-
The American Journal of Surgery (2014) 208, 690-694
Surgical Education
A better way to teach knot tying: a randomizedcontrolled trial
comparing the kinesthetic andtraditional methods
Emily Huang, M.D., M.Ed.a,*, Hueylan Chern, M.D., FACSa,Patricia
OSullivan, Ed.D.b, Brian Cook, B.S.c, Erik McDonald, B.S.c,Barnard
Palmer, M.D., M.Ed.d, Terrence Liu, M.D., FACSd,Edward Kim, M.D.,
FACSa
aDepartment of Surgery, University of California San Francib
sco, San Francisco, 513 Parnassus Avenue,S-321, San Francisco,
CA 94143-0470, USA; Department of Medicine, University of
California SanFrancisco, San Francisco, CA, USA; cSchool of
Medicine, University of California San Francisco, SanFrancisco, CA,
USA; dDepartment of Surgery, University of California San
Francisco-East Bay,Oakland, CA, USA
KEYWORDS:Surgical education;Knot
tying;Kinesthetic;Technical;Skill;Basic skills
There were no relevant financial rela
The authors declare no conflicts of i
This manuscript is not submitted els
Abstract presented at the Northern C
Investigation or Education Research Aw
* Corresponding author. Tel.: 11-60E-mail address:
emily.huang2@ucsfm
Manuscript received February 25, 20
0002-9610/$ - see front matter
2014http://dx.doi.org/10.1016/j.amjsurg.20
AbstractBACKGROUND: Knot tying is a fundamental and crucial
surgical skill. We developed a kinesthetic
pedagogical approach that increases precision and economy of
motion by explicitly teaching suture-handling maneuvers and studied
its effects on novice performance.
METHODS: Seventy-four first-year medical students were
randomized to learn knot tying via either thetraditional or the
novel kinesthetic method. After 1 week of independent practice,
students were videotapedperforming 4 tying tasks. Three raters
scored deidentified videos using a validated visual analog scale.
Thegroups were compared using analysis of covariance with practice
knots as a covariate and visual analog scalescore (range, 0 to 100)
as the dependent variable. Partial eta-square was calculated to
indicate effect size.
RESULTS: Overall rater reliability was .92. The kinesthetic
group scored significantly higher thanthe traditional group for
individual tasks and overall, controlling for practice (all P ,
.004). The kines-thetic overall mean was 64.15 (standard deviation
5 16.72) vs traditional 46.31 (standard deviation 516.20; P , .001;
effect size 5 .28).
CONCLUSIONS: For novices, emphasizing kinesthetic suture
handling substantively improved per-formance on knot tying. We
believe this effect can be extrapolated to more complex surgical
skills. 2014 Elsevier Inc. All rights reserved.
tionships or any sources of support in the form of grants,
equipment, or drugs.
nterest.
ewhere for publication.
alifornia Chapter of the ACS Annual Meeting in San Francisco,
CA, on June 8, 2013, and won a Best Clinical
ard. Abstract presented at the ACS Annual Clinical Congress in
Washington, DC, on October 8, 2013.
9-936-0827; fax: 11-415-502-1259.edctr.org
14; revised manuscript April 7, 2014
Elsevier Inc. All rights reserved.
14.05.028
Delta:1_given nameDelta:1_surnameDelta:1_given
nameDelta:1_surnameDelta:1_given nameDelta:1_surnameDelta:1_given
nameDelta:1_surnamemailto:[email protected]://crossmark.crossref.org/dialog/?doi=10.1016/j.amjsurg.2014.05.028&domain=pdfhttp://dx.doi.org/10.1016/j.amjsurg.2014.05.028http://dx.doi.org/10.1016/j.amjsurg.2014.05.028
-
E. Huang et al. A better way to teach knot tying 691
Surgical knot tying is almost always the first technical
relative lengths to change. The tail end of the suture
skill a surgical learner is requested to perform in theoperating
room. Learners approach this moment withexcitement and trepidation,
as the moment when theytransition from being observers of surgery
to beingparticipants. For the learner (and the patient), this is
alsoa high-stakes event: Demonstration of competence (orfailure)
both reflects on the learners capacities and affectsfuture
participation opportunities in the operating room,whereas the
performance of the knot-tying act affects, inhowever small a
measure, the patients actual surgicaloutcome. Optimally, preparing
learners to perform basicsurgical skills such as knot tying in vivo
is thus animportant goal of any basic surgical education program.1
To address this goal, programs have made significantefforts to
incorporate more basic surgical skills training intoundergraduate
medical education and early residencytraining,2 as well as to
standardize curricular materials andinstructional pedagogies.3
Physical resource and time limita-tions in the form of duty-hours
restrictions have alsocompelled considerable changes in graduate
medical educa-tion over the last decade, necessitating development
of waysto efficiently train surgical learners.4 Against the
backdrop ofthis complex environment, the humble surgical knot
providesa perfect focus for beginning to understand and improve
theways in which we think about teaching surgery.
Surgical knots must be of high quality to securely
bindstructures. A less obvious principle, particularly to
novices,is that knots are simply the products of a process thatmust
be executed with great precision and finesse. If asurgeon avulses a
blood vessel in the process of ligating itby erratically pulling on
the sutures, he has entirelydefeated the purpose of the knot.
Surgical educationalmaterials have always emphasized the steps of
the process,showing pictures of the spatial configuration of the
handsand suture ends as a knot is formed, as well as the
product,usually highlighting the final appearance of a square
knot.5
How to form these spatial configurations in an atrau-matic
manner is a matter of kinesthetics: finely attunedawareness of
sensory input and control of motor outputthat is akin to body
positioning and balance in sports.Expert surgeons intuitively
perform suture-handling ma-neuvers to tie knots fluidly, but
novices cannot learn thesemaneuvers without explicit instruction.
An analysis ofnovice knot-tying errors by Rogers et al6 provides
vividillustration of this fact. They identified 4 common
beginnererrors (frequency):
1. Too much motion in right hand (38%),2. Failure to maintain
consistent tension (17%),3. Hands too close to knot (13%), and4.
Failure to cross hands (7%).
Most of these errors stem from a single root cause:failure to
obtain and then maintain a comfortable workingdistance from the
knot. For example, novices often hold thesuture ends too loosely
and slide up on them, causing their
becomes too short to easily loop into knots, which results
infumbling, uneven tension, and the use of extra fingers toform the
loop (the 2 most frequent errors, as observed byRogers et al6). By
teaching some key suture-handling ma-neuvers (gathering, sliding,
and locking) and emphasizingkinesthetic awareness, we address these
root causes of errorand teach trainees to establish and maintain an
ideal,balanced position from which it is easy to tie knotssmoothly
without excessive or erratic lifting, fumbling,and dropping of
suture.
The kinesthetic curriculum7 incorporates a clear andconcise
practical glossary to improve communication be-tween instructors
and students and builds up on basicsuture-handling (pretying)
maneuvers to show learnersnot only how to tie a knot but also how
to manipulate the su-ture to lay it down precisely. The teaching
manual andaccompanying video provide step-by-step instructions
withspecific attention to the relevant details of setup,
technique,and recovery. Because the method aligns with principles
ofcognition for deliberate practice in the acquisition of
tech-nical skills,810 we postulated that emphasizing
kinestheticsuture handling would improve performance on knot
tying,even over a very short instructional time. Furthermore,
webelieve that focusing on teaching kinesthetics in surgerycan help
trainees improve technical performance even onmore advanced
surgical skills. Therefore, we undertookthis study to compare
novice learners instructed using tradi-tional versus kinesthetic
methods.
Methods
We recruited first-year medical students from theUniversity of
California, San Francisco (UCSF) School ofMedicine to participate
in this randomized controlled studyas part of a basic surgical
skills elective. The study wasperformed under an institutional
review boardexemptedprotocol. None of the students had any prior
experience inknot tying or other surgical skills. The individual
studentswere randomly assigned to 1 of the 2 groups: learning to
tiesurgical knots via the traditional or kinestheticmethods before
beginning the elective.
All students attended a 2-hour knot-tying teaching sessionin the
Surgical Skills Center with expert faculty instructorswho had
previously been identified as strong teachers. Thetraditional
method group was taught by faculty who hadnever previously been
exposed to the kinesthetic method toavoid any potential bias, and
followed teaching principlesfrom the American College of Surgeons
Surgical SkillsCurriculum for Residents.5 The kinesthetic method
groupwas taught by faculty familiar with the kinesthetic method,and
followed kinesthetic teaching principles.7 Both groupsreceived the
same amount of face-to-face instructionaltime, and the average
instructor to student ratio was 1:6. Af-ter the initial
instructional session, students were providedwith links to
instructional YouTube videos to promote
-
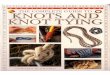
Figure 1 Knot-tying tasks. Clockwise from top left: tying at
surface, tying at depth, atraumatic tie, and square knot.
692 The American Journal of Surgery, Vol 208, No 4, October
2014
deliberate practice at home.11,12 Students in the
traditionalmethod group were directed to a video using the
traditionalmethod, whereas students in the kinesthetic method
groupwere directed to the video A Kinesthetic Curriculum
forTeaching Knot Tying by UCSF Surgical Skills Center.13
All students were given a package of 2-0 silk sutures forhome
practice and required to save and submit at least 8 cmof practice
knots at the second session 2 weeks later, tocontrol for variable
practice. During the second session inthe skills laboratory,
students were given approximately10 minutes to warm up and then
videotaped while perform-ing 4 tasks designed to simulate real
situations in theoperating room (Fig. 1).
(1) Tying at surface: students tied 6 throws onto a Pen-rose
drain attached to a tying board; students were al-lowed to throw
hitches or square knots.
(2) Tying at depth: students tied 6 throws onto a hook in-side a
cup, designed to simulate tying in a hole inthe operating room.
(3) Atraumatic tying: students tied 6 throws onto a rubberband
looped around a regular metal spoon, with thegoal of not moving the
spoon at all.
(4) Square knot: students tied 6 throws onto a Penrosedrain
attached to a tying board; knots had to liedown square.
During the assessment session, trained observers re-corded knot
quality (ie, the knot securely binds the tiedstructure, all throws
are laid down securely with no airknots) as adequate or not
adequate.
All videos were deidentified and then scored by 3 UCSFsurgical
faculty raters using a visual analog scale for globalrating. Raters
were blinded to the randomization, and
furthermore, none of the raters were aware of the contentof the
kinesthetic curriculum to prevent bias based on anyobservable
characteristic maneuvers. The raters were askedto provide a global
score (0 to 100 points by placing amarker along the visual analog
scale) considering bothoverall performance (poor to excellent) and
their likelihoodof allowing this student to tie knots in their
operating room(unlikely to likely).
Data from the kinesthetic and traditional method groupswere
analyzed in 2 ways. First, the 2 groups were comparedusing t tests
for each task. Second, the 2 groups werecompared using an analysis
of covariance, with submittedpractice knot length as a covariate to
control for practice,and the averaged score (0 to 100) for the 3
raters as thedependent variable. Partial eta-square was calculated
toindicate overall effect size (ES). For each task, wecompared the
2 groups using a t test and calculated theES using the Cohen d.14
We also compared knot quality be-tween the 2 groups using the
chi-square statistic.
Results
Seventy-four students agreed to participate and 70completed the
full study (37 in the traditional methodgroup and 33 in the
kinesthetic method group). Using 3raters, we had a reliable measure
with an interclasscorrelation coefficient of .92. Practice, as
indicated bylength of knots tied, was not significantly different
betweenthe traditional and kinesthetic method groups (31.4 cm;SD 5
14.4 vs 28.6 cm, SD 5 12.6; P 5 .55).
The kinesthetic method group scored significantlyhigher than the
traditional method group on each individual
-
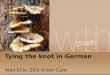
Figure 2 Postintervention performance on individual
knot-tyingtasks: kinesthetic and traditional method groups.
E. Huang et al. A better way to teach knot tying 693
task (Fig. 2). All P values were less than .004 and
ESs,calculated using the Cohen d were between .32 and
.52(moderate). Overall, when controlling for practice,
thekinesthetic method was more effective than the traditionalwhen
averaging across all tasks (P , .001; Fig. 3). OverallES,
calculated using eta-square and adjusted for practice,was .28
(small-moderate).
Knot quality, as assessed by trained observers, was
notsignificantly different between the 2 groups except in the
taskof tying at depth, where the kinesthetic method groupperformed
significantly better (79% vs 54% of students tyingadequate knots;
P5 .03). Knot quality was acceptable overall.
Comment
Novices learning to tie surgical knots via the kines-thetic
method performed significantly better than theirpeers. This effect
was seen despite the very limitedinstructional time (2 hours) and
practice time (2 weeks).We found the greatest difference between
the 2 groups inthe task of tying at depth, a common scenario
encounteredin the operating room. The apparatus used to simulate
thissituation (a hook inside a cup) was only 1 inch deep, very
Figure 3 Mean postintervention performance across 4 knot-tying
tasks: kinesthetic and traditional method groups.
similar to depths trainees might encounter in basicprocedures
such as an inguinal hernia repair. The kines-thetic method group
performed comparatively better onthis task, both on global
assessment of videotaped perfor-mance and assessment of knot
quality. We postulate thatthis is because tying at depth is a skill
that requiresincreased dexterity in handling the additional length
ofsuture, precisely the skill component that the kinestheticmethod
emphasizes.
The kinesthetic group also performed better on tyingsquare knots
despite having less instructional time specif-ically devoted to
teaching square knots. During the teach-ing session, the
kinesthetic group initially focused onsuture manipulation and
practiced tying half-hitch knots.Only after demonstration of
rudimentary proficiency withthe half-hitch knot was the square knot
introduced near theend of the session. In contrast, the traditional
groupsprimary learning goal from the beginning was to tie
squareknots. That the kinesthetic group performed better onsquare
knots further supports the argument that carefulsuture manipulation
and creation of an optimal workingdistance are the fundamental
underpinnings of all knottying.
The key elements of the kinesthetic curriculumdgather-ing,
sliding, and lockingdare not novel. In fact, most of us,if not all,
use these very maneuvers when we tie knots in theoperating room.
What is novel and effective about thekinesthetic method, as
demonstrated in this study, is that forthe first time, we present
the learner with a complete andaccurate description of how surgeons
tie knots.
According to the Fitts and Posner theory on skillacquisition,
during the cognitive (beginning) stage oflearning, the novice needs
to understand how to performthe task. Without this solid
foundational understanding,learners may spend more time in the
associative (second)stage, and through many hours of practice,
trial, and error,they may eventually reach the autonomous (final)
stage.10
In the case of knot tying, most trainees will pick upthe skills
of suture handling over months or years withcontinued practice and
exposure. However, given the cur-rent external pressures faced by
surgical education, thistype of inefficiency in teaching is no
longer an affordableluxury if our trainees are to maximize their
participationand learning in the operating room.
A potential point of concern may be the emphasis placedon
teaching the half-hitch knot, also known as a slip knot.Effective
instruction in every technical discipline fromsports to music
follows a logical progression from simple tocomplex tasks. The half
hitch is a simple knot that requiresone to alternate only the
orientation of the loop with eachknot. This allows learners to hone
their skills of suturemanipulation and rotation of the wrist to
form knots. Thesquare knot has an added layer of complexity because
itrequires one to orient the sutures in a specific sequence andto
pull them in equal and opposite directions. As the resultsof our
study show, learners who follow a progression fromhalf-hitch knot
to square knot fare better than those who
-
694 The American Journal of Surgery, Vol 208, No 4, October
2014
start with the more difficult square knot, which often leadsto
cognitive overload.
One could also make the contention that the gatheringmaneuver is
important for tying at depth, amore advanced skill,and that its
omission from introductory traditional knot-tyingcurriculum is
appropriate. However gathering is necessaryfor much more than just
tying at depth, it is also essential forcontrolling relative suture
lengths and creating optimal workingdistances. We should also
distinguish tying in a truly deepspace, such as the pelvis, from
tying in a shallow cavity. Thelatter is a skill required even for
novices. Our apparatus fortying at depth replicated typical depths
seen in basic pro-cedures. Even at a depth of an inch, gathering
was necessary.
The last obvious limitation of this study is the shortduration
of instruction and limited assessment of learners.Long-term
retention of skills and degree of transfer into theactual operating
room are unproven. The full impact of thekinesthetic method as part
of a longitudinal curriculumremains to be demonstrated. However, we
believe that theeffect seen here would likely be enhanced by
deliberatepractice over a longer period of time.
In the context of the bigger picture of surgical education,our
experience with teaching surgical knot tying has promptedus to
focus on the details of how we teach and to be aware ofthe
unconscious competence that characterizes the expertblind spot.15
Although many tasks may simply require repet-itive practice and
exposure, there may be opportunities for sig-nificant improvement
in the quality of instruction through amore careful analysis of the
key steps and guiding principles.
Acknowledgment
The authors would like to acknowledge and thank WendyFong,
Operations Manager at the UCSF Surgical SkillsCenter, for her
technical assistance in conducting this study.
References
1. Scott DJ, Dunnington GL. The new ACS/APDS skills
curriculum:
moving the learning curve out of the operating room. J
Gastrointest
Surg 2008;12:21321.
2. Cosman P, Hemli JM, Ellis AM, et al. Learning the surgical
craft: a
review of skills training options. ANZ J Surg 2007;77:83845.
3. Sanfey H, Ketchum J, Bartlett J, et al. Verification of
proficiency in basic
skills for postgraduate year 1 residents. Surgery
2010;148:75967.
4. Reznick RK, MacRae H. Teaching surgical skillsdchanges in
the
wind. N Engl J Med 2006;355:26649.
5. Rogers DA, Ketchum J. Knot tying. In: ACS/APDS Surgical
Skills
Curriculum for Residents: Phase 1. Available at:
http://elearning.
facs.org/course/view.php?id53. Accessed June 30, 2014.6. Rogers
DA, Regehr G,MacDonald J. A role for error training in surgical
technical skill instruction and evaluation. Am J Surg
2002;183:2425.
7. Kim E, Chern H, Huang E, et al. How to Teach Knot Tying: A
Kinesthetic
Approach. MedEdPORTAL; 2013. Available at:
www.mededportal.org/
publication/9328. Accessed June 30, 2014.
8. Dreyfus SE, Dreyfus HL. A five-stage model of the mental
activities
involved in directed skill acquisition. California: University
of Califor-
nia Berkeley Operations Research Center; 1980.
9. Ericsson KA, Krampe RT, Tesch-Romer C. The role of deliberate
prac-
tice in the acquisition of expert performance. Psychol Rev
1993;100:
363406.
10. Fitts PM, Posner MI. Human Performance. Oxford: Brooks &
Cole;
1967.
11. Jowett N, LeBlanc V, Xeroulis G, et al. Surgical skill
acquisition with
self-directed practice using computer-based video training. Am J
Surg
2007;193:23742.
12. Xeroulis GJ, Park J, Moulton CA, et al. Teaching suturing
and knot-
tying skills to medical students: a randomized controlled
study
comparing computer-based video instruction and (concurrent and
sum-
mary) expert feedback. Surgery 2007;141:4429.
13. UCSF Surgical Skills Center. A kinesthetic curriculum for
teaching
knot tying. San Francisco, CA. Available at:
http://www.youtube.com/
watch?v5XhTh6ke6mks. Accessed June 30, 2013.14. Cohen J.
Statistical Power Analysis for the Behavioral Sciences. Hill-
sdale, NJ: Lawrence Erlbaum Associates; 1988.
15. Nickerson R. How we knowdand sometimes misjudgedwhat
others
know: imputing ones own knowledge to others. Psychol Bull
1999;
125:73759.
http://refhub.elsevier.com/S0002-9610(14)00367-5/sref1http://refhub.elsevier.com/S0002-9610(14)00367-5/sref1http://refhub.elsevier.com/S0002-9610(14)00367-5/sref1http://refhub.elsevier.com/S0002-9610(14)00367-5/sref2http://refhub.elsevier.com/S0002-9610(14)00367-5/sref2http://refhub.elsevier.com/S0002-9610(14)00367-5/sref3http://refhub.elsevier.com/S0002-9610(14)00367-5/sref3http://refhub.elsevier.com/S0002-9610(14)00367-5/sref4http://refhub.elsevier.com/S0002-9610(14)00367-5/sref4http://elearning.facs.org/course/view.php?id=3http://elearning.facs.org/course/view.php?id=3http://elearning.facs.org/course/view.php?id=3http://refhub.elsevier.com/S0002-9610(14)00367-5/sref6http://refhub.elsevier.com/S0002-9610(14)00367-5/sref6http://www.mededportal.org/publication/9328http://www.mededportal.org/publication/9328http://refhub.elsevier.com/S0002-9610(14)00367-5/sref8http://refhub.elsevier.com/S0002-9610(14)00367-5/sref8http://refhub.elsevier.com/S0002-9610(14)00367-5/sref8http://refhub.elsevier.com/S0002-9610(14)00367-5/sref9http://refhub.elsevier.com/S0002-9610(14)00367-5/sref9http://refhub.elsevier.com/S0002-9610(14)00367-5/sref9http://refhub.elsevier.com/S0002-9610(14)00367-5/sref10http://refhub.elsevier.com/S0002-9610(14)00367-5/sref10http://refhub.elsevier.com/S0002-9610(14)00367-5/sref11http://refhub.elsevier.com/S0002-9610(14)00367-5/sref11http://refhub.elsevier.com/S0002-9610(14)00367-5/sref11http://refhub.elsevier.com/S0002-9610(14)00367-5/sref12http://refhub.elsevier.com/S0002-9610(14)00367-5/sref12http://refhub.elsevier.com/S0002-9610(14)00367-5/sref12http://refhub.elsevier.com/S0002-9610(14)00367-5/sref12http://www.youtube.com/watch?v=XhTh6ke6mkshttp://www.youtube.com/watch?v=XhTh6ke6mkshttp://www.youtube.com/watch?v=XhTh6ke6mkshttp://refhub.elsevier.com/S0002-9610(14)00367-5/sref13http://refhub.elsevier.com/S0002-9610(14)00367-5/sref13http://refhub.elsevier.com/S0002-9610(14)00367-5/sref14http://refhub.elsevier.com/S0002-9610(14)00367-5/sref14http://refhub.elsevier.com/S0002-9610(14)00367-5/sref14A
better way to teach knot tying: a randomized controlled trial
comparing the kinesthetic and traditional
methodsMethodsResultsCommentAcknowledgmentReferences