Embed Size (px)
Citation preview

A case-control study of melanomas of the soles and palms (Australia and Scotland)
Adele Green1,*, Margaret McCredie2, Rona MacKie3, Graham Giles4, Peta Young1, Colin Morton3,Lea Jackman1 & Vicky Thurs®eld41Queensland Institute of Medical Research, Brisbane, Queensland, Australia; 2Cancer Epidemiology Unit, New SouthWales Cancer Council, Sydney, Australia, and the Department of Preventive and Social Medicine, University of Otago,Dunedin, New Zealand; 3Department of Dermatology, University of Glasgow, Glasgow, Scotland; 4CancerEpidemiology Unit, Anti-Cancer Council of Victoria, Melbourne, Australia (*Author for correspondence)
Received 19 March 1998; accepted in revised form 16 July 1998
Key words: cancer, chemicals, injury, melanoma, nevi, risk factors.
Abstract
Objectives: Because the factors that in¯uence risk of acral melanomas on the soles and palms in Whitepopulations are unknown, we investigated these in a multi-center case-control study.Methods: Cases of melanoma of the feet and hands diagnosed from 1987±93 in persons aged over 18 years wereascertained in eastern Australia and western Scotland. There were 275 cases of melanoma on the soles andpalms matched to 496 controls (selected from the electoral roll) in Australia, and 36 cases matched to 72controls (nominated by general practitioners) in Scotland.Results: Acral melanoma was strongly associated with high total body nevus counts (adjusted relative risk[RR] = 6.3, 95% con®dence interval [CI] = 2.5±15.6), and with nevi on the soles (RR = 7.5, CI = 3.0±18.6).There were also signi®cant positive associations with a penetrative injury of the feet or hands (RR = 5.0,CI = 3.0±8.6) and with heavy exposure to agricultural chemicals (RR = 3.6, CI = 1.5±8.3). Sun-sensitivecomplexions, cumulative sun exposure and a past history of nonmelanoma skin cancer were also associated withincreased risk of acral melanoma. Current cigarette smoking was inversely related to acral melanoma(RR = 0.6, CI = 0.4±0.9).Conclusions: Melanomas of the soles and palms resemble other cutaneous melanomas in their association withsun exposure, but are distinguished from them by their strong positive associations with nevi on the soles,previous penetrative injury, and exposure to agricultural chemicals, and by their inverse association withsmoking.
Introduction
The factors leading to acral melanoma arising on thesole or palm have not been speci®cally studied inCaucasians. Melanomas on these sites are of interestbecause they arise on skin that receives little if any sunexposure, unlike cutaneous melanomas on other ana-tomic sites. Consistent with this, the incidence rates ofplantar melanoma among Caucasians (Whites) andother races are reported to be similar: less than 0.5 per100,000 [1, 2]. Although pre-existing melanocytic neviand trauma have been suggested as risk factors [3±4],®rm evidence is lacking. We aimed to explore the factorsassociated with acral melanomas in Whites of similar
ancestry living in Australia (low latitude) and Scotland(high latitude).
Materials and methods
Subjects
Australia: Cases of melanoma which occurred anywhereon the feet or hands were ascertained from the popu-lation-based cancer registries of Queensland, New SouthWales and Victoria, for the period 1987±93. Cancernoti®cations and histopathology reports for each casewere searched manually to identify, when available, the
Cancer Causes and Control 10: 21±25, 1999. 21Ó 1999 Kluwer Academic Publishers. Printed in the Netherlands.

anatomical site of the primary tumor. Cases aged 18years or over whose treating doctors gave consent forthem to be contacted were eligible for inclusion, andwere invited to participate in the study via completion ofa self-administered questionnaire. To reduce survivalbias, spouses or children were requested to complete thequestionnaires when possible for deceased cases. Foreach case, two people matched by gender, age, and stateof residence were randomly chosen from the stateelectoral roll (enrollment after age 18 is compulsory)and sent a letter explaining the purpose of the study andinviting them to participate. Those able to be contactedand capable of completing the questionnaire wereconsidered eligible.Scotland: Persons over 18 years of age residing in thewest of Scotland who were diagnosed with acralmelanoma in the period 1987±93 and who were regis-tered on the Scottish Melanoma Group database wererecruited. All diagnoses were histologically reviewed andcon®rmed. The general practitioner for each case wasasked to nominate three unselected age- and gender-matched controls who lived locally and the ®rst two whoagreed to participate were included in the study.
Data collection and analysis
All subjects answered a questionnaire containingstandard items concerning ethnicity, height, weight,education, and smoking habit. In Australia, this wasself-administered and in Scotland, it was administered bya trained interviewer. This difference was dictated by thedifferent spread of each study population, being exten-sive (across 20 degrees of latitude) in eastern Australia,and limited (within four degrees of latitude) in westernScotland. Details of all places of residence, occupations,and associated sun exposure (mainly outdoors; mixedindoors/outdoors; mainly indoors) were recordeddecade-by-decade by means of a simpli®ed lifetimecalendar. For each age period, subjects were also askedabout chemical exposures: whether they had beenexposed to any agricultural sprays, pesticides, etc., andif so to name the type of chemical. Questions aboutknown melanoma risk factors were included such aspropensity to burn or tan, natural skin and hair colors,degree of freckling in childhood, general `moliness' of theskin (tendency to melanocytic nevi) compared withstandard diagrams, and estimated number of nevi onsoles, palms, and digits speci®cally (self-counted inAustralia; counted by a nurse in Scotland). Each personwas asked `Have you ever had any serious injury or long-standing irritation to your hands or feet?' and if yes, thetime since injury, the site of injury, and the type of injury.Histories of previous skin cancers and other cancers, and
family history of melanoma were obtained. All subjectswere also asked to mark with a cross on a body map(including magni®ed outlines of the surfaces of a handand a foot) the precise location of any melanomas theyhad had diagnosed.An index of lifetime sun exposure after age 20 (sun
exposure patterns are usually similar in childhood andschool years) was calculated by weighting the propor-tion of years of occupational life (weekdays) spentoutdoors, by amount of sun exposure in all jobs held(weighting factors for different jobs: `outdoor' = 1;`mixed indoor/outdoor' = 0.5; `indoor' = 0). The siteof each melanoma (e.g., toe, back of hand) was usuallyavailable from pathology forms, while exact location(being unobtainable from routine forms) was taken asthe location indicated by each case on the body map.Crude odds ratios (OR) were calculated as estimates ofrelative risk (RR) with 95% con®dence limits (CI).Conditional logistic regression models matched on ageand gender were ®tted using the SAS statistical packagewith adjustment for skin type in the sun exposureanalyses, and for country of residence in the combinedanalyses, and only the adjusted estimates arising fromthese models have been presented.
Results
Of the 820 cases of melanoma of the hands and feetidenti®ed in eastern Australia between 1987 and 1993,contact permission was not obtained from 163 doctors(20%) most of whom either had no recent contact withthe patients concerned or the doctors themselves wereuncontactable due to death or retirement. Twenty-eightcases (three percent) were deceased with no known next-of-kin; 82 (10%) could not be traced; and four casesspoke no English. There were no systematic or signi®-cant differences between the cases who were contactedand those who were not in terms of age, gender, andyear of diagnosis. Of the 542 patients eligible for thestudy, 494 returned completed questionnaires (73 ofwhich were completed by proxies), representing a 91%response rate among those eligible, and a study inclusionrate of 60% of all identi®ed cases. A total of 1,210people randomly selected from the electoral roll aspossible controls were invited to take part, of whom 901(74%) agreed and returned completed questionnaires.There were a total of 275 cases of acral melanoma takenas those which occurred on the soles (119) or palms (14);toes (63) or ®ngers (31) (almost all of which were locatedon the ventral or lateral surfaces); and nailbeds (48). Theremaining 219 cases occurred on the backs of hands andfeet. Only results for acral melanoma are presented here.
22 A. Green, et al.

Of the 143 cases identi®ed in the west of Scotland forthe period 1987±93, 75 (52%) were deceased withoutproxy respondents being contacted, leaving 68 caseswho were approached regarding participation. Com-pleted questionnaires were received from 44 persons(65%), 36 of whom had acral melanoma (soles or toes,26; palms or ®ngers, 10). Cases who participated weresimilar to those who did not, with regard to their age,gender, and year of diagnosis. Among the 108 possiblecontrols contacted, 88 (81%) answered questionnaires.Analyses were carried out separately for each country,and then on the combined Australian and Scottishdataset of 311 cases of acral melanoma and 568 controlsexcept when there were too few Scottish subjectsexposed to certain factors to carry out conditionallogistic regression. Analyses in relation to these factorswere restricted to Australian subjects as indicated.In both Australia and Scotland, annual incidence
rates of plantar melanoma, the most common site ofacral melanoma, were less than 0.5 per 100,000. Ap-proximately 60% of all acral melanoma occurred inwomen in both countries, and around three-quarters ofAustralian cases and 90% of Scottish cases were foundin persons aged over 50 years. Cases tended to havefewer years of education than controls in both studypopulations, though the difference was not signi®cant.Neither ancestry (classi®ed as northern European,Australian, Mediterranean, or Asian) nor body massindex (BMI) was associated with acral melanoma inAustralia, although there was a positive association withBMI (>25) in Scotland which was of borderlinesigni®cance after adjustment for level of education(RR = 2.6; CI = 1.0±7.0) compared with BMI in thenormal range. Smoking was negatively associated withdisease after adjustment for age and gender, withRR = 0.6 (CI = 0.4±0.9) for smokers, and RR = 0.8(CI = 0.6±1.1) among ex-smokers, compared with non-smokers, and estimates were unchanged after adjust-ment for social class.Several pigmentary characteristics were positively
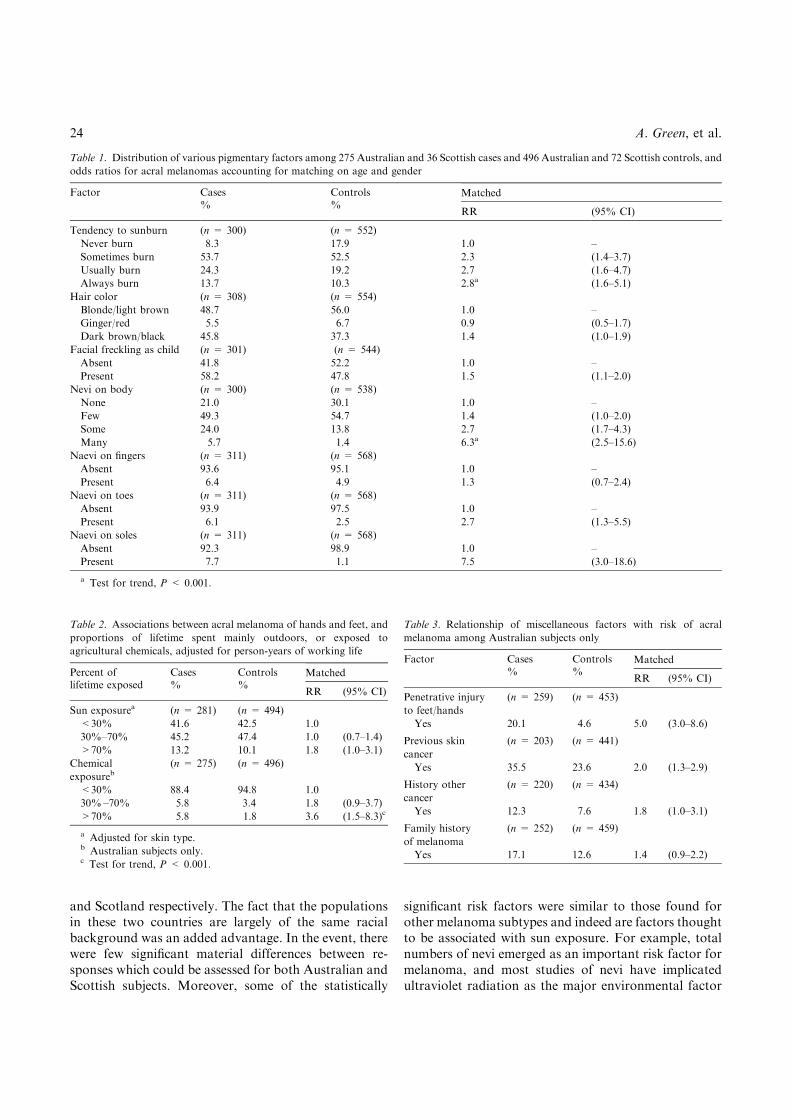
associated with acral melanomas in both populations(Table 1). Compared with those whose skins neverburned, those who burned were at two to three timesthe risk of acral melanoma. Facial freckling (RR = 1.5)and dark brown or black hair color (RR = 1.4) werealso associated. Relative risks were raised for increasingnumbers of nevi in general, and on speci®c sites(Table 1). People who assessed themselves (or in Scot-land were assessed by a trained nurse) as having somenevi, were at approximately three times the risk of thosewith no nevi; those reporting many nevi on their bodywere at over six times the risk of acral melanoma. Thestrongest site-speci®c association was with number of
nevi on the soles. More than seven percent cases butonly one percent controls had one or more plantar nevi(RR = 7.5, CI = 3.0±18.6).In Australia and Scotland, people with the highest
estimated sun exposure had the same, signi®cantly raisedrisk of acral melanoma after adjustment for age, gender,and skin type though the trend was not signi®cant(Table 2). Also, exposure to agricultural chemicals wassigni®cantly associated with acral melanoma (data avail-able only for Australian subjects) (Table 2). Results werenot altered by adjustment for sun exposure. Chemicals,predominantly cited by cases were agricultural spraysand herbicides. Further analysis showed a signi®cantassociation (P < 0.005) between increasing chemicalexposure and plantar nevi irrespective of melanomastatus, with people in the heavy exposure category attwice the odds of having plantar nevi compared withthose with little or no chemical exposure.The remaining factors could only be assessed in
relation to acral melanomas among Australian subjects.People who recalled a serious penetrative injury to theirfeet or hands were at a ®vefold increase in risk of acralmelanoma (RR = 5.0; CI = 3.0±8.6) compared withthose who did not recall such an injury (Table 3). (Amore site-speci®c risk of injury was not calculable usinga control group.) There was no association with havinghad a chronic skin condition affecting soles or palms. Ahistory of previous skin cancer and a history of cancerother than skin cancer were both associated with acralmelanoma, the latter with borderline signi®cance. Theweak association with a family history of melanoma wasnot signi®cant (Table 3).
Discussion
The initial impetus to this study was a desire to identifyfactors other than ultraviolet light exposure that mightcontribute to cutaneous malignant melanoma. Studies ofmelanoma incidence which can distinguish acral fromsuper®cial spreading, nodular, and lentigo malignamelanoma suggest that the incidence of acral melanomais probably not rising, and is certainly not behaving likesuper®cial spreading lesions [5]. This appears to applywhether the de®nition of acral is used for the histopath-ological subtype or for lesions on the extremities.Furthermore, acral melanoma incidence appears to besimilar in all racial types [1]. We therefore reasoned thata study of risk factors predisposing to acral melanomamight throw some light on factors other than ultravioletradiation in the development of melanoma, and sodecided to compare acral melanoma in countries withhigh and low ambient sun exposure, namely Australia
Melanomas on soles and palms 23
and Scotland respectively. The fact that the populationsin these two countries are largely of the same racialbackground was an added advantage. In the event, therewere few signi®cant material differences between re-sponses which could be assessed for both Australian andScottish subjects. Moreover, some of the statistically
signi®cant risk factors were similar to those found forother melanoma subtypes and indeed are factors thoughtto be associated with sun exposure. For example, totalnumbers of nevi emerged as an important risk factor formelanoma, and most studies of nevi have implicatedultraviolet radiation as the major environmental factor
Table 1. Distribution of various pigmentary factors among 275 Australian and 36 Scottish cases and 496 Australian and 72 Scottish controls, and
odds ratios for acral melanomas accounting for matching on age and gender
Factor Cases Controls Matched% %
RR (95% CI)
Tendency to sunburn (n = 300) (n = 552)
Never burn 8.3 17.9 1.0 ±
Sometimes burn 53.7 52.5 2.3 (1.4±3.7)
Usually burn 24.3 19.2 2.7 (1.6±4.7)
Always burn 13.7 10.3 2.8a (1.6±5.1)
Hair color (n = 308) (n = 554)
Blonde/light brown 48.7 56.0 1.0 ±
Ginger/red 5.5 6.7 0.9 (0.5±1.7)
Dark brown/black 45.8 37.3 1.4 (1.0±1.9)
Facial freckling as child (n = 301) (n = 544)
Absent 41.8 52.2 1.0 ±
Present 58.2 47.8 1.5 (1.1±2.0)
Nevi on body (n = 300) (n = 538)
None 21.0 30.1 1.0 ±
Few 49.3 54.7 1.4 (1.0±2.0)
Some 24.0 13.8 2.7 (1.7±4.3)
Many 5.7 1.4 6.3a (2.5±15.6)
Naevi on ®ngers (n = 311) (n = 568)
Absent 93.6 95.1 1.0 ±
Present 6.4 4.9 1.3 (0.7±2.4)
Naevi on toes (n = 311) (n = 568)
Absent 93.9 97.5 1.0 ±
Present 6.1 2.5 2.7 (1.3±5.5)
Naevi on soles (n = 311) (n = 568)
Absent 92.3 98.9 1.0 ±
Present 7.7 1.1 7.5 (3.0±18.6)
a Test for trend, P < 0.001.
Table 2. Associations between acral melanoma of hands and feet, and
proportions of lifetime spent mainly outdoors, or exposed to
agricultural chemicals, adjusted for person-years of working life
Percent of Cases Controls Matchedlifetime exposed % %
RR (95% CI)
Sun exposurea (n = 281) (n = 494)
<30% 41.6 42.5 1.0
30%±70% 45.2 47.4 1.0 (0.7±1.4)
>70% 13.2 10.1 1.8 (1.0±3.1)
Chemical
exposureb(n = 275) (n = 496)
<30% 88.4 94.8 1.0
30%±70% 5.8 3.4 1.8 (0.9±3.7)
>70% 5.8 1.8 3.6 (1.5±8.3)c
a Adjusted for skin type.b Australian subjects only.c Test for trend, P < 0.001.
Table 3. Relationship of miscellaneous factors with risk of acral
melanoma among Australian subjects only
Factor Cases Controls Matched% %
RR (95% CI)
Penetrative injury
to feet/hands
(n = 259) (n = 453)
Yes 20.1 4.6 5.0 (3.0±8.6)
Previous skin
cancer
(n = 203) (n = 441)
Yes 35.5 23.6 2.0 (1.3±2.9)
History other
cancer
(n = 220) (n = 434)
Yes 12.3 7.6 1.8 (1.0±3.1)
Family history
of melanoma
(n = 252) (n = 459)
Yes 17.1 12.6 1.4 (0.9±2.2)
24 A. Green, et al.

in determining nevus numbers [6]. Cumulative sunexposure, history of previous skin cancer and fair skintype were all signi®cant risk factors for acral melanomaconsistent with a positive relation with sun exposure,although dark rather than fair hair was also associated.The lack of association with education observed for acralmelanoma in both Australia and Scotland is seen for allcutaneous melanoma in Australia, although it is incon-sistent with the positive gradients with melanoma inNorthern Hemisphere populations [6].There was an unexpected inverse association between
smoking and acral melanoma in Australian and Scottishstudy populations, not seen for other melanoma. Thismay re¯ect an unknown confounder, or there may be agenuine protective effect, for example, through decreasedperipheral arterial ¯ow as a result of cigarette smoking [7].Also histories of local trauma or of exposure to agricul-tural chemicals have not been identi®ed as risk factors forother subtypes of melanoma and are not sun exposure-related. Our data do not allow us to say whether thepenetrative injury was at the actual site at which the acralmelanoma subsequently developed. Similarly althoughacral nevi emerged as a signi®cant risk factor for acralmelanoma, review of a sample of the histology slidesavailable does not suggest that these nevi were precursorsto melanoma. Systematic observation bias is unlikely toexplain the association with acral nevi. In Scotland, atrained nurse counted nevi, while inAustralia results werebased on self-report and proxies' responses, with aweakerassociation between plantar nevi and acral melanomaamong proxies. Recall bias on the part of affected cases isalso considered unlikely to explain the observed associ-ations with injury and with chemical exposure sincecorresponding associations were not observed for mela-nomas on the dorsal surfaces of the feet and hands in theother part of this study (data not presented in this paper).The only other case-control study of acral melanoma todate was based on 60 cases of plantar melanoma and 256controls. Subjects were of mixed Indian and Hispanicancestry and were drawn from hospitals in Paraguay [4].As in the present study associations were found forreported plantar nevi and local injuries.Tendency to plantar nevi may be inherent or may be
associated with other factors, for example chemothera-peutic agents [8, 9] or perhaps agricultural chemicals assuggested by the present data. Local penetrative injurymay act at the promotional stage of acral melanomathrough stimulation of melanocytic cells by ®broblast
growth factor that is abundant in healing wounds. Theassociation with sun exposure again raises the possibilityof a `solar circulating factor', ®rst hypothesized by Leeand Merrill [10] to explain the occurrence of melanomaon sites that receive little direct sun exposure.In conclusion, it is important to distinguish cases of
acralmelanoma fromother cutaneousmelanomas and thisrelies on accurately recording the subsite of all melanomas,both on pathology forms and by cancer registries. Wesuggest that practitioners should be alerted to the possi-bility of acral melanoma among fair-skinned older pa-tients who present with an unusual acral lesion and whoalso have plantar nevi or give a history of penetrativeinjury or long exposure to agricultural chemicals.
Acknowledgements
The project was supported by the Queensland CancerFund, the New South Wales Cancer Council, and theAnti-Cancer Council of Victoria.
References
1. Stevens N, Liff J, Weiss N (1990) Plantar melanoma: is the
incidence of melanoma on the sole really higher in blacks than
whites? Int J Cancer 45: 691±693.
2. Dwyer P, MacKie RM, Watt DC, Aitchison TC (1993) Plantar
malignant melanoma in a white Caucasian population. Br J
Dermatol 128: 115±120.
3. Coleman W, Loria P, Reed R, Krementz E (1980) Acral
lentiginous melanoma. Arch Dermatol 116: 773±776.
4. Rolon PA, Kramarova E, Rolon HI, Khlat M, Parkin DM (1997)
Plantar melanoma: a case-control study in Paraguay. Cancer
Causes Control 8: 850±856.
5. MacKie R, Hunter JAA, Aitchison TC, et al. (1992) Cutaneous
malignant melanoma, Scotland, 1979±89. Lancet 339: 971±975.
6. International Agency for Research on Cancer (1992) Solar and
Ultraviolet Radiation. IARC Monogr Eval Carcinog Risks Humans,
Vol. 55. Lyon: IARC, 99±228.
7. Golledge J (1997) Lower-limb arterial disease. Lancet 350: 1459±
1465.
8. Hughes BR, Cunliffe WJ, Bailey CC (1989) The development of
excess numbers of benign melanocytic naevi in children after
chemotherapy for malignancy. Br Med J 299: 88±91.
9. Green A, Smith P, McWhirter W, et al. (1993) Melanocytic naevi
and melanoma in survivors of childhood cancer. Br J Cancer 67:
1053±1057.
10. Lee JAH, Merrill JM (1970) Sunlight and the aetiology of
malignant melanoma: a synthesis. Med J Aust 2: 846±851.
Melanomas on soles and palms 25





























