Embed Size (px)
Citation preview

HUMAN MUTATION 9:209�225 (1997)
© 1997 WILEY-LISS, INC.
HUMU 694
MUTATION UPDATE
A Clinical Overview of WT1 Gene Mutations
Melissa Little* and Christine WellsCentre for Molecular and Cellular Biology, The University of Queensland, St. Lucia, 4072 Australia; Fax: 61-7-3365-4388
Communicated by R.G.H. Cotton
Mutations in the WT1 gene were anticipated to explain the genetic basis of the childhood kidney cancer,Wilms‘ tumour (WT). Six years on, we review 100 reports of intragenic WT1 mutations and examinethe accompanying clinical phenotypes. While only 5% of sporadic Wilms’ tumours have intragenicWT1 mutations, >90% of patients with the Denys-Drash syndrome (renal nephropathy, gonadal anomaly,predisposition to WT) carry constitutional intragenic WT1 mutations. WT1 mutations have also beenreported in juvenile granulosa cell tumour, non-asbestos related mesothelioma, desmoplastic small roundcell tumour and, most recently, acute myeloid leukemia. Hum Mutat 9:209–225, 1997. © 1997 Wiley-
Liss, Inc.
KEY WORDS: Wilms’ tumour, WAGR syndrome, WT1, tumour-suppressor, Denys-Drash syndrome
INTRODUCTION
The WT1 gene encodes multiple isoforms of a zinc-finger containing protein (52-54kD) presumed toregulate the activity of a subset of target genes viaDNA binding (Rauscher 1993; Hastie, 1994). This10 exon gene produces four distinct WT1 isoformsresulting from the presence or absence of two alter-nate splices (Haber et al., 1991). The 51bp exon 5 isvariably spliced, has an undefined function and is notpresent in lower vertebrates (Carroll and Vize 1996;Kent et al., 1995). Use of an alternative splice donorsite at the end of exon 9 results in the insertion ofthree amino acids, lysine-threonine-serine (KTS), be-tween zinc fingers (ZF) 3 and 4. This insertion is alsopresent in the lower vertebrates (Carroll and Vize,1996; Kent et al., 1995) and affects the ability of theZF region to bind nucleic acids (Bickmore et al., 1992;Caricasole et al., 1996; Rauscher, 1993; Hastie, 1994).The ratio of WT1 isoforms is believed to be stabletemporally and spatially (Haber et al., 1991), withthe KTS alternate splice present in 80% of transcripts.
WT1 was isolated from the short arm of chromo-some 11, band p13 (Call et al., 1990; Gessler et al.,1990). This was the result of a positional cloning ef-fort aimed at identifying the gene responsible for thechildhood kidney cancer, Wilms‘ tumour (WT). Theregion was of particular interest as cytogeneticallyvisible deletions of 11p with a common overlap ofband p13 had been reported in both sporadic WTand WT in association with the contiguous gene syn-drome WAGR (WT, Aniridia, Genitourinary anoma-
lies and mental Retardation) (Francke et al., 1979).It was presumed that a tumour suppressor gene layin this region and that, as is the case for the Rb1gene in retinoblastoma, inactivation of both copiesof this gene would lead to tumorigenesis (KnudsonJr. and Strong 1972). Hence the excitement whenWT1 appeared to encode a transcription factor. Sixyears since the isolation of WT1, the estimated per-centage of Wilms’ tumours with WT1 mutations isonly 10–15% (Reddy and Licht, 1995). However, theintensive investigation afforded to WT1 has revealedsome remarkable facts about the normal physiologicalfunction of this gene and has shed significant light onthe molecular pathology of the Denys-Drash syndrome.
WT1 is expressed during vertebrate developmentwithin the kidneys, gonads, spleen and the lining ofthe abdominal cavity (mesothelium) (Armstrong etal., 1992; Pritchard-Jones et al., 1990). Within thekidney, expression commences as the ureteric budreaches the metanephric mesenchyme. This coincideswith a transition from mesenchyme to epitheliumwhich results in tubule formation, progressivearborisation and the eventual formation of the renaltubules and glomeruli. WT1 expression increases asthis process continues, marking the S and comma-shaped bodies and peaking in the podocyte layer ofthe glomerulus (Pritchard-Jones et al., 1990). Reflect-ing this, mice constitutionally homozygous for inac-
Received 28 March 1996; accepted 3 April 1996.
*Correspondence to Dr. Melissa Little.

210 LITTLE AND WELLS
tivation of WT1 lack both kidneys and gonads(Kreidberg et al., 1993). However, heterozygotes forthe same knockout show no ill effects and do not goon to develop Wilms’ tumour. Nevertheless, both thepattern of expression and the phenotype of the knock-out animal verify an important role for this gene inurogenital development. They also point the wayclinically, since the subgroup of WT patient with as-sociated genital anomalies have a far higher rate ofWT1 mutation, directly reflecting the true functionof this gene during development (Pelletier et al.,1991a; Pelletier et al., 1991b). More recently, avariety of other tumour types have been demon-strated to carry WT1 mutations (Ladanyi andGerald, 1994; Park et al., 1993b), including acutemyeloid leukemia (King-Underwood et al., 1996;Pritchard-Jones et al., 1994), each contributinginsight toward the true function of the gene. It ispossible that this gene will ultimately become ofmore clinical relevance to these types of cancerthan to Wilms’ tumour itself.
WT1 Mutations in the Denys-DrashSyndrome Patients
Wilms’ tumour represents one of the most com-mon solid tumours of childhood with a frequency of1 in 10,000 live births (Matsunaga, 1981). Althoughapproximately 90% of Wilms’ tumours arise as spo-radic unilateral lesions, WT is also seen in associa-tion with a number of congenital anomaly syndromes.The most pivotal with respect to the isolation of acandidate gene has been WAGR, as previously dis-cussed. Wilms’ tumour is also associated with theextremely rare Denys-Drash syndrome (DDS) (De-nys et al., 1967; Drash et al., 1970). This syndrometraditionally encompassed patients with the triad ofcongenital nephrotic syndrome leading to end-stagerenal failure, XY pseudohermaphroditism and Wilms’tumour. The kidney pathology characteristic of DDSis mesangial sclerosis (Eddy and Mauer, 1985). WhileDDS patients do not display 11p deletions, the com-bination of genital and renal anomalies led to an in-vestigation of WT1 involvement. Such patients wereshown to be constitutionally heterozygous for WT1point mutations (Pelletier et al., 1991a), with themutation reaching homozygosity/hemizygosity in thetumours of almost all cases (Little et al., 1993). Fur-ther investigations have identified similar constitu-tional mutations in related patients such that thedefinition of DDS has now been relaxed to includeXY individuals with a range of genital anomalies frommild to severe as well as XX individuals displayingnephropathy and WT (reviewed in Hastie, 1994).Some of these XX females have streak gonads, but
the majority have no gonadal anomalies. By way ofdefinition, the triad of features classified as DDSshould remain nephropathy involving mesangialsclerosis, WT and genital/intersex anomalies(Eddy and Mauer, 1985). The term incompleteDDS (Bardeesy et al., 1994) is used for patients withnephropathy together with genital anomaly ORWilms’ tumour, the validity of which has been borneout by the mutation analysis. Table 1 lists a total of48 complete and incomplete DDS patients. From allthe studies cited here, only three patients with thiscombination of clinical features have failed to dis-play a constitutional WT1 mutation (Baird et al.,1992b; Nordenskjold et al., 1994).
A Hot Spot for Mutation
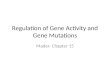
Table 1 shows that the zinc finger region contains92% of WT1 mutations in DDS. This bias is high-lighted in Figure 1. The first study examining WT1in DDS patients demonstrated constitutional het-erozygosity for exon 9 (ZF3) missense mutationswithin all 10 patients examined (Pelletier et al.,1991a) with 8/10 individuals displaying a C to T sub-stitution resulting in the replacement of arginine 394with tryptophan (R394W). This ‘hot spot’ remainsthe most commonly reported DDS WT1 mutation,being present in 39.6% (19/48) of the patients re-viewed here (see Fig. 1). Exon 9 itself shows a highfrequency of mutations accounting for 60.4% (29/48) of all mutations and 76.3% (29/38) of all mis-sense mutations. WT1 missense mutations within thezinc finger region affect either amino acids involveddirectly in DNA binding (62.5%; 30/48), such asR394W, or the cysteine and histidine residues criti-cal for ZF structure (16.7%; 8/48). All these missensemutations interrupt DNA binding capacity in vitro(Little et al., 1995; Pelletier et al., 1991a). The sameoccurs as a result of all termination mutations,whether due to nonsense point mutations (6.3%; 3/48), frameshift termination due to deletion (2.1%;1/48) or insertion (4.2%; 2/48). The final class of DDSpatients (6.3%; 3/48) contain intron 9 point muta-tions which prevent the inclusion of the KTS alter-native splice between ZF3 and ZF4.
It could be argued that this clustering of muta-tions within the zinc fingers has been biased by a pref-erential examination of exons 7-10 in such patients.Table 6 provides a list of the WT1 exons screened forWT1 mutations in each study and clearly the zincfinger containing exons are most frequently exam-ined. However, as noted previously, there are veryfew DDS patients analysed in which no mutation hasbeen detected. Conversely, despite considerable at-

A CLINICAL OVERVIEW OF WT1 GENE MUTATIONS 211
TABLE 1. WT-1 Mutations Associated With Denys-Drash Syndrome (n=48)
Patient Sex:genotype/ Clinicalnos. phenotype description Exon Mutationsa Constitb Tumourc Author
1 XY Male nephrotic 3 Y221X Het N/A Bardeesy et al.,syndome, bilat. (663CÃG) 1994WT, bilat.cryptochidism
2 XY Ambiguous DDS nephropathy, 6 821insG Het N/A Baird et al.,bilat. WT FR-STOP 1992b
(274+0)d
3 XX Female nephrotic 6 827delA Het N/A Bardeesy et al.,syndrome unilat. FR-STOP 1994WT (275+11)
4 XY Ambiguous DDS nephropathy, int. 6 897+1GÃC, Het Hom Schneider et al.,unilat. WT presumed 1993
splicing fromexon 4-7 or 5-7& FR-STOP(249+6 or266+6)
5 XX Female DDS nephropathy, 7 C330Y Het No Bruening et al.,PRB (989GÃA) tumour 1992
6 XX Female DDS nephropathy, 8 C355Y Hom Hom Kikuchi et al.,unilat. WT, no PRB (1064GÃA) 1995;
Sakai et al.,1993
7 N/A Female DDS nephropathy, 8 C360G Het Het Little et al.,cerebral atrophy, (1078TÃG) 1993unilat. WT
8 XY Female DDS nephropathy 8 C360Y Het No Clarkson et al.,(1079GÃA) tumour 1993
9 XY Ambiguous DDS nephropathy, 8 R362X Het Hom Clarkson et al.,micropenis, (1084CÃT) 1993;cryptorchidism, Little et al.,hypospadias, bilat. 1993WT
10 XY Female DDS nephropathy, 8 R366H Het No Pelletier et al.,dysgenic testis, (1097GÃA) tumour 1991agonadoblastomae
11 XY Ambiguous DDS nephropathy, 8 R366H Het N/A Baird et al.,unilat. WT (1097GÃA) 1992b
12 XY Female DDS nephropathy, 8 R366H Het No Devriendt et al.,diaphragmatic (1097GÃA) tumour 1995hernia, PRB
13 XY Female DDS nephropathy 8 R366H Het No Norden-(1097GÃA) tumour skjold et al.
1995a14 XY Male DDS nephropathy, 8 H373Q Het No Little et al.,
hypospadias (1119CÃG) tumour 199315 XY Female DDS nephropathy, 8 H377Y Het No Coppes et al.,
bilat. nephrectf, (1129CÃT) tumour 1992inherited fromunaffected father
16 XY Ambiguous DDS nephropathy, 8 H377R Het Hemi Norden-hypospadias, (1130AÃG) skjold et al.,unilat. WT, bilat. 1994cryptorchidism.
17 N/A Male DDS nephropathy, 9 1157 insA Het No Ogawa et al.,(ESRF), bilat. FR-STOP tumour 1993acryptorchidism, (386+11)hypospadias.
18 N/A Ambiguous DDS nephropathy 9 R394W Het No Pelletier et al.,(1180CÃT) tumour 1991a
19 XY Ambiguous DDS nephropathy, 9 R394W Het Hemi Pelletier et al.,WT, juvenile (1180CÃT) 1991agranulosa celltumourg
20 XX Female DDS nephropathy, 9 R394W Het N/A Pelletier et al.,bilat. WT (1180CÃT) 1991a
(continued)

212 LITTLE AND WELLS
TABLE 1. WT-1 Mutations Associated With Denys-Drash Syndrome (n=48) (Continued)
Patient Sex:genotype/ Clinicalnos. phenotype description Exon Mutationsa Constitb Tumourc Author
21 XX Female DDS nephropathy, 9 R394W Het N/A Pelletier et al.,WT (1180CÃT) 1991a
22 XY Ambiguous DDS nephropathy, 9 R394W Het N/A Pelletier et al.,WT (1180CÃT) 1991a
23 XY Ambiguous DDS nephropathy, 9 R394W Het Hemi Pelletier et al.,WT (1180CÃT) 1991a
24 XX Female DDS nephropathy, 9 R394W Het Hemi Pelletier et al.,streak gonad & (1180CÃT) 1991anormal femalegenitalia, WT
25 XY Ambiguous DDS nephropathy, 9 R394W Het N/A Baird et al.,unilat. WT (1180CÃT) 1992b
26 XY Female DDS nephropathy, 9 R394W Het No Baird et al.,bilat. nephrect. (1180CÃT) tumour 1992b;
Little et al.,1993
27 XY Female DDS nephropathy, 9 R394W Het N/A Baird, et al.,unilat. WT (1180CÃT) 1992b;
Clarkson et al.,1993
28 XY Ambiguous DDS nephropathy, 9 R394W Het N/A Bruening et al.,Wilms� tumour (1180CÃT) 1992
29 XY Female DDS nephropathy, 9 R394P N/A Hemi (?) Bruening et al.,WT (1181GÃC) 1992
30 XX Female DDS nephropathy, 9 R394W Het No Coppes et al.,bilat. WT (1180CÃT) tumour 1992
31 XY Ambiguous DDS nephropathy, 9 R394W Het No Coppes et al.,bilat. nephrect. (1180CÃT) tumour 1992
32 XY Ambiguous DDS nephropathy, 9 R394W Het N/A Poulat et al.,unilat. WT (1180CÃT) 1993
33 XX Female DDS nephropathy, 9 R394W Het N/A Sakai et al.,unilat. WT (1180CÃT) 1993
34 XY Female DDS nephropathy, 9 R394W Het No Sakai et al.,dysgenic gonads (1180CÃT) tumour 1993
35 XY Female DDS nephropathy, 9 R394W Het No Tsuda et al.,pseudohermaphro- (1180CÃT) tumour 1993ditism
36 XY Ambiguous DDS nephropathy, 9 R394W Het N/A Norden-hypospadias, bifid (1180CÃT) skjold et al.,scrotum, unilat. 1994WT, bilat.cryptorchidism
37 XY Male mesangial and 9 R394W Het N/A Webb et al.,glomerular (1180CÃT) 1995sclerosis,hypospadias
38 XY Ambiguous DDS nephropathy, 9 D396N Het N/A Pelletier et al.,WT (1186GÃA) 1991a
39 XY Male DDS nephropathy, 9 D396N Het N/A Baird et al.,unilat. WT (1186GÃA) 1992b
40 XX Female DDS nephropathy, 9 D396N Het Hom Little et al.,bilat. WT (1186GÃA) 1993
41 XY Ambiguous DDS nephropathy, 9 D396N Het Hom Norden-hypospadias, bifid (1186GÃA) skjold et al.,scrotum, unilat. 1994WT, bilat.cryptorchidism.
42 XX Female DDS nephropathy, 9 D396N Het Hemi Norden-unilat. WT (1186GÃA) skjold et al.,
199443 XX Female DDS nephropathy, 9 D396G Het No Pelletier et al.,
(1187AÃG) tumour 1991a44 XX Female DDS nephropathy, 9 L398P Het N/A Tsuda et al.,
unilat. WT (1993TÃC) 199345 XX Female DDS nephropathy, 9 H401Y Het N/A Baird & Cowell
unilat. WT (1201CÃT) 1993
(continued)

A CLINICAL OVERVIEW OF WT1 GENE MUTATIONS 213
tention, there has never been a mutation found inexon 10 in a DDS patient.
WT with Genital Anomalies Versus Denys-DrashSyndrome
Patients displaying WT with associated genitalanomalies are listed in Table 2. The distinction be-tween incomplete DDS and WT with associated geni-tal anomalies lies in the absence of nephropathy inthe latter. The mutation patterns in this group (seeFig. 1; Table 2) differ from those in Table 1 in thatthere are no ZF or missense mutations and less of theN-terminus remains in this group of patients. All re-sult in termination prior to exon 7. Four patients inTable 1 (patients 1-4) displayed similar mutations tothose seen in Table 2, with only mild genital anoma-lies in the male individuals. However, the separationof these two groups of patients has not revealed aclear basis for the absence of nephropathy. Table 2patients may simply emphasise the variation in pen-etrance of WT1 mutations, as they could be diag-nosed as incomplete DDS based on their genotype.
Dominant-Negative Activity in DDS
The unifying feature of WT1 mutation in DDSpatients is the removal or inactivation of DNA bind-
ing by the zinc fingers (Little et al., 1995). The samecould be said for patients in Table 2. The phenotypicdistinction lies in the nephropathy of DDS patients(Table 1). It has been argued that the apparent domi-nant-negative (antimorph) nature of DDS mutationsresults from the involvement of the remaining N-ter-minal portion of the protein in WT1 self-association,without being able to participate in transcriptionalregulation. Thus self-association between wildtypeand DDS mutant WT1 prevents normal WT1 func-tion. The subnuclear localisation of different isoformsvaries, with the –KTS-containing isoforms showinga diffuse nuclear staining while the +KTS-contain-ing isoforms are seen in nuclear ‘speckles’ correspond-ing to the spliceosomes (Larsson et al., 1995). Thefunctional significance of this localisation pattern isnot yet understood. However, mutant WT1 contain-ing R394W or ZF3 truncation mutations whether con-taining KTS or not, also move to the ‘speckles’ (Larssonet al., 1995; Englert et al., 1995). Thus, self-associationbetween wildtype and DDS mutant proteins may re-move the wildtype protein from the DNA and into thespeckles inappropriately (Englert et al., 1995).
How much of the N-terminus is necessary for self-association? In vitro assays show that self associationdomain/s reside within the first 180 amino acids of WT1
TABLE 1. WT-1 Mutations Associated With Denys-Drash Syndrome (n=48) (Continued)
Patient Sex:genotype/ Clinicalnos. phenotype description Exon Mutationsa Constitb Tumourc Author
46 XY Female DDS nephropathy, int. 9 1228+5h Het No Bruening et al.,GÃA tumour 1992(lack of+KTSisoform)
47 XY Female DDS nephropathy, int. 9 1228+5GÃA Het No Konig et al.,(lack of tumor 1993+KTSisoform)
48 XY Ambiguous nephrotic int. 9 1228+5GÃA Het No Bardeesy et al.,syndrome (lack of tumour 1994
+KTSisoform)
aNucleotides are counted from the A of the start codon.bPresence of Heterozygosity (Het) or homozygosity (Hom) for the mutation in constitutional material.cPresence of Het, Hom or hemizygosity (Hemi) within the tumour.dFR-STOP, frameshift resulting in a termination (last correct amino acid + number of additional amino acids prior to termination).eNot examined for mutations.fBilateral nephrectomy.gAlso reported in Table 5.h+N refers to the number of nucleotides into the intron from the preceding exon. The 9 nucleotides of the KTS alternate splice areregarded as exonic, representing nucleotides 1220-1228.Notes on Tables 1�5: Mutation nomenclature as per Beaudet and Tsui, 1993. Nucleotides are numbered from the A of the common startATG and include the 51bp of exon 5 and 9bp of the KTS alternate splice. Amino acids are numbered from the same ATG (total protein of449 amino acids, including exon 5 and KTS alternate splices). Some reports investigated mutations at the transcript level without fullycharacterising the mutation at a genomic level and others investigated mutations at the genomic level without verifying resultant tran-script. Where an end product was not verified, it is listed as presumed and a premature termination is calculated from the primarysequence. BWS, Beckwith-Wiedemann syndrome; DDS, Denys-Drash syndrome; WAGR, Wilms� tumour, aniridia, genitourinary abnor-malities, mental retardation syndrome; WT, Wilms�s tumour, ESRF, end stage renal failure; PRB, persistent renal blastema; N/A, informa-tion not available; int; intron; Unilat, unilateral; bilat., bilateral; LOH, loss of constitutional heterozygosity; mon., months.

214 LITTLE AND WELLS
(Reddy et al., 1995). The most 5´ truncation seen in aDDS patient results in a truncation within exon 3 (pa-tient 1), which supports this in vitro data. In compari-son, the mutation in patient 49 created a terminationat amino acid 29 (see Table 2), leaving too few aminoacids to allow for WT1 protein self-association (GregHolmes, personal communication). This patient wasan XY male with bilateral cryptorchidism and a horse-shoe kidney, but no nephropathy. This would supportthe hypothesis that while the renal nephropathy of DDSmay result from self-association with a mutant protein,the genital anomalies are more likely to result from adecrease in wildtype protein, thereby explaining theirpresence in WAGR patients.
Several factors confound this model particulardominant-negative model. The first of these comesfrom those DDS patients with intron 9 mutations (pa-tients 46–48) in which the only disturbance is a lackof expression of transcripts containing the +KTSinsertion from one WT1 allele. In contrast to previ-ous models, presumably less WT1 protein now re-sides in the nuclear ‘speckles’. Yet this disturbanceto isoform ratios has led to the pathology observed(such a mutation has not been reported in the ab-sence of nephropathy). A mouse model of DDS hasbeen created in which a ZF 3 truncation results inthe characteristic nephropathy seen in DDS patients(Charles Patek, personal communication). Unexpect-
FIGURE 1. Ideogram of the WT1 transcript indicating allreported intragenic mutations according to the clinicalphenotype. The 10 exons are represented as boxes in lin-
ear order, with the introns represented as gaps betweeneach exon. Both alternately spliced regions (exon 5 andKTS) are shaded.

A CLINICAL OVERVIEW OF WT1 GENE MUTATIONS 215
edly, while the levels of mutant and wildtype tran-scripts are equivalent, the level of the mutant pro-tein appears to be far less than that of wildtypeprotein, yet a phenotype is observed. This clearlycomplicates the interpretation that DDS results fromcompetition between mutant and wild-type proteinfor self-association, although the interactions betweenisoforms may be far more complex than a simpledimerisation. Finally, although +KTS-containingisoforms predominantly reside in the nuclear ‘speck-les’, there is evidence that they also participate intranscriptional regulation, but show different DNAbinding affinities and specificities to isoforms lackingthis insertion (Bickmore et al., 1992; Caricasole etal., in press, Little et al., in press). In addition, WT1ZFs, particularly those containing this alternate splice,can bind RNA as well as DNA (Caricasole et al.,1996; Larsson et al., 1995) further complicating WT1function. In conclusion, as with many diseases oncelinked with a causative gene, it is difficult to resolvethe phenotype with genotype.
There has been a gradual altering of the pheno-typic characteristics of DDS based upon the pres-ence of WT1 mutation. Is this relaxation of definitionto include female and XY individuals with mildergenital anomalies hindering progress in understand-ing the molecular aetiology of DDS? From a clinicalviewpoint, this relaxation is justified as early prophy-lactic nephrectomy and transplantation in such pa-tients may be necessary to address the risk of Wilms’tumour. At the molecular level, we must be wary oftrying to fit all patients thus described as DDS intoone aetiological model when all the information isnot available. At the level of phenotype, reports foreach patient vary in their depth of clinical and patho-logical description, while at the level of genotype we
still do not understand when, where, how, upon whatgenes and under the influence of what genes WT1acts. There is undoubtedly a strong bias in patientswith classical DDS for C-terminal ZF inactivatingmutations. If only those patients with an XY karyo-type and female external genitalia are considered(n=13; listed as XY females in Table 1), all muta-tions are exon 8 or 9 missense mutations or intron 9mutations which result in lack of the +KTS inser-tion. While, less affected patients (XY male, XX fe-male, XY ambiguous) share the same mutations, thosewith the originally described XY pseudohermaphro-ditism may share defects in other modifier genes lead-ing to a more severe phenotype.
WT1 and Sporadic Wilms� Tumour
Table 3 lists all of the fully characterised WT1 in-tragenic mutations in patients presenting with Wilms’tumour alone. In contrast to the high success ratefor WT1 mutation detection in DDS, the screeningof a great many unilateral and bilateral sporadicWilms’ tumours has been remarkably unproductive.Within the 14 reports used to compile Table 3, 518patients with WT were examined with 6.0% (34 in-dividuals) showing intragenic WT1 mutations (seeTable 6; note that this Table also includes studies ofother tumour types). This information is complicatedby the fact that many of the larger reports includeDDS and WAGR patients as well as sporadic patientsand don’t detail clinical data for any patients otherthan those shown to carry a mutation. By discount-ing those patients shown to have a WT1 mutationbut displaying DDS, WAGR or WT with genitalanomalies (reported in Tables 1, 2, and 4), 26 (5.1%)patients displaying WT without any associatedanomalies were shown to carry WT1 intragenic mu-
TABLE 2. Intragenic WT1 Mutations in Wilms� Tumour Patients With Associated Genital Anomalies,Excluding Denys-Drash Syndrome and WAGR Patients (n=4)
Patient Sex:genotype/ Clinicalnos. phenotype description Exon Mutations Constit Tumour Author
49 XY Male WT, bilat. 1 87 ins5 Het Hom Huff et al.,cryptorchidism, FR-STOP 1995horseshoe kidney (29+60)
50 N/A bilat. WT, 4 674 del17a Het Hom Pelletier et al.,hypospadias, FR-STOP 1991bundescended left (223+4)testicle.
51 N/A Male bilat. WT, bilat. 6 Y271X Het Hemi Nordenskjoldcryptorchidism, (813CÃG) et al., 1995b
52 N/A hypospadias, unilat. 6 875 delG Het Hom Pelletier et al.,WT, bilat. FR-STOP 1991bcryptorchidism. (291+15) AlsoFather with history present inof WT. father (constit).
a17 bp deletion from 674A to 690A inclusive. Nomenclature as per Beaudet and Tsui (1993).

216 LITTLE AND WELLS
TABLE 3. Intragenic WT1 Mutations in Sporadic Wilms� Tumour Patients (n=26)
Patient Genotype/ Clinicalno. Age phenotype description Exon Mutations Constit Tumour Author
53 5 years N/A WT 1 80 del4 Nil Het Huff et al.,FR-STOP (27+60) 1995
54 11.5 N/A Female WT, no PRB, 1 375 del5 Nil Hemi Gessler et al.,mon. glomeruloscl- FR-STOP (125+2) (large 1994
erosis, deletioninterstitial of othernephritis. allele)
55 4 years Female unilat. WT, 2 F154S Nil Heta Park et al.,PRB, putative (461TÃC) 1993aBWS
56 11 Female unilat. WT, 2 484 ins4 (dup. Nil Homa Park et al.,mon. PRB 480C-484T) 1993a
FR-STOP (161+18)57 4 years XY Male WT, PRB, 2 P180S N/A Het Gessler et al.,
minor foot (541CÃT) 1994anomaly
58 N/A N/A sporadic 8/3 R362X (1084CÃT) Nil Hom Varanasi et al.,unilat. WT /581ins7 (One on 1994
FR-STOP (194+31) eachallele)
59 1 year N/A Female bilat. WT int4 747+1 del 11kb; Het Hom Huff et al.,splicing from exon (One on 19914 to 7 & FR-STOP each(299+8) allele)
60 8 mon. N/A bilat. del. presumed splicing Het Hom Nordenskjoldmultifocal WT 6&7 from exon 4-8 or et al., 1995b
5-8; presumed FR-STOP (249+0 or266+0)
61 12 mon. Male unilat. WT 6&7 del8kb Het Hom Tadokoro, et al.(recombination 1992event betweenintron 5&7);presumed splicingfrom exon 5-8 &FR-STOP (266+0)
62 N/A N/A sporadic 7 R302X Het Hom Kosters et al.,unilat. WT (901CÃT) 1995
63 N/A N/A sporadic unilat. 7 S336Y Nil Het Varanasi et al.,WT (1013CÃA) 1994
64 11 Female sporadic unilat. 8 R362X Het Hom Coppes et al.,mon. WT (1084CÃT) 1993
65 N/A N/A sporadic unilat. 8 R362X Nil Hom Varanasi et al.,WT (1084CÃT) 1994
66 N/A N/A sporadic unilat. 8 R362X Nil Hom Kosters et al.,WT (1084CÃT) 1995
67 N/A N/A sporadic unilat. 8 1085 del9ÃCA Nil Het Varanasi et al.,WT FR-STOP 1994
(362+15)68 3 years N/A sporadic unilat. 8 R366C Nil Het Little et al.,
WT (1096CÃT) 1992c69 13 Male WT, PRB 8 H373Y N/A Hemi Gessler et al.,
mon. (1117CÃT) 199470 N/A N/A sporadic unilat. 9 1152 ins13 & Nil Hom Varanasi et al.,
WT 1158delAA 199471 11 Femaleb bilat. WT 9 R390X Het Het/ Little et al.,
mon. (1168CÃT) Homc 1992c72 N/A N/A WT 9 R390X N/A N/A Quek et al.,
(1168CÃT) 199373 N/A N/A sporadic unilat. 9 R390X Nil Hom Varanasi et al.,
WT (1168CÃT) 199474 7 years Female sporadic unilat. 9 R394W Het Hom Akasaka et al.,
WT 1180CÃT 199375 N/A N/A sporadic unilat. 9/int9 1213 del25ÃT Nil Het Haber et al.,
WT ZF3 spliced out, (with 1990transcript remains LOH ofin frame 11p)
(continued)

A CLINICAL OVERVIEW OF WT1 GENE MUTATIONS 217
TABLE 3. Intragenic WT1 Mutations in Sporadic Wilms� Tumour Patients (n=26) (Continued)
Patient Genotype/ Clinicalnos. Age phenotype description Exon Mutations Constit Tumour Author
76 N/A N/A sporadic unilat. int9 del>1.85kb Nil Hom Algar et al.,WT removing ZF4, 1995
1.4kb transcript77 4 years Male sporadic unilat. 10 1297 insC Nil Hom Coppes et al.,
WT FR-STOP (432+86) 199378 2 years N/A Female sporadic unilat. 10 1297 delCG Nil Hom Coppes et al.,
WT FR-STOP (432+86) 1993
aIn both the tumour and the PRB.bKaryotyped after publication: 46XXcLOH in one tumour resulting in homozygosity, but other tumour showing no LOH.
tations. Such a calculation is further confounded bythe fact that few studies have examined all exons,most avoided the 5´ end of exon 1 and many em-ployed the single strand conformational polymor-phism (SSCP) technique which does not detect allmutations. Other extensive studies restricted them-selves to gross deletions or 11p allele loss. Thus, thebest available estimates would suggest that gross re-arrangements of WT1 are seen in approximately 10%
TABLE 4. Intragenic Mutations of the Remaining WT1 Allele of Patients With Large Constitutional 11p13 Deletions (n=11)
Patient Sex:genotype/ Clinicalnos. phenotype description Exon Mutations Constit Tumour Author
79 XY Female WT, aniridia 1 230 del34 del. Hemi Huff et al.,FR-STOP 11p12- 1995(77+1) 11p14.2
80 XY N/A WAGR 1 345 del19 del. Hemi Huff et al.,FR-STOP 11p11-p14 1995(116+94)
81 XY Male WT, PRB, no 2 455 del5 del. 11p13 Hemi Gessler et al.,aniridia, FR-STOP 1994cardiomegaly. (152+24)
82 XY N/A WAGR, del. splicing del. 11p13 Hemi Brown et al.,unilat. WT 2&3 exon1-4; 1992;
FR-STOP Brown et al.,(147+7) 1993
83 XY Male WAGR, 3 G201D del. 11p13 Hemi Park et al.,unilat. WT (602GÃA) 1993c
84 N/A bilat. WT, 4 W238X del.11p13 Hemi Nordenskjoldaniridia, (713GÃA) et al., 1995bmentalretardation.
85 XY Male WAGR, 7 904 delC del. 11p13 Hemi Gessler et al.,unilat. WT, no FR-STOP 1993PRB (301+4)
86 N/A WAGR, 7 936 ins10 del. 11p13 Hemi Baird et al.,unilat. WT FR-STOP 1992a
(312+6)87 N/A Female WAR int. 7 1045+3 ins14: del. 11p12- Hemi Santos et al.,
presumed 11p14.3 1993splicing exon6-8 & FR-STOP(298+33)
88 N/A WAGR, 8 R362X del. 11p13 Hemi Baird et al.,unilat. WT (1084CÃT) 1992a
89 XY Ambiguous WAGR, WT 9 R390X putative Hemi Gessler et al.,(1168CÃT) large del. 1994
of tumours (Reddy and Licht, 1995) and at least 5%of sporadic Wilms’ tumours contain WT1 intragenicmutations.
Most mutations in this group of patients involvetruncations, although missense mutations extendingfrom exon 2 to 9 are also seen (see Fig. 1). Several ofthe mutations present are identical to mutations inDDS patients. However, while the ZF region still con-tains 72% of the mutations, there is less bias towards

218 LITTLE AND WELLS
exon 9 and deletions of exon 10 are observed, whereasmutations within this exon have never been reportedin DDS. The absence of the associated features of DDSin these patients is explained by the lack of a constitu-tional WT1 mutation in most cases. Mutations are usu-ally restricted to the tumour, where they have beenreported as homozygous (patients, 56, 58, 65, 66, 70,73, 76, 77 and 78) or heterozygous, with (patients 54,69 and 75) or without (patients 53, 55, 63, 67 and 68)accompanying 11p13 deletion or LOH. However, someof these individuals do carry constitutional mutationssimilar or identical to those in DDS, despite only pre-senting with bilateral (patients 59, 60, and 71) or evenunilateral WT (patients 61, 62, 64 and 74). A consti-tutional mutation in a bilateral patient is understand-able, and constitutional WT1 mutations in sporadicunilateral patients may indicate that the diagnosis hasbeen premature and that a second tumour is likely. Onemay ask, however, why other features did not alsopresent in patients 59, 60 and 71. Thus Wilms’ tumourpatients carrying constitutional WT1 mutations,whether presenting with unilateral or bilateral WT,could also be considered as incomplete DDS. As a cor-ollary of this, should any patient carrying a constitu-tional WT1 mutation be monitored for gonadoblastomaand nephropathy after treatment for their tumor? Therehas been rare reports of sporadic WT patients with nogenital anomalies reaching end-stage renal failure overten years after presenting with the tumour (Schmitt etal., 1995). A recent report from the National Wilms’Tumor Study Group in the US (Ritchey et al., 1996)suggest a significant level of renal failure (RF) follow-ing bilateral WT. However, excluding those diagnosedas DDS, most RF resulted from a need for bilateral ne-phrectomy or was radiation induced nephritis. The juryis out for sporadic unilateral WT as the correlationbetween RF and WT1 mutation in these patients wasnot investigated. With regard to a risk of gona-doblastoma, this is rare even in complete DDS patients.Thus, if the sexual phenotype of a sporadic WT pa-tient matches their karyotype, the risk appears very low.
Second Mutations in WAGR Patients
Large chromosome 11p13 deletions encompass-ing the Pax6 gene and the WT1 gene are known tobe responsible for the WAGR syndrome. The loss ofone copy of the Pax6 gene is sufficient to cause ani-ridia in these patients (Hanson et al., 1993). How-ever, it has been assumed that inactivation of thesecond copy of WT1 is required for the developmentof a Wilms’ tumour. Certainly, some tumors inWAGR patients show loss of the wildtype allele (Callet al., 1990; Gessler et al., 1990). In those where suchan event has not been seen, small intragenic WT1
mutations have been searched for. Table 3 lists thoseWAGR and WT patients with large constitutional11p13 deletions in which intragenic mutations havebeen identified within the remaining WT1 allele ofthe tumour. It is difficult to estimate the frequencyof such ‘second hit’ mutations as most studies investi-gated a large series of WT patients including not onlyWAGR/11p13 deletion patients. All but one of themutations in this group involve premature truncation.The mutations are spread widely from exon 1 to 9 withno bias towards ZF region mutations (see Fig. 1). While70% of these mutations would qualify as dominant-negative mutants according to the prediction ofBardeesy et al. (1994), these mutations follow the lossof the first WT1 allele. They therefore occur late andpresumably in a single cell to result in a tumour.
Is Inactivation of WT1 Necessary or Sufficient forWT Initiation?
A bilateral WT patient has been described carry-ing a constitutional WT1 mutation where heterozy-gosity for the mutation was seen in one tumour andhomozygosity in the other. This provided evidencethat inactivation of both copies of WT1 may be suf-ficient, but not necessary for WT initiation (Little etal., 1992c). In all Wilms’ tumours apparently het-erozygous for WT1 mutations, accompanyingmutation(s) at other loci were presumed to have re-sulted in tumour initiation. However, WT1 mutationshave also been reported in those regions of non-ma-lignant persistent renal blastema (PRB; also referredto as nephroblastomatosis or nephrogenic rests) of-ten found surrounding or within the same kidney asa WT. In one case, the mutations were homozygous(patient 56). This suggests that two mutations inWT1 are NOT sufficient for the development of aWT. Inactivation of WT1 may instead result in thecondition of PRB and perhaps it is this condition it-self which should be considered analogous to the ad-enoma in the multi-stage process described for coloncancer. In the other case of PRB carrying a WT1 mu-tation (patient 55), the mutation was heterozygous.If heterozygosity for such a mutation is sufficient forPRB, one would expect that all DDS patients shouldshow PRB (Park et al., 1993a). In agreement withthis, 83% of DDS patients display the presence ofPRB in comparison to 28% and 14% of bilateral andunilateral WT respectively (Heppe et al., 1991).However, if heterozygosity for a WT1 mutation wasenough to initiate PRB, no normal renal tissue wouldbe expected. A DDS patient apparently lacking PRBhas been described in which the constitutional WT1mutation was actually homozygous (patient 6), sug-gesting that factors additional to WT1 mutation are

A CLINICAL OVERVIEW OF WT1 GENE MUTATIONS 219
required for both PRB and WT. This suggests an ex-tremely early role for WT1 in the neoplastic process.
The picture painted here would suggest that spo-radic WT rarely has anything to do with WT1. Asexemplified by alteration to methylation status of thecyclin dependent kinase inhibitor (p16) promoter inNSCLC, the activity of a gene can be disturbed otherthan by intragenic mutations (Merlo et al., 1995).WT1 is not imprinted (Little et al., 1992b), so relax-ation of imprinting is not a factor. An extensive analy-sis of the WT1 promoter has also failed to reveal anymutations in Wilms’ tumour (Grubb et al., 1995). Itis still possible that long distance effects altering tissuespecificity, transcript stability or isoform ratios are in-volved. However, the aetiology of Wilms’ tumour mustnow focus on the mutations leading to the next stagesof initiation and progression.
A Role for Other Loci in Wilms� Tumour
Even before the isolation of WT1, it was clear thatchromosome 11p allele loss in Wilms’ tumour wasoften restricted to 11p15. The 11p15 locus is referredto as WT2. Preferential loss of heterozygosity (LOH)of maternal 11p15 alleles suggests the involvementof an imprinted gene (Hoban et al., 1995; Schroederet al., 1987). Conveniently, the tightly linked andinversely imprinted genes insulin-like growth factor2 (IGF2) and H19 lie at 11p15 (Reik et al., 1995).Wilms’ tumour is seen in 10% of patients with thefetal overgrowth condition Beckwith Wiedemannsyndrome (BWS) (Haas et al. 1986). BWS patientscan show 11p15 trisomy (Haas et al., 1986; Pettenatiet al., 1986) or 11p15 paternal isodisomy (Henry etal., 1991) and familial BWS has been tightly linkedto the insulin-IGF2 gene cluster at 11p15.5 (Koufoset al., 1989). IGF2 imprinting is relaxed in someWilms’ tumours (Ogawa et al., 1993b; Rainier et al.,1993), further strengthening the association betweenBWS, Wilms’ tumour and IGF2, but stopping shortof proving that this gene is involved in Wilms’ tu-mour aetiology. However, WT1 has been shown toregulate the expression of IGF2 in vitro via promoterbinding (Drummond et al., 1994). This is intriguingin light of the recent cloning of the gene responsiblefor Simpson-Golabi-Behmel syndrome (SGBS).SGBS is another overgrowth condition, showing strik-ing overlap with BWS, in which patients show a pre-disposition to Wilms’ tumour (Pilia et al., 1996).Intragenic deletions within the mesoderm-specificproteoglycan, GPC-3, located on the X chromosome,have now been shown in SGBS. This proteoglycan isthought to mediate the binding of IGF2 to the IGF2receptor, thereby controlling the growth of the em-bryonic mesoderm (Pilia et al., 1996).
Chromosome 16q has also been identified as a siteof LOH in Wilms’ tumour (Maw et al., 1992), with16q LOH associated with tumour progression andpoor prognosis (Grundy et al., 1994). Recently, apatient with BWS was reported with a balancedt(11;16) (p15;q13) translocation, possibly linkingboth 16q and 11p in the aetiology of BWS and WT(Newsham et al., 1995). A candidate gene from thisregion is uvomorulin (Maw et al., 1992), a moleculeinvolved in cell adhesion/cell-cell interactions. WTis also seen in association with hyperparathyroidism-jaw tumour syndrome (HPT-JT), which has now beenlinked to 1q21-31 (Szabo et al., 1995). Chromosome1q trisomy, frequently as a result of translocationswith 1q21 breakpoints, is seen in 20% of WT(Slaterand Mannens, 1992). A target binding site for WT1has now been mapped to 1q21-22 (Negus et al.,1996). WT is also infrequently seen in Li-Fraumenisyndrome, in which patients show constitutional p53mutations (Hartley et al., 1993). There has also beenevidence that WT1 and p53 can undergo protein-protein interactions (Maheswaran et al., 1993),modulating the activity of p53 on its own targets(Maheswaran et al., 1995). While p53 is over-expressed in most WT (Lemoine et al., 1992), p53mutations have only been seen in anaplastic WT, forwhich the prognosis is poor (Bardeesy et al., 1995;Malkin et al., 1994).
Cytogenic Evidence for Other Wilms�Tumour Loci
Cytogenic analyses from many groups also impli-cate 1p (Maw et al., 1992; Slater and Mannens,1992), 7q, 7p (Wilmore et al., 1994), 11q (Radice etal., 1995) and trisomy 18 (Olson et al., 1995) inWilms’ tumour aetiology, possibly at different stagesof tumorigenesis (Slater and Mannens, 1992). A lo-cus for familial WT (representing only 1% of all WT)also remains unknown with lack of linkage being es-tablished to 11p13, 11p15 (Grundy et al., 1988; Huffet al., 1988) and 16q (Huff et al., 1992). In short,what was assumed to represent a simple genetic modelof cancer, as was the case for retinoblastoma, is a com-plicated as any adult tumour. Several questions needto be addressed: Is there a role for WT1 in GPS-3regulation? Is IGF2, or any of the other genes identi-fied as being regulated by WT1 in vitro, also regu-lated by WT1 in vivo? Does Wilms’ tumour resultfrom mutation at various points of a single pathway,or are disturbances to each of these loci independentlyleading to the same phenotype? Wilms’ tumour islikely to end up being the phenotypic convergenceof mutations in many different genes, possibly alongthe same pathway, but that still remains to be seen.

220 LITTLE AND WELLS
WT1 Mutations in Other Tumours
Table 5 lists WT1 mutations seen in other types ofcancer (see also Fig. 1). While mutations of WT1 insporadic Wilms’ tumour have proven to be uncom-mon events, some predictions of WT1 involvementbased on the known wildtype expression pattern andfunction of this protein have proven accurate. Thus,patients with Wilms’ tumour in association with geni-tal and/or renal anomalies have a high rate of WT1mutation and the observation of WT1 mutation inthe juvenile granulosa cell tumour of a DDS patientwas not surprising (Pelletier et al., 1991a). WT1knockout mice, while lacking kidneys and gonads,die during midgestation apparently due to diaphrag-matic and pericardial insufficiency (Kreidberg et al.,1993). A DDS patient has also been described withdiaphragmatic hernia (Devriendt et al., 1995). Suchdisturbances may result from aberrant mesothelial de-velopment as WT1 is expressed in the lining of theabdominal cavity (Pritchard-Jones et al., 1990). WT1mutations were therefore predicted in mesothelioma,a ‘hunch’ that bore fruit when a WT1 mutation wasreported in a non-asbestos related mesothelioma (Park
et al., 1993b). A speculation of more importance hasbeen that the expression of WT1 in spleen (Pritchard-Jones et al., 1990), together with an increased rate ofleukemia as a secondary malignancy in WAGR (Hartleyet al., 1994; Moss et al., 1989), may indicate an in-volvement of WT1 in this form of cancer. A WT1 mu-tation was subsequently reported in the secondary adultmyeloid leukemia (AML) of a WAGR patient (patient99). This intragenic mutation was restricted to theAML and was not seen in the WT of the same pa-tient. Following on from this, the same group have nowobserved WT1 mutations in 4 adult leukemia patients(patients 90, 92, 93 and 100). They estimate that 15%of AML will involve WT1 mutations and have alsodemonstrated that WT1 may be a useful marker of re-sidual disease. These may be the most important cor-relations made to date between WT1 mutation anddisease. Based on the experience with AML and Wilms’tumour, one slightly more obscure connection whichshould be pursued is the observation of WT1 overex-pression in melanoma cell lines, in contrast to its ab-sence in melanocytes (Rodeck et al., 1994).
In contrast, a study of a diverse group of geni-
TABLE 5. Intragenic WT1 Mutations in Other Tumours (n=12)
Patientnos. Clinical description Exon Mutations Constit Tumour Author
90 33 yr old male, acute 1/7 363 insA; FR-STOP N/A Hom/one King-Underwoodmyeoblastic leukaemia (121+8)/937 ins4; on each et al., 1996(FAB type M1) FR-STOP (312+4) allele
91 adult female 6 S273G Nil Hom Park et al., 1993bmulticystic peritoneal (817AÃG)mesothelioma
92 25 yr old female, acute 7 897 ins5 N/A Het King-Underwoodlymphoblastic FR-STOP (299+8) et al., 1996leukaemia (FAB L2)
93 22 yr old female, acute 7 902 ins4 N/A Het King-Underwoodmyeloblastic leukaemia FR-STOP (300+16) et al., 1996(FAB M2)
94-97 Desmoplastic small 8 In frame Nil t(11;22) Ladanyi andround cell tumour translocation (p13;q12) Gerald, 1994
between EWS Same in(22q12) exon 7 and all fourWT1 exon 8, casesresulting in achimeric transcript.
98 pre-B cell leukemia 8 S365F N/A N/A Call et al., 1990(clone WT33) (1094CÃT)
99 WAGRa, secondary 9 C385Y 11p12-14 Hemi Pritchard-Jonesleukemia (1154GÃA) del. et al., 1994(mutation seen inleukemic bone marrow)
100 18 yr old male acute 9 R390X N/A Het King-Underwoodpromyelocytic (1168CÃT) et al., 1996leukemia (AML (M3))
19 DDS nephropathy, WT, 9 R394W Het Hemi Pelletier et al.,juvenile granulosa cell (1180CÃT) 1991atumourb
aTumour mutation reported refers to leukemia only.bAlso reported in Table 1.

A CLINICAL OVERVIEW OF WT1 GENE MUTATIONS 221
tourinary cancers only found WT1 mutations inWilms’ tumours (Quek et al., 1993; see Table 6).Extensive analysis of adult ovarian, endometrialand fallopian tube cancer revealed no WT1 mu-tations (Bruening et al., 1993; see Table 6), de-
spite overexpression of WT1 in these cancers. Intesticular cancer, one group found no WT1 muta-tions (Looijenga et al., 1994; see Table 6), whileanother group reported a high level of 11p LOHand a WT1 gene polymorphism in Norwegian pa-
TABLE 6. Patient Numbers, Exons Scanned, and Screening Methods for All Studies Reviewed,Including Those Where No Mutations Were Detected
WT-1 Mutations/Author Patients Screeneda Exons Scanned Method Used*
Akasaka et al., 1993 1/18 9 SSCPAlgar et al., 1995 1/21 1(252C)b-10 Southern blotBaird et al., 1992a 2/3 1-10 SSCPBaird et al., 1992b 6/8 1-10 SSCPBaird and Cowell, 1993 1/1 8, 9 DSBardeesy et al., 1994 3/3 1-10 SSCPBrown et al., 1992; 1993 1/20 1-10 SSCPBruening et al., 1992 4/4 1-10 SSCPBruening et al., 1993 0/40c 1-10 SSCPClarkson et al., 1993 3/3 1(213C)-10 SSCPCoppes et al., 1992 3/3 1-10 SSCPCoppes et al., 1993 3/50 7-10 SSCPDevriendt et al., 1995 1/1 8, 9 DSGessler et al., 1993 1/1 7 SSCPGessler et al., 1994 6/77 1(252C)-10 SSCPGrubb et al., 1995 0/39 1.2 kb of promoter SSCPHaber et al., 1990 1/8 1(373C); 7-10 RT-PCR/DSHuff et al., 1991 1/53d 1(252C)-10 Southern blotHuff et al., 1995 4/80 1 SSCPKikuchi et al., 1995 1/1 7-10 SSCPKing-Underwood et al., 1996 4/36 1(199C)-10 SSCPKonig et al., 1993 1/1 1-10 SSCPKosters et al., 1995 2/38 7-10 SSCPLadanyi and Gerald, 1994 4/5e 7-9 RT-PCR/DSLittle et al., 1992c 2/32 7-10 CMCLittle et al., 1993 5/5 7-10 CMCLooijenga et al., 1994 0/33f 2, 6 DSNordenskjold et al., 1994 4/5 2-10 DSNordenskjold et al., 1995a 1/27 2-10 DGGENordenskjold et al., 1995b 3/27 2-10 DGGEOgawa et al., 1993a 1/1 9 DSPark et al., 1993a 2/17 2-10 SSCPPark et al., 1993b 1/1g 2-10 SSCPPark et al., 1993c 1/1 1-10 SSCPPelletier et al., 1991a 10/10 1-10 SSCPPelletier et al., 1991b 2/2 1-10 SSCPPoulat et al., 1993 1/1 8, 9 SSCPPritchard-Jones et al., 1994 1/1 7-10 SSCPQuek et al., 1993 1/8h 9 SSCPSakai et al., 1993 3/3 N/A SSCPSantos et al., 1993 1/1 7-10 SSCPSchneider et al., 1993 1/1 2, 4, 6-10 SSCPTadokoro et al., 1992 1/42 4-10 Southern BlotTsuda et al., 1993 2/2 8, 9 DSVaranasi et al., 1994 6/98 5´UTR-10 SSCPWebb et al., 1995 1/1 9 CMC
aNumber of patients found to have WT-1 mutations/Total number of patients screened.bExon 1 screening from nucleotide indicated.cCancers of the female reproductive tract.dRefers to tumour number, not patient number.eDesmoplastic small round cell tumours.fTesticular seminomas and nonseminomatous germ cell tumours.gMesothelioma.hOne Wilms� tumour and 7 other urogenital cancers examined.*CMC, chemical mismatch cleavage; DGGE, denaturation gradient gel electrophoresis; DS, direct sequencing; RT-PCR, reverse tran-scription polymerase chain reaction; SSCP, single strand conformational polymorphism. When an entire exon was not examined, themost 5´ nucleotide in the screening is indicated. *Includes patients in Table 3.

222 LITTLE AND WELLS
tients (Heimdal et al., 1994), but did not searchfor WT1 coding sequence mutations.
Finally, the aggressive condition desmoplasticsmall round cell tumour (DSRCT) involves bal-anced translocations between 22q12 and 11p13.These have been shown to result in fusion pro-teins between the EWS gene, a putative RNAbinding nuclear protein of unknown function, andWT1 (Ladanyi and Gerald, 1994). The resultingchimeric protein incorporates the first 7 exons ofEWS and ZFs 2 to 4 of WT1.
Is WT1 a Tumour Suppressor?
It may be asked why overexpression of a tumoursuppressor would indicate an involvement in a par-ticular type of cancer. WT1 is also overexpressed inWilms’ tumour itself. While this was originallythought to represent the overexpression of a mutantform, this has not proven to be the case. WT1 is alsooverexpressed in myeloid and lymphoid leukemias(Miwa et al., 1992; Miyagi et al., 1993). However,WT1 appears to downregulate during differentiationof the leukemic cell line K562 (Phelan et al., 1994)and antisense experiments have also shown thatthe inactivation of WT1 in K562 leads to reducedproliferation and apoptosis (Algar et al., 1996).Thus, the term ‘tumour-suppressor’ appears inap-propriate. Disturbances to the ratios of the fourWT1 isoforms has been observed in Wilms’ tumours(Simms et al., 1995) and may be oncogenic on itsown. WT1 protein has been shown to bind its ownpromoter, presumably to facilitate autoregulation(Rupprecht et al., 1994). It is possible that the com-plicated balance of WT1 isoforms needed to carryout all the as yet unfathomed functions of WT1 canalso be disturbed by an excess of expression.
A Clinical Perspective
In summary, the WT1 gene is critical for the nor-mal development of the urogenital tract. Mutationsin both copies of this gene may be sufficient for pre-disposition to Wilms’ tumour but probably representa very early step in the tumorigenetic pathway. Theless than 5% of Wilms’ tumour patients with genitalanomalies have a high rate of WT1 mutation. In spo-radic WT, at least 5% carry intragenic WT1 muta-tions with a further 10% demonstrating gross WT1rearrangements. 11p LOH is lower in bilateral Wilms’tumour (Little et al., 1992a), whereas bilateral tu-mours appear to show intragenic WT1 mutationsmore often. As earlier discussed, familial WT repre-sents only 1% of all WT, is rarely associated with otheranomalies and has never been linked to 11p13 (Huffet al., 1988), suggesting that WT1 screening is not
useful here. However, there have been two reportswhere a father has passed an intragenic WT1 muta-tion on to an affected child. One patient suffered fromDDS, yet the parent was unaffected (Coppes et al.,1992). The other patients displayed Wilms’ tumourand genital anomalies, while the father also sufferedfrom Wilms’ tumour (Pelletier et al., 1991b), rein-forcing the variable penetrance of such mutations.
The Future of WT1 and Wilms� Tumour
It is now time for WT1 and Wilms’ tumour re-search to diverge. We have reviewed the extensiveevidence that many other loci are involved in Wilms’tumour, and identifying such genes must now gainprominence in Wilms’ tumour research. Conversely,WT1 is now known to be a key inducer of urogenitaldevelopment, directing the induction of the uretericbud, the mesenchyme to epithelial transition withinboth metanephros and genital ridge and the forma-tion and maintenance of the glomeruli. The repeatedassociation of XY genital/gonadal anomalies and WT1mutation would suggest there is still much to be learntregarding the role of WT1 in sex determination, andpossibly other clinical conditions in which WT1 ismutated. In addition, WT1 mutations are involvedin the development of a number of other tumourtypes, including DSRCT, mesothelioma and AML.Thus WT1 research must move away from Wilms’stumour to focus on how WT1 regulates developmentand why disturbances in such a gene can go on tocause cancer in adulthood.
ACKNOWLEDGMENTS
We would like to thank Dr. Geoffrey Machin,Permaente Medical Group Incorporated, Oakland,CA, Drs. Jonathan Licht and Dr. Josina Reddy, TheBrookdale Centre, New York, NY and Dr. KathyWilliamson, MRC Human Genetics Unit, Edinburghfor their clinical and scientific advice and assistancein compiling this data.
REFERENCES
Akasaka Y, Kikuchi H, Nagai T, Hiraoka N, Kato S, Hata J (1993) Apoint mutation found in the WT1 gene in a sporadic Wilms tu-mour without genitourinary abnormalities is identical with themost frequent point mutation in Denys-Drash syndrome. FEBS317:39–43.
Algar EM, Kenney MT, Simms LA, Smith SI, Kida Y, Smith PJ (1995)Homozygous intragenic deletion in the WT1 gene in a sporadicWilms’ Tumour associated with high levels of expression of a trun-cated transcript. Hum Mutat 5:221–227.
Algar EM, Khromykh T, Smith SI, Blackburn DM, Bryson GJ, SmithPJ (1996) A WT1 antisense oligonucleotide inhibits prolifera-tion and induces apoptosis in lyeloid leukemia cell lines. Onco-gene (in press).
Armstrong JF, Pritchard-Jones K, Bickmore WA, Hastie ND, Bard JB

A CLINICAL OVERVIEW OF WT1 GENE MUTATIONS 223
(1992) The expression of the Wilms’ tumour gene, WT1, in thedeveloping mammalian embryo. Mech Dev 40:85–97.
Baird P, Groves N, Haber D, Houseman D, Cowell J (1992a) Identifi-cation of mutations in the WT1 gene in tumours from patientswith the WAGR syndrome. Oncogene 7:2141–2149.
Baird P, Santos A, Groves N, Jadresic L, Cowell J (1992b) Constitu-tional mutations in the WT1 gene in patients with Denys-Drashsyndrome. Hum Mol Genet 1:301–305.
Baird P, Cowell J (1993) A novel zinc finger mutation in a patientwith Denys-Drash syndrome. Hum Mol Genet 2:2193–2194.
Bardeesy N, Zabel B, Schmitt K, Pelletier J (1994) WT1 mutationsassociated with incomplete Denys-Drash syndrome define a do-main predicted to behave in a dominant-negative fashion. Ge-nomics 21:663–664.
Bardeesy N, Beckwith JB, Pelletier J (1995) Clonal expansion andattenuated apoptosis in Wilms’ tumors are associated with p53gene mutations. Cancer Res 55:215–219.
Beaudet AL, Tsui L-C (1993) A suggested nomenclature for desig-nating mutations. Hum Mutat 2:245–248.
Bickmore WA, Oghene K, Little MH, Seawright A, van HeyningenV, Hastie ND (1992) Modulation of DNA binding specificity byalternative splicing of the Wilms’ tumor wt1 gene transcript. Sci-ence 257:235–237.
Brown K, Watson J, Poirer V, Mott M, Berry P, Maitland N (1992)Inactivation of the remaining allele of the WT1 gene in a Wilms’tumour from a WAGR patient. Oncogene 7:763–768.
Brown K, Wilmore H, Mott M, Berry P, Maitland N (1993) Low fre-quency of mutations in the WT1 coding region in Wilms’ tumor.Genes Chromosomes Cancer 8:74–79.
Bruening W, Bardeesy N, Silverman B, Cohn R, Machin G, AronsonA, Houseman D et al (1992) Germline intronic and exonic mu-tations in the Wilms’ tumour gene (WT1) affecting urogenitaldevelopment. Nature Genet 1:144–148.
Bruening W, Gros P, Sato T, Stanimir J, Nakamura Y, Housman D,Pelletier J (1993) Analysis of the 11p13 Wilms’ tumor suppressorgene (WT1) in ovarian tumors. Cancer Invest. 11:393–399.
Call K, Glaser T, Ito C, Buckler A, Pelletier J, Haber D, Rose E et al(1990) Isolation and characterization of a zinc finger polypeptidegene at the human chromosome 11 Wilms’ tumor locus. Cell60:509–520.
Caricasole A, Duarte A, Larsson S, Hastie N, Little M, Holmes G,Todorov I et al (1996) RNA binding by the Wilms’ tumor sup-pressor (WT1) zinc finger proteins. Proc Natl Acad Sci USA (inpress).
Carroll T, Vize P (1996) The Wilms’ tumor suppressor gene is in-volved in the development of disparate kidney forms: evidencefrom expression in the Xenopus pronephros. Developmental Dy-namics (in press).
Clarkson P, Davies H, Williams D, Chaudhary R, Hughes I, PattersonM (1993) Mutational screening of the Wilms’ tumour gene, WT1,in males with genital abnormalities. J Genet Med 30:767–772.
Coppes M, Liefers G, Higuchi M, Zinn A, Balfe J, Williams B (1992)Inherited WT1 mutation in Denys-Drash syndrome. Cancer Res52:6125–6128.
Coppes M, Lierers G, Paul P, Yeger H, Williams B (1993) Homozy-gous somatic WT1 point mutations in sporadic unilateral Wilms’tumor. Proc Natl Acad Sci USA 90:1416–1419.
Denys P, Malvaux P, van den Berghe H, Tanghe W, Proesmans W(1967) De pseudohermaphrodisme masculin, d’une tumeur deWilms, d’une nephropathie parenchymateuse et d’un mosaicismeXX/XY. Archives Francaises de Pediatrie 24:729–739.
Devriendt K, Deloof E, Moerman P, Legius E, Vanhole C, de ZegherF, Proesmans W et al (1995) Diaphragmatic Hernia in Denys-Drash Syndrome. Am J Med Genet 57:97–101.
Drash A, Sherman F, Harmann W, Blizzard R (1970) A syndrome of
pseudohermaphroditism, Wilms’ tumor, hypertension and degen-erative renal disease. J Pediatr 76:585–593.
Drummond IA, Rupprecht HD, Rohwer-Nutter P, Lopez-Guisa JM,Madden SL, Rauscher F Jr, Sikhatme VP (1994) DNA recogni-tion by splicing variants of the Wilms’ tumor suppressor, WT1.Mol Cell Biol 14:3800–3809.
Eddy A, Mauer S (1985) Pseudohermaphroditism, glomerulopathyand Wilms’ tumor (Drash syndrome): Frequency in end-stagerenal failure. J Pediatr 106:584–587.
Englert C, Vidal M, Maheswaran S, Ge YM, Ezzell RM, IsselbacherKJ, Haber DA (1995) Truncated WT1 mutants alter the sub-nuclear localisation of the wild-type protein. Proc Natl Acad SciUSA 92(26):11960–11964.
Francke U, Holmes LV, Atkins L, Ricciardi VM (1979) Aniridia-Wilms’tumor association: evidence for specific deletion of 11p13.Cytogenet Cell Genet 24:185–192.
Gessler M, Poustka A, Cavenee W, Neve RL, Orkin SH, Bruns GAP(1990) Homozygous deletion in Wilms’ tumours of a gene identi-fied by chromosome jumping. Nature 343:774–778.
Gessler M, Konig A, Moore J, Qualman S, Arden K, Cavenee W,Bruns G (1993) Homozygous inactivation of WT1 in a Wilms’tumor associated with the WAGR syndrome. Genes ChromosomesCancer 7:131–136.
Gessler M, Konig A, Arden K, Grundy P, Orkin S, Sallan S, Peter Cet al (1994) Infrequent mutation of the WT1 gene in 77 Wilms’tumors. Hum Mutat 3:212–222.
Grubb GR, Yun K, Reeve AE, Eccles MR 1995) Exclusion of theWilms’ tumour gene (WT1) promoter as a site of frequent muta-tion in Wilms’ tumour. Oncogene 10:1677–1681.
Grundy P, Koufos A, Morgan K, Li F, Meadows A, Cavenee W (1988)Familial predisposition to Wilms’ tumour does not map to theshort arm of chromosome 11. Nature 336:374–376.
Grundy P, Wilson B, Telzerow P, Zhou W, Paterson MC (1994) Uni-parental disomy occurs infrequently in Wilms tumor patients. AmJ Hum Genet 54:282–289.
Haas O, Zoubek A, Grumayer E, Gadner H (1986) Constitutionalinterstitial deletion of 11p11 and pericentric inversion of chro-mosome 9 in a patient with Widemann-Beckwith syndrome andhepatoblastoma. Cancer Genet Cytogenet 23:95–104.
Haber D, Buckler A, Glaser T, Call K, Pelletier J, Sohn R, DouglassE et al (1990) An internal deletion with an 11p13 zinc fingergene contributes to the development of Wilms’ tumor. Cell61:1257–1269.
Haber DA, Sohn RL, Buckler A, Pelletier J, Call KM, Housman DE(1991) Alternative splicing and genomic structure of the Wilms’tumor gene WT1. Proc Natl Acad Sci USA 88:9618–9622.
Hanson I, Seawright A, Hardman K, Hodgson S, Zaletayer D, FeketeG, Van Heyningen V (1993) Pax6 mutations in aniridia. HumMol Genet 2:915–920.
Hartley A, Birch J, Tricker K, Wallace S, Kelsey A, Harris M (1993)Wilms’ tumour in the Li-Fraumeni Cancer Family Syndrome.Cancer Genet Cytogenet 67:133–135.
Hartley AL, Birch JM, Harris M, Blair V, Morris Jones PH,Gattameneni HR, Kelsey AM (1994) Leukemia, lymphoma, andrelated disorders in families of children diagnosed with Wilms’tumor. Cancer Genet Cytogenet 77:129–133.
Hastie ND (1994) The genetics of Wilms’ tumor—A case of dis-rupted development. Ann Rev Genet 28:523–558.
Heimdal K, Lothe R, Fossa S, Borresen A (1994) Association studiesof a polymorphism in the Wilms’ tumor 1 locus in Norwegianpatients with testicular cancer. Int J Cancer 58:523–526.
Henry I, Bonaiti-Pellie C, Chehenesse V, Beljord V, Schwartz C, Uter-mann G, Junien C (1991) Uniparental disomy in a genetic can-cer-predisposing syndrome. Nature 351:665–667.

224 LITTLE AND WELLS
Heppe R, Koyle M, Beckwith J (1991) Nephrogenic rests in Wilms’tumor patients with Drash syndrome. J Urol 145:1225–1228.
Hoban P, Heighway J, White G, Baker B, Gardner J, Birch J, Morris-Jones P et al (1995) Genome-wide loss of maternal alleles in anephrogenic rest and Wilms’ tumour from a BWS patient. HumGenet 95:651–656.
Huff V, Compton DA, Chao L, Strong L, Geiser C, Saunders G (1988)Lack of linkage of familial Wilms’ tumour to chromosomal band11p13. Nature 336:377–378.
Huff V, Miwa H, Haber D, Call KN, Housman D, Strong LC,Saunders GF (1991) Evidence for WT1 as a Wilms’ tumor (WT)gene: intragenic germinal deletion in bilateral WT. Am J HumGenet 48:997–1003.
Huff V, Reeve AE, Leppert M, Strong LC, Douglass EC, Geiser CF, LiFP et al (1992) Nonlinkage of 16q markers to familial predisposi-tion to Wilms’ tumor. Cancer Res 52:6117–6120.
Huff V, Jaffe N, Saunders G, Strong L, Villalba F, Ruteshouser E (1995)WT1 exon 1 deletion/insertion mutations in Wilms’ Tumor pa-tients associated with di- and trinucleotide repeats and deletionhotspot consensus sequences. Am J Hum Genet 56:84–90.
Kent J, Coriat A-M, Hastie ND, van Heyningen V (1995) The evolu-tion of WT1 sequence and expression pattern in vertebrates.Oncogene (in press).
Kikuchi H, Akasaka Y, Kurosawa Y, Yoneyama H, Kato S, Hata J(1995) A critical mutation in both WT1 alleles is not sufficientto cause Wilms’ tumor. FEBS Letters 360:26–28.
King-Underwood L, Renshaw J, Pritchard-Jones K (1996) Mutationsin the Wilms’ tumours gene WT1 in leukaemias. Blood (in press).
Knudson AG Jr., Strong LC (1972) Mutation and cancer: A modelfor Wilms’ tumor of the kidney. JNCI 48:313–324.
Konig A, Jakubiczka S, Wieacker P, Schlosser H, Gessler M (1993)Further evidence that imbalance of WT1 isoforms may be involvedin Denys-Drash syndrome. Hum Molec Genet 2:1967–1968.
Kosters R, Adams V, Hassam S, Schafer R, Schmid M, Moos R, BrinerJ (1995) Mutational analysis of the tumor suppressor gene WT1—detection of a novel homozygous point mutation in sproadic uni-lateral Wilms’ tumor. Int J Oncol 7:1103–1107.
Koufos A, Grundy P, Morgan K, Aleck KA, Hadro T, Lampkin BC,Kalbakji A et al (1989) Familial Wiedemann-Beckwith syndromeand a second Wilms’ tumor locus both map to 11p15.5. Am JHum Genet 44:711–719.
Kreidberg JA, Sariola H, Loring JM, Maeda M, Pelletier J, HousmanD, Jaenisch R (1993) WT-1 is required for early kidney develop-ment. Cell 74:679–691.
Ladanyi M, Gerald W (1994) Fusion of the EWS and WT1 genes inthe desmoplastic small round cell tumor. Cancer Res 12:350–359.
Larsson SH, Charlieu J-P, Miyagawa K, Engelkamp D, RassoulzadeganM, Ross A, Cuzin F et al (1995) Subnuclear localization of WT1in splicing or transcription factor domains is regulated by alterna-tive splicing. Cell 81:391–401.
Lemoine NR, Hughes CM, Cowell JK (1992) Aberrant expression ofthe tumour suppressor gene p53 is very frequent in Wilms’ tu-mours. J Path 168:237–242.
Little MH, Clarke J, Byrne J, Dunn R, Smith PJ (1992a) Allelic losson chromosome 11p is a less frequent event in bilateral than inunilateral Wilms’ tumours. Eur J Cancer 28A:1876–1880.
Little MH, Dunn R, Byrne JA, Seawright A, Smith PJ, Pritchard-Jones K, van Heyningen V et al (1992b) Equivalent expression ofpaternally and maternally inherited WT1 alleles in normal fetaltissue and Wilms’ tumors. Oncogene 7:635–641.
Little M, Prosser J, Condie A, Smith P, Van Heningen V, Hastie N(1992c) Zinc finger mutations within the WT1 gene in Wilms’tumor patients. Proc Natl Acad Sci USA 89:4791–4795.
Little M, Williamson K, Mannens M, Kelsey A, Gosden C, Hastie N,van Heyningen V (1993) Evidence that WT1 mutations in De-
nys-Drash syndrome patients may act in a dominant-negative fash-ion. Hum Molec Genet 2:259–264.
Little M, Holmes G, Bickmore W, van Heyningen V, Hastie N, Wain-wright B (1995) DNA binding capacity of the WT1 protein isabolished by Denys-Drash syndrome WT1 point mutations. HumMolec Genet 4:351–358.
Little M, Holmes G, Pell L, Duarte A, Caricasole A, Ward A, Wain-wright B (1996) A novel target for the Wilms’ tumour suppressorprotein (WT1) is bound by a unique combination of zinc fingers.Oncogene 13:1461–1469.
Looijenga L, Abraham M, Ghillis A, Saunders G, Oosterhuis J (1994)Testicular germ cell tumors of adults show deletions of chromo-somal bands 11p13 and 11p15.5, but no abnormalities within thezinc finger regions and exons 2 and 6 of the Wilms’ tumor 1 gene.Genes Chromosomes Cancer 9:153–160.
Maheswaran S, Park S, Bernard A, Morris J, Rauscher F, Hill D, HaberD (1993) Physical and functional interaction between WT1 andp53 proteins. Proc Natl Acad Sci USA 90:5100–5104.
Maheswaran S, Englert C, Bennett P, Heinrich G, Haber DA (1995)The WT1 gene product stabilizes p53 and inhibits p53-mediatedapoptosis. Genes & Development 9:2143–2156.
Malkin D, Sexsmith E, Yeger H, Williams B, Coppes M (1994) Muta-tions of the p53 tumor suppressor gene occur infrequently inWilms’ tumor. Cancer Res 54:2077–2079.
Matsunaga E (1981) Genetics of Wilms’ tumor. Hum Genet57:231–246.
Maw MA, Grundy PE, Millow LJ, Eccles MR, Dunn RS, Smith PJ,Feinberg AP et al (1992) A third Wilms’ tumor locus on chromo-some 16q. Cancer Res 52:3094–3098.
Merlo A, Herman J, Mao L, Lee D, Gabrielson E, Burger P, Baylin Set al (1995) 5´ CpG island methylation is associated with tran-scriptional silencing of the tumour suppressor p16/CDKN2/MTS1in human cancers. Nature Med 1:686–692.
Miwa H, Beran M, Saunders GF (1992) Expression of the Wilms’tumor gene (WT1) in human leukemias. Leukemia 6:405–409.
Miyagi T, Ahuja H, Kubota T, Kubonishi I, Koeffler HP, Miyoshi I(1993) Expression of the candidate Wilms’ tumor gene, WT1, inhuman leukemia cells. Leukemia 7:970–977.
Moss T, Strauss L, Das L, Feig S (1989) Secondary leukemia follow-ing successful treatment of Wilms’ tumor. Am J Pediat HematolOncol 11:158–161.
Negus K, Holmes G, Wicking C, Wainwright B, Little M (1996) +P5,a novel target binding site for the Wilms’ tumour suppressor 1(WT1) gene, maps to human chromosome 1 band q21-22.Cytogenet Cell Genet 72:306–309.
Newsham I, Kindler-Rohrborn A, Daub D, Cavenee W (1995) AConstitutional BWS-Related t(11;16) Chromosome Transloca-tion Occurring in the Same Region of Chromosome 16 Impli-cated in Wilms’ Tumors. Genes Chromosomes Cancer 12:1–7.
Nordenskjold A, Friedman E, Anvret M (1994) WT1 mutations inpatients with Denys-Drash syndrome—A novel mutation in exon8 and paternal allele origin. Hum Genet 93:115–120.
Nordenskjold A, Fricke G, Anvret M (1995a) Absence of muta-tions in the WT1 gene with XY gonadal dysgenesis. Hum Genet96:102–104.
Nordenskjold A, Friedman E, Sandstedt B, Soderhall S, Anvret M(1995b) Constitutional and somatic mutations in Wilms’ tumorpatients. Int J Cancer 63:516–522.
Ogawa O, Eccles M, Yun K, Mueller R, Holdaway M, Reeve A (1993a)A novel insertional mutation at the third zinc finger coding re-gion of the WT1 gene in Denys-Drash syndrome. Hum MolecGenet 2:203–204.
Ogawa O, Eccles MR, Szeto J, McNoe LA, Yun K, Maw MA, SmithPJ et al (1993b) Relaxation of insulin-like growth factor II geneimprinting implicated in Wilms’ tumour. Nature 362:749–751.

A CLINICAL OVERVIEW OF WT1 GENE MUTATIONS 225
Olson J, Hamilton A, Breslow N (1995) Non-11p constitutional chro-mosome abnormalities in Wilms’ tumor patients. Med PediatrOncol 24:305–309.
Park S, Bernard A, Bove K, Sens D, Hazen-Martin D, Garvin A,Haber D (1993a) Inactivation of WT1 in nephrogenic rests, ge-netic precursors to Wilms’ tumour. Nature Genet 5:363–367.
Park S, Schalling M, Bernard A, Maheswaran S, Shipley G, RobertsD, Fletcher J et al (1993b) The Wilms’ tumour gene WT1 is ex-pressed in murine mesoderm-derived tissues and mutated in ahuman mesothelioma. Nature Genet 4:415–420.
Park S, Tomlinson G, Nisen P, Haber D (1993c) Altered trans-acti-vational properties of a mutated WT1 gene product in a WAGR-associated Wilms’ tumor. Cancer Res 53:4757–4760.
Pelletier J, Bruening W, Kashtan C, Mauer S, Manivel J, Stiegel J,Houghton D et al (1991a) Germline mutations in the Wilms’tumor suppressor gene are associated with abnormal urogenitaldevelopment in Denys-Drash Syndrome. Cell 67:437–447.
Pelletier J, Bruening W, Li F, Haber D, Glaser T, Housman D (1991b)WT1 mutations contribute to abnormal genital system develop-ment and hereditary Wilms’ tumour. Nature 353:431–434.
Pettenati M, Haines J, Higgins R, Wappener R, Palmer C, Weaver D(1986) Wiedemann-Beckwith syndrome: presentation of clinicaland cytogenetic data on 22 new cases and review of the litera-ture. Hum Genet 74:143–154.
Phelan SA, Lindberg C, Call KM (1994) Wilms’ tumor gene, WT1,mRNA is down-regulated during induction of erythroid andmegakaryocytic differentiation of K562 cells. Cell Growth &Diff 5:677–686.
Pilia G, Hughes-Benzie R, MacKenzie A, Baybayan P, Chen E, HuberR, Neri G et al (1996) Mutations in GPC3, a glypican gene, causeSimpson-Golabi-Behmel syndrome. Nature Genet 12:241–247.
Poulat F, Morin D, Konig A, Brun P, Giltay J, Sultan C, Dumas R et al(1993) Distinct molecular origins for Denys-Drash and Frasiersyndromes. Hum Genet 91:285–286.
Pritchard- Jones K, Fleming S, Davidson D, Bickmore W, PorteusD, Gosden C, Bard J et al (1990) The candidate Wilms’ tu-mor gene is involved in genitourinary development. Nature346:194–197.
Pritchard-Jones K, Renshaw J, King-Underwood L (1994) The Wilmstumor (WT1) gene is mutated in a secondary leukaemia in aWAGR patient. Hum Molec Genet 3:1633–1637.
Quek H, Show V, Tock E (1993) The 3rd zinc finger of the WT1gene is mutated in Wilms tumour but not in a broad range ofother urogenital tumours. Anticancer Res 13:1575–1580.
Radice P, Perotti D, De Benedetti V, Mondini P, Radice M, Pilotti S,Luksch R et al (1995) Allelotyping in Wilms’ tumors identifies aputative third tumor suppressor gene on chromosome 11. Ge-nomics 27:497–501.
Rainier S, Johnson LA, Dobry CJ, Ping AJ, Grundy PE, Feinberg AP(1993) Relaxation of imprinted genes in human cancer. Nature362:747–749.
Rauscher F (1993) The WT1 Wilms’ tumour gene product: a devel-opmentally regulated transcription factor in the kidney that func-tions as a tumour suppressor. FASEB J 7:896–903.
Reddy JC, Licht JD (1995) The WT1 Wilms’ tumor suppressor gene:How much do we really know? BBB Rev Cancer.
Reddy JC, Morris JC, Wang J, English MA, Haber DA, Shi Y, LichtJD (1995) WT1-mediated transcriptional activation is inhib-ited by dominant negative mutant proteins. J Biol Chem270:10878–10884.
Reik W, Brown K, Schneid H, Lebouc Y, Bickmore W, Maher E (1995)Imprinting in the Beckwith-Wiedemann syndrome suggested byan altered imprinting pattern in the IGF2-H19 domain. HumMolec Genet 4:2379–2385.
Ritchey M, Green D, Thomas P, Smith G, Haase G, Shochat S,Moksness J et al (1996) Renal failure in Wilms’ tumor—A reportfrom the National Wilms’ Tumor Study Group. Med Pediatr Oncol26:75–80.
Rodeck U, Bossler A, Kari C, Humphreys CW, Gyorfi T, Maurer J,Thiel E et al (1994) Expression of the wt1 Wilms’ tumor geneby normal and malignant human melanocytes. Int J Cancer59:78–82.
Rupprecht H, Drummond I, Madden S, Rauscher F, Sukhatme V(1994) The Wilms’ tumour suppressor gene WT1 is negativelyautoregulated. J Biol Chem 269:6198–6206.
Sakai A, Tadokoro K, Yanagisawa H, Nagafuchi S, Hoshikawa N,Suzuki T, Kohsaka T et al (1993) A novel mutation of the WT1gene (A tumor suppressor gene for Wilms tumor) in a patientwith Denys-Drash syndrome. Hum Molec Genet 2:1969–1970.
Santos A, Osorio Almeida L, Baird P, Silva J, Boavida M, Cowell J(1993) Insertional inactivation of the WT1 gene in tumour cellsfrom a patient with WAGR syndrome. Hum Genet 92:83–86.
Schmitt K, Zabel B, Tulzer G, Eitelberger F, Pelletier J (1995) Neph-ropathy with Wilms’ tumour or gonadal dysgenesis: incompleteDenys-Drash syndrome or separate diseases? Eur J Pediatr154:577–581.
Schneider S, Wildhardt G, Ludwig R, Royer Pokora B (1993) Exonskipping due to a mutation in a donor splice site in the WT-1gene is associated with Wilms’ tumor and severe genital malfor-mations. Hum Genet 91:599–604.
Schroeder W, Chao L-Y, Dao D, Strong L, Pathak S, Riccardi V, LewisW et al (1987) Nonrandom loss of maternal chromosome 11 al-leles in Wilms’ tumors. Am J Hum Genet 40:413–420.
Simms L, Algar E, Smith P (1995) Splicing of exon 5 in the WT1gene is disrupted in Wilms’ tumour. Eur J Cancer.
Slater RM, Mannens MM (1992) Cytogenetics and molecular genet-ics of Wilms’ tumor of childhood. [Review]. Cancer GenetCytogenet 61:111–121.
Szabo J, Heath B, Hill V, Jackson C, Zarbo R, Mallette L, Chew S etal (1995) Hereditary hyperparathyroidism-jaw tumor syndrome:the endocrine tumor gene HPRT2 maps to chromosome 1q21-31. Am J Hum Genet 56:944–950.
Tadokoro K, Fujii H, Ohshima A, Kakizawa Y, Shimizu K, Sakai A,Sumiyoshi K et al (1992) Intragenic homozygous deletion of theWT1 gene in Wilms’ tumor. Oncogene 7:1215–1221.
Tsuda M, Sakiyama T, Kitagawa T, Watanabe S, Watanabe T, Taka-hashi S, Kawaguchi H et al. (1993) Molecular analysis of twoJapanese cases of Denys-Drash syndrome. J Inherit Metab Dis-ease 16:876–880.
Varanasi R, Bardeesy N, Ghahremani M, Petruzzi M, Nowak N, AdamM, Grundy P et al (1994) Fine structure analysis of the WT1gene in sporadic Wilms’ tumors. Proc Natl Acad Sci USA91:3554–3558.
Webb N, Lewis M, Williamson K, van Heyningen V, Bruce J, LendonM, Postlethwaite R (1995) Do children with diffuse mesangialsclerosis in association with mutations of the Wilms’ tumour sup-pressor gene (WT1) require bilateral nephrectomy? PediatrNephrol 9:252–253.
Wilmore HP, White GF, Howell RT, Brown KW (1994) Germlineand somatic abnormalities of chromosome 7 in Wilms’ tumor.Cancer Genet Cytogenet 77:93–98.