Embed Size (px)
Citation preview

The Science of the Total Environment 300(2002) 23–35
0048-9697/02/$ - see front matter� 2002 Elsevier Science B.V. All rights reserved.PII: S0048-9697Ž02.00169-9
A case–control study of childhood leukemia in Woburn,Massachusetts: the relationship between leukemia incidence and
exposure to public drinking water
Kevin Costas*, Robert S. Knorr, Suzanne K. Condon
Bureau of Environmental Health Assessment, 250 Washington Street, Boston, MA 02108-4619, USA
Received 8 July 2001; accepted 1 April 2002
Abstract
A 1981 Massachusetts Department of Public Health study confirmed a childhood leukemia cluster in Woburn,Massachusetts. Our follow-up investigation attempts to identify factors potentially responsible for the cluster. Woburnhas a 130-year industrial history that resulted in significant local deposition of tannery and chemical manufacturingwaste. In 1979, two of the city’s eight municipal drinking water wells were closed when tests identified contaminationwith solvents including trichloroethylene. By 1986, 21 childhood leukemia cases had been observed(5.52 expectedduring the seventeen year period) and the case–control investigation discussed herein was begun. Nineteen cases and37 matched controls comprised the study population. A water distribution model provided contaminated public waterexposure estimates for subject residences. Results identified a non-significant association between potential forexposure to contaminated water during maternal pregnancy and leukemia diagnosis,(odds ratios8.33, 95% CI 0.73–94.67). However, a significant dose–response relationship(P-0.05) was identified for this exposure period. Incontrast, the child’s potential for exposure from birth to diagnosis showed no association with leukemia risk. Wideconfidence intervals suggest cautious interpretation of association magnitudes. Since 1986, expected incidence hasbeen observed in Woburn including 8 consecutive years with no new childhood leukemia diagnoses.� 2002 Elsevier Science B.V. All rights reserved.
Keywords: Leukemia; Drinking water; Tap water; Trichloroethylene
1. Introduction
The city of Woburn, Massachusetts is locatedapproximately 13 miles north-west of Boston andhas a population of approximately 36 000 individ-uals. For over 130 years the community was hostto a variety of industries including greenhouses,leather manufacturers and chemical manufacturers
*Tel.: q1-617-624-5757; fax:q1-617-624-5777.E-mail address: [email protected](K. Costas).
creating products such as arsenic based pesticides, textiles, paper, TNT and animal glues. Complaintsby citizens regarding water quality and ambientair odors date back for over 100 years. In thespring of 1979, two city-owned public water sup-ply wells (commonly referred to as wells G andH) were closed after they were found to becontaminated with arsenic(0.0020 ppm), trichlo-roethylene(TCE) (267 ppb), tetrachloroethylene(21 ppb), chloroform (11.8 ppb), and low levelsof other organic compounds.

24 K. Costas et al. / The Science of the Total Environment 300 (2002) 23–35
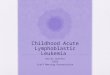
Fig. 1. Number of cases of childhood leukemia diagnosed by year of diagnosis in Woburn, MA, Jan. 1969–Oct. 1997.
Groundwater migration models have been usedto demonstrate the plausibility that contaminatedgroundwater reached wells G and H prior to 1979although no sampling data from the wells prior to1979 exist. The potential for human exposurecreated the need to assess the distribution of thewater from wells G and H through the municipalsystem and the development of a water distributionmodel to assess exposure. Questionable water qual-ity was linked to Woburn’s extensive industrialhistory and the resulting deposition of industrialwaste into the nearby Aberjona river and ground-water aquifers that underlie the city(Tarr, 1987;Durant et al., 1990).
Twelve cases of childhood leukemia(Fig. 1)were diagnosed in Woburn between January 1969and December 1979, spurring an epidemiologicalinvestigation conducted by the MassachusettsDepartment of Public Health(MDPH) (Cutler etal., 1986) with the assistance of the United StatesCenters for Disease Control(CDC). Researchersin the original MDPH investigation had no infor-mation regarding the pattern of water distribution
from wells G and H throughout the city of Woburnand thus assessed exposure based on residentialproximity to contaminated wells alone. They con-cluded that:(1) the incidence of childhood leuke-mia was significantly elevated in Woburn through1979; (2) the majority of the excess cases weremales;(3) six of the cases(half of the childhoodleukemias diagnosed by that time) were diagnosedwhile residing in a single census tract in eastWoburn; (4) no association could be foundbetween environmental hazards and the increasedincidence of childhood leukemia. Between 1980and 1986, nine additional cases were diagnosedbringing the total number of childhood leukemiasdiagnosed since 1969 to 21. Although cases from1980 to 1986 appeared to be more evenly distrib-uted throughout the community, the consistentelevated incidence over time continued to concerncitizens and public officials and demonstrated aneed for further investigation.
From June 1986 through January 1994 no newcases of childhood leukemia were diagnosed inWoburn while slightly more than three cases would

25K. Costas et al. / The Science of the Total Environment 300 (2002) 23–35
have been expected(0.4 casesyyear) during thattime. Two additional childhood leukemia caseswere reported to the Massachusetts Cancer Regis-try in 1994 and one in 1997. If the entire timeperiod from 1969 to 1997(the most current yearof Massachusetts cancer incidence data availableat the time of this publication) is considered, therate of childhood leukemia that would have beenexpected for the 27-year period is less than halfof that observed(24 observed, 11 expected).
2. Materials and methods
The Woburn Childhood Leukemia Follow-UpStudy is a matched case–control study. A case isdefined as a child who was:(1) diagnosed withleukemia prior to their 19th birthday;(2) diag-nosed between 1 January 1969 and 31 August1989; and(3) a resident of Woburn at the time oftheir diagnosis. In January of 1982 hospitalsthroughout Massachusetts were mandated to reportall cancer incident cases to the MassachusettsCancer Registry(MCR). Childhood leukemia inci-dence information since that date for this investi-gation was provided by the MCR. Cases diagnosedprior to 1982 were identified by contacting localpediatric health professionals likely to treat chil-dren from Woburn and by contacting all greater-Boston childhood oncology centers that treatedchildren with leukemia.
2.1. Study population
Two controls for each case were selected fromWoburn Public School records on a geographicallyrandom basis within the community. Controls werechosen from an alphabetic list of all children ofthe same grade level as each case and matched onrace, sex and date of birth plus or minus 3 months.Controls must have been Woburn residents at thetime of diagnosis of the matched case. Matchingby age was essential to assure that cases and theirmatched controls would have had the opportunityto be exposed to similar physical environments(municipal playgrounds and schools) or consump-tion of Woburn public water during the sameperiod of childhood development and history ofthe wells’ operation.
2.2. Data collection
All parents were interviewed in person by thispaper’s first author except for two instances wherefathers were interviewed by telephone. The motherwas considered the primary respondent althougheach parent was administered a separate question-naire. If parents lived apart, interviews were con-ducted with each parent separately. If studysubjects resided with the parents, the subjects wereasked not to be present during the interview.
The study questionnaire was designed to gatherinformation specific to risk factors for leukemia.The mothers’ questionnaire included questionsconcerning demographic and lifestyle characteris-tics, medical history information, environmentaland maternal occupational exposures and use ofpublic drinking water in the home. The fathers’questionnaires focused on their occupational his-tories, including occupational exposures. Electro-magnetic field exposure(Committee on thePossible Effects of Electromagnetic Fields on Bio-logical Systems, 1997; NIEHS Working GroupReport, 1999; Gurney et al., 1996) was assessedby use of a power distribution wire code scheme(Kaune and Savitz, 1994) specific to each house-hold of residence.
2.3. Wells G and H exposure assessment
The most complete assessment of exposure towater from wells G and H would ideally includethe concentration history of each of the contami-nants delivered to each residence during the activelifetime of the wells. The only available contami-nant information resulted from samples taken fromthe wells immediately prior to their closure. Sincemore detailed information was not available con-cerning how the levels of contamination may havechanged over time, the exposure assessmentassumed that the wells were contaminated to thesame degree the entire time they were on line.Exposure was therefore assessed based upon thepotential for a residence to receive water fromwells G and H and not on actual contaminantconcentration in the wells. A hydraulic mixingcomputer model describing Woburn’s water distri-bution system(Murphy, 1991) was utilized for

26 K. Costas et al. / The Science of the Total Environment 300 (2002) 23–35
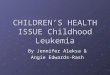
Fig. 2. Geographic distribution of water drawn from contaminated wells G and H during periods of ‘limited use’.
this investigation which allowed for a more refinedexposure assessment based on the distribution ofcontaminated water potentially delivered to eachWoburn resident.
In order to apply the water model to the studypopulation, detailed residential information gath-ered for all cases and controls was collected atinterview. A residential history was obtained formother and child from 2 years prior to conceptionto date of case diagnosis for each case. The sametime boundaries were used for the case’s matchedcontrol. The etiologic period is defined as theperiod 2 years prior to conception for each case tothe date of case diagnosis. Analyses in this reportaddress the etiologic period in its entirety and bytime segments. For each member of the studypopulation, seven exposure scores were calculated.The first was a cumulative exposure score for theentire etiologic period, the second was calculatedfor the pre-conception period, the third for thepregnancy overall, the fourth, fifth and sixth wereeach for a trimester of pregnancy, and the seventhfor the period of time between birth and casediagnosis.
The water distribution model(Murphy, 1991)described the flow patterns of water through
Woburn during the lifetime of wells G and H. Themodel uses data describing the physical layout ofWoburn’s municipal water system and informationregarding the pumping cycles of wells G and H aswell as other active uncontaminated wells that fedWoburn’s municipal water system. ‘ExposureIndex’ values for roughly 50 hydraulically differentneighborhoods known as user demand areas(Figs.2 and 3) were calculated for each month thecontaminated wells were on-line. The exposureindex is defined as the product of the fraction ofthe month when any contaminated water reacheda particular node and, during that period of themonth, the fraction of the water supplied to thatnode which came from the contaminated wells.For example, if during half(0.50) of a certainmonth one-third(0.33) of the water delivered tonode ‘X’ came from wells G and H then theexposure index for that node for that month wouldbe (0.50) (0.33) or 0.165.
Field validation of the model was accomplishedthrough the estimate of deposition concentrationsof a known fluoride tracer. Validation results indi-cated that the model was capable of predicting theboundaries of the geographic areas receiving wellsG and H water to an accuracy of a several house

27K. Costas et al. / The Science of the Total Environment 300 (2002) 23–35
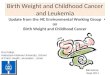
Fig. 3. Geographic distribution of water drawn from contaminated wells G and H during periods of ‘broad use’.
block area. It was able to predict mixture concen-trations with an average error within 10% of theknown concentration. Nearly 70% of the modelpredictions were within 20% of the known vali-dation concentrations.
In general the Woburn water supply distributionsystem takes water pumped from the eight citywells and delivers it through a pipe network toresidential and business consumers. The system’soperators use pump control valves, water storagetanks, and reservoirs to regulate the water distri-bution. Storage facilities have regular emptyingand filling cycles corresponding to user demand.
As seasonal water demands varied, increasedwater demands were met by supplementing Wob-urn’s water supply with water from wells G andH. Figs. 2 and 3 depict user demand areas withinWoburn that would have received water from wellsG and H in typical months of limited(Fig. 2) andbroad(Fig. 3) wells G and H use. The degree ofshading represents the amount of water receivedform the wells with the darkest areas receiving thehighest contaminated water concentrations. Therewere certain periods during the life cycle of thewells when nearly all areas of Woburn, even thosefurthest from the wells, may have received some
water from wells G and H. At other times onlyareas immediately proximal to wells G and Hreceived water from them. The water model wasdesigned to account for each month’s well usevariability including periods when wells G or Hmay have been intermittently taken off-line as wellas potential maximum, minimum and average city-wide water demand conditions.
Assignment of an exposure value for each sub-ject by exposure period required:(1) assignmentof each subject address to a hydrologically distinctarea along the pipe network;(2) summing expo-sure values to create cumulative exposure valuesfor each address; and(3) calculating cumulativeexposure for all Woburn residences in which astudy subject lived during the wells’ operation.Exposure data were assessed using two methods.First, data specific to each month of residencewere summed based upon the location of theresidence to yield a cumulative exposure score.Second, water exposure data were averaged overtime. For example, if a study subject had relativelylittle exposure for most of the time period ofconcern but had particularly high exposure for ashort time, the subject might have the same cumu-lative exposure as someone who had fairly steady

28 K. Costas et al. / The Science of the Total Environment 300 (2002) 23–35
Table 1Distribution of childhood leukemia cases by age at diagnosis and sex between 1969 and 1986, Woburn, MA
Years of age Total cases(%) Total cases by sex Participatingat diagnosis
Male (%) Female(%)cases(%)a
0–4 9(43) 8 (50) 1 (20) 9 (47)5–9 4(19) 3 (19) 1 (20) 3 (16)
10–14 7(33) 4 (25) 3 (60) 6 (32)15–19 1(5) 1 (6) 0 (0) 1 (5)
Total 21(100%) 16 (100%) 5 (100%) 19 (100%)
Two families, each with a male case, chose not to participate in this investigation.a
exposure for many years. Average and cumulativeexposure metrics were assessed as independentvariables and then entered as components of sep-arate multivariate analyses.
The beginning date of pregnancy was taken tobe the date of a mother’s last menstrual period(LMP) and the end of pregnancy was taken to bethe date of birth(DOB). First and second trimes-ters were defined in 14-week intervals beginningwith the date of LMP. The third trimester beganon the date 28 weeks after LMP and ended on theDOB. The beginning and end dates of most preg-nancies did not coincide with the first or last dayof a month. When a pregnancy or trimester beganor ended some time during a month, the exposurevalue for that month was calculated using thenumber of days during the month that the preg-nancy actually occurred.
2.4. Data analysis
Statistical analyses included calculation of sim-ple descriptive statistics, univariate and multivar-iate analyses. Descriptive and univariatecalculations were completed using the ANALYSISand STATCALC functions of Epi Info, version5.01 epidemiologic software for microcomputers(Dean et al., 1990). Conditional logistic regressionwas performed using SAS statistical software(SASSoftware, 1988) PHGLM procedure. A proportion-al hazards model was used to fit the conditionallogistic regression to a case–control study design.Beta coefficients and standard errors were used forthe determination of odds ratios as estimates ofrelative risk and their confidence intervals. Corre-lation coefficients were generated using SAS sta-
tistical software CORR procedure. Trends in therelative risks with increasing exposure were eval-uated using Chi Square and SAS PHGLM proce-dures. The 0.05 probability level was usedthroughout the analysis in the construction ofconfidence intervals and statistical significancetesting. Variables were chosen for use in covariatemodels based on significance in univariate analy-ses. Parental occupations and industries wereexamined based on their potential as risk factorsfor leukemia. Occupations in the petrochemicaland leather industries, machining, and farming forexample have been associated in the literature withleukemia incidence(Linet, 1985).
To increase the precision of our analyses, acomposite covariate methodology described byTukey (1991) was used. In this method, a singlecovariate term is created to represent several cov-ariates. The term is a weighted summation of thesingle term significance of each covariate wheneach covariate is run in an individual regressionanalysis. Wells G and H water exposure scoreswere not normally distributed but demonstrated apattern whereby half the subjects had little or noexposure. The remaining subjects were distributedthroughout the exposure range, few subjects dem-onstrating mid-level exposures and the majority ofthe remaining subjects at the high end of theexposure range. Categorical analysis therefore,became the analytic method of choice.
3. Results
Cases were generally male and less than 9 yearsof age(Table 1). Thirteen children were under 9years old(62%), seven children were between the

29K. Costas et al. / The Science of the Total Environment 300 (2002) 23–35
Table 2Relationship between case–control status and selected main effects, Woburn, MAa
Main effect Exposure Cases Controls Odds ratiosb
category Ns19 Ns37 O.R.(95% CI)
Maternal Never 9 22 1.00alcohol consumption Ever 10 15 1.50(0.54, 4.20)during pregnancy
Breast-fed Never 12 34 1.00study subject Ever 7 3 10.17(1.22, 84.50)
Paternal grandfather Never 11 29 1.00diagnosed with cancer Ever 8 8 2.01(0.73, 5.58)
Father worked in Never 6 27 1.00high risk industryc Ever 13 16 2.55(0.78, 8.30)
Public water was Never 4 17 1.00subject’s primary beverage Ever 15 20 3.03(0.82, 11.28)
Selected main effects had 10 or more positive responses at interview and odds ratio)s1.5.a
Odds ratios as estimates of relative risk calculated using a conditional logistic regression model.b
High risk industries are industry categories consistently identified in the literature to have been associated with leukemiac
incidence.
ages of 10 and 14 years old(33%) and 16 cases(76%) were male. Ten of the male cases and twoof the female cases were deceased at the time ofthis investigation. Nineteen of the 21 case-families(91%) agreed to be interviewed. The two casefamilies who refused to participate in the presentinvestigation were families of male cases whowere deceased. One child was between 5 and 9years of age at diagnosis, the other was between10 and 14 years of age at diagnosis. One of thesefamilies participated in the original(Cutler et al.,1986) MDPH study.
The cases were diagnosed as belonging to threehistopathologic types of leukemia. Seventeen caseswere identified as acute lymphocytic leukemia(ALL ), three cases as acute myelocytic leukemia(AML ) and one case as chronic myelocytic leu-kemia(CML). Both refusal families had cases thatwere diagnosed with ALL.
Two controls were interviewed for each of the19 cases that agreed to participate. For one controlit was subsequently learned that residential infor-mation used to select the control was in error andthe control did not fit the study subject definition.This control was eliminated from the analysis andnot replaced as the error was discovered only afteranalysis had begun.
Table 2 presents results of univariate analysesfor main effects for which there were 10 or morepositive responses at interview and an odds ratiogreater than or equal to 1.5. Analyses revealed thatfamily history of cancer, maternal smoking andalcohol consumption and potential exposure to 60Hz EMF (Gurney et al., 1996) were generally notvery different among cases and controls. Paternalgrandfathers of cases were more likely to havebeen diagnosed with some form of cancer thancontrols. No specific type of cancer seemed morepredominant however. Maternal alcohol consump-tion during pregnancy was weakly and non-signif-icantly associated with leukemia diagnosis. Therewas a statistically significant association betweenhaving been breast-fed and childhood leukemiaincidence. When asked questions specific to life-style habits results indicated that leukemia caseswere three times more likely to have tap water orbeverages made from tap water as their primarybeverage compared to their matched controls.Stratification by histologic subtype made no dif-ference in study results.
Interview data confirmed that all study subjectresidences used public water to supply their homesduring the etiologic period. The water distributionmodel generated average weekly exposure index

30 K. Costas et al. / The Science of the Total Environment 300 (2002) 23–35
Table 3Relationship between case–control status and cumulative exposure to water from contaminated municipal drinking water wells(wells G & H) by exposure time period, Woburn, MA
Exposure Exposure Cases Control Unadjusted Adjustedb
time period category Ns19 Ns37 odds ratiosa odds ratios�% �% O.R.(95% CI) O.R. (95% CI)
From 2 years Never 3 15.8 13 35.1 1.00 1.00before conception Ever 16 84.2 24 64.9 1.99(0.52, 7.71) 2.39 (0.54, 10.59)to case diagnosis(full etiologic period)
During 2 years Never 11 57.9 25 67.6 1.00 1.00before conception Ever 8 42.1 12 32.4 1.77(0.39, 8.00) 2.61 (0.47, 14.37)
During Never 9 47.4 25 67.6 1.00 1.00pregnancy Ever 10 52.6 12 32.4 5.70(0.67, 48.25) 8.33 (0.73, 94.67)
From birth to Never 7 36.8 16 43.2 1.00 1.00diagnosis Ever 12 63.2 21 56.8 1.36(0.00, 5.38) 1.18 (0.28, 5.05)
Odds ratios as estimates of relative risk calculated using a conditional logistic regression model.a
Adjusted using a composite covariate. Adjusted to control for socio-economic status, maternal smoking during pregnancy,b
maternal age at birth of child and breast-feeding.
scores for study subjects that ranged from 0.00 toa maximum of 0.23 throughout the entire studyperiod. Cumulative exposure scores ranged from0.00 to 10.00 for subjects who may have beenexposed consistently starting prenatally to the timeof case diagnosis. As Table 3 indicates, for thefull etiologic period, 16 cases and 24 controls hadat least some potential for exposure to water fromthe contaminated wells. The relative risk of leu-kemia was more than twice as greatwadjusted oddsratio (OR)s2.39x for those who had at least somepotential for exposure during the etiologic periodthan for those who did not, though the 95%confidence intervals(CI) for this statistical analy-sis are wide and the odds ratio is not statisticallysignificant(CI 0.54–10.59).
Those individuals with the potential for at leastsome exposure during the period limited to 2 yearsbefore conception(8 cases and 12 controls) had asimilar level of relative risk with an adjusted ORof 2.61(CI 0.47–14.37). During the pregnancy 10cases and 12 controls had at least some potentialfor exposure to water from the contaminated wells(crude ORs5.70, CI 0.67, 48.25). The relativerisk of leukemia was more than eight times asgreat(ORs8.33) for those who had the potentialfor exposure than those who did not(CI 0.73–94.67). In contrast, those individuals with the
potential for exposure during the period from birthto diagnosis(12 cases and 21 controls) had nearlyno elevation in risk of leukemia based uponcontaminated water exposure(adjusted ORs1.18,CI 0.28–5.05).
Regarding the potential for a dose–responserelationship associated with water exposure, tri-chotomous parameterization for the entire etiologicperiod and each of the three exposure time periodsub-categories showed the strongest relationshipwith leukemia (Table 4). Those most exposedduring pregnancy had more than 14 times greaterrisk of childhood leukemia than those with nopotential for exposure during pregnancy(adjustedORs14.30, CI 0.92–224.52). The ‘Least’ expo-sure level had an elevated relative risk which wasmuch smaller relative to the ‘Never’ exposurelevel with an adjusted relative risk of 3.53(CI0.22–58.14). Results are not statistically signifi-cant and wide confidence intervals are indicativeof the small number of cases and controls percategory. A statistical test for trend across exposurecategories was significant for the period duringpregnancy(P-0.05), suggesting a dose–responserelationship between drinking water exposure dur-ing pregnancy and childhood leukemia. A dose–response association was not evident for any ofthe other exposure time periods.

31K. Costas et al. / The Science of the Total Environment 300 (2002) 23–35
Table 4Dose–response relationship between case–control status and cumulative exposure to water from contaminated municipal drinkingwater wells(wells G and H) exposure time period, Woburn, MA
Exposure Exposure Cases Control Unadjusted Adjustedc
time period categorya Ns19 Ns37 odds ratiosb odds ratios�% �% O.R.(95% CI) O.R. (95% CI)
From 2 years Never 3 15.8 13 35.1 1.00 1.00before conception Least 9 47.4 11 29.8 4.52(0.78, 26.41) 5.00 (0.75, 33.50)to case diagnosis Most 7 36.8 13 35.1 2.41(0.45, 13.01) 3.56 (0.51, 24.78)(full etiologic period)
During 2 years Never 11 57.8 25 67.6 1.00 1.00before conception Least 4 21.1 6 16.2 1.82(0.34, 9.64) 2.48 (0.42, 15.22)
Most 4 21.1 6 16.2 1.68(0.26, 11.04) 2.82 (0.30, 26.42)
From birth to Never 7 36.8 16 43.2 1.00 1.00diagnosis Least 7 26.8 9 24.4 2.24(0.41, 12.37) 1.82 (0.31, 10.84)
Most 5 26.4 12 32.4 0.98(0.20, 4.71) 0.90 (0.18, 4.56)
During Never 9 47.4 25 67.6 1.00 1.00d
pregnancy Least 3 15.8 8 21.6 2.36(0.20, 28.48) 3.53 (0.22, 58.14)Most 7 36.8 4 10.8 14.00(0.98, 195.60) 14.30(0.92, 224.52)
Exposure category cut points are based on no exposure as the lowest category and the two higher categories divided such thata
50% of exposed subjects are in each exposed parameter.Odds ratios as estimates of relative risk calculated using a conditional logistic regression model.b
Adjusted using a composite covariate. Adjusted to control for socio-economic status, maternal age at birth of child and breast-c
feeding.Test for trend is significant(P-0.05).d
As a method of addressing the variability inexposure values and to minimize the effect ofextreme exposure values that exist within exposurecategories, exposure was further assessed usingnormalized exposure scores. Average monthlyexposure values were generated for the exposureperiod associated with the time of the pregnancyas exposure scores during this time period haddemonstrated the strongest association with diseaseoutcome. Normalized, unadjusted relative risk esti-mates for exposure during pregnancy were consis-tent with previous results and demonstrated apositive statistically significant associationbetween disease status and exposure(ORs9.97,CI 1.22–81.22). The trimester of pregnancy inwhich wells G and H water had the strongestassociation with leukemia incidence could not bedetermined with confidence since a high degree ofstatistical correlation(colinearity) was identifiedbetween trimesters.
4. Discussion
The findings in this study suggest that therelative risk of developing childhood leukemia wasgreater for those children whose mothers werelikely to have consumed water from wells G andH during pregnancy than for those who did not.The risk of leukemia significantly increased as theamount of contaminated water from wells G andH delivered to the households increased. In con-trast, there appeared to be no association betweenthe development of childhood leukemia and con-sumption of water from wells G and H by thechildren themselves prior to their diagnosis.Adjustment using a composite covariate did notchange the direction or pattern of the identifiedassociations. The magnitude of the risk estimatesoften increased after adjustment but the pointestimates must be interpreted with caution as smallsample size contributes to wide confidenceintervals.

32 K. Costas et al. / The Science of the Total Environment 300 (2002) 23–35
Lagakos et al.(1986) examined the 12 child-hood leukemia cases known at the time of theirstudy and their potential for exposure to waterfrom wells G and H by the use of a preliminaryversion of the water distribution model used inthis investigation. Results suggested an associationbetween the potential for exposure to wells G andH water and childhood leukemia when exposureoccurred between birth and the time of case diag-nosis. No association with exposure during preg-nancy is identified.
Our investigation suggests an association duringpregnancy but not for exposure after birth. Theseconclusions, although they appear inconsistentwith Lagakos et al.(1986) may not in fact becompletely inconsistent for two reasons. First, theLagakos et al.(1986) investigation included onlythe 12 childhood leukemia cases known at thattime. Our larger body of data is more likely toallow for refinement of exposure-outcome associ-ations. Second, the Lagakos et al.(1986) exposureassessment is based on total yearly exposure esti-mates. Yearly estimates would not provide thesensitivity necessary for assessment of exposureduring specific months of pregnancy or for groupsof months where strong shifts in contaminatedwater distribution occurred. During pregnancy, forexample, Lagakos et al.(1986) assigned annualexposure values based on the mother’s residencein the year the pregnancy ended, even if themajority of the pregnancy occurred in the previousyear. In our study population, more than one-thirdof the cases would have been assigned an exposurescore representing a calendar year different thanthat which included the first trimester. Although itis likely that any misclassification of exposure inLagakos’ work is non-differential, our work illus-trates the potential to have masked a positiveassociation with pregnancy. The temporal distri-bution of leukemia diagnosis demonstrates an ele-vation in incidence followed by a prolonged period(June 1986–February 1994) with no cases. Basedon Massachusetts’s population data, the expectednumber of leukemia cases in Woburn is 0.4yyear.If we examine incidence from the time the wellsopened and include all available years of Woburnchildhood leukemia incidence data(1969–1997),there would have been between 11 and 12 child-
hood leukemia cases expected when in fact 24were observed. The pattern of incidence however,demonstrates that the majority of cases wereobserved from the date the wells went on linethrough the 7 years following well closure. Ele-vations in rates while wells were in operationcould represent effects initiated during that timewhile the 7 years of continued elevation afterclosure could represent cases initiated by exposurewhile the wells were still on line. When morerecent years of incidence are considered indepen-dently (1988–1997), four childhood leukemiadiagnoses would have been expected while threewere observed suggesting the childhood leukemiarate is returning to normal.
No association was identified between smokingduring pregnancy and leukemia risk, a findinggenerally consistent with recent literature(Siegel,1993; Brondum et al., 1999). Associations identi-fied with maternal alcohol consumption, havingbeen breast-fed, and paternal occupation(Table 2)have also not been supported in recent publications(Schutz et al., 1999; Smulevich et al., 1999; Davis,1998; Shu et al., 1999; Ringborg, 1998; Infante-Rivard et al., 2000). No association was identifiedbetween leukemia risk and power line wire codeas a surrogate indicator for exposure to 60 HzEMF.
Levels of potential exposure to contaminatedwell water did not follow any simple parametricdistribution. For this reason, to reduce the impactof the potential for misclassification, analyses wereconducted with categorical variables. We believethe potential for misclassification of exposure tocontaminated water to have had little effect on ourresults based on water model validation resultspreviously discussed(Murphy, 1991). To furtherlimit misclassification however, our survey instru-ment provided opportunities for redundant confir-mation of drinking water sources and residentialwater supply. In certain instances, cases differedin age by many years, resulting in the potentialfor recall bias particularly with regard to waterconsumption during pregnancy. Non-response biasamong case parents is also a concern. It could beargued that case parents would be motivated toreport higher levels of tap water consumption insupport of the proposed connection between con-

33K. Costas et al. / The Science of the Total Environment 300 (2002) 23–35
taminants and leukemia incidence. These types ofmisclassification are limited by our methodology,however, as exposure levels to contaminated waterare based on residential history, not parental rec-ollection of water consumption habits.
Current literature supports the plausibility thatdrinking water as a vehicle for environmentalexposure can have an effect on intrauterine devel-opment. Kramer et al.(1992) found that chloro-form in drinking water was associated with anincreased risk of intrauterine growth retardation.Bove et al.(1995) found an association betweencertain contaminants including TCE in drinkingwater and adverse reproductive outcomes. Swan etal. (1998) identified a relationship with tap waterconsumption and spontaneous abortion and Walleret al. (1998) found a statistically significant asso-ciation between trihalomethanes in drinking waterand spontaneous abortion. Despite the fact thatcontaminants investigated differ in the above cita-tions, these studies suggest a chemical agent’spotential to affect fetal growth.
Although TCE was among the chemical agentsfound to be contaminating wells G and H, othersolvents and metals were detected(Cutler et al.,1986). There are no data to demonstrate howcontaminant concentrations may have varied overtime or even if other compounds not found in thesample such as benzene or chlordane, which werefound in soil, may have been in the water prior toor after sampling. Judgement regarding the plau-sibility of the exposure–outcome relationship inthis investigation must focus on the poorly under-stood relationship between multiple chemicalexposures potentially including but not limited toTCE (McLaughlin and Blot, 1997; Hansen et al.,2001; Infante-Rivard et al., 2001) and their rela-tionship to adverse human health.
Investigations which examined health effects ofexposure to complex mixtures of chemicals includea Canadian case–control study of exposure todrinking water contaminants(trihalomethanes,selected metals, and nitrates). This study did notfind any association between prenatal exposureand childhood leukemia, but reported modest asso-ciations of childhood leukemia and postnatal expo-sure to trihalomethanes, chloroform and zinc(Infante-Rivard et al., 2001). A case–control study
of children with brain tumors did not find aconsistent pattern of association between residen-tial use of a well contaminated with a mix ofneurocarcinogens during pregnancy and subse-quent brain tumors(Mueller et al., 2001).
A study of a groundwater contamination mixtureand childhood cancer in Dover Township(OceanCounty), New Jersey revealed a statistically sig-nificant association and consistency in multiplemeasures of association between prenatal exposureto contaminated well water and leukemia in femalechildren wCase–control study of childhood cancersin Dover Township(Ocean County), New Jersey,2001x. This relationship was strongest for motherswho consumed public drinking water during preg-nancy and not related to the amount of waterconsumed by the children themselves prior todiagnosis.
It is important for us to acknowledge that ourconclusions are based upon imprecise point esti-mates, resulting from the inherent limited statisticalsensitivity associated with the study of rare disease.Statistical significance is most often consideredthe most important criterion for causal inference.Our limited ability to demonstrate significancewarrants cautious interpretation of the precise mag-nitude of risk. Nevertheless, we present data thatare adjusted for a comprehensive array of potentialand actual confounders, and are based on exposureestimates generated from a thorough examinationof municipal water distribution(Murphy, 1991;Wartenberg et al., 2000). Our conclusions arebased on our study’s ability to generate a body ofevidence that addresses several other criteria forcausal inference(Massachusetts Department ofPublic Health, 1997; Weed and Hursting, 1998;US Surgeon General’s Advisory Committee inSmoking and Health, 1964; Hill, 1965). We dem-onstrate a consistently positive association betweenexposure and risk, a statistically significant dose–response relationship, and a decrease in risk afterthe removal of the pathway of exposure. Our majorfinding, the association of potential fetal expo-sure(s) to contaminated water and childhood leu-kemia, coupled with evidence in the literature offetal effects from water contaminants emphasizesthe need for further research to more clearly

34 K. Costas et al. / The Science of the Total Environment 300 (2002) 23–35
understand human sensitivity to both individualand multiple chemical exposures.
Acknowledgments
We would like to thank researchers at theMassachusetts Department of Public HealthBureau of Environmental Health Assessment(BEHA) who assisted in the preparation of thisreport as well as the Massachusetts Cancer Regis-try who provided the cancer incidence data. Thewater distribution model was prepared by theBEHA with funds in part provided by the USAgency for Toxic Substances and Disease Registry(ATSDR) for our earlier study of reproductiveoutcomes in Woburn. We would like to also thankthe members of the ATSDR Community Assis-tance Panel(CAP) for their comments, sugges-tions, and support during the conduct of this andother epidemiologic investigations in Woburn.
References
Bove FJ, Fulcomer MC, Lotz JB, Esmart J, Dufficy EM,Savrin JE. Public drinking water contamination and birthoutcomes. Am J Epidemiol 1995;141(9):850–862 (May 1).
Brondum J, Shu XO, Steinbuch M, Severson RK, Potter JD,Robison LL. Parental cigarette smoking and the risk ofacute leukemia in children. Cancer 1999;85(6):1380–1388(Mar 15).
Case–control study of childhood cancers in Dover Township(Ocean County), New Jersey. Volume II: final technicalreport, draft for public comment. December. New JerseyDepartment of Health and Senior Services, 2001.
Committee on the Possible Effects of Electromagnetic Fieldson Biological Systems. Possible health effects of exposureto residential electric and magnetic fields. Washington DC:National Research Council, National Academy Press, 1997.
Cutler JJ, Parker GS, Rosen S, Prenney B, Healey R, CaldwellGG. Childhood leukemia in Woburn, Massachusetts. PublicHealth Rep 1986;101(2):201–205.
Davis MK. Review of the evidence for an association betweeninfant feeding and childhood cancer. Int J Cancer Suppl.1998;11:29–33.
Dean AG, Dean JA, Buron AH, Dicker RC. Epi info, Version5: a word processing database and statistics program forepidemiology on microcomputers. Stone Mountain, Georgia:USD, Incorporated, 1990.
Durant JL, Zemach JJ, Hemond HF. The history leatherindustry waste contamination in the Aberjona watershed: amass balance approach. Curr Eng Practice 1990 Fall; 41–66.
Gurney JG, Mueller BA, Davis S, Schwartz SM, Stevens RG,Kopecky KJ. Childhood brain tumor occurrence in relationto residential power line configurations, electric heatingsources, and electric appliance use. Am J Epidemiol1996;143(2):120–128 (Jan 15).
Hansen J, Raaschou-Nielsen O, Christenses JM, Johnson I,McLaughlin JK, Lipworth L, Blot WJ, Olsen JH. Cancerincidence among Danish workers exposed to trichloroeth-ylene. J Occup Environ Med 2001;43(2):133–139 (Feb).
Hill AB. The environment and disease: association or causa-tion? Proc R Soc Med 1965;58:295–300.
Infante-Rivard C, Fortier I, Olson E. Markers of Infection,breast-feeding and childhood acute lymphoblastic leukae-mia. Br J Cancer 2000;83(11):1559–1564 (Dec).
Infante-Rivard C, Olson E, Jacques L, Ayotte P. Drinkingwater contamination and childhood leukemia. Epidemiology2001;12(1):13–19 (Jan).
Kaune WT, Savitz DA. Simplification of the Wetheimer–Leeper wire code. Bioelectromagnetics 1994;15(4):275–282.
Kramer MD, Lynch CF, Isacson P, Hanson JW. The associationof waterborne chloroform with intrauterine growth retarda-tion. Epidemiology 1992;3(5):407–413 (Sep).
Lagakos SW, Wessen BJ, Zelen J. An analysis of contaminatedwell water and health effects in Woburn, Massachusetts. JAm Stat Assoc 1986;81(295):583–596.
Linet MS. The leukemias: epidemiologic aspects, monographsin epidemiology and biostatistics, vol. 6. Oxford UniversityPress, 1985.
Massachusetts Department of Public Health. Woburn childhoodleukemia follow-up study. Boston MA: Bureau of Environ-mental Health Assessment, 1997.
McLaughlin JK, Blot WJ. A critical review of trichloroethyleneand perchloroethylene and risk of renal-cell cancer. Int ArchOccup Environ Health 1997;70(4):222–231.
Mueller BA, Newton K, Holly EA, Preston-Martin S. Residen-tial water source and the risk of childhood brain tumors.Environ Health Perspect 2001;109(6):551–556 (Jun).
Murphy PJ. Exposure to wells G and H in Woburn, Massa-chusetts. Boston, Massachusetts: Massachusetts Departmentof Public Health, 1991.
NIEHS Working Group Report. Assessment of health effectsfrom exposure to power-line frequency electric and magneticfields EMFRAPID program, May, NIH Publication NO. 99-4493. 1999.
Ringborg U. Alcohol and risk of cancer. Alcohol Clin ExpRes 1998;22(7 Suppl):323S–328S (Oct, Review).
SAS Software, Version 6, 1988. SAS Institute Inc., SASCircle, Box 8000, Cary, NC 27512.
Schutz J, Kaatsch P, Kaletsch U, Meinert R, Michaelis J.Association of childhood cancer with factors related topregnancy and birth. Int J Epidemiol 1999;28(4):631–639(Aug).
Shu XO, Linet MS, Steinbuch M, Wen WQ, Buckley JD,Neglia JP, Potter JD, Reaman GH, Robison LL. Breast-feeding and risk of childhood acute leukemia. J Natl CancerInst 1999;91(20):1765–1772 (Oct).

35K. Costas et al. / The Science of the Total Environment 300 (2002) 23–35
Siegel M. Smoking leukemia: evaluation of a causal hypothe-sis. Am J Epidemiol 1993;138(1):1–9.
Smulevich VB, Solionova LG, Belyakova SV. Parental occu-pation and other factors and cancer risk in children: I.Study methodologyyoccupational factors. Int J Cancer1999;83(6):712–717 (Dec).
Swan SH, Waller K, Hopkins B, Windham G, Fenster L,Schaefer C, Neutra RR. A prospective study of spontaneousabortion: relation to amount and source of drinkingwater consumed in early pregnancy. Epidemiology1998;9(2):126–133 (March).
Tarr JA. History of pollution in Woburn, Massachusetts, inreview of EPA Report Titled:(Wells G&H Site RemedialInvestigation Report Part I, Woburn, Massachusetts, vol. 2.Boxborough, Massachusetts: Geo Trans, Inc, 1987.
Tukey JW. Use of many covariates in clinical trials. Int StatRev 1991;59(2):123–255.
US Surgeon General’s Advisory Committee in Smoking andHealth. US Department of Health. Education and Welfare.Public Health Service. Washington. DC: US GPO. DHHSpublication No.(PHS 103). 1964.
Waller K, Swan SH, DeLorenze G, Hopkins B. Trihalometha-nes in drinking water and spontaneous abortion. Epidemi-ology 1998;9(2):134–140 (Mar).
Wartenberg D, Reyner D, Siegel Scott C. Trichloroethyleneand cancer; epidemiologic evidence. Environ Health Per-spect 2000;108(Suppl 2):161–176.
Weed DL, Hursting SD. Biologic plausibility in causal infer-ence: current method and practice. Am J Epidemiol1998;147(5):415–425 (Mar 1).