Embed Size (px)
Citation preview
1 3
Arch Gynecol ObstetDOI 10.1007/s00404-014-3175-y
GynecOlOGIc enDOcrInOlOGy AnD reprODuctIve MeDIcIne
A comparative study of obstetric outcomes in electively or spontaneously reduced triplet pregnancies
Emre Okyay · Sabahattin Altunyurt · Didem Soysal · Oktay Kaymak · Sunullah Soysal · Nuri Danisman · Bulent Gulekli
received: 13 May 2013 / Accepted: 31 January 2014 © Springer-verlag Berlin Heidelberg 2014
group. preterm delivery rates were significantly lower in both twin and elective reduction groups compared to tri-plet and spontaneous reduction groups (p < 0.001). pro-portion of women giving birth at term was not different in elective reduction and twin groups, and they were sig-nificantly higher compared to spontaneous reduction group (p = 0.024). perinatal mortality rates of both elective reduction and twin groups were significantly less than those in the triplet group (p = 0.045 and p < 0.001, respectively).Conclusions Obstetric outcomes of triplets from IvF or ovulation induction cycles undergoing elective reduction are better than ongoing triplet and spontaneous reduction groups and are similar to that of dichorionic twins.
Keywords Assisted reproduction · Multiple pregnancy · Fetal reduction · Outcomes
Introduction
Multiple pregnancies (Mps) are undesired complications of infertility treatments. In vitro fertilization (IvF) units extensively apply a variety of policies to avoid this compli-cation such as decreasing doses of drugs used in ovulation induction and restricting the number of transferred embryos in IvF cycles [1]. However, Mps in infertility treatments have not been entirely eliminated yet.
Multiple pregnancies are associated with adverse perina-tal outcomes including preeclampsia, gestational diabetes, preterm labor and prematurity and low birth weight infants [1–5]. It has been stated that increased perinatal mortality and morbidity rates are mainly related to gestational age and birth weight at delivery and they have been shown to be positively correlated with number of fetuses in Mps [1, 3, 6].
Abstract Purpose this study aimed at evaluating the pregnancy outcomes of IvF triplets which are spontaneously or elec-tively reduced to twins and to compare them with non-reduced triplets and twins.Methods retrospective analysis of trichorionic triplets and dichorionic twins of IvF pregnancies.Results preeclampsia rate was significantly higher in tri-plet group (p = 0.014). premature contractions requiring tocolysis were seen more often in spontaneous reduction and triplet groups compared to elective reduction and twin groups (p < 0.001). elective reduction and twin groups had significantly lower rate of infants weighing less than 1,500 g than those of triplets (p < 0.001). Highest rate for infants weighing over 2,500 g was found in primary twin
e. Okyay (*) Division of reproductive endocrinology, Department of Obstetrics and Gynecology, Dokuz eylul university School of Medicine, Balcova, 35340 Izmir, turkeye-mail: [email protected]
S. Altunyurt Division of perinatology, Department of Obstetrics and Gynecology, Dokuz eylul university School of Medicine, Izmir, turkey
D. Soysal Department of Obstetrics and Gynecology, Dokuz eylul university School of Medicine, Izmir, turkey
O. Kaymak · S. Soysal · n. Danisman Division of perinatology, Zekai tahir Burak Maternity teaching Hospital, Ankara, turkey
B. Gulekli Division of reproductive endocrinology, Department of Obstetrics and Gynecology, Dokuz eylul university School of Medicine, Izmir, turkey

Arch Gynecol Obstet
1 3
Multifetal pregnancy reduction is a procedure that is used to reduce triplets or higher order pregnancies to twin or singleton pregnancies to improve adverse outcomes. recently published studies and a meta-analysis have also shown that the fetal reduction (Fr) is associated with decreased rates of preterm birth, low birth weight, overall pregnancy loss in triplets reduced to twins [1, 7–11]. How-ever, other reports suggested that this relationship is not as pronounced in triplets as it is in quadruplets or even higher order multiple pregnancies. therefore, fetal reduction still remains a controversial subject in the management of tri-plets, although it reduces the rate of prematurity [6, 12–14]. this suggestion was attributed to the data that no signifi-cant differences were observed for perinatal mortality and the neonatal survival rates in triplets who did or did not undergo reduction to twins. this finding was attributed to recent progress in prenatal care of triplets in neonatal inten-sive care units [14].
Despite the fact that Fr has well-known positive influ-ences on pregnancy outcomes, improving results of expect-ant management of triplets are becoming much more important issues for practitioners who provide counseling to infertile couples about making a decision on their preg-nancies, because Fr leads to serious ethical, social, emo-tional problems and dilemmas on infertile couples. Addi-tionally, some couples having a triplet pregnancy at the beginning spontaneously lose one of their babies during the first trimester. However, there are a few studies about the outcomes of spontaneous reduction in the literature [9, 15, 16]. While Ata et al. [9] and Skiadas et al. [15] reported that spontaneous reduction and Fr have similar gestational length compared to primary twins, Dickey et al. [16] noted that they had lesser fetal weight and were born earlier than non-reduced twins.
In presented study, we aimed to report our experience in 43 cases of triplet pregnancies electively reduced to twins. In the literature, there are a few reports with a larger num-ber of cases regarding pregnancy outcomes in Sr or Fr of triplets in assisted reproductive pregnancies, but none of them had any data for antenatal complications such as preeclampsia, GDM, placental abruption and perinatal outcomes. therefore, we also aimed to present the data of prenatal complications as well as pregnancy outcomes of triplets which were spontaneously or electively reduced to twins and to analyze results of these two reduction groups by comparing them with expectantly managed triplets and primary twins.
Materials and methods
the study population consisted of women who achieved pregnancy after ovulation induction or assisted reproductive
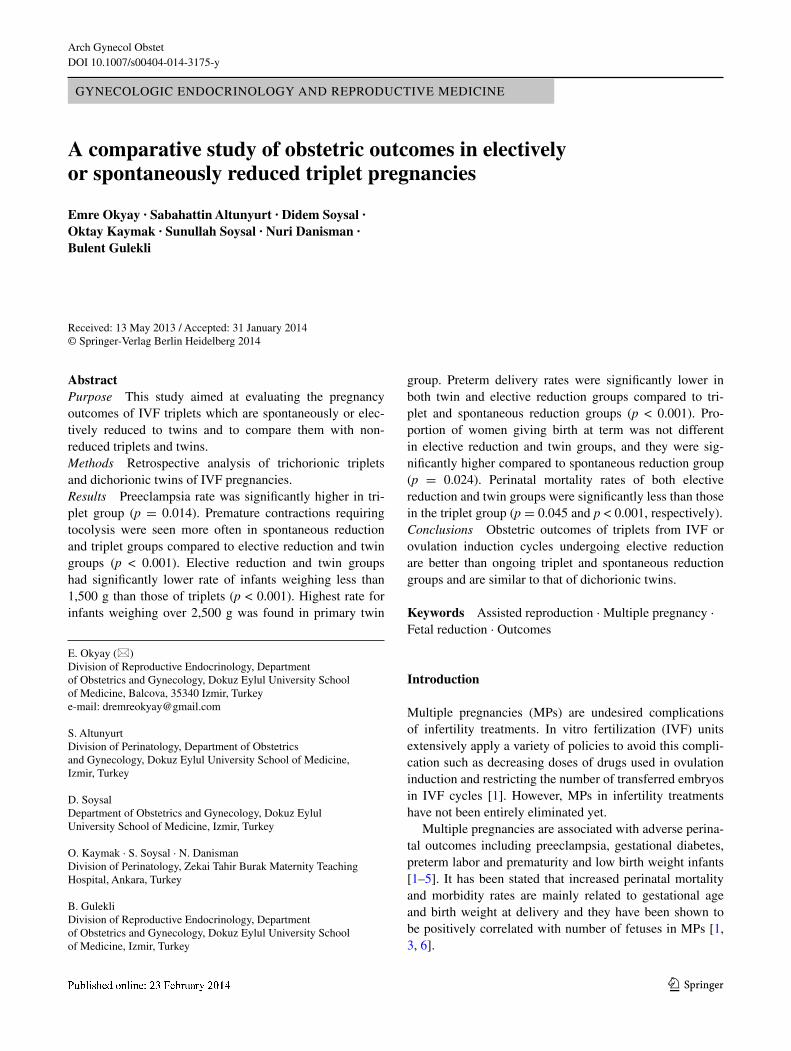
techniques at two institutions. One of these centers is Dokuz eylul university School of Medicine department of obstetrics and gynecology which is a tertiary referral center of Aegean region and the other one is Dr. Zekai tahir Burak research and training Hospital which is also a tertiary referral center of central Anatolia region in turkey. During study period, we found 1,945 ongoing clinical pregnancies that were the results of IvF or ovulation induction treat-ments and that were admitted to our antenatal outpatient clinic in the first trimester. there were 370 pregnancies with complete follow-up or pregnancy outcome informa-tion (Fig. 1). We analyzed perinatal data of 137 triplet preg-nancies, 43 of which were electively reduced (er group) and 29 of which were spontaneously reduced (Sr group) to twins in the first trimester during a 10-year period from January 2003 to June 2012. All patients were counseled by obstetricians for triplet pregnancy and fetal reduction pro-cedure. If the patient declined embryo reduction, she was expectantly managed (n = 65). patients who were expect-antly managed and completed pregnancy as triplet were included in the triplets group. Outcomes of these pregnan-cies were compared with those of the primary dizygotic twin pregnancies (twins group, n = 233). 170 patients who did not complete information about their obstetric follow-up, the triplets which had a monochorionic twin set or were reduced to singletons, monochorionic twin pregnancies and the quadruplets or higher order pregnancies reduced to twins were excluded. All women had ultrasonographic documentation of number of embryos with fetal heart beat activity within 8 weeks gestation. the gestational age was determined on the basis of the last menstrual period and confirmed by ultrasound. chorionicity was confirmed with ultrasonography and postnatal pathologic reports. this study was approved by the local research ethics commit-tees of two centers. Signed informed consent was provided from all women included in this study before recruitment. Selective fetal reduction procedure has been described pre-viously [17]. All procedures were performed transabdomi-nally by the same experienced operators (S.A. and n.D.) between 11 and 14 weeks’ gestation. Fetuses were chosen for reduction based on previously defined criteria [10, 18].
A diagnosis of preterm labor was made based on the clinical criteria of regular uterine contractions accompa-nied by a change in cervical dilation, effacement or both or initial presentation with regular contractions and cervical dilation of at least 2 cm between 20 0/7 weeks of gestation and 36 6/7 weeks of gestation according to the previously defined American college of Obstetrics and Gynecology criteria [19]. preeclampsia was defined as hypertension (systolic blood pressure ≥140 mmHg after 24 weeks gesta-tion) plus proteinuria (urine protein concentration ≥300 mg in a 24-h urine sample) [20]. Diagnosis of Gestational Dia-betes Mellitus (GDM) was made using a sequential model
Arch Gynecol Obstet
1 3
of universal screening with a 50-g 1 h glucose challenge test and if serum glucose level was >140 mg/dl at 1 h; procedure was followed by a diagnostic 100-g 3 h oral glucose tolerance test [21]. If more than one of four glu-cose values for a 3 h 100-g oral glucose tolerance test were abnormal (Fasting: greater than 95 mg/dl, 1 h: greater than 180 mg/dl, 2 h: greater than 155 mg/dl, 3 h: greater than 140 mg/dl) then the gestational diabetes was diagnosed.
perinatal mortality was defined as the fetal deaths that occur after 22 completed weeks of pregnancy and in the first 27 full days of life [22].
Statistical analysis was performed using Student t test, χ2 test (or the Fisher’s exact test) Mann–Whitney U test, One-way AnOvA or Kruskal–Wallis tests and univariate logistic regression test where appropriate. p < 0.05 was considered statistically significant.
Results
ninety-four of a total of 137 patients who had triplet preg-nancies did not accept fetal reduction procedure after
n = 1945 clinical pregnancies were admitted to antenatal outpatient clinic (All women were the result of IVF or ovulation induction treatments)
n = 1 had monochorionic twins pairs
n = 4 were spontaneously reduced to singleton
n = 1 was electively reduced to singleton
n = 65 Expectantly managed
n = 43 Electively reduced to twins
n = 1259 (64.7 %) were singleton
n = 686 (35.3 %) were multiple pregnancies
n = 7 (0.36 %) were quadruplets
n = 508 (26,1 %) were twins n = 178 (9.2 %) were triplets
n = 35 had no complete follow-up data or
were delivered another center
n = 137 Triplets had complete data and were included in the analysis
n = 29 Spontaneously reduced to twins
n = 37 were monochorionic twins
n = 68 were diagnosed "vanishing twin"
n = 170 had no complete follow-up data or
were delivered another center
n = 233 Primary twins had complete data and were included in the analysis
Fig. 1 patients’ flow charts
Arch Gynecol Obstet
1 3
counseling (94/137; 68,6 %). there was no significant dif-ference between the study groups for clinical characteris-tics of the cases (table 1).
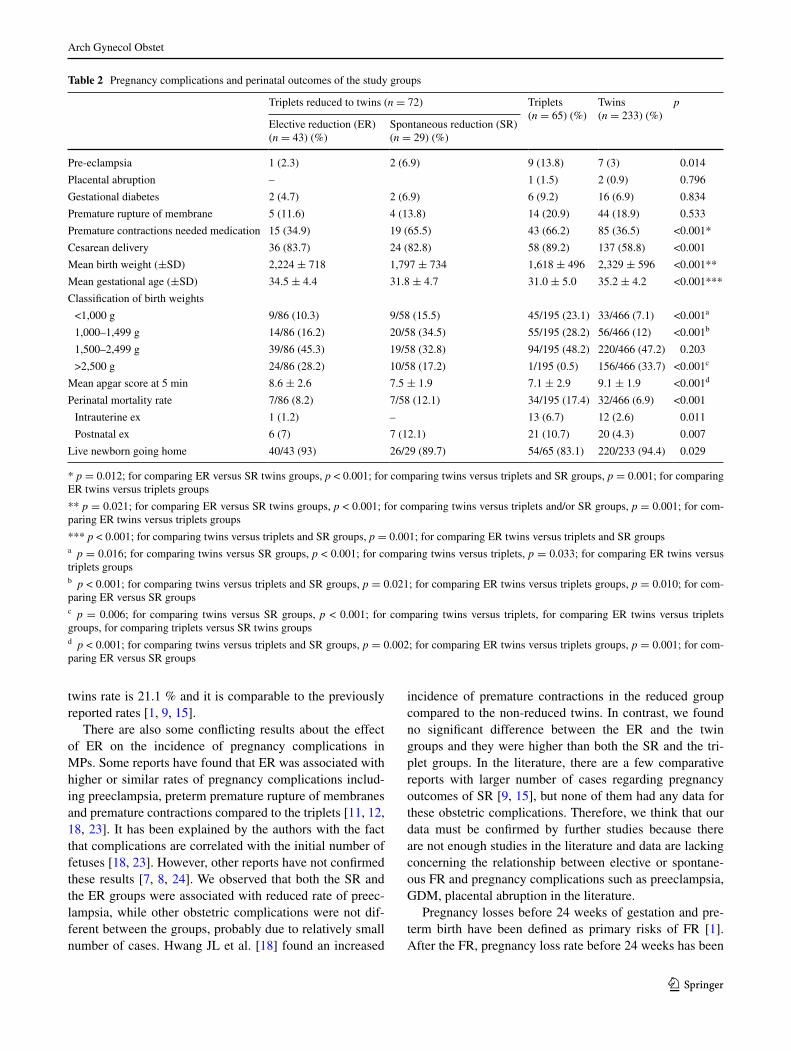
pregnancy complications and obstetric outcomes are shown in table 2. While we did not observe any signifi-cant differences in the rates of gestational diabetes and premature rupture of membranes between the groups, preeclampsia rate was significantly higher in the triplets group than in the other three groups. premature contrac-tions requiring tocolysis were seen more often in the Sr and the triplet groups compared to the er and the twin groups. But this difference was not found between the er and the twin groups and between the Sr and the tri-plet groups. comparison of the Apgar scores at 5 min, mean gestational age and birth weights showed similar results. For infants who weighed less than 1,000 g and between 1,000 and 1,500 g, the elective reduction and the twin groups had significantly lower rate than those of the triplets. there was no significant difference in the per-centage of infants below 1,000 g between the er and the Sr groups. However, for the infants weighing between 1,000 and 1,500 g, we observed that the Sr groups had significantly higher rate compared to the er group. the primary twin group had the highest rate for infants over 2,500 g.
the number of postnatal deaths was not significantly different between the groups except the twin versus the tri-plet groups and the twin versus the Sr groups (p = 0.003 and p = 0.021, respectively). Intrauterine fetal demise rate was significantly lower in both the twin and the Sr groups, compared with the triplet groups (p = 0.023 and p = 0.044, respectively). perinatal mortality rates in both the er and the twin groups were less than the triplet group. these results were significantly different (p = 0.045 and p < 0.001, respectively). However, there was a significant difference between the twins versus the triplet groups for the rate of at least one living newborn going home. When compared for the mode of delivery, the twins group had the lowest cesarean rates.
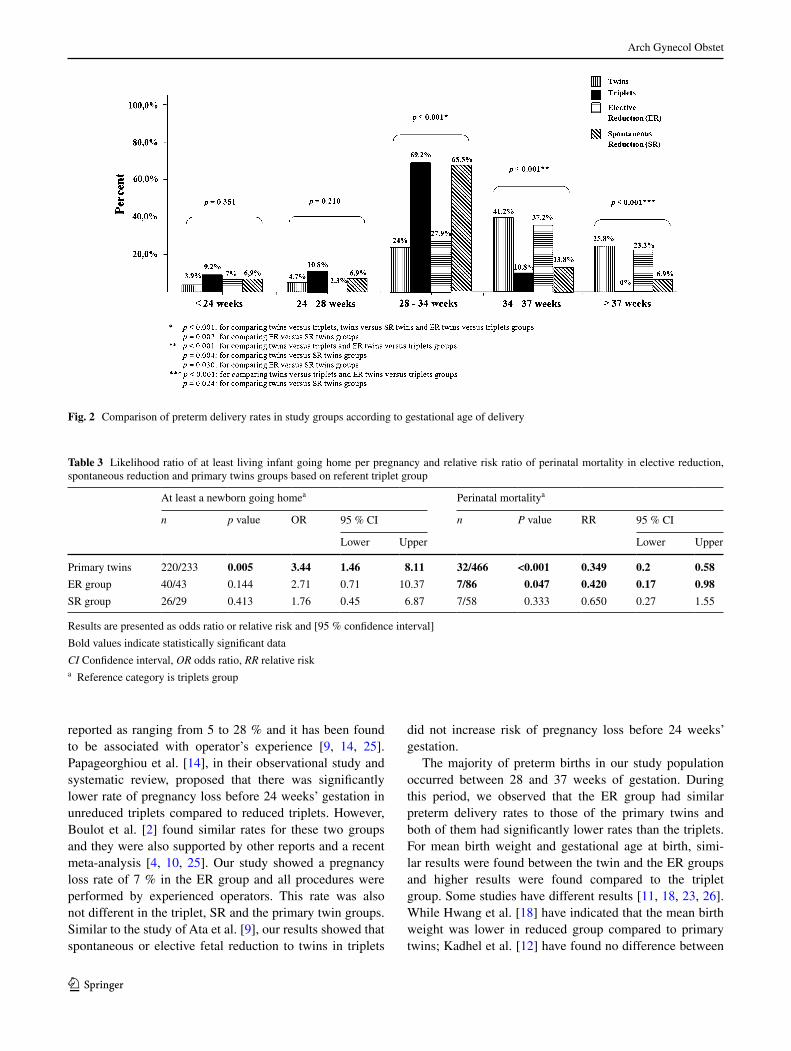
We also classified the gestational age at the time of delivery into four groups. two hundred and ninety-eight of a total of 370 patients (80.5 %) were diagnosed as preterm labor. Figure 2 shows preterm delivery rates in the groups based on this classification. the percentage of cases who delivered before 28 weeks of gestation was similar among the groups. Between 28 weeks to 37 weeks of gestation, preterm delivery rates were significantly lower in both the twin and the er groups compared to the triplet and the Sr groups. these rates were similar between the er and the twin groups and between the Sr and the triplet groups. the proportion of women giving birth at term was not differ-ent in the er and the twin groups, and it was significantly higher compared to the Sr group. none of the patients in the triplet group delivered after 37 weeks of gestation.
We also calculated the likelihood ratios of perinatal mor-tality and at least one infant going home for pregnancies in the twin, Sr and the er groups compared to triplet preg-nancies. compared to cases who continued triplet preg-nancy, the likelihood ratios of take-home at least a baby were not different for women who had either Sr or er. However, women who had er to twins or primary twins were significantly less likely to be exposed to perinatal mortality compared to the triplets and the Sr groups. these results are outlined in table 3.
Discussion
Although selective Fr should be considered as no doubt procedure for quadruplets or above [1], it is now a contro-versial issue for triplets, especially for pregnancies achieved with Arts, due to improving results of expectant managed triplets and raising social and ethical problems [13]. Dur-ing the study period, in our tertiary referral centers, we per-formed Fr to twin procedures in 43 of 137 (31.4 %) tricho-rionic triplets. this rate is lower than that in the previous reports [1, 9, 11, 15], probably due to moral and religious beliefs of our study population. Spontaneously reduced to
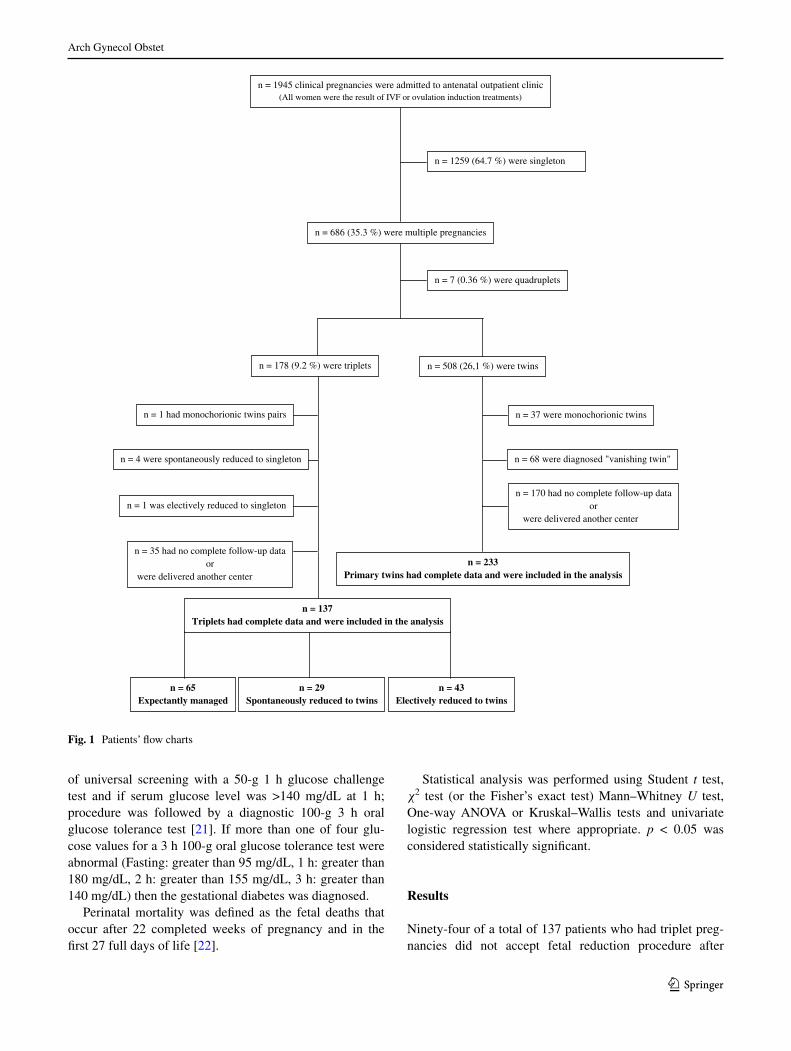
Table 1 comparison of the maternal ages and clinical data between the groups
a Data presented as mean ± SD
triplets reduced to twins (n = 72) triplets (n = 65) (%) twins (n = 233) (%) p
electively (n = 43) (%) Spontaneously (n = 29) (%)
Maternal age (years)a 29.6 ± 4.8 30.1 ± 4.4 28.9 ± 4.5 30.08 ± 5.3 0.388
primigravida (n) 40 (93) 24 (82.8) 54 (83.1) 190 (81.5) 0.132
pre-pregnancy BMI (kg/m2)a 23.6 ± 4.2 23.6 ± 3.8 26 ± 3.9 23.5 ± 3.7 0.912
Weight gain (g)a 15.9 ± 6.01 15.4 ± 6.1 19.5 ± 3.3 15.2 ± 6.1 0.218
Infertility treatment (n)
In vitro fertilization 43 (100) 28 (96.6) 61 (93.8) 210 (90.1) 0.103
Ovulation induction 0 1 (3.4) 4 (6.2) 23 (9.9)
Arch Gynecol Obstet
1 3
twins rate is 21.1 % and it is comparable to the previously reported rates [1, 9, 15].
there are also some conflicting results about the effect of er on the incidence of pregnancy complications in Mps. Some reports have found that er was associated with higher or similar rates of pregnancy complications includ-ing preeclampsia, preterm premature rupture of membranes and premature contractions compared to the triplets [11, 12, 18, 23]. It has been explained by the authors with the fact that complications are correlated with the initial number of fetuses [18, 23]. However, other reports have not confirmed these results [7, 8, 24]. We observed that both the Sr and the er groups were associated with reduced rate of preec-lampsia, while other obstetric complications were not dif-ferent between the groups, probably due to relatively small number of cases. Hwang Jl et al. [18] found an increased
incidence of premature contractions in the reduced group compared to the non-reduced twins. In contrast, we found no significant difference between the er and the twin groups and they were higher than both the Sr and the tri-plet groups. In the literature, there are a few comparative reports with larger number of cases regarding pregnancy outcomes of Sr [9, 15], but none of them had any data for these obstetric complications. therefore, we think that our data must be confirmed by further studies because there are not enough studies in the literature and data are lacking concerning the relationship between elective or spontane-ous Fr and pregnancy complications such as preeclampsia, GDM, placental abruption in the literature.
pregnancy losses before 24 weeks of gestation and pre-term birth have been defined as primary risks of Fr [1]. After the Fr, pregnancy loss rate before 24 weeks has been
Table 2 pregnancy complications and perinatal outcomes of the study groups
* p = 0.012; for comparing er versus Sr twins groups, p < 0.001; for comparing twins versus triplets and Sr groups, p = 0.001; for comparing er twins versus triplets groups
** p = 0.021; for comparing er versus Sr twins groups, p < 0.001; for comparing twins versus triplets and/or Sr groups, p = 0.001; for com-paring er twins versus triplets groups
*** p < 0.001; for comparing twins versus triplets and Sr groups, p = 0.001; for comparing er twins versus triplets and Sr groupsa p = 0.016; for comparing twins versus Sr groups, p < 0.001; for comparing twins versus triplets, p = 0.033; for comparing er twins versus triplets groupsb p < 0.001; for comparing twins versus triplets and Sr groups, p = 0.021; for comparing er twins versus triplets groups, p = 0.010; for com-paring er versus Sr groupsc p = 0.006; for comparing twins versus Sr groups, p < 0.001; for comparing twins versus triplets, for comparing er twins versus triplets groups, for comparing triplets versus Sr twins groupsd p < 0.001; for comparing twins versus triplets and Sr groups, p = 0.002; for comparing er twins versus triplets groups, p = 0.001; for com-paring er versus Sr groups
triplets reduced to twins (n = 72) triplets (n = 65) (%)
twins (n = 233) (%)
p
elective reduction (er) (n = 43) (%)
Spontaneous reduction (Sr) (n = 29) (%)
pre-eclampsia 1 (2.3) 2 (6.9) 9 (13.8) 7 (3) 0.014
placental abruption – 1 (1.5) 2 (0.9) 0.796
Gestational diabetes 2 (4.7) 2 (6.9) 6 (9.2) 16 (6.9) 0.834
premature rupture of membrane 5 (11.6) 4 (13.8) 14 (20.9) 44 (18.9) 0.533
premature contractions needed medication 15 (34.9) 19 (65.5) 43 (66.2) 85 (36.5) <0.001*
cesarean delivery 36 (83.7) 24 (82.8) 58 (89.2) 137 (58.8) <0.001
Mean birth weight (±SD) 2,224 ± 718 1,797 ± 734 1,618 ± 496 2,329 ± 596 <0.001**
Mean gestational age (±SD) 34.5 ± 4.4 31.8 ± 4.7 31.0 ± 5.0 35.2 ± 4.2 <0.001***
classification of birth weights
<1,000 g 9/86 (10.3) 9/58 (15.5) 45/195 (23.1) 33/466 (7.1) <0.001a
1,000–1,499 g 14/86 (16.2) 20/58 (34.5) 55/195 (28.2) 56/466 (12) <0.001b
1,500–2,499 g 39/86 (45.3) 19/58 (32.8) 94/195 (48.2) 220/466 (47.2) 0.203
>2,500 g 24/86 (28.2) 10/58 (17.2) 1/195 (0.5) 156/466 (33.7) <0.001c
Mean apgar score at 5 min 8.6 ± 2.6 7.5 ± 1.9 7.1 ± 2.9 9.1 ± 1.9 <0.001d
perinatal mortality rate 7/86 (8.2) 7/58 (12.1) 34/195 (17.4) 32/466 (6.9) <0.001
Intrauterine ex 1 (1.2) – 13 (6.7) 12 (2.6) 0.011
postnatal ex 6 (7) 7 (12.1) 21 (10.7) 20 (4.3) 0.007
live newborn going home 40/43 (93) 26/29 (89.7) 54/65 (83.1) 220/233 (94.4) 0.029
Arch Gynecol Obstet
1 3
reported as ranging from 5 to 28 % and it has been found to be associated with operator’s experience [9, 14, 25]. papageorghiou et al. [14], in their observational study and systematic review, proposed that there was significantly lower rate of pregnancy loss before 24 weeks’ gestation in unreduced triplets compared to reduced triplets. However, Boulot et al. [2] found similar rates for these two groups and they were also supported by other reports and a recent meta-analysis [4, 10, 25]. Our study showed a pregnancy loss rate of 7 % in the er group and all procedures were performed by experienced operators. this rate was also not different in the triplet, Sr and the primary twin groups. Similar to the study of Ata et al. [9], our results showed that spontaneous or elective fetal reduction to twins in triplets
did not increase risk of pregnancy loss before 24 weeks’ gestation.
the majority of preterm births in our study population occurred between 28 and 37 weeks of gestation. During this period, we observed that the er group had similar preterm delivery rates to those of the primary twins and both of them had significantly lower rates than the triplets. For mean birth weight and gestational age at birth, simi-lar results were found between the twin and the er groups and higher results were found compared to the triplet group. Some studies have different results [11, 18, 23, 26]. While Hwang et al. [18] have indicated that the mean birth weight was lower in reduced group compared to primary twins; Kadhel et al. [12] have found no difference between
Fig. 2 comparison of preterm delivery rates in study groups according to gestational age of delivery
Table 3 likelihood ratio of at least living infant going home per pregnancy and relative risk ratio of perinatal mortality in elective reduction, spontaneous reduction and primary twins groups based on referent triplet group
results are presented as odds ratio or relative risk and [95 % confidence interval]
Bold values indicate statistically significant data
CI confidence interval, OR odds ratio, RR relative riska reference category is triplets group
At least a newborn going homea perinatal mortalitya
n p value Or 95 % cI n P value rr 95 % cI
lower upper lower upper
primary twins 220/233 0.005 3.44 1.46 8.11 32/466 <0.001 0.349 0.2 0.58
er group 40/43 0.144 2.71 0.71 10.37 7/86 0.047 0.420 0.17 0.98
Sr group 26/29 0.413 1.76 0.45 6.87 7/58 0.333 0.650 0.27 1.55

Arch Gynecol Obstet
1 3
reduced and non-reduced triplets for birth weight. How-ever, our findings were consistent with many other reports with larger case series and a recent published meta-analysis [1, 4, 7, 9, 10, 14, 15, 25]. no patient was observed in our triplet group giving birth after 37 weeks of gestation. there were no significant differences between the er group and the primary twins for delivery at this gestational age. primary twins had the highest rate for giving birth after 37 weeks of gestation. classification of birth weights into four categories showed significantly lower rates in both the er and the twin groups for the rates of birth weight less than 1,000 and 1,500 g compared to the triplets group. correspondingly, we observed that the rate of infants born weighing above 2,500 g was higher in these groups. there-fore, as in preterm deliveries pregnancy outcomes have been suggested to be strongly dependent on mean birth weight and gestational age, we think that probably improv-ing results related to the er procedure might be attributed to this consideration. Differently, in the spontaneous reduc-tion group, mean birth weight and mean gestational age at birth were lower than primary twins. We also observed sig-nificant differences between the Sr and the primary twin groups in all birth weight groups and the Sr group had higher incidence of preterm delivery. Our findings support a recently noted suggestion that Sr was associated with diminished birth weight and gestational length compared to unreduced controls having same number of fetuses [16]. Although Ata et al. [9] have found higher preterm delivery rates in their Sr groups compared to primary twins, unlike our findings, they have concluded that there were no dif-ferences between the groups with regard to gestational length. these conflicting results may be due to relatively small case series in a few reports and in our study over 37 weeks of gestation was regarded as term pregnancy. In our comparative analysis of the er and the Sr groups, for birth weight under 1,000 g and above 2,500 g, the Sr and the er groups were not different, whereas the Sr group had significantly higher rates than the er group for those between 1,000 and 1,500 g. Similarly, there is no difference in preterm birth rate before 28 weeks and after 37 weeks of gestation between the Sr and the er groups. these results are consistent with the other two reports compared to Sr [9, 15]. Although we detected no significant differ-ences between the triplet and the Sr groups for mean birth weight, gestational age at birth and birth weight groups under 2,500 g, a higher incidence of term pregnancies after 37 weeks of gestation and birth weight above 2,500 g were observed in the Sr group compared to the triplets. In other two previous reports, there were no data for comparative analysis based on birth weight. therefore, these findings should also be confirmed by further studies.
Our study demonstrated that perinatal mortality rate in both the er and the twin groups were less than the triplet
group. correspondingly, our univariate analysis showed that the relative risks for perinatal mortality referred to tri-plets were 0.34 (95 % cI, 0.2–0.58) for primary twins and 0.42 (95 % cI, 0.17–0.98) for elective reduction group. Also, papageorghiou At et al. [14], in their study and sys-tematic review, concluded that although er reduced the rate of preterm delivery in triplets, it did not influence perinatal mortality rate. In contrast, in a recent cochrane analysis and another meta-analysis [7, 27], supporting our findings, it has been revealed that er is associated with a decreased risk according to both preterm delivery and neonatal death. Ata B et al. [9], in their study, have concluded that Sr was similar to primary twins for obstetric outcomes. However, in our regression analysis, we observed that Sr did not have any reducing effect in perinatal mortality compared to the triplets. Sr group had less improving outcomes and this finding supports the hypothesis that placental impair-ments due to intrauterine “crowding” and multiple implan-tation sites might cause spontaneous reduction which might lead to other complications in advanced period of gestation. Although our study suggested that obstetric outcomes of er was similar to primary twins, we think that further studies including large number of cases are required to do a similar proposition in terms of pregnancy outcomes of Sr.
In conclusion, elective fetal reduction, compared with expectantly managed triplets seems to be associated with decreased obstetric complications and preterm delivery rates, increased gestational age at birth and birth weight as well as improved perinatal mortality rates regardless of increased miscarriage rates. Also, outcomes are compa-rable to those of primary twins. therefore, it is an impor-tant treatment option for higher order multiple pregnancies although there are several challenges of ethical and moral beliefs. these protective effects of fetal reduction on preg-nancy outcomes and perinatal mortality rates appear to be limited in triplets which were spontaneously reduced to twins. However, comparative, prospective, well-designed further studies with longer follow-up and larger number of cases are needed between presented study groups for ante-natal, perinatal and early and late postnatal outcomes, par-ticularly in infertile couples.
Conflict of interest none.
References
1. practice committee of American Society for reproductive Medi-cine (2012) Multiple gestation associated with infertility therapy: an american society for reproductive medicine practice commit-tee opinion. Fertil Steril 97:825–834
2. Boulot p, vignal J, vergnes c, Dechaud H, Faure JM, Hedon B (2000) Multifetal reduction of triplets to twins: a prospective comparison of pregnancy outcome. Hum reprod 15:1619–1623
Arch Gynecol Obstet
1 3
3. Ferraretti Ap, Goossens v, de Mouzon J, Bhattacharya S, cas-tilla JA, Korsak v et al (2012) european IvF-monitoring (eIM); consortium for european Society of Human reproduction and embryology (eSHre). Assisted reproductive technology in europe, 2008: results generated from european registers by eSHre. Hum reprod 27(9):2571–2584
4. Antsaklis A, Souka Ap, Daskalakis G, papantoniou n, Koutra p, Kavalakis y, Mesogitis S (2004) embryo reduction versus expect-ant management in triplet pregnancies. J Matern Fetal neonatal Med 16(4):219–222
5. Hasson J, Shapira A, Many A, Jaffa A, Har-toov J (2011) reduc-tion of twin pregnancy to singleton: does it improve pregnancy outcome? J Matern Fetal neonatal Med 24(11):1362–1366
6. Skrablin S, Kuvacic I, Jukic p, Kalafatic D, peter B (2002) Hos-pitalization vs. outpatient care in the management of triplet gesta-tions. Int J Gynaecol Obstet 77(3):223–229
7. Dodd J, crowther c (2004) Multifetal pregnancy reduction of tri-plet and higher-order multiple pregnancies to twins. Fertil Steril 81(5):1420–1422
8. yaron y, Bryant-Greenwood pK, Dave n, Moldenhauer JS, Kramer rl, Johnson Mp, evans MI (1999) Multifetal pregnancy reductions of triplets to twins: comparison with nonreduced tri-plets and twins. Am J Obstet Gynecol 180(5):1268–1271
9. Ata B, rasillo lJ, Sukhdeo S, Son Wy, tan Sl, Dahan MH (2011) Obstetric outcomes of IvF trichorionic triamniotic triplets which are spontaneously or electively reduced to twins. J Assist reprod Genet 28(12):1217–1222
10. Wimalasundera rc (2010) Selective reduction and termination of multiple pregnancies. Semin Fetal neonatal Med 15(6):327–335
11. lipitz S, uval J, Achiron r, Schiff e, lusky A, reichman B (1996) Outcome of twin pregnancies reduced from triplets compared with nonreduced twin gestations. Obstet Gynecol 87(4):511–514
12. Kadhel p, Olivennes F, Fernandez H, vial M, Frydman r (1998) Are there still obstetric and perinatal benefits for selective embryo reduction of triplet pregnancies? Hum reprod 13(12):3555–3559
13. Skrablin S, Kuvacic I, Kalafatic D, peter B, Gveric-Ahmeta-sevic S, letica-protega n, polak-Babic J (2002) perinatal care improves the outcome of triplets. eur J Obstet Gynecol reprod Biol 104(1):26–31
14. papageorghiou At, Avgidou K, Bakoulas v, Sebire nJ, nicolaides KH (2006) risks of miscarriage and early preterm birth in tricho-rionic triplet pregnancies with embryo reduction versus expect-ant management: new data and systematic review. Hum reprod 21(7):1912–1917
15. Skiadas cc, Missmer SA, Benson cB, Acker D, racowsky c (2011) Spontaneous reduction before 12 weeks’ gestation and selective reduction similarly extend time to delivery in in vitro
fertilization of trichorionic-triamniotic triplets. Fertil Steril 95(2):596–599
16. Dickey rp, taylor Sn, lu py, Sartor BM, Storment JM, rye pH et al (2002) Spontaneous reduction of multiple pregnancy: inci-dence and effect on outcome. Am J Obstet Gynecol 186(1):77–83
17. Berkowitz rl, lynch l, lapinski r, Bergh p (1993) First-trimester transabdominal multifetal pregnancy reduction: a report of two hundred completed cases. Am J Obstet Gynecol 169(1):17–21
18. Hwang Jl, pan HS, Huang lW, lee cy, tsai yl (2002) com-parison of the outcomes of primary twin pregnancies and twin pregnancies following fetal reduction. Arch Gynecol Obstet 267(2):60–63
19. American college of Obstetricians and Gynecologists, com-mittee on practice Bulletins—Obstetrics (2012) AcOG practice bulletin no. 127: Management of preterm labor. Obstet Gynecol 119(6):1308–1317
20. Brown MA, lindheimer MD, de Swiet M, van Assche A, Moutquin JM (2001) the classification and diagnosis of the hypertensive disorders of pregnancy: statement from the Inter-national Society for the Study of Hypertension in pregnancy (ISSHp). Hypertens pregnancy 20(1):IX–XIv
21. Kaymak O, Iskender ct, ustunyurt e, yildiz y, Doganay M, Danisman n (2011) retrospective evaluation of perinatal out-come in women with mild gestational hyperglycemia. J Obstet Gynaecol res 37(8):986–991
22. tanaka S, Stock SJ, yamamoto y, Kondejewski J, Olson DM (2010) understanding perinatal mortality. Obstet Gynecol 20(11):317–322
23. Groutz A, yovel I, Amit A, yaron y, Azem F, lessing JB (1996) pregnancy outcome after multifetal pregnancy reduction to twins compared with spontaneously conceived twins. Hum reprod 11(6):1334–1336
24. Smith-levitin M, Kowalik A, Birnholz J, Skupski DW, Hut-son JM, chervenak FA, rosenwaks Z (1996) Selective reduc-tion of multifetal pregnancies to twins improves outcome over nonreduced triplet gestations. Am J Obstet Gynecol 175(4 pt 1):878–882
25. leondires Mp, ernst SD, Miller Bt, Scott rt Jr (2000) triplets: outcomes of expectant management versus multifetal reduction for 127 pregnancies. Am J Obstet Gynecol 183(2):454–459
26. Melgar cA, rosenfeld Dl, rawlinson K, Greenberg M (1991) perinatal outcome after multifetal reduction to twins compared with nonreduced multiple gestations. Obstet Gynecol 78(5 pt 1):763–767
27. Dodd JM, crowther cA (2003) reduction of the number of fetuses for women with triplet and higher order multiple pregnan-cies. cochrane Database Syst rev (2):cD003932





![Omphalocele, exstrophy of cloaca, imperforate anus and …oaji.net/pdf.html?n=2015/1334-1433441479.pdf · sonography may indicate an OEIS complex [3,7]. Many pregnancies electively](https://img.pdfslide.us/doc/110x75/5ae31d867f8b9a5d648d7b24/omphalocele-exstrophy-of-cloaca-imperforate-anus-and-oajinetpdfhtmln20151334-.jpg)