Embed Size (px)
Citation preview
A child with oedema
Constantinos J. Stefanidis
“A. Kyriakou” Children's Hospital Athens, Greece
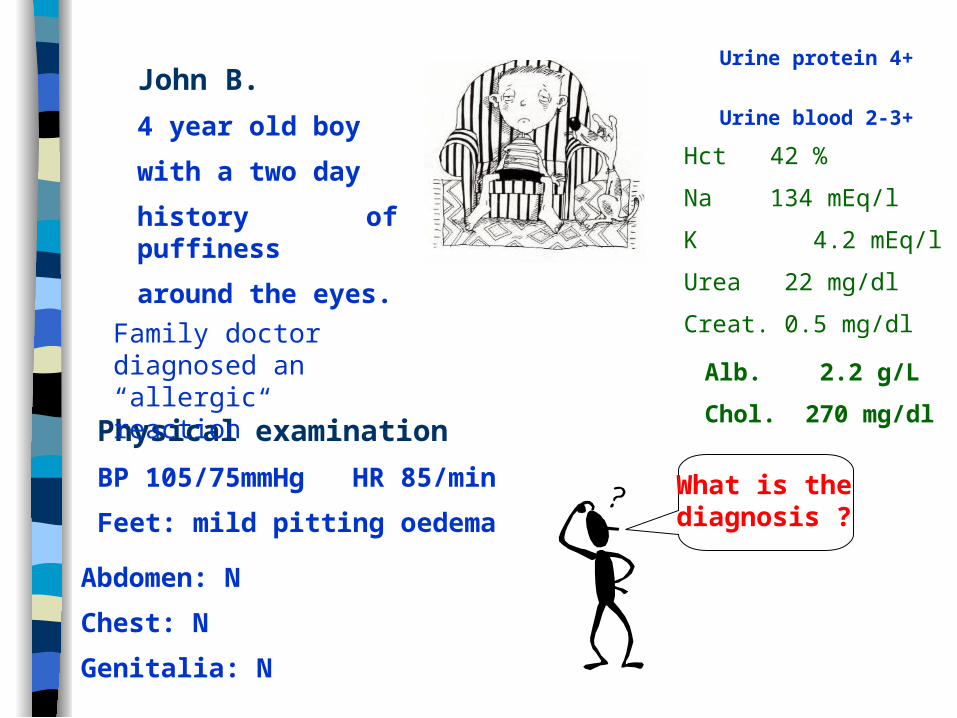
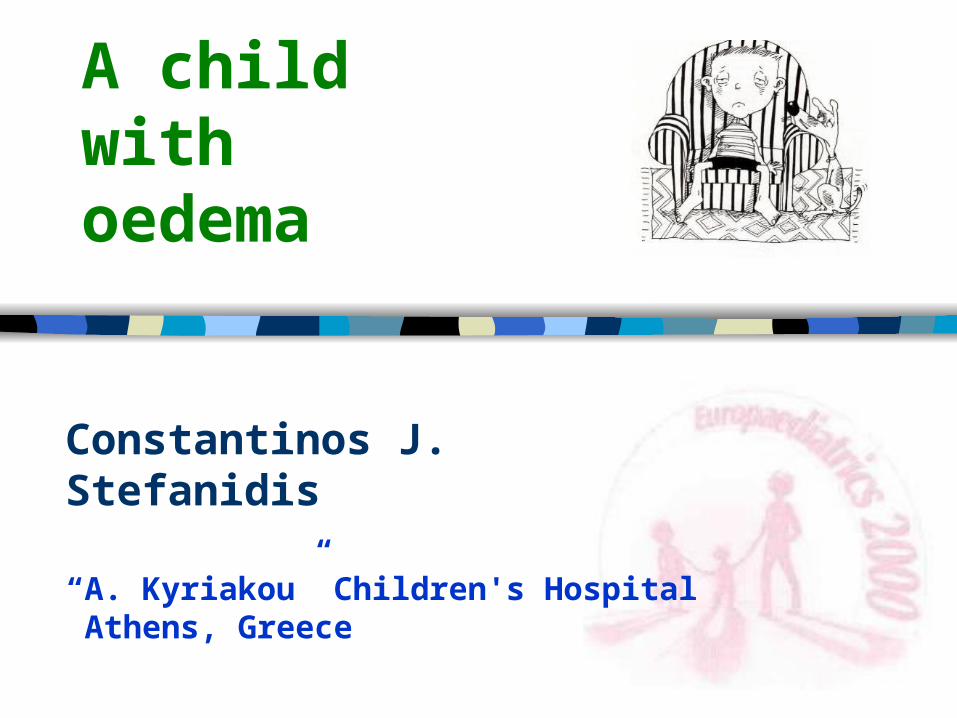
What is the diagnosis ?
Urine protein 4+
Urine blood 2-3+
Hct 42 %
Na 134 mEq/l
K 4.2 mEq/l
Urea 22 mg/dl
Creat. 0.5 mg/dl
John B.
4 year old boy
with a two day
history of puffiness
around the eyes.
Physical examination
BP 105/75mmHg HR 85/min
Feet: mild pitting oedema
Alb. 2.2 g/L
Chol. 270 mg/dl
Family doctor diagnosed an “allergic reaction”
Abdomen: N
Chest: N
Genitalia: N
Idiopathic nephrotic syndrome (NS)
Oedema
Low plasma albumin <25 g/L
Severe proteinuria
>40 mg/m2/hr or Pr : Cr >200 mg/mmol (1.8 mg/mg)
NS may be accompanied by:
• haematuria,
• arterial hypertension and
• decreased GFR
(NS with a nephritic course)
John should be admitted at the Hospital ?
All children with newly diagnosed NS should be admitted at the Hospital. The goals are:
Removal of fluid overload.
Reduction and disappearance of proteinuria.
Prevention of complications (infection, thrombosis).
Why John has oedema ???
Removal of fluid overload. Reduction and disappearance of proteinuria.
Prevention of complications (infection, thrombosis).
Management
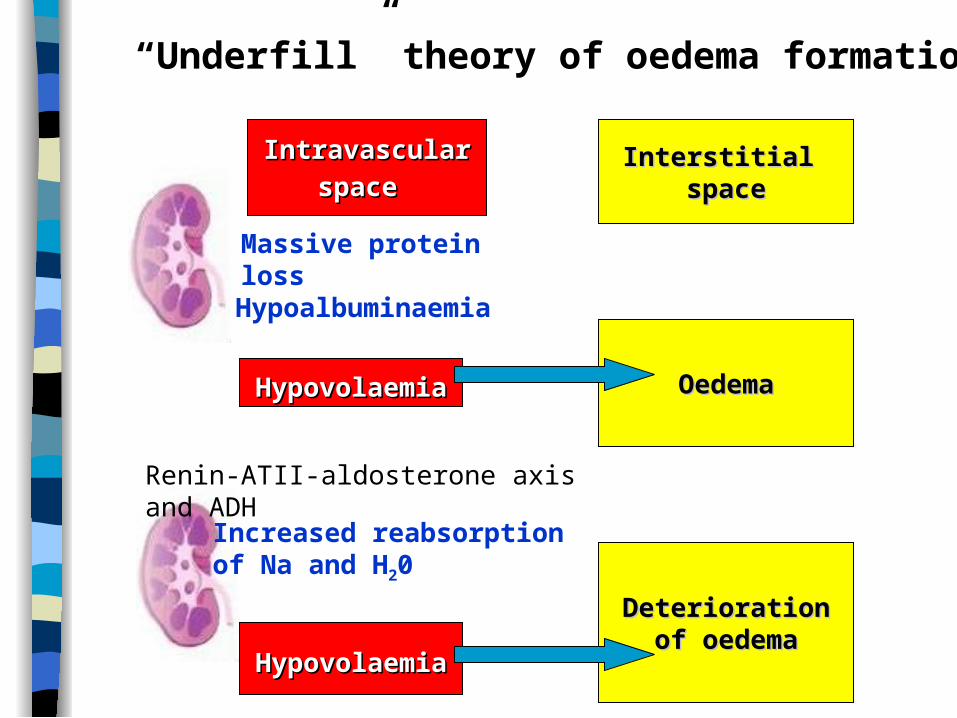
IntravascularIntravascular
spacespace Interstitial Interstitial
spacespace
Massive protein loss
Hypoalbuminaemia
Renin-ATII-aldosterone axis and ADH
Increased reabsorptionof Na and H20
HypovolaemiaHypovolaemia
DeteriorationDeteriorationof oedemaof oedema
“Underfill” theory of oedema formation
HypovolaemiaHypovolaemia OedemaOedema
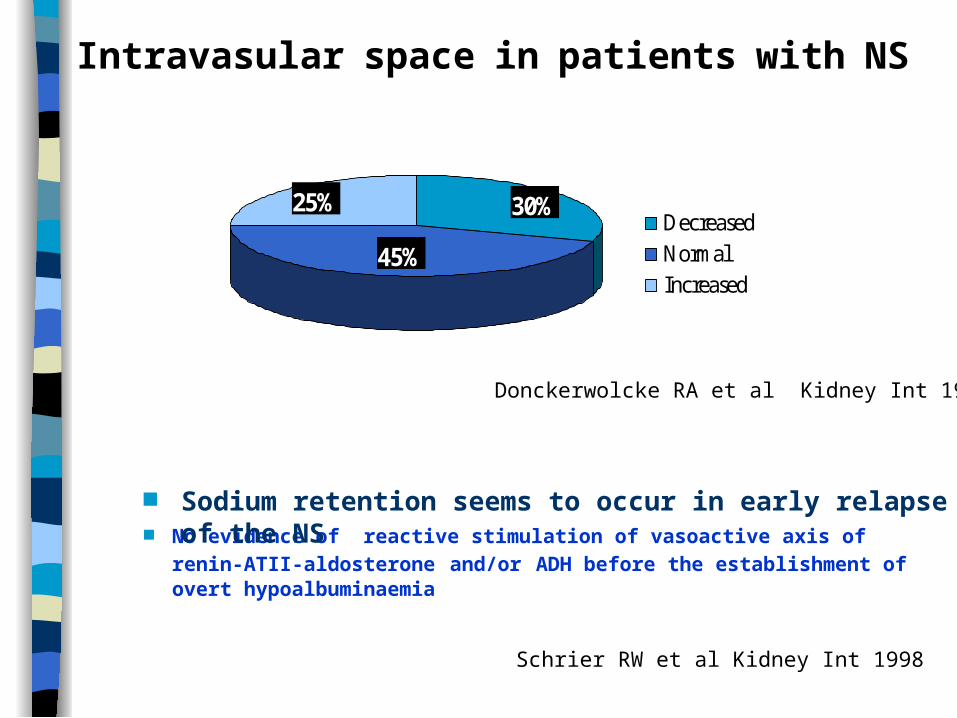
30%
45%
25%DecreasedNormalIncreased
Donckerwolcke RA et al Kidney Int 1997
Intravasular space in patients with NS
No evidence of reactive stimulation of vasoactive axis of renin-ATII-
aldosterone and/or ADH before the establishment of overt hypoalbuminaemia
Schrier RW et al Kidney Int 1998
Sodium retention seems to occur in early relapse of the NS
IntravascularIntravascular
spacespace Interstitial Interstitial
spacespace
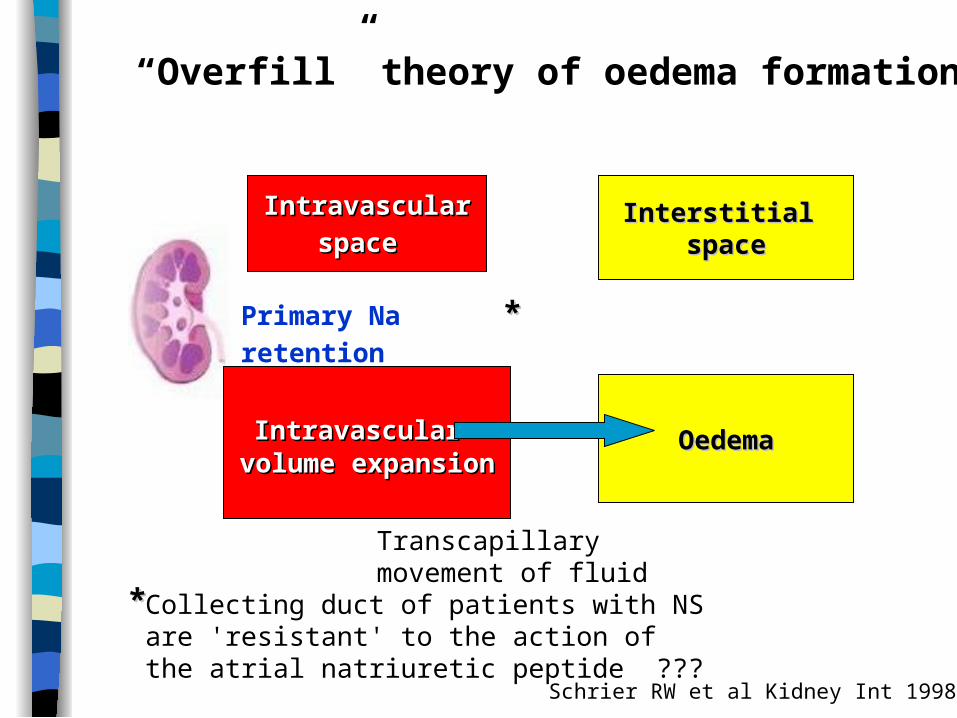
“Overfill” theory of oedema formation
**Collecting duct of patients with NS are 'resistant' to the action of the atrial natriuretic peptide ???
Primary Na retention **
Schrier RW et al Kidney Int 1998
IntravascularIntravascular volume expansionvolume expansion
OedemaOedema
Transcapillary movement of fluid
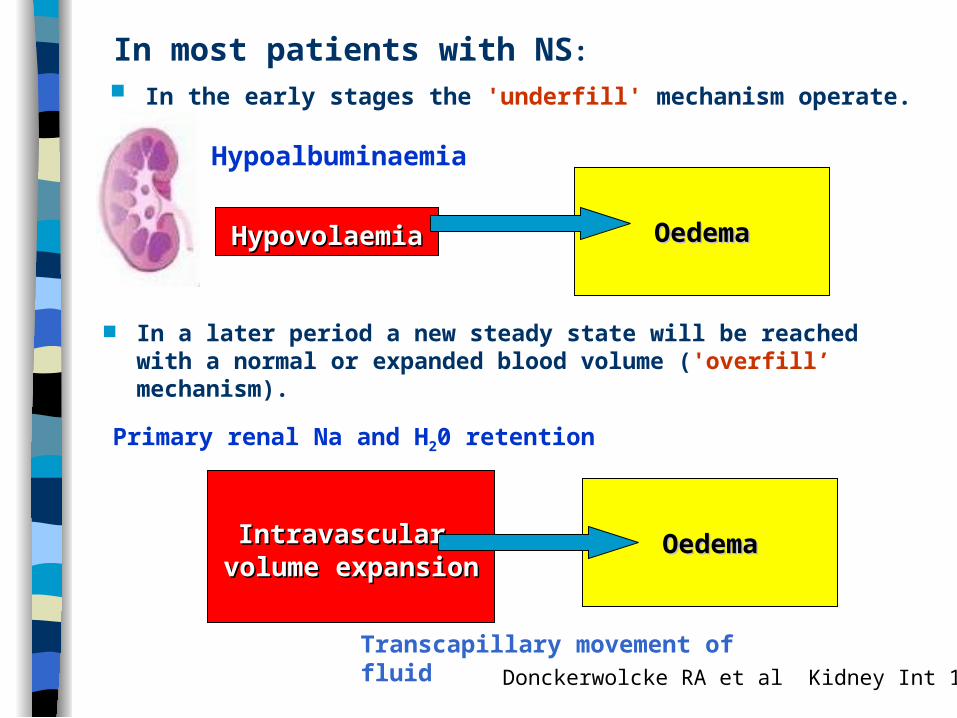
In most patients with NS:
HypovolaemiaHypovolaemia
Hypoalbuminaemia
OedemaOedema
In the early stages the 'underfill' mechanism operate.
In a later period a new steady state will be reached with a normal or expanded blood volume ('overfill’ mechanism).
Donckerwolcke RA et al Kidney Int 1997
IntravascularIntravascular volume expansionvolume expansion
OedemaOedema
Transcapillary movement of fluid
Primary renal Na and H20 retention
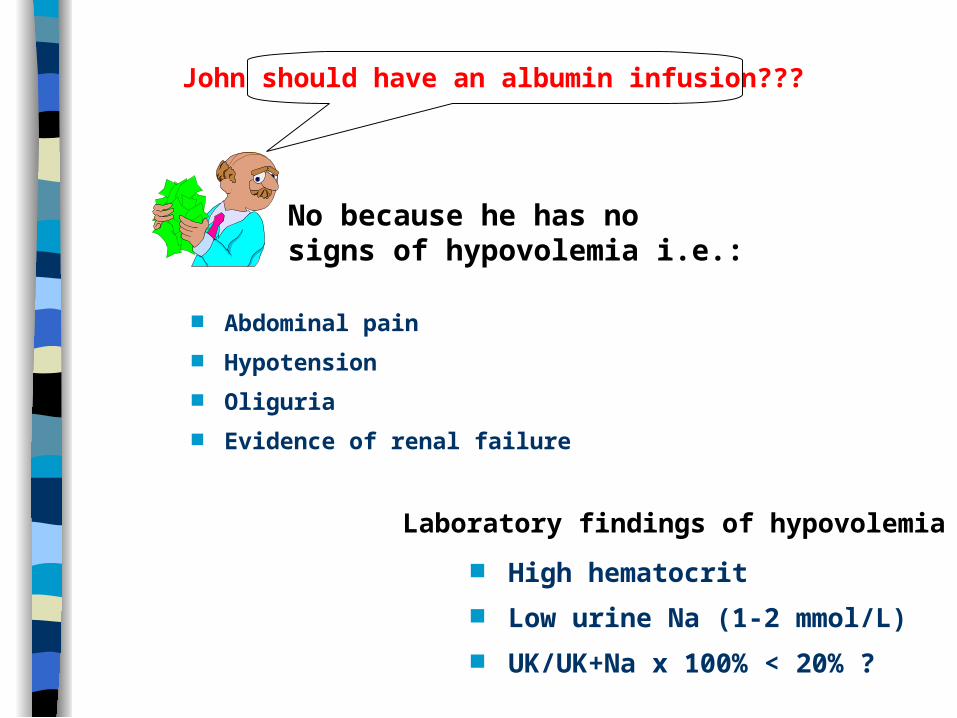
John should have an albumin infusion???
Abdominal pain
Hypotension
Oliguria
Evidence of renal failure
No because he has no signs of hypovolemia i.e.:
Laboratory findings of hypovolemia :
High hematocrit
Low urine Na (1-2 mmol/L)
UK/UK+Na x 100% < 20% ?
Diuretics: In significant oedema and absence of hypovolemia Frusemide and spironolactone 1mg/kg/day.
John should have diuretics???
Hypertension Correction of hypervolemia or hypovolemia. Nifedipine 0,5-1 mg/kg/day and /or atenolol 0,5-1 mg/kg/day.
Removal of fluid overload. Reduction and disappearance of proteinuria.
Prevention of complications (infection, thrombosis).
Management
For how long John should have prednisolone ?
Prednisone (pz): 60 mg/m2/day (or 2mg/kg ideal body weight).Not exceeding a total dose of 80mg/day for one month.
The 2nd month 40 mg/m2 of pz in a single dose every 48 hrs. (Total treatment period of 2 months).
France: One month course of daily , followed by 2 months of alternate day pz (2mg/kg). Then pz is decreased by 0.5mg/kg every 2 weeks. (Total treatment period of 4-5 months).
Germany: 6 weeks course of daily, followed by 6 weeks of alternate day pz. (Total treatment period of 3 months).
Initial steroid therapy. The protocol of theInternational Study of Kidney Diseases in Children
From the late 60's until 80's the ISKDC provided a classification of NS
Early non-responder: proteinuria does not normalize within 4 weeks of daily pz therapy
Relapse: Proteinuria > 40mg/d/m2 (or Albustix 2+ or >) on three consecutive days.
Definitions
Frequent relapses: >2 relapses within 6 months of initial response.
Steroid dependence: 2 consecutive replapses occuring during pz treatment or within 14 days of its cessation.

2115
36
17
61
47
34
81
44
0
20
40
60
80
100
Infrequentrelapses
Frequentrelapses
Total
6 + 6 weeks 4 + 4 weeks 3 + 3 weeks
Prednizone 60 mg/m2/24hrs + 40 mg/m2/48hrs
Brodehl J Clin Nephrol 1991
Initial steroid therapy and frequency of relapses (%)
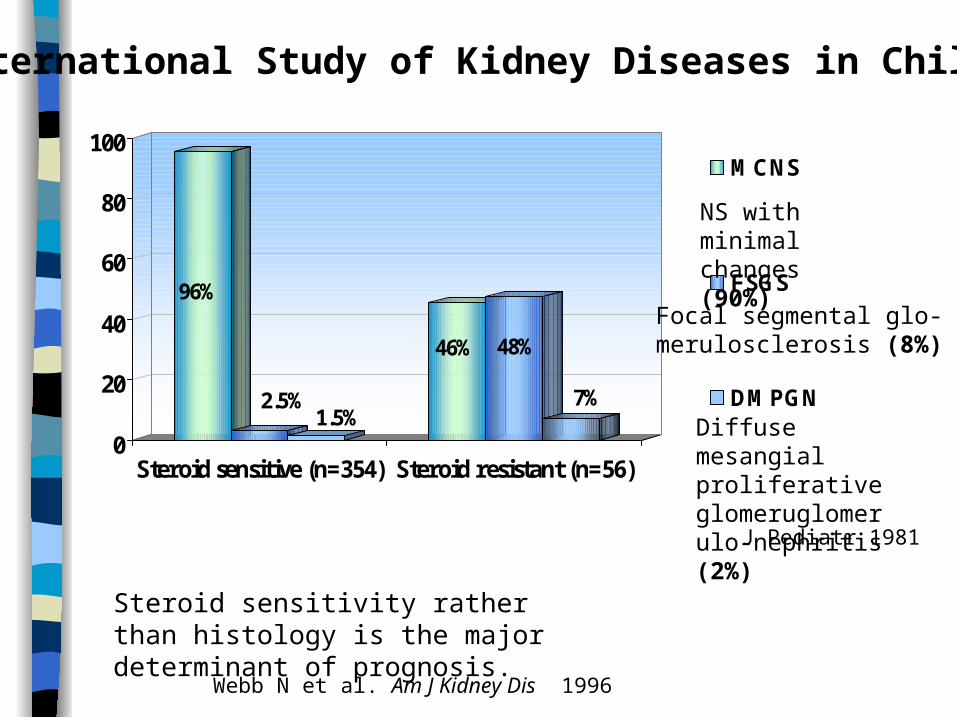
96%
2.5%1.5%
46% 48%
7%
0
20
40
60
80
100
Steroid sensitive (n=354) Steroid resistant (n=56)
MCNS
FSGS
DMPGN
International Study of Kidney Diseases in Children
NS with minimal changes (90%)
Focal segmental glo-merulosclerosis (8%)
Diffuse mesangial proliferative glomeruglomerulo-nephritis (2%)
J Pediatr 1981
Steroid sensitivity rather than histology is the major determinant of prognosis.
Webb N et al. Am J Kidney Dis 1996
Pretreatment indications• Age < 6 months or > 12 years• Nephritic findings (macroscopic hematuria or microscopic and hypertension)• Renal failure
The frequency of relapses alone is not an indication for biopsy.
Webb N et al. Am J Kidney Dis 1996
John has hematuria should he have a renal biopsy ?
23% of children with MCNSand 67 % with FSGS had microscopic hematuria ISKD J Pediatr 1981
Post treatment indication of renal biopsy• Steroid resistance• Frequent relapses before cyclosporin
Removal of fluid overload. Reduction and disappearance of proteinuria.
Prevention of complications (infection, thrombosis).
Management
John should have antibiotics and/or anticoagulation treatment ???

Antibiotics In the oedematous child with gross ascites oral penicillin 125-250 mg BID.
Diet Salt restriction. Normal protein intake. Calorie control.
Activity The child should be mobilized.
What about his diet and activity ???
Prevention of thrombosis by correction of hypovolemia.
Parents should have a booklet with information about the disease.
Children with NS should receive immunization as normal unless they have been taking pz daily for more than one week. Life vaccines can be given only if the child is on a low dose pz.
What parents should know about NS ?
Parents should know that NS is a chronic disease and they should get prepared for possible relapses.
Parents should be informed that chickenpox and measles are major threats and should go to the Hospital if their child is exposed.
Ehrich JHH Drukker A Rec Adv Pediatr 1999
Key points for clinical practice
Childhood NS is a chronic disease and cannot be left untreated.
Steroid-sensitive NS, the most frequently form of childhood NS is a relatively mild form of the disease virtually without long term impairment of glomerular filtration rate.
Steroid-sensitive NS tends to relapse. This requires clear therapeutic strategies to try and keep the patients in long lasting remissions and to minimise the adverse effects of long-term corticosteroid therapy.
Relapses should be detected at home beforethe onset of symptomatic NS by daily
'dipstix' for urinary protein.