Embed Size (px)
Citation preview
Krisandra Allen, MPH Foodborne Disease Epidemiology Assistant
Division of Surveillance and Investigation Virginia Department of Health
Field Epidemiology Seminar: April 30, 2013
Understand symptoms, modes of transmission, and epidemiology of hand, foot, and mouth disease (HFMD)
Identify emerging strains of virus causing severe HFMD outbreaks worldwide
Describe the unique epidemiological characteristics of a local outbreak of HFMD
http://www.heraldsun.com.au/news/national/northern-sydney-on-alert-over-virus/story-fndo317g-1226607174917
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6112a5.htm
http://www.familypracticenews.com/news/across-specialties/single-article/emerging-enterovirus-strain-causes-severe-hfmd/4aca5718cf07551663110248e48a4b4d.html
http://tuoitrenews.vn/society/8515/handfootmouth-disease-infects-12400-people-killing-4
http://www.boston.com/dailydose/2012/07/10/can-deadly-form-hand-foot-and-mouth-disease-hit-the/AlPWSYABnUQCfFB77Ug9cP/story.html
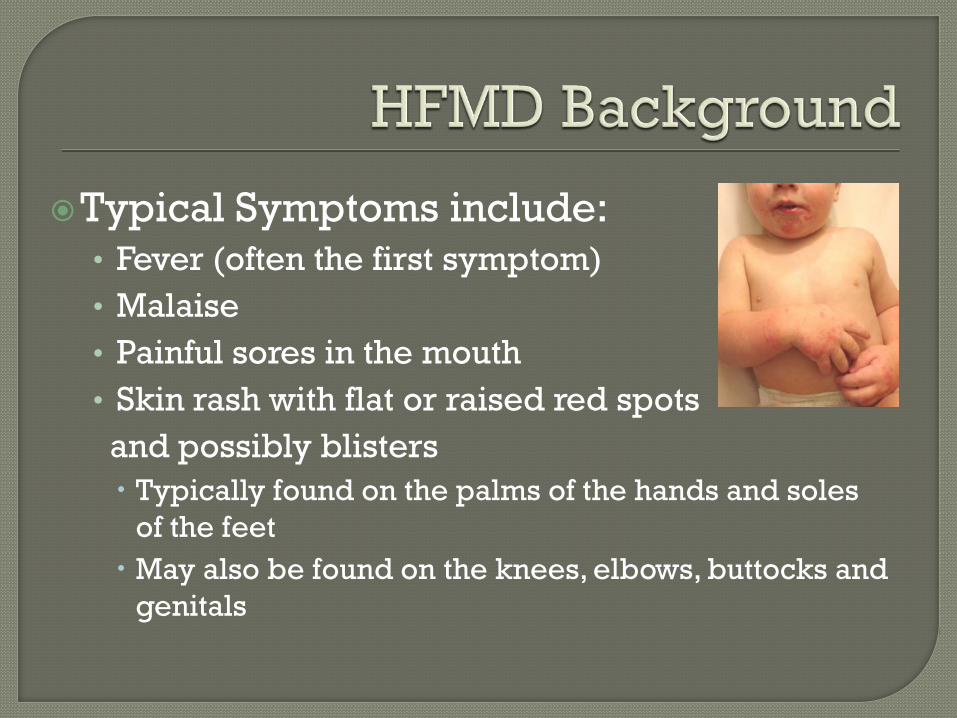
Typical Symptoms include: • Fever (often the first symptom) • Malaise • Painful sores in the mouth • Skin rash with flat or raised red spots and possibly blisters Typically found on the palms of the hands and soles
of the feet May also be found on the knees, elbows, buttocks and
genitals
Incubation period 3-7 days Usually self-limiting and resolves in 7-10
days Modes of transmission include:
• Respiratory secretions – contact and aerosol • Contact with blister fluid • Objects contaminated by feces from infected
individuals
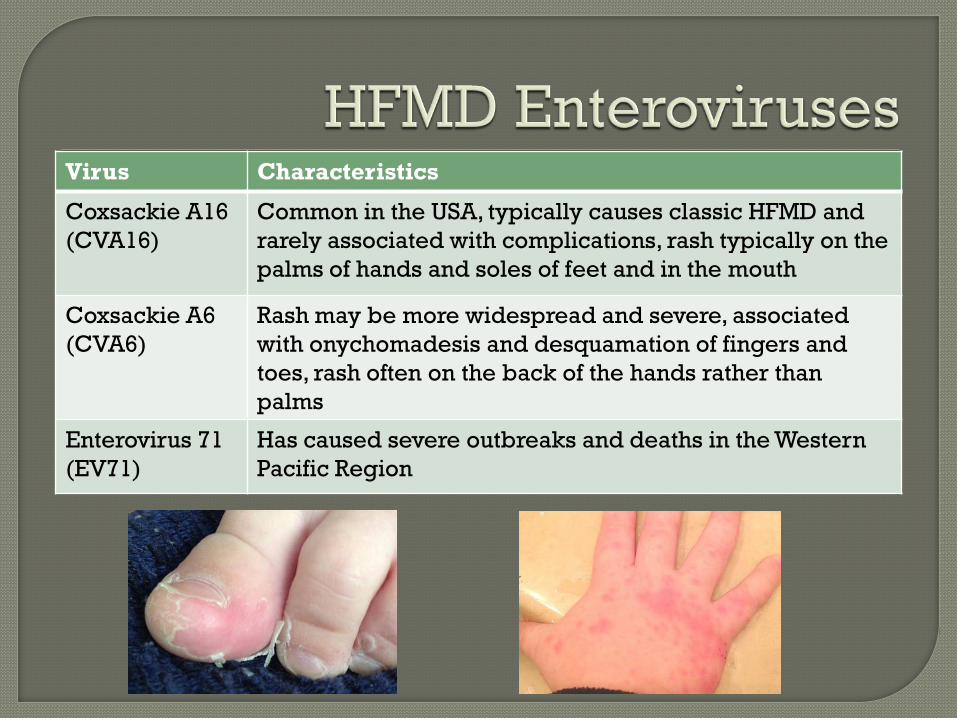
Virus Characteristics
Coxsackie A16 (CVA16)
Common in the USA, typically causes classic HFMD and rarely associated with complications, rash typically on the palms of hands and soles of feet and in the mouth
Coxsackie A6 (CVA6)
Rash may be more widespread and severe, associated with onychomadesis and desquamation of fingers and toes, rash often on the back of the hands rather than palms
Enterovirus 71 (EV71)
Has caused severe outbreaks and deaths in the Western Pacific Region

0
2
4
6
8
10
12
14
16
18
20
2010 2011 2012
Nu
mb
er o
f Rep
orte
d O
utb
reak
s
Year
Number of HFMD Outbreaks Reported to Virginia Department of Health by Setting 2010-2012
School (K-12)
Daycare / Pre-K
College / University
0
1
2
3
4
5
6
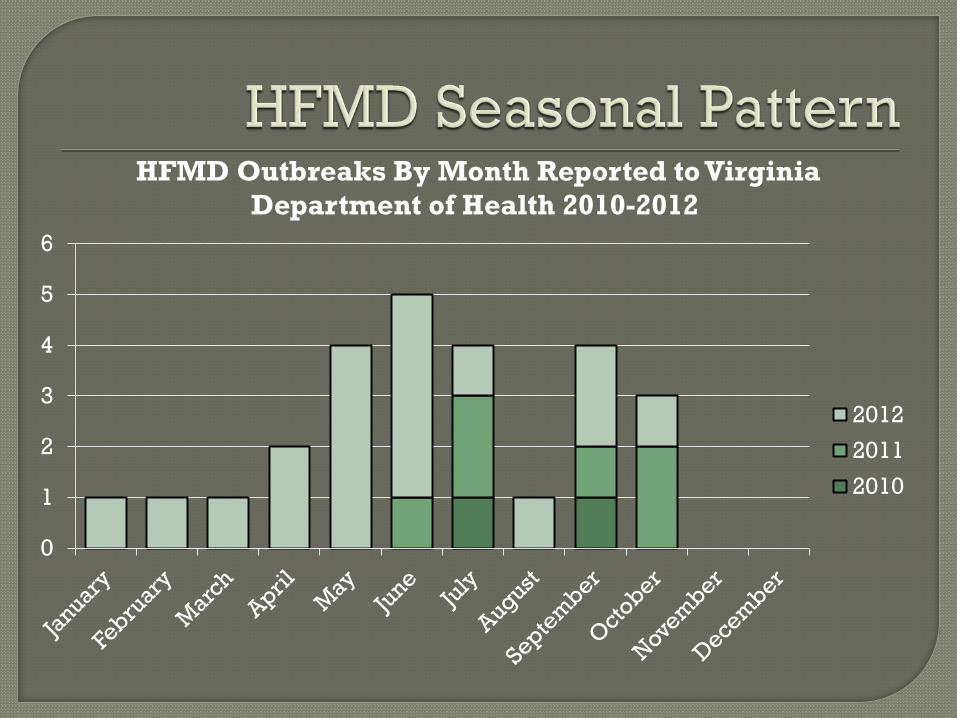
HFMD Outbreaks By Month Reported to Virginia Department of Health 2010-2012
2012
2011
2010
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
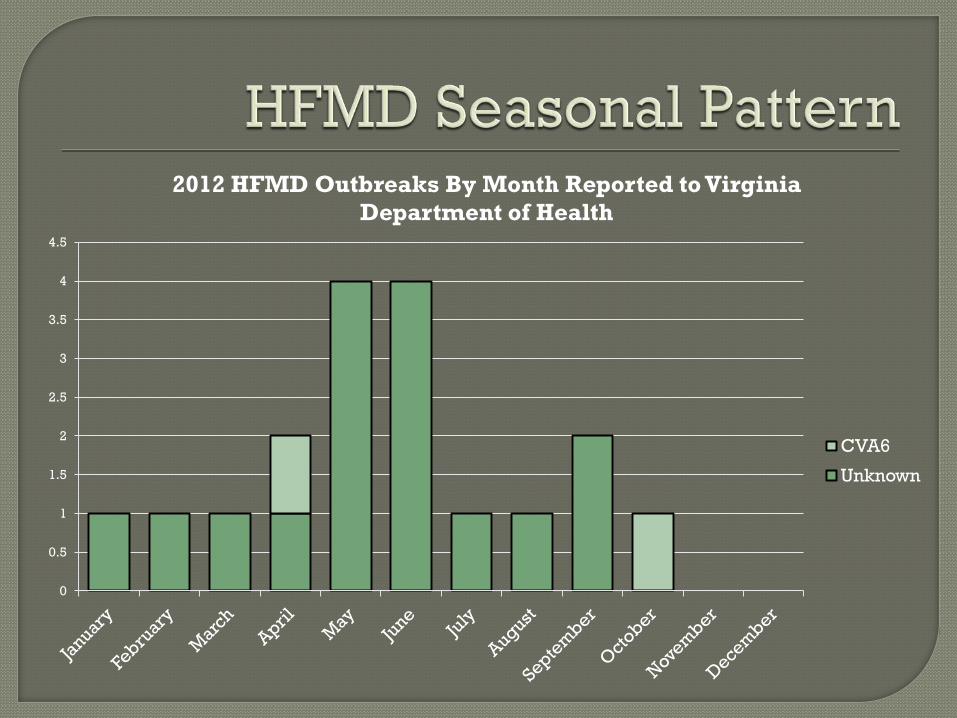
2012 HFMD Outbreaks By Month Reported to Virginia Department of Health
CVA6
Unknown
Piedmont Health District notified in September 2012 by the director of the Student Health Clinic at College A of several students diagnosed with HFMD
Literature review found no previous HFMD outbreaks in a College setting
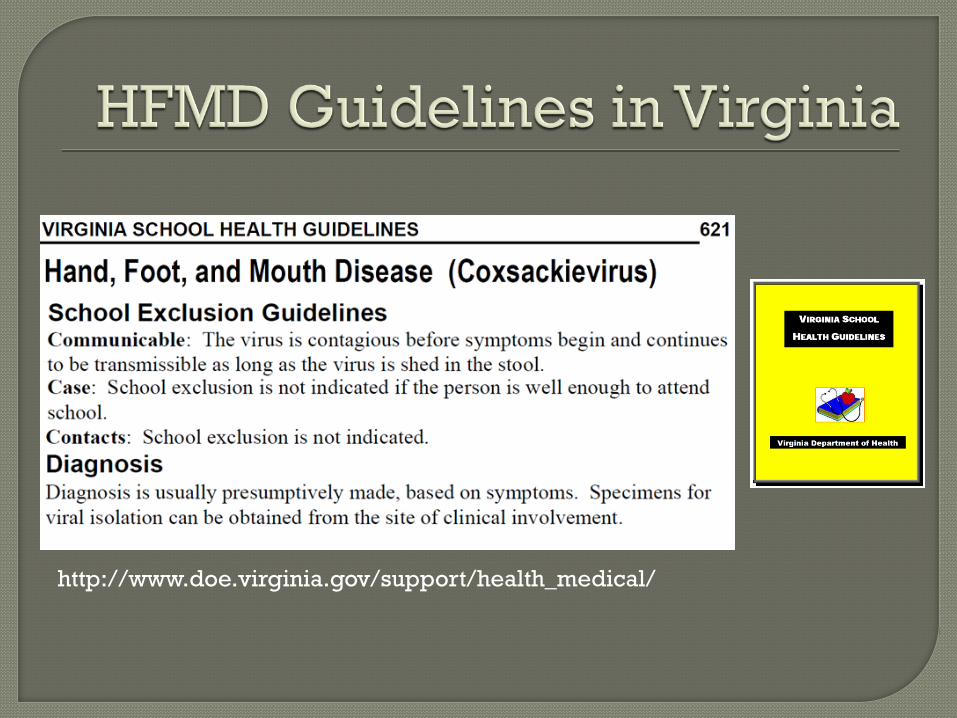
http://www.doe.virginia.gov/support/health_medical/
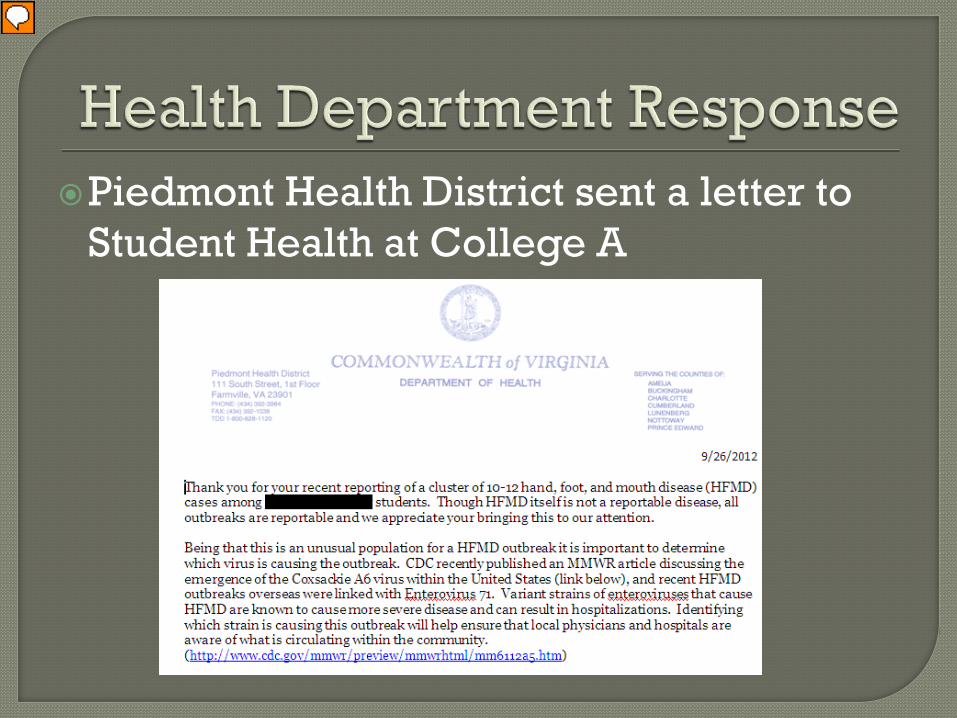
Piedmont Health District sent a letter to Student Health at College A
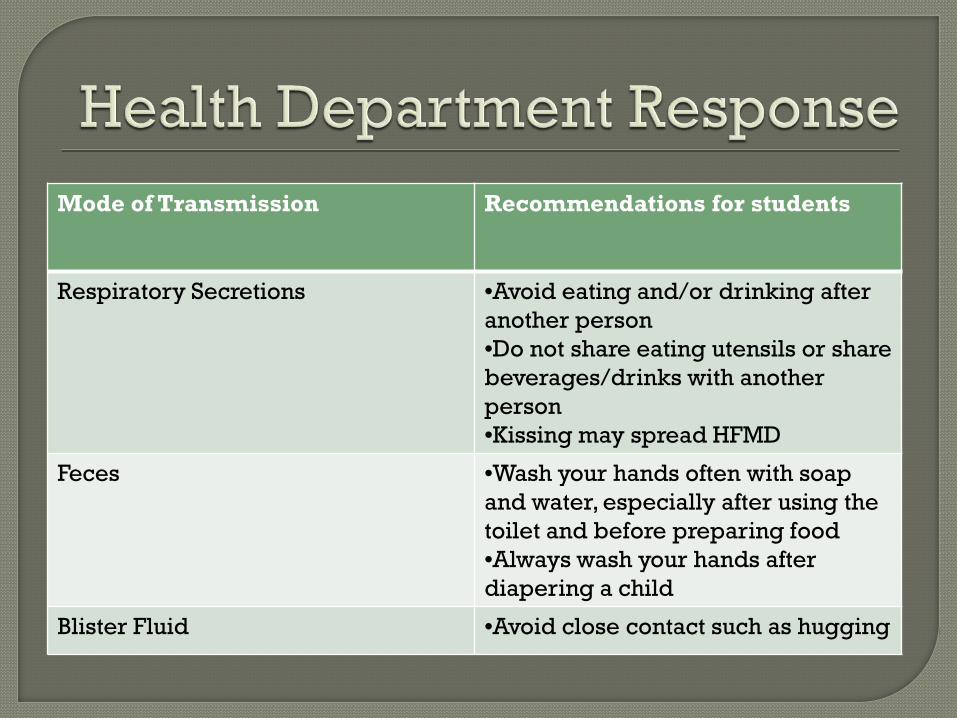
Mode of Transmission Recommendations for students
Respiratory Secretions •Avoid eating and/or drinking after another person •Do not share eating utensils or share beverages/drinks with another person •Kissing may spread HFMD
Feces •Wash your hands often with soap and water, especially after using the toilet and before preparing food •Always wash your hands after diapering a child
Blister Fluid •Avoid close contact such as hugging
College A puts infection control recommendations for students on the school website
Nearby University B contacted to make them aware of an increase in HFMD cases among adults in the Health District • Student Health Director reports one case • Sample collection kits taken to University B
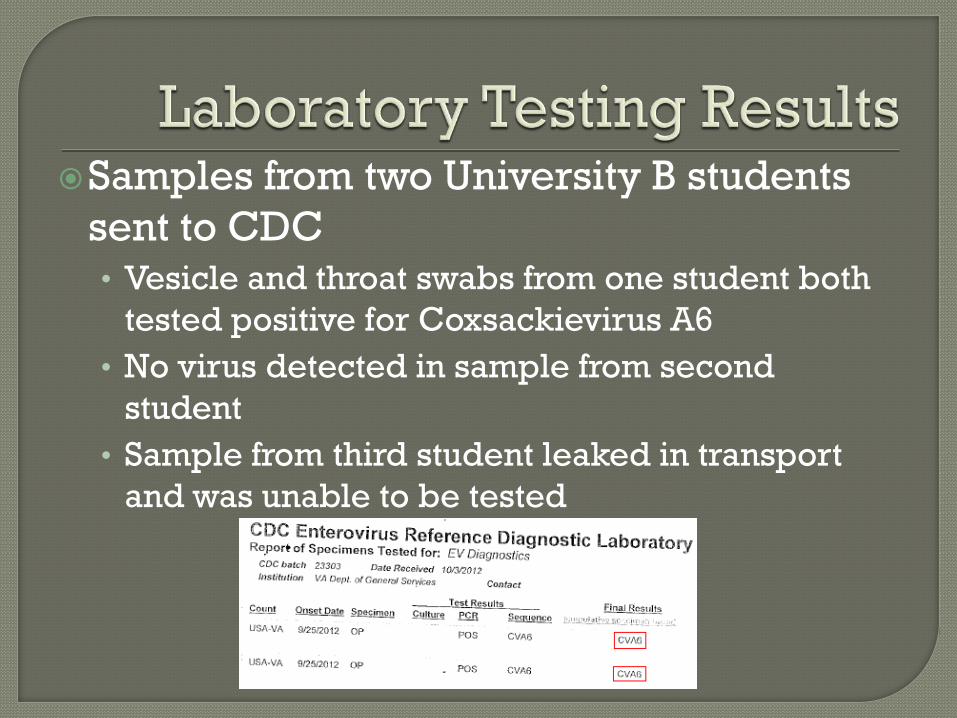
Samples from two University B students sent to CDC • Vesicle and throat swabs from one student both
tested positive for Coxsackievirus A6 • No virus detected in sample from second
student • Sample from third student leaked in transport
and was unable to be tested
Outbreaks have been reported in Finland, Taiwan, Japan, Spain, France since 2008
First reported outbreak in USA occurred November 2011- February 2012 • Alabama, Connecticut, California, and Nevada
reported cases of severe HFMD • 25 cases tested positive at CDC for Coxsackie
A6
0
1
2
3
4
5
6
7
8
9
10
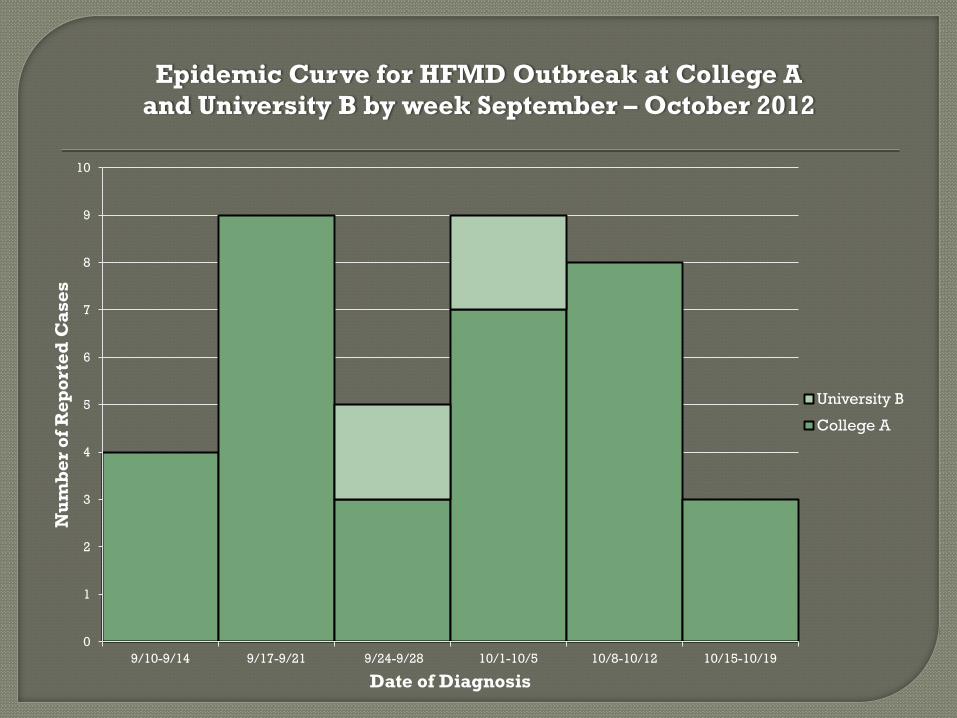
9/10-9/14 9/17-9/21 9/24-9/28 10/1-10/5 10/8-10/12 10/15-10/19
Nu
mb
er o
f Rep
orte
d C
ases
Date of Diagnosis
Epidemic Curve for HFMD Outbreak at College A and University B by week September – October 2012
University B
College A
University C, located less than 100 miles from College A and University B
Outbreak not reported to Health Department
HFMD outbreak reported in school newspaper article October 17th • Article reported 16 cases in September and 8
cases in October
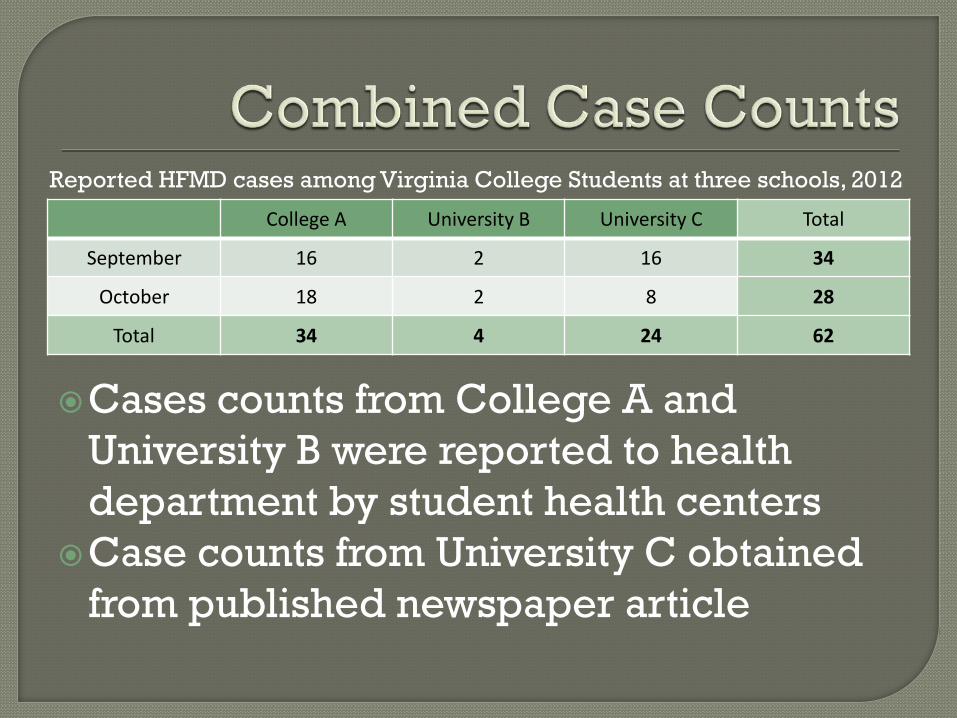
College A University B University C Total
September 16 2 16 34
October 18 2 8 28
Total 34 4 24 62
Cases counts from College A and University B were reported to health department by student health centers
Case counts from University C obtained from published newspaper article
Reported HFMD cases among Virginia College Students at three schools, 2012
HFMD is an emerging disease worldwide with the potential for viruses to move around the globe
College students are a population at risk for outbreaks of HFMD
Lab testing is important to confirm HFMD outbreaks and identify what strains are circulating in the population
Angela West, Central Region Epidemiologist, VDH
Dr. Alexander Samuel, Piedmont Health District Director, VDH
Marilyn B. Freeman, Immunology/Virology and Drug Testing Group Manager, DCLS
Jun Yang, Senior Epidemiologist, VDH Student Health Center Directors at
College A and University B
Österback R, Vuorinen T, Linna M, Susi P, Hyypiä, Waris M. Coxackievirus A6 and hand, foot, and mouth disease, Finland. Emerg Infect Dis [serial on the Internet]. 2009 Sep [04/18/2013]. Available from http://wwwnc.cdc.gov/eid/article/15/9/09-0438.htm
Wei SH, Huang YP, Liu MC, et al. An outbreak of coxsackievirus A6 hand, foot, and mouth disease associated with onychomadesis in Taiwan, 2010. BMC Infect Dis 2011;11:346.
Fujimoto T, Iizuka S, Enomoto M, et al. Hand, foot and mouth disease caused by coxsackievirus A6, Japan, 2011. Emerg Infect Dis 2012;18:337–9.
Mirand A, Henquell C, Archimbaud C, Ughetto S, Antona D, Bailly JL, etal. Outbreak of hand, foot and mouth disease/herpangina associated with coxsackievirus A6 and A10 infections in 2010, France: a large citywide, prospective observational study. Clin Microbiol Infect. 2012;18:E110–8. http://dx.doi.org/10.1111/j.1469-0691.2012.03789.x
Centers for Disease Control and Prevention. Notes from the field: Severe hand, foot, and mouth disease associated with coxsackievirus a6 - Alabama, Connecticut, California, and Nevada, November 2011-February 2012. MMWR 2012;61:213-4.
http://www.purdue.edu/newsroom/research/2012/120301RossmannEnterovirus.html
Enterovirus-71 Model





























