Embed Size (px)
Citation preview
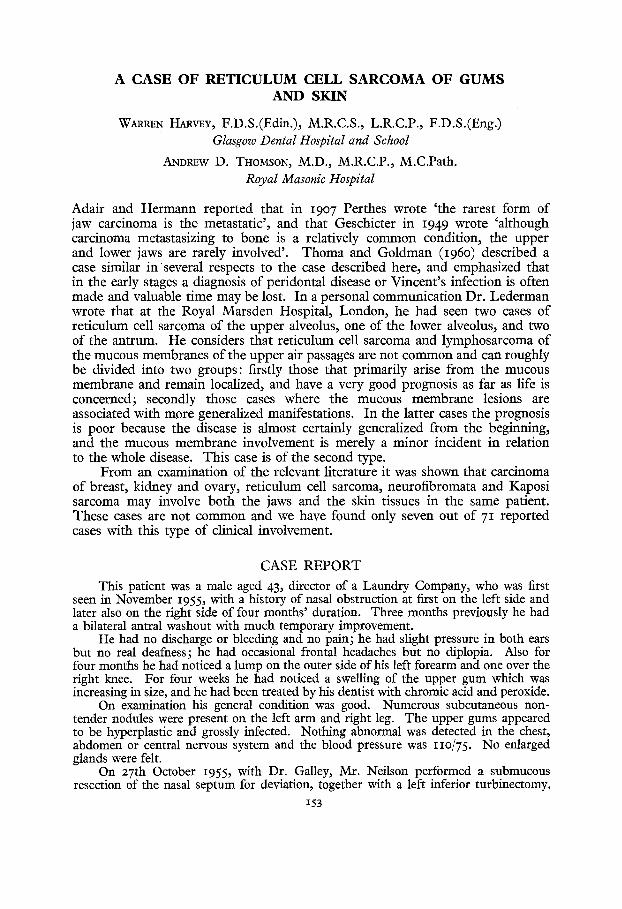
A CASE OF RETICULUM CELL SARCOMA OF GUMS AND SKIN
WARREN HARVEY, F.D.S.(Edin.), M.R.C.S., L.R.C.P., F.D.S.(Eng.) Glasgow Dental Hospital and School
ANDREW D. THOMSON, M.D., M.R.C.P., M.C.Path. Royal Masonic Hospital
Adair and Hermann reported that in I9O7 Perthes wrote ' the rarest form of jaw carcinoma is the metastatic', and that Geschicter in I949 wrote 'although carcinoma metastasizing to bone is a relatively common condition, the upper and lower jaws are rarely involved'. Thoma and Goldman (I96O) described a case similar in several respects to the case described here, and emphasized that in the early stages a diagnosis of peridontal disease or Vincent's infection is often made and valuable t ime may be lost. In a personal communication Dr. Lederman wrote that at the Royal Marsden Hospital, London, he had seen two cases of reticulum cell sarcoma of the upper alveolus, one of the lower alveolus, and two of the antrum. He considers that reticulum cell sarcoma and lymphosarcoma of the mucous membranes of the upper air passages are not common and can roughly be divided into two groups: firstly those that primarily arise from the mucous membrane and remain localized, and have a very good prognosis as far as life is concerned; secondly those cases where the mucous membrane lesions are associated with more generalized manifestations. In the latter cases the prognosis is poor because the disease is almost certainly generalized from the beginning, and the mucous membrane involvement is merely a minor incident in relation to the whole disease. This case is of the second type.
From an examination of the relevant literature it was shown that carcinoma of breast, kidney and ovary, reticulum cell sarcoma, neurofibromata and Kaposi sarcoma may involve both the jaws and the skin tissues in the same patient. These cases are not common and we have found only seven out of 71 reported cases with this type of clinical involvement.
CASE R E P O R T
This patient was a male aged 43, director of a Laundry Company, who was first seen in November I955, with a history of nasal obstruction at first on the left side and later also on the right side of four months' duration. Three months previously he had a bilateral antral washout with much temporary improvement.
He had no discharge or bleeding and no pain; he had slight pressure in both ears but no real deafness; he had occasional frontal headaches but no diplopia. Also for four months he had noticed a lump on the outer side of his left forearm and one over the right knee. For four weeks he had noticed a swelling of the upper gum which was increasing in size, and he had been treated by his dentist with chromic acid and peroxide.
On examination his general condition was good. Numerous subcutaneous non- tender nodules were present on the left arm and right leg. The upper gums appeared to be hyperplastic and grossly infected. Nothing abnormal was detected in the chest, abdomen or central nervous system and the blood pressure was I IO/75. No enlarged glands were felt.
On 27th October I955, with Dr. Galley, Mr. Neilson performed a submucous resection of the nasal septum for deviation, together with a left inferior turbinectomy.
I53
154 B R I T I S H J O U R N A L OF ORAL SURGERY
Bilateral antral puncture revealed pus in the left antrum and, in view of the gum condition, a left inferior antrostomy was performed. A cutaneous nodule was removed for histological examination.
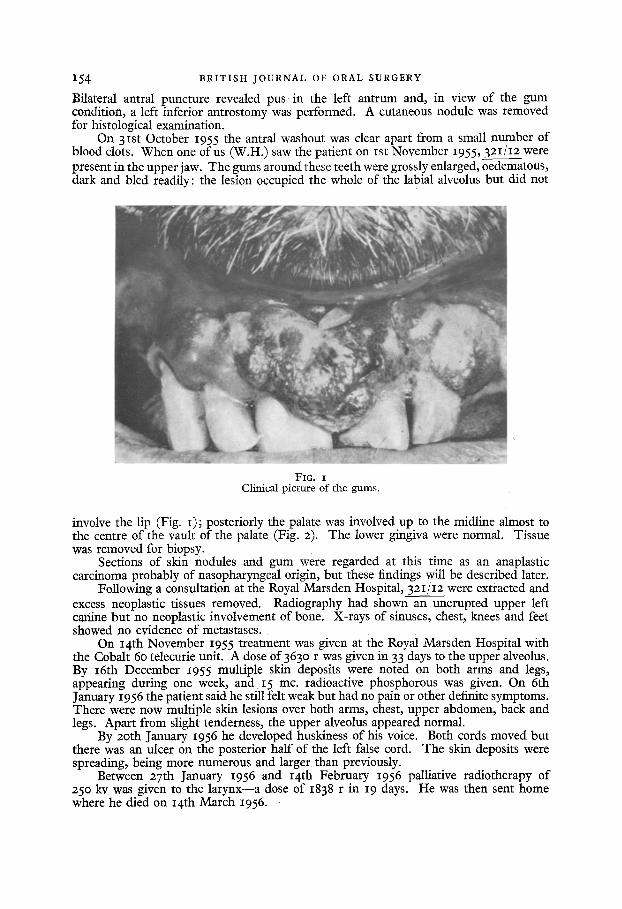
On 3ISt October 1955 the antral washout was clear apart from a small number of blood clots. When one of us (W.H.) saw the patient on ISt November 1955, 3zI / I2 were present in the upper jaw. The gums around these teeth were grossly enlarged, oedematous, dark and bled readily: the lesion occupied the whole of the labial alveolus but did not
FIG. I Clinical picture of the gums.
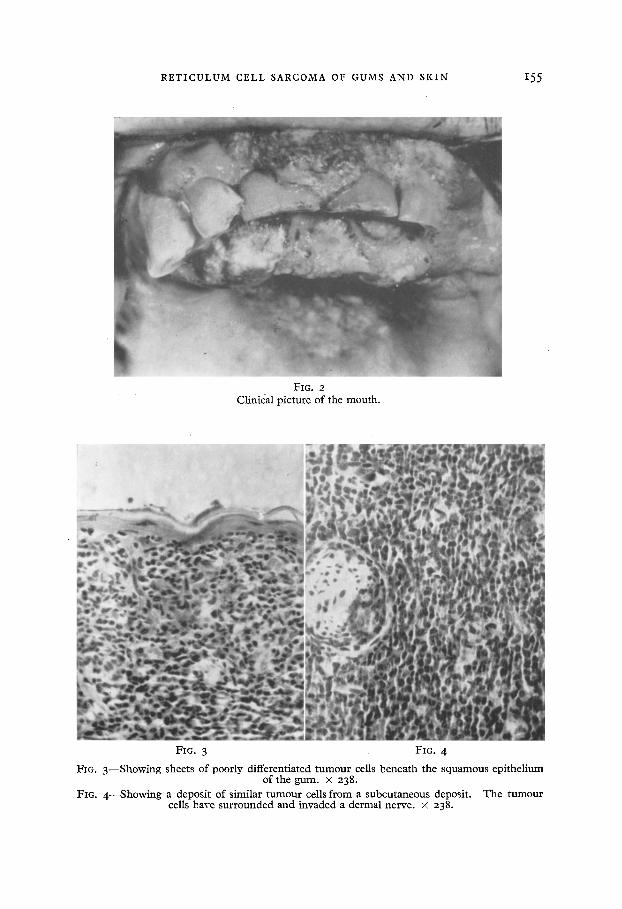
involve the lip (Fig. I); posteriorly the palate was involved up to the midline almost to the centre of the vault of the palate (Fig. 2). The lower gingiva were normal. Tissue was removed for biopsy.
Sections of skin nodules and gum were regarded at this time as an anaplastic carcinoma probably of nasopharyngeal origin, but these findings will be described later.
Following a consultation at the Royal Marsden Hospital, 3 2 I / I 2 w e r e extracted and excess neoplastic tissues removed. Radiography had shown an unerupted upper left canine but no neoplastic involvement of bone. X-rays of sinuses, chest, knees and feet showed no evidence of metastases.
On 14th November I955 treatment was given at the Royal Marsden Hospital with the Cobalt 6o telecurie unit. A dose of 363o r was given in 33 days to the upper alveolus. By I6th December I955 multiple skin deposits were noted on both arms and legs, appearing during one week, and 15 me. radioactive phosphorous was given. On 6th January 1956 the patient said he still felt weak but had no pain or other definite symptoms. There were now multiple skin lesions over both arms, chest, upper abdomen, back and legs. Apart from slight tenderness, the upper alveolus appeared normal.
By 2oth January 1956 he developed huskiness of his voice. Both cords moved but there was an ulcer on the posterior half of the left false cord. The skin deposits were spreading, being more numerous and larger than previously.
Between 27th January I956 and I4th February I956 palliative radiotherapy of 250 kv was given to the larynx--a dose of I838 r in 19 days. He was then sent home where he died on I4th March I956.
R E T I C U L U M CELL SARCOMA OF GUMS AND SKIN 155
FIG. 2 Clinical pic ture o f the mou th ,
FIG. 3 FIG. 4
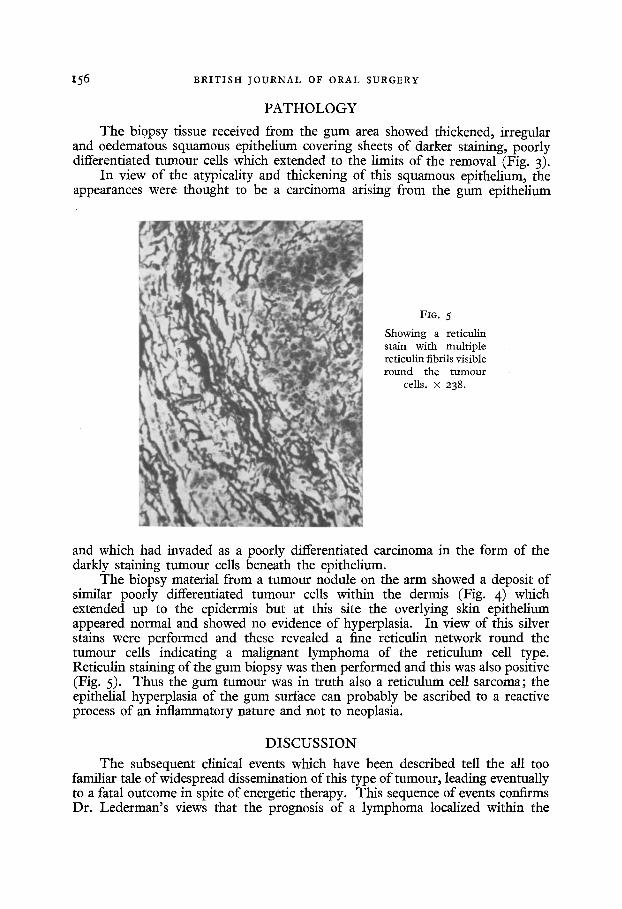
FIG. 3 - - S h o w i n g sheets o f poorly differentiated t u m o u r cells benea th the s q u a m o u s ep i the l ium of the g u m . × 238.
FIG. 4 - - S h o w i n g a deposi t o f s imilar t u m o u r cells f rom a subcu taneous deposit . T h e t u m o u r cells have s u r r o u n d e d and invaded a dermal nerve . × 238.
I56 BRITISH JOURNAL OF ORAL SURGERY
P A T H O L O G Y
The biopsy tissue received from the gum area showed thickened, irregular and oedematous squamous epithelium covering sheets of darker staining, poorly differentiated tumour cells which extended to the limits of the removal (Fig. 3).
In view of the atypicality and thickening of this squamous epithelium, the appearances were thought to be a carcinoma arising from the gum epithelium
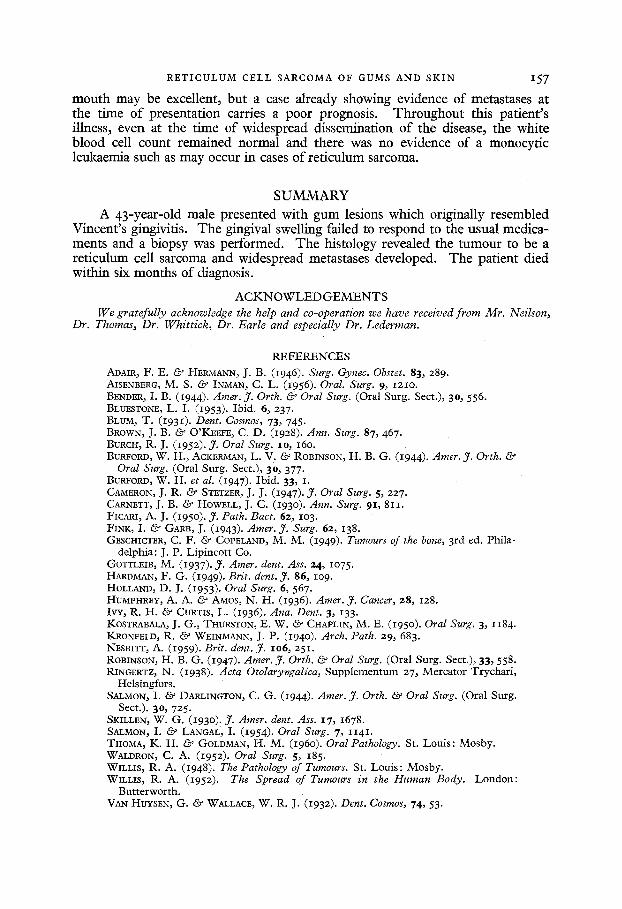
FIG. 5
Showing a reticulin stain with multiple reticulin fibrils visible round the tumour
cells. × 238.
and which had invaded as a poorly differentiated carcinoma in the form of the darkly staining tumour cells beneath the epithelium.
The biopsy material from a tumour nodule on the arm showed a deposit of similar poorly differentiated tumour cells within the dermis (Fig. 4) which extended up to the epidermis but at this site the overlying skin epithelium appeared normal and showed no evidence of hyperplasia. In view of this silver stains were performed and these revealed a fine reticulin network round the tumour cells indicating a malignant lymphoma of the reticulum cell type. Reticulin staining of the gum biopsy was then performed and this was also positive (Fig. 5). Thus the gum tumour was in truth also a reticulum cell sarcoma; the epithelial hyperplasia of the gum surface can probably be ascribed to a reactive process of an inflammatory nature and not to neoplasia.
D I S C U S S I O N
The subsequent clinical events which have been described tell the all too familiar tale of widespread dissemination of this type of turnout, leading eventually to a fatal outcome in spite of energetic therapy. This sequence of events confirms Dr. Lederman's views that the prognosis of a lymphoma localized within the
RETICULUM C E L L SARCOMA OF GUMS AND SKIN I57
mouth may be excellent, but a case already showing evidence o f metastases at the time o f presentation carries a poor prognosis. Throughout this patient's illness, even at the t ime o f widespread dissemination o f the disease, the white blood cell count remained normal and there was no evidence o f a monocyf ic leukaemia such as may occur in cases o f reficulum sarcoma.
SUMMARY A 43-year-old male presented with gum lesions which originally resembled
Vincent's gingivitis. The gingival swelling failed to respond to the usual medica- ments and a biopsy was performed. The histology revealed the tumour to be a reticulum cell sarcoma and widespread metastases developed. The patient died within six months of diagnosis.
A C K N O W L E D G E M E N T S We gratefully acknowledge the help and co-operation we have received from Mr. Neilson,
Dr. Thomas, Dr. Whittick, Dr. Earle and especially Dr. Lederman.
REFERENCES
ADAIR, F. E. Co' HER-MANN, J. B. (1946). Surg. Gynec. Obstet. 83, 289. AISENBERG~ M. S. & INMAN, C. L. (1956). Oral. Surg. 9, 121o. BENDER, I. B. (1944). Amer. ft. Orth. & Oral Surg. (Oral Surg. Sect.), 3o, 556. BLUESTONE, L. I. (1953). Ibid. 6, 237. BLUM, T. (1931). Dent. Cosmos, 73, 745. BROWN, J. B. & O'KEEFE, C. D. (I928). Ann. Surg. 87, 467. BURCH, R. J. (1952). ft. Oral Surg. IO, 16o. BURFORD, W. H., ACKERMAN, L. V. & ROBINSON, H. B. G. (I944). Amer. ft, Orth. &
Oral Surg. (Oral Surg. Sect.), 30, 377- BUREORD, W. H. et al. (1947). Ibid. 33, I. CAMERON, J. R. & STETZER, J. J. (1947). J. Oral Surg. 5, 227. CAgNETT, J. B. & HOWELL, J. C. (193o). Ann. Surg. 9x, 811. FICARI, A. J. (I95O). ft. Path. Bact. 62, IO3. FINK, I. & GARB, J. (I943). Amer. J. Surg. 62, I38. GESCHICTER, C. F. & COPELAND, M. M. (I949). Turnouts of the bone, 3rd ed. Phila-
delphia: J. P. Lipincott Co. GOTTLEIB, M. (I937)- ft. Amer, dent. Ass. 24, IO75. HARDMAN, F. G. (I949). Brit. dent. ,7. 86, lO9. HOLLAND, D. J. (1953). Oral Surg. 6, 567. HUMPHREY, A. A. • AMOS, N. H. (1936). Amer. J. Cancer, 28, 128. IvY, R. H. & CURTIS, L. (1936). Ana. Dent. 3, 133. KOSTRABALA, J. G., THURSTON, E. W. ~o' CHAPLIN, M. E. (I95O). Oral Surg. 3, 1184. KRONEEID, R. ~9' WEINMANN, J. P. (I94O). Arch. Path. 29, 683. NESBITT, A. (1959). Brit. dent. ft. IO6, 251. ROBINSON, H. B. G. (I947). Amer. ft. Orth. & Oral Surg. (Oral Surg. Sect.), 33, 558. RINGERTZ, N. (I938). Acta Otolaryngalica, Supplementum 27, Mercator Trychari,
Helsingfors. SALMON, I. if_.9' DARLINGTON, C. G. (I944). Amer. J. Orth. & Oral Surg. (Oral Surg.
Sect.). 30, 725 • SKILLEN, W. G. (1930) r J. Amer. dent. Ass. x7, 1678. SALMON, I. & LAN~AL, I. (I954). Oral Surg. 7, 1141. THOMA, K. H. & GOLDMAN, H. M. (I96O). Oral Pathology. St. Louis: Mosby. WALDRON, C. A. (I952). Oral Surg. 5, 185. WILLIS, R. A. (1948). The Pathology of Turnouts. St. Louis: Mosby. WILLIS, R. A. (1952). The Spread of Turnouts in the Human Body. London:
Butterworth. VAN HUYSEN, G. & WALLACE, W. R. J. (1932). Dent. Cosmos, 74, 53.

















![Endoplasmic reticulum[1]](https://img.pdfslide.us/doc/110x75/58ed5fc71a28aba1678b4611/endoplasmic-reticulum1.jpg)