamel can inhibit subsequent caries like progression in a severe demineralisation-
remineralisation model in the laboratory by up to 85 per cent (2). CO2 and diode laser
irradiation of the enamel surface can both increase fluoride uptake; however, laser energy
parameters must be carefully controlled in order to limit increases in pulpal temperature and
alterations to the enamel surface (73, 74).

19
2. Anticariogenetic properties of CPP-ACP (GC Tooth MousseTM)
Solutions containing calcium and phosphate ions have limited effect on remineralisation, due
to the low solubility of calcium and phosphate salts. The multiple phosphoferyl residues of
the CPP bind to nanoclusters of ACP in supersaturated solutions, thereby preventing growth
to the critical size required for phase transformations (75). The CPP molecules contain a
cluster of phosphoseryl residues which markedly increase the apparent solubility of calcium
phosphate by stabilizing amorphous calcium phosphate (ACP) under neutral and alkaline
conditions. CPP-ACP can promote the formation of fluorapatite deep in the subsurface lesion
(69).
The proposed anticariogenic mechanism of CPP-ACP involves the incorporation of the nano-
complexes into dental plaque and onto the tooth surface, thereby acting as a calcium and
phosphate reservoir (68). This mechanism is ideal for the prevention of enamel
demineralisation as there appears to be an inverse association between plaque calcium and
phosphate levels and measured caries experience. The localized CPP-ACP nanocomplexes act
to buffer free calcium and phosphate ions in the plaque fluid, in order to maintain a state of
supersaturation of ACP with respect to enamel mineral, thereby limiting enamel
demineralisation and enhancing remineralisation (53, 76).
CPP-ACP can be incorporated into supragingival dental plaque by binding to the surfaces of
bacterial cells, to components of the intercellular plaque matrix and to adsorbed
macromolecules on the tooth surface. All these interactions may then lead to the formation of
a less cariogenic plaque (75). Enamel lesions which have been remineralized with topical
exposure to CPP-ACP have been shown to be more resistant to subsequent acid challenge
compared with normal remineralized enamel as CPP-ACP is able to promote the
remineralisation of enamel subsurface lesions with hydroxyapatite.

20
In addition, the relatively low carbonate environment of the CPP-ACP treated subsurface
lesion may also exhibit both improved crystallinity and lower microstrain than might be found
in normal tooth enamel (32, 77)
CPP stabilize calcium, phosphate and hydroxide (fluoride) ions preventing spontaneous
precipitation of hydroxyapatite (fluorapatite). The CPP stabilized calcium, phosphate and
hydroxide (fluoride) ions substantially promote remineralisation of enamel subsurface lesions
and therefore have the potential as a superior form of fluoride for the prevention and
remineralisation of incipient carious lesions and for the remineralisation of hypomineralized
enamel lesions generally.
3. Mechanism of action of fluoride (Elmex Medical Gel®)
Why caries prevalence reduced during the last 20 years is difficult to say. Strong evidence
exists, however, that the near universal use of fluoride containing products such as toothpaste,
mouthrinses and topical gels (used at home or applied in the dental office by the dentist) have
been major contributors. Earlier reductions of caries has resulted from the fluoridation of
public water supplies in many communities (2). Fluoride has three principal topical
mechanisms of action:
Inhibiting bacterial metabolism.
The bacteria in the plaque produce acids and decrease the pH. A portion of the fluoride
present in the plaque fluid combines with hydrogen ions to form hydrogen fluoride (HF). The
HF molecules diffuse rapidly into the cell. The HF molecules dissociates in the cell which
makes the inner cell more acid and release fluoride ions, that interfere with the enzymatic
activity of the bacteria (2).

21
Inhibiting demineralisation
Different forms of apatite are present. The carbonated hydroxyapatite, or CAP, of our teeth is
more soluble in acid than hydroxyapatite, or HAP (HAP = Ca10 (PO4)6(OH)2. Fluorapatite, or
FAP (unit cell stoichiometry of Ca10 (PO4)6F2) in which the OH- ion in pure hydroxyapatite is
completely replaced by an F– ion, is even more resistant to dissolution in an acid environment,
so fluoride inhibit demineralisation. If fluoride is present in the aqueous solution surrounding
the crystals, it absorbs strongly to the surface of the CAP and acts as a potent protection
mechanism against dissolution of the CAP of the enamel of the tooth. When the bacteria
generate acids, the fluoride present in the plaque fluid, travel with the acid into the subsurface
of the tooth and adsorb to the crystal surface and protect it. When the fluoride is concentrated
into a new crystal by remineralisation, it modifies the crystal resistance to dissolution.
Fluoride incorporated into the tooth during tooth development is insufficient to play an
important role in the caries protection. So it is important to have a high level of fluoride
surrounding CAP crystals to inhibit the demineralisation by an acid attack of bacteria (2).
Fluoride concentrations as found in dental plaque have biological activity on critical virulence
factors of Mutans Streptococci in vitro, such as acid production and glucan synthesis (78).
Enhancing remineralisation
When fluoride is adsorbed to the crystal surface, it attracts calcium ions, followed by
phosphate ions leading to new mineral formation. The new formed crystal structure is
composed of HAP and FAP. CAP is no longer present in the crystal. Since the solubility of
HAP and FAP is much lower than that of CAP, the newly formed crystal is less soluble in an
acid environment. The critical pH for hydroxyapatite (the pH at which it starts to dissolve and
hence it lost) is 5.5, however between pH 4.5 and 5.5 saliva and plaque fluids are still
supersaturated with regard to fluorapatite and will tend to precipitate and preventing the loss

22
of mineral ions. pH levels lower than 4.5 have been measured in the plaque around the
brackets and the bands. Several methods have been suggested to improve the cariostatic effect
of fluoride at low pH. Acid-resistant coatings of calcium fluoride or titanium fluoride on the
enamel surface and the use of fluoride in combination with anti-microbial have been
suggested (43).
A problem with fluoride ions is that, in the presence of salivary calcium and phosphates ions,
a rapid deposition of these ions occurs in the surface layer of the enamel lesion. This
deposition in the surface layer then blocks further ion penetration into the body of the carious
lesion thus limiting deeper remineralisation (7). Two mol fluoride ions are required for every
10 mol of calcium and 6 mol of phosphate ions to remineralize enamel subsurface lesions
with fluorapatite.
Figure 2: Schematic representation of demineralisation followed by remineralisation in the caries process. If remineralisation is successful, the final result is a crystal with a surface layer of "fluorapatitelike" mineral of low solubility. (Reproduced from Featherstone (1) with permission of the publisher. Copyright ©1999, Munksgaard.)

23
Hence for many applications of topical fluorides the level of calcium and phosphate ions is
the limiting factor for remineralisation (69, 79).
Elmex medical gel® contains the amine fluorides: olaflur and dectaflur. Amine fluorides
(NaF) act like surfactants, reducing the surface tension of saliva, and forming a homogeneous
film on all oral surfaces. This is due to their molecular structure: the fluoride ion is bound to
an organic fatty acid amine fragment. Amine fluorides cover the tooth surfaces with a
homogenous molecular layer. This continuous film prevents rapid rinsing off by the saliva
and thus active for a longer period (80).
4. Interaction of CPP-ACP and fluoride (MI Paste PlusTM)
Recently, fluoride has been incorporated into the CPP-ACP complex (CPP-ACPF) and was
shown to promote remineralisation; the deposited mineral is with fluorapatite. The level of
remineralisation (up to 57%) was able to return translucency of the treated enamel to that of
sound enamel. The use of CPP-ACP with fluoride and its synergistic effect on enamel
remineralisation have been attributed to the formation of CPP-stabilized amorphous calcium
fluoride phosphate resulting in the increased concentrations of bioavailable calcium and
phosphate ions. (69, 79)

24
5. Quantifying enamel demineralisation
White spot lesions are not detectable visually until they progressed 200-300µm into the
enamel (81). A reliable and reproducible detection of dental caries by clinical examination has
been recognized as a problem for decades. Variable approaches has been taken to recognize
WSL (82).
There are invasive and non-invasive diagnostic methods. In this in-vitro study we choose the
micro-radiography, which is considered as the ‘‘gold standard’’.
Non-invasive diagnostic methods:
A non-invasive diagnostic method, such as visual detection and observation of fluorescence,
preservers the tooth in its entirety. It can be used in vivo.
Visual detection
The most evident method is based on a visual detection of the labial surfaces of the teeth, but
it cannot help detecting caries in very early stage. There are different indices for scoring the
amount of decalcification like for example the white spot lesion index from Gorelick (table 1),
from Andersson (table 2) or the white spot lesion index from Banks and Richmond (table 3)
(8, 49, 60). According to Torlakovic et al., WSL’s colour intensity might predict the depth of
enamel demineralisation as well as traditional WSL scoring (7).
An indirect way of visual inspection is by computerized image analysis of digital photographs.
This is a more reliable and reproductive way than direct visual detection (83).

25
Score Definition
1 No white spots
2 Thin white border: With a guideline of <33% of the vestibular surface
3 Thick white border. With a guideline between 33 and 66% of the vestibular surface
4 White spot and cavitation or covering more than 66% of the vestibular surface
TABLE 1 The white spot lesion index from Gorelick (8).
Score Definition
0 No visible colour change
1 Slight white colour change, only visible after air drying
2 Slight colour change with certain marked white areas
3 White consistent colour change
4 Distinct white colour change
TABLE 2 The white spot lesion index from Andersson (60).
Score Definition
0 No decalcification
1 Decalcification covering <50% of the gingival/ mesial/ distal/ occlusal zone
2 Decalcification covering >50% of the gingival/ mesial/ distal/ occlusal zone
3 Decalcification covering 100% of the gingival/ mesial/ distal/ occlusal zone or severe
decalcification with cavitations
TABLE 3 The white spot lesion index from Banks and Richmond (49).

26
Observation of fluorescence
Fluorescence makes it possible to detect caries in an initial stage. The QLF (Quantitative
Light induced Fluorescence) is an optical, visible light-based system that can be used to detect
and quantify early demineralisation of enamel. The clinical use of QLF is limited by several
confounding factors in caries-risk adolescents but seems to be a sensitive method that is
suitable for the detection of visually undetected initial caries lesions (10, 84).
Organic (bacterial by-products) and inorganic materials present on the tooth surface absorb
the red laser light (wave length of 655 nm) and emit this light as near-infrared fluorescent
light. Changes in the tooth substance associated with the amount of bacterial by-products are
reflected as an increase in the re-emitted fluorescent light and thus the difference between
sound and decayed areas is recognized by the PLM (Polarized Light Microscope, Kavo
DIAGNOdent). The amount of fluorescence relates more closely to bacterial presence than to
the mineral content of the tooth (63, 85).
Other detection methods with fluorescence is possible with a Vistaproof, Dye-Enhanced laser
fluorescence or DELF, optical coherence tomography or OCT, fiberoptic transillumination,
Electronic caries monitor or ECM, a colorimeter, etc (3, 21, 86, 87).
Invasive diagnostic methods:
To quantify a demineralisation by the invasive way, the teeth need to be extracted. For in-
vitro and microscopic investigation, slices are needed.

27
Microscopes
Transverse microradiography (TMR) is a standardized method in studies on
de/remineralisation of teeth for decades and considered as the ‘‘gold standard’’ for the
determination of mineral loss or gain in experimentally induced incipient carious lesions. This
method has been used for the comparison and validation of other newly developed caries
detection techniques. The TMR provides a very precise quantitative measurement of the
mineral content (88). A representative microradiography image of sectioned enamel is
represented on figure 3. The body of the lesion with the remineralisation is clearly visible.
The scanning electron microscopy SEM can be used to observe the surface morphology (89).
The transmission electron microscopy or TEM, Atomic Force Microscopy, Confocal laser-
scanning microscope and X-ray scanning analytical microscope are alternative microscopes
(90).
Figure 3: Representative microradiography images of sectioned enamel specimens. The body of the lesion with the remineralisation is clearly visible.

28
Others
Micro-CT, a 3-D tool, is also able to detect artificial caries lesions after remineralisation and
may be used to substitute TMR and PLM in in-vitro studies of caries (88). However, micro-
CT is less precise than microradiography.
Cross sectional hardness or CSH: is not very accurate for estimating the mineral content, but
it gives some information regarding the mechanical (physical strength) properties of the
lesions, which are not provided by TMR; therefore, it should be advised to combine different
methods to analyse enamel demineralisation, in order to get more information about the
properties of the lesions (91).
The nano indentation (92), the electron probe micro-analyser (93) and superficial
microhardness (SMH) can also be used for quantifying WSL.

29
Aim of this study
The aim of this study was to compare the in vitro effects of fluoride, casein phosphopeptide-
amorphous calcium phosphate (CPP-ACP) and CPP-ACPF products on remineralisation of
white spots after 6 and 12 weeks, and to compare them with a control group.
The null hypothesis to be tested was that there is no statistically significant difference in
remineralisation between the fluoride, the CPP-ACP and the CPP-ACPF products on white
spot lesions after 6 and 12 weeks.

30
Methodology
Preparation of enamel blocks
96 premolars (24 patients with 4 premolars) were collected from various dental practices
(informed consent was obtained nr B 670 2010 10019). The teeth were washed in tap-water
and stored in 0.1% thymol solution at 4° C. Premolars with a healthy enamel surface were
selected and included in the study. Teeth with dental caries, fluorosis and other
hypermineralized lesions, pitting or cracks, hypoplastic areas, large irregularities of enamel
structure were excluded. An enamel surface layer was removed to avoid a potentially fluoride
rich layer and the individual enamel differences as shown in figure 4 (13). The premolars
were sectioned in two parts: a buccal side and a palatal side. In order to divide the tooth, a
diamond saw, water-cooled, cutting machine was used. To avoid interference of general tissue
demineralisation of the crown, the entire part was covered by acid-resistant nail varnish
except the area of interest.
Figure 4: An enamel surface layer was removed to avoid a potentially fluoride rich layer and the individual enamel difference.

31
Artificial white spot lesions
White spot lesions were created in this area with the demineralisation solution of Ten Cate
and Duijsters (2.2 mM CaCl2.2H2O + 2.2 mM NaH2PO4 + 50 mM CH3COOH (94). pH was
adjusted to pH 4.4 using 1M KOH) during 96 h to have a lesion depth of 150-200 µm deep on
every half premolar (95). This method produces a subsurface enamel demineralisation without
surface erosion.
pH-cycling regime
Ten Cate and Duijsters introduced a dynamic model concept with alternating periods of de-
and remineralisation (94). The pH-cycling protocol simulates in vivo high caries risk
condition and simultaneously measures the net result of the inhibition of demineralisation and
the enhancement of remineralisation. This solution approximates the mineral ion composition
and supersaturation of saliva as originally reported by ten Cate and Duijsters (78, 94). The re-
and demineralisation solutions in the pH-cycling regime were renewed every day.
- Demineralisation stage (20ml/sample, during 6h/day at 37°C) used an acid buffer
containing demineralized H2O with 2mM Ca(Ca(NO3)2), 2 mM PO4 (KH2PO4) and 75 mM
acetate. pH was adjusted to 4.3 using 1M KOH.
- Remineralisation solution (20ml/sample, during 17h/day at 37°C) contained calcium
and phosphate at a known degree of saturation (1.5mM Ca and 0.9mM PO4) to mimic the
remineralizing properties of saliva. This solution contained demineralized H2O with 130-150
mM KCL (to provide background ionic strength) 100 mM TRIS, 1.5 mM Ca(NO3)2. 4H2O,
0.2 mM KH2PO4, and 140mM KCL. pH was adjusted to 7 using 1M HCL.

32
All 192 parts underwent 3 days the pH-cycling regime without the fluoride dentifrices
treatment to allow baseline values of calcium uptake and loss to be determined. After these 3
days brushing of the teeth was started.
Study design
The premolar parts were divided in four groups: a fluoride group (Elmex medical gel®,
GABA Benelux), a CPP-ACP group (Tooth MousseTM, GC Europe), a CPP-ACPF (Mi Paste
PlusTM, GC Europe) and a control group. The three active groups were brushed with toothpaste
(1450 ppm fluoride); the control group just underwent the pH-cycling regime. Table 4
represents the different test products, their application and their content.
Table 4: Ingredients and concentration range of tested agents, according to manufacturers’ specification.
Test products Application Content
Elmex Medical Gel® GABA, Lörrach, Germany
Gel 1x / week 3 minutes
Water, Amine fluoride (Olaflur and Dectaflur) Sodium fluoride Propylene glycol, Hydroxyethyl cellulose Fluoride content: 12,500 ppm
Gc Tooth MousseTM GAC Europe, Nieuwegein, the Netherlands
Gel Daily 3 minutes
Water CPP-ACP glycerol, D-sorbitol, CMC-Na, propylene glycol, silicon dioxide, titanium dioxide, xylitol, phosphoric acid, flavoring, zinc oxide, sodium saccharin, ethyl p-hydroxybenzoate, magnesium oxide, guar gum, propyl p-hydroxybenzoate, butyl p-hydroxybenzoate
Mi Paste PlusTM GAC Europe, Nieuwegein, the Netherlands
Gel Daily 3 minutes
CPP-ACP Sodium Fluoride (900 ppm) water, glycerol, d-sorbitol, CMC-Na, propylene glycol, silicon dioxide, titanium dioxide, xylitol, phosphoric acid, flavoring, sodium saccharin, ethyl p-hydroxybenzoate, propyl p-hydroxybenzoate, butyl p-hydroxybenzoate

33
Fluoride group (Elmex medical gel®): The premolar parts were brushed with conventional
toothpaste (1450 ppm fluoride) every day. Once a week, after brushing with conventional
toothpaste, Elmex medical gel® was applied during 180 seconds and rinsed before putting it
back in the pH-cycling regime. These were the instructions of the manufacturer.
CPP-ACP group (GC Tooth MousseTM): Every day after brushing with conventional
toothpaste (1450 ppm fluoride) the GC Tooth MousseTM was applied during 3 minutes.
Afterwards the teeth were placed in the remineralisation solution.
CPP-ACPF group (Mi Paste PlusTM): Every day after brushing with conventional toothpaste
(1450 ppm fluoride) the Mi Paste PlusTM was applied during 3 minutes. Afterwards the teeth
were placed in the remineralisation solution.
Control group: Control group without fluoride or CPP-ACP, underwent the pH-cycling
regime.
Microradiography
Changes in the mineral content and the lesion depths of the experimental caries lesions were
measured using transverse microradiography (TMR). At least three different enamel sections
were cut across the lesion window. These sections were x-rayed with an aluminium step-
wedge at 20kV and 15mA for 6 minutes (PW1830, Philips, Eindhoven, the Netherlands).
WSL exhibiting an intact surface zone were included. A second examiner evaluated the
photos. The average of three measurements per WSL was obtained for the different
parameters.

34
The lesion characteristics as defined by Theuns were the different parameters, evaluated in
this study (1). The mineral content in the lesion (volume fraction of the mineral) was plotted
against the depth.
- DTL = total depth of the lesion, defined as the depth at which no further increase in
mineral content was observed (µm)
- DBL = depth of the MBL point = depth of the body of the lesion (µm)
- DSL = depth of the MSL point = depth of the surface layer (µm)
- MSL= maximum mineral content of the surface layer (%)
- MBL= minimum mineral content of the body of the lesion (%)
- BMC= the basic mineral content (%)
- VD = volume of demineralisation (as shown in figure 5B) (µm %)
- NBL= the number of body lesions
The mineral contents were calculated with the standard use of 85% apatite.
Figure 5: Schematic drawing of the microradiography procedure. A Lesion characteristics as defined by Theuns: the maximum mineral content of the surface layer (MSL) and the point at which this maximum is reached (DSL), the minimum mineral content of the lesion body (MBL) and the point at which this minimum is reached (DBL) and the depth of the lesion (DTL). B Schematic drawing of the area representing the dissolved mineral (shaded part) (1).

35
Statistics
Descriptive statistics to calculate the range, mean, median and standard deviation.
A Student’s t-test was used to compare the palatal and the buccal side for the different
parameters (DBL, DSL, DBL, MSL, MBL, BMC and VD).
The Mann–Whitney U test, a non-parametric test, was used to compare the volume of
demineralisation between 6 and 12 weeks in the 4 groups.
The MANOVA, multivariate analysis of variance, compared the multivariate means (DSL-
MSL, DBL-MBL, and DTL-BMC) between the four groups at the different time periods and
between the 6 and 12 weeks.
The Friedman test, a non-parametric statistical test, was used to compare the volume of
demineralisation for the three experimental groups mutually.
The Wilcoxon signed-rank test, a non-parametric statistical hypothesis test, was used to
compare the volume of demineralisation between two related samples.
A Pearson Chi-Square test and a Fisher’s exact test were used to compare the amount of body
lesions between the groups mutually and between 6 and 12 weeks. .
The Intraclass Correlation Coefficient, a descriptive statistic, was used for assessing the
reliability between two measurements.
A p-value less than 0.05 was considered as statistically significant.

36
Results
The Student’s t-tests for different parameters indicated that there were no statically significant
differences between the palatal and buccal sides of the teeth. Most of the p-values were larger
than 0.344 showing no difference between buccal and palatal side (table 5). Only the p-value
for the DBL measurements after 6 weeks was smaller (p=0.096) but was still not significant.
Table 5: P-values after different Student’s t-tests comparing the buccal and palatal side at 6 weeks and
12 weeks. P>0.05 is not significant.
Time
Parameters 6w 12w DTL(µm) 0,870 0,922 DBL(µm) 0,096 0,770 DSL(µm) 0,408 0,804 MSL (%) 0,855 0,664 MBL (%) 0,495 0,854 BMC (%) 0,838 0,344
VD (%.µm) 0,783 0,655

37
In this in vitro study, due to the fact that there was no statically significant difference between
buccal and palatal side, these sides are considered as the same side. For the different
parameters, the average of the buccal and palatal values was taken. Descriptive statistics of
the different parameters at 6 and 12 weeks are shown in table 6.
Table 6: Descriptive statistics, mean and standard deviation, of the different parameters after 6 and 12 weeks.
Time Parameters Elmex® Gc Tooth MousseTM Mi Paste PlusTM Control
Mean (SD) Mean (SD) Mean (SD) Mean (SD)
6w DTL(µm) 155,69 (38,62) 188,18 (50,94) 153,12 (64,93) 203,26 (55,06)
DBL(µm) 68,98 (26,88) 80,98 (46,67) 57,76 (34,94) 91,08 (33,21)
DSL(µm) 41,13 (16,76) 47,46 (26,71) 32,59 (17,38) 49,91 (17,84)
MSL (%) 44,74 (15,29) 46,69 (18,70) 44,89 (39,74) 45,50 (12,82)
MBL (%) 33,35 (11,80) 32,74 (11,89) 26,15 (10,01) 27,08 (11,04)
BMC (%) 68,70 (1,91) 69,88 (1,91) 59,73 (11,24) 65,39 (5,83)
VD(%.µm) 3607,43 (1010,54) 3532,84 (1545,52) 3689,70 (1988,62) 4702,64 (2677,47)
12w DTL(µm) 72,38 (44,49) 77,12 (35,61) 83,59 (21,10) 231,73 (74,24)
DBL(µm) 10,20 (16,03) 10,62 (13,50) 16,82 (13,91) 105,67 (55,31)
DSL(µm) 7,51 (14,02) 5,71 (7,32) 9,59 (8,06) 52,83 (22,38)
MSL (%) 5,82 (10,92) 9,09 (12,27) 10,98 (9,20 38,79 (12,34)
MBL (%) 4,72 (9,16) 6,89 (8,72) 8,96 (7,80) 20,22 (5,11)
BMC (%) 63,98 (3,75) 64,08 (3,99) 67,28 (1,77) 67,45 (3,41)
VD(%.µm) 1461,93 (673,36) 1727,80 (814,16) 2339,18 (799,61) 6801,59 (3111,57)

38
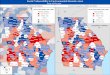
The multivariate test (Wilks' Lambda) of the three different points, DSL-MSL, DBL-MBL
and DTL-BMC, revealed a strong significant difference (p<0.001) for the different
experimental groups between 6 and 12 weeks. No significant difference was found for the
control group (p=0.402). A graphical demonstration or is shown in figure 6.
A B
C D
Figure 6: Mean changes of mineral loss and lesion depth for the different groups after 6 and 12 weeks. A = Elmex Medical Gel®, B = GC Tooth Mousse™, C= Mi Paste Plus™ D = Control group. Each curve shows the three different points, DSL-MSL, DBL-MBL and DTL-BMC.

39
A Mann-Whitney U test showed a significant decrease (p<0.05) for the volume of
demineralisation for the different experimental groups but again not significant difference for
the control group.
The multivariate test (Wilks' lambda exact test) compared the groups two by two at 6 weeks
and at 12 weeks.
At 6 weeks, only BMC-DTL differed significantly for the mineral content and the lesion
depth for the fluoride group versus the control group (p=0.045) and for CPP-ACPgroup
versus CPP-ACPFgroup (p=0.041) (figure 7).
At 12 weeks, the difference was highly significant (p<0.001) for the comparison between the
three experimental groups and the control group for the different parameters. BMC-DTL was
also statistically significant lower for CPP-ACPF versus the fluoride group (p=0.025) and the
CPP-ACP group (p=0.030) (table 7).
The Friedman test showed no statistically significant difference for the volume of
demineralisation (VD), for the 3 experimental groups between 6 and 12 weeks. When
comparing pairwise the different experimental groups with the control group using the
Wilcoxon matched-pairs signed rank test, the VD was statistically significant lower for each
experimental group versus the control group (p=0.007).

40
Figure 7: Schematic representations of the experimental groups and the control group at 6 weeks (A) and at 12 weeks (B).
Table 7: P-values were calculated using the Wilks' lambda exact test, for 6 weeks and 12 weeks. (* Significant p-values).
Significance level
Time Parameter Elmex® vs.
GC Tooth MousseTM
Elmex® vs.
Mi Paste PlusTM
Elmex® vs.
control group
GC Tooth MousseTM
vs. Mi Paste PlusTM
GC Tooth MousseTM
vs. control group
Mi Paste PlusTM
vs. control group
6w MSL-DSL 0,790 0,547 0,492 0,357 0,894 0,129
MBL-DBL 0,543 0,378 0,098 0,406 0,269 0,132
BMC-DTL 0,249 0,067 0,045* 0,041* 0,096 0,142
12w MSL-DSL 0,446 0,388 < 0.001* 0,108 < 0.001* < 0.001*
MBL-DBL 0,681 0,429 < 0.001* 0,318 < 0.001* < 0.001*
BMC-DTL 0,953 0,025* < 0.001* 0,030* < 0.001* < 0.001*
A B

41
The number of body lesions resembles the mineral uptake and loss patterns of mineral
distribution in the subsurface layer. A variety in number of body lesions (NBL) is presented in
this study (figure 8), NBL=0, lack of body lesions; NBL=1, one body lesion; NBL=2, two or
more body lesions.
Figure 8: Histograms of the number of body lesions at 6 weeks (time 1) and 12 weeks (time 2) in intervention
and control groups.

42
The Pearson Chi-Square test and the Fisher’s Exact test showed no significant difference
between the four groups after 6 weeks, and a highly significant difference after 12 weeks
(p<0.001) (Table 8).
Time Chi-square tests Exact Sig. (2-sided) 1 Pearson Chi-Square 0,70 Fisher ‘s Exact Test 0,55
2 Pearson Chi-Square < 0.001* Fisher ‘s Exact Test < 0.001*
A strong statistically significant difference (p<0.001) was demonstrated by the same tests (the
Pearson Chi-Square and the Fisher‘s Exact Test) for the experimental groups between 6 and
12 weeks. Despite the fact that the p-value for the control group equals 0.026 the results are
still significant (table 9).
Table 9: P-values are calculated using the Pearson Chi-Square test and Fisher‘s Exact Test for the four experimental groups between 6 and 12 weeks.
Paste Chi-square tests Exact Sig. (2-sided) Elmex® Pearson Chi-Square < 0.001 Fisher ‘s Exact Test < 0.001 Gc Tooth MousseTM Pearson Chi-Square < 0.001
Fisher ‘s Exact Test < 0.001 Mi Paste Plus TM Pearson Chi-Square < 0.001 Fisher ‘s Exact Test < 0.001
Control Pearson Chi-Square 0,022
Fisher ‘s Exact Test 0,024
Table 8: P-values are calculated using the Pearson Chi-Square test and Fisher‘s Exact Test between the four
groups, for 6 weeks (time 1) and 12 weeks (time 2) (* Significant p-values).

43
The Intraclass Correlation Coefficient, a descriptive statistic, was used for assessing the
reliability between two measurements on the same white spots but on a different time by the
same examiner. The Intraclass Correlation Coefficient (ICC) varying from 0.671 (substantial
agreement) to 0.918 (almost perfect) showed a strong correlation.
Due to the fact that one examiner did all the measurements exclusively, only the ICC for
single measures is demonstrated in table 10.
Table 10: The Intraclass Correlation Coefficients for the different parameters.
*Fleiss Kappa Coefficient Interpretation
< 0 Poor agreement
0.01 – 0.20 Slight agreement
0.21 – 0.40 Fair agreement
0.41 – 0.60 Moderate agreement
0.61 – 0.80 Substantial agreement
0.81 – 1.00 Almost perfect agreement
Parameters ICC 95% Confidence Interval Fleiss interpretation*
Lower Bound Upper Bound DTL (µm) .761 0,294 0,935 Substantial agreement DBL (µm) .918 0,706 0,979 Almost perfect DSL (µm) .846 0,496 0,959 Almost perfect MSL (%) .665 0,105 0,905 Substantial agreement MBL (%) .657 0,091 0,902 Substantial agreement BMC (%) .833 0,464 0,956 Almost perfect VD (%.µm) .671 0,116 0,907 Substantial agreement NBL .816 0,421 0,951 Almost perfect

44
Discussion
A pH-cycling model mimics the dynamics of mineral loss and gain. The high level of
scientific control, should result in lower intrinsic variability of the in vitro models and so
smaller sample size are required (78). However, in vitro experiments cannot fully simulate the
physiologic conditions of the mouth and statistically significant findings do not always equate
to clinically significant findings (96).
Despite many investigations, the efficacy of various remineralisation methods is still difficult
to define. Comparison of the results of these studies is not always possible due to the lack of
homogeneity in the research protocols. In the literature, different methodologies were
described to create white spot lesions. Some authors used polyacrylic acid (Carbopol), others
used 37% phosphoric acid for 30 seconds or a demineralisation solution during 14 days (15,
25, 96, 97). In our study, we used a demineralisation solution by ten Cate and Duijsters for
96h to produce artificial carious lesions (depth of 150-200 µm) (94). A similar method is
used by several other authors (78, 98-100).
Furthermore, there are several ways to quantify remineralisation of WSL. Bailey et al. used a
visual inspection to rate WSL, while others used more quantitative evaluation. Jayarajan et al.
observed the surface morphology (SEM) in combination with a polarized light microscope
(DIAGNOdent®) (101). Pai et al. chose the QLF computer imaging and SEM to make their
measurements (89). The QLF measuring method is used in many studies (31, 102, 103). This
technique has the ability to quantify enamel lesions in an objective way, but it has been stated
that QLF is not suitable for inter-patient comparison (104). In our study, transverse
microradiography (TMR) was used to quantify the mineral content. TMR is considered as the
‘‘gold standard’’ for the determination of mineral loss or gain in experimentally induced
initial carious lesions. The TMR provides a very precise quantitative measurement of the
mineral content (88, 105).

45
In the literature, different experimental periods for the intervention were found. The total
experimental period of this study was based on the instructions of the manufacturer of
toothpastes: a clinical advice to the patient to use the pastes for at least 8 to 12 weeks before
expecting a visually clinical result. A similar protocol was used in other studies (103, 106,
107). In this study we evaluated a first group after 6 weeks to see the results on a short time
usage of the experimental toothpastes and a second group after 12 weeks, which is the
recommended therapy duration. The lesions depth and the mineral content decreased
significantly between 6 and 12 weeks. This could be due to the distribution of the mineral.
The TMR could not show the organic matrix, so further study is needed to explain this
phenomena.
Care has to be taken to standardize the participant’s background. In many studies, variables in
the model (such as hard tissue substrate, diet, biofilm formation, and intra-oral site) are
controlled and standardized to improve the power of the study. In our study we wanted to
exclude this factor by distributing four premolars from the same patient into the four study
groups. An enamel surface layer was removed from each premolar (buccal and palatal) to
avoid a potentially fluoride rich layer and to reduce the individual enamel differences. Despite
these measures, a large diversity of results in each study group was observed.
Clinically lingual surfaces are less prone to caries in comparison to the buccal surfaces (30).
This may be explained by differences in surface morphology, plaque retention, salivary flow
and mechanical cleaning of surfaces by the tongue but also by the shape of the brackets. WSL
development on buccal surfaces is 4.8 times higher than the number of new WSL developing
or progressing on bracketed lingual surfaces. Van der Veen et al. concluded in an in vivo
study that lingual brackets are in favour of buccal brackets, when considering caries outcome
on the smooth surfaces (31). In this study, the buccal of the palatal/lingual side were
separated. However, Student’s t-tests for different parameters showed no statistically
significant differences between both sides. Due to these results no distinction was made
between the palatal and buccal sides.

46
In this in vitro study, the lesion depth but also the mineral content of the WSL decreased
significantly after 12 weeks for the experimental toothpastes (the fluoride, the CPP-ACP and
the CPP-ACPF group) but there were no significant differences between the three different
experimental groups in regression of the WSL.
Fluoride therapy is the most frequently used for caries prevention and remineralisation
methods (38). The repeated application of highly concentrated fluoride gels, like Elmex
Medical gel 12.500ppm, prevent enamel loss by demineralisation (108). However, from the
literature we know that high doses of fluoride are less appropriate for remineralisation or
treatment of white spots. A high concentration of fluoride indeed blocks the surface layer
pores due to crystal growth and prevents further remineralisation of the lesion once the
surface layer is full remineralized (109). Therefore, Øgaard et al. warned against treating
WSL with concentrated fluoride agents (16, 101).
Professor Reynolds (University of Melbourne, Australia) could isolate calcium and phosphate
transporter (CPP) out of cow milk which can capture calcium and phosphate in a soluble
estate. This complex was called CPP-ACP (“casein phosphopeptide” and “amorphous calcium
phosphate”) (76). CPP-ACP was claimed to have the ability to reduce demineralisation and
promote remineralisation by releasing calcium and phosphate ions.
Demineralisation occurs when the pH in the oral environment falls below 5.5, allowing
calcium and phosphate ions to diffuse from the enamel surface. The localized CPP-ACP
nanocomplexes act to buffer free calcium and phosphate ions in the plaque fluid, thereby
limiting enamel demineralisation and enhancing remineralisation (53, 76). Calcium and
phosphate needs to penetrate the surface layer in order to deposit minerals within the body of
the lesion (101).

47
Contradictory results have been reported in the literature about the remineralisation effect of
CPP-ACP on WSL. Recent clinical investigations showed less promising results. Ogata et al.
reported an insufficient effect of remineralisation on enamel subsurface lesions with the use of
CPP-ACP alone. There was no statistically significant difference between the CPP-ACP and
the control with respect to mineral loss; the addition of low levels of fluoride was needed to
observe lesion regression. In contrast, Wu et al. concluded that ACP with or without fluoride
reduced WSL size. After 3 months, Wu’s study demonstrated that fluoride toothpaste alone
was equally effective as CPP-ACP treatment at lesion remineralisation. In a clinical trial by
Bailey et al., the use of CPP-ACP cream enhanced the regression of WSL compared with
placebo (68, 106). The clinical benefits of CPP-ACP paste for the treatment of WSL are not
yet substantiated by credible scientific evidence. In theory, CPP-ACP would seem like an
ideal remineralizing agent for early caries, as discussed in a review by Zero in 2009 (110).
Since 2006 there exists MI Paste Plus which combines CPP-ACP and fluoride. CPP-ACPF,
containing 900 ppm of NaF, increases the salivary concentrations of calcium, inorganic
phosphate and fluoride. CPP prevents spontaneous precipitation and allowed penetration of
the ions deep into the subsurface lesion. This resulted in an increased remineralisation
throughout the body of the lesion whereas the fluoride-alone products tended to remineralize
predominantly in the surface layer (111).
Jayarajan et al. studied the remineralisation effect of CPP-ACP and CPP-ACPF compared to
the remineralisation potential of saliva. Even though saliva has some remineralisation
potential it cannot increase the levels of calcium and phosphate release. CPP-ACPF, an
excellent local slow-delivery system, showed a much higher amount of remineralisation of
WSL. CPP-ACPF is an. The three different groups suggest remineralisation in the same order,
with the CPP-ACPF showing the greatest amount of mineral deposits. CPP-ACPF can
enhance the level of remineralisation of enamel subsurface lesions when the product is used in
situ. The fluoride ions are adsorbed onto the surface of enamel crystals, inhibiting dissolution
and increasing remineralisation. The softened surface lesions remineralize faster and more

48
completely than subsurface lesions. Jayarajan et al. advised to include CPP-ACPF in the
routine hygiene and maintenance instructions for reversing or arresting white spot lesions in
orthodontic patients (101). The Beerens’ group compared, during 3 months CPP-ACPF, with
a control paste in a clinical study. They found no advantage for use of the fluoridated CPP-
ACP paste over regular oral hygiene in WSL regression as measured by QLF (103). Similarly,
Bröchner et al. in a prospective clinical trial using non-fluoridated CPP-ACP paste, found
WSL regression to be comparable with traditional toothpaste after a 4- week treatment period
(102, 106). The study of Shen et al. showed additional benefit in remineralisation of enamel
subsurface lesions with the CPP-ACPF (111). A significant enhancement of fluoride ion’s
ability to remineralize enamel subsurface lesions in situ by CPP–ACP confirmed previous
results showing the same effect as Reynolds' studies where the CPP–ACP was used
immediately after a fluoride-containing toothpaste (69). The conflicting results of these
clinical trials may be related to the method of assessment of WSL regression but also to the
different time periods of application.

49
Critical evaluation
In our study we used conventional toothpaste (1450ppm) in combination with three
experimental products (fluoride, CPP-ACP and CPP-ACPF). The control group had no
contact with toothpaste or experimental products. To investigate the difference in
remineralisation capacity of the tooth paste of experimental products, further research is in
progress.
The formula for 2 means from Pocock was used to calculate the sample size.
n= ����� x = ���
�µ�µ���
n = sample size
�����= is a function of power and significance level
�= the standard deviation
µ1 = the anticipated mean response for the standard or control treatment.
µ2 = the anticipated mean response for the alternative treatment and hence the minimum
clinically important difference (µ2 – µ1) between treatment arms that we would like to detect.
With 27 subjects per group, the trial has 80% power to detect a significant difference of 32,7%
in lesion depth between the 6 and 12 weeks at the 5% significance level. In this study, we had
only 24 subjects in each group.

50
Conclusions
Based on the results of this study, there were no significant differences between the three
different experimental groups in regression of the WSL.
Only after 12 weeks, there was a statistically significant improvement of lesion depths for the
three experimental toothpastes compared with the control group. The lesion depth but also the
mineral content of the WSL decreased significantly after 12 weeks for the experimental
toothpastes. Tough, there is a strong significant difference between the experimental groups
and the control group.
The application of a CPP-ACP or CPP-ACPF paste provides compared with a highly
concentrated amine fluoride, no additional benefit in the regression of WSL.

51
References
1. Theuns HM. The influence of in-vitro and in-vivo demineralzing conditions on dental enamel. .
1987. PubMed PMID: 6959998. PhD thesis, Nederlands instituut voor Praeventieve Gezondheidszorg
2. Featherstone JD. The science and practice of caries prevention. J Am Dent Assoc. 2000
Jul;131(7):887-99. PubMed PMID: 10916327. Epub 2000/08/01. eng.
3. Tranaeus S, Shi XQ, Angmar-Mansson B. Caries risk assessment: methods available to
clinicians for caries detection. Community Dent Oral Epidemiol. 2005 Aug;33(4):265-73. PubMed
PMID: 16008633. Epub 2005/07/13. eng.
4. Mukumoto M, Ohshima T, Ozaki M, Konishi H, Maeda N, Nakamura Y. Effect of microbubbled
water on the removal of a biofilm attached to orthodontic appliances - An in vitro study. Dental
materials journal. 2012;31(5):821-7. PubMed PMID: 23037846. Epub 2012/10/06. eng.
5. Tanner AC, Sonis AL, Lif Holgerson P, Starr JR, Nunez Y, Kressirer CA, et al. White-spot lesions
and gingivitis microbiotas in orthodontic patients. J Dent Res. 2012 Sep;91(9):853-8. PubMed PMID:
22837552. Pubmed Central PMCID: PMC3420397. Epub 2012/07/28. eng.
6. Du M, Cheng N, Tai B, Jiang H, Li J, Bian Z. Randomized controlled trial on fluoride varnish
application for treatment of white spot lesion after fixed orthodontic treatment. Clin Oral Investig.
2012 Apr;16(2):463-8. PubMed PMID: 21331637. Epub 2011/02/19. eng.
7. Torlakovic L, Olsen I, Petzold C, Tiainen H, Ogaard B. Clinical color intensity of white spot
lesions might be a better predictor of enamel demineralization depth than traditional clinical grading.
Am J Orthod Dentofacial Orthop. 2012 Aug;142(2):191-8. PubMed PMID: 22858328. Epub
2012/08/04. eng.
8. Gorelick L, Geiger AM, Gwinnett AJ. Incidence of white spot formation after bonding and
banding. Am J Orthod. 1982 Feb;81(2):93-8. PubMed PMID: 6758594. Epub 1982/02/01. eng.
9. Goswami M, Saha S, Chaitra TR. Latest developments in non-fluoridated remineralizing
technologies. Journal of the Indian Society of Pedodontics and Preventive Dentistry. 2012 Jan-
Mar;30(1):2-6. PubMed PMID: 22565510. Epub 2012/05/09. eng.

52
10. Boersma JG, van der Veen MH, Lagerweij MD, Bokhout B, Prahl-Andersen B. Caries
prevalence measured with QLF after treatment with fixed orthodontic appliances: influencing factors.
Caries Res. 2005 Jan-Feb;39(1):41-7. PubMed PMID: 15591733. Epub 2004/12/14. eng.
11. Vivaldi-Rodrigues G, Demito CF, Bowman SJ, Ramos AL. The effectiveness of a fluoride
varnish in preventing the development of white spot lesions. World journal of orthodontics. 2006
Summer;7(2):138-44. PubMed PMID: 16779972. Epub 2006/06/20. eng.
12. Liu H, Sun J, Dong Y, Lu H, Zhou H, Hansen BF, et al. Periodontal health and relative quantity
of subgingival Porphyromonas gingivalis during orthodontic treatment. Angle Orthod. 2011
Jul;81(4):609-15. PubMed PMID: 21306224. Epub 2011/02/11. eng.
13. Mayne RJ, Cochrane NJ, Cai F, Woods MG, Reynolds EC. In-vitro study of the effect of casein
phosphopeptide amorphous calcium fluoride phosphate on iatrogenic damage to enamel during
orthodontic adhesive removal. Am J Orthod Dentofacial Orthop. 2011 Jun;139(6):e543-51. PubMed
PMID: 21640866. Epub 2011/06/07. eng.
14. Ogaard B. Prevalence of white spot lesions in 19-year-olds: a study on untreated and
orthodontically treated persons 5 years after treatment. Am J Orthod Dentofacial Orthop. 1989
Nov;96(5):423-7. PubMed PMID: 2816842. Epub 1989/11/01. eng.
15. Karlinsey RL, Mackey AC, Stookey GK. In vitro remineralization efficacy of NaF systems
containing unique forms of calcium. Am J Dent. 2009 Jun;22(3):185-8. PubMed PMID: 19650602.
Epub 2009/08/05. eng.
16. Ogaard B, Rolla G, Arends J, ten Cate JM. Orthodontic appliances and enamel
demineralization. Part 2. Prevention and treatment of lesions. Am J Orthod Dentofacial Orthop. 1988
Aug;94(2):123-8. PubMed PMID: 3165239. Epub 1988/08/01. eng.
17. O'Reilly MM, Featherstone JD. Demineralization and remineralization around orthodontic
appliances: an in vivo study. Am J Orthod Dentofacial Orthop. 1987 Jul;92(1):33-40. PubMed PMID:
3300270. Epub 1987/07/01. eng.
18. Ekanayake LS, Sheiham A. Reducing rates of progression of dental caries in British
schoolchildren. A study using bitewing radiographs. Br Dent J. 1987 Oct 24;163(8):265-9. PubMed
PMID: 3479139. Epub 1987/10/24. eng.

53
19. Kidd EA, Fejerskov O. What constitutes dental caries? Histopathology of carious enamel and
dentin related to the action of cariogenic biofilms. J Dent Res. 2004;83 Spec No C:C35-8. PubMed
PMID: 15286119. Epub 2004/08/03. eng.
20. Robertson MA, Kau CH, English JD, Lee RP, Powers J, Nguyen JT. MI Paste Plus to prevent
demineralization in orthodontic patients: a prospective randomized controlled trial. Am J Orthod
Dentofacial Orthop. 2011 Nov;140(5):660-8. PubMed PMID: 22051486. Epub 2011/11/05. eng.
21. Pine CM, ten Bosch JJ. Dynamics of and diagnostic methods for detecting small carious
lesions. Caries Res. 1996;30(6):381-8. PubMed PMID: 8946093. Epub 1996/01/01. eng.
22. Karlinsey RL, Mackey AC, Stookey GK, Pfarrer AM. In vitro assessments of experimental NaF
dentifrices containing a prospective calcium phosphate technology. Am J Dent. 2009 Jun;22(3):180-4.
PubMed PMID: 19650601. Epub 2009/08/05. eng.
23. Derks A, Katsaros C, Frencken JE, van't Hof MA, Kuijpers-Jagtman AM. Caries-inhibiting effect
of preventive measures during orthodontic treatment with fixed appliances. A systematic review.
Caries research. 2004 Sep-Oct;38(5):413-20. PubMed PMID: 15316184. Epub 2004/08/19. eng.
24. Al Maaitah EF, Adeyemi AA, Higham SM, Pender N, Harrison JE. Factors affecting
demineralization during orthodontic treatment: a post-hoc analysis of RCT recruits. Am J Orthod
Dentofacial Orthop. 2011 Feb;139(2):181-91. PubMed PMID: 21300246. Epub 2011/02/09. eng.
25. Behnan SM, Arruda AO, Gonzalez-Cabezas C, Sohn W, Peters MC. In-vitro evaluation of
various treatments to prevent demineralization next to orthodontic brackets. Am J Orthod
Dentofacial Orthop. 2010 Dec;138(6):712 e1-7; discussion -3. PubMed PMID: 21130326. Epub
2010/12/07. eng.
26. Johnson D. MI Paste Plus research. Am J Orthod Dentofacial Orthop. 2012 May;141(5):526;
author reply PubMed PMID: 22554734. Epub 2012/05/05. eng.
27. Artun J, Brobakken BO. Prevalence of carious white spots after orthodontic treatment with
multibonded appliances. Eur J Orthod. 1986 Nov;8(4):229-34. PubMed PMID: 3466795. Epub
1986/11/01. eng.
28. Mitchell L. Decalcification during orthodontic treatment with fixed appliances--an overview.
Br J Orthod. 1992 Aug;19(3):199-205. PubMed PMID: 1390575. Epub 1992/08/01. eng.

54
29. Trimpeneers LM, Dermaut LR. A clinical evaluation of the effectiveness of a fluoride-releasing
visible light-activated bonding system to reduce demineralization around orthodontic brackets. Am J
Orthod Dentofacial Orthop. 1996 Aug;110(2):218-22. PubMed PMID: 8760850. Epub 1996/08/01.
eng.
30. Pulido MT, Wefel JS, Hernandez MM, Denehy GE, Guzman-Armstrong S, Chalmers JM, et al.
The inhibitory effect of MI paste, fluoride and a combination of both on the progression of artificial
caries-like lesions in enamel. Operative dentistry. 2008 Sep-Oct;33(5):550-5. PubMed PMID:
18833861. Epub 2008/10/07. eng.
31. van der Veen MH, Attin R, Schwestka-Polly R, Wiechmann D. Caries outcomes after
orthodontic treatment with fixed appliances: do lingual brackets make a difference? Eur J Oral Sci.
2010 Jun;118(3):298-303. PubMed PMID: 20572865. Epub 2010/06/25. eng.
32. Sudjalim TR, Woods MG, Manton DJ. Prevention of white spot lesions in orthodontic practice:
a contemporary review. Aust Dent J. 2006 Dec;51(4):284-9; quiz 347. PubMed PMID: 17256301. Epub
2007/01/30. eng.
33. Maxfield BJ, Hamdan AM, Tufekci E, Shroff B, Best AM, Lindauer SJ. Development of white
spot lesions during orthodontic treatment: perceptions of patients, parents, orthodontists, and
general dentists. American journal of orthodontics and dentofacial orthopedics : official publication
of the American Association of Orthodontists, its constituent societies, and the American Board of
Orthodontics. 2012 Mar;141(3):337-44. PubMed PMID: 22381494. Epub 2012/03/03. eng.
34. Lynch RJ, Navada R, Walia R. Low-levels of fluoride in plaque and saliva and their effects on
the demineralisation and remineralisation of enamel; role of fluoride toothpastes. Int Dent J.
2004;54(5 Suppl 1):304-9. PubMed PMID: 15509081. Epub 2004/10/29. eng.
35. Derks A, Kuijpers-Jagtman AM, Frencken JE, Van't Hof MA, Katsaros C. Caries preventive
measures used in orthodontic practices: an evidence-based decision? Am J Orthod Dentofacial
Orthop. 2007 Aug;132(2):165-70. PubMed PMID: 17693365. Epub 2007/08/19. eng.
36. Geiger AM, Gorelick L, Gwinnett AJ, Griswold PG. The effect of a fluoride program on white
spot formation during orthodontic treatment. American journal of orthodontics and dentofacial
orthopedics : official publication of the American Association of Orthodontists, its constituent
societies, and the American Board of Orthodontics. 1988 Jan;93(1):29-37. PubMed PMID: 3276146.
Epub 1988/01/01. eng.

55
37. Benson PE, Shah AA, Millett DT, Dyer F, Parkin N, Vine RS. Fluorides, orthodontics and
demineralization: a systematic review. J Orthod. 2005 Jun;32(2):102-14. PubMed PMID: 15994984.
Epub 2005/07/05. eng.
38. Geiger AM, Gorelick L, Gwinnett AJ, Benson BJ. Reducing white spot lesions in orthodontic
populations with fluoride rinsing. American journal of orthodontics and dentofacial orthopedics :
official publication of the American Association of Orthodontists, its constituent societies, and the
American Board of Orthodontics. 1992 May;101(5):403-7. PubMed PMID: 1590288. Epub 1992/05/01.
eng.
39. O'Reilly MM, Featherstone. De and remineralization around orthodontic fixed appliances: an
in vitro study. journal of dental research. 1985;64(301).
40. Benson PE, Parkin N, Millett DT, Dyer FE, Vine S, Shah A. Fluorides for the prevention of white
spots on teeth during fixed brace treatment. Cochrane Database Syst Rev. 2004 (3):CD003809.
PubMed PMID: 15266503. Epub 2004/07/22. eng.
41. Derks A, Katsaros C, Frencken JE, van't Hof MA, Kuijpers-Jagtman AM. Caries-inhibiting effect
of preventive measures during orthodontic treatment with fixed appliances. A systematic review.
Caries Res. 2004 Sep-Oct;38(5):413-20. PubMed PMID: 15316184. Epub 2004/08/19. eng.
42. Todd MA, Staley RN, Kanellis MJ, Donly KJ, Wefel JS. Effect of a fluoride varnish on
demineralization adjacent to orthodontic brackets. Am J Orthod Dentofacial Orthop. 1999
Aug;116(2):159-67. PubMed PMID: 10434089. Epub 1999/08/06. eng.
43. Ogaard B, Duschner H, Ruben J, Arends J. Microradiography and confocal laser scanning
microscopy applied to enamel lesions formed in vivo with and without fluoride varnish treatment.
European journal of oral sciences. 1996 Aug;104(4 ( Pt 1)):378-83. PubMed PMID: 8930586. Epub
1996/08/01. eng.
44. Alexander SA, Ripa LW. Effects of self-applied topical fluoride preparations in orthodontic
patients. Angle Orthod. 2000 Dec;70(6):424-30. PubMed PMID: 11138645. Epub 2001/01/04. eng.
45. Bergstrand F, Twetman S. Evidence for the efficacy of various methods of treating white-spot
lesions after debonding of fixed orthodontic appliances. Journal of clinical orthodontics : JCO. 2003
Jan;37(1):19-21. PubMed PMID: 12621744. Epub 2003/03/08. eng.
46. Kleber CJ, Milleman JL, Davidson KR, Putt MS, Triol CW, Winston AE. Treatment of
orthodontic white spot lesions with a remineralizing dentifrice applied by toothbrushing or mouth

56
trays. The Journal of clinical dentistry. 1999;10(1 Spec No):44-9. PubMed PMID: 10686860. Epub
2000/02/25. eng.
47. Tezel H, Ergucu Z, Onal B. Effects of topical fluoride agents on artificial enamel lesion
formation in vitro. Quintessence Int. 2002 May;33(5):347-52. PubMed PMID: 12014163. Epub
2002/05/17. eng.
48. Wiegand A, Magalhaes AC, Attin T. Is titanium tetrafluoride (TiF4) effective to prevent carious
and erosive lesions? A review of the literature. Oral Health Prev Dent. 2010;8(2):159-64. PubMed
PMID: 20589250. Epub 2010/07/01. eng.
49. Banks PA, Chadwick SM, Asher-McDade C, Wright JL. Fluoride-releasing elastomerics--a
prospective controlled clinical trial. Eur J Orthod. 2000 Aug;22(4):401-7. PubMed PMID: 11029829.
Epub 2000/10/13. eng.
50. Gjorgievska E, Nicholson JW, Grcev AT. Ion migration from fluoride-releasing dental
restorative materials into dental hard tissues. Journal of materials science Materials in medicine.
2012 Jul;23(7):1811-21. PubMed PMID: 22532098. Epub 2012/04/26. eng.
51. Shen P, Cai F, Nowicki A, Vincent J, Reynolds EC. Remineralization of enamel subsurface
lesions by sugar-free chewing gum containing casein phosphopeptide-amorphous calcium phosphate.
J Dent Res. 2001 Dec;80(12):2066-70. PubMed PMID: 11808763. Epub 2002/01/26. eng.
52. Cai F, Shen P, Morgan MV, Reynolds EC. Remineralization of enamel subsurface lesions in situ
by sugar-free lozenges containing casein phosphopeptide-amorphous calcium phosphate. Aust Dent J.
2003 Dec;48(4):240-3. PubMed PMID: 14738126. Epub 2004/01/24. eng.
53. Reynolds EC, Cai F, Shen P, Walker GD. Retention in plaque and remineralization of enamel
lesions by various forms of calcium in a mouthrinse or sugar-free chewing gum. J Dent Res. 2003
Mar;82(3):206-11. PubMed PMID: 12598550. Epub 2003/02/25. eng.
54. Sudjalim TR, Woods MG, Manton DJ, Reynolds EC. Prevention of demineralization around
orthodontic brackets in vitro. Am J Orthod Dentofacial Orthop. 2007 Jun;131(6):705 e1-9. PubMed
PMID: 17561043. Epub 2007/06/15. eng.
55. Sonju Clasen AB, Ogaard B, Duschner H, Ruben J, Arends J, Sonju T. Caries development in
fluoridated and non-fluoridated deciduous and permanent enamel in situ examined by
microradiography and confocal laser scanning microscopy. Adv Dent Res. 1997 Nov;11(4):442-7.
PubMed PMID: 9470502. Epub 1998/02/21. eng.

57
56. Rolla G, Melsen B. On the mechanism of the plaque inhibition by chlorhexidine. J Dent Res.
1975 Jun;54 Spec No B:B57-62. PubMed PMID: 237021. Epub 1975/06/01. eng.
57. Eriksen HM, Gjermo P. Incidence of stained tooth surfaces in students using chlorhexidine-
containing dentifrices. Scand J Dent Res. 1973;81(7):533-7. PubMed PMID: 4520617. Epub
1973/01/01. eng.
58. Knosel M, Bojes M, Jung K, Ziebolz D. Increased susceptibility for white spot lesions by
surplus orthodontic etching exceeding bracket base area. American journal of orthodontics and
dentofacial orthopedics : official publication of the American Association of Orthodontists, its
constituent societies, and the American Board of Orthodontics. 2012 May;141(5):574-82. PubMed
PMID: 22554751. Epub 2012/05/05. eng.
59. Mattousch TJ, van der Veen MH, Zentner A. Caries lesions after orthodontic treatment
followed by quantitative light-induced fluorescence: a 2-year follow-up. Eur J Orthod. 2007
Jun;29(3):294-8. PubMed PMID: 17483494. Epub 2007/05/08. eng.
60. Andersson A, Skold-Larsson K, Hallgren A, Petersson LG, Twetman S. Effect of a dental cream
containing amorphous cream phosphate complexes on white spot lesion regression assessed by laser
fluorescence. Oral Health Prev Dent. 2007;5(3):229-33. PubMed PMID: 17977295. Epub 2007/11/06.
eng.
61. Willmot DR. White lesions after orthodontic treatment: does low fluoride make a difference?
J Orthod. 2004 Sep;31(3):235-42; discussion 02. PubMed PMID: 15489367. Epub 2004/10/19. eng.
62. Welbury RR, Carter NE. The hydrochloric acid-pumice microabrasion technique in the
treatment of post-orthodontic decalcification. Br J Orthod. 1993 Aug;20(3):181-5. PubMed PMID:
8399050. Epub 1993/08/01. eng.
63. Al-Khateeb S, Forsberg CM, de Josselin de Jong E, Angmar-Mansson B. A longitudinal laser
fluorescence study of white spot lesions in orthodontic patients. Am J Orthod Dentofacial Orthop.
1998 Jun;113(6):595-602. PubMed PMID: 9637561. Epub 1998/06/24. eng.
64. Van Croonenburg EJ, Woltgens JH, Qua CJ, De Blieck-Hogervorst JM. Comparison of the
effects of 0.1% F- and 0.025% F- on mineral loss in enamel under intra oral cariogenicity test
conditions. J Biol Buccale. 1986 Sep;14(3):177-81. PubMed PMID: 3464587. Epub 1986/09/01. eng.
65. Ardu S, Castioni NV, Benbachir N, Krejci I. Minimally invasive treatment of white spot enamel
lesions. Quintessence Int. 2007 Sep;38(8):633-6. PubMed PMID: 17823680. Epub 2007/09/08. eng.

58
66. Cai F, Manton DJ, Shen P, Walker GD, Cross KJ, Yuan Y, et al. Effect of addition of citric acid
and casein phosphopeptide-amorphous calcium phosphate to a sugar-free chewing gum on enamel
remineralization in situ. Caries Res. 2007;41(5):377-83. PubMed PMID: 17713338. Epub 2007/08/24.
eng.
67. Reynolds EC. Calcium phosphate-based remineralization systems: scientific evidence? Aust
Dent J. 2008 Sep;53(3):268-73. PubMed PMID: 18782374. Epub 2008/09/11. eng.
68. Bailey DL, Adams GG, Tsao CE, Hyslop A, Escobar K, Manton DJ, et al. Regression of post-
orthodontic lesions by a remineralizing cream. J Dent Res. 2009 Dec;88(12):1148-53. PubMed PMID:
19887683. Epub 2009/11/06. eng.
69. Reynolds EC, Cai F, Cochrane NJ, Shen P, Walker GD, Morgan MV, et al. Fluoride and casein
phosphopeptide-amorphous calcium phosphate. J Dent Res. 2008 Apr;87(4):344-8. PubMed PMID:
18362316. Epub 2008/03/26. eng.
70. Glockner K, Ebeleseder K, Stadtler P. [The bleaching of stained anterior teeth]. Schweiz
Monatsschr Zahnmed. 1997;107(5):413-25. PubMed PMID: 9304185. Epub 1997/01/01. Das Bleichen
von verfarbten Frontzahnen. fre
71. Knosel M, Attin R, Becker K, Attin T. External bleaching effect on the color and luminosity of
inactive white-spot lesions after fixed orthodontic appliances. Angle Orthod. 2007 Jul;77(4):646-52.
PubMed PMID: 17605483. Epub 2007/07/04. eng.
72. Wiegand A, Schreier M, Attin T. Effect of different fluoridation regimes on the microhardness
of bleached enamel. Oper Dent. 2007 Nov-Dec;32(6):610-5. PubMed PMID: 18051012. Epub
2007/12/07. eng.
73. Gonzalez-Rodriguez A, de Dios Lopez-Gonzalez J, del Castillo Jde D, Villalba-Moreno J.
Comparison of effects of diode laser and CO2 laser on human teeth and their usefulness in topical
fluoridation. Lasers in medical science. 2011 May;26(3):317-24. PubMed PMID: 20422239. Epub
2010/04/28. eng.
74. Harazaki M, Hayakawa K, Fukui T, Isshiki Y, Powell LG. The Nd-YAG laser is useful in
prevention of dental caries during orthodontic treatment. The Bulletin of Tokyo Dental College. 2001
May;42(2):79-86. PubMed PMID: 11588818. Epub 2001/10/09. eng.

59
75. Rose RK. Effects of an anticariogenic casein phosphopeptide on calcium diffusion in
streptococcal model dental plaques. Arch Oral Biol. 2000 Jul;45(7):569-75. PubMed PMID: 10785520.
Epub 2000/04/29. eng.
76. Reynolds EC. Remineralization of enamel subsurface lesions by casein phosphopeptide-
stabilized calcium phosphate solutions. J Dent Res. 1997 Sep;76(9):1587-95. PubMed PMID: 9294493.
Epub 1997/09/19. eng.
77. Iijima Y, Cai F, Shen P, Walker G, Reynolds C, Reynolds EC. Acid resistance of enamel
subsurface lesions remineralized by a sugar-free chewing gum containing casein phosphopeptide-
amorphous calcium phosphate. Caries Res. 2004 Nov-Dec;38(6):551-6. PubMed PMID: 15528910.
Epub 2004/11/06. eng.
78. Buzalaf MA, Hannas AR, Magalhaes AC, Rios D, Honorio HM, Delbem AC. pH-cycling models
for in vitro evaluation of the efficacy of fluoridated dentifrices for caries control: strengths and
limitations. J Appl Oral Sci. 2010 Jul-Aug;18(4):316-34. PubMed PMID: 20835565. Epub 2010/09/14.
eng.
79. Cochrane NJ, Saranathan S, Cai F, Cross KJ, Reynolds EC. Enamel subsurface lesion
remineralisation with casein phosphopeptide stabilised solutions of calcium, phosphate and fluoride.
Caries Res. 2008;42(2):88-97. PubMed PMID: 18204252. Epub 2008/01/22. eng.
80. Naumova EA, Niemann N, Aretz L, Arnold WH. Effects of different amine fluoride
concentrations on enamel remineralization. Journal of dentistry. 2012 Sep;40(9):750-5. PubMed
PMID: 22677913. Epub 2012/06/09. eng.
81. Winston AE, Bhaskar SN. Caries prevention in the 21st century. J Am Dent Assoc. 1998
Nov;129(11):1579-87. PubMed PMID: 9818575. Epub 1998/11/18. eng.
82. Topping GV, Pitts NB. Clinical visual caries detection. Monogr Oral Sci. 2009;21:15-41.
PubMed PMID: 19494673. Epub 2009/06/06. eng.
83. Willmot DR, Benson PE, Pender N, Brook AH. Reproducibility of quantitative measurement of
white enamel demineralisation by image analysis. Caries Res. 2000 Mar-Apr;34(2):175-81. PubMed
PMID: 10773636. Epub 2000/04/25. eng.
84. Heinrich-Weltzien R, Kuhnisch J, Ifland S, Tranaeus S, Angmar-Mansson B, Stosser L.
Detection of initial caries lesions on smooth surfaces by quantitative light-induced fluorescence and

60
visual examination: an in vivo comparison. Eur J Oral Sci. 2005 Dec;113(6):494-8. PubMed PMID:
16324139. Epub 2005/12/06. eng.
85. Aljehani A, Tranaeus S, Forsberg CM, Angmar-Mansson B, Shi XQ. In vitro quantification of
white spot enamel lesions adjacent to fixed orthodontic appliances using quantitative light-induced
fluorescence and DIAGNOdent. Acta Odontol Scand. 2004 Dec;62(6):313-8. PubMed PMID: 15848974.
Epub 2005/04/26. eng.
86. Jablonski-Momeni A, Schipper HM, Rosen SM, Heinzel-Gutenbrunner M, Roggendorf MJ, Stoll
R, et al. Performance of a fluorescence camera for detection of occlusal caries in vitro. Odontology /
the Society of the Nippon Dental University. 2011 Jan;99(1):55-61. PubMed PMID: 21271327. Epub
2011/01/29. eng.
87. Kang H, Jiao JJ, Lee C, Le MH, Darling CL, Fried D. Nondestructive Assessment of Early Tooth
Demineralization Using Cross-Polarization Optical Coherence Tomography. IEEE J Sel Top Quantum
Electron. 2010 Jul;16(4):870-6. PubMed PMID: 21660217. Pubmed Central PMCID: 3109909. Epub
2011/06/11. Eng.
88. Lo EC, Zhi QH, Itthagarun A. Comparing two quantitative methods for studying
remineralization of artificial caries. J Dent. 2010 Apr;38(4):352-9. PubMed PMID: 20079396. Epub
2010/01/19. eng.
89. Pai D, Bhat SS, Taranath A, Sargod S, Pai VM. Use of laser fluorescence and scanning electron
microscope to evaluate remineralization of incipient enamel lesions remineralized by topical
application of casein phospho peptide amorphous calcium phosphate (CPP-aCP) containing cream. J
Clin Pediatr Dent. 2008 Spring;32(3):201-6. PubMed PMID: 18524269. Epub 2008/06/06. eng.
90. Watari F. In situ quantitative analysis of etching process of human teeth by atomic force
microscopy. J Electron Microsc (Tokyo). 2005 Jun;54(3):299-308. PubMed PMID: 16148016. Epub
2005/09/09. eng.
91. Magalhaes AC, Moron BM, Comar LP, Wiegand A, Buchalla W, Buzalaf MA. Comparison of
cross-sectional hardness and transverse microradiography of artificial carious enamel lesions induced
by different demineralising solutions and gels. Caries Res. 2009;43(6):474-83. PubMed PMID:
20016178. Epub 2009/12/18. eng.
92. Cheng ZJ, Wang XM, Cui FZ, Ge J, Yan JX. The enamel softening and loss during early erosion
studied by AFM, SEM and nanoindentation. Biomed Mater. 2009 Feb;4(1):015020. PubMed PMID:
19193971. Epub 2009/02/06. eng.

61
93. Chu JS, Fox JL, Higuchi WI, Nash WP. Electron probe micro-analysis for subsurface
demineralization and remineralization of dental enamel. J Dent Res. 1989 Jan;68(1):26-31. PubMed
PMID: 2910956. Epub 1989/01/01. eng.
94. ten Cate JM, Duijsters PP. Alternating demineralization and remineralization of artificial
enamel lesions. Caries research. 1982;16(3):201-10. PubMed PMID: 6953998. Epub 1982/01/01. eng.
95. Benson PE, Higham SM, Pender N. An in vitro assessment using transverse microradiography
of the effect on mineral loss of etching enamel for in situ studies. Orthod Craniofac Res. 2003
Nov;6(4):242-9. PubMed PMID: 14606528. Epub 2003/11/11. eng.
96. Ballard RW, Hagan JL, Phaup AN, Sarkar N, Townsend JA, Armbruster PC. Evaluation of 3
commercially available materials for resolution of white spot lesions. Am J Orthod Dentofacial Orthop.
2013 Apr;143(4 Suppl):S78-84. PubMed PMID: 23540640. Epub 2013/04/12. eng.
97. Al-Khateeb S, Exterkate R, Angmar-Mansson B, ten Cate JM. Effect of acid-etching on
remineralization of enamel white spot lesions. Acta odontologica Scandinavica. 2000 Feb;58(1):31-6.
PubMed PMID: 10809397. Epub 2000/05/16. eng.
98. Rana R, Itthagarun A, King NM. Effects of dentifrices on artificial caries like lesions: an in vitro
pH cycling study. Int Dent J. 2007 Aug;57(4):243-8. PubMed PMID: 17849682. Epub 2007/09/14. eng.
99. Itthagarun A, Wei SH, Wefel JS. The effect of different commercial dentifrices on enamel
lesion progression: an in vitro pH-cycling study. Int Dent J. 2000 Feb;50(1):21-8. PubMed PMID:
10945176. Epub 2000/08/17. eng.
100. Thaveesangpanich P, Itthagarun A, King NM, Wefel JS. The effects of child formula
toothpastes on enamel caries using two in vitro pH-cycling models. Int Dent J. 2005 Aug;55(4):217-23.
PubMed PMID: 16167610. Epub 2005/09/20. eng.
101. Jayarajan J, Janardhanam P, Jayakumar P. Efficacy of CPP-ACP and CPP-ACPF on enamel
remineralization - an in vitro study using scanning electron microscope and DIAGNOdent. Indian
journal of dental research : official publication of Indian Society for Dental Research. 2011 Jan-
Feb;22(1):77-82. PubMed PMID: 21525682. Epub 2011/04/29. eng.
102. Brochner A, Christensen C, Kristensen B, Tranaeus S, Karlsson L, Sonnesen L, et al. Treatment
of post-orthodontic white spot lesions with casein phosphopeptide-stabilised amorphous calcium
phosphate. Clinical oral investigations. 2011 Jun;15(3):369-73. PubMed PMID: 20383545. Epub
2010/04/13. eng.

62
103. Beerens MW, van der Veen MH, van Beek H, ten Cate JM. Effects of casein phosphopeptide
amorphous calcium fluoride phosphate paste on white spot lesions and dental plaque after
orthodontic treatment: a 3-month follow-up. European journal of oral sciences. 2010
Dec;118(6):610-7. PubMed PMID: 21083623. Epub 2010/11/19. eng.
104. Anderson P, Bollet-Quivogne FR, Dowker SE, Elliott JC. Demineralization in enamel and
hydroxyapatite aggregates at increasing ionic strengths. Archives of oral biology. 2004
Mar;49(3):199-207. PubMed PMID: 14725811. Epub 2004/01/17. eng.
105. Mensinkai PK, Ccahuana-Vasquez RA, Chedjieu I, Amaechi BT, Mackey AC, Walker TJ, et al. In
situ remineralization of white-spot enamel lesions by 500 and 1,100 ppm F dentifrices. Clinical oral
investigations. 2012 Aug;16(4):1007-14. PubMed PMID: 21750917. Epub 2011/07/14. eng.
106. Pliska BT, Warner GA, Tantbirojn D, Larson BE. Treatment of white spot lesions with ACP
paste and microabrasion. The Angle orthodontist. 2012 Sep;82(5):765-9. PubMed PMID: 22352382.
Epub 2012/02/23. eng.
107. Wu G, Liu X, Hou Y. Analysis of the effect of CPP-ACP tooth mousse on enamel
remineralization by circularly polarized images. The Angle orthodontist. 2010 Sep;80(5):933-8.
PubMed PMID: 20578866. Epub 2010/06/29. eng.
108. Knosel M, Forslund L, Jung K, Ziebolz D. Efficacy of different strategies in protecting enamel
against demineralization during fixed orthodontic treatment. Journal of orofacial orthopedics =
Fortschritte der Kieferorthopadie : Organ/official journal Deutsche Gesellschaft fur Kieferorthopadie.
2012 May;73(3):194-203. PubMed PMID: 22576861. Epub 2012/05/12. eng.
109. ten Cate JM, Featherstone JD. Mechanistic aspects of the interactions between fluoride and
dental enamel. Critical reviews in oral biology and medicine : an official publication of the American
Association of Oral Biologists. 1991;2(3):283-96. PubMed PMID: 1892991. Epub 1991/01/01. eng.
110. Zero DT. Recaldent--evidence for clinical activity. Advances in dental research. 2009;21(1):30-
4. PubMed PMID: 19717408. Epub 2009/09/01. eng.
111. Shen P, Manton DJ, Cochrane NJ, Walker GD, Yuan Y, Reynolds C, et al. Effect of added
calcium phosphate on enamel remineralization by fluoride in a randomized controlled in situ trial.
Journal of dentistry. 2011 Jul;39(7):518-25. PubMed PMID: 21621580. Epub 2011/05/31. eng.

Annexe
Prof. Dr. G. De Pauw, Afdelingshoofd Dienst Orthodontie De Pintelaan 185 9000 GENT, BELGIË
Informatie-toestemmingsformulier (voor
Geachte heer, mevrouw Beste patiënt, Eerder heeft uw tandarts/kaakchirurg u voorgesteld bij u meerdere tanden om bepaalde redenen (bijvoorbeeld omwille van te weinig plaats in de kaak) te laten verwijderen. Invan mijn master-na-master opleiding orthodontie ben ik een experiment gestart, waarbij ik tanden verzamel, met de bedoeling verschillende tandpasta’s te vergelijken. Nu zou ik u willen vragen of u bereid bent uw getrokken tanden af te staan in hetwetenschappelijk onderzoek. Dit onderzoek is goedgekeurd door het ethisch comité UZGent. Maar deze goedkeuring dient niet beschouwd te worden als aansporing om deel te nemen aan deze studie. Doel en verloop van het onderzoekGraag zou ik 3 verschillende tandpasta’s vergelijken (Elmex Medical GelMousseTM, MI Paste PlusTM) met een controlegroep (gewone tandpasta).Het wordt een studie waarin ik de grootte en diepte van white spots (= ontkalkingen op de tand) ga evalueren na ze zelf te hebben gecreëerd. White spots komen in veel gevallen voor na een orthodontische behandeling. Voor mijn studie heb ik 4 intacte voorkiezen van dezelfde patiënt nodig. En in totaal zouden er een 40-tal patiënten deelnemen (160 tanden). Praktische gegevens:
- Deelname aan deze studie brengt geen therapeutisch voordeel met zich mee. - Er zullen voor u geen extra kosten zijn. Alle onkosten i.v.m. de studie worden door
het ziekenhuis gedragen.- Het onderzoek is volledig anoniem. De gegevens worden strikt v
zonder vermelding van uw naam bewaard. De privacy zal dus volledig worden gerespecteerd.
- Als u toch liever heeft dat uw tanden niet gebruikt worden voor dit experiment, dan kan u zonder enig probleem weigeren. Een eventuele weigering om uwstaan zal zeker geen invloed hebben op een eventuele verdere behandeling.
Mag ik u vragen om op de ommezijde te tekenen voor akkoord, indien u bereid bent uw tanden af te staan in het kader van dit experiment? Vriendelijk dank. Charlotte Van Elst Specialist orthodontie in opleidingTel: 093326893
toestemmingsformulier (voor patiënten tussen de 12 en 18 jaar en ouders)
Eerder heeft uw tandarts/kaakchirurg u voorgesteld bij u meerdere tanden om bepaalde redenen (bijvoorbeeld omwille van te weinig plaats in de kaak) te laten verwijderen. In
master opleiding orthodontie ben ik een experiment gestart, waarbij ik tanden verzamel, met de bedoeling verschillende tandpasta’s te vergelijken. Nu zou ik u willen vragen of u bereid bent uw getrokken tanden af te staan in het
Dit onderzoek is goedgekeurd door het ethisch comité UZGent. Maar deze goedkeuring dient niet beschouwd te worden als aansporing om deel te nemen aan deze studie.
Doel en verloop van het onderzoek verschillende tandpasta’s vergelijken (Elmex Medical Gel®, Gc Tooth
) met een controlegroep (gewone tandpasta). Het wordt een studie waarin ik de grootte en diepte van white spots (= ontkalkingen op de
f te hebben gecreëerd. White spots komen in veel gevallen voor na een orthodontische behandeling. Voor mijn studie heb ik 4 intacte voorkiezen van dezelfde patiënt nodig. En in totaal zouden
tal patiënten deelnemen (160 tanden).
Deelname aan deze studie brengt geen therapeutisch voordeel met zich mee. Er zullen voor u geen extra kosten zijn. Alle onkosten i.v.m. de studie worden door het ziekenhuis gedragen. Het onderzoek is volledig anoniem. De gegevens worden strikt vzonder vermelding van uw naam bewaard. De privacy zal dus volledig worden
Als u toch liever heeft dat uw tanden niet gebruikt worden voor dit experiment, dan kan u zonder enig probleem weigeren. Een eventuele weigering om uwstaan zal zeker geen invloed hebben op een eventuele verdere behandeling.
Mag ik u vragen om op de ommezijde te tekenen voor akkoord, indien u bereid bent uw tanden af te staan in het kader van dit experiment?
Specialist orthodontie in opleiding
63
patiënten tussen de 12 en 18 jaar en ouders)
Eerder heeft uw tandarts/kaakchirurg u voorgesteld bij u meerdere tanden om bepaalde redenen (bijvoorbeeld omwille van te weinig plaats in de kaak) te laten verwijderen. In functie
master opleiding orthodontie ben ik een experiment gestart, waarbij ik tanden verzamel, met de bedoeling verschillende tandpasta’s te vergelijken. Nu zou ik u willen vragen of u bereid bent uw getrokken tanden af te staan in het kader van dit
Dit onderzoek is goedgekeurd door het ethisch comité UZGent. Maar deze goedkeuring dient niet beschouwd te worden als aansporing om deel te nemen aan deze studie.
®, Gc Tooth
Het wordt een studie waarin ik de grootte en diepte van white spots (= ontkalkingen op de f te hebben gecreëerd. White spots komen in veel gevallen voor
Voor mijn studie heb ik 4 intacte voorkiezen van dezelfde patiënt nodig. En in totaal zouden
Deelname aan deze studie brengt geen therapeutisch voordeel met zich mee. Er zullen voor u geen extra kosten zijn. Alle onkosten i.v.m. de studie worden door
Het onderzoek is volledig anoniem. De gegevens worden strikt vertrouwelijk en zonder vermelding van uw naam bewaard. De privacy zal dus volledig worden
Als u toch liever heeft dat uw tanden niet gebruikt worden voor dit experiment, dan kan u zonder enig probleem weigeren. Een eventuele weigering om uw tanden af te staan zal zeker geen invloed hebben op een eventuele verdere behandeling.
Mag ik u vragen om op de ommezijde te tekenen voor akkoord, indien u bereid bent uw

Wij, ondergetekende, ………………………………………………………………, ouders van …………………………………………………………geven hierbij de toestemming om zijn/haar tanden, die om tandheelkundige/orthodontische redenen werden verwijderd, af te staan in het kader van een onderzoek. Voor de vrijwilliger: Datum Handtekening Voor de ouders: Datum
Wij, ondergetekende, ………………………………………………………………, ouders van ………………………………………………………… geven hierbij de toestemming om zijn/haar tanden, die om tandheelkundige/orthodontische
rd, af te staan in het kader van een onderzoek.
Datum Handtekening
Handtekening
64
Wij, ondergetekende, ………………………………………………………………, ouders van
geven hierbij de toestemming om zijn/haar tanden, die om tandheelkundige/orthodontische
Datum Handtekening
Handtekening

Prof. Dr. G. De Pauw Afdelingshoofd Dienst Orthodontie De Pintelaan 185 9000 GENT BELGIË Informatie-toestemmingsformulier (voor patiënten ouder dan 18 jaar ) Geachte heer, mevrouw Beste patiënt, Eerder heeft uw tandarts/kaakchirurg u redenen (bijvoorbeeld omwille van te weinig plaats in de kaak) te laten verwijderen. In functie van mijn master-na-master opleiding orthodontie ben ik een experiment gestart, waarbij ik tanden verzamel, met de bedoeling verschillende tandpasta’s te vergelijken. Nu zou ik u willen vragen of u bereid bent uw getrokken tanden af te staan in het kader van dit wetenschappelijk onderzoek. Dit onderzoek is goedgekeurd door het ethisch comité UZGent. Maar deze goedkeuriniet beschouwd te worden als aansporing om deel te nemen aan deze studie. Doel en verloop van het onderzoekGraag zou ik 3 verschillende tandpasta’s vergelijken (Elmex Medical GelMousseTM, MI Paste PlusTM) met een controlegroep (gewoHet wordt een studie waarin ik de grootte en diepte van white spots (= ontkalkingen op de tand) ga evalueren na ze zelf te hebben gecreëerd. White spots komen in veel gevallen voor na een orthodontische behandeling. Voor mijn studie heb ik 4 intacte voorkiezen van dezelfde patiënt nodig. En in totaal zouden er een 40-tal patiënten deelnemen (160 tanden). Praktische gegevens:
- Deelname aan deze studie brengt geen therapeutisch voordeel met zich mee. - Er zullen voor u geen extra kosten zijn.
het ziekenhuis gedragen.- Het onderzoek is volledig anoniem. De gegevens worden strikt vertrouwelijk en
zonder vermelding van uw naam bewaard. De privacy zal dus volledig worden gerespecteerd.
- Als u toch liever heeft dat uw tanden niet gebruikt worden voor dit experiment, dan kan u zonder enig probleem weigeren. Een eventuele weigering om uw tanden af te staan zal zeker geen invloed hebben op een eventuele verdere behandeling.
Mag ik u vragen om op de ommezijde tanden af te staan in het kader van dit experiment? Vriendelijk dank. Charlotte Van Elst Specialist orthodontie in opleidingTel: 093326893 Faculteit Geneeskunde en Gezondheidswetenschappen
De Pintelaan 185 P8, B-9000 Gent
toestemmingsformulier (voor patiënten ouder dan 18 jaar )
Eerder heeft uw tandarts/kaakchirurg u voorgesteld bij u meerdere tanden om bepaalde redenen (bijvoorbeeld omwille van te weinig plaats in de kaak) te laten verwijderen. In functie
master opleiding orthodontie ben ik een experiment gestart, waarbij ik bedoeling verschillende tandpasta’s te vergelijken. Nu zou ik u
willen vragen of u bereid bent uw getrokken tanden af te staan in het kader van dit
Dit onderzoek is goedgekeurd door het ethisch comité UZGent. Maar deze goedkeuriniet beschouwd te worden als aansporing om deel te nemen aan deze studie.
Doel en verloop van het onderzoek Graag zou ik 3 verschillende tandpasta’s vergelijken (Elmex Medical Gel®
) met een controlegroep (gewone tandpasta). Het wordt een studie waarin ik de grootte en diepte van white spots (= ontkalkingen op de tand) ga evalueren na ze zelf te hebben gecreëerd. White spots komen in veel gevallen voor na een orthodontische behandeling.
4 intacte voorkiezen van dezelfde patiënt nodig. En in totaal zouden tal patiënten deelnemen (160 tanden).
Deelname aan deze studie brengt geen therapeutisch voordeel met zich mee. Er zullen voor u geen extra kosten zijn. Alle onkosten i.v.m. de studie worden door het ziekenhuis gedragen. Het onderzoek is volledig anoniem. De gegevens worden strikt vertrouwelijk en zonder vermelding van uw naam bewaard. De privacy zal dus volledig worden
heeft dat uw tanden niet gebruikt worden voor dit experiment, dan kan u zonder enig probleem weigeren. Een eventuele weigering om uw tanden af te staan zal zeker geen invloed hebben op een eventuele verdere behandeling.
Mag ik u vragen om op de ommezijde te tekenen voor akkoord, indien u bereid bent uw tanden af te staan in het kader van dit experiment?
Specialist orthodontie in opleiding
Faculteit Geneeskunde en Gezondheidswetenschappen – Vakgroep Tandheelkunde 9000 Gent
65
voorgesteld bij u meerdere tanden om bepaalde redenen (bijvoorbeeld omwille van te weinig plaats in de kaak) te laten verwijderen. In functie
master opleiding orthodontie ben ik een experiment gestart, waarbij ik bedoeling verschillende tandpasta’s te vergelijken. Nu zou ik u
willen vragen of u bereid bent uw getrokken tanden af te staan in het kader van dit
Dit onderzoek is goedgekeurd door het ethisch comité UZGent. Maar deze goedkeuring dient niet beschouwd te worden als aansporing om deel te nemen aan deze studie.
®, Gc Tooth
Het wordt een studie waarin ik de grootte en diepte van white spots (= ontkalkingen op de tand) ga evalueren na ze zelf te hebben gecreëerd. White spots komen in veel gevallen voor
4 intacte voorkiezen van dezelfde patiënt nodig. En in totaal zouden
Deelname aan deze studie brengt geen therapeutisch voordeel met zich mee. Alle onkosten i.v.m. de studie worden door
Het onderzoek is volledig anoniem. De gegevens worden strikt vertrouwelijk en zonder vermelding van uw naam bewaard. De privacy zal dus volledig worden
heeft dat uw tanden niet gebruikt worden voor dit experiment, dan kan u zonder enig probleem weigeren. Een eventuele weigering om uw tanden af te staan zal zeker geen invloed hebben op een eventuele verdere behandeling.
te tekenen voor akkoord, indien u bereid bent uw

Ik, ondergetekende, ………………………………………………………………, geefhierbij de toestemming om mijn werden verwijderd, af te staan in het kader van een onderzoek. Voor de vrijwilliger: Datum Handtekening
Ik, ondergetekende, ………………………………………………………………, geefmijn tanden, die om tandheelkundige/orthodontische redenen
werden verwijderd, af te staan in het kader van een onderzoek.
Datum Handtekening
66
Ik, ondergetekende, ………………………………………………………………, geef tanden, die om tandheelkundige/orthodontische redenen
Datum Handtekening