-
8/2/2019 A Comparison Between Adults With Conduct Disorder
1/18
The Psychological Record, 2000, 50, 203-219
A COMPARISON BETWEEN ADULTS WITH CONDUCT DISORDERAND NORMAL
CONTROLS ON A CONTINUOUS PERFORMANCETEST: DIFFERENCES IN IMPULSIVE
RESPONSECHARACTERISTICSDONALD M. DOUGHERTY, JAMES M. BJORK, DAWN M.
MARSH,and F. GERARD MOELLERUniversity of Texas - Houston Health
Science Center
Continuous Performance Test (CPT) responding wascompared between
15 adults with a history (childhood/adolescent)of Conduct Disorder
(CD) and 15 normal controls. Of particularinterest was whether
response latencies and commission errors,which have been suggested
to be measures of impulsivity, woulddiffer between the groups. The
CPT procedure used included twoconditions: Immediate Memory Task
and Delayed Memory Task(IMT/DMT; Dougherty et aI., 1998). Both the
IMT (0.5-s delay) andDMT (3.5-s delay with distracter stimuli at
0.5-s intervals) requiredthe subject to respond if a briefly
displayed number was identicalto the one presented before it.
Stimuli included target (identicalmatch), catch (four of five
digits matched), and novel (no match).Participants completed six
22-min testing sessions scheduledacross a single day.The most
significant findings were that the CDgroup (compared to the control
group) had (a) elevatedcommission errors (responses to catch
stimuli); (b) lower stimulusdiscriminability (between target and
catch stimuli); and (c) shorterresponse latencies. These results
are consistent with the fewprevious studies indicating that these
parameters are related toimpulsive behaviors.
A number of different approaches have been used to study
impulsiveresponding in the laboratory. One of the most popular
methods is theoperant model, which defines impulsive responding as
a choice for asmaller immediate reinforcer over a larger delayed
reinforcer. Theadvantages of this approach are its rich history
from which comparisonscan be made and the clearly defined responses
that are amenable tostatistical and theoretical analyses (see
Anslie, 1975, for a review). As aresult, the operant conditioning
perspective remains a popular model forinvestigating impulsive
choice behavior in both humans and nonhumans(e.g., Green &
Rachlin, 1996; Rachlin, Raineri, & Cross, 1991). It is
importantThis research was supported by grants from the National
Institute on Alcoholism andAlcohol Abuse (AA-10095 & AA-10828)
and the National Institute on Drug Abuse (DA-08425). Requests for
reprints or the computerized memory tasks used in this study
shouldbe directed to Donald M. Dougherty, Department of Psychiatry
& Behavioral Sciences, 1300Moursund Street, Houston, TX 77030.
(E-mail: [email protected]).
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
2/18
204 DOUGHERTY ET AL.
to recognize, however, that impulsivity measured by operant
methodologymay be only one type of impulsive behavior. Impulsivity
is multidimensional,in that it involves several aspects of
behavior. For example, Barratt andcolleagues (Barratt, 1985;
Patton, Stanford, & Barratt, 1995) have proposeda three-factor
model of impulsivity. Their theory views impulsiveness as
acombination of three distinct factors: (a) motor impulsiveness,
which is actingon the spur of the moment and having an inconsistent
lifestyle; (b) attentionalimpulsiveness, which is an inability to
focus on the task at hand and apropensity for racing and
interrupted thoughts; and (c) nonplanningimpulsiveness, which is
the inability to plan and think carefully, along with alack of
enjoyment of challenging mental tasks. All three factors
includedimensions of arousal, information processing, and social
learning. Supportfor the three-factor theory has been provided by a
factor analyses of theBarratt Impulsiveness Scale-11 (Patton et
aI., 1995), a psychometricinstrument of impulsivity.The operant
approach to the study of impulsiveness falls primarily
intoBarratt's (1985) nonplanning factor of impulsiveness. However,
in order tostudy impulsiveness from a different perspective, we
used a modifiedversion of the Continuous Performance Test (CPT;
Rosvold, Mirsky,Sarason, Bransome, & Beck, 1956), a popular
measure of attentionalcapacity. There have been some studies
indicating that attentional deficits,as measured by the CPT, may be
related to impulsive behaviors (seediscussion below). This approach
differs from the operant approach in that ithas characteristics
that would seem to involve both the attentional and/ormotor factors
of the three-factor theory of impulsiveness.The CPT typically
requires participants to respond selectively to aseries of stimuli
(e.g., abstract shapes, letters, or numbers) that arepresented
briefly and rapidly (usually pre&entations and delays of
lessthan 500 ms). Since its inception, the CPT has been modified
many times,but usually the subject responds to identify a single
target stimulus (e.g.,"0") or a series of target stimuli (e.g., "A"
followed by "X") which remainsconstant throughout a testing
session. These CPT procedures have beenused to identify and
characterize attentional deficits in a variety of
subjectpopulations including attention deficit disorder in children
and adults(Halperin, Wolf, Greenblatt, & Young, 1991),
schizophrenics and personsat-risk for schizophrenia (see reviews by
Erlenmeyer-Kimling &Cornblatt,1987; Nuechterlein & Dawson,
1984), as well as persons with learningdisabilities (Dykman,
Ackerman, & Oglesby, 1979; Swanson, 1981).Despite the number of
variations, the CPT yields several key data,each parameter believed
to evaluate different components of attentionalprocessing. Three
primary measures are used. First, omission errors (ormisses) are
failures to respond to a target stimulus. Most researchersagree
that these errors represent deficits in sustained attention
orvigilance. Second, commission errors (or false alarms) are
responsesmade to stimuli other than target stimuli. Researchers
have varied in boththe way they have defined commission errors (in
various paradigms) andin the interpretation of these errors. Some
have defined commission
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
3/18
CONDUCT DISORDER AND CPT PERFORMANCE 205
errors as any response to a nontarget stimulus and have
suggestedelevated frequency of these errors represents impulsive
responding(O'Dougherty, Nuechterlein, & Drew, 1984; Sykes,
Douglas, Weis, &Minde, 1971). However, others disagree with the
breadth of thisinterpretation (Halperin et aI., 1988, 1991; Sostek,
Buchsbaum, &Rapoport, 1980; Sykes, Douglas, & Morgenstern,
1973; Wohlberg &Kornetsky, 1973) and define impulsive-type
commission errors as asubset of all errors in which incomplete
processing of a stimulus similarto the target leads to a rapid, but
incorrect response. These more narrowlydefined commission errors
may be more indicative of impulsive behavior.And third, latencies
are the delay between the onset of a stimulus and theparticipant's
response. Latencies provide information about the
temporalrequirements for processing, indicate how difficult a
discrimination is in aparticular CPT task, and may also give an
indication about how differentpopulations process stimuli before
responding (Dougherty et aI., 1998;Halperin et aI., 1988, 1991).The
present study was primari'ly concerned with two of the
abovemeasures, commission errors and response latencies, because
they maybe related to impulsivity. Although some authors may
disagree with thisinterpretation, at least part of the skepticism
surrounding thisinterpretation stems from the fact that little
effort has been made toexternally validate these measures with
populations having impulsecontrol problems. The use of commission
errors and latencies asmeasures of impulsivity are consistent with
the "fast-guess" model ofimpulsivity, whereby judgment or accuracy
is found to be compromised forthe sake of speed (Oilman, 1966;
Vellot, 1971). According to this model,making decisions takes a
certain amount of processing time anddecisions (or responses) made
before processing has been completedare impulsive (Sergeant &
Sholten, 1985; Sperling, 1984; Vellot, 1971). Inother words,
commission errors result from failure to withhold responsesuntil a
stimulus identity could be completely processed, and are
thereforeimpulsive. When this model is applied to the commission
errors andresponse latencies of the CPT, it follows that impulsive
responding wouldbe characterized by shorter latencies and more
commission errors(because stimuli have not been completely
processed).
CPT research with adults with histories of conduct disorder has
beenscant. However, other data exist which suggest that men with
conductdisorder histories may represent a population likely to
evidence CPTperformance deficits. Behavioral disinhibition has been
extensivelyresearched in the context of EEG responses evoked during
go/no-go tasks.Like the CPT, these tasks require subjects to
respond to a target stimulusand to withhold responses to an
inhibitory stimulus. In particular, in humansthe neural processes
involved in withholding responses to rapidly presentednontarget
stimuli generated a substantial P300 EEG wave compared tobrain
activity when processing a target stimulus (discussed in Roberts,
Rau,Lutzenberger, & Birbaumer, 1994). Interestingly, men with a
history ofchildhood conduct disorder (CD) have been shown to have
blunted frontal
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
4/18
206 DOUGHERTY ET AL.
cortex electroencephalographic (P300) activity to nontarget
stimuli (Bauer,1997). Moreover, in these men, the number of conduct
disorder symptomsprior to age 15 correlated negatively with frontal
P300 amplitude during atask similar to the CPT used in the present
study. Additionally, P300amplitude has been shown to be inversely
proportional to BarrattImpulsiveness Scale scores (Barratt, 1965;
Branchey, Buydens-Branchey, &Horvath, 1993). This literature
suggests that persons with histories of DSMIII-R-defined conduct
disorder represent an ideal population in which todetermine the
external validity of CPT commission errors and latency asmeasuring
impulsiveness.Some studies have found increased commission error
rates and shorterlatencies in other impulsive populations. For
example, Halperin et al. (1991)found certain types of commission
errors on the CPT ("A followed by X"version) to be more frequently
made by children with attention deficitdisorder (compared to normal
controls), and that reaction times (latencies)were shorter in
duration. Commission error rates are also elevated innonalcoholic
subjects having a family (parental) history of
alcohol-relatedproblems (Miner, 1984; unpublished dissertation) or
history of OWl arrests(Koch & Morguet, 1985). These studies
indirectly support the idea thatcommission error rates and
latencies are perhaps related to impulsive ordisinhibited
behaviors/traits.To investigate this possibility, we used a
recentlydeveloped CPT procedure (The Immediate Memory Task and
DelayedMemory Task, IMT/DMT; Dougherty et aI., 1998).Specifically,
the main purpose of this study was to compare CPTperformance
between 15 controls and 15 adults with a
self-reportedchildhood/adolescent history of behavior that would
have met criteria forconduct disorder (CD). We chose CD individuals
because impulsivenesshas been an important factor in explaining
this common childhoodcondition (Loeber, 1990; Quay, 1988; Schachar,
Tannock, & Logan, 1993).Gorenstein and Newman (1980) included
CD in a constellation of"syndromes of disinhibition" which they
proposed to have a commonfoundation of disinhibited, impulsive
behaviors. Because externalizeddisinhibition is a main feature of
CD (Windle & Windle, 1993), wehypothesized that adults with a
history of childhood CD would havemaintained several impulsive
traits, and that these would be evidenced inthe IMT/DMT performance
in the following ways: (1) higher rates of falsealarm commission
errors, (2) shorter response latencies, (3) lowerstimulus
discriminability, and (4) liberal responding strategy (measured
bythe signal detection parameter Beta). Furthermore, we
hypothesized thatthese measures would be related to scores on a
self-reported measure ofimpulsivity, the Barratt Impulsivity Scale
(BIS-11; Patton et aI., 1995).
MethodSubjectsThe conduct disorder group (n = 15) consisted of
persons who metcriteria for childhood/adolescent conduct disorder
(CD) with onset before
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
5/18
CONDUCT DISORDER AND CPT PERFORMANCE 207
age 15. Diagnosis was made using the Antisocial Personality
Disorder(ASPD) modute of the Structured Clinical Interview for
DSM-III-R Axis IIDisorders (SCID-II; Spitzer, Williams, Gibbon,
& First, 1990; at the time of thestudy the SCID-II fo r DSM-IV
was not yet available). In the CD group, 2subjects were Caucasian,
1 was Hispanic, and 12 were African-American.The mean age and years
of education for this group were 30.5 + SO 7.4, and11.0 + SO 1.36,
respectively. Subjects in the control group (n =15) wererecruited
to demographically resemble the CD group with respect to
age,education, and race, with the highest matching priorities
placed on age andeducation. In the control group, 6 were Caucasian,
3 were Hispanic, and 6were African-American. The mean age and years
of education for this groupwere 27.6 + SO 6.4 and 13.6 + SO 1.9,
respectively.Both groups were recruited from the community using
newspaperadvertisements. Prospective participants were screened in
a brieftelephone interview and callers who reported no psychiatric
history wereinvited to a subsequent on-site interview. The on-site
interview consistedof a medical history interview and a Structured
Clinical Interview for DSMIV Axis I disorders (First, Spitzer,
Gibbon, & Williams, 1996), as well asthe SCID-II for DSM-III-R
(Spitzer, Williams, Gibbon, & First, 1990).Applicants were not
admitted for study if the interviews indicated asignificant current
medical condition or the presence of current or pastAxis I disorder
other than substance abuse.
For both study groups, participation in the research study was
voluntaryand informed consent was obtained. All methods and consent
forms wereapproved by the University of Texas-Houston Institutional
Review Board.Subjects were told that the study was concerned with
memory and motorperformance; no mention was made of impulsivity,
either verbally or in theconsent forms. After completing the last
testing session and otherpsychometric measures subjects were paid
approximately $45.Testing schedule. Each subject participated
throughout 1 day.Subjects began testing at 0800 hrs, at which time
they submitted breathand urine samples for tests of current alcohol
or other drug use; allsubject samples tested negative. Subjects
then completed a total of sixCPT sessions (using the Immediate
Memory Task I Delayed MemoryTask, described below), with each of
these sessions beginning at 0830,0930, 1030, 1130, 0130, and 0330.
Lunch was provided at noon.Physical apparatus. Behavioral testing
was performed in 1.8-m x 1.8-m sound-insulated chamber equipped
with an IBM-compatible colormonitor, a ventilation fan (which
provided masking noise), and a twobutton computer mouse. A computer
located in an adjacent roomcontrolled and monitored experimental
events.Continuous Performance TestA modification of the original
CPT, the Immediate Memory Task IDelayed Memory Task (IMT/DMT;
Dougherty et aI., 1998) was used forthis investigation. In each
testing session, the two task conditions (IMTand DMT) alternated in
5-min testing blocks with a 30-s rest period
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
6/18
208 DOUGHERTY ET AL.
preceding each block. The IMT was always first and alternated
with theDMT, with each presented twice. As a result, testing
sessions lastedexactly 22 minutes. Both conditions are described
below.Immediate Memory Task (IMT). This task was designed to
measure briefattentional capacity. A series of 5-digit numbers
(e.g., 73021) were displayedon the monitor for 0.5 s and separated
by a 0.5-s blackout period. Each ofthe digits measured 2.0 cm wide
x 3.3 cm high, and the numbers werepresented on the computer
monitor in black on a white background.There were several distinct
types of stimuli presented and types ofresponses that could be
made. Subjects were instructed to respond on thecomputer's left
mouse button when a 5-digit number (the target stimulus)appeared
that was exactly like the preceding stimulus. The probability of
atarget stimulus was 33%. A response made while a target stimulus
appearedon the monitor, or made before the next stimulus appeared
(1.0 s total), wasrecorded as a correct detection (hit). A failure
to respond to a target stimuluswas recorded as an omission error
(miss). In addition to target stimuli, therewas a 33% probability
that a catch stimulus would appear. A catch stimuluswas a number
that differed from the preceding number by one of the fivedigits
(its position and value was determined randomly). Responses
(errors)made to catch stimuli were considered commission errors
(false alarms).The remaining stimuli, novel stimuli (numbers),
which were not either targetor catch trials were called filler
stimuli and responses made to these stimuli
were categorized as "other errors:' [Note: A novel stimulus
always followed atarget or catch trial.]Delayed Memory Task (DMT).
This task was designed to measure asubject's ability to retain a
stimulus and identify it after a longer delay(compared to the IMT
above). The primary difference between this task andthe IMT was
that all stimuli (including target, catch, and filler) were
separatedby the number "12345:' which was repeated three times at
the same rate andduration as all other stimuli. For example, one
possible sequence involving atarget stimulus would be: 39863,
12345, 12345, 12345, 39863. Subjectswere instructed to ignore the
"12345" and only to remember and identifystimuli separated by the
series of "12345" numbers. These stimuli, "12345:'were designated
as distracter stimuli. Presenting these distracter stimuliallowed
us to increase task difficulty, to control for rates of visual
stimuluspresentation, and to improve task sensitivity.In addition
to the number of responses made to each type of stimulus,response
latencies for correct detections and commission errors
wererecorded. The time between onset of stimulus presentation and
aresponse was recorded in milliseconds.Psychometric
InstrumentsBarratt Impulsiveness Scale (BIS). The BIS (Version 11,
Patton et al.,1995) is a self-completed, 30-item questionnaire on
which participantsrate their frequency of several common impulsive
behaviors and traits(e.g., "I do things without thinking" ) or
nonimpulsive behaviors/traits(scored in reverse; e.g., "I am
self-controlled") on a scale from 1
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
7/18
CONDUCT DISORDER AND CPT PERFORMANCE 209
("rarely/never") to 4 ("almost always/always"). In order to
examine therelationship between impulsivity and CPT performance,
severalcorrelations were made between BIS scores and parameters of
the CPT.Wisconsin Card Sorting Test (WCST). The WCST (Computer
Version-2; Curtiss &Tuttle, 1993; Heaton, Curtiss, Tuttle,
& PAR Staff, 1993) is aneuropsychological test that purportedly
measures deficits in frontal lobeor "executive functioning." This
test involves memory, abstraction, andsensitivity to performance
feedback. A subject is instructed to match acard to one of a set of
four stimulus cards based on an unknown sortingdimension (color,
shape, or number of symbols) which changesperiodically during
testing. To determine whether our two groups differed
in WCST performance, we compared percentage of errors,
percentage ofperseverative responses (continuing to match by an
incorrect sortingprinciple), and number of categories
completed.Beck Depression and Anxiety Inventories. As part of our
screeningprocedure subjects completed the Beck Depression (BDI;
Beck, Rush,Shaw, & Emery, 1979) and the Beck Anxiety
Inventories (BAI; Beck,Brown, Epstein, & Steer, 1988). These
instruments were only used toquickly identify persons with possible
psychiatric problems and tocompare subclinical symptoms between our
two groups.The BDI is a commonly used self-report instrument which
provides anumerical index of symptomatology associated with
depression. On the
BDI, the rater selects from a series of numerically graded
statementspertaining to mood, self-worth, suicidal thoughts, and
somaticsymptomatology during the previous week. On the BAI, the
respondentassigns a rating from 0-3 to the severity of symptoms of
anxiety, such asfear of dying, breathing difficulty, and
unsteadiness.Data Analysis. Response latencies to target and catch
stimuli,percentages of correct detections (responses to target
stimuli),percentages of commission errors (responses to similar but
not identicalstimuli), discriminability (d'), and Beta Values
(description of d' and Betaparameters appears below in results)
were analyzed in repeatedmeasures analyses of variance in a 2 x 6 x
2 design, with task type (IMTvs. DMT) and session (1-6) as
within-subject factors, and group (CD vs.control) as the
between-subject factor. In the latency analysis, stimulustype
(target vs. catch) was also included as a within-subject factor.
Finally,response latencies, commission errors (false alarms),
correct detections,and BIS scores were correlated using Spearman
correlation. Otherbetween-group differences in demographic
variables and psychometricinstruments were assessed using
independent t tests or chi-square tests(where appropriate). In
previous studies we have failed to detect a withinsession effect of
block (time) on any parameter of IMT and DMTperformance (e.g.,
Dougherty et aI., 1998). For this reason, data from thetwo blocks
within each testing session were averaged. Additionally,because of
the near absence of responses to random and/or distracter"12345"
stimuli, statistical analysis of rates of these types of errors
wasnot appropriate, and brief"descriptive data are presented
instead.
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
8/18
210 DOUGHERTY ET AL.
All correllations were conservatively calculated using
Spearman'snonparametric tests because of the number of correlations
being done.
ResultsIndependent t tests and chi-square tests indicated that
the two subjectgroups did not significantly differ (p > .05) in
age, gender, or racialcomposition. The control group averaged 2.6
years more education than the
eo group, which was statistically different [28) = 4.28, P <
.001]. APearson's chi-square test showed the incidence of past
substanceabuse/dependence between the eD (n = 7) and control groups
(n = 3) wasnot significantly different (p> .05). Independent t
tests showed commissionerror rates and latencies for IMT and OMT
conditions did not differ (p> .05)between subjects with or
without a history of substance abuse/dependence.BAI and BDI scores
indicated no significant between-groupdifferences in subclinical
symptoms of anxiety or depression. Additionally,using independent t
tests .we found no group differences in any
component of WeST performance (p > .40 for % errors, %
perseverativeresponses, and number of categories completed).
Psychometricmeasures (WeST, BIS, BOI, and BAI) were not obtained
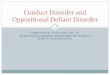
from 2 subjects.Correct detections (hits). Subjects made responses
to the majority oftarget stimuli presented in both the IMT and OMT,
making a few morecorrect detections on the IMT than on the OMT
[main effect of task typeF(1, 28) =7.504, p = 011]. These data
appear in Figure 1. The main effectof session showed a slight, but
Significant, increase in correct detectionsacross sessions [F(5,
140) =2.632, P = 026]. The main effect of groupwas not significant,
indicating that the groups did not differ in the rates ofcorrect
detections [F(1, 28) = 0.718, p = .404].
100en 90c0 80-+-'0a> 70-'Q)0 60+-'0 50)L -L -a 40( )+-' 30cQ)
20L -a> 10..
0 1
Immediate Memory Task
___ Conduct Disorder Group_ Control Group
234 5Session 6
100908070605040302010
Delayed Memory Task
O ~ - - ~ - - ~ - - ~ ~ - - ~ -1 234 5Session 6
Figure 1. Percentages of correct detections (correct responses
to target stimuli) made forthe conduct disorder and control groups
in the IMT (left panel) and the DMT (right panel)across six testing
sessions (error bars represent the SEM.).
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
9/18
CONDUCT DISORDER AND CPT PERFORMANCE 211
All higher-order interaction effects were not significant: task
type xsubject group [F(1, 28) =0.013, P= .909], session x subject
group [F(5,140) =0.70, P= .622], task type x session [F(5, 140)
=0.88, P= .496],and task type x session x subject group [F(5, 140)
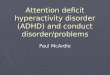
=0.278, P= 924].Commission errors (false alarms). The CD subjects
madeapproximately twice as many commission errors (responses made
tosimilar but not identical stimuli) than controls in both the IMT
and DMT[F(1, 28) = 28.915, P< .0001]. These data appear in
Figure 2. The maineffects of task type [F(1, 28) =1.485, P= 233]
and session [F(5, 140) =1.066, P= 381] on commission error rates
were not significant.All other effects were not significant: task
type x subject group [F(1,28) =0.102, P = .752], session x subject
group [F(5, 140) =0.820, p =.537], task type x session [F(S, 140) =
1.76S, p = .124], and task type xsession x subject group [F(5,140)
= 0.856, p = .512].
o50
t::: 40Wc::o 30.-E 20(Jc::
10Q)a.
1
Immediate Memory Task
- I I - Conduct Disorder Group-e- Control Group
23456Session
50
40
30
20
10
1
Delayed Memory Task
23456SessionFigure 2. Rates of commission errors (responses to
"catch" stimuli which differed from theprevious stimulus by only
one digit). Percentages of catch stimuli to which the
conductdisorderand control groups responded in the IMT and the DMT
appear in the left and rightpanels, respectively (error bars
represent the SEM.).
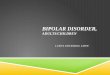
Discriminability (dJ. The signal detection parameter d', the
measure ofdiscriminability between signal and noise (Le., between
target and catch stimuli),was calculated and appears in the top
panels of Figure 3. For d', higher valuesindicate better
discriminability. These values were calculated using
standardizedformulas taken from Gescheider (198S, p. 97). The main
effect of memory tasktype was significant, indicating that
discrimination was more difficult in the DMTcompared to the IMT
[F(1, 28) =31.950, p < .0001]. Also, CD subjects had d'values
that were significantly lower than controls for both tasks [main
effect ofgroup was F(1, 28) =36.418, p < .0001].All other
effects and interactions were not significant: session [F(5, 140)
=0.S21 , P= 760], session x subject group [F(S, 140) =0.431, P=
83], session xmemory task type [F(5, 140) =0.497, p = 778], subject
group x memory task
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
10/18
212 DOUGHERTY ET AL.
type [F(1 ,28) = 1.863, P= .183], and session x memory task type
x subject group[F(5, 140) = 0.472, P= .797].Beta. An identical
analysis was performed using the signal detectionparameter Beta.
These data appear in the bottom panels of Figure 3. Beta scoresgive
an indication of how subjects' response criteria are distributed
(e.g., eitherconservative or liberal). Higher scores indicate a
more conservative responsestrategy. These values were calculated
using standardized formulas taken fromGescheider (1985, p. 97).
Subjects with histories of CD did not respond moreliberally than
controls to CPT stimuli in general. Beta was not Significantly
higher incontrols compared to CD subjects [F{1, 28) = 1.059, P =
.312]. All subjects weremore conservative in responding to DMT
stimuli (higher beta values) than IMTstimuli [memory task type main
effect F{1,28) =23.824, P< .0001].
Immediate Memory Task Delayed Memory Task3 3--- Conduct Disorder
Group-e-- Control Group2 +-+ +- + + +. 2
'"C
1 1
o ~ - - ~ - - ~ - - ~ - - ~ - - ~ o ~ - - ~ - - ~ - - ~ - - ~ -
- ~ 1 2 3 4 5 6 1 2 3 4 5 6
3 3-... Conduct Disorder Group-e-- Control Group
0>2::J 2-ro>ro
.....
1
o ~ - - ~ - - ~ - - ~ - - ~ - - ~ 1 2 345 6 1 2 345 6Session
SessionFigure 3. Shown in this figure are the signal detection
parameters d' and Beta.Discriminability (d') between target and
catch stimuli in the IMT and DMT are shown for theIMT and DMT in
the top panels. Response bias (Beta) values in the IMT and the DMT
areshown in the bottom panels (error bars represent the SEM).
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
11/18
CONDUCT DISORDER AND CPT PERFORMANCE 213
All other effects were not significant: session [F(5,140) =
1.303,. P =.266], session x subject group [F(5,140) = 1.127, P =
.349], session xmemory task type [F(5, 140) =0.964, P= 442],
subject group x memory tasktype [F(1,28) = 1.31, P = .261], and
session x memory task type x subjectgroup [F(5,140) =1.578, P=
170].Response latencies. As shown in Figure 4, response latencies
were shorterfor the CD subjects compared to controls across both
memory tasks [main effectof group F(1, 28) =4.211 , P= 049]. Across
all subjects, latencies were shorterin the IMT than the DMT [main
effect of memory task type [F(1 , 28) = 56.893, P< .0001]. The
memory task type x group interaction was not significant [F(1,
28)=0.349, P= 559]. In addition, there was also a main effect of
session [F(5, 140)=2.651, P= 025], with latencies becoming shorter
in succeeding sessions. Thiseffect was not specific to group or to
task [session x group F(5, 140) =1.262, P= 283; session x task F(5,
140) =0.813, p= 542].
700.-..
650Ec::.::..600c:Q) 550+- 'ctS...JQ) 500enc:0g.450Q)a: 400 1
Immediate Memory Task___ Control-Target___ Control-Catch
700
- . . - Conduct Disorder- Target 650--+- Conduct
Disorder-Catch
23456Session
600550500450
1
Delayed Memory Task
23456SessionFigure 4. Response latencies (measured in ms) to
target and catch stimuli on the IMT (leftpanel) and the DMT (right
panel) .
There was no main effect of stimulus type [target vs. catch;
F(1, 28) = 2.582,P= 119] on latency, but the data suggested higher
order interactions of stimulusby task type. For example, although
response latencies to catch and targetstimuli in the IMT were
strikingly similar, there was a trend for longer latencies forcatch
stimuli compared to target stimuli in the DMT [stimulus x task type
F(1, 28)=3.581, P= 068]. Moreover, the session by stimulus
interaction [F(5, 140) =3.171, P = .009] indicated that subjects
took longer to respond to catch stimuliacross sessions, and the
session x stimulus x memory task type interactionrevealed a trend
for this to be specific to the DMT [F(5, 140) =2.181, P= 069].With
respect to between-group differences, a significant stimulus x
groupinteraction [F(1, 28) = 4.750, P = .037] suggested that CD
subjects (but notcontrols) had longer latencies to catch stimuli
than target stimuli. No other higherorder interactions were
Significant.
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
12/18
214 DOUGHERTY ET AL.
Commission errors corresponded to shorter response times.
IMTcommission error rates negatively correlated with mean IMT
latencies (r= -.620,p < .0002), as did DMT commission error
rates with mean DMT latencies (r =-.740, P< .0001). These
Spearman correlations appear in the top panels ofFigure 5. To
determ ine whether or not the differences in latencies could
beresponsible for the differences in commission error rates between
our twogroups, we reanalyzed the between-group differences with
latency added as acovariate. In this analysis we found that
adjusted mean commission error ratesbetween the two groups were
still significantly different in the IMT [group maineffect F(1, 27)
=22.044, P= 0001] and DMT [F{1, 27) =24.186, P< .0001].
Immediate Memory Task Delayed Memory TaskC/) 80 80-.6202 -.7403r
= r ='- - p = 0002W 70 70 p < .0001c 0 60 60-/)C/) 50 - 50 E E
40 40U .. . .. '+ - 30 300 ... ) 20 20 :.c . E . ::J 10 10Z c 0
0300 400 500 600 700 800 900 300 400 500 600 700 800 900)
Mean Latency (in ms) Mean Latency (in ms)
80 80e r = .4229 r = .1915 .0250 70 .3291= P =c 60 60.-/) I/) 50
50E E 40 400 U 30 30+- '- Q) 20 20 .c E 10 10:JZC 0 0m 40 45 50 55
60 65 70 75 80 85 40 45 50 55 60 65 70 75 80 85) BIS Total Score
BIS Total Score
Figure 5. These figures show Spearman's rho correlations between
mean response latenciesand mean number of commission errors (top
panels) and between the Barratt ImpulsivenessScale (BIS-11) and
mean number of commission errors (bottom panels). Ellipses indicate
.90normal density using the means, standard deviations, and
correlations from the data. The toppanels show a negative
correlation between the number of commission errors and latency
forboth IMT and DMT. The bottom panels show a positive correlation
between the number ofcommission errors and the BIS total score
(possible score range: 30-120 points), although thisrelationship
was not significant for the DMT condition.
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
13/18
CONDUCT DISORDER AND CPT PERFORMANCE 215
Other errors. Responding to random (novel) or distracter stimuli
("12345" inthe DMT) was rare in both groups, suggesting that all
subjects could easilydiscriminate stimuli which differed noticeably
from target stimuli. These errorresponses were made to less than 1
of these stimUli. Collectively, rates ofthese sporadic responses
were not suitable for an analysis of variance.Psychometric
measures. Barratt Impulsiveness Scale (BIS-11 ; Patton et aI.,1995)
total scores were significantly higher for CD subjects (Mean =67.3,
SO =7.4) than for controls [M =57.1, SO =13.9; 26) =2.43, P= 0225].
The BISnonplanning subscale scores were also higher for the CD
subjects (M=30.9, 'SO =6.9) than for controls [M=23.07, SO =6.6; ~
2 6 ) =3.081, P= 0048].Neither tt"le motor nor the attentional BIS
subscales were significantlydifferent between groups.BIS scores
were correlated with IMT/DMT commission error rates(averaged across
the six sessions; Figure 5) to determine how impulsivity in
theIMT/DMT (conceptua lized here as high commission error rates and
shorterlatencies) related to an external measure of impulsivity.
Across all subjects, BISscores correlated positive ly with IMT
commission error rates (r = .42, P= .025)but not with DMT
commission error rates (r = .19, P = .329). Correlationsbetween the
BIS and response latencies (target and catch stimuli latencies
eachaveraged across sess ions) showed no significant relationship
for either the IMT(r= -.19, p= 341) or the DMT (r= .01, P=
926).
DiscussionWe hypothesized that adults whose childhood/adolescent
behavior met theStructured Clinical Interview for DSM-III-R
(Spitzer et aI., 1990) criteria forConduct Disorder (CD) would
perform in a manner consistent with what previousCPT researchers
have proposed as impulsive response characteristics.Compared to
control subjects, CD subjects had significantly (a) higher rates
ofcommission errors (Le., more false alarms) on both the IMT and
DMT; (b) shorterresponse latencies (approximately 100 ms); and (c)
lower discriminability (d)
between target and catch stimuli.Not only were significant
differences observed in IMT/DMT behaviorbetween the two groups, but
the BIS total and nonplanning subtrait scores for theCD group were
significantly higher than the control group. The BIS total
scorealso Significantly correlated with IMT, but not DMT commission
error rates, whichis very likely a reflection of fundamental
differences in the tasks. The IMT requiresfast, repetitive
discriminations and is more closely related to previous CPT
tasks,while the DMT is a more difficult task with the inclusion of
delays and distracterstimuli. The greater difficulty of the DMT has
probably contributed to an increasein variability which reduces the
likelihood of finding a meaningful relationship withthe BIS scores.
However, overall, the data seem to provide further support for
thecontention that CPT commission errors may be related to
impulsivity.Our findings are especially interesting given that
there exists data indicatingthat electrophysiological responses to
commission errors (on tasks similar toIMT/DMT) differ between
various populations. For example, men with historiesof conduct
disorder prior to age 15 have been shown to have blunted
frontal
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
14/18
216 DOUGHERTY ET AL.
cortex electroencephalographic (P300) activity in a task similar
to the one usedin our study (Bauer, 1997). The P300 wave is
generally considered an indicationof attention or interest.
Interestingly, Bauer reported that P300 amplitudedecrements were
not evident when subjects were deciding whether to respondto target
stimuli, but rather the P300 deficit was evident only when subjects
werepresented with stimuli analogous to the CPT catch stimuli of
this study. Moreover,these P300 decrements were only found in men
with conduct disorder historyprior to age 15. Additionally, P300
amplitude has been shown to be inverselyproportional to Barratt
Impulsiveness Scale scores (Barratt, 1965; Branchey etaI., 1993).
This neurophysiological data, together with our present
findings,suggest that conduct disorder prior to age 15 may predict
discrimination andresponse inhibition deficits as an adult.Although
the studies described above collectively support the contentionthat
commission errors may be an indicator of impulsive behavior, some
cautionshould be exercised. Only a handful of studies (mostly with
children) haveexamined the relationship between commission errors
and impulsivity. Otherinterpretations of the data are plausible.
For example, group differences inlatencies and commission error
rates may be the result of attentional, memory,or perhaps sensory
deficits of adults with a history of conduct disorder. Thesefactors
could explain why the CD group showed longer commission
errorlatencies compared to the control group. While commission
error rates and theoverall CD group latencies were significantly
different than controls for both IMTand DMT conditions as we
hypothesized, the specific commission error latencygroup difference
did not support our hypothesis.Some of the parameters of the
IMT/DMT procedures may have maximizeddifferences in commission
error rates and are worth noting. First, previousstudies have often
used liberal definitions of commission errors, such as
definingthese errors as any response made to some stimulus other
than the targetstimulus. We suggest that defining commission error
responses in this mannerlimits the interpretation of the data. It
cannot be determined whether the errorsare made because the subject
cannot discriminate between signal (target) andnoise (other
stimuli), or whether the errors are a result of a population's
elevatedarousal levels (e.g., ADHD Children). Procedures that more
conservatively definecommission errors allow for a comparison of
two types of error rates betweenstimuli which are both similar to,
and different from, the target stimuli. Differentialresponding to
these two error types would provide clues to whether responseswere
due to discriminability or to higher arousal levels.Second,
increasing the task difficulty compared to earlier CPT
versionsprovided more distinctive differences between groups. The
magnitude of thedifferences in commission error rates between
groups was large. Previousstudies which used easier CPT procedures
engendered relatively low rates ofcommission errors, and so
differences between normal and patient populationswere small.
Generally, commission error rates were less than 100;0,
withdifferences between populations being less than 5%. Previous
researchindicates that detecting subtle differences in attention in
adult populationsappears to be dependent on the difficulty of the
CPT procedure used; easiertasks are not as sensitive as difficult
tasks (for a discussion see Cornblatt & Keilp,
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
15/18
CONDUCT DISORDER AND CPT PERFORMANCE 217
1994}. Additionally, in order to better discriminate between
populations(especially between adult populations) the task should
be of sufficient difficulty toproduce sufficient numbers of errors
to allow for a better separation betweenpopulations. A higher
commission error rate may be more sensitive to theintroduction of
independent variable manipulations. .There are a number of obvious
routes that future research, examining therelationship between
commission errors and impulsivity, should take. First,the effects
of drugs of abuse and medications on commission errors shouldbe
studied. This can be approached from two different perspectives:
(a)studying the effects of medications (e.g., stimulants) on
commission errorrates, and (b) how drugs of abuse (e.g., alcohol)
may increase commissionerror rates. The expectation, from an
impulsivity approach, would be thatalcohol would increase impulsive
responding, and stimulants (at therapeuticdoses) would decrease
impulsive responding. In fact, a recent study with 18social alcohol
drinkers (Dougherty et aI., 1999) found that small doses ofalcohol
(achieving BACs of approximately 0.035) increased commission
errorrates, and changes in performance were .specific to these
errors. Second,commission error rates should be studied by
systematically examining theeffects of contingencies on performance
to determine whether or notdifferences between populations can be
minimized. And third, otherneuropsychological measures should be
taken in an attempt to determine thenature of the deficits between
populations and to explore whether otherinterpretations of data
could account for these observed differences.
ReferencesANSLIE, G. (1975). Specious reward: A behavioral
theory of impulsiveness and impulsecontrol. Psychological Bulletin,
82(4),463-496.BARRAlT, E. S. (1965). Factor analysis of some
psychometric measures ofimpulsiveness and anxiety. Psychological
Reports, 16,547-554.BARRATI, E. S. (1985). Impulsiveness subtraits:
Arousal and information processing. InJ. T. Spence & C. E.
Izard (Eds.), Motivation, Emotion, and Personality (pp. 137-146).
North-Holland, NY: Elsevier Science Publishers B.V.BAUER, L. O.
(1997). Frontal P300 decrements, childhood conduct disorder,
familyhistory, and the prediction of relapse among abstinent
cocaine abusers. Drug and
Alcohol Dependence, 44, 1-10.BECK, A. T., BROWN, G., EPSTEIN,
N., & STEER, R. S. (1988). An inventory formeasuring clinical
anxiety: Psychometric properties. Journal of Consulting andClinical
Psychology, 56 , 893-897.BECK, A. T., RUSH, A. J., SHAW, B. F.,
& EMERY, G. (1979). Cognitive theory ofdepression. New York:
The Guilford Press.BRANCHEY, M. H., BUYDENS-BRANCHEY, L., &
HORVATH, T. B. (1993). Event relatedpotentials in substance abusing
individuals after long term abstinence. AmericanJournal
ofAddiction, 2, 141-148.CORNBLATI, B. A., & KEILp, J. G.
(1994). Impaired attention, genetics, and thepathophysiology of
schizophrenia. Schizphrenia Bulletin, 20, 31-46.CURTISS, G., &
TUTTLE, K. (1993). Wisconsin card sorting test: Computer version
2[Program Manual]. Odessa, FL: Psychological Assessment Resources,
Inc .
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
16/18
218 DOUGHERTY ET AL.
DOUGHERTY, D. M., MOELLER, F. G., STEINBERG, J. L., MARSH, D.
M., HINES, S.E., & BJORK, J. M. (1999). Alcohol increases
commission error rates for acontinuous performance test.
Alcoholism: Clinical and Experimental Research,23(8),
1342-1351.DOUGHERTY, D. M., STEINBERG, J., WASSEF, A. A., MEDEARIS,
D., CHEREK, D. R.,& MOELLER, F. G. (1998). Immediate versus
delayed visual memory taskperformance among schizophrenic patients
and normal controls. PsychiatryResearch, 79, 255-265.DYKMAN, R. A.,
ACKERMAN, P. T., & OGLESBY, D. M. (1979). Selective and
sustainedattention in hyperactive, learning-disabled and normal
boys. Journal of NeNous
and Mental Disease, 167,288-297.ERLENMEYER-KIMLING, L., &
CORNBLATT, B. (1987). High-risk research inschizophrenia: A summary
of what has been learned. Journal of PsychiatricResearch, 21 ,
401-411.FIRST, M. B., SPITZER, R. L., GIBBON, M., &WILLIAMS, J.
B. W. (1996). StructuredClinical Interview for DSM-IV Axis I
Disorders: Non-patient Edition (SCID-NP).Biometrics Research
Department, New York State Psychiatric Institute, NY.GESCHEIDER, G.
A. (1985). Psychophysics: Method, theory, and application (p.
97).Hillsdale, NJ: Lawrence Erlbaum.GORENSTEIN, E. E., &
NEWMAN, J. P. (1980). Disinhibitory psychopathology: A
newperspective and a model for research. Psychological Review, 87,
301-315.GREEN, L., & RACHLIN, H. (1996). Commitment using
punishment. Journal of theExperimental Analysis of Behavior, 65(3):
593-601.HALPERIN, J. M., WOLF, L., GREENBLATT, E. R., & YOUNG,
G. (1991). Subtype
analysis of commission errors on the continuous performance test
in children.Developmental Neuropsychology, 7, 207-217.HALPERIN, J.
M., WOLF, L. E., PASCUALVACA, D. M., NEWCORN, J. H., HEALEY, J.M.,
O'BRIEN, J. D., MORGANSTEIN, A., &YOUNG, J. G. (1988).
Differentialassessment of attention and impulsivity in children.
Journal ofAmerican Academyof Child and Adolescent Psychiatry, 27,
326-329.HEATON, R. K., CURTISS, G., TUTTLE, K., & PAR STAFF
(1993). Wisconsin CardSorting Test: Computer (Version 2) [Computer
Software]. Odessa, FI:Psychological Assessment Resources, Inc
.KOCH, M., &MORGUET, M. (1985). Investigation in the use of a
vigilance test in psychomedical assessment. Blutalkohol, 22,
391-396.LOEBER, R. (1990). Development and risk factors of juvenile
antisocial behavior anddelinquency. Clinical Psychology Review, 10,
1-41.MILLER, R. C. (1984). The effect of ow doses ofalcohol on
human behavior. Unpublisheddoctoral thesis, University of Texas at
Austin.NUECHTERLEIN, K. H., & DAWSON, M. E. (1984). Information
proceSSing andattentional functioning in the developmental course
of schizophrenic disorders.Schizophrenia Bulletin, 10,
160-203.OLLMAN, R. (1966). Fast guess in choice reaction time.
Psychonomic Sciences, 6, 155-156.O'DOUGHERTY, M., NUECHTERLEIN, K.
H., & DREW, B. (1984). Hyperactive andhypoxic children: Signal
detection, sustained attention, and behavior. Journal ofAbnormal
Psychology, 93, 178-191.PATTON, J. M., STANFORD, M. S., &
BARRATT, E. S. (1995). Factor structure of theBarratt Impulsiveness
Scale. Journal of Clinical Psychology, 51, 768-774.QUAY, H. C.
(1988). The behavioral reward and inhibition system in childhood
behaviordisorder. In L. M. Bloomingdale (Ed.), Attention Deficit
Disorder (Vol. 3, pp. 176-186). New York: Spectrum.
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
17/18
CONDUCT DISORDER AND CPT PERFORMANCE 219
RACHLIN, H., RAINERI, A., & CROSS, D. (1991). Subjective
probability and delay.Journal of the Experimental Analysis of
Behavior, 55(2), 233-244.ROBERTS, L. E., RAU, H., LUlZENBERGER, W.,
&BIRBAUMER, N. (1994). MappingP300 waves onto inhibition:
Go/No-Go discrimination. Electroencephalographyand Clinical
Neurophysiology, 92, 44-55.ROSVOLD, H. E., MIRSKY, A., SARASON, I.,
BRANSOME, E. D., JR., & BECK, L. H.(1956). A continuous
performance test of brain damage. Journal of ConsultingPsychology,
20, 343-350.SCHACHAR, R. J., TANNOCK, R., & LOGAN, G. (1993).
Inhibitory control,impulsiveness, and attention deficit
hyperactivity disorder. Clinical PsychologyReview,
13,721-739.SERGEANT, J. A., & SHOLTON, C. A. (1985). On
resources strategy limitations inhyperactivity: Cognitive
impulsivity reconsidered. Journal of Child Psychology
andPsychiatry, 25, 809-819.SOSTEK, A. J., BUCHSBAUM, M. S., &
RAPOPORT, J. L. (1980). Effects ofamphetamine on vigilance
performance in normal and hyperactive children.Journal of Abnormal
Child Psychology, 8, 491-500.SPERLING, G. (1984). A unified theory
of attention and Signal detection. In R.Parasuraman &D. R.
Davies (Eds.), Varieties of attention (pp. 103-181). New
York:Academic.SPllZER, R. L., WILLIAMS, J. B. W., GIBBON, M., &
FIRST, M. B. (1990). Structuredclinical interview for DSM-III-R -
personality disorders (SCID-II, Version 1.0).Washington, DC:
American Psychiatric Press.SWANSON, L. (1981). Vigilance deficit in
learning disabled children: A signal detection
analysis. Journal of Child Psychology and Psychiatry, 22,
393-399.SYKES, D. H., DOUGLAS, V. I., & MORGENSTERN, G. (1973).
Sustained attention inhyperactive children. Journal of Child
Psychology and Psychiatry, 14, 213-220.SYKES, D. H., DOUGLAS, V.
I., WEISS, G., & MINDE, K. K. (1971). Attention inhyperactive
children and the effect of methylphenidate (Ritalin). Journal of
ChildPsychology and Psychiatry, 12, 129-139.WINDLE, M.,
&WINDLE, R. C. (1993). The continuity of behavioral expression
amongdisinhibited and inhibited childhood subtypes. Clinical
Psychology Review, 13, 741-761.WOHLBERG, G. W., & KORNETSKY, C.
(1973). Sustained attention in remittedschizophrenics. Archives of
General Psychiatry, 28, 533-537.YELLOT, J. I. (1971). Corrections
for fast guessing and speed-accuracy-tradeoff in choicereaction
time. Journal of Mathematical Psychology, 8,159-199.
-
8/2/2019 A Comparison Between Adults With Conduct Disorder
18/18
220 DOUGHERTY ET AL.