Embed Size (px)
Citation preview

i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 1022–1033
journa l h omepage: www.i jmi journa l .com
A combined disease management and process modelingapproach for assessing and improving care processes: A fallmanagement case-study
Marjan Askaria,∗, Richard Westerhofb, Saied Eslamia, Stephanie Medlocka,Sophia E. de Rooij c, Ameen Abu-Hannaa
a Department of Medical Informatics, Academic Medical Center, Amsterdam, The Netherlandsb Dutch College of General Practitioners, The Netherlandsc Department of Internal and Geriatric Medicine, Academic Medical Center, Amsterdam, The Netherlands
a r t i c l e i n f o
Article history:
Received 4 November 2012
Received in revised form
14 June 2013
Accepted 15 June 2013
Keywords:
Process modeling
Disease management
Healthcare process assessment
Quality of care evaluation
a b s t r a c t
Objectives: To propose a combined disease management and process modeling approach for
evaluating and improving care processes, and demonstrate its usability and usefulness in a
real-world fall management case study.
Methods: We identified essential disease management related concepts and mapped them
into explicit questions meant to expose areas for improvement in the respective care pro-
cesses. We applied the disease management oriented questions to a process model of a
comprehensive real world fall prevention and treatment program covering primary and
secondary care. We relied on interviews and observations to complete the process models,
which were captured in UML activity diagrams. A preliminary evaluation of the usability
of our approach by gauging the experience of the modeler and an external validator was
conducted, and the usefulness of the method was evaluated by gathering feedback from
stakeholders at an invitational conference of 75 attendees.
Results: The process model of the fall management program was organized around the clin-
ical tasks of case finding, risk profiling, decision making, coordination and interventions.
Applying the disease management questions to the process models exposed weaknesses in
the process including: absence of program ownership, under-detection of falls in primary
care, and lack of efficient communication among stakeholders due to missing awareness
about other stakeholders’ workflow.
The modelers experienced the approach as usable and the attendees of the invitational
conference found the analysis results to be valid.
Conclusions: The proposed disease management view of process modeling was usable and
useful for systematically identifying areas of improvement in a fall management program.
Although specifically applied to fall management, we believe our case study is characteristic
nage
of various disease ma∗ Corresponding author at: Academic Medical Center, Department of
Netherlands. Tel.: +31 20 5667875; fax: +31 20 6919840.E-mail address: [email protected] (M. Askari).
1386-5056/$ – see front matter © 2013 Elsevier Ireland Ltd. All rights reshttp://dx.doi.org/10.1016/j.ijmedinf.2013.06.011
ment settings, suggesting the wider applicability of the approach.
© 2013 Elsevier Ireland Ltd. All rights reserved.
Medical Informatics, Meibergdreef 15, 1105 AZ Amsterdam, The
erved.

i n f
1
1
ActAitioctaui
ofiscafusttapaafsiatictcfls
dtii
1
ADmtwee[
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l
. Introduction
.1. Process modeling (PM)
process is a series of activities, for example a business pro-ess is a set of business activities that are ordered accordingo a set of procedural rules with service delivery as its goal.
model of a (business) process describes, often diagrammat-cally, how components in that process work and collaborateogether; it provides a high level specification of processes thats independent of any management system [1]. An importantbjective of a process model is its applicability as a conceptualonstruct for better understanding and communicating abouthe components of the underlying process. Sometimes it islso used for inference, for example to simulate the processnder various conditions or to redesign the process to improve
ts efficiency or feasibility.Among the various approaches to process modeling, object
riented (OO) methods are particularly popular [1,2]. The Uni-ed Modeling Language (UML) is an important OO modelingtandard and consists of a language for specifying, visualizing,onstructing and documenting software and non-softwarertifacts [3]. UML is a composite of various diagram typesor static and dynamic models. The static diagrams show thenderlying structure of a system (such as the components andtructure of an organization). The dynamic diagrams capturehe behavior and interactions of the components in a sys-em. Central to process description in UML is the concept ofctivity [2,4]. The activity diagram offers comprehensive sup-ort for the workflow (process flow) and data perspectives,llowing the majority of the constructs encountered whennalyzing this perspective to be directly captured [2,3]. There-ore we used the UML activity diagram (UML-AD) to representequences of actions for this study. Although process model-ng has been widely applied to branches such as industry, it haslso been recently applied to health care [5–8]. An example ofhe application of UML (activity, use-case, and class diagrams)n health care is the visualization of the hospital-based can-er registration processes by Shiki et al. [5]. The approach inhis work is valuable because it demonstrates how systemati-ally modeling and visualizing the core activities, informationows, and the staff involved had contributed to a comprehen-ive understanding of how (cancer) registries work.
Current work in process modeling focuses on how toescribe and visualize processes systematically. However,here is little uniformity on how to use these models for qual-ty assessment of the underlying processes, especially whent comes to emerging health care provision strategies.
.2. Disease management (DM)
ccording to the Care Continuum Alliance (CCA) (formerlyisease Management Association of America, DMAA), diseaseanagement is a system of coordinated health care interven-
ions and communications for populations with conditions in
hich patient self-care efforts are significant [9]. DM is a strat-gy aimed at providing efficient and effective care for patients,specially to those patients suffering from chronic conditions10]. The goal of disease management is to provide effective
o r m a t i c s 8 2 ( 2 0 1 3 ) 1022–1033 1023
and efficient care to a specific patient group by, among otherthings, improving the involvement of the patient, task transferof (collaborative) work (for example from specialist to generalpractitioner), and the use of scientific evidence in clinical prac-tice [11,12]. In Europe, increasingly more hospitals and otherlocal care organizations practice their own disease manage-ment programs at the micro level, which have been successful.These programs should be emulated in full delivery systems,to realize these same advantages on a larger scale [13].
The CCA lists the following components of full-service dis-ease management:
• Population identification processes;• Evidence-based practice guidelines;• Collaborative practice models to include physician and
support-service providers;• Patient self-management education (may include primary
prevention, behavior modification programs, and compli-ance/surveillance);
• Process and outcomes measurement, evaluation, and man-agement;
• Routine reporting/feedback loop (may include communi-cation with patient, physician, health plan and ancillaryproviders, and practice profiling).
DM essentially consists of desiderata that the provided careshould meet. Evaluations of the disease management pro-grams are often methodologically difficult [12,14]. DM does notprovide a systematic link between these desiderata and pre-specified properties of the underlying health care provision.This impedes assessment of the extent to which an alreadyimplemented health care program is DM-compliant, and inturn, misses opportunities to systematically improve compo-nents or the whole program by increasing its compliance toDM requirements.
There are relevant attempts at assessing the effective-ness of integrated care programs, for example, those basedon elements of the Chronic Care Model (CCM) [15]. CCM isan evidence based conceptual model developed by Wagneret al. in 2001 [16] for care delivery to chronic care patients.Although CCM and DM use or emphasize different compo-nents [12], they do share many objectives such as the needto manage increasingly complex multidisciplinary care forchronic patients. The following concepts in CCM are alreadyaddressed in DM: “patient education”, “guideline use”, “infor-mation systems”, and “personnel type”. There is also clearoverlap in the concepts “system delivery design” and “self-management” in both CCM and DM. In contrast, the conceptof “provider education” from CCM is not addressed explicitly inDM. Like DM, CCM lacks a systematic link between its desider-ata and assessment of the underlying health care provision.Therefore, in their study [15] Wagner et al. designed a shortsurvey to enquire about the implementation state of CCM con-cepts for health care programs. The survey was then appliedto chronic care management programs using interviews andsite visits [15]. The topics of the survey are stated at a high
level of abstraction making it useful to globally characterizeand assess a large number of care programs. The survey top-ics are however not geared toward a detailed assessment fora particular care program.
1024 i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 1022–1033
Table 1 – DM concepts and related key questions for evaluating the care processes.
DM Interpretation Questions Examples of assessment andquality improvement
questions
Populationidentificationprocesses
There exists aspecific patientpopulation and acorrespondingmechanism for itsidentification.
• Is there a populationidentification mechanism thatidentifies members of thispopulation?
• To what extent does theidentification process tax thesubjects?
• Is there a mechanism to obtainthe sensitivity and specificity ofthe screening instrument withinthe subpopulation?
• What is the sensitivity andspecificity of the screeninginstrument?
• Is there an administrative systemfor tracing the subjects that refuseto participate or subjects that testnegatively at the moment ofpopulation identification?• Is there any mechanism to findthe reasons for refusing the test?
Evidence-basedpractice guidelines
Use of evidencebased guidelines andpracticingevidence-basedmedicine.
• Are there evidence-basedguidelines available at the decisionmaking moments?
• What is the level of adherence toguidelines?
• Is there a maintenancemechanism within the currentprocesses for evidence basedguidelines?
• To which degree do the peopleresponsible for following theguideline agree with the whole orpart of the guideline(s)?
• Is there a mechanism to measurethe agreement on the whole orpart of the guideline(s)?
• Where in the process canguideline based decision supportbe used?
• Is there a computerized decisionsupport system (CDSS), providingfeedback such as alerts orreminders, available at thedecision making moments?
Collaborativepractice models toinclude physicianand support-serviceproviders
Collaborative modelsin which all theparticipantslink/share thecommunityresources inside andoutside of theorganization.
• Are there defined roles, includingprotocols, among participants? Isthere an explicit process owner?
• Are stakeholders aware of theirpartners?
• Is there a systemdelivering/explaining the type ofservices provided by otherparticipants in the program?
• How optimal is the use of otherresources?
• Is there a mechanism tointroduce and facilitate the use ofa partner’s resources?
Patientself-managementand education
Includes primaryprevention, behaviormodificationprograms, and com-pliance/surveillance
• Is there a patientself-management program (e.g.primary prevention program)available?
• Is the self-management programaligned with the goals of theprogram?
• Is there a mechanism to motivatethe patient to attend the program?
• Is the patient empowered forher/his crucial role in maintaininghis/her health? If not, how shouldempowerment be promoted?
• Is there a mechanism to assessthe patient’s knowledge andcapabilities in order to adapt theself-management educationprogram to provide tailoredinformation?
• What is the effect of theself-management education on(e.g.) awareness, knowledge,behavior of the patient and patientoutcomes?
• Is there a program for continuouseducation?

i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 1022–1033 1025
Table 1 (Continued)
Process andoutcomesmeasurement,evaluation, andmanagement
Includes evaluationsof the processes, andoutcomemeasurement
• Are (key) process and outcomequality indicators defined?
• Are the (key) quality indicatorsdefined according to explicitcriteria?
• Is there a mechanism to registerthe (key) quality indicators andoutcome?• Is there a mechanism to evaluatethe quality of care based on theindicators?• Is there a continuous monitoringmechanism available?• Is there a mechanism for actingupon the (key) quality indicators?
Routinereporting/feedbackloop to individualsparticipating in theprocess (patient,
Includescommunication withpatient, physician,health plan andother providers, and
• Is there a mechanism to report tothe stakeholders including theprocess owner?
• Where can technology, such asIT, be used for feedback andreporting?
• Are there report templates forthe individual participants?
• How should a routinereporting/feedback loop be
gecme
mictm
1
Taac
avTttfcmmgda
1
Taic
physician, etc.) practice profiling
Another work suggested the Development Model for Inte-rated Care (DMIC), which described nine clusters of 89lements that are thought to contribute to the integration ofare [17]. This framework overlaps with DM and CCM and isore detailed than both, but like DM and CCM it does not
xploit process models for assessing the care programs.Hence, in spite of efforts toward standardizing measure-
ent and evaluation of DM principles or other evaluation andmprovement methods [14,15,18], no attempts were made toombine process modeling and structured desiderata to assesshe quality of care programs and identify areas for improve-
ent.
.3. Aim
he aim of this paper was to propose and evaluate a combinedpproach of DM and PM in which process models constituten important link between the DM desiderata and the healthare program.
Specifically, we propose in this paper a combined PM-nd DM-oriented approach in which process models areiewed and systematically assessed from a DM perspective.his DM perspective is represented by a series of ques-
ions, distilled from the DM desiderata that analysts needo address. We aim to demonstrate the usability and use-ulness of this approach to a real-world fall managementase-study. Our approach is meant to contribute to PMethodology by enriching it with an accessible proceduralethod for examining processes of disease management pro-
rams, and to the analysis and improvement of other specificisease management programs by the application of thispproach.
.4. Case study: fall-management
o illustrate our approach, we apply it to a case study of fall prevention program. Falls in elderly persons form anmportant societal problem and a major public health con-ern [19–21]. This is of particular concern in western countries
generated?
such as the Netherlands due to the increasing number ofpersons aged 65 years and older (increase from 2.15 mil-lion in 2000 to 2.72 million in 2012). The increase in thenumber of persons of 80 years and older is even sharper,comprising a 37% increase from 500,339 in 2000 to 686,015in 2012 [22]. Annually, about 30% of the community-dwellingpersons aged 65 years and older fall once, and around 15%fall twice or more [19,20]. The high incidence and severeconsequences of falls underlie the need for primary and sec-ondary preventive measures. Although an increased fall riskis not a disease, management of all risk factors contributingto the fall risk shares many characteristics of disease man-agement in terms of focusing on a specific subpopulation,having a population-based approach to identify persons atrisk, intervening with specific programs of care, shared care,and measuring clinical and other outcomes. There are someinitiatives addressing the process of fall prevention programs,but focusing on only specific aspects such the informationinfrastructure underlying the process [23,24]. There is hencestill a need for systematic methods for integrally describing,evaluating and improving the process of fall prevention andmanagement.
Our case study involves a homecare organization, sixprimary care practices, and two departments of a ter-tiary university teaching hospital, the Amsterdam AcademicMedical Center: an emergency department and a ded-icated (secondary) fall prevention outpatient clinic. Thefall-management program was set up as a cooperativeeffort to coordinate care for fall-prone patients betweenthese facilities. Representatives from all stakeholders, includ-ing nurses specialized in falls, primary care physicians,geriatricians and other clinicians, and managers partici-pated in the study. Although patients are also stake-holdersin this case-study, we did not involve them yet becausethe focus was mainly on the characteristics of the pro-cess of provided care. Patients’ involvement would be
especially beneficial in addressing in-depth quality assess-ment such as the questions stated in the last column ofTable 1.
1026 i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 1022–1033
Table 2 – Result of the final analysis based on the whole fall management program.
DM concepts Questions Application bythe modelera
Application bythe externalvalidationb
Population identificationprocesses
• Is there a populationidentification mechanism thatidentifies members of thispopulation?
Yes Yes
• Is there a mechanism to obtainthe sensitivity and specificity ofthe screening instrument withinthe population?
No Not able to answer
• Is there an administrative systemfor tracing the subjects that refuseto participate or subjects that testnegatively at the moment ofpopulation identification?
No No
• Is there any mechanism to findthe reasons for refusing the test?
Yes Yes
Evidence-basedpractice guidelines
• Are there evidence-basedguidelines available at the decisionmaking moments?
Yes Yes
• Is there a maintenancemechanism within the currentprocesses for evidence basedguidelines?
No Not able to answer
• Is there a mechanism to measurethe agreement on the whole orpart of the guideline(s)?
No No
• Is there a computerized decisionsupport system (CDSS), providingfeedback such as alerts orreminders, available at thedecision making moments?
No Not able to answer
Collaborativepractice models toinclude physicianand support-serviceproviders
• Are there defined roles, includingprotocols, among participants? Isthere an explicit process owner?
No Not able to answer
• Is there a systemdelivering/explaining the type ofservices provided by otherparticipants in the program?
Not completely Not able to answer
• Is there a mechanism tointroduce and facilitate the use ofa partner’s resources?
Not completely No
• Is there a patientself-management program (e.g.primary prevention program)available?
Yes Yes
Patientself-managementeducation
• Is there a mechanism to motivatethe patient to attend the program?
Yes Yes
• Is there a mechanism to assessthe patient’s knowledge andcapabilities in order to adapt theself-management educationprogram to provide tailoredinformation?
No No
• Is there a program for continuouseducation?
No No
Process andoutcomesmeasurement,evaluation, andmanagement
• Are (key) process and outcomequality indicators defined?
Not completely Not able to answer
• Is there a mechanism to registerthe (key) quality indicators andoutcome?
No Not able to answer

i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 1022–1033 1027
Table 2 (Continued)
• Is there a mechanism to evaluatethe quality of care based on theindicators?
No Not able to answer
• Is there a continuous monitoringmechanism available?
No Not able to answer
Is there a mechanism for actingupon the (key) quality indicators?
No Not able to answer
Routine reporting/feedback loop toindividuals participating in theprocess (patient, physician, etc.)
• Is there a mechanism to report tothe stakeholders including theprocess owner?
Yes Yes
• Are there report templates forthe individual participants?
Yes Not able to answer
n propture
1p
Tabb
aqi
ooictnptapt
2
Ooatactf
-
-
-
a The result of the application of the framework to the fall preventiob Testing the capability of the model without knowledge that was ca
.5. Short description of the current fall managementrogram
here are two recruitment options for entry into the fall man-gement program: patients who are included in the programy the Emergency Department after a fall and those includedy the homecare organization or a general practitioner.
Patients included by the Emergency Department receive anssessment of fall history (by post) using a self-assessmentuestionnaire, followed by a treatment plan which may
nclude a referral to the outpatient fall clinic.Homecare nurses routinely screen new clients who are
lder than 65 years for fall risk. If there is an increased riskf falling, a home management program is started includ-
ng self management, checking the patient’s medication, andhecking the home for safety after receiving permission fromhe general practitioner (GP). Up to four visits of a homecareurse with the patient may be scheduled. A brief report on theatient-specific program is sent to the general practitioner athe end of all the home visits. The general practitioner maylso initiate the fall prevention program by referring patientserceived as at-risk to the hospital’s outpatient fall clinic or tohe homecare organization.
. Methods
ur approach combines process modeling with the principlesf disease management (DM). The desiderata of disease man-gement are reformulated as questions, which are appliedo a process model to allow verification of the disease man-gement criteria. This process is illustrated in the real-worldase study of fall management described earlier. The steps inhe process of developing and validating our approach are asollows:
Formulating DM related concepts as questions◦ Requirements for questions about a DM concept.◦ Question derivation.
Modeling the health care processes and applying the DMquestions in the case-study.
Validation of the fall management case-study results andthe approach.
cesses during the process modeling development by the modeler.d from the interviews by the external modeler
◦ Gauging the experience of the modeler: usability of themethod.
◦ Validating the correctness and prioritizing the findings:the usefulness of the approach.
◦ Gauging the experience of an external validator withoutthe knowledge of interviews.
We address below each of these steps.
2.1. Formulating DM related concepts as questions
Using the criteria of CCA for DM, an expert panel of 4 medicalinformaticians and 2 physicians proposed questions and cri-tiqued them in several rounds until consensus was reached.The panel translated each concept into two sets of questions:the first set of questions was meant to assess whether thatconcept is realized in the processes.
The second set of questions consisted of detailed ques-tions to quantify the concept in the first set. For example,if in the first set we ask whether there is a mechanism toregister sensitivity of an instrument then in the second setwe would ask how sensitive the instrument is. While thefirst set addresses the structure of the provided care process,the second addresses performance-related aspects of the careprocess. [Table 1, column 2 and 3].
2.1.1. Requirements for questions about a DM conceptQuestions in the first set were considered to be answerabledichotomously. Our panel formulated the questions related toeach concept requiring that a question should either:
• Verify the availability of a mechanism for the realization ofthe DM concept in the process (e.g. existence of a mecha-nism for population identification), or
• Assess the quality of the implementation of the DM concept.For example we may ask whether there are mechanismsto obtain the sensitivity and specificity of the populationidentification).
Questions in the second set quantify the concept in theprocess and therefore may be numeric or open-ended.

c a l i
1028 i n t e r n a t i o n a l j o u r n a l o f m e d i2.1.2. Question derivationThe general procedure to design the questions was based onidentifying (a) the underlying sub-process of a DM criterion,(b) the relevant attributes of the sub-process elements, and(c) the mechanisms through which the sub-process is opera-tionalized.
To illustrate this procedure we give an example of the DMcriterion “Population identification process” which is aimedat testing whether an individual belongs to the target DMgroup. The panel viewed this criterion as a sub-process inwhich there are individuals taking a test. For test the panelsuggested attributes of a generic test such as cost, sensi-tivity, specificity, pass, fail, administration etc. Questionsrelated to relevant attributes and mechanisms pertaining tothe sub-process and attributes of its elements were thencaptured in the framework. For example, the panel lookedat the mechanism that operationalizes the sub-process: isthere a mechanism, and how is it implemented, to ver-ify membership to the target group (e.g. enquiry by mailor computerized questionnaire). Considering the attributesof test such as sensitivity, specificity and fail give rise toquestions such as “Is there a mechanism to obtain the sen-sitivity and specificity of the screening instrument withinthe subpopulation?” and “Is there an administrative systemfor tracing the subjects that refuse to participate or subjectsthat test negatively at this moment of population identifi-cation?” Answering these questions in a structured manneraided assessing the quality of the process and of its improve-ment.
Table 1, which presents the main result of this first step,shows the DM criteria, a brief description, the key questions,and examples of questions related to quantitative assessmentand quality improvement.
2.2. Modeling the health care processes and applyingthe DM questions in the case-study
The purpose of a care process model can be to explain the pro-cess to stakeholders as well as to facilitate analysis. A recentreview of business process modeling techniques suggested theUML activity diagram as one of the best choices for achievingthese goals [2]. We obtained process models by having a mod-eler perform (semi-structured) interviews with stakeholdersto recognize essential sub-processes with special focus onworkflows, information/data sources involved, and organiza-tional aspects (such as organizational boundaries). In applyingthis approach to our case study we used an adapted UML-AD2.0 for the activity diagrams, where the modeler used UML’s“swimlanes” and paid specific attention to identifying infor-mation sources used in the processes. Swimlanes in UML arelines, often vertical, which visually distinguish responsibili-ties or roles in processes. For example, modeling a physicianinteracting with a patient requires two lanes, one for each.We paid specific attention to identifying information sources
used in the processes. After drafting, the UML models werereviewed by the stakeholders. Areas for improving the processwere identified by addressing the DM questions related to theprocess model.n f o r m a t i c s 8 2 ( 2 0 1 3 ) 1022–1033
2.3. Validation of the fall management case-studyresults and the approach
This step consists of the following three sub-steps.
(1) Gauging the experience of the modeler: usability of themethodTo assess the usability of applying the approach as such tothe case-study we interviewed the modeler. The assess-ment focused on the ease and ability of the modeler toexpress the process as he perceived it and to apply thequestions to the process model. We asked the modeler twospecific questions: (1) whether the approach allowed forexpressing what he wanted to state and (2) whether andwhere he encountered difficulties in the modeling process.
(2) Validating the correctness and prioritizing the findings:the usefulness of the approachIn an invitational symposium of 75 attendees and apanel of 9 experts, the stakeholders and other relevantinterested parties (consisting of general practitioners,homecare employees, nurses and geriatricians) validatedthe results pertaining to the fall management case-study.The results were presented to the attendees, who wereasked to assess the correctness of the problems pre-sented and prioritize their importance. The second setof questions was used to quantify the problems and findimprovement solutions.
(3) Gauging the experience of an external validator withoutthe knowledge of interviewsIn addition to the experience of modeler, an external val-idator assessed the process of fall management using onlythe UML activity diagrams and the DM questions withouthaving the knowledge that was gained during the inter-views. The validator was blinded to the interviews and themodeling process itself.
3. Results: application of the approach tothe case-study
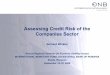
The process models revealed that care activities, in theprimary as well as the hospital care, could be adequately cat-egorized in a pattern of five steps as illustrated in Fig. 1.
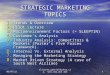
After drafting the process model in the activity diagramsfor all stakeholders in the program, we applied the DM ques-tions to the model. The bottlenecks were identified based onanswering the DM questions in each stakeholder’s processmodel, and are represented by the label «bottleneck» in themodel diagram. An example activity diagram showing theprocess followed at the homecare organization, including thesteps in the process, activities, and bottlenecks, is presentedin Figs. 2 and 3. In Fig. 2, in the swimlane of the BackofficeEm-ployee, we encounter at the bottom left the subprocess “GPnotification,” which refers to notifying the GP about patientsthat are not motivated to take the homecare fall preventionprogram but are at high risk of falling. The bottleneck box
associated with this subprocess states that homecare does nothave an administrative system to keep track of these patientsand therefore that the organization cannot measure the sen-sitivity and specificity of their triage instrument.
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 1022–1033 1029
Fig. 1 – Generic profiling process for fall risk assessment and management. Case finding: this step selects patients thatmight be at elevated risk of falling. Risk profiling: this step sets up a patient-specific fall risk profile based on additionalinformation such as identified risk factors pertaining to falls. Decision making: In this step decisions are made thatdetermine the patient’s treatment plan.Coordination: In this step interventions are planned and consultations scheduled tor stic
tAaatppsqee“
3
3tWartiown
3fiItcpTafiTnfttbe(bai
ealize the treatment plan. Interventions: In this step diagno
The results of the application of the DM questions to all ofhe fall management care processes are presented in Table 2.n answer of “no” to any of the DM questions indicates anrea for improvement. When the modeler could not find thenswers from the models with the knowledge gained duringhe interviews, an answer of “no” was assigned. For exam-le: in Fig. 3, part P1.5: There is no mechanism to assess theatient’s knowledge and capabilities in order to adapt theelf-management education program, so the answer to theuestion “Is there a mechanism to assess the patient’s knowl-dge and capabilities in order to adapt the self-managementducation program to provide tailored information?” will beno.”
.1. Results of the validation of the approach
.1.1. Gauging the experience of the modeler: usability ofhe method
e interviewed the modeler for a preliminary (subjective)ssessment of the usability of the approach. The modelereported that the UML activity diagram could easily capturehe process activities as expressed by the stakeholders includ-ng the flow and presence of the concepts/activities and flowf the data. He however reported that organizational aspectsere harder to capture and therefore extracting these dataeeded extra interviews and efforts.
.1.2. Validating the correctness and prioritizing thendings: the usefulness of the approachn the symposium the attendees were asked to comment onhe correctness of the findings. The findings were communi-ated with the audience through a large projector showing therocess models, presented per organization and as a whole.he bottlenecks were mapped on the process models. Thettendees were (plenarily) invited to comment on each set ofndings and on the final set of findings of the whole program.he attendees agreed on all items of the problem list and theeed to address them. They offered additional suggestions
or improvements. In addition, they were asked to prioritizehe findings for implementation. Some of the identified bot-lenecks were not considered a top priority for improvement,ut others were designated as key improvement findings. Forxample, introducing a computerized decision support system
CDSS) in homecare was acknowledged as an improvementut was not designated a high priority. In contrast, findinggood solution for general practitioners (GPs) for systemat-cally identifying patients at high risk of falling was assigned
and (preventive) treatment procedures are performed.
high priority, and decision support in the GP setting wasconsidered an appropriate tool to achieve this goal. The atten-dees also indicated that having a clear definition of the rolesand follow-up procedures for the GPs was considered a keyimprovement action. In addition, the GP was thought to be asuitable process manager for monitoring the follow-up proce-dures.
The application of our approach led to solution proposals.As an example, the introduction of CDSS also facilitates theautomation of key quality indicator monitoring and report-ing. In addition, solutions for empowering elderly patientsincluded employment of web-engineering to develop usefulwebsites for continued and tailored education, for example tohelp them prepare their visit to the GP or to understand howto prevent a second fall.
3.1.3. Gauging the experience of an external validatorwithout the knowledge of interviewsTo assess whether the process model and DM questions couldbe used to identify problem areas without additional knowl-edge of the process, the questions were separately applied tothe process model by an external validator who had not par-ticipated in the interviews or modeling process. The externalvalidator was less able to apply all the questions to the pro-cesses. The validator was able to answer 11 out of 22 (50%) ofthe questions using the process model alone. In particular, thevalidator found that it was difficult to distinguish omissionsin the real-world process from omissions in the model. Forexample, one can not tell by inspecting the diagram whetherthe screening instrument used had an adequate sensitivityand specificity.
4. Discussion
We proposed a systematic approach to assess and improvea healthcare program in which process models are evaluatedby a set of disease management criteria, cast as applicablequestions. The application of this approach to an extensivefall management program involving different partners fromprimary and secondary care demonstrated the feasibility ofthis approach.
This is the first approach suggesting and applying the com-
bination of DM and process modeling to evaluate health careprocesses. This approach is not only relevant to DM but alsoto other related approaches such as the chronic care model(CCM) and the Development Model for Integrated Care (IDMC).
1030 i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 1022–1033
Fig. 2 – The case finding step in homecare fall prevention program: The intaker decides based on three screening questionswhether further intervention is required to reduce the risk of falling. After authorization by the GP, up to four home visitsessions will be initiated. GP: general practitioner; EPR: electronic patient record; PPR: paper-based patient record system.AC stands for the home care organization, and the number indicates the form type used (including medium (digital, paper)).The different intensities of gray indicate the location of the activities: dark gray indicates nurse office, lighter gray indicatesthe patient’s home and no color indicates the back-office. Swimlanes show the actors of the activities. Transitions (fork,
ralle
join) indicate the division of an action state into multiple paFor example, to extend our approach to accommodate CCMone should add questions such as: “is there a mechanism foreducating the stakeholders?” and; “is there a mechanism totest the stakeholder’s knowledge?”.
The UML activity diagram seems to offer adequate expres-sivity to represent activity and data flows that the modelerintended to model. Although the validator was able to
l states or merging several action states together.
answer many questions correctly based on the processmodel, there is an opportunity for extending the activitydiagram to specifically facilitate answering the questionsafter, instead of during, the modeling task without the
knowledge that is gained during the interviews. In addi-tion, in contrast to the control-flow dimension which activitydiagrams can easily represent, it might be beneficial to
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 1022–1033 1031
Figure 3 – Processes of risk profiling and fall prevention intervention in home care, the second to fifth steps. GP: generalp
ettis
iTa
ractitioner; EPR: electronic patient records.
xtend these diagrams with notations or other diagramshat address the questions pertaining to the organiza-ional aspects. This implies that stakeholders should alsonclude those knowledgeable about the organizational dimen-ions.
Explicit process models also facilitate to some degree the
ndependence between the roles of modeler and evaluator:he modeler is technically skilled in translating reality into(semi-formal) model and the evaluator (e.g. someone from
the quality and safety department or a manager) shouldbe able to understand the model and apply the relevantquestions to it. It is inevitable that health delivery willchange over time and the process models need to beupdated to keep up with these changes. Many changes,however, will be local in nature requiring only small incre-
mental changes to the model and will probably necessitatere-applying only a small subset of the DM-related perspec-tive.
c a l i n f o r m a t i c s 8 2 ( 2 0 1 3 ) 1022–1033
Summary pointsWhat we already know:
• The current theory in process modeling (PM) focuseson how to describe and visualize processes systemat-ically but provides no guidance on how to use thesemodels for the assessment of the underlying (care)processes.
• Disease management (DM) is a strategy aimed atproviding efficient and effective care for patients espe-cially those suffering from chronic conditions, but inessence DM states desiderata without a systematiclink to verifying whether care processes adhere tothese desiderata.
What this study adds:
• Modeling care processes explicitly and applying a setof questions distilled from the DM desiderata to theseprocesses is a powerful way to understand, commu-nicate and assess a programme’s health care delivery.Specifically the models focus on health care activitiesand the questions address the existence of the neces-sary underlying mechanisms for implementing eachDM concept as well as assess the quality of the con-cept’s implementation.
• Application of our DM–PM approach to a fall manage-ment program involving a homecare organization, agroup of general practitioners, and an academic hos-pital’s Emergency Department and an outpatient fallclinic provided useful insights in the fall managementprocesses; exposed many important shortcomings;and gave way to improvement suggestions.
1032 i n t e r n a t i o n a l j o u r n a l o f m e d i
A main strength of our approach is its capability of mergingtwo disciplines: one for describing and visualizing processesand the other for stating desirable properties about theseprocesses. This offers the opportunity to draw on whatis already known in each discipline and augment itwith its counterpart. In addition, the application of thisapproach helps to systematically identify solution propos-als. Nevertheless, the suggested solutions still need to beimplemented and their benefit should be tested in prac-tice.
Although DM, and particularly the use of information tech-nology in DM, is thought to be promising, there are no explicitprocedural cues that help health IT design to capitalize on thispromise. Our suggested approach allows analysts, designers,and maintainers of health care IT systems to systematicallyelucidate requirements design and sustain systems while (1)staying in agreement with DM principles and (2) using visualyet semi-formal models that support communication amongstakeholders.
Our work has some limitations. First, our evaluation of theapproach is preliminary: we worked with one, albeit com-plex, case study and one modeler at a time. Hence we donot know what the inter-rater agreement would have beenif the evaluation had been conducted in parallel by anotherteam or using a different approach. We also did not trythe implied solutions in clinical practice. Second, althoughthe identified weaknesses in the process were consideredsound, the mapping between the DM categories and thequestions is inherently subjective. We do not have a goldstandard to assess the soundness and completeness of thequestions, and hence it is possible that questions have beenoverlooked. We attempted to formulate the questions at themost generic level possible, but the researchers were awareof the fall prevention at the time the questions were writ-ten. By the same token, formulating the model itself alsoresulted in the inclusion and adaptation of questions. Ourquestions may hence have a bias toward processes similar toour case study. We however believe that we propose a sim-ple yet potentially useful approach, as demonstrated in ourcase study, for visualizing and structuring the evaluation ofthe clinical processes and focusing discussion about a DMprogram.
Further research includes comparing results obtained byour approach with those obtained without it, applicationsof the approach to other domains and testing whetherthe set of questions needs adaptation, and measuring theinter-rater reliability by repeating the evaluation by extraobservers and assessing the usefulness of the proposed solu-tions.
5. Conclusion
We anticipate that our approach will be useful to others whowish to identify shortcomings in complex care processes and
contribute to a meaningful discussion about a DM program.At a minimum, the approach’s value stems from its system-atic checklist nature, guiding interviews and facilitating themodeling task to capture richer process models.Funding
This research was partly funded by ZonMw (The NetherlandsOrganization for Health Research and Development) bygrants for the PROFIT (#300020010) and ICOVE (#311020302)projects.
Authors’ contributions
MA, RW, AAH, and SR conceived the study and study design.RW performed the interviews and modeled the processes(described in his Masters thesis). MA, SE, AAH, SR SM, RWtranslated the concepts of DM to questions and validated itwith the stakeholders, a process that was coordinated by MA.SM acted as the external validator. MA drafted the manuscript.All authors helped interpreting the data and participated inthe design and critical revision of the manuscript and readand approved the final version.

i n f
C
TNp
r
Maglione, M.J. Suttorp, et al., Interventions for the
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l
onflict of interest
he authors declare that they have no conflicts of interest.o information reported in the manuscript was previouslyresented.
e f e r e n c e s
[1] W. Sadiq, M.E. Orlowska, Analyzing process models usinggraph reduction techniques, Inform. Syst. 25 (2) (2000)117–134.
[2] R.S. Aguilar-Saven, Business process modelling: review andframework, Int. J. Prod. Econ. 90 (2003) 129–149.
[3] N. Russell, W.M.P. Van der Aalst, A.H.M. Ter Hofstede, On thesuitability of UML 2.0 activity diagram for business processmodelling, in: Third Asia-Pacific Conference on ConceptualModelling (APCCM2006), Hobart, Australia, 2006.
[4] G. Booch, J. Rumbaugh, I. Jacobson, The Unified ModelingLanguage User Guide, Addison Wesley Longman, Inc.,Reading, Massachusetts, USA, 1999.
[5] N. Shiki, Y. Ohno, A. Fujii, T. Murata, Y. Matsumura, UnifiedModeling Language (UML) for hospital-based cancerregistration processes, Asian Pac. J. Cancer Prev. 9 (4) (2008)789–796.
[6] S. Garde, P. Knaup, R. Herold, Qumquad: a UML-basedapproach for remodeling of legacy systems in health care,Int. J. Med. Inform. 70 (2-3) (2003) 183–194.
[7] D. Lyalin, W. Williams, Modeling cancer registrationprocesses with an enhanced activity diagram, Methods Inf.Med. 44 (1) (2005) 11–13.
[8] P. Staccini, M. Joubert, J.F. Quaranta, D. Fieschi, M. Fieschi,Modelling health care processes for eliciting userrequirements: a way to link a quality paradigm and clinicalinformation system design, Int. J. Med. Inform. 64 (2-3)(2001) 129–142.
[9] http://www.dmaa.org/dm definition.asp[10] K.M. Lemmens, A.P. Nieboer, C.P. van Schayck, J.D. Asin, R.
Huijsman, A model to evaluate quality and effectiveness ofdisease management, Qual. Saf. Health Care 17 (6) (2008)447–453.
[11] A. Linden, J. Adams, N. Roberts, Evaluation methods indisease management: determining program effectiveness,Commissioned by the Disease Management Association ofAmerica, October 2003.
o r m a t i c s 8 2 ( 2 0 1 3 ) 1022–1033 1033
[12] L.P. Casalino, Disease management and the organization ofphysician practice, JAMA 293 (4) (2005) 485–488.
[13] U. Svensk, Disease management at the system level—aneffective way to improve health care, Int. J. Health Care Qual.Assur. 9 (7) (1996) 4–8.
[14] K. Fitzner, J. Sidorov, D. Fetterolf, D. Wennberg, E. Eisenberg,M. Cousins, et al., Principles for assessing diseasemanagement outcomes, Dis. Manage. 7 (3) (2004) 191–201.
[15] E.H. Wagner, C. Davis, J. Schaefer, M. Von Korff, B. Austin, Asurvey of leading chronic disease management programs:are they consistent with the literature? Manage. Care Q 7 (3)(1999) 56–66.
[16] E.H. Wagner, B.T. Austin, C. Davis, M. Hindmarsh, J. Schaefer,A. Bonomi, Improving chronic illness care: translatingevidence into action, Health Aff. (Millwood) 20 (6) (2001)64–78.
[17] M.M. Minkman, Vermeulen R.P., Ahaus K.T., Huijsman R.,The implementation of integrated care: the empiricalvalidation of the development model for integrated care,BMC Health Serv. Res. 11 (2011) 177.
[18] T.W. Wilson, J. Gruen, T. William, D. Fetterolf, P. Minalkumar,R.G. Popiel, et al., Assessing return on investment ofdefined-population disease management interventions, J.Comm. J. Qual. Saf. 30 (11) (2004) 614–621.
[19] M.E. Tinetti, M. Speechley, S.F. Ginter, Risk factors for fallsamong elderly persons living in the community, N. Engl. J.Med. 319 (26) (1988) 1701–1707.
[20] A.M. Tromp, J.H. Smit, D.J. Deeg, L.M. Bouter, P. Lips,Predictors for falls and fractures in the Longitudinal AgingStudy Amsterdam, J. Bone Miner. Res. 13 (12) (1998)1932–1939.
[21] Guideline for the prevention of falls in older persons,American Geriatrics Society, British Geriatrics Society, andAmerican Academy of Orthopaedic Surgeons panel on fallsprevention, J Am Geriatr Soc 49 (5) (2001) 664–672.
[22] CBS: Statistics Netherlands-StatLine database, 2012.[23] S.T. Liaw, N. Sulaiman, C. Pearce, J. Sims, K. Hill, H. Grain,
et al., Falls prevention within the Australian general practicedata model: methodology, information model, andterminology issues, J. Am. Med. Inform. Assoc. 10 (5) (2003)425–432.
[24] J.T. Chang, S.C. Morton, L.Z. Rubenstein, W.A. Mojica, M.
prevention of falls in older adults: systematic review andmeta-analysis of randomised clinical trials, BMJ 328 (7441)(2004) 680.