Embed Size (px)
Citation preview

A Cluster Randomized Clinical Trial Comparing FunctionalCapacity Evaluation and Functional Interviewing as Componentsof Occupational Rehabilitation Programs
Douglas P. Gross • Alexander K. Asante • Maxi Miciak • Michele C. Battie •
Linda J. Carroll • Ambrose Sun • Marti Mikalsky • Rene Huellstrung •
Riikka Niemelainen
� Springer Science+Business Media New York 2013
Abstract Purpose Functional capacity evaluations (FCE)
are used to identify work abilities and are commonly inte-
grated into rehabilitation programs. We studied whether
integrating FCE into rehabilitation leads to better outcomes
for injured workers. Methods A cluster randomised con-
trolled trial was conducted at a workers’ compensation
rehabilitation facility (registration ISRCTN61284905).
Clinicians were randomised into 2 groups: 1 group used
FCE while another conducted semi-structured functional
interviews. Outcomes included recommendations following
assessment, rehabilitation program outcomes including
functional work levels and pain intensity, as well as com-
pensation outcomes at 1, 3, and 6 months after assessment.
Analysis included Mann–Whitney U, Chi square and t tests.
Results Subjects included 225 claimants of whom 105 were
tested with FCE. Subjects were predominantly employed
(84 %) males (63 %) with sub-acute musculoskeletal con-
ditions (median duration 67 days). Claimants undergoing
FCE had *15 % higher average functional work levels
recommended at time of assessment (Mann–Whitney
U = 4,391.0, p \ 0.001) but differences at other follow-up
times were smaller (0–8 %), in favour of functional inter-
viewing, and not statistically significant. Clinically impor-
tant improvement during rehabilitation in functional
work level (0.9/4, SRM = 0.94), pain intensity (2.0/10,
SRM = 0.88) and self-reported disability (21.8/100,
SRM = 1.45) were only observed in those undergoing the
functional interview. Conclusions Performance-based FCE
integrated into occupational rehabilitation appears to lead to
higher baseline functional work levels compared to a semi-
structured functional interview, but not improved RTW
rates or functional work levels at follow-up. Functional
interviewing has potential for efficiency gains and higher
likelihood of clinically important improvement following
rehabilitation, however further research is needed.
Keywords Return-to-work � Compensation �Occupational injuries � Vocational rehabilitation �Disability insurance
Introduction
Given the substantial human, economic and societal burden
of musculoskeletal disorders, improved management
strategies are needed [1, 2]. Especially important are
strategies aimed at facilitating sustainable return-to-work
(RTW) for non-specific conditions (e.g. back, neck or
shoulder pain) where diagnostic imaging cannot be relied
Electronic supplementary material The online version of thisarticle (doi:10.1007/s10926-013-9491-4) contains supplementarymaterial, which is available to authorized users.
D. P. Gross (&) � M. C. Battie
Department of Physical Therapy, University of Alberta,
2-50 Corbett Hall, Edmonton, AB T6G 2G4, Canada
e-mail: [email protected]
D. P. Gross � A. Sun � M. Mikalsky � R. Huellstrung �R. Niemelainen
Workers’ Compensation Board-Alberta Millard Health,
Edmonton, AB, Canada
A. K. Asante
Alberta Health Services, Calgary Zone, Calgary, AB, Canada
M. Miciak
Faculty of Rehabilitation Medicine, University of Alberta,
Edmonton, AB, Canada
L. J. Carroll
School of Public Health, University of Alberta, Edmonton,
AB, Canada
123
J Occup Rehabil
DOI 10.1007/s10926-013-9491-4

on to determine resolution and readiness to return to
activity [3]. This has led to the development of perfor-
mance-based assessment tools such as functional capacity
evaluations (FCE) aimed at determining patients’ work
ability [4].
FCE has become an important component of many
functional restoration and other rehabilitation programs
[5–7]. It is often used to determine whether rehabilitation is
needed and then as an outcome measure before and after
rehabilitation. When compared to self-report functional
measures (i.e. tools relying on patients to indicate their
abilities using questionnaire, interview, clinical history,
etc.) performance-based FCE administered by a trained
therapist (i.e. actually having patients lift, carry, walk, etc.
in the clinic) has traditionally been considered more useful,
trustworthy and ‘‘objective’’ or free of bias [7–10]. How-
ever, such testing is time-consuming, requires specialized
equipment and is typically as expensive as advanced
diagnostic imaging procedures. Testing is also frequently
associated with pain reports [11, 12] and does not appear
entirely ‘‘objective’’ as previously supposed. Performance
appears to be determined not only by physiological
capacity, but by a variety of other psychological and social
factors including disability perceptions, self-efficacy
beliefs, pain intensity, and testing context [13–16]. More
critically, it has been demonstrated that FCE results are not
predictive of outcome following multidisciplinary reha-
bilitation after controlling for the number of pre-admission
health care visits [17] and is only modestly predictive of
future RTW [18–21]. Self-report measures (i.e. interview
or paper-based questionnaires) are typically less burden-
some for both patients and clinicians [22], but have been
criticized for relying totally on the patient’s ‘‘subjective’’
perspective and are less frequently relied on [23].
Whether FCE is superior to self-report measures and
actually worth the added burden has not been formally
evaluated via controlled clinical trial [24]. Several cross-
sectional studies have been performed looking at the corre-
lation between self-report and performance-based functional
measures in individuals with back pain [13, 15, 25–27].
Consistently, moderate correlations have been observed
indicating these different methods are measuring related
constructs. However, results from self-report measures have
been found to be systematically lower than performance
testing, with self-estimates of lifting ability during FCE
lower by 3–8 kg [15, 25]. The clinical implication of this
lower estimation is unknown, but potentially could lead to
limited or reduced RTW recommendations (i.e. return to
light duty as opposed to medium or heavy work). There is
also the possibility that lower functional levels limit reinte-
gration possibilities available to patients who do not have
jobs to return to.
Our objective was to examine whether performance-
based FCE enhances the occupational rehabilitation of
workers’ compensation claimants beyond information
gained from self-report measures. We hypothesized that:
(1) claimants undergoing performance-based FCE as part
of RTW assessment would demonstrate higher functional
work levels at time of baseline evaluation as compared to
claimants undergoing functional interviewing due to the
systematic lower estimations obtained with self-report
measures observed in previous cross-sectional studies; (2)
claimants undergoing either FCE or a self-report functional
interview would have comparable rates of overall RTW;
but (3) claimants undergoing FCE would RTW at higher
work levels due to the higher functional levels observed
with performance testing.
Methods
Design
A cluster randomised controlled trial design was used with
analysis at the level of individual claimant and an allocation
ratio of 1:1 [28]. Our clinical trial registration number was
ISRCTN61284905 and no important changes were made to
the methods after trial commencement. The design and
methodology were similar to that used successfully in eval-
uating a short-form Functional Capacity Evaluation (FCE)
protocol within the same jurisdiction [29]. The research was
conducted at the Alberta Workers’ Compensation Board’s
(WCB-Alberta) rehabilitation facility in Edmonton, Canada.
Data were extracted from WCB-Alberta administrative and
clinical databases, which have previously been used for
research purposes [5]. The University of Alberta’s Health
Research Ethics Board approved this study.
Study Sample
Between November 28, 2011 and January 10, 2012, all
claimants undergoing work assessment at the WCB-
Alberta facility were eligible for entry into the study. Data
were routinely collected as part of program evaluation
procedures, with the exception of follow-up telephone
interviews, which were voluntary. Exclusion criteria
included participation in a shoulder rehabilitation pilot
program that was being undertaken concurrently with this
study, claimants diagnosed with serious hearing impair-
ment (sufficient to make an interview impossible or unre-
alistic), explicit instruction from the claimant’s case
manager to conduct FCE, or non-musculoskeletal disorders
such as traumatic head injury, tumour or infection. Other-
wise, the sample was made of all claimants assessed at the
J Occup Rehabil
123

facility during the study timeframe. As little within-cluster
dependence was anticipated (claimants are assigned to
therapists in a non-systematic, relatively random fashion
based on the referral question and next available assess-
ment opening in the computerized scheduling system),
sample size estimates were adjusted using a small inflation
factor (intracluster correlation = 0.05) [30, 31]. We aimed
for 100 claimants per group and enrollment was stopped
when we achieved these numbers to avoid disruption of
service delivery at the rehabilitation facility.
Clinical Trial and Randomisation Procedures
Within the WCB-Alberta system, claimants are systemat-
ically referred for RTW assessment when they have not yet
returned to work, have ongoing functional difficulty related
to their compensable injury, and are being considered for
multidisciplinary occupational rehabilitation [17, 32]. The
WCB-Alberta rehabilitation facility is contracted to con-
duct these assessments and currently all RTW assessments
contain a component of performance-based functional
assessment using FCE. The objective of these assessments
is to determine whether the claimant is capable of returning
to pre-accident work duties and, if not, to determine if
further rehabilitation is indicated.
To evaluate whether performance-based FCE enhances
the process, we created a comparison group of claimants
who underwent assessment without FCE. Due to feasibility
issues related to the current WCB-Alberta rehabilitation
facility’s admission process, instead of randomly allocating
individual claimants to study groups we randomised cli-
nicians administering work assessments. Claimants were
therefore considered to have entered clusters of individuals
assessed by the same therapist. Clinicians at the facility
who were trained in administering the WorkWell FCE
were randomly allocated to one of two groups. One group
was asked to continue regular procedures that included
FCE, while the second group was asked to stop using FCE
and were trained to conduct ‘self-report’ assessments using
semi-structured functional interviewing.
Randomization was done by two of the study research-
ers (DPG and MM) who were blind to the allocation
sequence using a computerized random number generator
(www.random.org). Clinicians were each assigned a ran-
dom number, with even numbers allocated to the FCE
group. Randomisation resulted in 15 clinicians in the FCE
group and 15 in the ‘self-report’ group. After training, one
clinician in the ‘self-report’ group dropped out for personal
reasons unrelated to the study. Average age and years
working at the workers’ compensation facility of clinicians
in the FCE group was 39.8 and 9.5 years respectively,
comparable to the ‘self-report’ group (mean age = 38.0
years, mean experience = 9.8 years, range 2–23 years).
All of these clinicians had previously been trained in the
WorkWell FCE protocol and were using it within their
current daily practice at the facility. Study researchers were
available to answer questions throughout the study and
held weekly status update meetings with clinicians, but
clinicians independently made all claimant level manage-
ment decisions.
Due to the nature of work assessment, neither clinicians
nor claimants were blind to group allocation. However,
claimants were not aware of the study and were therefore
blind to group membership, including at time of follow-up
telephone interviews. Additionally, outcome evaluation
was performed in a blinded fashion via obtaining infor-
mation on claims outcomes from WCB administrative
databases and keeping telephone interviewers blind to
group status (conducted by a independent polling firm who
had no other information about the subjects).
Measures
Intervention Variable
The primary comparison made was between performance-
based and ‘self-report’ functional assessment groups. A
dichotomous intervention variable was created indicating
group allocation by identifying the assessing clinician
using the facility database.
Apart from the form of functional assessment, all other
aspects of the RTW assessment process were comparable
across all claimants. Assessing clinicians reviewed claim-
ants’ files, took a detailed history, and performed a mus-
culoskeletal examination. Claimants were also asked to
complete the SF-36 [33], Pain Disability Index [34], a
10-point Pain Visual Analogue Scale (VAS) [35], and a
physical job demands questionnaire for comparison with
determined functional levels. Functional ability levels were
compared to physical demands of the claimants’ jobs for
determination of work ability and readiness to RTW.
Physical demands were determined in both study groups
using either the physical job demands questionnaire,
employer-reported job demands, or workplace evaluation
when this information was available prior to the functional
assessment.
Performance-Based FCE
Functional ability is currently assessed at the facility via
the proprietary WorkWell (Duluth, MN) FCE. Claimants
within this study had been referred for a basic WorkWell
1-day FCE protocol, which is done when the claimant is
being considered as a candidate for rehabilitation. The
comprehensive 2-day WorkWell protocol, conducted after
other rehabilitation options have been exhausted and claim
J Occup Rehabil
123

closure is being considered, was examined in a related but
separate study. The WorkWell FCE involves a series of
performance tests including manual handling, positional
testing, mobility and coordination tests [36, 37]. The pro-
tocol typically takes 2–4 h to complete. To make maxi-
mum effort and performance judgments, clinicians observe
subjects’ physiological and biomechanical response to
testing to determine when maximum physical ability has
been reached [23, 38]. Performance on the FCE items is
synthesized into an overall functional work level in the
categories of sedentary (up to 5 kg), light (5–10 kg),
medium (10–20 kg), or heavy/very heavy ([20 kg). These
categories are important measures in many workers’
compensation systems as they are frequently used in RTW
planning, vocational rehabilitation (i.e. supported job
searching or retraining), and for setting earnings loss sup-
plements in cases of permanent disability. Within the
WCB-Alberta jurisdiction these levels facilitate commu-
nication across stakeholders and are used to describe
overall functional work ability following RTW assessment,
results of worksite assessments and employer ratings of
physical job demands, and are used to guide many claim-
ant-level RTW and indemnity-related decisions. To make
specific RTW decisions, clinicians compare claimant
ability to required job demands. Claimants meeting or
exceeding job demands are deemed suitable for RTW,
while those not meeting job demands are typically referred
for multidisciplinary occupational rehabilitation or a single
service provider (i.e. physiotherapy or chiropractic). The
WorkWell FCE has been shown to have acceptable reli-
ability [37, 39], construct validity as a measure of work-
related ability [40], and modestly predicts future RTW [18,
19, 21]. Claimants in the FCE group who were selected to
undergo multidisciplinary rehabilitation following assess-
ment had exercise and activity prescriptions made based on
FCE results and also underwent FCE at time of discharge
from the program. For analysis, we identified whether
claimants had undergone FCE as well as the clinician-
recommended functional work level category.
Self-report Functional Assessment
Numerous self-report measures are available for informing
RTW decisions, including questionnaires and interviews.
[41, 42] For this study, we used a semi-structured func-
tional interview approach that was previously developed
based on items in the WorkWell FCE [15]. In this func-
tional interview respondents are questioned about their
ability for the various activities that are tested during the
FCE protocol. The functional interview working document
that was used by clinicians during the study shows the
various items in the assessment and is available in
Appendix 1 in supplementary material. Claimants are
asked to identify to what level they would be able to
maximally perform for each activity (i.e. lifting or carrying
in kilograms, bending or standing in minutes) and this was
synthesized into an overall functional work level using the
same categories of sedentary/light/medium/heavy. To
make RTW decisions based on information gained, clini-
cians compare reported function to physical demands of the
job the worker would be returning to. If clarification was
needed on the various activities in question, pictures of the
activities were shown. Additionally, clinicians have access
to a detailed list of objects and their respective weights that
could be referred to when completing the assessment to
assist claimants in making estimations.
Previous research indicated that the manual handling
component of this functional interview correlates moder-
ately well (r = 0.50–0.73) with actual performance on the
corresponding WorkWell FCE items, supportive of its
construct validity as a measure of work-related function
[15]. However, consistent with other self-report measures,
results were systematically lower than FCE performance
testing with self-estimates of lifting ability lower by 3–8 kg
[15, 25]. Reliability of the tool has not previously been
examined, however prior to study implementation the full
semi-structured functional interview process was pilot
tested at a separate rehabilitation facility. Additionally,
during the course of the study the researchers held weekly
status update meetings with clinicians in the functional
interview group. This allowed us to monitor compliance
with the interview protocol, answer questions that arose,
and resolve any concerns expressed regarding the protocol.
There was also close communication between the study
clinicians and their facility ‘team leads’ that were also
members of the investigative team.
Prior to beginning the trial, clinicians assigned to the
‘self-report’ group were trained in how to conduct this
semi-structured functional interview. Training consisted of
a full-day session of instruction, including demonstration
and practice on use of functional interviewing. To assist
with conducting the interviews, clinicians were also
instructed on some of the basic principles of motivational
interviewing which aim to resolve ambivalence [43]. Cli-
nicians were instructed that the interviews should be col-
laborative, evocative (i.e. eliciting claimants’ own answers,
values and motivation), yet demonstrate respect for
claimant autonomy. For analysis, we identified whether
claimants had been assessed with the functional interview
or FCE and we obtained data on the clinician-recom-
mended functional work level category.
To avoid contamination, claimants in the self-report
functional interview group selected to undergo rehabilita-
tion were not exposed to FCE testing at any time during
their rehabilitation. Treatment clinicians were also trained
to perform semi-structured functional interviews and used
J Occup Rehabil
123

this assessment technique during rehabilitation and at dis-
charge assessment. Thus, exercise and activity prescrip-
tions along with RTW recommendations made during
rehabilitation were informed by functional interview
results.
Potential Confounders
To control for the possibility of unequal group formation,
information was obtained on a number of potential con-
founders. This included age, gender, number of days
between injury and assessment, job attachment status, pre-
accident annual salary, education level, marital status,
diagnosis, part of body injured, Human Resources and
Skills Development Canada’s National Occupational
Classification (NOC) [44], primary language and whether
an interpreter was involved in the assessment, and claimant
scores on the self-report pain, disability and health status
instruments completed during the assessment. These vari-
ables were chosen based on our previous studies within this
jurisdiction showing some predictive value or due to the-
oretical rationale for considering the variables as potential
confounders. We also determined the percentage of
claimants who underwent multidisciplinary rehabilitation
following assessment.
Outcome Measures
RTW outcomes included proxy indicators of work status
from the compensation database. We extracted information
on RTW and rehabilitation recommendations made by
clinicians at time of assessment. Using the compensation
administrative database, we also determined whether
claimants were receiving any wage replacement benefits.
Potential benefits included partial or total temporary dis-
ability benefits (received when claimants are off work for
part of or a complete day of work) or vocational rehabili-
tation benefits (received when claimants are undergoing
supported job search or retraining). Each of these was
extracted at time of assessment and at approximately the
same intervals as the follow-up interviews (30, 90, and
180 days post-assessment). These measures are commonly
used as indicators of RTW within compensation contexts,
and were available for 100 % of our sample [45]. After the
trial commenced, the decision was made to extract com-
pensation outcomes on any type of wage replacement
benefits (not just total temporary disability benefits) at the
same intervals as the telephone interviews (instead of
measuring time to benefit suspension), largely due to the
relatively small percentage of claimants receiving time loss
benefits at time of assessment.
Another important goal was to examine differences on
level of sustained work following assessment (i.e. heavy,
medium, light, sedentary or not working), with one group
judged superior if they returned to significantly higher lev-
els. As mentioned above, work levels are routinely used in
standardized occupational descriptions and are one outcome
of the work assessment at the rehabilitation facility [44].
Work levels described in the NOC are rated as sedentary (up
to 5 kg), light (5–10 kg), medium (10–20 kg), or heavy/
very heavy ([20 kg) [44]. To determine work levels after
the assessment, telephone contacts were made by an expe-
rienced polling firm (Leger Marketing). As work levels
frequently transition over time (due to job changes, pro-
gression of modified duties, etc.) follow-up contacts
occurred at multiple points in the subsequent year. Claim-
ants were contacted at 1, 3, and 6 months post-assessment.
Questions asked included whether the claimant was work-
ing, and if not working for what reason. In those who were
working, we asked claimants to rate their work level as
sedentary, light, medium, or heavy/very heavy [44]. We also
inquired about whether they were working full or part time
hours and whether they were working full or modified
duties.
For claimants who underwent multidisciplinary reha-
bilitation programs at the facility, we examined before and
after measures of functional work level category. We also
evaluated before and after measures of self-reported pain,
disability and health status and program completion,
duration and RTW outcomes. The decision was made to
evaluate these outcomes after the trial commenced, since
information was not available on claimant satisfaction rates
(as was originally planned) yet these are important clinical
outcomes following rehabilitation. All of these measures
were available within the facility’s clinical database.
Potential Harms
To monitor adverse or unintended effects, we tracked
serious negative outcomes experienced during or following
the assessments (i.e. new injuries during the assessment)
and complaints received about assessments from compen-
sation case managers.
Analysis
Initially, all data records were reviewed in order to ascer-
tain if any data issues, such as missing data, outliers or out
of range values, existed within the data set. Descriptive
statistics were then calculated. Related to cluster random-
ised trials, Donner and Klar have stated that an analysis at
the individual level that properly accounts for the effect of
clustering is equivalent to an appropriately weighted clus-
ter-level analysis [46]. To determine if a clustering effect
occurred, we examined differences across clusters on
claimant characteristics. We also examined intracluster
J Occup Rehabil
123

correlation using kappa and intraclass correlation coeffi-
cients for all of the primary and secondary outcomes. To
test our hypotheses and determine whether differences
existed between groups on the dichotomous proxy indictors
of RTW status (i.e. compensation benefit reception) at the
various follow-up intervals, Chi squared tests were per-
formed. To test our hypotheses and determine whether
differences existed between groups on the ordinal-level
functional work level categories at baseline and at the
various follow-up intervals, Mann–Whitney U tests were
performed. To determine absolute size of the effects,
functional level scores were also considered on a scale of
1–4 and mean differences were calculated. Groups were
statistically on all other outcomes using either non-para-
metric Mann–Whitney U, Chi square or t tests. Standard-
ized response means were also calculated on the pre-post
rehabilitation measures. Stratification and multivariable
analyses were used to evaluate whether variables that were
different between groups at baseline had an important
confounding effect. All analyses were conducted within the
originally assigned groups. A 0.05 alpha level was used to
judge statistical significance. All analyses were conducted
using SPSS 20 (Chicago, IL).
Results
Claimant Characteristics and Adequacy
of Randomisation Process
During the study timeframe, 225 workers’ compensation
claimants were assessed: 105 underwent FCE and 120 were
assessed using the functional interview. The higher number
of claimants assessed in the interview group was due to
increased efficiency of the assessment process (claimants
no longer needed to be cleared medically for maximal
performance testing). Twenty claimants were excluded
from the study (17 were participating in a pilot shoulder
rehabilitation program, and 3 had been referred explicitly
for performance-testing by their WCB case manager either
for comparison to previous FCE or for assessment with and
without a gait aide). A detailed study flow chart showing
the number of therapists enrolled and claimants at each step
of the study is available as supplementary material.
Claimant characteristics are detailed in Table 1. The
majority were employed (84 %) males (63 %) working in
the ‘trades and transport’ industry (49 %). Claimants in the
FCE and functional interview groups were similar on most
claimant characteristics examined (see Table 1), but a
statistically significant difference was observed on sex and
marital status. Claimants in the FCE group were less likely
to be male (55 vs. 71 %) and more likely to be married (56
vs. 43 %). No statistically significant differences were
Table 1 Characteristics of claimants referred for return-to-work
assessment
Entire
sample
(n = 225)
Interview
group
(n = 120)
FCE group
(n = 105)
Mean (SD) or percent
Age (years) 43.2 (13.1) 43.9 (13.0) 42.5 (13.3)
Accident to
admission (days)
167 (639) 180 (832) 151 (295)
Median = 67 Median = 62 Median = 72
Gross annual salary
($10 k CDN)
42.8 (29.3) 43.5 (29.6) 42.0 (29.1)
Sex (% male)* 63.1 70.0 55.2
Employed at time of
assessment (% yes)
83.6 81.1 86.7
Currently working 50.7 47.5 54.3
Language
(% English)
96.9 97.1 97.1
Interpreter involved
(% yes)
4.0 3.3 4.8
Education level
Grade 8 or less 4.4 4.2 4.8
Partial high school 11.6 14.2 8.6
High school
diploma
23.8 25.8 21.0
Partial technical
school
8.4 9.2 7.6
Technical diploma 12.4 12.5 12.4
Partial university 4.9 2.5 7.6
University degree 6.7 5.8 7.6
Not specified 28.0 25.8 30.5
Marital status*
Married/common
law
49.3 43.3 56.2
Single 24.9 33.3 15.2
Divorced/separated 8.9 9.2 8.6
Widowed 1.3 0.8 1.9
Not specified 15.6 13.3 18.1
Diagnosis
Sprain/strain/
non-specific
69.8 66.7 73.3
Fracture 11.1 12.5 9.5
Trauma 17.3 20.0 14.3
Dislocation 0.9 0.8 1.0
Carpal tunnel
syndrome
0.9 0 1.9
Part of body
Upper extremity/
shoulder
34.7 30.0 40.0
Back/trunk 31.6 29.2 34.3
Lower extremity 20.4 23.3 17.1
Neck 2.2 3.3 1.0
Other/multiple
body parts
11.1 14.2 7.6
J Occup Rehabil
123

observed between groups on the self-report pain, disability
or health-related quality of life questionnaires completed
during the work assessment. Scores indicated that claim-
ants experienced moderate levels of pain and disability,
and reported substantially reduced physical and mental
health compared with normative scores [47].
While no significant differences existed in claimant
characteristics between groups, there was a statistically
significant difference between groups in the discipline of
the assessing clinician. Clinicians conducting FCE were
more likely to be occupational therapists (72 vs. 21 %)
while those conducting functional interviews were more
likely to be physical therapists (24 vs. 14 %) or exercise
therapists/kinesiologists (55 vs. 14 %). However, there
were no statistically significant differences observed in any
study outcomes across therapist discipline indicating that
this difference likely did not impact results. When testing
for a clustering effect, the only claimant characteristic that
was statistically different across therapist clusters out of 23
individual and clinical assessment variables tested was
marital status (p = 0.02), indicating that a clustering effect
was unlikely. As expected, intracluster correlation coeffi-
cients for the various outcome measures were small,
ranging from 0.001 to 0.03.
Follow-Up Rates
There was complete ascertainment of outcomes assessed
through the facility database that included RTW recom-
mendations and functional levels at time of assessment and
discharge from rehabilitation, and all compensation wage
replacement benefit data. Some missing data was observed
on the self-report pain and disability questionnaires at time
from discharge from rehabilitation with 76 of 104 (73 %)
having complete data on these measures. No statistically
significant or clinically important differences were observed
on any characteristic or outcome measure between those
with or without missing data on these questionnaires.
Functional work level after assessment was ascertained
through telephone interviews. Overall rate of participation
in follow-up telephone interviews was 38 %, with follow-up
rates at 1, 3, and 6 months of 34, 24, and 22 % respectively.
Statistical testing indicated that compared to those who did
not participate, those interviewed were more likely to have
undergone a functional interview (45.0 vs. 29.5 %,
p = 0.02) and less likely to have back injuries (17 vs.
41 %), but were otherwise comparable on other descriptive
variables.
Work Assessment and Rehabilitation Outcomes
Approximately 48 % of claimants were recommended to
RTW following assessment, but 71 % were also recom-
mended for some form of rehabilitation (53 % underwent
multidisciplinary rehabilitation). Only 12 % had no other
interventions recommended, with all of these recommen-
dations similar between groups.
A statistically significant difference was observed
between groups on functional work level determined at
time of assessment (see Table 2). Claimants undergoing
FCE were less likely to be rated at a sedentary work level
(12 % in FCE group vs. 31 % for interview, Mann–
Table 1 continued
Entire
sample
(n = 225)
Interview
group
(n = 120)
FCE group
(n = 105)
National
occupational
classification
Management 1.8 0.8 2.9
Business, finance
and admin
10.7 16.7 3.8
Natural and applied
sciences
2.7 3.3 1.9
Health occupations 8.4 5.8 11.4
Education,
government, etc.
0.4 0 1.0
Art, culture,
recreation and
sport
0.4 0 1.0
Sales and service 19.1 19.2 19.0
Trades and
transport
48.9 46.7 51.4
Natural resources
and agriculture
3.1 3.3 2.9
Manufacturing and
utilities
4.4 4.2 4.8
Pain Visual
Analogue Scale
(out of 10,
n = 223)
4.6 (2.4) 4.6 (2.5) 4.5 (2.3)
Percent Pain
Disability Index
(n = 223)
45.7 (23.2) 47.0 (23.3) 44.2 (23.2)
SF36 raw scores
(n = 212)
Physical function 55.4 (23.6) 53.6 (25.2) 57.5 (21.6)
Role physical 31.6 (27.5) 30.0 (27.0) 33.3 (28.1)
Bodily pain 34.6 (19.0) 33.0 (19.9) 36.3 (18.6)
General health 67.5 (19.0) 67.6 (17.6) 67.2 (20.5)
Vitality 48.5 (20.8) 47.3 (20.9) 49.8 (20.5)
Social function 52.9 (27.8) 49.6 (28.5) 56.8 (26.6)
Role emotional 59.6 (31.8) 58.8 (32.9) 60.5 (30.7)
Mental health 63.6 (21.3) 62.2 (20.9) 65.2 (21.9)
* Statistically significant difference observed between groups
(p \ 0.05)
J Occup Rehabil
123

Table 2 Comparison of return-to-work assessment and rehabilitation program outcomes between groups
Entire sample (n = 225) Interview GROUP (n = 120) FCE group (n = 105)
Mean (SD) or percent
Assessment outcomes
Functional level determined at assessment*
Sedentary (\5 kg) 22.0 30.8 12.4
Light (6–10 kg) 25.8 27.5 23.8
Medium (10–20 kg) 43.1 38.3 48.6
Heavy/very heavy ([20 kg) 8.9 3.3 15.2
Assessment discharge outcome
Return-to-work 47.8 46.7 47.6
Fit-to-work 51.8 52.5 51.4
Not fit-to-work/other 0.4 0.8 1.0
Reason for not returning to work
Referred for further rehab services 70.6 76.2 66.7
Not job attached 12.6 12.7 13.0
Looking for employment 0.8 1.5 0
Retirement 0.9 1.5 0
Other reason 13.4 7.9 20.4
Rehabilitation recommendation
Multidisciplinary rehabilitation program 52.5 47.5 58.2
No intervention recommended 12.4 16.7 7.6
Single service provider (i.e. PT or Chiro) 35.1 35.8 34.3
Anticipated duration of rehabilitation (weeks)* 4.0 (1.3) 4.3 (1.5) 3.8 (0.9)
Actually underwent rehabilitation 46.2 40.8 52.4
(n = 104) (n = 49) (n = 55)
Underwent multidisciplinary rehabilitation
Type of program
Functional restoration 95.0 93.9 96.1
Complex chronic pain 5.0 6.1 3.9
Actual program duration (weeks) 2.7 (1.1) 2.9 (0.9) 2.6 (1.2)
Completed program 89.4 93.9 85.5
Admission functional work levels*
Sedentary (\5 kg) 19.2 24.5 14.5
Light (6–10 kg) 26.0 32.7 21.8
Medium (10–20 kg) 47.1 42.9 50.9
Heavy/very heavy ([20 kg) 7.7 0 12.7
Admission Pain Visual Analogue Scale (out of 10) 4.6 (2.3) 4.8 (2.6) 4.5 (2.0)
Admission Percent Pain Disability Index 48.1 (21.4) 49.6 (21.8) 46.8 (21.2)
Admission SF36 Raw Scores
Physical function 53.6 (22.3) 50.0 (24.7) 56.8 (21.2)
Role physical 28.1 (26.8) 24.7(25.8) 31.1 (27.5)
Bodily pain* 32.9 (19.7) 28.2 (19.6) 37.1 (19.0)
General health 67.7 (19.5) 70.2 (16.4) 65.6 (21.7)
Vitality 48.5 (20.4) 47.3 (21.9) 49.7 (19.2)
Social function 50.9 (27.4) 47.2 (28.6) 54.2 (26.2)
Role emotional 57.0 (32.6) 57.1 (36.2) 56.9 (29.4)
Mental health 61.5 (21.9) 60.3 (22.8) 62.6 (21.3)
SF36 Physical Health Composite Score* 33.8 (7.9) 32.1 (7.5) 35.3 (7.9)
J Occup Rehabil
123

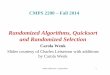
Whitney U = 4,391.0, p \ 0.001). On average, claimants
undergoing FCE were rated as capable of performing
heavier work (mean 2.7/4 for FCE vs. 2.1/4 out of 4 for
functional interview, p \ 0.001), representing a mean dif-
ference of 0.6/4 (15 %). Differences between groups on
functional work levels recommended by the assessing cli-
nician are shown graphically in Fig. 1. Due to the imbal-
ance between groups on male/female ratio, a stratified
analysis was conducted based on sex. Differences between
groups remained statistically significant in both males and
females, with claimants undergoing FCE consistently rated
higher. Despite the differences observed on functional
work levels, no statistically significant differences were
observed on clinician RTW or rehabilitation recommen-
dations after assessment (see Table 2). However, claimants
undergoing the functional interview had significantly
higher average anticipated lengths of rehabilitation (4.3 vs.
3.8 weeks).
Among claimants who underwent multidisciplinary
rehabilitation, a statistically significant between-group
difference on baseline assessment functional work levels
was observed, however, differences on discharge func-
tional work levels were not statistically significant.
Functional work level change scores between admission
assessment and discharge were significantly lower in the
FCE group (Mann–Whitney U = 1,078.5, p \ 0.001).
Claimants in the FCE group experienced a lower mean
improvement of 0.3/4 (SRM = 0.35) compared with the
interview group that experienced a mean improvement of
0.9/4 (SRM = 0.94). These results remained statistically
significant (p \ 0.001) after controlling for sex and marital
status. Claimants who underwent the ‘self-report’ func-
tional interview also had significantly higher anticipated
durations of rehabilitation (4.3 vs. 3.8 weeks) indicating
clinicians thought these claimants would take longer to
achieve their functional goals. Differences between groups
on actual program durations were small and not statistically
significant (2.9 weeks for interview group vs. 2.6 weeks
for FCE group, p = 0.07). Other rehabilitation program
outcomes were comparable between groups, however,
claimants who underwent performance-based FCE reported
significantly higher pain and disability levels at time of
discharge from rehabilitation (see Table 2). Clinically
important improvements in pain and reported disability
following rehabilitation were only observed in the inter-
view group which experienced a mean improvement on the
Table 2 continued
(n = 104) (n = 49) (n = 55)
Sf36 Mental Health Composite Score 41.7 (13.2) 41.4 (14.5) 41.9 (12.1)
Rehabilitation discharge outcome
Return-to-work 83.7 83.7 83.6
Fit-to-work 16.3 16.3 16.4
Not fit-to-work/other 0 0 0
Discharge functional work levels
Sedentary (\5 kg) 8.1 10.2 6.0
Light (6–10 kg) 13.1 12.2 14.0
Medium (10–20 kg) 46.5 40.8 52.0
Heavy/very heavy ([20 kg) 32.3 36.7 28.0
Discharge pain VAS (out of 10, n = 76)* 3.0 (2.3) 2.5 (2.2) 3.6 (2.2)
Discharge Percent Pain Disability Index (n = 76)* 30.5 (23.7) 25.3 (23.0) 36.1 (23.5)
Discharge SF36 Raw Scores (n = 76)
Physical function 68.1 (24.0) 69.8 (25.2) 66.3 (22.9)
Role physical 47.2 (28.3) 49.5 (30.1) 44.7 (26.4)
Bodily pain 49.5 (22.1) 53.1 (24.5) 45.6 (18.9)
General health 69.2 (20.3) 72.0 (16.8) 66.1 (23.3)
Vitality 55.5 (20.0) 57.0 (20.3) 53.8 (19.9)
Social function 64.7 (29.1) 69.2 (27.1) 59.9 (30.8)
Role emotional 64.8 (29.2) 66.2 (30.5) 63.3 (28.1)
Mental health 66.0 (21.8) 69.9 (18.9) 61.9 (24.1)
SF36 Physical Health Composite Score 40.6 (9.1) 41.4 (10.0) 39.8 (8.0)
Sf36 Mental Health Composite Score 44.0 (12.3) 45.7 (11.4) 42.1 (13.2)
* Statistically significant difference observed between groups (p \ 0.05)
J Occup Rehabil
123

Pain VAS = 2.0/10 (SRM = 0.88) and PDI = 21.8/100
(SRM = 1.45) compared with mean improvement in the
FCE group on the Pain VAS = 0.6/10 (SRM = 0.30) and
PDI = 9.5/100 (SRM = 0.37). These results remained
statistically significant (p \ 0.001) after controlling for
baseline pain and disability reports as well as sex and
marital status. None of the other variables tested had an
important confounding effect.
Compensation Outcomes
No statistically significant differences were observed
between groups on any of the compensation outcomes (see
Table 3). Outcomes were quite positive, with 92 % of
claimants off all wage replacement benefits by 180 days
after assessment in both groups.
Telephone Interview Outcomes
No statistically significant differences were observed
between groups on any of the key outcomes obtained
during telephone interviews (see Table 3). Our hypothesis
related to higher functional work levels after undergoing
FCE was not supported as reported working levels were
similar between groups (mean = 2.6, 2.6, 2.7 for FCE and
2.6, 2.8, 3.0 for interview at 1, 3, and 6 months respec-
tively, [ 0.05). This represents mean differences between
groups ranging from 0/4 to 0.3/4 in favour of the interview
(0–8 %). At the 3- and 6-month follow-up interview
Fig. 1 Comparison of functional work levels recommended by
assessing clinician at time of return-to-work assessment. Differences
are statistically significant (Mann–Whitney test p \ 0.001, n = 225)
Table 3 Comparison of workers’ compensation and telephone
interview outcomes between groups
Variable Interview
group
FCE group
(n = 120)
p value
(n = 105)
Compensation benefit
outcomes
Number/
percent
Receiving benefits at
assessment
Total temporary 40 (33.3) 30 (28.6) 0.44
Partial temporary 15 (12.5) 21 (21.0) 0.09
Total vocational 0 (0) 0 (0)
Partial vocational 0 (0) 0 (0)
Any compensation benefits 55 (45.8) 51 (48.6) 0.68
Benefits at 30-days post
assessment
Total temporary 26 (21.7) 13 (12.4) 0.07
Partial temporary 22 (18.3) 22 (21.0) 0.62
Total vocational 0 (0) 0 (0)
Partial vocational 0 (0) 0 (0)
Any compensation benefits 48 (40.0) 35 (33.3) 0.30
Benefits at 90-days post
assessment
Total temporary 7 (5.8) 2 (1.9) 0.13
Partial temporary 4 (3.3) 5 (4.8) 0.59
Total vocational 0 (0) 3 (2.9) 0.06
Partial vocational 2 (1.7) 1 (1.0) 0.64
Any compensation benefits 13 (10.8) 11 (10.5) 0.93
Benefits at 180-days post
assessment
Total temporary 2 (1.7) 1 (1.0) 0.64
Partial temporary 3 (2.5) 2 (1.9) 0.76
Total vocational 0 (0) 1 (1.0) 0.28
Partial vocational 3 (2.5) 1 (1.0) 0.38
Any compensation benefits 8 (6.7) 5 (4.8) 0.54
Telephone interview outcomes Number/percent or mean (SD)
Participated in interview 54 (45.0) 31 (29.5) 0.02
Reported pre-injury demands
(n = 76)
Sedentary 8 (16.3) 4 (14.8) 0.61
Light 4 (8.2) 2 (7.4)
Medium 19 (38.8) 7 (25.9)
Heavy/very heavy 18 (36.7) 14 (51.9)
Self-rated work ability
compared to lifetime best
(out of 10)
1 month (n = 76) 6.0 (3.1) 6.9 (2.7) 0.20
3 months (n = 54) 7.5 (2.4) 7.4 (2.8) 0.91
6 months (n = 49) 6.5 (2.9) 6.1 (2.7) 0.66
Numeric pain rating (out
of 10)
1 month 4.1 (2.6) 3.3 (2.3) 0.20
3 months 3.2 (2.4) 2.5 (2.6) 0.36
6 months 3.3 (2.7) 4.0 (2.4) 0.38
J Occup Rehabil
123

intervals, a higher percentage of claimants in the functional
interview group reported working at a heavy/very heavy
level (33 and 40 vs. 27 and 31 % respectively) although
this difference was not statistically different (p = 0.9 and
0.09). Due to the imbalance in telephone interview follow-
up rates between claimants with back and non-back related
injuries, we conducted a stratified analysis on all key out-
come measures. This analysis indicated part of body was
not an important confounding variable.
Adverse or Unintended Effects
No new or re-injuries associated with assessments were
reported during the trial, however we did receive 5 com-
plaints from case managers. These all questioned the use of
functional interviews instead of performance-based FCE.
Case managers consistently considered the functional
interviews to be less ‘objective’ than FCE.
Discussion
Performance-based FCE does not appear to enhance out-
comes when integrated into the process of occupational
rehabilitation. While claimants undergoing performance-
based FCE were rated as capable of performing substan-
tially higher functional work levels (*15 % higher with
FCE) at baseline as compared to those who underwent a
semi-structured functional interview, no statistically sig-
nificant or clinically meaningful differences were observed
on the functional work levels or compensation outcomes at
any other follow-up period. Claimants who underwent the
‘self-report’ functional interview also had significantly
higher anticipated durations of rehabilitation indicating
Table 3 continued
Variable Interview
group
FCE group
(n = 120)
p value
(n = 105)
1-month work outcomes
Work status
Regular duties full time 8 (16.3) 8 (29.6) 0.27
Regular duties part time 3 (6.1) 1 (3.7)
Modified duty full time 11 (22.4) 6 (22.2)
Modified duty part time 10 (20.4) 1 (3.7)
Not working 17 (34.7) 11 (40.7)
Work lifting requirements at 1
month
Sedentary 9 (28.1) 5 (31.2) 0.85
Light 3 (9.4) 2 (12.5)
Medium 12 (37.5) 4 (25.0)
Heavy/very heavy 8 (25.0) 5 (31.2)
Why not working at 1 month?
Unable due to injury 9 (52.9) 1 (9.1) 0.01
Unemployed but seeking
work
2 (11.8) 4 (36.4)
In retraining due to injury 5 (29.4) 2 (18.2)
Not working for other
reasons
0 (0) 4 (36.4)
New injury 1 (5.9) 0 (0)
3-month outcomes
Work status
Regular duties full time 23 (62.2) 8 (47.1) 0.61
Regular duties part time 2 (5.4) 1 (5.9)
Modified duty full time 4 (10.8) 1 (5.9)
Modified duty part time 2 (5.4) 1 (5.9)
Not working 6 (16.2) 6 (35.3)
Work lifting requirements at
3 months
Sedentary 6 (20.0) 2 (18.2) 0.90
Light 5 (16.7) 3 (27.3)
Medium 9 (30.0) 3 (27.3)
Heavy/very heavy 10 (33.3) 3 (27.3)
Why not working at
3 months?
Unable due to injury 3 (50.0) 3 (50.0) 0.94
Unemployed but seeking
work
1 (16.7) 0 (0)
In retraining due to injury 1 (16.7) 2 (33.3)
Not working for other
reasons
1 (16.7) 1 (16.7)
6-month outcomes
Work status
Regular duties full time 17 (51.5) 9 (56.2) 0.97
Regular duties part time 4 (12.1) 2 (12.5)
Modified duty full time 3 (9.1) 1 (6.2)
Modified duty part time 1 (3.0) 1 (6.2)
Not working 8 (24.2) 3 (18.8)
Table 3 continued
Variable Interview
group
FCE group
(n = 120)
p value
(n = 105)
Work lifting requirements at
6 months
Sedentary 2 (8.0) 4 (30.8) 0.09
Light 6 (24.0) 0 (0)
Medium 7 (28.0) 5 (38.5)
Heavy/very heavy 10 (40.0) 4 (30.8)
Why not working at
6 months?
Unable due to injury 3 (37.5) 1 (33.3) 0.78
Unemployed but seeking
work
2 (25.0) 1 (33.3)
Not working for other
reasons
2 (25.0) 0 (0)
New injury 1 (12.5) 1 (33.3)
J Occup Rehabil
123

clinicians thought these claimants would take longer to
achieve their functional goals. However, by 1-month after
assessment all functional and RTW outcomes were com-
parable between groups, even slightly favouring the func-
tional interview group.
Within the subgroup of claimants who underwent mul-
tidisciplinary rehabilitation, the performance-based FCE
group was assessed as having significantly higher func-
tional work levels at admission assessment when compared
to the functional interview group, but discharge functional
levels were comparable. Indeed, claimants in the functional
interview group improved their functional work levels to a
greater extent than the FCE group. Unexpectedly, only
claimants in the functional interview group experienced
clinically important improvements in reported pain inten-
sity [48] and disability ratings [49] over the course of their
rehabilitation despite having worse bodily pain and phys-
ical health scores at admission. This was despite non-sig-
nificant, fairly small (*2.5 days) differences in overall
program duration between the two groups and could
potentially be due to pain exacerbation (i.e. flare-up) that is
frequently associated with performance-based FCE testing
due to the maximal physical effort required [11, 12].
Findings indicate that a semi-structured functional inter-
view incorporating some of the principles of motivational
interviewing used by clinicians who are trained and expe-
rienced in FCE may be as clinically useful as performance-
based FCE, with potential for efficiency gains and likeli-
hood of greater improvement in some clinical outcomes.
The observation that function demonstrated during
performance-based FCE is higher than self-reported ability
is consistent with previous research [15, 25]. Prior studies
have indicated that outcomes from self-report measures are
systematically lower than performance testing, with self-
estimates of lifting ability lower by 3–8 kg. However, this
is the first study to attempt to rigorously evaluate whether
these differences are sustainable and translate into
improved clinical and RTW outcomes. Results suggest that
these differences do not lead into improved outcomes.
However, further research is needed to determine if our
findings are repeatable in other jurisdictions and contexts.
The fact that we received complaints from compensation
case managers during the study indicates there is some
perceived value of performance-based assessment among
relevant stakeholders. We are currently examining the issue
of stakeholder perceptions of FCE within this jurisdiction
in an associated qualitative study.
Strengths of this study include the use of cluster ran-
domized controlled trial methods incorporated into a
pragmatic clinical context. Data were gathered in an actual
clinical setting as part of routine patient care and few
restrictions were placed on our sample, indicating it should
be fairly representative of this population. We were able to
obtain 100 % follow-up on the compensation outcomes,
and randomisation appeared adequate with the exception of
more OTs randomized to conduct functional interviews.
However, clinician discipline was not associated with
outcomes and little evidence of a clustering effect was
observed indicating the unequal clinical disciplines did not
influence outcomes. Other limitations include low partici-
pation in follow-up interviews (38 %). This is consistent
with research involving workers’ compensation claimants
[50]. However, few systematic differences were observed
between those who did and not participate in follow-up
contacts and stratified analysis showed there was no con-
founding by body part affected which differed between
groups. Of interest, we found that claimants undergoing
functional interview instead of FCE were much more likely
to participate in follow-up interviews. It may be that asking
claimants to thoroughly discuss their functional difficulties
at assessment made them more open to participate in
subsequent discussions. While reliability of the functional
interview has not been previously tested, there is some
prior evidence of construct validity of the manual handling
component and this study provides further validity evi-
dence for its utility as a measure of work ability. Further
research on the functional interview is recommended
including evaluation of its reliability and other psycho-
metric properties.
Conclusion
Performance-based FCE integrated into occupational
rehabilitation appears to lead to higher baseline functional
levels compared to a semi-structured functional interview,
but not improved RTW rates or functional work levels at
follow-up. Functional interviewing has potential for effi-
ciency gains and higher likelihood of improved functional
work levels, pain and disability following rehabilitation.
Further research is indicated on the reliability and validity
of the functional interview tool.
Acknowledgments This research was supported with funds from
WorkSafeBC through the Focus on Tomorrow program. WCB-
Alberta Millard Health assisted with data acquisition and study
implementation. The clinical trial registration number was IS-
RCTN61284905 and the protocol can be accessed at the following
website: http://www.controlled-trials.com/ISRCTN61284905/. The
authors have no competing interests or financial arrangements that
would represent a conflict of interest for this research.
References
1. Martin BI, Deyo RA, Mirza SK, Turner JA, Comstock BA,
Hollingworth W, et al. Expenditures and health status among
J Occup Rehabil
123

adults with back and neck problems. JAMA. 2008;
299(6):656–64.
2. Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud
C, et al. Disability-adjusted life years (DALYs) for 291 diseases
and injuries in 21 regions, 1990–2010: a systematic analysis for
the Global Burden of Disease Study 2010. Lancet. 2012;
380(9859):2197–223.
3. Hadler NM. Occupational musculoskeletal disorders. 3rd ed.
Philadelphia: Lippincott Williams & Wilkins; 2005.
4. Innes E, Straker L. A clinician’s guide to work-related assess-
ments: 1-purposes and problems. WORK. 1998;11:183–9.
5. Gross DP, Haws C, Niemelainen R. What is the rate of functional
improvement during occupational rehabilitation in workers’
compensation claimants? J Occup Rehabil. 2012;22(3):292–300.
6. Rainville J, Kim RS, Katz JN. A review of 1985 Volvo Award
winner in clinical science: objective assessment of spine function
following industrial injury: a prospective study with comparison
group and 1-year follow-up. Spine. 2007;32(18):2031–4.
7. Mayer TG, Gatchel RJ, Kishino N, Keeley J, Capra P, Mayer H,
et al. Objective assessment of spine function following industrial
injury. A prospective study with comparison group and one-year
follow-up. Spine. 1985;10(6):482–93.
8. Isernhagen SJ. The comprehensive guide to work injury man-
agement. Gaithersburg, MD: Aspen; 1995.
9. Wind H, Gouttebarge V, Kuijer PP, Sluiter JK, Frings-Dresen
MH. The utility of functional capacity evaluation: the opinion of
physicians and other experts in the field of return to work and
disability claims. Int Arch Occup Environ Health. 2006;
79(6):528–34.
10. Menard MR, Hoens AM. Objective evaluation of functional
capacity: medical, occupational, and legal settings. JOSPT.
1994;19(5):249–60.
11. Soer R, Groothoff JW, Geertzen JH, van der Schans CP, Reesink
DD, Reneman MF. Pain response of healthy workers following a
functional capacity evaluation and implications for clinical
interpretation. J Occup Rehabil. 2008;18(3):290–8.
12. Reneman MF, Kuijer W, Brouwer S, Preuper HR, Groothoff JW,
Geertzen JH, et al. Symptom increase following a functional
capacity evaluation in patients with chronic low back pain: an
explorative study of safety. J Occup Rehabil. 2006;16(2):
197–205.
13. Gross DP, Battie MC. Factors influencing results of functional
capacity evaluations in workers’ compensation claimants with
low back pain. Phys Ther. 2005;85(4):315–22.
14. Reneman MF, Kool J, Oesch P, Geertzen JH, Battie MC, Gross
DP. Material handling performance of patients with chronic low
back pain during functional capacity evaluation: a comparison
between three countries. Disabil Rehabil. 2006;28(18):1143–9.
15. Asante AK, Brintnell ES, Gross DP. Functional self-efficacy
beliefs influence functional capacity evaluation. J Occup Rehabil.
2007;17(1):73–82.
16. van Abbema R, Lakke SE, Reneman MF, van der Schans CP, van
Haastert CJ, Geertzen JH, et al. Factors associated with functional
capacity test results in patients with non-specific chronic low
back pain: a systematic review. J Occup Rehabil. 2011;. doi:10.
1007/s10926-011-9306-4.
17. Gross DP, Battie MC. Predicting timely recovery and recurrence
following multidisciplinary rehabilitation in patients with com-
pensated low back pain. Spine. 2005;30(2):235–40.
18. Gross DP, Battie MC, Cassidy JD. The prognostic value of
functional capacity evaluation in patients with chronic low back
pain: part 1: timely return to work. Spine. 2004;29(8):914–9.
19. Matheson LN, Isernhagen SJ, Hart DL. Relationships among
lifting ability, grip force, and return to work. Phys Ther.
2002;82(3):249–56.
20. Kuijer PP, Gouttebarge V, Brouwer S, Reneman MF, Frings-
Dresen MH. Are performance-based measures predictive of work
participation in patients with musculoskeletal disorders? A sys-
tematic review. Int Arch Occup Environ Health. 2012;
85(2):109–23.
21. Streibelt M, Blume C, Thren K, Reneman MF, Mueller-Fahrnow
W. Value of functional capacity evaluation information in a
clinical setting for predicting return to work. Arch Phys Med
Rehabil. 2009;90(3):429–34.
22. Matheson LN, Matheson ML, Grant J. Development of a measure
of perceived functional ability. J Occup Rehabil. 1993;3:15–30.
23. Isernhagen SJ. Functional capacity evaluation: rationale, proce-
dure, utility of the kinesiophysical approach. J Occup Rehabil.
1992;2(3):157–68.
24. Reneman MF, Soer R, Gross DP. Developing research on per-
formance-based functional work assessment: report on the first
international functional capacity evaluation research meeting.
J Occup Rehabil. 2013;. doi:10.1007/s10926-013-9425-1.
25. Brouwer S, Dijkstra PU, Stewart RE, Goeken LN, Groothoff JW,
Geertzen JH. Comparing self-report, clinical examination and
functional testing in the assessment of work-related limitations in
patients with chronic low back pain. Disabil Rehabil. 2005;
27(17):999–1005.
26. Reneman MF, Jorritsma W, Schellekens JM, Goeken LN. Con-
current validity of questionnaire and performance-based disabil-
ity measurements in patients with chronic nonspecific low back
pain. J Occup Rehabil. 2002;12(3):119–29.
27. Wittink H, Rogers W, Sukiennik A, Carr DB. Physical func-
tioning: self-report and performance measures are related but
distinct. Spine. 2003;28(20):2407–13.
28. Elbourne DR, Campbell MK. Extending the CONSORT state-
ment to cluster randomized trials: for discussion. Stat Med.
2001;20(3):489–96.
29. Gross DP, Battie MC, Asante AK. Evaluation of a short-form
functional capacity evaluation: less may be best. J Occup Reha-
bil. 2007;17(3):422–35.
30. Klar N, Donner A. Current and future challenges in the design
and analysis of cluster randomization trials. Stat Med.
2001;20(24):3729–40.
31. Eldridge S, Cryer C, Feder G, Underwood M. Sample size cal-
culations for intervention trials in primary care randomizing by
primary care group: an empirical illustration from one proposed
intervention trial. Stat Med. 2001;20(3):367–76.
32. Stephens B, Gross DP. The influence of a continuum of care
model on the rehabilitation of compensation claimants with soft
tissue disorders. Spine. 2007;32(25):2898–904.
33. McHorney CA, Ware JE Jr, Raczek AE. The MOS 36-Item Short-
Form Health Survey (SF-36): II. Psychometric and clinical tests
of validity in measuring physical and mental health constructs.
Med Care. 1993;31(3):247–63.
34. Pollard CA. Preliminary validity study of the pain disability
index. Percept Mot Skills. 1984;59(3):974.
35. Finch E, Brooks D, Stratford P, Mayo N. Physical rehabilitation
outcome measures: a guide to enhanced clinical decision making.
2nd ed. Toronto: Canadian Physiotherapy Association; 2002.
36. Soer R, Poels BJ, Geertzen JH, Reneman MF. A comparison of
two lifting assessment approaches in patients with chronic low
back pain. J Occup Rehabil. 2006;16(4):639–46.
37. Brouwer S, Reneman MF, Dijkstra PU, Groothoff JW, Schelle-
kens JMH, Goeken LNH. Test-retest reliability of the Isernhagen
Work Systems Functional Capacity Evaluation in patients with
chronic low back pain. J Occup Rehabil. 2003;13:207–18.
38. Reneman MF, Jaegers S, Westmaas M, Goeken L. The reliability
of determining effort level of lifting and carrying in a functional
capacity evaluation. Work. 2002;18:23–7.
J Occup Rehabil
123

39. Reneman MF, Dijkstra PU, Westmaas M, Goeken LN. Test-retest
reliability of lifting and carrying in a 2-day functional capacity
evaluation. J Occup Rehabil. 2002;12(4):269–75.
40. Gross DP, Battie MC. Construct validity of a kinesiophysical
functional capacity evaluation administered within a worker’s
compensation environment. J Occup Rehabil. 2003;13(4):
287–95.
41. Durand MJ, Loisel P, Hong QN, Charpentier N. Helping clini-
cians in work disability prevention: the work disability diagnosis
interview. J Occup Rehabil. 2002;12(3):191–204.
42. Andrew Walsh D, Jane Kelly S, Sebastian Johnson P, Rajkumar
S, Bennetts K. Performance problems of patients with chronic
low-back pain and the measurement of patient-centered outcome.
Spine. 2004;29(1):87–93.
43. Shannon R, Hillsdon M. Motivational interviewing in musculo-
skeletal care. Musculoskeletal Care. 2007;5(4):206–15.
44. National Occupational Classification: Occupational descriptions.
Employment and Social Development Canada; 2011. Online
resource accessed October 30, 2013. Website: www.hrsdc.gc.ca/
eng/jobs/lmi/noc/index.shtml.
45. Krause N, Dasinger LK, Deegan LJ, Brand RJ, Rudolph L.
Alternative approaches for measuring duration of work disability
after low back injury based on administrative workers’ com-
pensation data. Am J Ind Med. 1999;35(6):604–18.
46. Donner A, Klar N. Pitfalls of and controversies in cluster ran-
domization trials. Am J Public Health. 2004;94(3):416–22.
47. Hopman WM, Towheed T, Anastassiades T, Tenenhouse A,
Poliquin S, Berger C, et al. Canadian normative data for the SF-
36 health survey. Canadian Multicentre Osteoporosis Study
Research Group. CMAJ. 2000;163(3):265–71.
48. Farrar JT, Portenoy RK, Berlin JA, Kinman JL, Strom BL.
Defining the clinically important difference in pain outcome
measures. Pain. 2000;88(3):287–94.
49. Soer R, Reneman MF, Vroomen PC, Stegeman P, Coppes MH.
Responsiveness and minimal clinically important change of the
pain disability index in patients with chronic back pain. Spine.
2012;12(11):1035–9.
50. Gross DP, Battie MC. Functional capacity evaluation perfor-
mance does not predict sustained return to work in claimants with
chronic back pain. J Occup Rehabil. 2005;15(3):285–94.
J Occup Rehabil
123


















![Black-Box Certification with Randomized Smoothing: A ...Black-Box Certification with Randomized Smoothing: A Functional Optimization Based Framework classifier with f] ˇ 0, then](https://img.pdfslide.us/doc/110x75/5fea16fbf0d2f6487630690b/black-box-certification-with-randomized-smoothing-a-black-box-certiication.jpg)