Embed Size (px)
Citation preview

A comparison of mechanisms underlying disturbances ofbleeding caused by spontaneous dysfunctional uterine
bleeding or hormonal contraception
Ian S.Fraser1, Martha Hickey and Jing-yu Song
Sydney Centre for Reproductive Health Research, Department of Obstetrics and Gynaecology, Universityof Sydney, Sydney, NSW 2006, Australia
'To whom correspondence should be addressed
Recent research has not been able to demon-strate close endometrial morphological correla-tions with specific abnormalities of menstrualbleeding, but has pointed to an increasingnumber of molecular mechanisms that may beinvolved in the occurrence of certain formsof abnormal uterine bleeding. Ovulatory andanovulatory dysfunctional uterine bleeding(DUB) and progestogen-related breakthroughbleeding (BTB) are three conditions with quitedifferent clinical characteristics. It is also prob-able that the local endometrial molecular mech-anisms associated with these three menstrualdisturbances are quite different Ovulatory DUBis associated with a series of vascular andhaemostatic disturbances that all appear tocontribute to increased loss of blood and tissuefluid at menstruation. Anovulatory DUB isassociated with obvious disturbances of endo-metrial histology, vascular morphology and fra-gility, with variable and increased blood flow.Progestogen-related BTB is associated with amultitude of morphological and functionalendometrial changes that appear to relate pre-dominantly to a patchy capillary origin for thebleeding. Many molecular and cellular changeshave been observed in all three conditions. It isnot yet known whether there is a single, butdifferent, underlying mechanism responsible forthese multiple abnormalities in each of the threeclinical situations.
Key words: abnormal menstrual bleeding/dysfunc-tional uterine bleeding/endometrium/hormonalcontraception/menstruation
Introduction
Disturbances of menstrual bleeding are a majormedical and social problem for women, theirfamilies and the health services. In fact, disturb-ances of bleeding are relatively common in allage groups between 10 and 55 years. Menstrualdisorders are the second most common gynaeco-logical condition resulting in hospital referral(Coulter et al, 1989), and affect up to one-thirdof women of child-bearing age (Hallberg et al,1966; Gath et al., 1987). One of the commonestof these conditions is dysfunctional uterine bleed-ing. For those women using hormonal contracept-ive methods, minor disturbances of menstrualbleeding (breakthrough bleeding; BTB) are a com-mon occurrence, and represent the most frequentreason stated for discontinuation of progestogen-only contraceptive methods (Belsey et al, 1988).Irregular bleeding with hormonal contraceptiontends to be light in volume, but may be frequentor prolonged. Women may interpret prolongedbleeding as heavy (Fraser, 1983a), and be con-cerned for the long-term health effects of extendedbleeding episodes. Because these contraceptivemethods are safe, effective, flexible and econom-ical, and there are no established methods ofregulating the bleeding without the addition ofoestrogens, disturbances of the menstrual bleedingpattern represent a considerable managementproblem.
The term dysfunctional uterine bleeding (DUB)refers to excessively heavy, prolonged or frequentbleeding (most commonly heavy, i.e. menorrhagia)which is not caused by pregnancy or any recogniz-able pelvic or systemic disease (Fraser, 1989).DUB is a diagnosis of exclusion, and will apply
Human Reproduction Volume 11 Supplement 2 1996 O European Society for Human Reproduction & Embryology 165
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from

LS.Frastr, M.Hickey and J.-ySong
in 40-60% of cases of excessive menstrual bleeding(Cameron, 1989; Fraser, 1989). Ovarian cyclesassociated with excessive bleeding may be ovulat-ory or anovulatory. In modern Western society,DUB is ovulatory in ~80% of cases (Cameron,1989). Bleeding in these circumstances tends tobe heavy and/or prolonged, but is generally regular.Anovulatory DUB is seen most commonly at thebeginning and end of reproductive life, and maybe irregular and/or excessive (Schroder, 1954). Itneeds to be recognized that there are widespreaddifferences in the definition of 'dysfunctional uter-ine bleeding', especially in the USA where ovulat-ory DUB is not widely acknowledged as a specificcondition (Allen-Davis and Schlaff, 1995; Fraser,1996).
Regardless of its perceived cause, menstrualbleeding that fails to occur at regular or predictabletimes, or bleeding that is of markedly reducedor excessive quantity, is poorly accepted by themajority of women (Snowden and Christian, 1983).The implication of this is that many women willbe more favourably disposed to a contraceptivemethod if it causes regular periods with normalflow than if there is some departure from thenorm. This study was carried out >15 years ago(Snowden and Christian, 1983), and in manyWestern societies nowadays it appears that youngwomen will often be happy to accept amenorrhoea,provided that the method has a high contraceptiveefficacy and that the amenorrhoea is not likely tosignify a risk of pregnancy. Women are alsosensitive to more subtle characteristics of menstrualbleeding, such as the colour, composition andodour of the loss. For many women, disruptionsin menstrual bleeding have perceived implicationsfor health and fertility. However, it is not widelyrecognized that spontaneous disturbances of men-strual patterns are quite common at all ages. Manywomen accept and tolerate these well, providedthat serious pathology has been excluded and thatdisturbances are of limited duration.
Ovulatory dysfunctional uterine bleeding
Clinical characteristics and endocrinology
This condition is characterized by excessive men-strual bleeding (usually very heavy), usually at
fairly regular intervals and with a pattern of dailymenstrual loss similar to normal menses, with~90% of the flow occurring during the first 3 days(Haynes et al., 1979). The onset of bleedingcoincides with oestradiol and progesterone with-drawal during luteolysis, and the circulating pituit-ary and gonadal hormone patterns during thepreceding 4 weeks are indistinguishable from nor-mal (Haynes et al., 1979; Eldred and Thomas,1994).
Endometrial morphology and tissue breakdown
Normal menstruation involves the breakdown,remodelling and repair of the functional endomet-rial layers, and there is some evidence that disrup-tions of this process at a number of stages mayresult in changes in the quantity and pattern ofmenstrual loss. Endometrial destruction and regen-eration are largely controlled by local factors,although the initial trigger comes from fallingoestradiol and progesterone concentrations follow-ing luteolysis. Lysosomes release hydrolyticenzymes in pre-menstrual endometrium that appearto contribute to tissue breakdown, bleeding, remod-elling and subsequent regeneration (Henzl et al.,1972; Christiaens etal, 1982). These organelles aresensitive to falling concentrations of progesterone,and it is unclear whether they have a primary orsecondary role in the onset of endometrial men-strual breakdown. Endometrial lysosomal enzymeactivity in women with ovulatory DUB is increased,and this activity is also observed in women withmenorrhagia secondary to intrauterine device(IUD) use (Wang, 1994). Matrix metalloproteinases(MMP) also act to degrade most components of theextracellular matrix and are regulated by ovariansteroid hormones (Rodgers et al., 1994). Excessiveor prolonged tissue degradation due to MMPactivity could result in increased or prolongedmenstrual bleeding. Certain MMP are stronglyexpressed in menstrual endometrium (Salamonsen,1996). There is also recent evidence consistentwith the hypothesis that decreasing concentrationsof progesterone result in a fall in the endometrialtissue concentrations of neutral endopeptidase (aglycosylated zinc metallopeptidase capable ofinactivating a number of endocrine and paracrinepeptides) and a consequent rise in tissue concentra-
166
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from

Mechanisms underlying disturbances of bleeding
tions of locally synthesized endothelins which maybe responsible for the vasoconstriction leading tothe onset of tissue breakdown. This release ofendothelins may be attenuated in ovulatory DUB(Marsh, 1996).
Endometrial leukocytes are known to beinvolved in tissue destruction and regeneration. Inthe normal menstrual cycle there is a substantialpre-menstrual increase in endometrial stromalgranulated lymphocytes, T lymphocytes andmacrophages. Polymorphonuclear leukocytes onlyappear in uterine tissues at the onset of menstru-ation (Kamat and Issacson, 1987; Buhner et aL,1988), and are often located near blood vesselsin the endometrium, where they may influencevascular permeability and integrity. Polymorphsalso appear in focal endometrial necrosis associatedwith high-dose progestogens (Song et aL, 1996).This influx of leukocytes into human endometriumis clearly influenced by changes in circulating (ortissue) steroid concentrations, especially progester-one and progestogens, and small populations ofthese cells have varying oestradiol and/or proges-terone receptor positivity (Tabibzadeh andSatyaswaroop, 1989).
Granulated stromal lymphocytes, macrophagesand other migratory leukocytes may be implicatedin the control of menstrual blood loss (MBL) andcontribute to mechanisms of excessive loss. Anexcessive leukocyte infiltrate has been associatedwith the copper IUD (Sheppard, 1987). Macro-phages may release platelet-activating factor (PAF)and prostaglandin (PG) E, both of which are potentvasodilators that could augment MBL. Mast cellsmay also secrete a range of vasoactive substances.
Endometrial vascular morphology, function andhaemostasis
There is a large body of evidence to implicate anumber of endometrial vascular and haemostaticabnormalities in the bleeding disturbances occur-ring with ovulatory DUB. The observations ofMarkee (1940) suggest that normal menstrualbleeding arises predominantly from the spiralarterioles, and is under the control of ovariansteroid hormones. The pattern of excessive men-strual bleeding in ovulatory DUB suggests that thebleeding site may also be arteriolar, but with a
change in the local control of endometrial bloodflow and haemostatic mechanisms. There is littleevidence that spiral arteriole morphology or density(Rees et aL, 1984) are altered in ovulatory DUB,but there may be an increase in the numbers ofsmall veins in the deep endometrium and innermyometrium (Houlihan et aL, 1989). Ovarian ster-oid hormones are known to have vasoactive effects,and the vessels of the functional layer of theendometrium show marked sensitivity to theirinfluence (Fraser and Peek, 1992). Oestrogencauses a fall in uterine vascular resistance and anincrease in endometrial blood flow (Fraser et aL,1987). This effect is lost with the appearanceof progesterone. The influence of oestrogen andprogesterone on the endometrial vasculatureappears to be by direct receptor-mediated effectson the arteriolar and venular musculature or bylocal mediators because receptors have not beendemonstrated on the endothelial cells in the func-tional layer (Perrot-Applanat et aL, 1988). Theactions of ovarian steroid hormones may be potenti-ated in DUB by the release of various localmediators through an increase in endometrial oes-trogen (ER) and progesterone receptors (PR) inglandular and stromal tissue (Gleeson et aL, 1993),but endometrial oestrogen and progesterone recep-tor expression is indistinguishable from normal inwomen with menorrhagia (Critchley et aL, 1994).
In women with ovulatory DUB there is a signi-ficant increase in endometrial blood flow comparedwith normal, and this is seen during the period ofraised oestradiol secretion in the foUicular phase(Fraser etal., 1987). There is a subsequent decreasein flow in the secretory phase, with a late premen-strual rise equivalent to that seen in normal cycles.It is unclear whether the increased endometrialflow in the follicular phase has any direct influenceon MBL. Blood flow within the endometriumduring days 1 and 2 of menstruation is probablyunder the control of complex local mechanisms,but these may be influenced by vascular changesearlier in the cycle.
The control of menstrual bleeding relies to aconsiderable extent on the timely and adequateconstriction of bleeding vessels. PG and endothel-ins appear to be powerful vasoactive substances inthe control of MBL, and their production is
167
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from

LS Jraser, M.Hlckey and J.-y-Song
regulated by circulating oestrogen and progesteroneconcentrations (Cameron et al, 1987; Smith andKelly, 1987). Ovulatory DUB is associated with ashift in the ratio of endometrial vasoconstrictingPGFza to vasodilatory PGEj (Smith et al, 1982)and an increase in the total endometrial concentra-tion of PG (Cameron et al, 1987). Smith et al.(1981) have also shown that there is an increasedcapacity for myometrial generation of prostacyclin(PGI2) from endometrial precursors in ovulatoryDUB. PGI2 is a vasodilatory PG and is a potentinhibitor of platelet aggregation. Endometrial tis-sues may also be more responsive to the action ofother vasodilatory PG (PGEJ via increased recep-tor concentrations in women with menorrhagia(Adelentado et al, 1988). Successful treatment ofovulatory DUB with PG synthetase inhibitors leadsto a reduction in endometrial concentrations ofPGF^ and PGE2 (Fraser, 1983b), and inhibits thebinding of PGE to its receptor (Rees et al, 1988).
Endothelins, located predominantly at the endo-metrial-myometrial junction (Cameron et al,1992), act as powerful vasoconstrictors and areresponsive to ovarian steroid concentrations(Maggi et al, 1991). Tissue endothelin concentra-tions may interact with relaxing factors such asendothelium-derived relaxing factor (EDRF), alsoknown as nitric oxide (NO; Goetz et al, 1988).Disrupted patterns of endothelin production mayprolong or increase MBL, either directly or viaNO production, and recent evidence suggests thatendothelin concentrations in the endometrium ofwomen with ovulatory DUB may be depressedsubstantially (Marsh, 1996).
Active fibrinolysis within the normal endomet-rium and uterine cavity prevents organized clotformation and the development of intrauterineadhesions. The 'defective' haemostasis seen innormal menstruation may be exaggerated in ovulat-ory DUB. Vascular plugs are loose and locatedinside vessels, and reduced fibrin concentrationsmake them unstable (Sheppard, 1990). OvulatoryDUB is associated with an increase in endometrialfibrinolysis (Rybo, 1966), and an increased concen-tration of tissue plasminogen activator (tPA) hasbeen observed in these women (Kasonde andBonnar, 1976). Overacu'vation of these fibrinolyticmechanisms may 'unbalance' the haemostatic sys-
tem, causing early breakdown of thrombi in theendometrial vessels and excessive blood loss.Excessive oestrogen stimulates fibrinolysis, andprogesterone inhibits this process by creating adecidual reaction with an increased concentrationof endogenous fibrinolytic inhibitors (Cassldn andAstedt, 1983). Mast cells may also play a role inthe defective haemostatic process. They have beenshown to degranulate pre-menstrually to secreteheparin, histamine and other substances(Salamonsen, 1996). Heparin stimulates endomet-rial fibrinolysis via the secretion of tPA, andhistamine causes endothelial cell contraction, creat-ing gaps between vascular endothelial cells toallow increased vascular fluid loss. In DUB, thesecretion of heparin-like substances is increased(Foley et al, 1978). There are also probablylocal effects on platelet function, preventing theirefficient aggregation, and the most likely candidatefor this role is the excessive generation of myometr-ial prostacyclin, demonstrated in ovulatory DUBby Smith et al. (1981).
Endometrial repair
For menstrual bleeding to cease, there must berepair of the epithelium and vascular endotheliuminitiated from the remaining basal layers of endo-metrium. Local factors are likely to play a centralrole in this reparative process. This aspect ofendometrial function may be disrupted in thosewomen with ovulatory DUB associated with pro-longation of bleeding, although it is probably intactin the majority who present with mehorrhagia(and normal patterns of menstrual loss). There isevidence that endometrial repair processes areconsiderably delayed following curettage, whichsuggests that under normal circumstances cellsor cellular products from residual areas of thefunctional layer are important in normal endomet-rial remodelling and repair (Johannisson et al.,1981). This makes it likely that regrowth fromthe basal layer alone is much less efficient, andexcessive shedding could have an impact on therate of regeneration.
During normal menstruation the superficialendometrial layers are lost and major endometrialremodelling occurs. Regeneration begins within24 h and is complete within 4-5 days of the
168
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from

Mechanisms underlying disturbances of bleeding
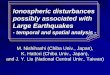
Figure 1. A putative scheme of interactions withinendometrium during menstruation. Disturbance of any ofthese mechanisms could potentially play a role in the rangeof different clinical disorders of menstruation (modified fromFraser, 1990). Key: MMP - matrix metalloproteinases; NEP -neutral endopeptidase; PLA2 - phospholipase A2; PGFj, -prostaglandin F2,; PGE2 - prostaglandin E2; eGL -endometrial granulated lymphocytes; PMNL -polymorphonuclear leucocytes; EDRF - endothelium-derivedrelaxing factor (nitric oxide); E2 - oestradiol; b-FGF - basicfibroblast growth factor, VEGF - vascular eodotheUal growthfactor.
onset of menstruation (Ferenczy, 1976a,b). Growthfactors in the endometrium may be crucial to thespeed and efficacy of the reparative process. Thesecretion of potent endometrial growth factors,such as vascular endothelial growth factor (VEGF),basic fibroblast growth factor (bFGF) and epi-dermal growth factor (EGF), is influenced bycirculating ovarian steroid hormones (Smith, 1990),although it is unclear how important any directeffect of oestradiol may be on epithelial prolifera-tion and repair in this situation. In DUB, delayedor incomplete endometrial repair could prolongmenstrual bleeding episodes, but nothing is knownabout such mechanisms. Cyclical angiogenesis in
the functional layer could be disrupted in DUB,such that new vessels fail to respond to the normalcontrol mechanisms of vasoconstriction and regen-eration. This may be more important in anovulatoryDUB. It is not known whether there are anysubtle disturbances of endometrial angiogenesis inovulatory DUB, although major disturbances couldnot be demonstrated (Peek et al, 1995a).
Anovulatory dysfunctional uterine bleeding
Clinical characteristics and endocrinology
This condition tends to be characterized by unpre-dictable, irregular, prolonged and/or excessivelyheavy episodes of bleeding. It is much morecommon at the extremes of reproductive life andis the only type of DUB widely acknowledged inthe USA (Allen-Davis and Schlaff, 1995). Manyperi-menopausal women will experience anovula-tory cycles interspersed with ovulatory or defectiveovulatory cycles, which makes their menstrualexperience quite unpredictable (Fraser, 1996). Thetype of bleeding that occurs after a particularanovulatory cycle will depend on the endometrialeffect of the peak, duration and rate of declineof serum oestradiol concentrations, and excessivebleeding is often associated with simple hyperplas-tic changes in the endometrium. Bleeding maybe light and intermittent, with lowish oestradiolconcentrations and proliferative endometrium, andwithdrawal bleeding may even not occur at all ifoestrogen withdrawal is gradual (Corner, 1942).Bleeding can occur at any time endocrinologicallyspeaking (when oestradiol concentrations are fal-ling, stable or even rising) from endometriumexposed to increased and unopposed oestradiolconcentrations (Brown et al, 1959; Fraser, 1976).In women with anovulatory DUB, the types ofoestrogen secreted by the ovaries are normal andtheir metabolism is also normal, but the pattern ofsecretion is greatly disturbed (Fraser and Baird,1974). Inappropriately high and fluctuating concen-trations of oestradiol and oestrone are secreted bymultifollicular ovaries (Schroder, 1954; Fraser andBaird, 1974), suggesting a primary disturbance ofintra-ovarian folh'cular control mechanisms or amarked disturbance of hypothalamic-pituitarygonadotrophin control.
169
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from

I-S-Fraser, MJIkkey and J.-y.Song
Endometnal morphology and breakdown
Major changes are seen in endometrial morphologyin women with simple hyperplasia as a con-sequence of excessive and unopposed ovarianoestradiol secretion (Schroder, 1954). This clinicalpicture can be so dramatic that it was knownpreviously as 'metropathia haemorrhagica',although it is now recognized as merely one endof the spectrum of severity of anovulatory DUB.In these women, the endometrium appears to breakdown erratically and unevenly in different parts ofthe cavity. SchrSder (1954) found scattered 'redpatches corresponding to thrombotic foci of nec-rotic disintegration' throughout the abnormallyproliferated tissue, even in women who were notbleeding at the time of examination. These necroticpatches were detected in up to 87% of endometrialspecimens from women with hyperplasia. Theborders of the necrotic tissue were usually sharplydefined from intact proliferative tissue, but therewere few histological signs of any tissue interactionat the interface.
Endometrial vascular morphology, function andhaemostasis
Hysteroscopic studies frequently demonstrate thepresence of large, thin-walled tortuous and fragilesuperficial endometrial vessels in women withhyperplasia or carcinoma, and these vessels maybe much larger than those commonly seen inprogestogen-only users.-. These abnormal vesselsare probably a key part of the aetiology of veryheavy bleeding in these women, although one alsohas to postulate a mechanism leading to trauma,other types of damage or excessive fragility of thevascular endothelium and overlying epitheliumin order for bleeding to begin. In hyperplasticendometrium, the growth of spiral arterioles issuppressed and the density of venous drainagewithin the inner myometrium is greatly increased(Beilby et al., 1971). These may both be morpholo-gical changes which interfere with normal vascularcontrol mechanisms.
Little is known about disturbances in the localendometrial environment that may lead to irregularmenstrual bleeding in anovulatory DUB. Endomet-rial blood flow rates are variable but tend to behigher than normal (Fraser et al., 1987). This may
reflect the oestrogen dominance in anovulatorycycles. In persistently proliferative endometrium,arachidonic acid availability is reduced and overallPG production is impaired (Smith et al, 1982).An imbalance in PG activity may alter vasculartone, endometrial blood flow and haemostatic func-tion. Without coordinated vasoconstriction anddilatation, patterns of menstrual bleeding are likelyto be disrupted. As yet, there is no information onthe possible role of endothelins in anovulatoryDUB. Information on fibrinolytic activity is lim-ited, but this activity may well be increased. Thereis recent evidence to suggest that endometrial nitricoxide (the endothelium-derived relaxing factor)release may be stimulated by oestrogen, and thiscould be part of the mechanism of increasedbleeding with anovulatory DUB.
Endometrial repair
Virtually nothing is known specifically about theendometrial events during recovery from an epis-ode of anovulatory bleeding. It is assumed thatincreased oestradiol concentrations will have asubstantial impact on the rate of surface repairand may sometimes lead to the development ofhyperplastic endometrium within a few days of anepisode of bleeding. The involvement of othergrowth factors is unknown.
Progestogen-related BTB mechanisms
Three previous symposia have been organized inthe last 17 years by the Special Programme ofResearch, Development and Research Training ofthe World Health Organization (the third beingorganized jointly with the National Institutes ofHealth, Washington, DC, USA) to address the issueof abnormal bleeding associated with the use oflong-acting hormonal contraceptives (Diczfalusyet al, 1980; d'Arcangues et al, 1990; Alexanderand d'Arcangues, 1992). A study of these threepublications demonstrates the extent of the progressthat has been made during this time in understand-ing the mechanisms of normal and abnormal men-struation. It also demonstrates the relative lackof progress that has been possible in the actualprevention and treatment of these bleeding disturb-ances. Nevertheless, the amount of progress made
170
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from

Mechanisms underlying disturbances of bleeding
Table L Effects within the endometrium contributing to progestogen-related breakthrough bleeding (BTB)
1 Need for some local oestrogen effect (BTB does not occur with true atrophy)2 Development of abnormally thin-walled and sometimes dilated superficial vessels (neovascularization)3 Development of increased vascular fragility
possible effect of minor trauma (uterine movement and contractions)leading to focal bleeding from thin-walled vessels
4 Focal release of destructive moleculesdamage to endothelium, leading to subepitbelial bleedsdamage to epithelium, landing to microbleeds and frank bleeding
5 Disturbances of vasoconstriction and haemostasisleading to effects on volume of menstrual flow
6 Disturbances of epithelial and endothelial repairleading to prolongation of bleeding
7 Other factors influencing local conditions within the endometrium include missed oral contraceptive pills, druginteractions and chlamydial cervicitis/endometritis
in understanding mechanisms is encouraging forfuture developments aimed at solving the clinicalproblems.
Clinical characteristics and endocrinology
BTB is generally worst during the first few monthsafter starting progestogen-only contraceptive use,and bleeding patterns then improve in the longterm. With methods like depot medroxyproges-terone acetate, amenorrhoea and oligomenorrhoeaare then common, while Norplant® users tend todevelop more regular patterns with average flow.Users of the intrauterine levonorgestrel-releasingsystem (Levonova®, Mirena®; Leiras, Finland) tendto develop extremely light but regular bleeds. Theinitial erratic episodes of bleeding common withthese methods are related to changes which occurin the endometrium, and do not generally correlatewith fluctuations in serum concentrations of endo-genous or exogenous steroids. Increasing evidencesuggests that a continuing low level oestrogeninfluence and a continuous progestogen exposureon the endometrium are necessary to allow erraticBTB to begin and be maintained (Table I). Otherfactors then come into play.
Increasing evidence suggests that a certain lim-ited amount of oestrogen effect within the endomet-rium, in addition to continuous progestogenexposure, is necessary for BTB to occur. In condi-tions close to complete histological atrophy, amen-orrhoea is the rule and BTB does not occur.As the continuous progestogen effect becomesincreasingly established with continued exposure,BTB generally becomes less and less. Those Norpl-
ant users with BTB tend to have higher circulatingconcentrations of oestradiol than those without.On the other hand, higher relative concentrationsof oestrogen will 'stabilize' the endometrium andminimize the incidence of BTB, as seen in com-bined oral contraceptive pill users. Even in pillusers with a fixed oestrogen-progestogen ratio,there is a significant incidence of BTB with pro-longed continuous use. It is likely that the localexpression of oestrogen and progesterone receptorsin different cell types within endometrium will turnout to be important in determining the conditionsnecessary for BTB to occur (Critchley et al, 1993;Lau and Rogers, 1996).
Any factor that interferes with the relativelyconstant circulating concentrations of contraceptivesteroids in users of long-acting methods, such asdrug interactions with rifampicin or anticonvuls-ants, may cause BTB. Local damage to the endo-metrial surface with superficial endometritis (orto the cervix with cervicitis) may also lead tounpredictable spotting.
Endometrial morphology and breakdown
Numerous authors have described the histologicalchanges that may occur in endometrium exposed tovarying concentrations of continuous progestogenexposure, but the simple message is that no particu-lar histological pattern appears to correlate withthe occurrence of BTB (Ober, 1970; Johannisson,1980; Maqueo, 1980). Only the development ofapparent extreme histological atrophy predicts aparticular menstrual pattern — amenorrhoea. Endo-metrial breakdown during BTB is probably patchy,
171
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from

L&Fraser, M.Hlckey and J.-y^ong
and bleeding is thought to occur from isolatedareas rather than uniformly across the whole endo-metrial surface.
Endometrial vascular morphology, function andhaemostasis
In progestogen-exposed endometrium there is areduction in spiral arteriole numbers and size withsubstantially reduced spiralling (Hourihan et al,1986). Microvascular density is increased by>50% (Rogers et al., 1993), endothelial gapsappear (Hourihan et al., 1991) and there is anincrease in the number of endothelial plasma-lemmal vesicles and contracted endothelial cells(Johannisson et al, 1982). Recently, hysteroscopicinspections have demonstrated scattered surfaceneovascularization in arborization patterns from acentral stem in women with BTB during Norplantuse (Hickey et al., 1996). Thin-walled, enlargedand apparently dilated surface vessels sometimesappear (Ober, 1970; Maqueo, 1980; Hourihan et al,1991; Song et al, 1995). Their significance hasbeen uncertain because they frequently do notcontain red cells on histological examination, andit is difficult to assess vascular dilatation in vitroas the vessels rapidly collapse (Rogers et al, 1993).However, recent in-vivo hysteroscopic examina-tions have demonstrated that these vessels (appar-ently thin-walled venules) are common on thesurface of the endorrietrium of women with BTBusing Norplant (Hickey et al, 1996). Currentevidence suggests that BTB originates from thesefragile superficial venules and the scatteredneovascular arborizations. Recent evidence,pointing to an increase in the expression of VEGFin Norplant-exposed endometrium, could be anexplanation for the appearance of these abnormalvessels (Smith, 1996).
There has been suspicion for some time of anincrease in the fragility of endometrial vessels inlong-acting progestogen users (Sarfati and Brux,1973; Fraser and Diczfalusy, 1980), but it has beenpossible to confirm this only recently by directhysteroscopic inspection of the endometrium(Hickey et al, 1996). The mechanism of thismarkedly increased fragility is not known, butcould be caused by subtle changes in basementmembrane structure, intercellular tight junctions,
intercellular adhesion molecules or integrity ofthe perivascular supporting structures. Endothelialgaps appear to be more common in progestogenusers (Shaw et al, 1981), suggesting that theloss of integrity of intercellular junctions may bethe culprit.
The destructive processes that result in normalbreakdown of the superficial endometrium at theonset of menstruation probably also play a part inthe erratic breakdown associated with BTB. Forabnormal bleeding to occur, there must be focalor generalized breakdown of both endothelial andepithelial layers, but it is not clear whether thisoccurs simultaneously in a coordinated fashion orif subepithelial bleeding leads to disruption of theoverlying epithelial layers. It is probable thatvarious different mechanisms are activated underdifferent circumstances, and that matrix metallo-proteinases (and their tissue inhibitors), lysosomes,free oxygen radicals, migratory white cells, cyto-kines and their regulatory systems may all beinvolved. Some MMP are intensely expressed innormal menstrual endometrium, but informationon their role in BTB is lacking (Courtoy, 1996;Salamonsen, 1996). Similarly, lysosomes play arole in normal menstruation, but their involvementin BTB is unclear. There is some evidence toconfirm an increase in the endometrial releaseof enzymes, like N-acetyl-|J-hexosaminidase, onprolonged exposure to levonorgestrel (Comillieet al, 1991). Free oxygen radical release has notbeen studied in progestogen-exposed endometrium.
The concentration of several types of migratoryleukocyte increases in progestogen-exposed endo-metrium (Booker et al, 1994; Song et al, 1996),with the potential for release of a range of destruct-ive as well as angiogenic and repair molecules.These leukocytes consist mainly of T-lymphocytes,endometrial granulated lymphocytes and macro-phages, although polymorphonuclear leukocyteconcentrations also increase when tissue necrosisor breakdown occurs (Song et al., 1996). There isno evidence of changes in mast cell function duringprogestogen-exposed cycles (Hourihan et al,1991), but more sensitive techniques may be neces-sary to confirm this. The actual role of each ofthese leukocyte types remains to be elucidated.
The role of endometrial vascular constriction and
172
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from

Mechanisms underlying disturbances of bleeding
dilatation in BTB is unknown, although arachidonicacid metabolism and endothelin expression appearto be disturbed in the endometrium of progestogenusers (White et al, 1991; Marsh, 1996). Thereappears to be a reduction in the endometrial secre-tion of cyclo-oxygenase enzyme products, whichis more than offset by an increase in the releaseof cytochrome-P450 epoxygenase products (Whiteet al, 1991). Both epoxide and hydroxyeicosatetra-enoic acid (HETES) release correlated with thenumber of bleeding days in long-term levonorges-trel users. An increase in prostaglandin epoxidesmay cause vasodilatation, and both epoxides andHETES may inhibit platelet aggregation while adecrease in endothelin expression may also leadto vasodilatation (Marsh, 1996). As yet, there isno information on the possible role of nitric oxideor other vasoactive substances in BTB.
Little information exists concerning possiblechanges in haemostatic mechanisms within theendometrium, although intravascular platelet andhaemostatic plugs appear to be more common inprogestogen users (Houlihan et al., 1986) andfibrinolytic activity is reduced. Immunostainingintensity for Von Willebrand Factor VHI-relatedantigen is increased in endometrial capillary endo-thelium of Norplant users, but the significance isunclear (Au and Rogers, 1993). There is also recentevidence for an increase in endometrial stromaland periglandular expression of angiotensin, whichmay relate to changes in vascular function orgrowth (Li, 1996).
Endometrial repair
The observation that episodes of progestogen-related BTB may be prolonged and frequent sug-gests that endometrial repair mechanisms may bedefective in this situation, although there is verylittle direct evidence to confirm this. Wonodireksoet al. (1993) have found the superficial endometrialepithelium to be absent in some of their Norplantusers, with evidence of defective cytokeratin ele-ments in the epithelial cytoskeleton of those womenin whom epithelium is present. There is very littleinformation available on the role of various growthfactors in normal or abnormal endometrial repairin these women.
Angiogenesis is the process of growth of new
blood vessels from existing vessels, and is anintegral part of the cyclical repair and regenerationprocess of normal endometrium. Using the partiallyspecific marker, proliferating cell nuclear antigen,Goodger et al. (1994) found evidence of reducedendothelial proliferation in women exposed toNorplant in whom endometrial microvascular den-sity was already increased (Rogers et al, 1993).The observation that growth of endometrial capil-lary endothelial cells exposed to certain syntheticprogestogens in culture is markedly inhibited mayalso be an indicator of impaired angiogenic mech-anisms (Peek et al., 1995b). Evidence of increasedVEGF in Norplant-exposed endometrium could bean explanation for the appearance of abnormalvascular morphology in these cases (Smith, 1996).As yet, there is no information on the possibleroles of different angiogenic, anti-angiogenic andother regulatory molecules that might be involvedin these apparently defective repair processes.
A comparison of the features of ovulatory andanovulatory DUB and progestogen-related BTB
An attempt has been made in Table II to compareand contrast some of the features that relate tospontaneous ovulatory and anovulatory DUB andto hormonal contraceptive-related BTB. A quickglance shows that there are substantial differencesbetween the three situations and that underlyingmechanisms of disturbed bleeding are probablyquite different. The number of molecules andpotentially interlinked molecular systems is solarge that there are almost certainly a number of'fail-safe' mechanisms within the endometriumcapable of reacting to change in other systems.Several abnormal interactions may sometimes benecessary before abnormal bleeding actuallyoccurs. Different interactions will lead to differentpatterns of abnormal bleeding. It would also be ofinterest to compare molecular mechanisms andvascular function in endometrium from womenwith spontaneous amenorrhoea to gain furtherinsights into features that may 'stabilize' the endo-metrium and its vasculature.
Conclusions
Mechanisms of abnormal menstrual bleeding areinfluenced by endogenous and exogenous steroid
173
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from

LS Jraser, MJilckey and J.-y.Song
Table IL Comparison of features of ovulatory and anovulatory dysfunctional uterine bleeding (DUB) and progestogen-associated breakthrough bleeding (BTB)
1234
5
678
91011
121314
15
1617
181920
21222324
Cycle bleeding patternPattern of daily menstrual lossMeasured menstrual blood lossHormone environment
Association with hormonalwithdrawalEndometrial blood flowOrigin of bleedingEndometrial histology
CytoskeletonSteroid receptor changesEndometrial vascular
morphology
Vascular fragilityVascular basement membraneEndothelial intercellular
junctionsLeukocytes (various)
Prostaglandins (PG)Endothelium-derived relaxing
factorVasoconstrictors — endothelinsEndometrial angiotensinVascular endothelial growth
factorLysosomal enzymesMatrix metalloproteinasesFibrinolytic activityEndometrial repair mechanisms
Ovulatory DUB
RegularNormalHeavyNormal menstrual cycle
Yes
Folh'cular phase increaseArteriolirNormal
UnknownUnknown7 Normal, minor anomalies
of small veins
NormalUnknown7 Normal
Increased
t PGEz, T PGI2
7 Normal
DecreasedUnknownUnknown
Some increaseUnknownIncreasedNormal
Anovulatoty DUB
IrregularProlongedHeavyHigh unopposed oestrogen
Usually
Variable increaseVenous/capillaryProliferative or hyperplastic
UnknownUnknown•I Arterioles, t distorted
thin-walled vessels
IncreasedUnknownUnknown
Unknown
•I PGEz, -1- PGI27 Increased
?DecreasedUnknownUnknown
UnknownUnknown? Increased? Abnormal
BTB
IrregularProlongedReducedContinuous progestogen
exposure.varying oestradiolSometimes
UnknownCapillary/venousSuppressed secretion or
atrophyMinor changesComplex4- Arterioles, T endothelial
structures, T thin-walledsuperficial dilated vessels
Increased7 Normal7 Decreased
Increase in EGL,macrophages, T cells
T PG epoxides, 7 other PG 1Unknown
VariableIncreasedIncreased
Subtle changesUnknown7 Suppressed7 Abnormal
EGL = endometrial granulated lymphocyte.
hormones, but their action is almost certainlymediated via a range of local endometrial factorson the endometrial vasculature. The bleeding sitein hormone-induced BTB may differ from that ofnormal menstrual bledding and excessive menstrualbleeding in both types of DUB. A capillary bleed-ing site for BTB may explain the observed charac-teristic pattern of prolonged and frequent lightbleeding.
Endometrial capillaries or their supporting struc-tures may be altered following exposure to exogen-ous steroid hormones, particularly long-actingprogestogen-only preparations, and this may leadto increased vascular fragility. The endothelialbasement membrane may be structurally or func-
tionally disrupted by prolonged progestogen expo-sure, allowing changes in vascular morphology(such as dilatation) and leakage of erythrocytes,causing BTB. Intercellular integrity may be com-promised by prolonged progestogen exposure, withthe disruption of endothelial (and epithelial) celltight junctions and diapedesis of erythrocytes.Epithelial integrity and mechanisms of repair maybe altered following exposure to steroid contracept-ives, such that blood loss from 'fragile' endometrialvessels escapes through the epithelium as BTB.These vessels may also be abnormal in size,structure and function. The addition of oestrogensafter prolonged progestogen exposure may promoteepithelial repair and limit endothelial bleeding.
174
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from

Mechanisms underlying disturbances of bleeding
Endometrial breakdown and repair are controlledby a wide variety of local substances, whichare influenced by circulating concentrations ofexogenous and endogenous steroid hormones. Dis-turbances in the concentrations and interactions ofthese factors are likely to be involved in changesin menstrual bleeding patterns. The roles of thosefactors affecting vascular integrity may be ofparticular importance in the genesis of BTB. Agreater understanding of these mechanisms willundoubtedly lead to improved ideas for the preven-tion and management of the various bleedingdisturbances. For example, it may be possible todesign a small biodegradable uterine implant thatcould release continuous low concentrations of anappropriate substance to counteract a particularmolecular disturbance. These could be designedfor different dosages and durations of action, oreven to release combinations.
ReferencesAdelentado, J.M., Rees, M.C.P., Lopez BemaL A. and
Tumbull, A.C. (1988) Increased uterine prostaglandinE receptors in menorrhagic women. Br. J. Obstet.Gynaecol, 95, 162-165.
Alexander, NJ. and d'Arcangues, C. (1992) Steroid. Hormones and Uterine Bleeding. AAAS Press,
Washington, DC, USA.
Allen-Davis, J.T. and Schlaff, W.D. (1995) Dysfunctionaluterine bleeding, polyps and fibroids. In Metzger, D.A.(ed.). The Endometrium. Infertility and ReproductiveMedicine Clinics of North America, Vol. 6, pp. 401-415. W.B. Saunders, Philadelphia, PA, USA.
Au, C.L. and Rogers, P.A.W. (1993) Immuno-histochemical staining of von Willebrand factor inhuman endometrium during the normal menstrualcycle. Hum. Reprod., 8, 17-23.
Beilby, J.O.W., Fairer-Brown, G. and Tarbit, M.H. (1971)The microvasculature of common uterineabnormalities, other than fibroids. J. Obstet. GynaecolBr. Commonwealth, 78, 361-368.
Belsey, E.M. and Task Force on Long-Acting SystemicAgents tor Fertility Regulation (1988) The associationbetween vaginal bleeding patterns and reasons fordiscontinuation of contraceptive use. Contraception,38, 207-235.
Booker, S.S., Jayanetti, C , Karalak, S. et al (1994)The effect of progesterone on the accumulation ofleucocytes in the human endometrium. Am. J. Obstet.Gynecol, 171, 139-142.
Brown, J.B., Kellar, RJ. and Matthew, G.D. (1959)
Urinary oestrogen excretion in certain gynaecologicaldisorders. J. Obstet. Gynaecol Br. Empire, 66, 177-211.
Bulmer, J.N., Johnson, ?M. and Bulmer, D. (1987)Leucocyte populations in human decidua andendometrium. In Gill, TJ. and Wegmann, TJ. (eds),Immunoregulation and Fetal Survival OxfordUniversity Press, Oxford, UK, pp. 111-134.
Cameron, I.T. (1989) Dysfunctional uterine bleeding.BaiUere's Clin. Obstet. Gynecol, 3, 315-328.
Cameron, I.T., Leask, R., Kelly, R.W. and Baird, D.T.(1987) Endometrial prostaglandins in women withabnormal menstrual bleeding. Prostaglandins,Lcukotrienes Med., 29, 249-258.
Cameron, I.T, Davenport, A.P., van Papendorp, C.et al. (1992) Endothelin-like reactivity in humanendometrium. J. Reprod. FertiL, 95, 623-628.
Casslen, B. and Astedt, B. (1983) Reduced plasminogenactivator content of endometrium in oral contraceptiveusers. Contraception, 28, 181-188.
Christiaens, G.C.M.L., Sixma, JJ. and Haspels, A.A.(1982) Hemostasis in menstrual endometrium: areview. Am. J. Reprod. Immunol, 5, 78-83.
Corner, G.W. (1942) The Hormones in HumanReproduction. Princeton University Press, Princeton,NJ, USA.
Cornillie, F., Brosens, I., Belsey, E.M. et al (1991)Lysosomal enzymes in the human endometrium: abiochemical study in untreated and levonorgestrel-treated women. Contraception, 43, 387-400.
Coulter, A., Noone, A. and Goldacre, M. (1989) Generalpractitioner's referrals to specialist outpatient clinics.Br. Med. J., 299, 304-308.
Courtoy, P.J. (1996) Hormonal control of matrixmetalloproteinase activity in the human endometrium:studies on fresh and cultured tissue. Hum. Reprod,11, in press.
Critchley, H.O.D., Bailey, D.A., Au, C.L. et al (1993)Immunohistochemica] sex steroid receptor distributionin endometrium from long-term subdermallevonorgestrel users and during the normal menstrualcycle. Hum. Reprod, 8, 1632-1639.
Critchley, H.O.D., Abberton, M.M., Taylor, N.H. et al(1994) Endometrial sex steroid receptor expression inwomen with menorrhagia. Br. J. Obstet. Gynaecol,101, 428-434.
Diczfalusy, E., Fraser, I.S. and Webb, F.T.G. (1980)Endometrial Bleeding and Steroidal Contraception.Pitman Press, Bath, UK.
Eldred, J.M. and Thomas, EJ. (1994) Pituitary andovarian hormone levels in unexplained menorrhagia.Obstet. Gynecol, 84, 775-778.
Ferenczy, A. (1976a) Studies on the cytodynamics ofhuman endometrial regeneration. I. Scanning electronmicroscopy. Am. J. Obstet. Gynecol, Y2A, (A-14.
175
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from

LS.Fraser, M.Hlckey and J.-y.Song
Ferenczy, A. (1976b) Studies on the cytodynamicsof human endometrial regeneration, n. Transmissionelectron microscopy and histochemistry. Am. J. Obstet.Gynecol, 124, 582-595.
Foley, M.E., Griffin, B.D. and ZugeL M. (1978) Heparin-like activity in uterine fluid. Br. Med. J., 11, 322-324.
Fraser, LS. (1976) Clinical manifestations and end-organ effects associated with abnormal gonadotrophinrelease. Clin. Obstet. Gynecol, 3, 591-614.
Fraser, LS. (1983a) A survey of approaches tomanagement of menstrual disturbances in womenusing injectable contraceptives. Contraception, 28,385-397.
Fraser, LS. (1983b) The treatment of menorrhagia withmefenamic acid. Res. Clin. Forums, 5, 93-99.
Fraser, LS. (1989) Treatment of menorrhagia. Baillere'sClin. Obstet. Gynecol, 3, 391-402.
Fraser, I.S. (1990) Towards a better understanding ofthe effects of progestogens on the mechanisms ofendometrial bleeding: recommendations for research.In: D'Arcangues, C , Fraser, I.S., Newton, J.R. andOdlind, V. (eds), Contraception and EndometrialBleeding. Cambridge: Cambridge University Press,pp. 491-520.
Fraser, I.S. (1996) Menstrual changes during theperimenopause. In Lobo, R. (ed.), The Perimenopause.Serono Symposium, Norwells, MA, USA, in press.
Fraser, I.S. and Baird, D.T. (1974) Blood production andovarian secretion rates of estradiol-17[$ and estrone inwomen with dysfunctional uterine bleeding. J. Clin.Endocrinol. Metab., 39, 564-570.
Fraser, I.S. and Diczfalusy, E. (1980) A perspective ofsteroidal contraception and abnormal bleeding: whatare the prospects for improvement? In Diczfalusy, E.,Fraser, I.S. and Webb, F.T.G. (eds), EndometrialBleeding and Steroidal Contraception. Pitman Press,Bath, UK, pp. 384^13.
Fraser, I.S. and Peek, MJ . (1992) Effects of exogenoushormones on endometrial capillaries. In Alexander,NJ. and d'Arcangues, C. (eds), Steroid Hormonesand Uterine Bleeding. AAAS Press, Washington, DC,USA, pp. 67-79.
Fraser, I.S., McCarron, G., Hutton, B. and Macey, D.(1987) Endometrial blood flow measured by xenon-133 clearance in women with normal menstrual cyclesand dysfunctional uterine bleeding. Am. J. Obstet.Gynecol, 156, 158-166.
Gath, D., Osborn, M. and Bungay, G. (1987) Psychiatricdisorder and gynaecological symptoms in middle-aged women: a community survey. Br. Med. J., 294,213-218.
Gleeson, N., Devitt, M., Sheppard, B.L. and Bonnar, J.(1993) Endometrial fibrinolytic enzymes in womenwith normal menstruation and dysfunctional uterinebleeding. Br. J. Obstet. GynaecoL, 100, 768-771.
Goetz, K.L., Wang, B.C. and Madwell, J.B. (1988)Cardiovascular, renal and endocrine responses tointravenous endothelin in conscious dogs. Am. J.PhysioL, 255, 1064-1068.
Goodger, A.M., Rogers, P.A.W. and Affandi, B. (1994)Endometrial endothelial cell proliferation in long-termusers of subdermal levonorgestrel. Hum. Reprod., 9,1647-1651.
Hallberg, L., Hogdahl A.M., Nilsson, L. and Rybo, G.(1966) Menstrual blood loss — a population study.Ada Obstet. Gyntcol Scand, 45, 320-351.
Haynes, PJ., Anderson, A.B.M. and Tumbull, A.C.(1979) Patterns of menstrual blood loss inmenorrhagia. Res. Clin. Forums, 1, 73-78.
Henzl, M.R., Smith, R.E., Boost, G. and Tyler, E.T.(1972) Lysosomal concept of menstrual bleeding inhumans. J. Clin. Endocrinol. Metab., 34, 860-875.
Hickey, M., Fraser, I.S., Dwarte, D. and Graham, S.(1996) Endometrial vasculature in Norplant* users:preliminary results from a hysteroscopic study. Hum.Reprod., 11, Suppl. 2, pp. 35-44.
Hourihan, H.M., Sheppard, B.L. and Bonnar, J. (1986)A morphometric study of the effect of oralnorethisterone or levonorgestrel on endometrial bloodvessels. Contraception, 38, 603-612.
Hourihan, H.M., Sheppard, B.L. and Bonnar, J. (1989)The morphologic characteristics of menstrualhaemostasis in patients with unexplained menorrhagia.Int. J. Gynecol. Pathol, 8, 221-229.
Hourihan, H.M., Sheppard, B.L., Belsey, E.M. andBrosens, LA. (1991) Endometrial vascular featuresprior to and following exposure to levonorgestrel.Contraception, 43, 375-385.
Johannisson, E. (1980) The influence of contraceptivesteroids on the histochemistry and cytochemistry ofthe normal endometrium. In Diczfalusy, E., Fraser,I.S. and Webb, F.T.G. (eds), Endometrial Bleedingand Steroidal Contraception. Pitman Press, Bath, UK,pp. 174-190.
Johannisson, E., Foumier, K. and Riotton, G. (1981)Regeneration of the human endometrium and thepresence of inflammatory white cells followingdiagnostic curettage. Acta Obstet Gynecol Scand.,60,451-457.
Johannisson, E., Landgren, B.-M. and Diczfalusy, E.(1982) Endometrial morphology and peripheral steroidlevels in women with and without intermenstrualbleeding during contraception with the 300 |ignorethisterone (NET) minipill. Contraception, 25,13-21.
Kamat, B.R. and Issacson, P.G. (1987) Theimmunocytochemical distribution of leucocytesubpopulations in human endometrium. Am. J. Pathol,127, 66-73.
Kasonde, JM. and Bonnar, J. (1976) Plasminogen
176
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from

Mechanisms underlying disturbances of bleeding
activators in the endometrium of women usingintrauterine contraceptive devices. Br. J. Obstet.GynaecoL, 83, 315-319.
Lau, T. and Rogers, P.A.W. (1996) In-situ hybridizationstudies on endometrial progesterone receptors inNorplant users and during the normal cycle. Hum.Reprod, 11, in press.
Li, X.-F. (1996) Dual role of angiotensin II in the humanendometrium. Hum. Reprod., 11, Suppl. 2, pp. 95-108.
Maggi, M., VanneUi, G.B. and Peri, A. (1991)Immunolocalisation, binding and biological activityof endothelin in rabbit uterus: effect of ovariansteroids. Am. J. PhysioL, 260, E292-E305._
Maqueo, M. (1980) Vascular and peri vascular changesin the endometrium of women using steroidalcontraceptives. In Diczfalusy, E., Fraser, I.S. andWebb, F.T.G. (eds), Endometrial Bleeding andSteroidal Contraception. Pitman Press, Bath, UK, pp.138-152.
Markee, J.E. (1940) Menstruation in intraocularendometrial transplants in the rhesus monkey. Contrib.EmbryoL, 28, 219-308.
Marsh, M. (1996) Endothelin and menstruation. Hum.Reprod, 11, Suppl. 2, pp. 83-89.
Ober, W.B. (1970) Morphologic changes in the uterusassociated with steroid contraceptives and intrauterinecontraceptive devices. Ada CytoL, 14, 156-184.
Peek, MJ., Markham, R. and Fraser, I.S. (1995a)Angiogenic activity in normal and dysfunctionaluterine bleeding endometrium; as measured by thechick chorioallantoic membrane assay. Exp. ToxicoLPathoL, 47, 256-261.
Peek, MJ., Markham, R. and Fraser, I.S. (1995b) Thseffects of natural and synthetic sex steroids on humandecidual endothelial cell proliferation. Hum. Reprod,10, 2238-2243.
Perrot-Applanat, M., Groyer-Pickard, M.T., Garcia, E.et aL (1988) Immunocytochemical demonstration ofestrogen and progesterone receptors in muscle cells ofuterine arteries in rabbits and humans. Endocrinology,123, 1511-1519.
Rees, M.C.P., Dunhill, M.S., Anderson, A.B.M. andTumbull, A.C. (1984) Quantitative uterine histologyduring the menstrual cycle related to measured bloodloss. Br. J. Obstet. GynaecoL, 91, 662-666.
Rees, M.C.P., Canete-Soler, R., Lopez-Bernal, A. andTurnbull, A.C. (1988) Effect of fenamates onprostaglandin E receptor binding. Lancet, U, 541-542.
Rodgers, W.H., Matrisian, L.M., Giudice, L.C. et aL(1994) Patterns of matrix metalloproteinase expressionin cycling endometrium imply differential functionsand regulation by steroid hormones. /. Clin. Invest.,94, 946-953.
Rogers, P.A.W., Au, C.L. and Affandi, B. (1993)Endometrial microvascular density during the normal
menstrual cycle and following exposure to long-termlevonorgestrel. Hum Reprod, 8, 1396-1404.
Rybo, G. (1966) Clinical and experimental studies onmenstrual blood loss. Acta Obstet. Gynecol. ScandSuppL, 45, 1-23.
Salamonsen, L. (1996) Matrix rnetalloproteinascs andmenstruation. Hum. Reprod, 11, in press.
Sarfati, R. and Brux, J. (1973) Vascular fragility ofthe endometrium under estrogen-progestin treatment.Treatment by disodium flavonate. Eur. J. Obstet.GynecoL Reprod BioL, 2, 87-94.
Schroder, R. (1954) Endometrial hyperplasia in relationto genital function. Am. J. Obstet. GynecoL, 68,294-309.
Shaw, ST., Macaulay, L.K., Aznar, R. et al. (1981)Effects of a progesterone-releasing intrauterinecontraceptive device on endometrial blood vessels: amorphometric study. Am. J. Obstet. GynecoL, 141,821-827.
Sheppard, B.L. (1987) Endometrial morphology changesin IUD users: a review. Contraception, 36, 1-10.
Sheppard, B.L. (1990) Coagulation and electronmicroscopy studies in menorrhagia. In Shaw, R.W.(ed.), Advances in Reproductive Endocrinology.Parthenon Press, Camforth, UK, Vol. 2, pp. 25-42.
Smith, S.K. (1990) The physiology of menstruation. InD'Arcangues, C , Fraser, I.S., Newton, J.R. andOdlind, V. (eds), Contraception and Mechanisms ofEndometrial Bleeding. Cambridge University Press,Cambridge, UK, pp. 33-41.
Smith, S.K. (1996) Vascular endothelial growth factorand the endometrium. Hum. Reprod, 11, Suppl. 2,pp. 56-61.
Smith, S.K. and Kelly, R.W. (1987) The effect of theantiprogestins RU486 and ZK98734 on the synthesisand metabolism of PGF^ and PGE2 in separatedcells from early human decidua. J. Clin. EndocrinoLMetab., 63, 527-537.
Smith, S.K., Abel, M.H., Kelly, R.W. and Baird, D.T.(1981) A role for prostacyclin (PGI2) in excessivemenstrual bleeding. Lancet, I, 522-524.
Smith, S.K., Abel, M.H., Kelly, R.W. and Baird, D.T.(1982) The synthesis of prostaglandins from persistentproliferative endometrium. J. Clin. EndocrinoLMetab., 55, 284-289.
Snowden, R. and Christian, B. (1983) Patterns andPerception of Menstruation. Croom Helm, London,UK.
Song, J.Y., Markham, R., Russell, P. et aL (1995) Theeffect of high-dose medium- and long-termprogestogen exposure on endometrial vessels. Hum.Reprod, 10, 797-800.
Song, J.Y., Russell, P., Markham, R. et aL (1996) Theeffect of high-dose progestogens on white cells andnecrosis in human endometrium. Hum. Reprod., 11,in press. 177
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from

LS Jraser, MJUckey and J.-y-Song
Tabibzadeh, S. and Satyaswaroop, P.G. (1989) Sexsteroid receptors in lymphoid cells of humanendometrium. Am. J. Clin. Pathol., 91, 656-663.
Wang, I.Y.S. (1994) The role of lysosomes in the humanendometrium. MD Thesis, University of Sydney,Sydney, Australia.
White, J.O., Sullivan, M.H.F., Patel L. et aL (1991)
Prostaglandin production in human endometriumfollowing continuous exposure to low-doselevonorgestrel released from a vaginal ring.Contraception, 43, 401-412.
Wonodirekso, S., Au, C.L., Hadisaputra, W. et al. (1993)Cytokeratins 8, 18 and 19 in endometrial epithelialcells during the normal menstrual cycle and in womenreceiving NorplanL Contraception, 48, 481-493.
178
at Pennsylvania State University on February 23, 2013
http://humrep.oxfordjournals.org/
Dow
nloaded from


![SCISCITATOR 2015 · [1]. Riverine communities experience two main types of disturbances: natural disturbances and anthropogenic disturbances. Natural disturbances in riverine ecosystems](https://img.pdfslide.us/doc/110x75/5f27dd3959f0c41da22eeec5/sciscitator-1-riverine-communities-experience-two-main-types-of-disturbances.jpg)