Embed Size (px)
Citation preview

International Orthopaedics (SICOT) (1985) 9: 147-152 International
Orthopaedics © Springer-Verlag 1985
A clinical study and classification of posterior spinal tuberculosis
K u s h K u m a r
Department of Orthopaedics, Mahatma Gandhi Institute of Medical Sciences Sevagram-Wardha (MS), India, 442102
Summary. Tuberculous involvement of the posterior elements o f the spine is uncommon. Review o f the literature reveals little information and there is scant mention o f this subject in standard textbooks o f orthopaedics. A study o f 27 cases o f such lesions seen over 6 years is presented, drawn from two se- parate centres, 21 from Central India and 6 f r o m South Eastern Iran. The clinical presentation, in- vestigations and treatment are analysed.
A new four point classification is described based upon the site o f the lesion, the stage o f the le- sion, associated lesions and neurological deficit.
R+sum~. L'atteinte tuberculeuse des blbments postb- rieurs du rachis n'est pas frbquente. La revue de la littbrature n'apporte que peu d'informations et les traitbs classiques d'orthopbdie ne donnent sur ce su-
jet que des notions sommaires. On prksente ici l'btude de 27 cas de tuberculose vertObrale postb- rieure observks en 6 ans, issus de deux centres dis- tincts, 21 du centre de l'Inde et 6 du Sud-est de l'Iran. Le tableau clinique, les examens complb- mentaires et le traitement sont analysbs.
Les auteurs proposent une classification nou- velle en quatre points tenant compte de l'emplace- ment et du stade kvolutif, de l'atteinte osseuse, des lbsions associbes et du dkficit neurologique.
Key words: Tuberculosis, Posterior spine, Classifi- cation
Spina l les ions are the c o m m o n e s t f o r m o f tuber - culosis o f b o n e a n d are seen in a b o u t 50% o f all pa t i en t s wi th skeletal tube rcu los i s [11, 19, 26]. A n y p a r t o f the sp ina l c o l u m n m a y be i n v o l v e d bu t it is m o s t c o m m o n l y seen in the dorsa l , d o r s o l u m - bar , l u m b a r a n d cerv ica l reg ions , in tha t o r d e r [3, 16]. I n m o r e t h a n 98% o f cases the b o d y o f the ve r t eb ra is i n v o l v e d a d j a c e n t to the disc. O t h e r
pa r t s o f the ve r t ebra , such as the p o s t e r i o r ele- m e n t s or ex t r adu ra l r eg ion , are r a re ly invo lved . Tube rcu lo s i s at these sites has no t b e e n d i scussed a d e q u a t e l y in the l i terature. This p a p e r r epo r t s de- tails o f 27 cases seen b y the a u t h o r ove r the last 6 years .
Material and methods
The present study is of patients seen in Central India [21] and South Eastern Iran [6] from 1977 to 1982. Ages ranged from 4 to 52 years with an average of 22.2 years. There were 17 males and 10 females. Nine cases had florid clinically detectable tu- berculosis elsewhere in the body. Six patients, though asymp- tomatic, had healed scars of previous Scrofula in the neck. One patient was suffering from miliary tuberculosis. There were two cases of reactivated infection.
After thorough clinical examination and investigation all patients were maintained on triple drug anti-tuberculous ther- apy in full dosage, and with rest from 3 to 6 months. Nineteen patients were admitted for operative decompression or exci- sion. The patients were followed up from 1.5 to 4.5 years from treatment. One died of miliary tuberculosis during treatment.
Clinical presentation
Pos te r io r sp ina l tube rcu los i s s h o u l d be suspec ted in the p r e s e n c e o f a co ld abscess, a p o s t e r i o r si-
Table 1.
Symptoms No. Percentage
Generalised weakness, symptoms related to tubercular toxaemia and localised pain in the back 8 30
Marked cachexia with chronic diffuse back ache 9 33
Swelling or discharging sinus in the back 20 74
Neurological deficit in the lower limbs 9 33
Radiating pain in groin or lower limbs 3 11
Chance detection 5 19

148 K. Kumar: A
nus, neurological deficit or spinal deformity. The presence of any of these signs should activate a high index of suspicion [Table I].
Cold Abscess
A cold abscess was found in 81.5% of cases of posterior spinal disease. The abscess presented in various forms (see Table 2).
In a few patients the abscesses could not be detected clinically but were seen radiologically as a paravertebral shadow. However not all para- vertebral shadows are abscesses and abscesses do not always cast a shadow. Following anti-tubercu- lous therapy a few of the abscesses disappeared, some diminished in size and some remained un- changed. Their contents however became thin and could be aspirated easily.
Sinuses
Sinuses were noted in 26% of cases and were char- acterized by undermined edges with serous or serosanguinous discharge, and a circle of pigmen- tation at the opening. Few of the sinuses dis- charged sequestra and, on probing, the posterior vertebral elements could not be reached in all cases. The sinuses when healed were deep with unstable scars and were at times adherent to un- derlying bone (Table 3). Many healed during anti- tuberculous therapy. Curettage or excision of the sinus was performed in those patients undergoing operation.
Neurological deficit
This was noted in 9 patients. Paraplegia was clas- sified according to the method of Goel [7]. Ac- cording to this classification nine patients had a neurological deficit ranging from grade I to grade III paraplegia and one patient had a grade IV type of paraplegia (Table 4). Most showed mainly motor involvement which was not only more se- vere but also earlier in appearance than its senso- ry counterpart. Reflexes disappeared last.
Spinal curvature
Spinal curvature alteration results primarily from the loss of stability of the anterior elements of the spine. Thus in most of our patients there was no abnormal spinal curvature. Four had a kyphosis and one had kypho-scoliosis. The latter was due to vertebral body collapse with rotation of the vertebra from lateral shift [24] due to associated apophyseal joint involvement.
clinical study and classification of posterior spinal tuberculosis
Table 2.
Type of Abscess No. Percentage
Abscess in the midline 4 18
Abscess near the midline or in the back 9 41
Bilateral abscesses in back 2 9
Psoas abscess 6 27
Abscess in Pettit's triangle 1 5
Table 3 .
Type of sinus No. Percentage
Midline discharging sinus 3 43
Sinus in Pettit's triangle 1 14
Healed deep sinus covered by unstable scar 2 29
Healed sinus adherent to the spinous processes 1 14
Table 4.
Paraplegia (after Goel)
Grade I: Weakness in the lower limbs appearing after exercise or prolonged walking. No sensory loss.
Weakness in the lower limbs but patient is able to manage work. On examination there is sensory dulling.
Lower limb weakness is severe enough to confine the patient to bed. Hypoaesthesia or anaesthesia present.
Complete sensory or motor loss with bladder and bowel involvement.
Grade II :
Grade III:
Grade IV:
Radiographic investigation
A well penetrated cone view or tomograms are es- sential in localisation of posterior spinal disease. Usually foci of less than 1 cm in diameter cannot be demonstrated by conventional radiographs [20] since the elements are superimposed on the body of the vertebra. Radiographs revealed isolated posterior element involvement in 21 cases (78%). Of these 12 involved the pedicle only, 4 the lami- na, 5 the transverse process and 1 the lamina and spinous process. No cases involved the spinous process alone. The lesions were distributed in the dorsal (16), dorso-lumber (8) and lumbar spine (3) respectively. Synovial involvement and crani- overtebral involvement was excluded from this study. Patients with a paravertebral shadow and associated osteoporosis were considered suspi-
K. Kumar: A clinical study and classification of posterior spinal tuberculosis 149
cious of tuberculosis. One patient developed a lyt- ic lesion of the pedicle during the course of inves- tigation. Three patients presented with cord com- pression but without evidence of tuberculosis. Myelography was indicated and invariably showed partial or complete block suggestive of extradural granuloma. There was no case of sub- dural absces.
Incidental detection of posterior spinal lesions
A small lytic lesion in the posterior elements of the vertebra was demonstrated radiologically in three patients suffering from back pain. In a fur- ther two posterior spinal involvement was detect- ed on intravenous urogram performed for chronic renal pathology (probably tuberculous in nature), and in one other case on a plain abdominal radio- graph taken for vague abdominal symptoms.
Table 6.
Cord Involvement Better Relatively poor prognosis prognosis
1. Degree Partial Complete
2. Duration Shorter Longer
3. Type Early onset Late onset
4. Rate of involvement Slow Rapid
5. Age Young Older
6. General condition Good Poor
ter bed was used until sound healing was consid- ered to have taken place. In other cases complete bedrest on a firm bed was employed. In a few cases early mobilisation had to be undertaken due to the development of pressure sores, but in most cases 3 - 6 months of complete bedrest was ad- vised.
Laboratory investigations
Repeated measurement of the erythrocyte sedi- mentation rate (ESR) was found to be a simple and dependable test for estimating the progress of the disease. The lymphocyte /monocyte ratio was not found to be of much prognostic value. Materi- al collected from every case was cultured for the acid fast bacillus (A.F.B.). Positive cultures after 6 -12 weeks incubation were seen in 5 out of 22 cases where pus or caseous material had been re- covered, and in 6 out of 15 cases where operative curettings were taken.
Operations
Excision or decompression of the lesion was per- formed in 19 cases (Table 5). These operations were performed under full antituberculous cover. In cases where there was lateral shift of the verte- bral column requiring fusion a prefabricated plas-
Table 5.
Operation No. Percentage
Aspiration (single or repeated) of the abscess
Curettage of the lesion and evacuation of the abscess
Laminectomy and excisional surgery of lesion
Laminectomy and excision of extradural granuloma
Curettage and excision of the lesion with spinal fusion
4 21
2 11
9 47
2 10.5
2 10.5
Results
All patients undergoing surgery for threatened cord compression without neurological signs did well postoperatively without evidence of recur- rence within a follow-up of between 1.5 and 4.5 years. Patients undergoing decompressive surgery for neurological deficit showed fair results. Those with extradural granuloma showed a very slow recovery time (6 -9 months following operation) and those with spinal tuberculoma failed to re- cover. The prognosis in respect of recovery of cord function was found to agree with that de- scribed by Tuli [23] in his book on "Tuberculosis of the Spine" (see Table 6).
Discussion
The literature on posterior spinal tuberculosis and extradural granuloma is so sparse that most of the standard text books of orthopaedics either describe it in a few lines or fail to mention it at all [1, 14, 25]. However in the developing countries where tuberculosis is a major problem it cannot be ignored. The exact incidence of posterior spi- nal disease is unknown. It has been estimated at less than 2% but may be between 5 and 10% in en- demic areas [8, 22]. Scott and Taor mention an in- cidence of 30.5%, which appears to be exception- ally high [21]. It may be that posterior vertebral body tuberculosis has also been included with tu- berculosis of the posterior elements by these au- thors.
Apart from the general signs and symptoms of toxaemia, which may be absent, slight pain and
150
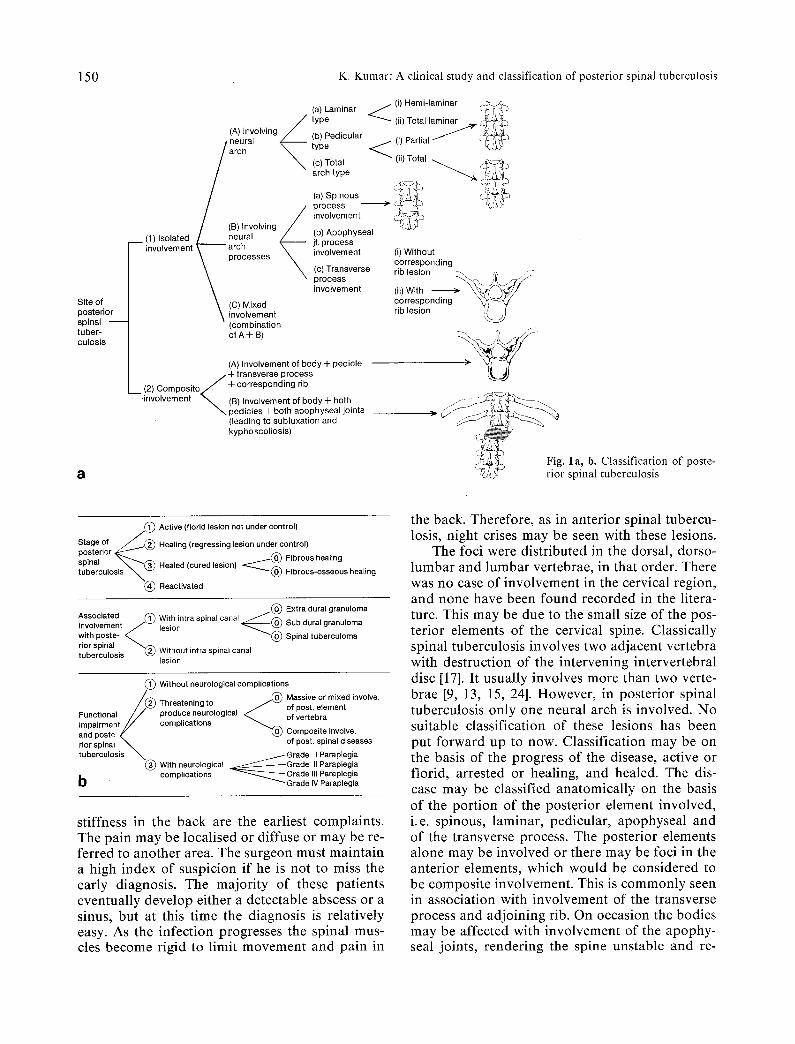
Site of posterior spinal tuber- culosis
a
K. Kumar: A clinical study and classification of posterior spinal tuberculosis
(a) Laminar / type
(A) Involving / / neural ~ (b) Pedicular type
arch /c) Total
arch type
(a) Spinous process involvement
/ (B) Involving (b) Apophyseal __ (1) Isolated / / n e u r a l /" . involvement y a r c h ~ ' it. process
~ processes ~ involvement
(c) Transverse process involvement
(C) Mixed \ involvement
(combination of A+B)
(A) Involvement of body -I- pedicle + transverse process
CompositeL / +corresponding rib (2) i , t r
,involvement ~ (B) Involvement of body+ both pedicles + both apophyseal joints (leading to subluxation and kyphoscoliosis)
~ (i) Hemi-laminar @s~-~/~
(ii) Total laminar ~,~'~1~ ~
(i) Without corresponding rib lesion ' ~ ' U (ii) With ~- corresponding rib lesion
i
/ / / - J~
/, • 1 a, b. Classification of poste-
~',~I rior spinal tuberculosis
Stage of j . @ Active (florid lesion not under control)
posterior ~ ' = " Healing (regressing lesion under control) spinal ~ ( ~ (~) Fibrous healing tuberculosis ~ Healed (curedlesion) ~ Fibrous-osseous healing
~ ) Reactivated
Associated (~) cana ~ / @ Extra dural granuloma involvement J With intra spinal I @ lesion Sub dural granuloma with poste- ~ .~ ~ @ Spinal tuberculoma rior spinal ~@ tuberculosis Without intra spinal canal
lesion
@ Without neurological complications / ~ . @ Massive or mixed involve,
/ '2@ Threatening to . ~ of post. element Functional / / produce neurological ~ . of vertebra mpa rment / / comphcstlons ~ f : . . . and poste-x// ~ ComposEte involve. rior spinal ~ of post. spinal diseases tuberculosis ~ / G r a d e I Paraplegia
(~) With neurological ~ G r a d e II Paraplegia complications ~ G r a d e III Paraplegia
b Grade IV Paraplegia
stiffness in the back are the earliest complaints. The pain may be localised or diffuse or may be re- ferred to another area. The surgeon must maintain a high index of suspicion if he is not to miss the early diagnosis. The majority of these patients eventually develop either a detectable abscess or a sinus, but at this time the diagnosis is relatively easy. As the infection progresses the spinal mus- cles become rigid to limit movement and pain in
the back. Therefore, as in anterior spinal tubercu- losis, night crises may be seen with these lesions.
The foci were distributed in the dorsal, dorso- lumbar and lumbar vertebrae, in that order. There was no case of involvement in the cervical region, and none have been found recorded in the litera- ture. This may be due to the small size of the pos- terior elements of the cervical spine• Classically spinal tuberculosis involves two adjacent vertebra with destruction of the intervening intervertebral disc [17]. It usually involves more than two verte- brae [9, 13, 15, 24]. However, in posterior spinal tuberculosis only one neural arch is involved. No suitable classification of these lesions has been put forward up to now. Classification may be on the basis of the progress of the disease, active or florid, arrested or healing, and healed. The dis- ease may be classified anatomically on the basis of the portion of the posterior element involved, i.e. spinous, laminar, pedicular, apophyseal and of the transverse process. The posterior elements alone may be involved or there may be foci in the anterior elements, which would be considered to be composite involvement. This is commonly seen in association with involvement of the transverse process and adjoining rib. On occasion the bodies may be affected with involvement of the apophy- seal joints, rendering the spine unstable and re-

K. Kumar: A clinical study and classification of posterior spinal tuberculosis 151
sulting in kyphoscoliosis or lateral shift of the spine, which will require spinal fusion.
Extradural granuloma, subdural abscess or spinal tuberculoma may be associated with poste- rior spinal tuberculosis [17]. On the basis of their neurological signs these lesions may be divided into three groups, those without neurological signs, those threatening to produce neurological complications (lesions involving a large portion of the neural arch or composite lesions) and those with established neurological complications of varying degree. Thus posterior spinal tuberculosis can be classified on the basis of site, stage of dis- ease, associated involvement and functional loss (Fig. 1 a and b).
A high lymphocyte count with a low monocyte count indicates high resistance, but the reverse in- dicates low resistance with a poor prognosis. The lymphocyte /monocyte ratio should therefore be more than 5 to 1 to favour operation [2]. This test, although said to be a better method of determin- ing the prognosis [25], was found to be no more helpful than simple repeated tests of the erythro- cyte sedimentation rate. Between 40% and 100% of positive cultures have been reported previously [4, 5, 22, 27] in contrast to the 20%-40% positive cultures in this series. This is most likely due to the fact that most patients in this series had re- ceived antituberculous therapy prior to obtaining cultures. This present study is comparable to that of Lakhanpal et al [121.
The advent of antituberculous drugs has revo- lutionised the treatment of bone and joint tuber- culosis in general and particularly of spinal dis- ease. The ability of antituberculous drugs to cure spinal foci was once doubted [8, 10, 18, 22] but is now well proved. Tuli et al. [24] obtained much higher concentrations of antituberculous drugs from human bone and questioned the convention- al concept of total surgical excision of bone le- sions [81.
The clinical evidence that these drugs are ef- fective in bone tuberculosis is shown by regres- sion of abscesses, sinuses and healing of the dis- ease. Reduction of the size of lesions following anti-tuberculous therapy but with failure to com- pletely control the disease, suggests that the cause is not failure of the drug to reach the lesion in suf- ficient concentration but that other factors may come into play, such as resistance of the organ- ism, non-compliance of the patient or mechanical problems, as may be encountered with a large se- questrum to which the drug may not have access.
Posterior spinal tuberculosis is notorious for causing early cord compression, probably due to mechanical pressure by the tuberculous debris in- to the spinal canal when recumbent. Therefore early surgery may have to be undertaken, not be- cause the efficacy of the anti-tuberculous drug is in doubt, but to reduce the actual bulk of the tu- berculous infection and debris which will elimi- nate the possible risk of cord compression. An ex- tradural granuloma, once suspected, should be excised, since if treated conservatively by anti- tuberculous therapy the granuloma will be re- placed by fibrous scar tissue which will maintain the compression.
References
1 Campbell (1980) Operative Orthopaedics, 6th edn, Vol. II, C.V. Mosby, Saint Louis Igaku Shoin Ltd Tokyo
2 Campos OP (1955) Bone and Joint Tuberculosis and its treatment. J Bone Joint Surg 37A: 937
3 Cleveland M, Bosworth DM (1942) Pathology of tubercu- losis of spine. J Bone Joint Surg 24:527-546
4 Dahl HK (1951) Examination of pH in tuberculosis pus. Acta Orthop Scand 20:176
5 Friedman B (1966) Chemotherapy of tuberculosis of the spine. J Bone Joint Surg 48A: 451-474
6 Girdlestone GR, Somerville EW (1952) Tuberculosis of Bone and Joint, 2nd Edn, Oxford University Press, Lon- don
7 Goel MK (1967) Treatment of Pott's paraplegia by op- eration. J Bone Joint Surg 49B: 674-681
8 Hodgson AR, Stock FE (1956) Anterior spinal fusion. A preliminary communication on the radical treatment of Pott's disease and Pott's paraplegia. Br J Surg 44: 266-275
9 Hodgson AR, Stock FE (1960) Anterior spinal fusion for the treatment of tuberculosis of the spine. J Bone Joint Surg 42A: 295-310
10 Hodgson AR, Skinsnes OK, Leong CY (1967) The pa- thogenesis of Pott's paraplegia. J Bone Joint Surg 49A: 1447 - 1156
11 Konstam PG (1963) Spinal tuberculosis in Nigeria. Ann R Coil Surg Eng 32:99-114
12 Lakhanpal VP, Tuli SM, Singh H, Sen PC (1974) The va- lue of histology culture and guinea pig inoculation exami- nation in osteo-articular tuberculosis. Acta Orthop Scand 45:36-42
13 Martin NS (1970) Tuberculosis of the spine (A study of the results of treatment during the last twenty five years). J Bone Joint Surg 52B: 613-628
14 Mercer W, Duthie RB (1967) Orthopaedic Surgery, 6th edn. Edward Anrold, London
15 Mukopadhaya B, Mishra NK (1957) Tuberculosis of the spine. Ind J Surg 19:59-81
16 Paus B (1964) Treatment for tuberculosis of the spine. Ac- ta Orthop Scand (Suppl): 72
17 Rahman N (1980) Atypical forms of spinal tuberculosis. J Bone Joint Surg 62B No. 2:162-165
18 Roar R (1958) Tuberculosis of the spine. J Bone Joint Surg 40B: 3-5
19 Sanchis-Olmos V (1948) Skeletal tuberculosis. Williams and Wilkins, Baltimore

152 K. Kumar: A clinical study and classification of posterior spinal tuberculosis
20 Schmorl G, Junghans H (1959) The human spine in health and disease. Grune, New York
21 Scott JE, Taor, WS (1982) The changing pattern of bone and joint Tuberculosis. J Bone Joint Surg 64 B: 250
22 Somerville EW, Wilkinson MC (1965) Girdlestone's Tu- berculosis of bone and joint, 3rd Edn. Oxford University Press, London
23 Tuli SM (1975) Tuberculosis of the spine. Amerind Pu- blishing Co. Pvt. Ltd, New Delhi.
24 Tuli SM, Kumar K, Sen PC (1977) Penetration of anti-
tubercular drugs in clinical osteoarticular tubercular le- sions. Acta Orthop Scand 48:362-368
25 Turek SL (1977) Orthopaedic principles and their applica- tion, 3rd Edn Lippincott, Philadelphia
26 Wilkinson MC (1949) Observations on the pathogenesis and treatment of skeletal tuberculosis. Ann R Coll Surg Engl 4:168-192
27 Wilkinson MC, Notley B (1953) Synovectomy and curet- tage in tuberculosis of joints. J Bone Joint Surg 35B: 209-223





























