Embed Size (px)
DESCRIPTION
A 75 year
Citation preview
7/18/2019 A 75 year
http://slidepdf.com/reader/full/a-75-year 1/8
SHERWIN C. CAYETANO MARCH 16, 2015
HISTOPATHOLOGY
A 75 year-old male with obstructive jaundice anda pancreatic head mass
CLINICAL HIS!"#
75 year-old male with past medical history signifcant or prostate cancer
status-post radical prostatectomy 15 years ago, who presented with
complaints o approximately diarrhea, dark urine, light stools, pruritus and
15 lb weight loss over the last month. e also admits to evers and chills.
e had a ew episodes o abdominal cramps over the last couple weeks
but denied persistent abdominal pain, nausea or vomiting. !aboratory
tests demonstrated the ollowing values" total bilirubin 1#.$ mg%dl, direct
bilirubin &.' mg%dl, (!) 1*1 +%!, () & +%!, alkaline phosphatase $5
+%!, amylase 57 +%! and lipase *$/ %!. ( 0) scan o the abdomen and
pelvis with contrast revealed a vague area o architectural distortion and
perhaps diminished enhancement within the pancreatic head that
measured between 1.5 to *.# cm. +n addition, multiple clustered, slightly
enlarged celiac-gastrohepatic ligament lymph nodes were identifed
together with a conglomerate peripancreatic nodal mass measures
approximately $.# x *. cm. iliary dilatation with possible distal common
bile duct stricture and dilatation o the gallbladder were also identifed.
$N%!SC!&IC "$"!'"A%$ CH!LAN'I!&ANC"$A!'"A&H#($"C&) AN% $N%!SC!&IC *L"AS!*N% ($*S)
7/18/2019 A 75 year
http://slidepdf.com/reader/full/a-75-year 2/8
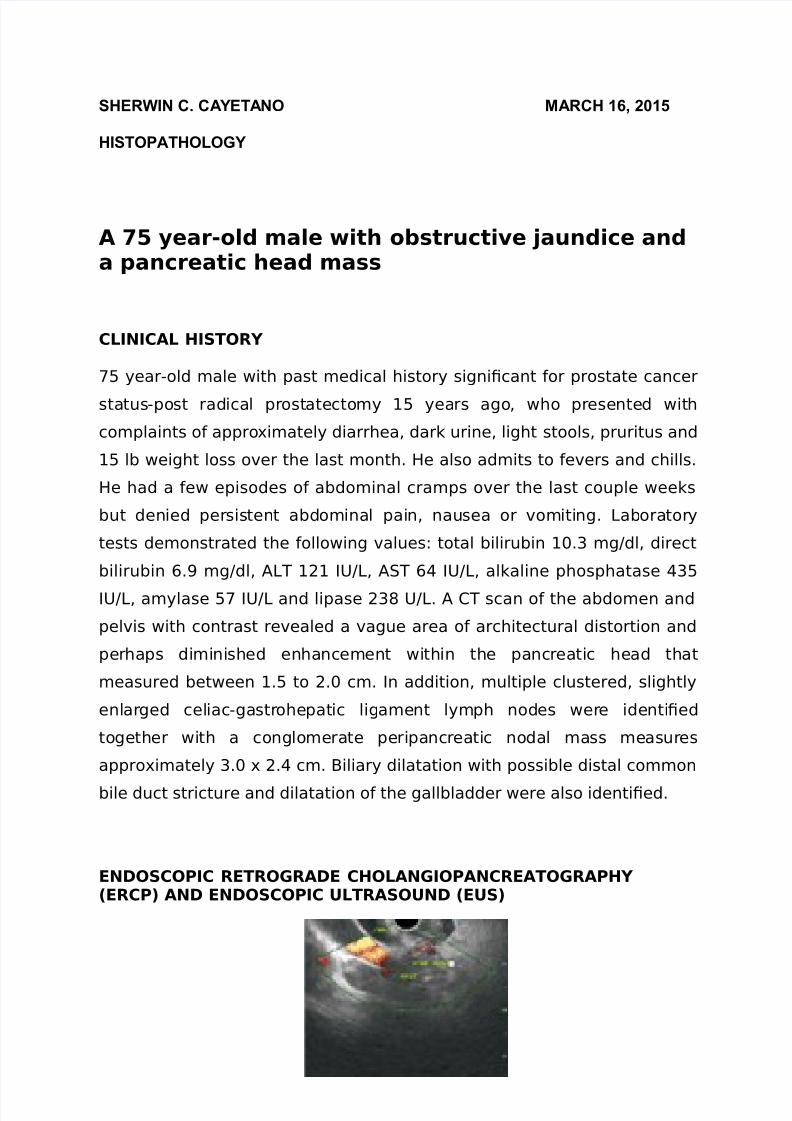
2ig. 1
(n 340 revealed small ma6or papilla, pancreatic duct stricture, severe
biliary stricture, and moderately dilated middle and third main bile duct. (
mucosal biopsy o the bile duct was submitted to surgical pathology. (n
3 showed a *.1 cm ill-defned solid hypoechoic mass in the pancreatic
head 2igure 18, irregularly contoured and ectatic pancreatic duct up to
mm in diameter8, ew abnormal peripancreatic head regional lymphs, and
suggestion o a stricture in the lower third o the main bile duct and
dilation in the gallbladder. 2ine needle aspiration o the pancreatic head
mass and peripancreatic lymph nodes was perormed.
C#!L!'IC +IN%IN'S
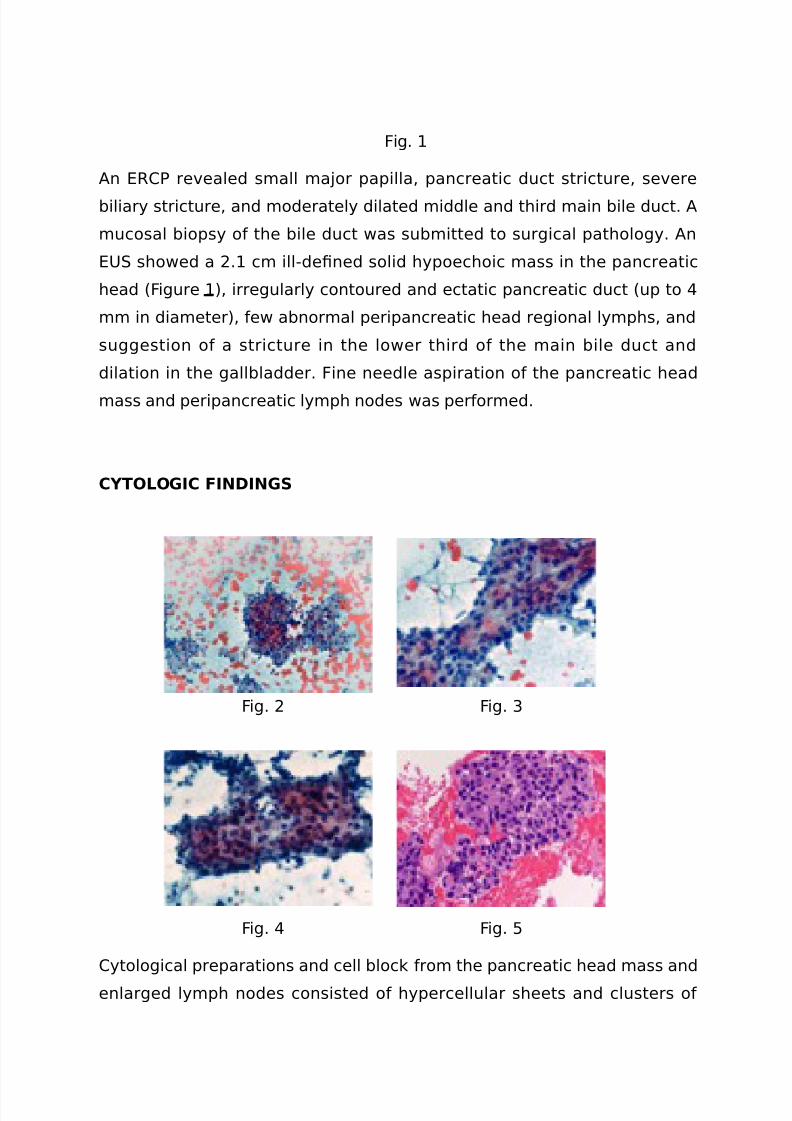
2ig. * 2ig. $
2ig. 2ig. 5
0ytological preparations and cell block rom the pancreatic head mass and
enlarged lymph nodes consisted o hypercellular sheets and clusters o
7/18/2019 A 75 year
http://slidepdf.com/reader/full/a-75-year 3/8
pleomorphic and cohesive atypical cells with abundant granular
cytoplasm, and an enlarged nucleus with a prominent eosinophilic
nucleolus. 9ccasional architectural, rosette or acinar ormation was also
seen. 2igures *, $, and 58.
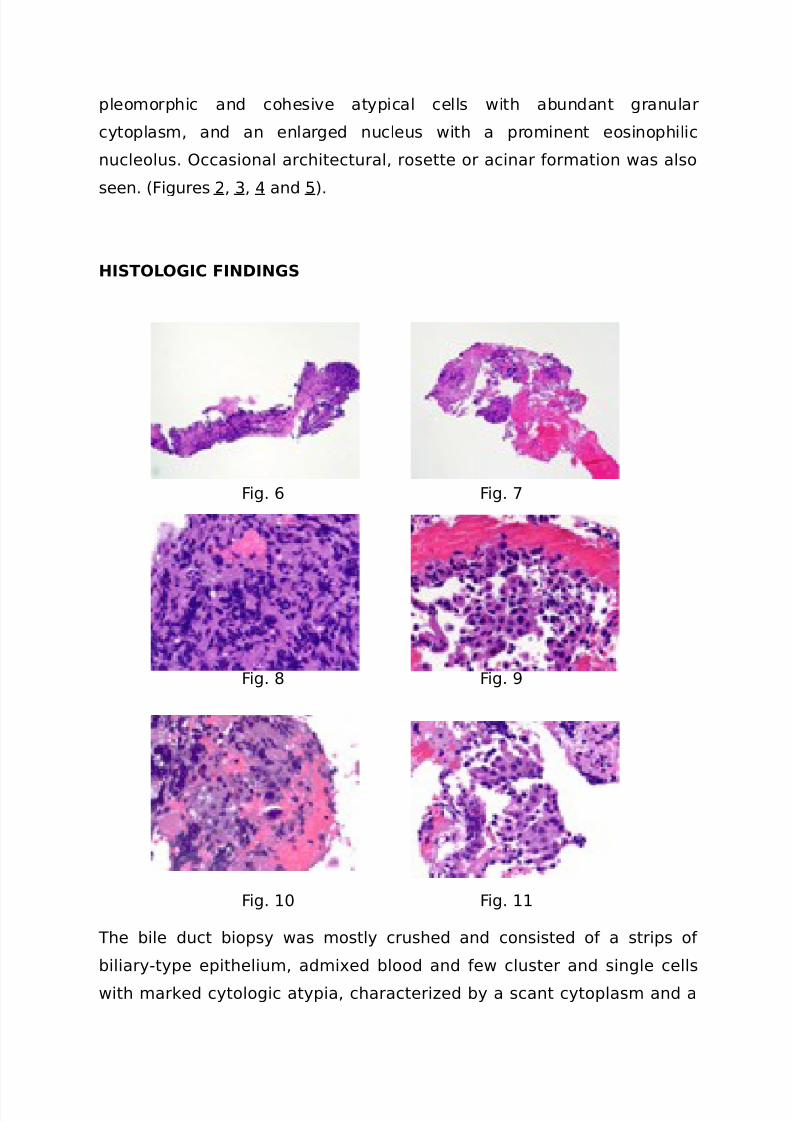
HIS!L!'IC +IN%IN'S
2ig. & 2ig. 7
2ig. / 2ig. '
2ig. 1# 2ig. 11
)he bile duct biopsy was mostly crushed and consisted o a strips o
biliary-type epithelium, admixed blood and ew cluster and single cells
with marked cytologic atypia, characteri:ed by a scant cytoplasm and a
7/18/2019 A 75 year
http://slidepdf.com/reader/full/a-75-year 4/8
hyperchromatic nucleus. (lthough crushed, these histologic fndings were
highly concerning or a poorly-di;erentiated neoplasm 2igures &, 7, /, ',
1# and 118.
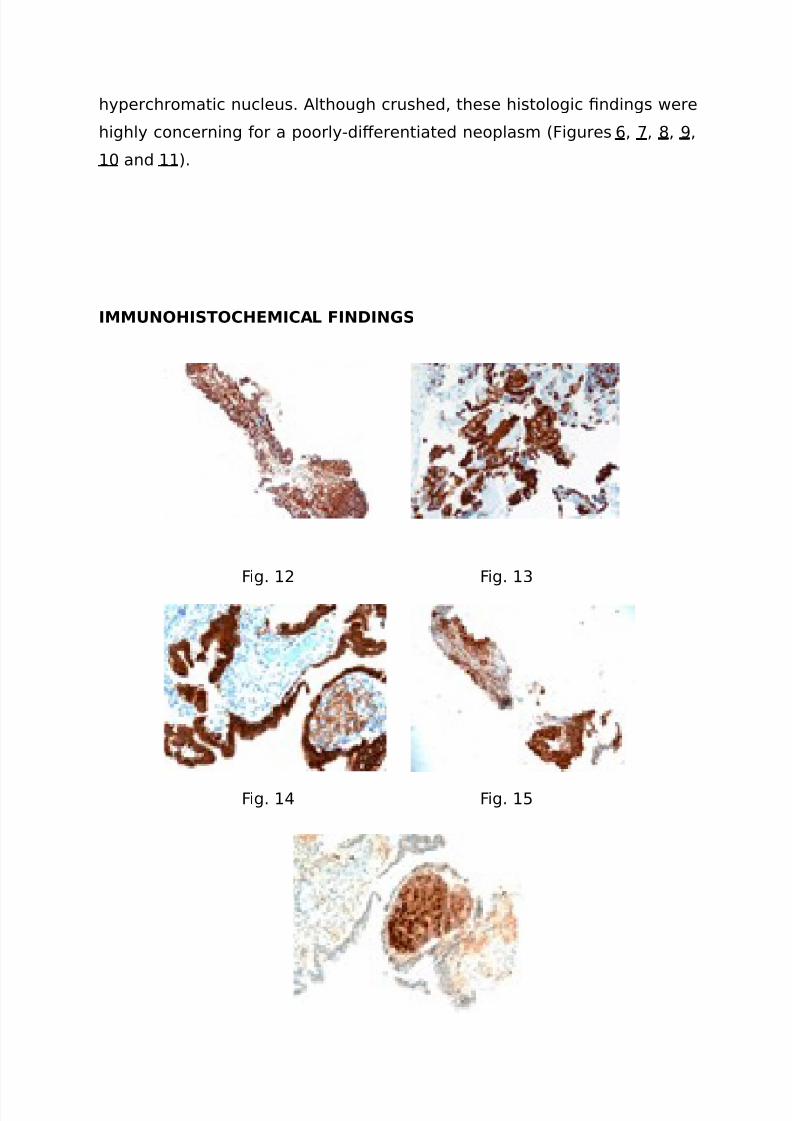
I,,*N!HIS!CH$,ICAL +IN%IN'S
2ig. 1* 2ig. 1$
2ig. 1 2ig. 15
7/18/2019 A 75 year
http://slidepdf.com/reader/full/a-75-year 5/8
2ig. 1&
+mmunohistochemical stains on the bile duct biopsy demonstrated the
atypical cells were positive or cytokeratin (31%(3$ 2igure 1*8, 0(< 5.*
2igure 1$8, 0=1' 2igure 1, note the weakly positive neoplastic cells and
strongly positive biliary-type epithelium8, and >kx$.1 2igures 15 and 1&,
note the di;use nuclear positivity o the neoplastic cells and the negative
staining o the biliary-type epithelium8? while negative or synaptophysin,
-1## protein, tyrosinase, trypsin, 0@5, 0@$, (, <( and 5#1.
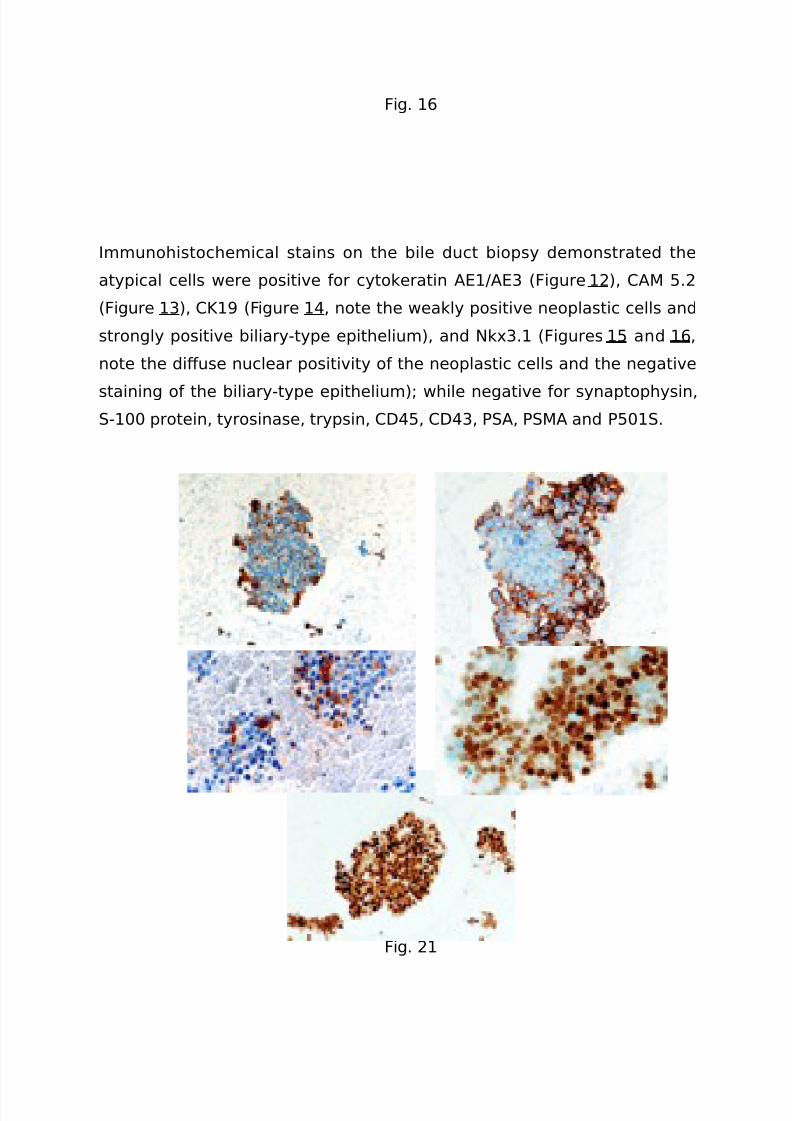
2ig. 17 2ig. 1/
2ig. 1' 2ig. *#
2ig. *1
7/18/2019 A 75 year
http://slidepdf.com/reader/full/a-75-year 6/8
+mmunohistochemical stains perormed on the cell block preparations
rom the pancreatic head fne needle aspirate showed
immunohistochemical positivity or 0=1' 2igure 178, er-3 2igure 1/8,
monoclonal 03( ocal8, ( ocal, 2igure 1'8, androgen receptor 2igure*#8 and >kx$.1 2igure *18? while negative or synaptophysin and trypsin.<etastatic prostatic adenocarcinoma.
"$+$"$NC$S
1. 3idt , Aergas <, chmidt 4, iedek <. <etastasis to the pancreas--an indication or pancreatic resectionB !angenbecks (rch urg. *##7
ep?$'*58"5$'-*. 3pub *##7 Aan *$.*. perti 0, asCuali 0, !iessi D, inciroli !, @ecet D, edra::oli .
ancreatic resection or metastatic tumors to the pancreas. A urg9ncol. *##$ Aul?/$$8"1&1-&.
$. howalter !, ager 3, Eeo 0A.<etastatic disease to the pancreasand spleen. emin 9ncol. *##/ (pr?$5*8"1&#-71. doi"1#.1#5$%6.seminoncol.*##7.1*.##/. 4eview.
. (dsay >F, (ndea (, asturk 9, =ilinc >, >assar , 0heng [email protected] tumors o the pancreas" an analysis o a surgical and
autopsy database and review o the literature. Firchows (rch. *## Aun?&8"5*7-$5. 3pub *## (pr 1.
5. 4eddy , 3dil , 0ameron A!, awlik )<, erman A<, Dilson <<,0ampbell =(, chulick 4@, (hu6a >, Golgang 0!. ancreaticresection o isolated metastases rom nonpancreatic primarycancers. (nn urg 9ncol. *##/ >ov?15118"$1''-*#&. doi"1#.1*5%s1#$-##/-#1#-7. 3pub *##/ ep 11.
&. Dilbert 0<, <onaco 3, 0ooper ), =halbuss G3. 3ndoscopicultrasound-guided fne-needle aspiration o metastases to the
pancreas" ( study o *5 cases. 0yto6ournal. *#11?/"7. doi"1#.1#$%17*-&1$.7'77'. 3pub *#11 (pr *1.
7. Folmar =3, Aones 0=, Hie .<etastases in the pancreas romnonhematologic neoplasms" report o *# cases evaluated by fne-needle aspiration. @iagn 0ytopathol. *## 9ct?$18"*1&-*#.
/. Durel , (li )I, <ontgomery 3(, egum , icks A, Doggins <,3berhart 0D, 0lark @, ieberich 0A, 3pstein A+, @e <ar:o (<. >=H$.1as a marker o prostatic origin in metastatic tumors. (m A urgathol. *#1# (ug?$/8"1#'7-1#5. doi"1#.1#'7%(.#b#1$e$1/1e&cb$.
7/18/2019 A 75 year
http://slidepdf.com/reader/full/a-75-year 7/8
'. Aacob A, 0hargari 0, auduceau 9, 2ayolle <, 0eccaldi , rat 2, !e<oulec , Fedrine !.ancreatic metastasis rom prostate cancer.0ase 4ep <ed. *#1#?*#1#"/*&*7$. doi" 1#.1155%*#1#%/*&*7$. 3pub*#1# <ay *$.
1#. <inni 2, 0asadei 4, eren:e , Dreco F<, <arrano >, <argiotta(, <arrano @. ancreatic metastases" observations o three casesand review o the literature. ancreatology. *##?&8"5#'-*#. 3pub*## (ug 1&.
%ISC*SSI!N
)his case illustrates the importance o documentation o proper
clinical history in pathology. )he pancreatic head mass 2>( and bile duct
biopsy specimens were compatible with involvement by an
adenocarcinoma that was 0=1' positive. 0onsidering the radiographic and
pathologic fndings, the biopsies were highly suspicious or a primary
pancreatic adenocarcinoma. >onetheless, the presence o prominent
macronucleoli, which is not a eature commonly seen in pancreatic
adenocarcinoma, prompted or urther characteri:ation o this pancreatic
neoplasm. )he di;erential diagnoses that were considered included other
pancreatic neoplasms, such as, acinar cell carcinoma, neuroendocrine
tumor%carcinoma and a metastasis.
=nowledge o the patientJs remote history o prostatic carcinoma
and the unusual cytologic%histologic eatures, prompted us to perorm a
panel o immunohistochemical stains that were consistent with a
metastasis rom the patientJs known prostate cancer. )he diagnosis
heavily relied on the immunoreactivity or >=H$.1, ( and androgen
receptor. 9ther diagnoses were excluded by the lack o immunostaining
or trypsin acinar cell carcinoma8, 1## protein and tyrosinase
metastatic melanoma8, and synaptophysin neuroendocrine
tumor%carcinoma8.
+t is well known that primary neoplasms o the pancreas are ar more
common than metastatic tumors. +n the literature, metastases to the
7/18/2019 A 75 year
http://slidepdf.com/reader/full/a-75-year 8/8
pancreas comprise approximately *K-K o pancreatic tumors 2ig. 1-*8.
+mportantly, autopsy data demonstrate that metastases to the pancreas
are common in those cases with di;use spread o primary cancer to
multiple organs, but exceedingly rare as an isolated metastatic lesion 2ig.8. )he most common primary tumors reported to metastasi:e to the
pancreas include renal cell, gastrointestinal colon and stomach8, breast
and lung carcinomas, melanomas and some sarcomas 2ig. -58.
nortunately, metastases to the pancreas oten occur as solitary masses
in the head o the pancreas in patients without history o malignancy, thus
resembling a pancreatic primary. (dditionally, in many cases and as seen
herein, the radiologic impression is also that o a primary tumor? however,
treatment options and prognosis are signifcantly di;erent. )his
underscores the importance o proper clinical history.
<etastatic prostatic adenocarcinoma to the pancreas is a rare
presentation, and has been reported as isolated case reports in the
3nglish literature. 3-2>( is the preerred method to assess these
tumors 2ig. &-78. )o arrive at the correct diagnosis, not only is knowledge
o the clinical history important, but a panel o immunohistochemicalstains is imperative. )hese include (, <(, androgen receptor and the
recently described >=H$.1. >=H$.1 has a high sensitivity and specifcity
or prostatic origin with the beneft o being a nuclear stain that is not
a;ected by anti-androgen therapy 2ig. /8.