Embed Size (px)
Citation preview
1
A Cardiologist’s Guide to Love
A brief overview of what everyone should know about Palpitations, Heartache and Heartbreak!
Eric J Dueweke, MD FACC
• No one has yet to offer to pay me for my opinion.
• No significant (or insignificant) industry relationships.
• References included on slides and available per request.
Disclosure
2

2
You decide to celebrate Valentines by seeing an urgent add onpatient to your clinic: 19 year old woman with no past medicalhistory who experienced three minutes of palpitations whiledrinking Red Bull and studying for an organic chemistry final.
Your Plan:
A. Tell her to drop organic chemistry and take finance; that’swhere the money is!
B. Echocardiogram, stress test, referral to EP.
C. Prescribe metoprolol; titrate to coma.
D. Reassure and offer an event recorder.
Palpitations
4
• Palpitations are an unpleasant awareness of the heartbeat.
• Common cause of presentation ~ estimated at 16%.
• Extensive differential diagnosis; benign to malignant.
• Cause is cardiac 43%, psychiatric 31%, other 10%.
Am J Med 1996; 100:138
What Are Palpitations and Why Do I Care?
5
3
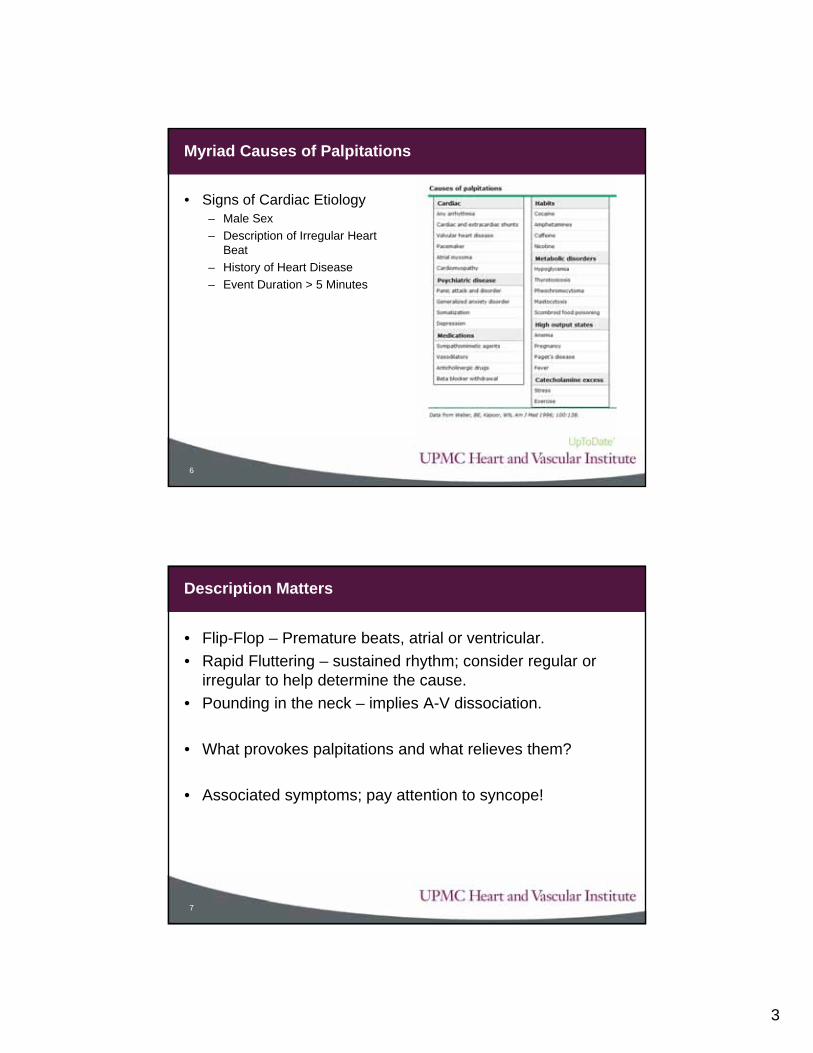
• Signs of Cardiac Etiology– Male Sex
– Description of Irregular Heart Beat
– History of Heart Disease
– Event Duration > 5 Minutes
Myriad Causes of Palpitations
6
• Flip-Flop – Premature beats, atrial or ventricular.
• Rapid Fluttering – sustained rhythm; consider regular or irregular to help determine the cause.
• Pounding in the neck – implies A-V dissociation.
• What provokes palpitations and what relieves them?
• Associated symptoms; pay attention to syncope!
Description Matters
7
4
• Electrocardiogram – Snapshot in Time
• 24 – 48 Hour Holter Monitor – Continuous, limited time.
• 30 Day Event Recorder – Series of 2-3 minute loops
• Implantable Loop Recorder – Long term monitoring
• An EKG is always a great place to start!– LVH, Q waves, Prolonged QT, Preexcitation, RBBB/LBBB
• EP Study, Echocardiogram, Stress Test, LHC
Testing - Choose Wisely
8
• High risk symptoms: Syncope, Chest Pain, Poorly Tolerated
• Known history of underlying cardiac disease
• Intractable or sustained symptoms
• Known diagnosis with challenge in management
• We are happy to see any patient who is concerned!
When Should I Refer?
9
5
• 54 year old male with a history of prior myocardial infarction has had several episodes of palpitations lasting several minutes. He often feels heavy beats in his neck. He thinks he passed out last time they occurred.
• What diagnosis are you considering?A. Sinus Tachycardia
B. AV Nodal Reentrant Tachycardia
C. Atrial Fibrillation
D. Premature Ventricular Contractions
E. Ventricular Tachycardia
Time for a Test of Knowledge
10
• 38 year old woman presents with palpitations occurring a couple times per month. They typically last 20 – 30 minutes. Last time she had the symptoms, they stopped abruptly after she picked up a heavy piece of furniture.
• What test do you order:A. Electrocardiogram
B. 24 Hour Holter Monitor
C. 30 Day Event Recorder
D. Implantable Loop Recorder
E. EP Study
The Beat Goes On
11
6
• Recognize when palpitations are likely to be benign.
• Recognize how to use testing to elucidate etiology.
• Know when to manage and when to ask for help.
Take Home Points
12
Heartache – Chest Pain
13
Most Popular Times for Breakup

7
Your 64 year old patient goes out on a date. He unfortunatelyforgot to ask you if he was healthy enough for romance andpresents to the emergency department 3 hours later withcrushing chest discomfort, radiating down both arms, relievedwith nitroglycerin and associated with nausea. What is themost worrisome clinical feature?
A. Crushing chest discomfort
B. Radiating down both arms
C. Relieved with nitroglycerin
D. Associated with nausea
E. He’s wearing Axe body spray.
Matters of the Heart
14
Rational Clinical Exam - JAMA
15
8
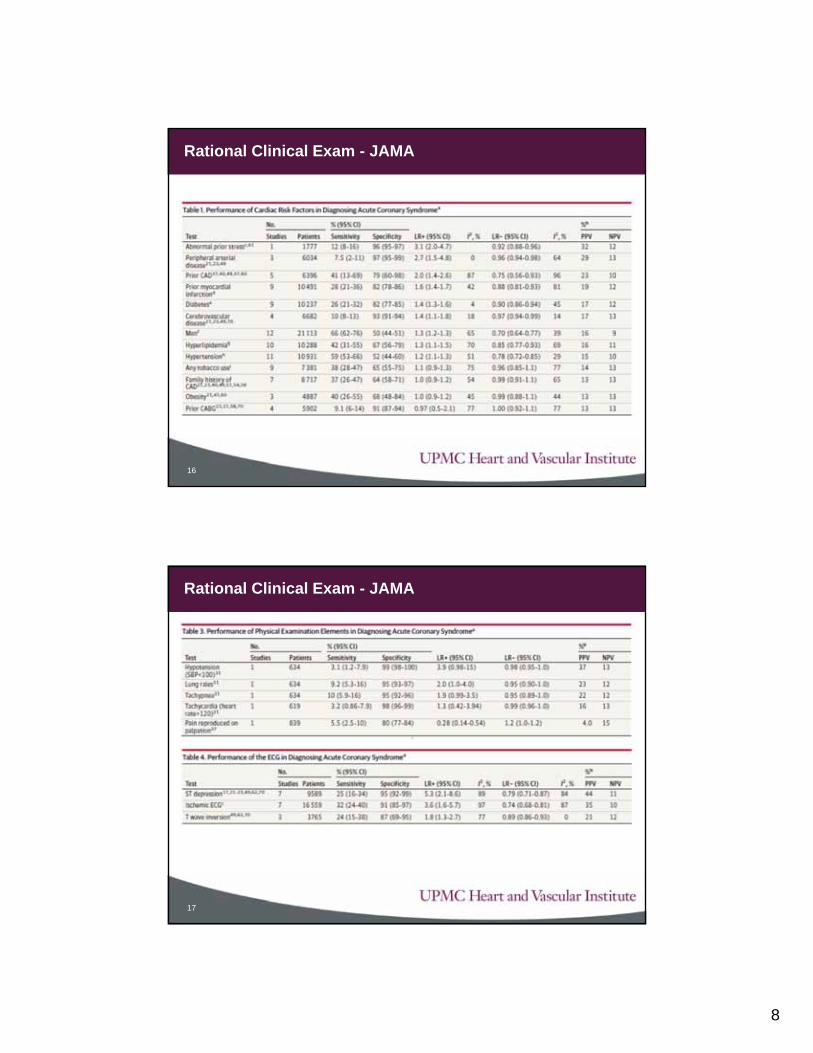
Rational Clinical Exam - JAMA
16
Rational Clinical Exam - JAMA
17
9
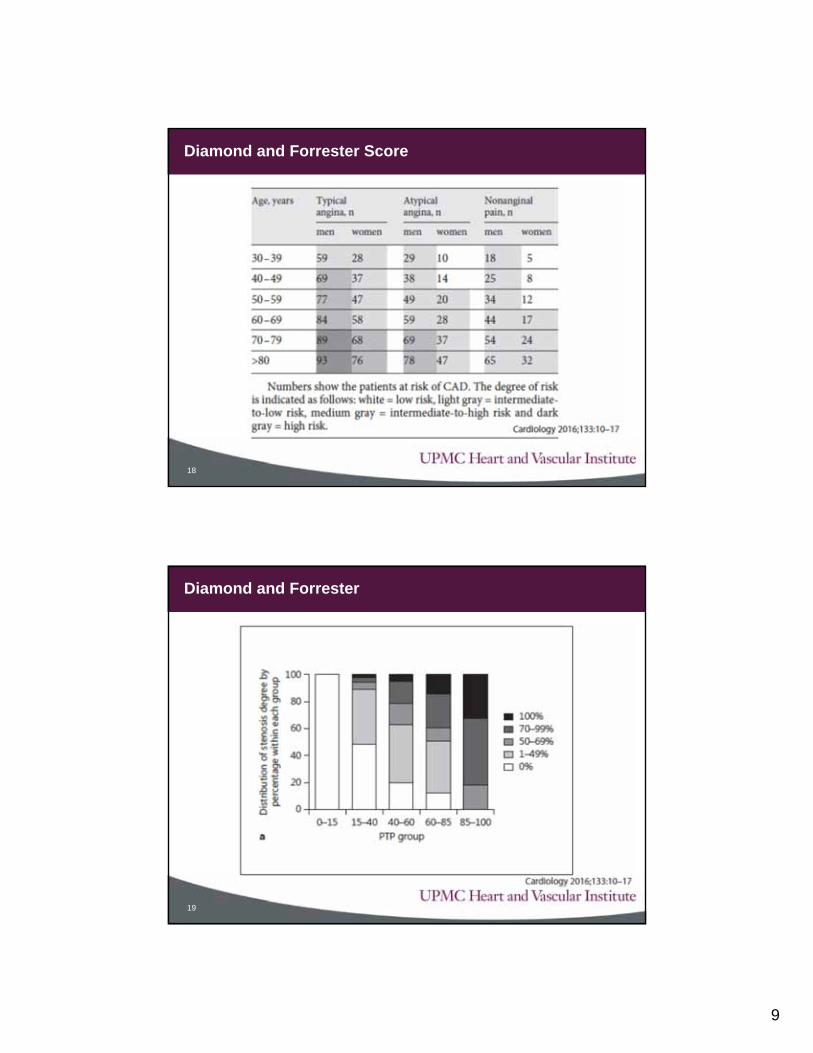
Diamond and Forrester Score
18
Diamond and Forrester
19

10
• Definition used from original Diamond Forrester Model1. Substernal Chest Pain or Discomfort
2. Provoked by Exertion or Emotional Stress
3. Relieved by Rest or Nitroglycerin
• Having 3/3 is typical, 2/3 atypical, 0-1 / non-specific.
Classification of Angina
20
Putting It All Together –HEART Score
21
11
• Diabetes
• Current (or recent < 1 month) Smoker
• Diagnosed Hypertension
• Diagnosed Hyperlipidemia
• Family History of CAD
• Obesity
HEART Score Risk Factors
22
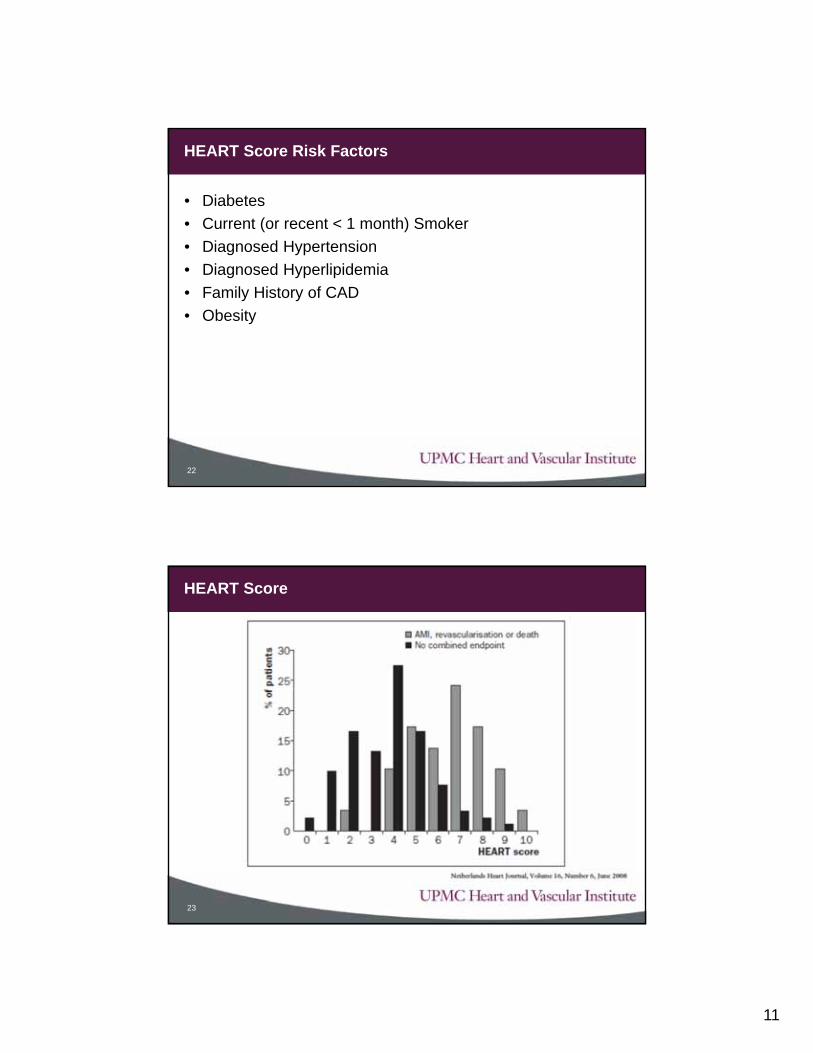
HEART Score
23
12
• When evaluating chestpain, risk assessmentis key.
• There are validatedalgorithms to help, useyour cell phone!
• Testing is only neededwhen it is going tochange management.
Take Home Points
24
You are in your heart-shaped Jacuzzi and the pager rings :
“STAT Consult: 98 year old male admitted with a hip fracture; troponin is 0.056 ng/mL….activate cath lab?”
Your Response:
A. Turn up the bubbles and ignore the page.
B. Transfer to cath lab; he’s Rob’s problem now.
C. Take an aspirin (and statin, beta blocker etc) and call me in the morning.
D. Tell Ortho to fix the hip and stress him next week.
Heartbreak – Elevated Troponin
26
13
• Universal Definition of an MI:– Rise / Fall of troponin with at least one value > 99th percentile.
– And….
• Symptoms of ischemia
• New pathologic Q waves on an EKG
• New ST-T changes or LBBB
• Confirmed coronary thrombus
• Imaging evidence of loss of myocardium
Heartbreak – So is it an MI?
27
• Type I – Plaque rupture leading to coronary thrombosis
• Type II – Secondary to supply/demand mismatch
• Type III – Sudden cardiac death
• Type IVa – Related to PCI
• Type IVb – Stent thrombosis
• Type V – Related to CABG
Types of MI
28
14
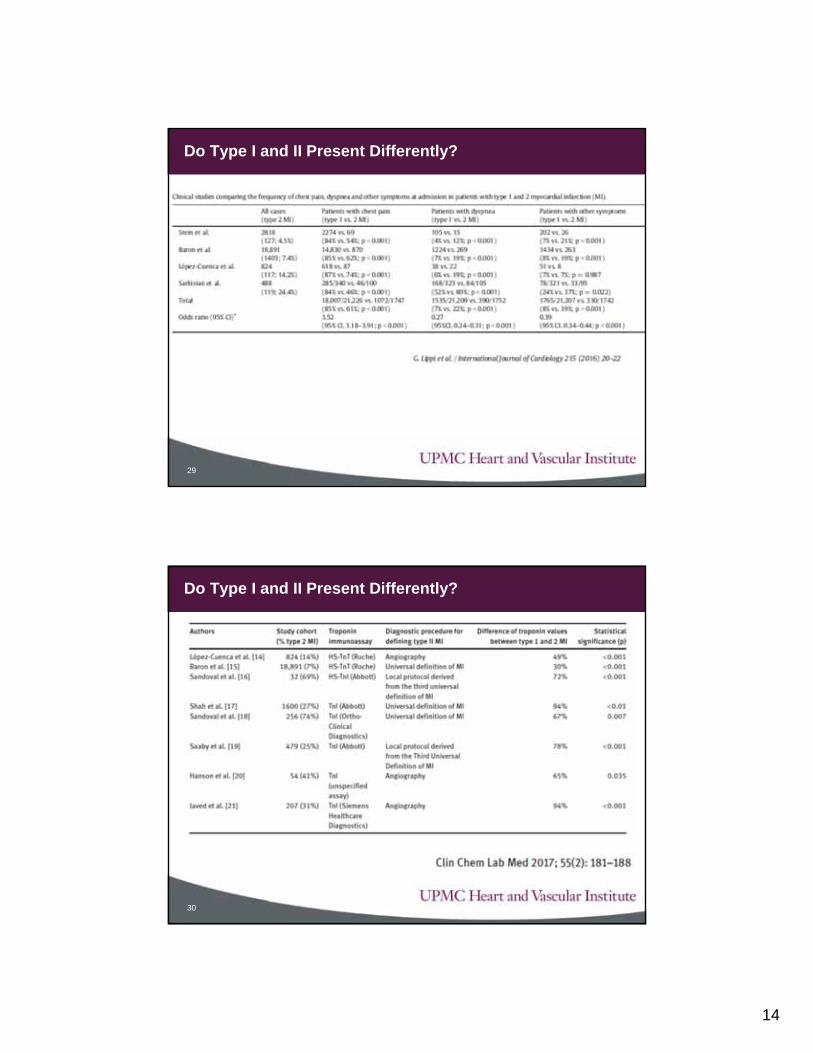
Do Type I and II Present Differently?
29
Do Type I and II Present Differently?
30
15
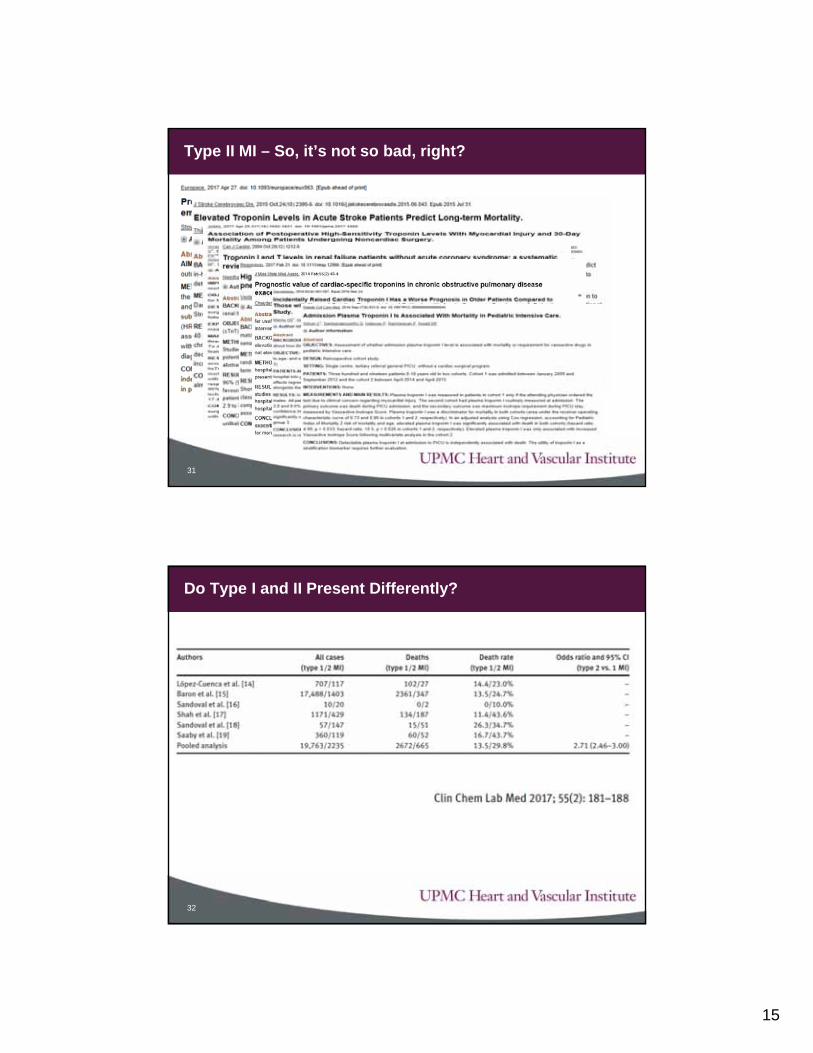
Type II MI – So, it’s not so bad, right?
31
Do Type I and II Present Differently?
32
16
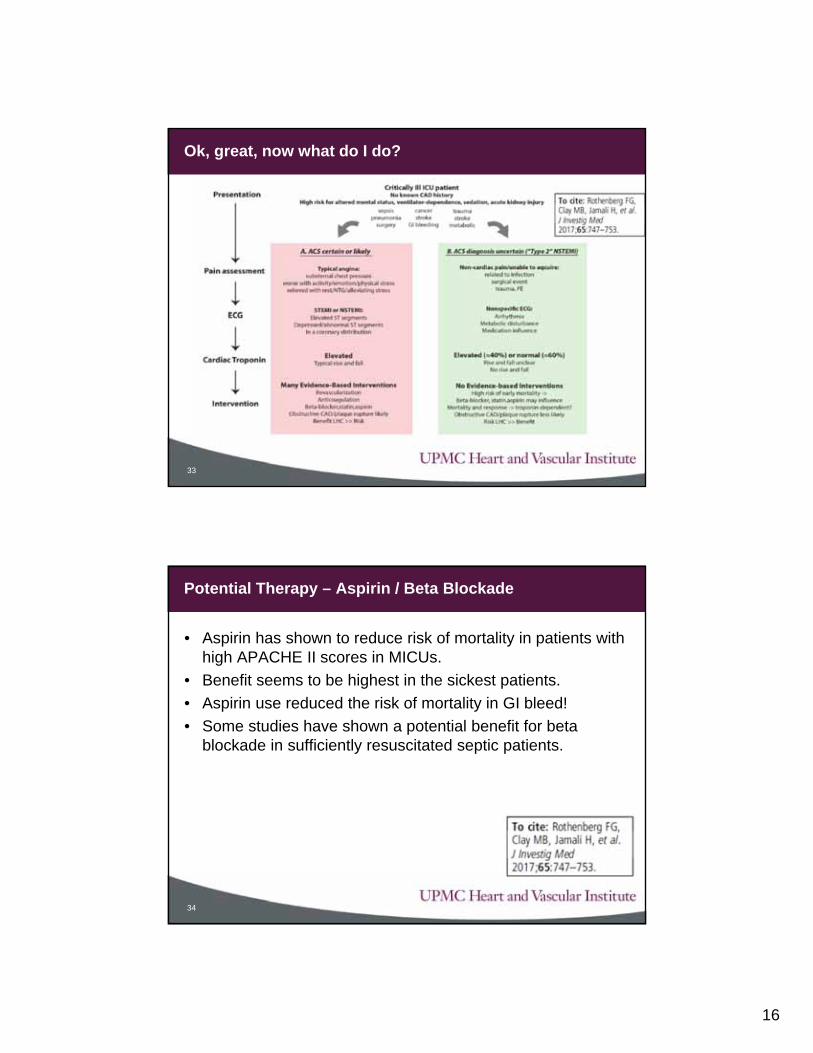
Ok, great, now what do I do?
33
• Aspirin has shown to reduce risk of mortality in patients with high APACHE II scores in MICUs.
• Benefit seems to be highest in the sickest patients.
• Aspirin use reduced the risk of mortality in GI bleed!
• Some studies have shown a potential benefit for beta blockade in sufficiently resuscitated septic patients.
Potential Therapy – Aspirin / Beta Blockade
34
17
• A meta-analysis in 2015 showed no benefit of statins inreducing mortality in critically ill patients.
• A subsequent study demonstrated that the benefit may bepresent in less-sick populations (lower APACHE II score).
• A large retrospective study was able to classify the benefitby the degree of troponin elevation – those with lower or noelevated troponin did better but there was no improvementin patients with high troponins.
Potential Therapy - Statins
35
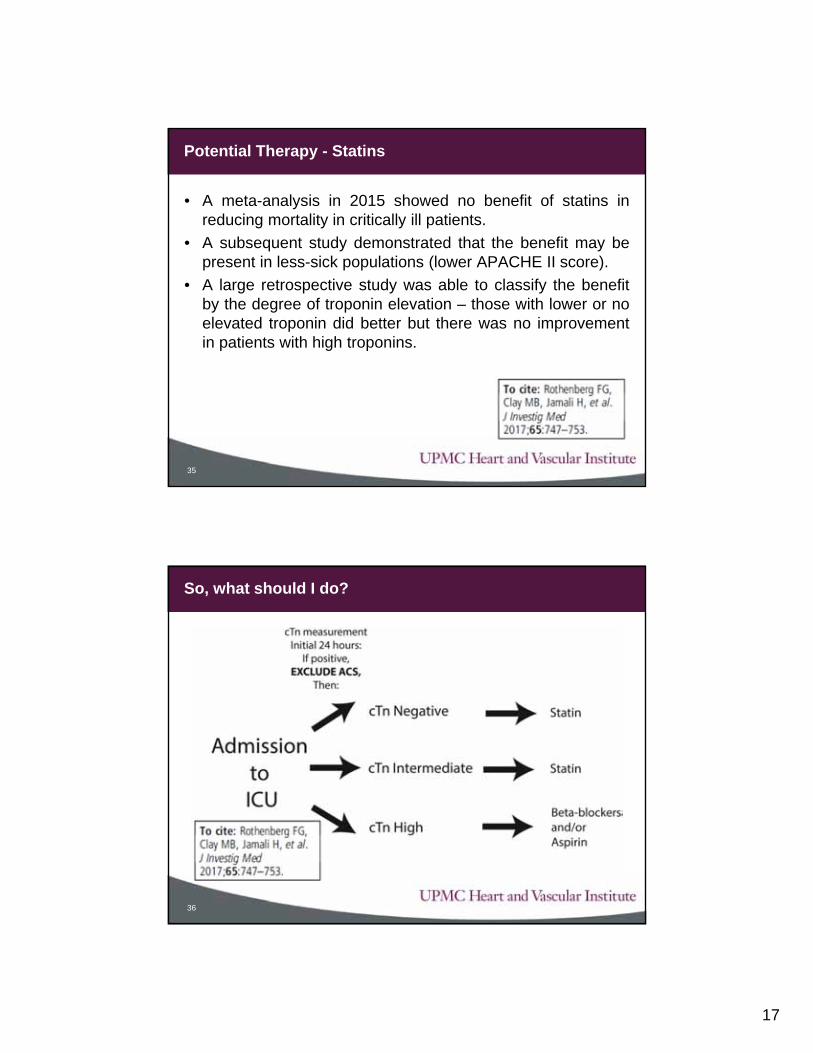
So, what should I do?
36
18
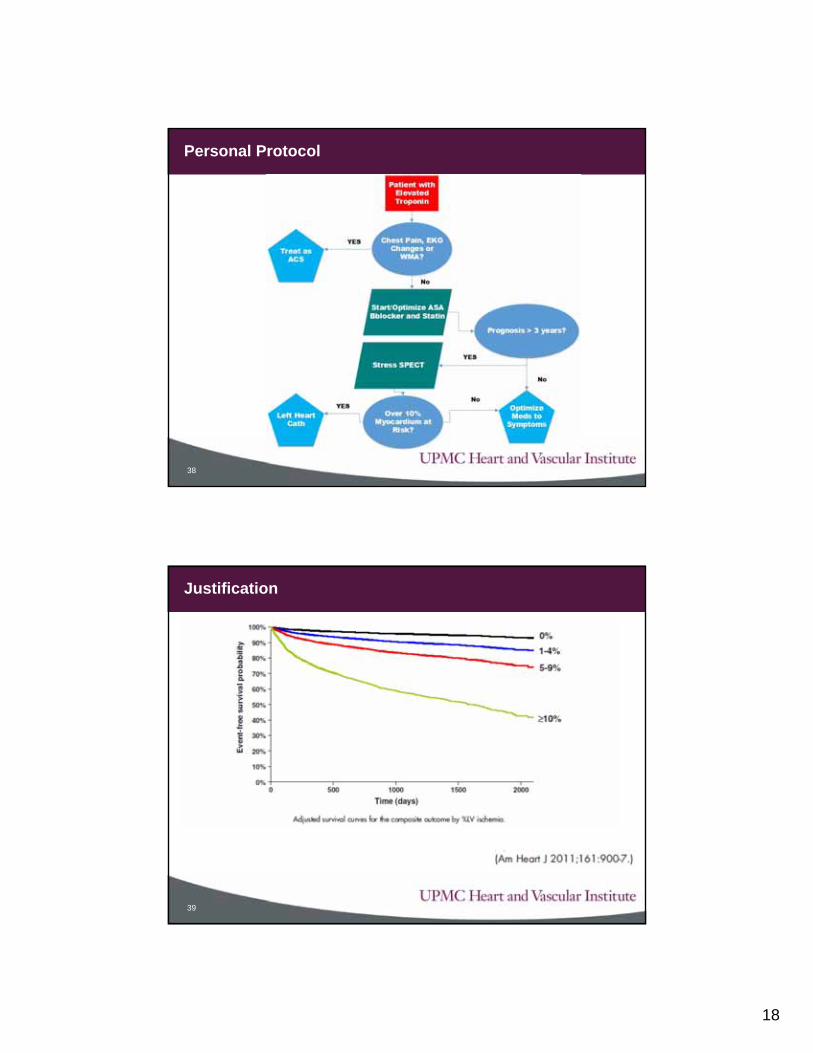
Personal Protocol
38
Justification
39
19
• Management of asymptomatic troponin elevation is challenging with a scant evidence basis compared to ACS.
• The indication to intervene is to make a patient feel better or live longer; when proof is lacking, perhaps doing nothing is better?
• We should be careful of what we call ACS.
Take Home Points
40