Embed Size (px)
Citation preview
A Campaign for Mental Health Under Way at Janssen Research & Development,
One of the Janssen Pharmaceutical Companies of Johnson & Johnson
Kamana Misra PhD, Founding Editor
The economic costs of mental illness will be more than cancer, diabetes, and respiratory ailments
put together. -‐ Tom Insel, Director, U.S. National Institute of Mental Health, at the World
Economic Forum, January 2015
On New Year’s Day the phone call came. A phone call no parent should ever receive. He thought
it was his daughter calling to say hello. Instead a male voice from his daughter’s phone
conveyed hesitantly that his daughter had just tried to end her life.
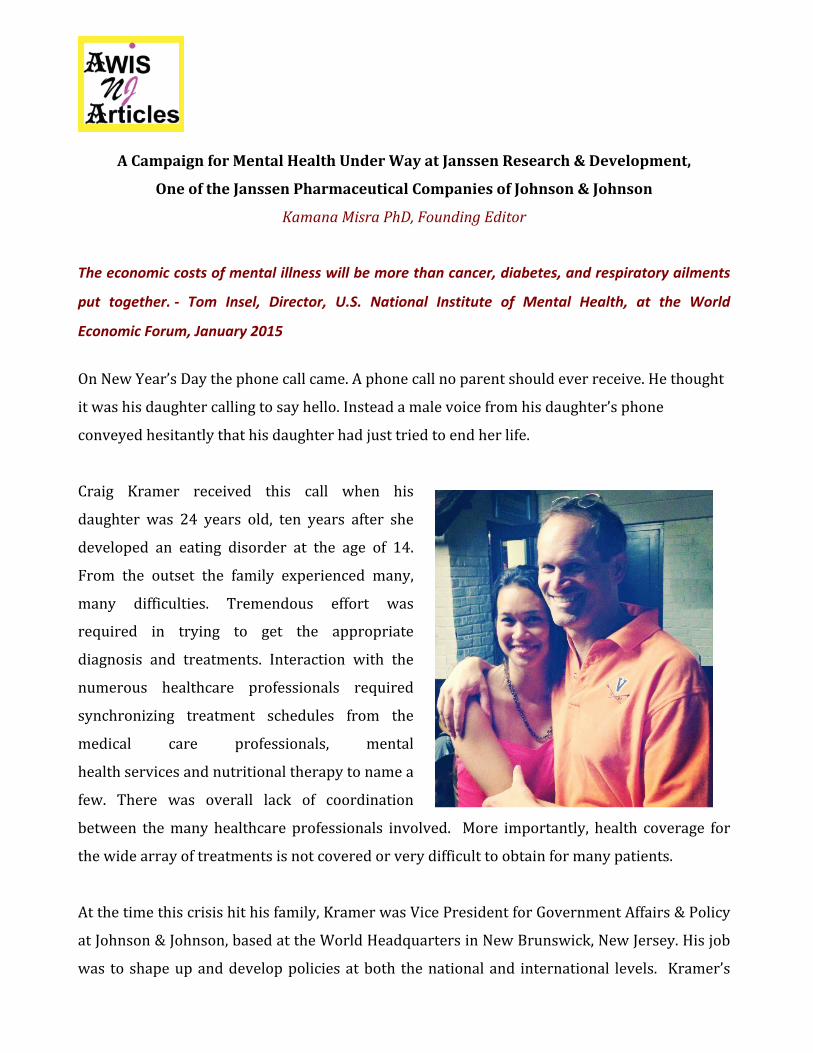
Craig Kramer received this call when his
daughter was 24 years old, ten years after she
developed an eating disorder at the age of 14.
From the outset the family experienced many,
many difficulties. Tremendous effort was
required in trying to get the appropriate
diagnosis and treatments. Interaction with the
numerous healthcare professionals required
synchronizing treatment schedules from the
medical care professionals, mental
health services and nutritional therapy to name a
few. There was overall lack of coordination
between the many healthcare professionals involved. More importantly, health coverage for
the wide array of treatments is not covered or very difficult to obtain for many patients.
At the time this crisis hit his family, Kramer was Vice President for Government Affairs & Policy
at Johnson & Johnson, based at the World Headquarters in New Brunswick, New Jersey. His job
was to shape up and develop policies at both the national and international levels. Kramer’s
personal experience showed him firsthand the sorry state of affairs for eating disorder patients
in terms of diagnosis, prognosis, inadequate insurance coverage, and beyond. He experienced
the tragic effects these disorders have not only on the patients, but also on the families and
communities in which they live and work. Once his daughter was in recovery, he decided to
utilize his expertise to champion a cause that remains gravely misunderstood and
misrepresented.
Kramer was fortunate to work with a company that is
committed to making life-‐changing, long-‐term
differences in human health throughout the world.
Through his efforts and the efforts of other Johnson &
Johnson leaders, the J&J Global Campaign for Mental
Health was initiated as a part of Neuroscience
External Affairs at Janssen Research & Development,
LLC, one of the Johnson & Johnson Pharmaceutical
Companies. Kramer was named Janssen and J&J’s first
Mental Health Ambassador and now leads an effort
that aims to transform mental healthcare globally by
raising awareness, reducing stigma, promoting
research, improving access, and ensuring better
patient outcomes. The Janssen R&D Neuroscience
Therapeutic Area, under the leadership of psychiatrist
and neuroscientist Husseini Manji, is leading new research areas to uncover the causes and
potential treatments for illnesses like treatment-‐resistant depression, suicidality, and other
mental illnesses.
Key initiatives on the mental health policy front include a global leaders' coalition to advocate
for proven, scalable reforms, and a CEO roundtable to develop "next-‐in-‐class" workplace mental
health practices. In his words, “It’s an uphill task, but there have been many great pilot programs

in recent years around the world. We hope that we can scale those up and advance and
replicatemental health solutions” ”
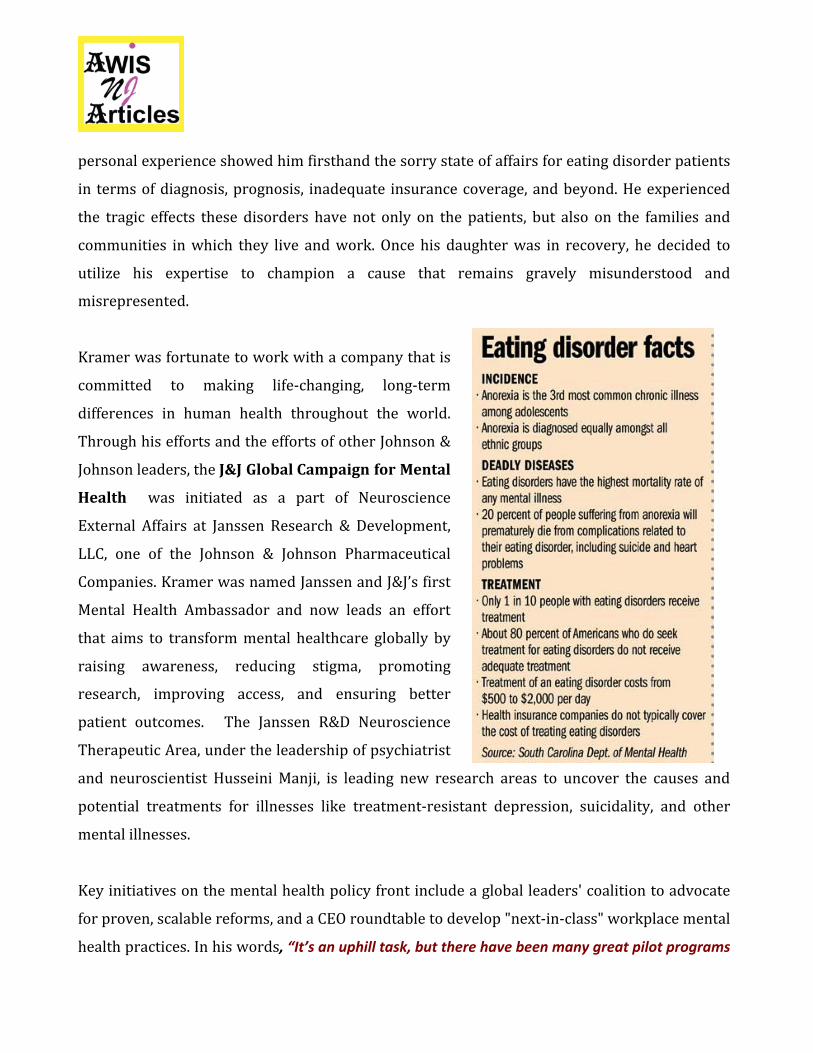
From a societal perspective eating
disorders are the most misunderstood
mental illnesses. These include
indications like anorexia nervosa,
bulimia nervosa, binge-‐eating disorder
and their variants. They are often
perceived with disdain, belittled as a
fad or a “phase”, or deemed a lifestyle
choice, and therefore overlooked as
serious disorders with potentially life-‐
threatening outcomes.
Compounding the misinformation is
the lack of scientific understanding
about mechanisms underlying disease
development and etiology. Fortunately, interest from the scientific community is shedding
some light on the bio-‐psychosocial risk factors associated with eating disorders.
Hunger Circuits.
Under normal conditions, food intake and energy expenditure are balanced by a homeostatic
system that maintains stability of body fat content over time, a biological process termed energy
homeostasis. Pathological disruption of these basic homeostasis and emergency circuits leads to
eating disorders like anorexia (1-‐4). Research efforts over the past 75 years have helped
neuroscientists to identify the involvement of the hypothalamus in controlling eating behavior.
The arcuate region of the hypothalamus (ARC) along with the CGRP neurons in the parabrachial
nucleus (PBN) regions of the brain play important roles in these hunger circuits. A simplified
hunger /feeding circuit depends on:
Haijiang Cai, Ph.D Assistant Professor, Dept. of Neuroscience, BIO5 Institute, University of Arizona.
Anorexia is a serious disorder with abnormal feeding behavior. Neural circuits control both the feeding defects and the underlying emotional behavior. These circuits could be druggable targets for therapy, but we don't know the complete details of these neural circuits. Technological progress in the last decade or so has allowed us to dissect the neural circuits at specific cell type levels, and we are beginning to understand how the circuits mediate eating disorder behavior. I believe we are closer, maybe a few decades (or shorter) away from understanding anorexia (and other eating disorders) at the neural circuits level, or a level that we can treat the disease.”
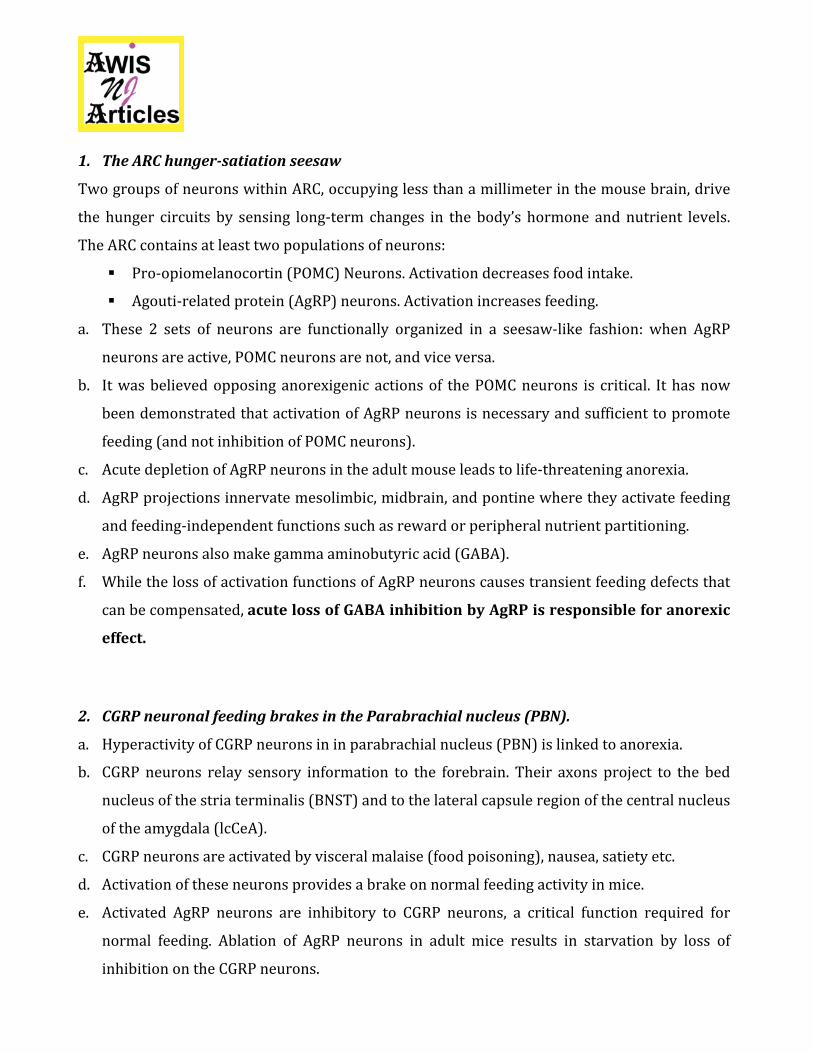
1. The ARC hunger-‐satiation seesaw
Two groups of neurons within ARC, occupying less than a millimeter in the mouse brain, drive
the hunger circuits by sensing long-‐term changes in the body’s hormone and nutrient levels.
The ARC contains at least two populations of neurons:
§ Pro-‐opiomelanocortin (POMC) Neurons. Activation decreases food intake.
§ Agouti-‐related protein (AgRP) neurons. Activation increases feeding.
a. These 2 sets of neurons are functionally organized in a seesaw-‐like fashion: when AgRP
neurons are active, POMC neurons are not, and vice versa.
b. It was believed opposing anorexigenic actions of the POMC neurons is critical. It has now
been demonstrated that activation of AgRP neurons is necessary and sufficient to promote
feeding (and not inhibition of POMC neurons).
c. Acute depletion of AgRP neurons in the adult mouse leads to life-‐threatening anorexia.
d. AgRP projections innervate mesolimbic, midbrain, and pontine where they activate feeding
and feeding-‐independent functions such as reward or peripheral nutrient partitioning.
e. AgRP neurons also make gamma aminobutyric acid (GABA).
f. While the loss of activation functions of AgRP neurons causes transient feeding defects that
can be compensated, acute loss of GABA inhibition by AgRP is responsible for anorexic
effect.
2. CGRP neuronal feeding brakes in the Parabrachial nucleus (PBN).
a. Hyperactivity of CGRP neurons in in parabrachial nucleus (PBN) is linked to anorexia.
b. CGRP neurons relay sensory information to the forebrain. Their axons project to the bed
nucleus of the stria terminalis (BNST) and to the lateral capsule region of the central nucleus
of the amygdala (lcCeA).
c. CGRP neurons are activated by visceral malaise (food poisoning), nausea, satiety etc.
d. Activation of these neurons provides a brake on normal feeding activity in mice.
e. Activated AgRP neurons are inhibitory to CGRP neurons, a critical function required for
normal feeding. Ablation of AgRP neurons in adult mice results in starvation by loss of
inhibition on the CGRP neurons.
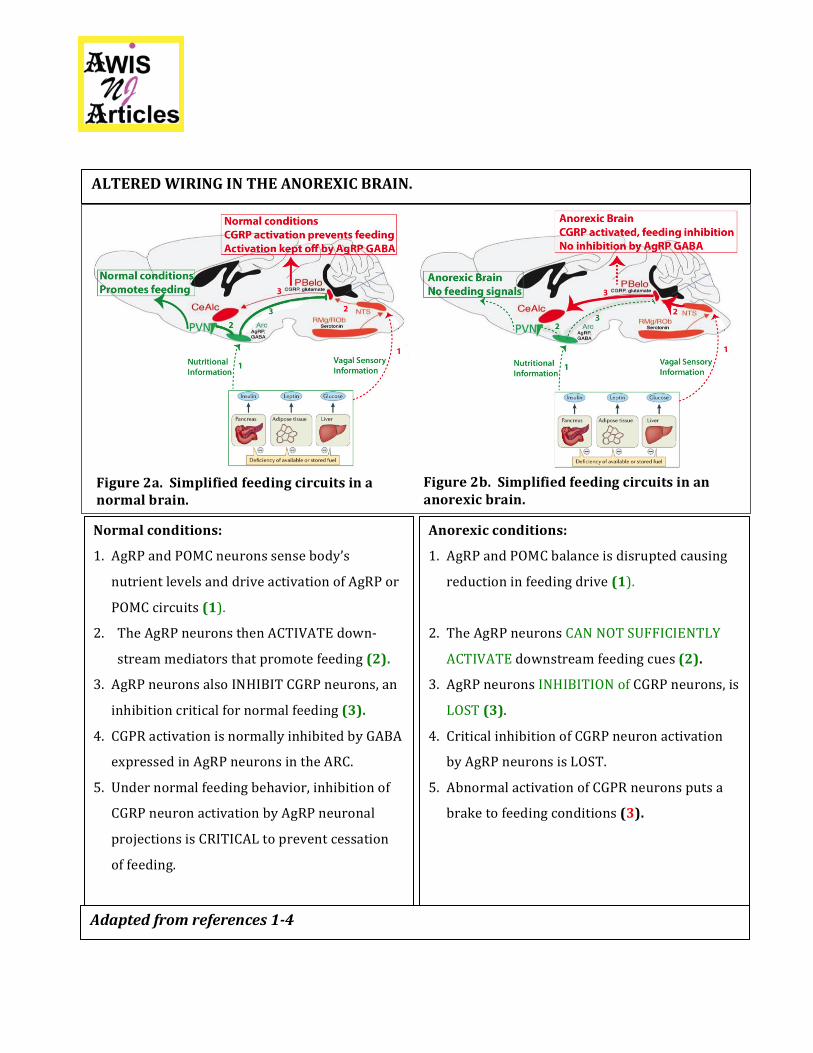
Figure 2b. Simplified feeding circuits in an anorexic brain.
Anorexic conditions:
1. AgRP and POMC balance is disrupted causing
reduction in feeding drive (1).
2. The AgRP neurons CAN NOT SUFFICIENTLY
ACTIVATE downstream feeding cues (2).
3. AgRP neurons INHIBITION of CGRP neurons, is
LOST (3).
4. Critical inhibition of CGRP neuron activation
by AgRP neurons is LOST.
5. Abnormal activation of CGPR neurons puts a
brake to feeding conditions (3).
Figure 2a. Simplified feeding circuits in a normal brain.
ALTERED WIRING IN THE ANOREXIC BRAIN.
Adapted from references 1-‐4
Normal conditions:
1. AgRP and POMC neurons sense body’s
nutrient levels and drive activation of AgRP or
POMC circuits (1).
2. The AgRP neurons then ACTIVATE down-‐
stream mediators that promote feeding (2).
3. AgRP neurons also INHIBIT CGRP neurons, an
inhibition critical for normal feeding (3).
4. CGPR activation is normally inhibited by GABA
expressed in AgRP neurons in the ARC. 5. Under normal feeding behavior, inhibition of
CGRP neuron activation by AgRP neuronal
projections is CRITICAL to prevent cessation
of feeding.
Although there is some progress in the field of eating disorder research, funding still remains
inadequate. To put it into perspective, compare dollars spent per patient supporting research
for eating disorders to dollars spent on autism and bipolar disorder 5:
• $0.74 cents for eating disorders
• $34.07 for autism
• $37.78 for bipolar disorder
The stigma and low public awareness are grave issues that slow down progress. We must work
together as a scientific community to change public perception and call for increased research
funding.
Kramer’s daughter Katharine’s story on personal struggles and inspiring recovery
fromanorexia can be found here.
“Mental illnesses occur more frequently, affect more people, require more prolonged treatment,
cause more suffering by the families of the afflicted, waste more of our human resources, and
constitute more financial drain upon both the public treasury and the personal finances of the
individual families than any other single condition.” -‐ John F. Kennedy, February 5, 1963.
REFERENCES:
1. Morton GJ, Meek, TH and Schwartz MW (2014) Neurobiology of food intake in health and disease.
Nat Rev Neurosci; 15(6):367–378.
2. Wu Q. Clark MS and Palmiter RD (2012). Deciphering a neuronal circuit that mediates loss of
appetite. Nature; 483(7391): 594–597.
3. Padilla SL, Qiu J, Soden ME, -‐-‐-‐ and Palmiter RD (2016) Agouti-‐related peptide neural circuits
mediate adaptive behaviors in the starved state. Nat Neurosci;19(5):734-‐41.
4. Meng F, Han Y, Srisai D, Belakhov V, Farias M, Xu Y, Palmiter RD, Baasov T, Wu Q (2016). New
inducible genetic method reveals critical roles of GABA in the control of feeding and metabolism.
Proc Natl Acad Sci;113(13):3645-‐50.
5. http://www.precisionnutrition.com/all-‐about-‐disordered-‐eating