Embed Size (px)
Citation preview
A 53-years-old woman presents with bilateral acrocyanosis of
feet
Presentation of Case
ID:
A 53 years old woman known case of hyperlipidemia, widow, native and resident of Baravat (is a city in the central district of Bam County, Kerman Province, Iran)
Chief complaint:
Black discoloration of toes

Presentation of Case
Present illness:
About twenty days before admission, the patient was suffering from fever and chills. 3 days later fever was stopped but edema of the lower extremities in feet was presented.
Two to three days after the onset of edema, purple discoloration was noticed at the fingertips of the left foot and the right foot on the next day.
Presentation of Case
Present illness (con.)
The cyanosis was progressive and the proximal portion
of the dorsal and palmar surfaces of the feet involves on
Following days.
After some days black discoloration and dryness of skin
was presented in fingertips specially in palmar surfaces
of feet.

Presentation of Case
Present illness (con.)
She did not complain of pain.
She had history of two abortions.
She had no history of cigarette smocking
She had no history of morning stiffness.
She had no hystory of raynaud’s phenomenon
Presentation of Case
Present illness (con.)
She had no history of weight loss , night sweats,
and long term fever.
She had no history of endovascular procedure.
She had no history of clotting event.
She reported a left knee effusion six mounths
earlier that was taped by the physician and
treated with intra articular injection.
Presentation of Case
Present illness (con.)
With these complains she came to a orthopedic
specialist. She first was admitted in orthopedic
ward and through a consultant transfer to internal
medicine ward.
Presentation of Case
PMH :
• Hyperlipidemia
• Left knee arthritis 6 months earlier
• Tow abortions
• No renal disease
• No thrombotic event
• No history of psychiatric disease
Presentation of Case
DH:
Tab atorvastatin 10 mg daily
There was no history of warfarin or heparin consumption
FH: Non significant
AH: Non significant
PH: Non significant
Cigarette smocking (-)
Presentation of CasePhysical Examination:
General appearance:
A middle age woman that was not ill and toxic, she was aware, awake and oriented
Vital signs:
BP: 90 / 60 PR: 90 RR: 16 T: 36.5 6c (oral)
Presentation of Case
Head and Neck:
• Pale conjunctiva
• There is no lymphadenopathy
• There is no evidence of ulcers in mouth and nose
• There is no rush or patch
• There is no bruit on neck
Presentation of Case
Chest:
• Heart: S1 S2 without any murmer
• Lungs: bilateral clear
Presentation of Case
Abdomen:
• There is no tenderness
• There is no organomegally
Presentation of Case
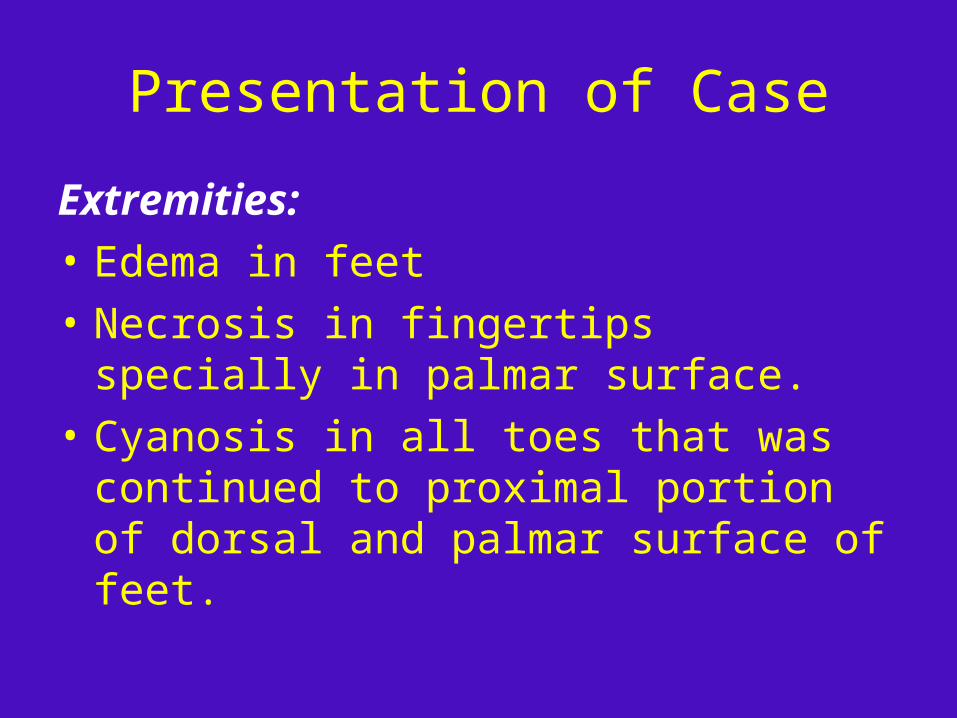
Extremities:
• Edema in feet
• Necrosis in fingertips specially in palmar surface.
• Cyanosis in all toes that was continued to proximal portion of dorsal and palmar surface of feet.
Presentation of Case
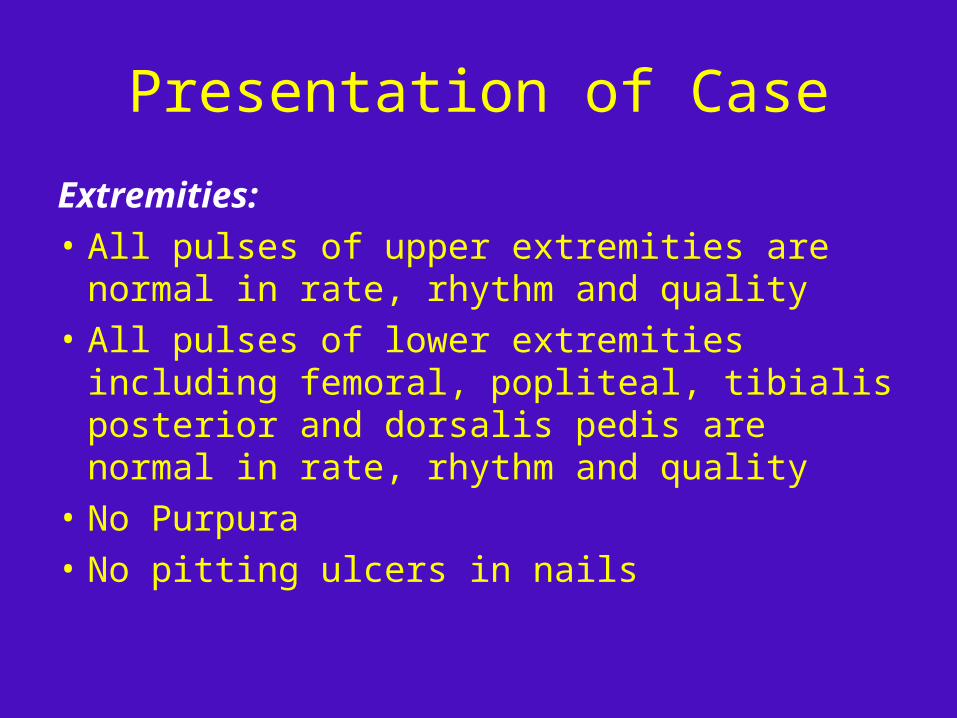
Extremities:
• All pulses of upper extremities are normal in rate, rhythm and quality
• All pulses of lower extremities including femoral, popliteal, tibialis posterior and dorsalis pedis are normal in rate, rhythm and quality
• No Purpura
• No pitting ulcers in nails

Presentation of Case
Examination of the joints:
• Peripheral joints:
normal range of motion,
no evidence of arthritis
• Central joints:
normal
Presentation of Case
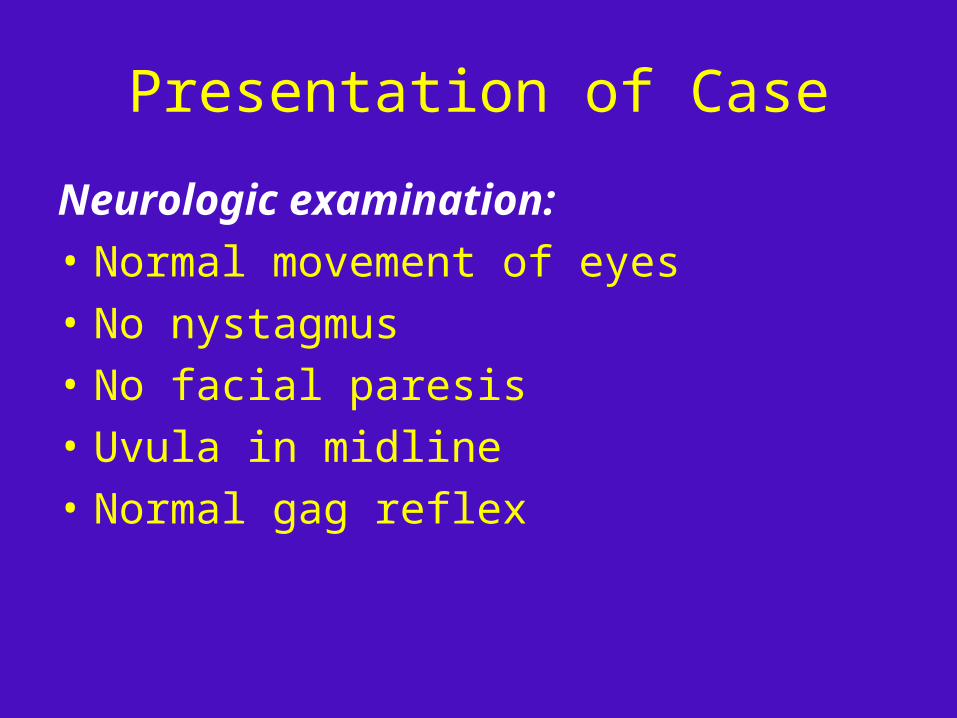
Neurologic examination:
• Normal movement of eyes
• No nystagmus
• No facial paresis
• Uvula in midline
• Normal gag reflex
Presentation of Case
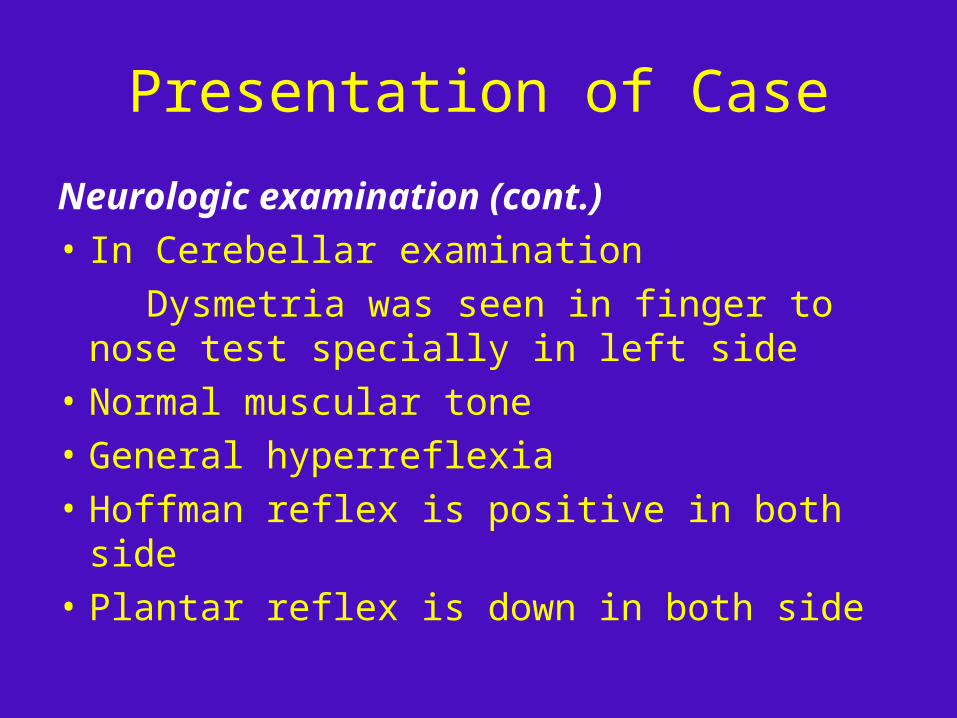
Neurologic examination (cont.)
• In Cerebellar examination
Dysmetria was seen in finger to nose test specially in left side
• Normal muscular tone
• General hyperreflexia
• Hoffman reflex is positive in both side
• Plantar reflex is down in both side

Presentation of Case
Neurologic examination (cont.)
• Forces:
upper extremities: proximal 4/5 and distal 5/5
lower extremities: proximal 3/5 and distal 5/5



acrocyanosis

acrocyanosis
• There is no uniform definition of acrocyanosis.
• Acrocyanosis is defined as a painless condition characterized by discoloration of different shades of blue in the distal parts of the body (most commonly in the hands, feet, and face) that is marked by symmetry and persistence of color changes aggravated by cold exposure, and which is frequently associated with local hyperhidrosis of hands and feet.
acrocyanosis
• Acrocyanosis should be distinguished from Raynaud’s phenomenon, pernio, erythromelalgia, and other members of group of conditions known as acrosyndromes
• Raynaud phenomenon is excessively reduced blood flow in response to cold or emotional stress, causing discolouration of the fingers, toes, and occasionally other areas.
• Raynaud's phenomenon is characterized by paroxysmal episode of triphasic or biphasic color change (white, red and bluish discoloration) of finger and toes.
• Chilblain or pernios is also developed after cold exposure in digits with erythematous and purplish discoloration. Other symptoms like itching, burning and pain are often present in contrast to acrocyanosis. Conspicuous edema of the digits and tenderness are also prominent features in perniosis. Blisters, pustules and ulcerations are frequently seen in severe cases.
acrocyanosis
• Primary (idiopathic, essential) When no apparent cause can be determined a benign condition may spontaneously resolve Is mostly a disease of young adults
acrocyanosis
• Although primary acrocyanosis is generally considered a benign condition implying no evolution to more serious problems, few studies report long-term follow-ups.
• Presence of pain, ulcerations and gangrene should lead to an alternative diagnosis.
• Age may be helpful in diagnosis as primary acrocyanosis often resolves in middle age.
• In primary acrocyanosis, there are no specific laboratory abnormalities
acrocyanosis
• Secondary Acrocyanosis is a manifestation of other
diseases may portend a worse prognosis some cases may be the first manifestation of
these conditions.
Secondary acrocyanosis
is often marked by asymmetryassociated with pain and tissue damagethe presence of various signs of the primary
disorder which may become fully manifest with the passage of time.
Causes of secondary acrocyanosis
• Hypoxemia
• Stroke
• Myocardial infarction
• Buerger’s disease
• Lung diseases
• Acrocyanosis of infancy
• Atheromatous embolism
• Connective tissue / rheumatologic diseases
Causes of secondary acrocyanosis
• Antiphpospholipid syndrome
• Eating disorders
• Neoplasms
• Hematologic disorders
• Drug exposure associations
• Toxicities
• Heritable diseases
• Orthostatic intolerance and postural tachycardia syndrome
Causes of secondary acrocyanosis
• Psychiatric
• Spinal cord injury
• Chronic hypertrophic and primary atrophic rhinitis
• Atopic dermatitis
• Hypersensitivity coronary syndrome (Kounis syndrome)
Causes of secondary acrocyanosis
Infections:
• HIV
• Psittacosis
• Mononucleosis
• Hepatitis C
• Acute bacterial endocarditis (septic emboli)
• Meningococcemia
Secondary acrocyanosis
• Tissue damage, including ulcerations and gangrene, may reflect the severity of the underlying primary condition and pain may be present.
Secondary acrocyanosis
blue toe syndrome:
atheromatous embolization of the terminal vessels in the setting of oral anticoagulant therapy, but also from plaque disruption during vessel catheterization.
Secondary acrocyanosis
Drug exposure associations:
• Tricyclic antidepressants, Interferon Vasopressors (terlipressin, dopamine) Sirolimus, Clonidine , Amphotericin B Phenazopyridine, Benzocaine, Propoxyphene , Bleomycin , Intravenous immune globulin , Butyl nitrite
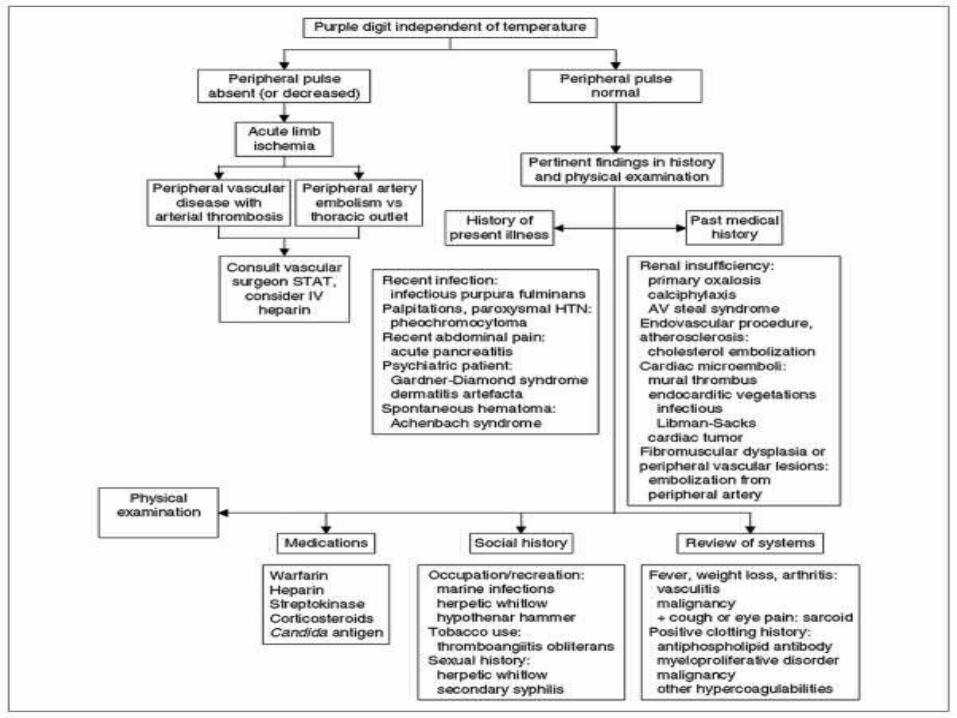
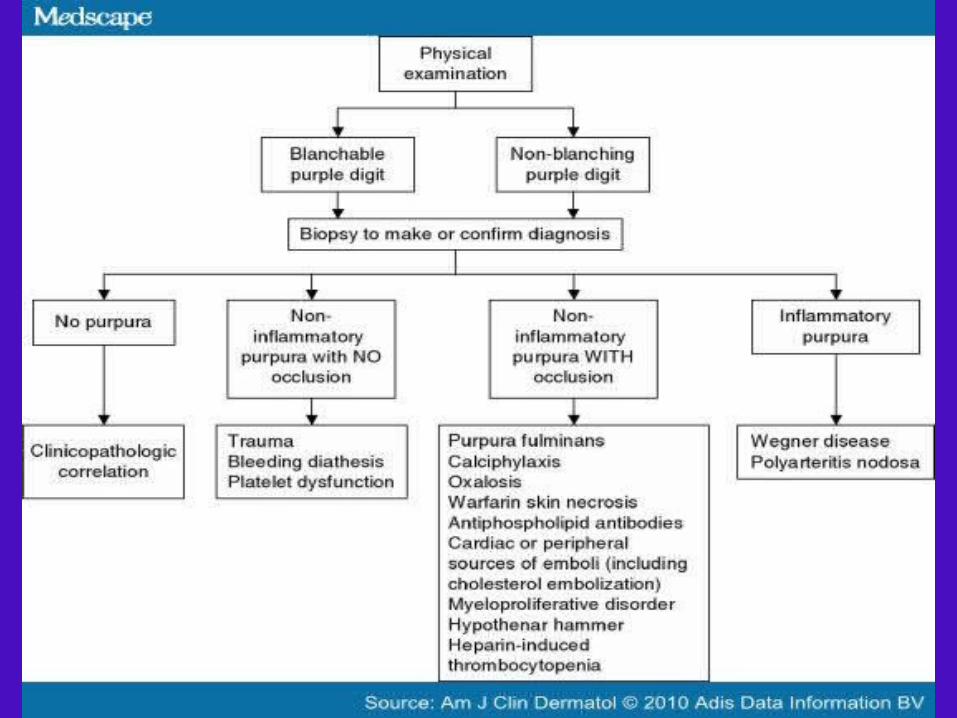
How to diagnosis the cause of secondry acrocyanosis
• A practical diagnostic algorithm of a ‘purple digit’ was offered by Brown et al. (Am j clin dermatol 2010; 11(2): 103-116)
• It is based on history and physical examination

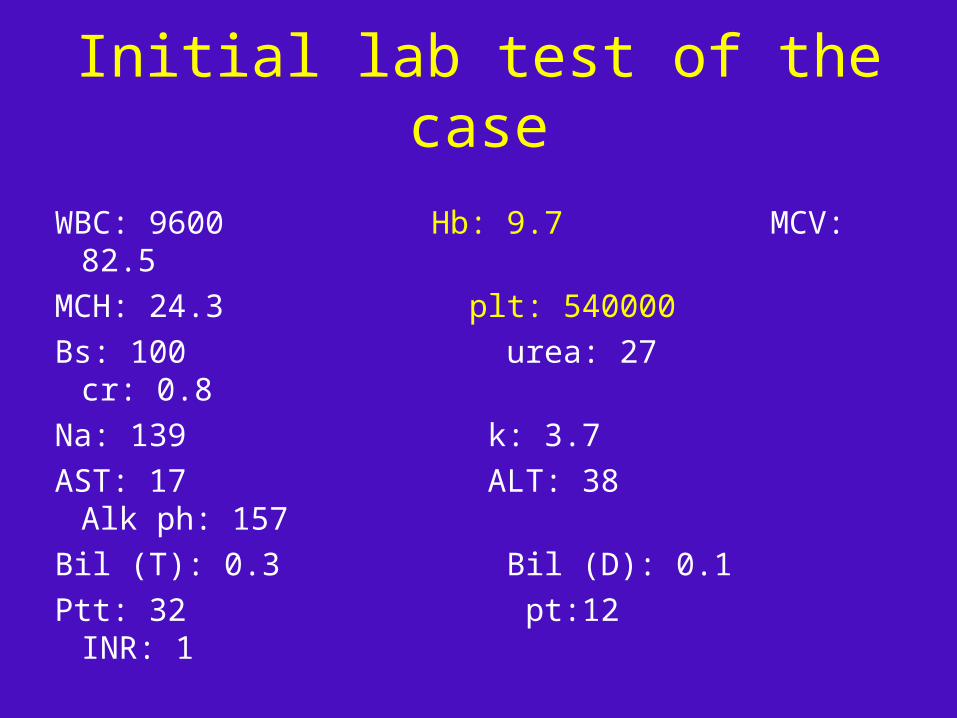
Initial lab test of the case
WBC: 9600 Hb: 9.7 MCV: 82.5
MCH: 24.3 plt: 540000
Bs: 100 urea: 27 cr: 0.8
Na: 139 k: 3.7
AST: 17 ALT: 38 Alk ph: 157
Bil (T): 0.3 Bil (D): 0.1
Ptt: 32 pt:12 INR: 1
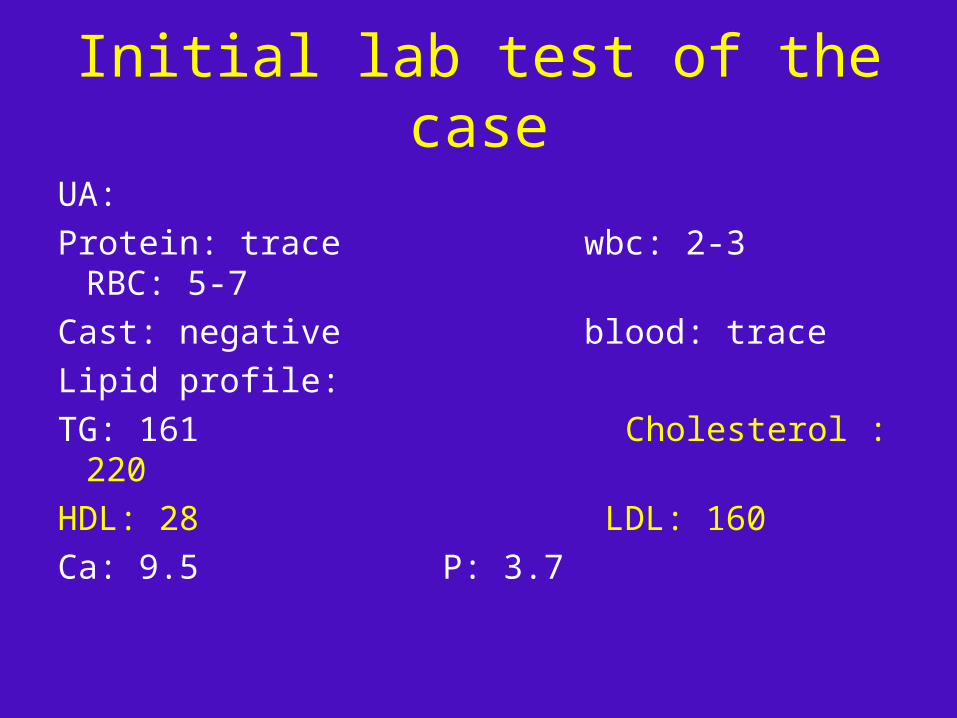
Initial lab test of the case
UA:
Protein: trace wbc: 2-3 RBC: 5-7
Cast: negative blood: trace
Lipid profile:
TG: 161 Cholesterol : 220
HDL: 28 LDL: 160
Ca: 9.5 P: 3.7

Diagnostic approach of the Case
According to:
• beginning of symptoms in cold season
• absence of pain
• No history of endovascular procidure
• no drug history except the use of Atorvastatin
• History of abortion
• Presence of necrosis
• Normal pulses of extremities
• Proxymal weakness
• Dysmetria in finger to nose test
• Anemia

Diagnostic approach of the Case
We consider the following DDx:
• Connective tissue disease
• Antiphospholipid syndrome
• Malignancy (paraneoplastic sundrome)
• Cryoglobulinemia
• Cryofibrinogenemia
• Cold agglutinin disease
Diagnostic workups of the Case
• CXR: no pathological finding
• Abdominopelvic sonography:
abnormal findings:Increased echo pattern of liver in favor of mild
to moderate fatty liver disease.Uterus and ovaries are atrophic
• Color doppler sonography of lower extremities: Normal
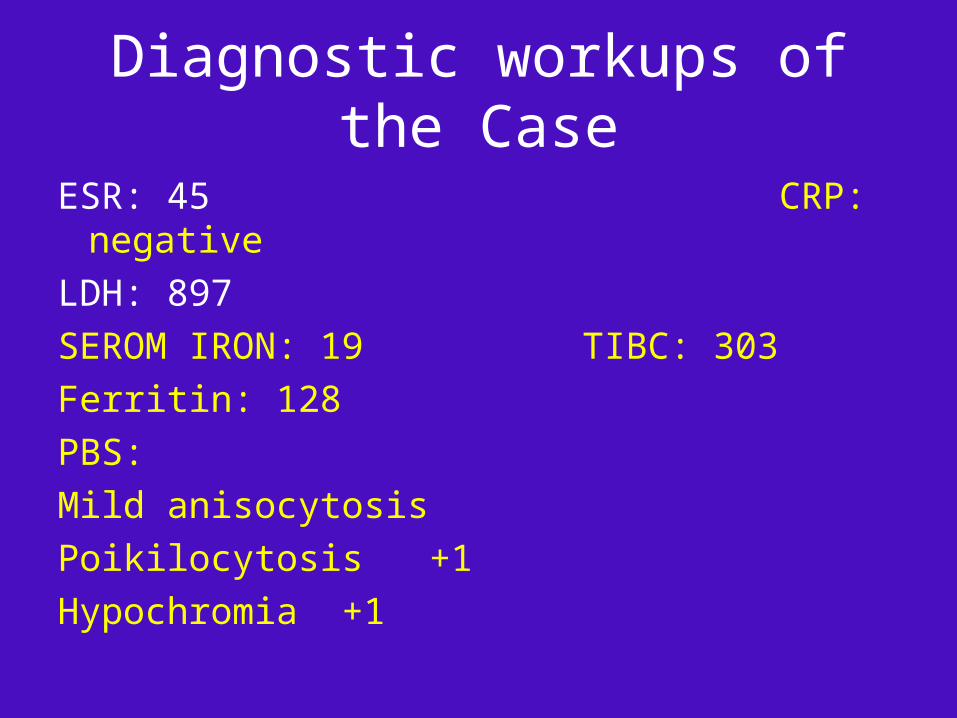
Diagnostic workups of the Case
ESR: 45 CRP: negative
LDH: 897
SEROM IRON: 19 TIBC: 303
Ferritin: 128
PBS:
Mild anisocytosis
Poikilocytosis +1
Hypochromia +1
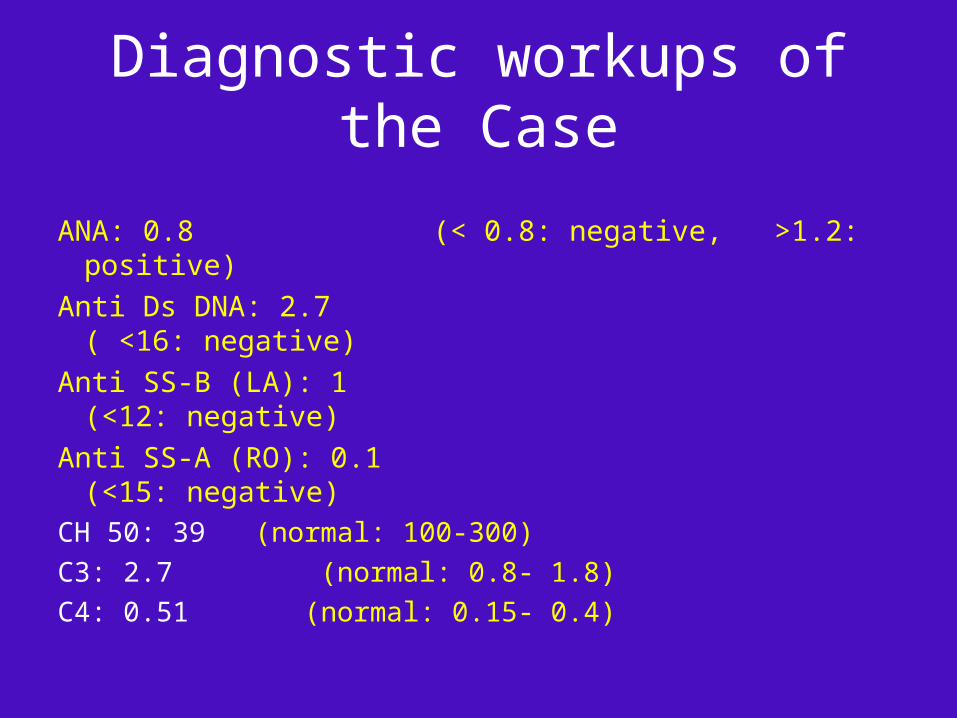
Diagnostic workups of the Case
ANA: 0.8 (< 0.8: negative, >1.2: positive)
Anti Ds DNA: 2.7 ( <16: negative)
Anti SS-B (LA): 1 (<12: negative)
Anti SS-A (RO): 0.1 (<15: negative)
CH 50: 39 (normal: 100-300)
C3: 2.7 (normal: 0.8- 1.8)
C4: 0.51 (normal: 0.15- 0.4)
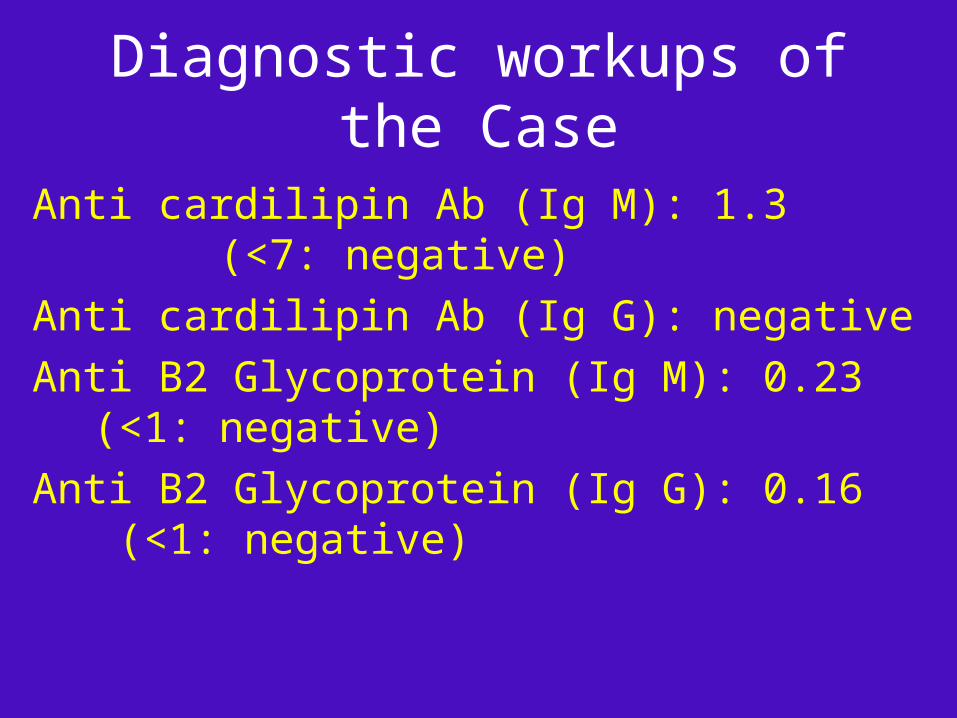
Diagnostic workups of the Case
Anti cardilipin Ab (Ig M): 1.3 (<7: negative)
Anti cardilipin Ab (Ig G): negative
Anti B2 Glycoprotein (Ig M): 0.23 (<1: negative)
Anti B2 Glycoprotein (Ig G): 0.16 (<1: negative)
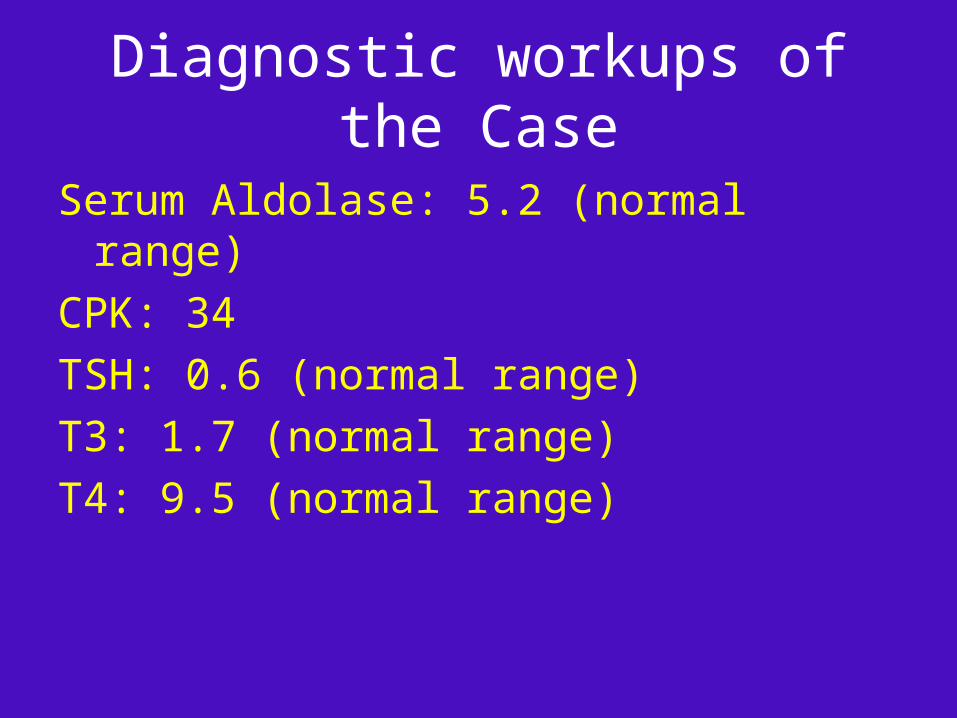
Diagnostic workups of the Case
Serum Aldolase: 5.2 (normal range)
CPK: 34
TSH: 0.6 (normal range)
T3: 1.7 (normal range)
T4: 9.5 (normal range)
Diagnostic workups of the Case
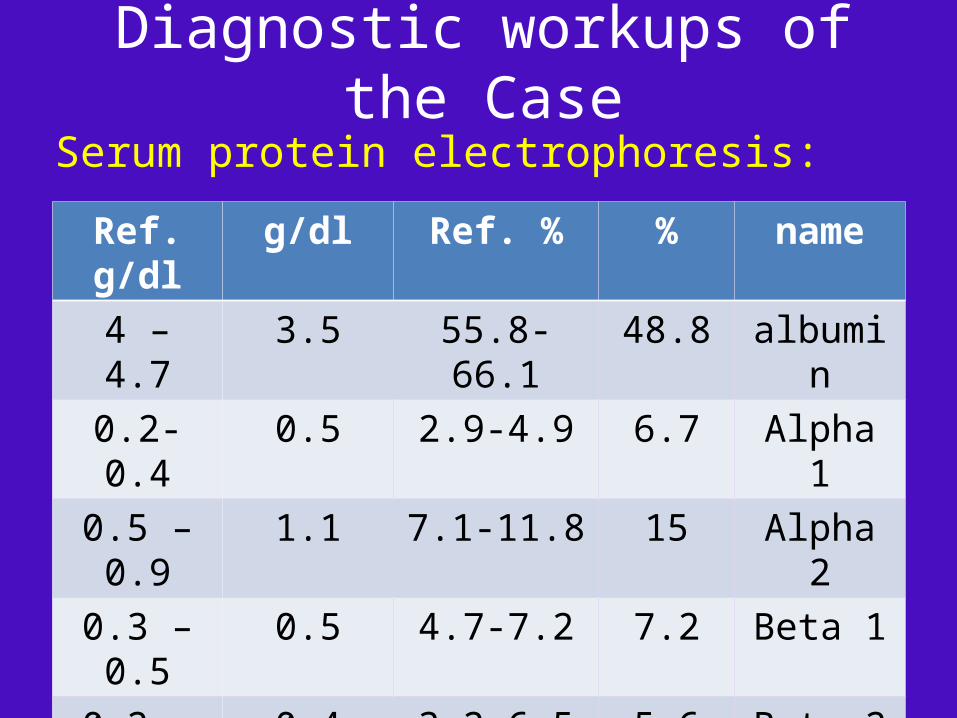
Serum protein electrophoresis:
name%Ref. %g/dlRef. g/dlalbumin48.855.8-66.13.54 – 4.7
Alpha 16.72.9-4.90.50.2- 0.4
Alpha 2157.1-11.81.10.5 – 0.9
Beta 17.24.7-7.20.50.3 – 0.5
Beta 25.63.2-6.50.40.2 – 0.5
Gamma 16.711.1-18.81.20.8 – 1.4
Diagnostic workups of the Case
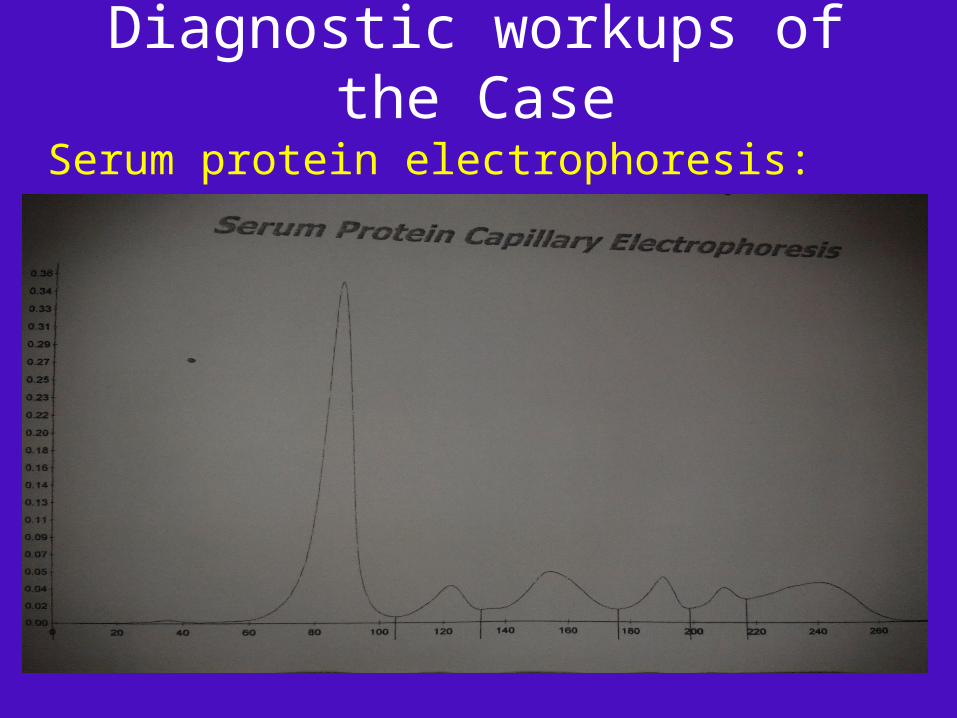
Serum protein electrophoresis:
Diagnostic workups of the Case
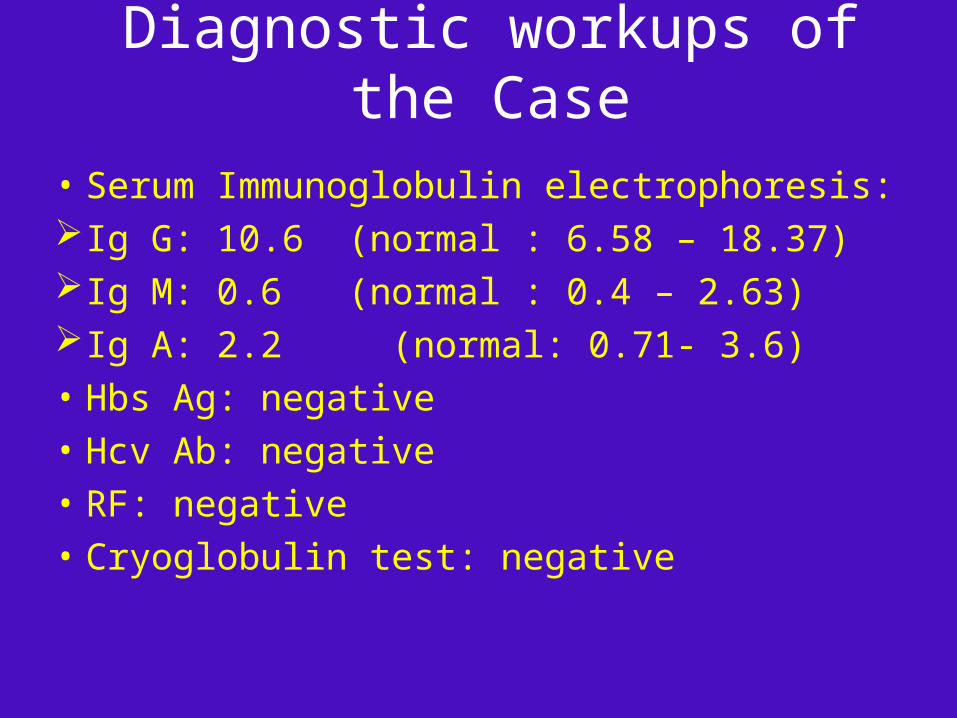
• Serum Immunoglobulin electrophoresis:Ig G: 10.6 (normal : 6.58 – 18.37)Ig M: 0.6 (normal : 0.4 – 2.63)Ig A: 2.2 (normal: 0.71- 3.6)
• Hbs Ag: negative
• Hcv Ab: negative
• RF: negative
• Cryoglobulin test: negative
Diagnostic workups of the Case
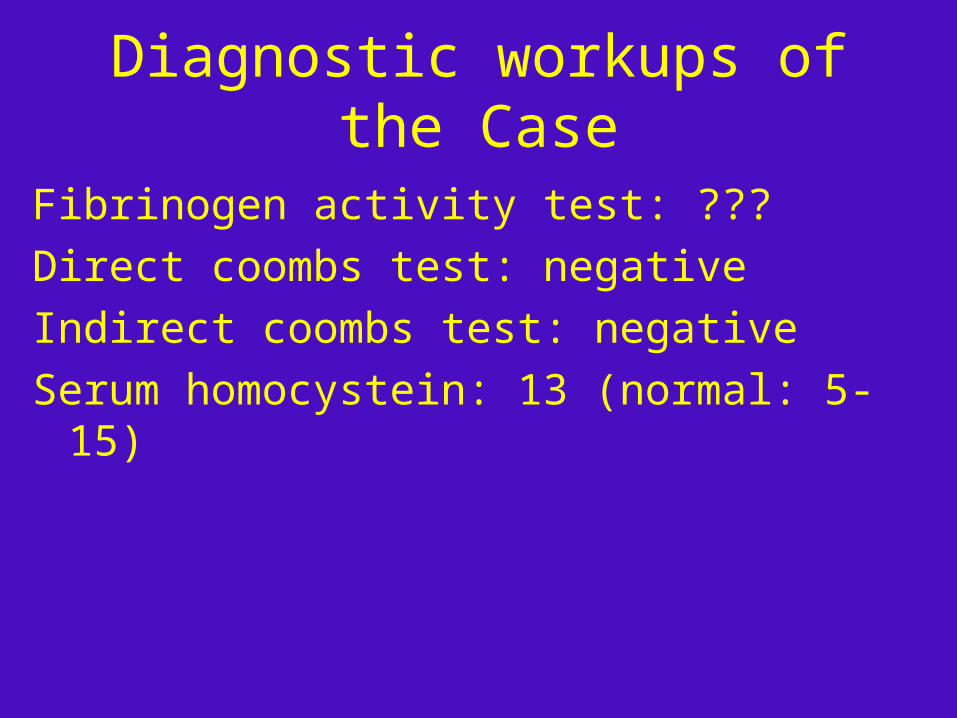
Fibrinogen activity test: ???
Direct coombs test: negative
Indirect coombs test: negative
Serum homocystein: 13 (normal: 5-15)

Diagnostic workups of Case
Spiral chest ct scan:
Lipomatosis changes in mediastin are seen
Lungs field are normal
Plueral effusion and LAP are not seen
Abdominopelvic ct scan with iv and oral contrast:
No gross abnormality is seen in liver, spleen, kidneys and pancreas
No ascitis is seen
No LAP is seen
Diagnostic workups of the Case
Brain MRI:
• Abnormal signal intensity foci are seen in periventricular and subcortical regions could be due to microvascular ischemic changes or vasculitis.
• Mild brain atrophy is seen.
Diagnostic workups of the Case
• EMG & NCV
Axonal early onset of sensorimotor peripheral polyneuropathy in lower limbs.

Abnormal findings
• Elevated ESR
• Elevated LDH
• Low levels of CH50 (It may be a laboratory error because the level of c3 and c4 was not decreased)
• Microvascular ischemic changes in brain MRI
• Axonal sensorimotor peripheral polyneuropathy in lower limbs in EMG-NCV

Findings on history, physical examination, initial
and Complementary lab tests are more
suggestive of vasculitis (primary or secondary)
although a diagnosis of underlying malignancy
can not be removed.





![HIGHLIGHTS OF PRESCRIBING INFORMATION Caution should …total, irreversible, bilateral congenital deafness when administered to a pregnant woman [Warnings and Precautions (5.5)]. Although](https://img.pdfslide.us/doc/110x75/5f6c061c593a6e5572386379/highlights-of-prescribing-information-caution-should-total-irreversible-bilateral.jpg)