Embed Size (px)
Citation preview
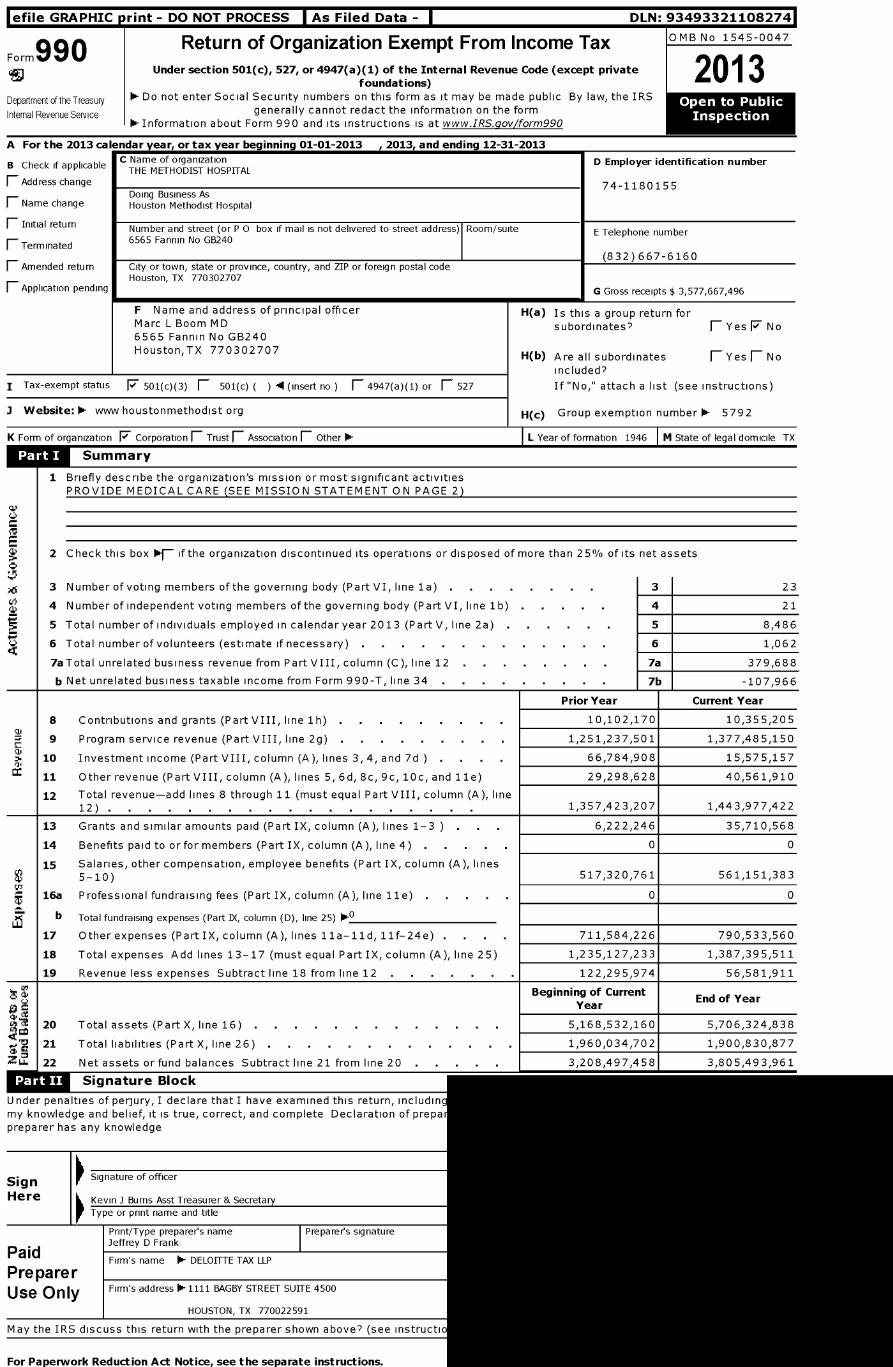
l efile GRAPHIC p rint - DO NOT PROCESS As Filed Data - DLN: 93493321108274
Form990 Return of Organization Exempt From Income Tax OMB No 1545-0047
Under section 501 ( c), 527, or 4947( a)(1) of the Internal Revenue Code ( except private2O1 3foundations)
Department of the Treasury Do not enter Social Security numbers on this form as it may be made public By law, the IRSOpen
Internal Revenue Service generally cannot redact the information on the formInspection
- Information about Form 990 and its instructions is at www.IRS.gov/form990
For the 2013 calendar year, or tax year beginning 01-01-2013 , 2013, and ending 12-31-2013
B Check if applicableC Name of organization D Employer identification numberTHE METHODIST HOSPITAL
F Address change 74-1180155Doing Business As
F Name change Houston Methodist Hospital
1 Initial return Number and street (or P 0 box if mail is not delivered to street address) Room/suite E Telephone number6565 Fannin No GB240
p Terminated(832)667-6160
-( Amended return City or town, state or province, country, and ZIP or foreign postal codeHouston, TX 770302707
1 Application pending G Gross receipts $ 3,577,667,496
F Name and address of principal officer H(a) Is this a group return forMarc L Boom MD subordinates? fl Yes F No6565 Fannin No GB240Houston,TX 770302707 H(b) Are all subordinates 1 Yes (- No
included?
I Tax-exempt status F 501(c)(3) 1 501(c) ( ) I (insert no (- 4947(a)(1) or F_ 527 If "No," attach a list (see instructions)
J Website : - www houstonmethodist org H(c) Group exemption number - 5792
K Form of organization F Corporation 1 Trust F_ Association (- Other 0- L Year of formation 1946 M State of legal domicile TX
Summary
1 Briefly describe the organization's mission or most significant activitiesPROVIDE MEDICAL CARE (SEE MISSION STATEMENT ON PAGE 2)
w
2 Check this box if the organization discontinued its operations or disposed of more than 25% of its net assets
3 Number of voting members of the governing body (Part VI, line 1a) . . . . . . . 3 23
4 Number of independent voting members of the governing body (Part VI, line 1 b) . . . . 4 21
5 Total number of individuals employed in calendar year 2013 (Part V, line 2a) . 5 8,486
6 Total number of volunteers (estimate if necessary) 6 1,062
7aTotal unrelated business revenue from Part VIII, column (C), line 12 . . . . . . . 7a 379,688
b Net unrelated business taxable income from Form 990-T, line 34 . . . . . . . . 7b -107,966
Prior Year Current Year
8 Contributions and grants (Part VIII, line 1h) . 10,102,170 10,355,205
9 Program service revenue (Part VIII, line 2g) . 1,251,237,501 1,377,485,150
N 10 Investment income (Part VIII, column (A), lines 3, 4, and 7d . . . 66,784,908 15,575,157
11 Other revenue (Part VIII, column (A), lines 5, 6d, 8c, 9c, 10c, and 11e) 29,298,628 40,561,910
12 Total revenue-add lines 8 through 11 (must equal Part VIII, column (A), line12) . . . . . . . . . . . . . . . . . . 1,357,423,207 1,443,977,422
13 Grants and similar amounts paid (Part IX, column (A), lines 1-3 ) . 6,222,246 35,710,568
14 Benefits paid to or for members (Part IX, column (A), line 4) . 0 0
15 Salaries, other compensation, employee benefits (Part IX, column (A), lines5-10) 517,320,761 561,151,383
16a Professional fundraising fees (Part IX, column (A), line 11e) 0 0
LLJb Total fundraising expenses (Part IX, column (D), line 25) 0-0
17 Other expenses (Part IX, column (A), lines h1a-11d, 11f-24e) . . . . 711,584,226 790,533,560
18 Total expenses Add lines 13-17 (must equal Part IX, column (A), line 25) 1,235,127,233 1,387,395,511
19 Revenue less expenses Subtract line 18 from line 12 122,295,974 56,581,911
Beginning of CurrentEnd of Year
Year
20 Total assets (Part X, l i n e 1 6 ) . . . . . . . . . . . . 5,168,532,160 5,706,324,838
% 21 Total l i a b i l i t i e s (Part X, l i n e 2 6 ) . . . . . . . . . . . . 1,960,034,702 1,900,830,877
ZLL 22 Net assets or fund balances Subtract line 21 from line 20 . 3,208,497,458 3,805,493,961
lijaW Signature Block
Under penalties of perjury, I declare that I have examined this return, includinmy knowledge and belief, it is true, correct, and complete Declaration of prepspreparer has any knowledge
SignSignature of officer
Here Kevin J Burns Asst Treasurer & Secretary
Type or print name and title
Print/Type preparer's name Preparers signatureJeffrey D Frank
PaidFirm's name 1- DELOITTE TAX LLP
Pre pare rUse Only Firm's address 1-1111 BAGBY STREET SUITE 4500
HOUSTON, TX 770022591
May the IRS discuss this return with the preparer shown above? (see instructs
For Paperwork Reduction Act Notice, see the separate instructions.

Form 990 (2013) Page 2
Statement of Program Service AccomplishmentsCheck if Schedule 0 contains a response or note to any line in this Part III .F
1 Briefly describe the organization's mission
To provide high quality, cost-effective health care that delivers the best value to the people we serve in a spiritual environment of caring inassociation with internationally recognized teaching and research
2 Did the organization undertake any significant program services during the year which were not listed onthe prior Form 990 or 990-EZ? . . . . . . . . . . . . . . . . . . . . . . fl Yes F No
If "Yes," describe these new services on Schedule 0
3 Did the organization cease conducting, or make significant changes in how it conducts, any programservices? F Yes F No
If "Yes," describe these changes on Schedule 0
4 Describe the organization's program service accomplishments for each of its three largest program services, as measured byexpenses Section 501(c)(3) and 501(c)(4) organizations are required to report the amount of grants and allocations to others,the total expenses, and revenue, if any, for each program service reported
4a (Code ) (Expenses $ 1,157,617,729 including grants of $ 35,710,568 ) (Revenue $ 1,377,414,459
SEE SCHEDULE OCurrently Houston Methodist Hospital operates 849 staffed beds in its Texas Medical Center facilities Houston Methodist Hospital recorded 398,831visits during 2013 which were comprised of 301,478 outpatient visits, 61,043 emergency room visits and 36,310 inpatient visits It also performed 15,876 inpatientsurgeries and 18,588 outpatient surgeries in 2013 The principal medical services available at Houston Methodist Hospital are Anesthesiology, Cardiovascular Surgery,Oral & Maxillofacial-Hospital Dentistry, Dermatology, Family Medicine, General Surgery, Internal Medicine, Atherosclerosis/Lipoprotein, Cardiology, ClinicalImmunology, Gastroenterology, General Medicine, Hematology, Hypertension, Infectious Diseases, Medical Genetics, Metabolic and Endocrine Diseases, NuclearMedicine, Oncology, Pharmacology, Pulmonary Diseases, Renal Diseases, Rheumatology, Neurophysiology, Neurosurgery, Obstetrics and Gynecology,Ophthalmology, Orthopedic Surgery, Otolaryngology-Head & Neck Surgery, Pathology, Pediatrics, Physical Medicine and Rehabilitation, Plastic Surgery, Psychiatry,Radiology, Radiotherapy, and Urology Houston Methodist Hospital also offers a range of additional patient services, including ambulatory surgery, a blood donorcenter, diabetes treatment in a dedicated inpatient unit, a rehabilitation center, a skilled nursing facility, and a broad range of preventive health care instruction,including smoking cessation, stress management, weight control, and cardiac and pulmonary rehabilitation General outpatient services offered by Houston MethodistHospital include audiology, speech pathology, psychiatric services, diagnostic cardiology (including nuclear cardiology, echocardiography, electrocardiography,pacemaker evaluation, and coronary catheterization), chronic renal dialysis, endoscopy, emergency services, general and diagnostic radiology (including fluoroscopy,ultrasound, mammography, myelography, CT scanning, and MRI), nuclear medicine, pathology, peripheral vascular laboratory, dermatology, physical medicine,radiotherapy, sleep studies and neurophysiologic evaluations, and surgery Houston Methodist Hospital operates a multi-organ transplant center Transplants beingperformed at present include kidney, heart, lungs, liver, pancreas, islet cell and bone marrow Houston Methodist Hospital performed the first islet cell transplant inTexas of liver cells from a donors pancreas to the liver of a diabetic patient resulting in donor cells producing insulin Houston Methodist Hospital responds to thecommunity's needs not only through the provision of medical care, but also through education of health professionals and patients, community health education,donations to health care related events and other services, and medical and health research
4b (Code ) (Expenses $ including grants of $ ) (Revenue $
4c (Code ) (Expenses $ including grants of $ ) (Revenue $
4d Other program services (Describe in Schedule 0 )
(Expenses $ including grants of $ ) (Revenue $
4e Total program service expenses- 1,157,617,729
Form 990 (2013)
Form 990 (2013) Page 3
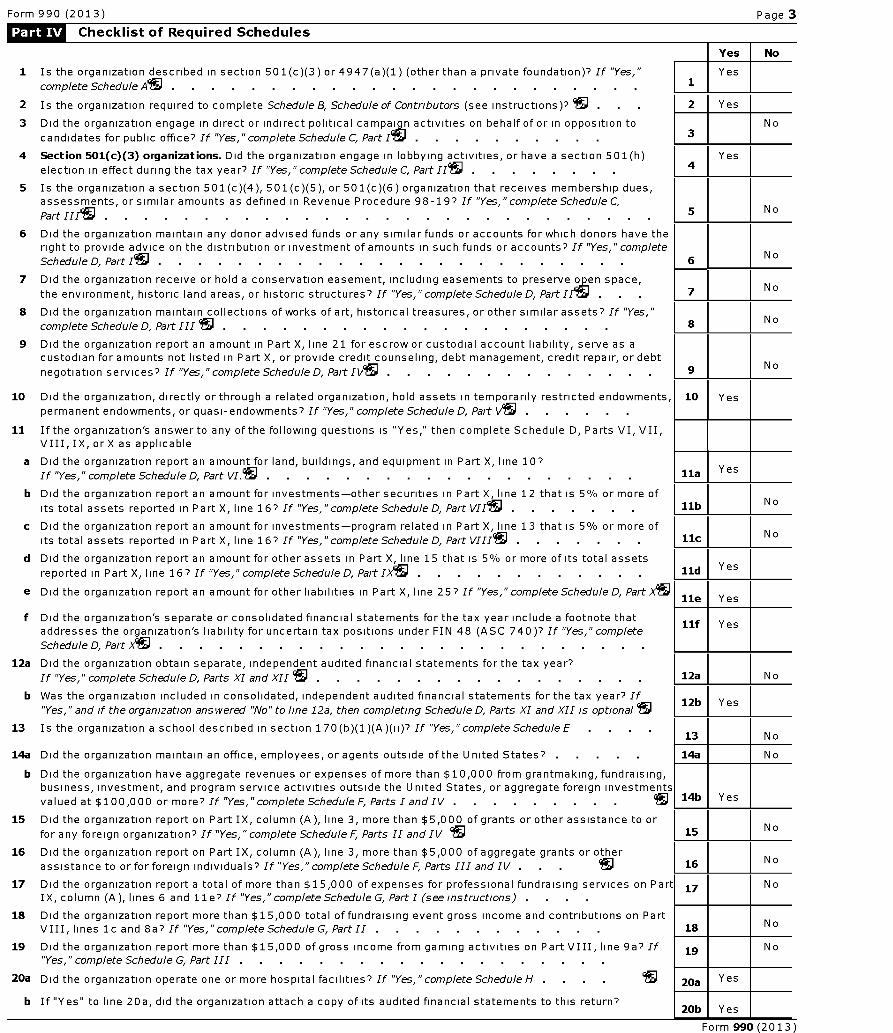
Checklist of Required Schedules
Yes No
1 Is the organization described in section 501(c)(3) or4947(a)(1) (other than a private foundation)? If "Yes," Yes
complete Schedule As . . . . . . . . . . . . . . . . . . . . . . . 1
2 Is the organization required to complete Schedule B, Schedule of Contributors (see instructions)? . 2 Yes
3 Did the organization engage in direct or indirect political campaign activities on behalf of or in opposition to No
candidates for public office? If "Yes,"complete Schedule C, Part Is . . . . . . . . . .
4 Section 501 ( c)(3) organizations . Did the organization engage in lobbying activities, or have a section 501(h) Yes
election in effect during the tax year? If "Yes "complete Schedule C Part II . . . . . . . 4, ,
5 Is the organization a section 501 (c)(4), 501 (c)(5), or 501(c)(6) organization that receives membership dues,assessments, or similar amounts as defined in Revenue Procedure 98-19? If "Yes," complete Schedule C,
Part HIS . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 N o
6 Did the organization maintain any donor advised funds or any similar funds or accounts for which donors have theright to provide advice on the distribution or investment of amounts in such funds or accounts? If "Yes,"complete
Schedule D, Part I . . . . . . . . . . . . . . . . . . . . . . 6N o
7 Did the organization receive or hold a conservation easement, including easements to preserve open space,
the environment, historic land areas, or historic structures? If "Yes,"complete Schedule D, Part IIS . 7 No
8 Did the organization maintain collections of works of art, historical treasures, or other similar assets? If "Yes,"N o
complete Schedule D, Part 111 19 . . . . . . . . . . . . . . . . . . . 8
9 Did the organization report an amount in Part X, line 21 for escrow or custodial account liability, serve as acustodian for amounts not listed in Part X, or provide credit counseling, debt management, credit repair, or debt
negotiation services? If "Yes," complete Schedule D, Part IV . . . . . . . . . . . . 9 No
10 Did the organization, directly or through a related organization, hold assets in temporarily restricted endowments, 10 Yespermanent endowments, or quasi-endowments? If "Yes,"complete Schedule D, Part V .
11 If the organization's answer to any of the following questions is "Yes," then complete Schedule D, Parts VI, VII,VIII, IX, or X as applicable
a Did the organization report an amount for land, buildings, and equipment in Part X, line 10?Yes
If "Yes," complete Schedule D, Part VI. . . . . . . . . . . . . . . . . . . . lla
b Did the organization report an amount for investments-other securities in Part X, line 12 that is 5% or more ofNo
its total assets reported in Part X, line 16? If "Yes," complete Schedule D, Part VIIS . . . . . . llb
c Did the organization report an amount for investments-program related in Part X, line 13 that is 5% or more ofNo
its total assets reported in Part X, line 16? If "Yes," complete Schedule D, Part VIII . . . . . . llc
d Did the organization report an amount for other assets in Part X, line 15 that is 5% or more of its total assetsYes
reported in Part X, line 16? If "Yes," complete Schedule D, Part IX' . . . . . . . . . . . . lid
e Did the organization report an amount for other liabilities in Part X, line 25? If "Yes," complete Schedule D, Part X I lle I Yes
f Did the organization's separate or consolidated financial statements for the tax year include a footnote thatllf Y
addresses the organization's liability for uncertain tax positions under FIN 48 (ASC 740)? If "Yes,"completees
Schedule D, Part X. . . . . . . . . . . . . . . . . . . . . . . . . .
12a Did the organization obtain separate, independent audited financial statements for the tax year?
If "Yes," complete Schedule D, Parts XI and XII . . . . . . . . . . . . . . . . . 12a N o
b Was the organization included in consolidated, independent audited financial statements for the tax year? If12b Yes
"Yes," and if the organization answered "No" to line 12a, then completing Schedule D, Parts XI and XII is optional
13 Is the organization a school described in section 170(b)(1)(A)(ii)? If "Yes," completeScheduleE . .13 No
14a Did the organization maintain an office, employees, or agents outside of the United States? . 14a No
b Did the organization have aggregate revenues or expenses of more than $10,000 from grantmaking, fundraising,business, investment, and program service activities outside the United States, or aggregate foreign investments
valued at $100,000 or more? If "Yes," complete Schedule F, Parts I and IV . . . . . . . . 14b Yes
15 Did the organization report on Part IX, column (A), line 3, more than $5,000 of grants or other assistance to or
for any foreign organization? If "Yes," complete Schedule F, Parts II and IV 95 115 No
16 Did the organization report on Part IX, column (A), line 3, more than $5,000 of aggregate grants or other
assistance to or for foreign individuals? If "Yes," complete Schedule F, Parts III and IV . . 16 No
17 Did the organization report a total of more than $15,000 of expenses for professional fundraising services on Part 17 NoIX, column (A), lines 6 and Ile? If "Yes," complete Schedule G, PartI (seeinstructions) . . . .
18 Did the organization report more than $15,000 total of fundraising event gross income and contributions on PartVIII, lines 1c and 8a? If "Yes," complete Schedule G, Part II . . . . . . . . . . . 18 No
19 Did the organization report more than $15,000 of gross income from gaming activities on Part VIII, line 9a? If 19 No"Yes," complete Schedule G, Part III . . . . . . . . . . . . . . . . . . .
20a Did the organization operate one or more hospital facilities? If "Yes,"completeScheduleH . . 20a Yes
b If "Yes" to line 20a, did the organization attach a copy of its audited financial statements to this return?20b I Yes
Form 990 (2013)
Form 990 (2013) Page 4
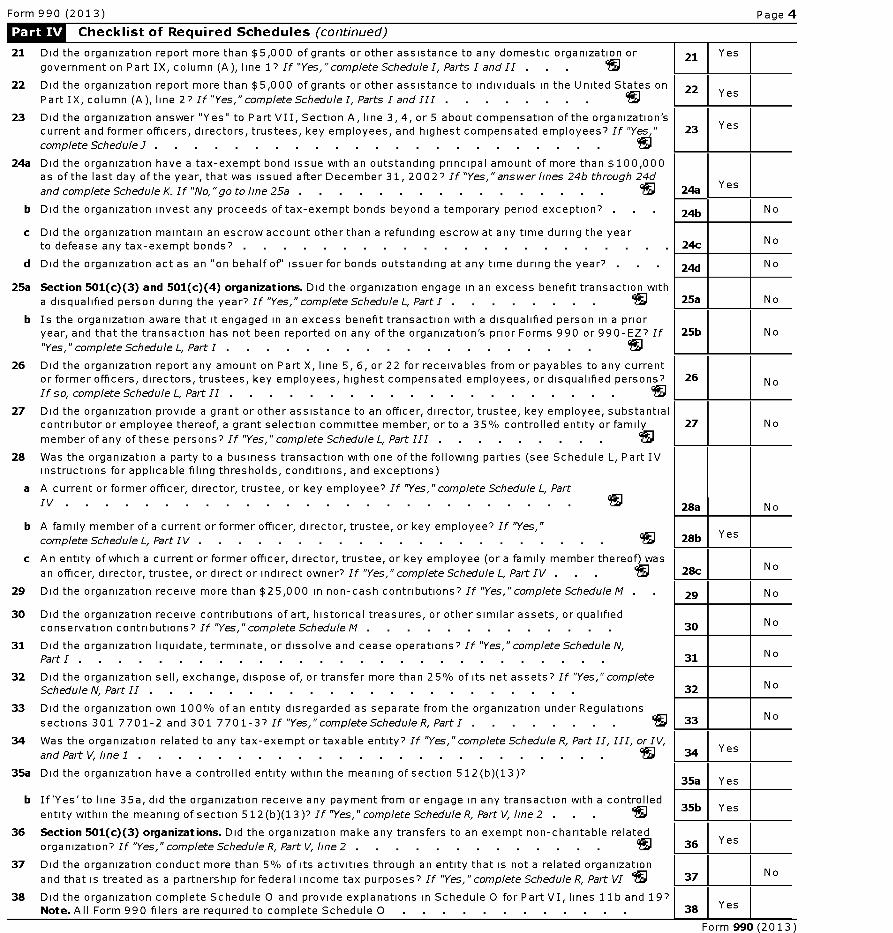
Checklist of Required Schedules (continued)
21 Did the organization report more than $5,000 of grants or other assistance to any domestic organization or
government on Part IX, column (A), line 1? If "Yes, "complete Schedule I, Parts I and II . . . IN
22 Did the organization report more than $5,000 of grants or other assistance to individuals in the United States on
Part IX, column (A), line 2? If "Yes," complete Schedule I, Parts I and III . . . . . . . . S
23 Did the organization answer "Yes" to Part VII, Section A, line 3, 4, or 5 about compensation of the organization'scurrent and former officers, directors, trustees, key employees, and highest compensated employees? If "Yes,"
complete Schedule J . . . . . . . . . . . . . . . . . . . . . . . IN
24a Did the organization have a tax-exempt bond issue with an outstanding principal amount of more than $100,000as of the last day of the year, that was issued after December 31, 2002? If"Yes," answer lines 24b through 24d
and complete Schedule K. If "No,"go to line 25a . . . . . . . . . . . . . . . .
b Did the organization invest any proceeds of tax-exempt bonds beyond a temporary period exception?
c Did the organization maintain an escrow account other than a refunding escrow at any time during the yearto defease any tax-exempt bonds? .
d Did the organization act as an on behalf of issuer for bonds outstanding at any time during the year?
25a Section 501(c)( 3) and 501 ( c)(4) organizations . Did the organization engage in an excess benefit transaction with
a disqualified person during the year? If "Yes," complete Schedule L, Part I . . . . . . . .
b Is the organization aware that it engaged in an excess benefit transaction with a disqualified person in a prioryear, and that the transaction has not been reported on any of the organization's prior Forms 990 or 990-EZ? If
"Yes," complete Schedule L, Part I . . . . . . . . . . . . . . . . . . . S
26 Did the organization report any amount on Part X, line 5, 6, or 22 for receivables from or payables to any currentor former officers, directors, trustees, key employees, highest compensated employees, or disqualified persons?
If so, complete Schedule L, Part II . . . . . . . . . . . . . . . . . . . .
27 Did the organization provide a grant or other assistance to an officer, director, trustee, key employee, substantialcontributor or employee thereof, a grant selection committee member, or to a 35% controlled entity or family
member of any of these persons? If "Yes," complete Schedule L, Part III . . . . . . . . . S
28 Was the organization a party to a business transaction with one of the following parties (see Schedule L, Part IVinstructions for applicable filing thresholds, conditions, and exceptions)
a A current or former officer, director, trustee, or key employee? If "Yes,"complete Schedule L, Part
IV . . . . . . . . . . . . . . . . . . . . . . . . . . IN
b A family member of a current or former officer, director, trustee, or key employee? If "Yes,"
complete Schedule L, Part IV . . . . . . . . . . . . . . . . . . . . .
c A n entity of which a current or former officer, director, trustee, or key employee (or a family member thereof) was
an officer, director, trustee, or direct or indirect owner? If "Yes,"complete Schedule L, Part IV . . .
29 Did the organization receive more than $25,000 in non-cash contributions? If "Yes,"completeScheduleM
30 Did the organization receive contributions of art, historical treasures , or other similar assets, or qualifiedconservation contributions? If "Yes," complete Schedule M . . . . . . . . . . . . .
31 Did the organization liquidate, terminate , or dissolve and cease operations? If "Yes," complete Schedule N,PartI . . . . . . . . . . . . . . . . . . . . . . . . . . .
32 Did the organization sell, exchange , dispose of, or transfer more than 25% of its net assets? If "Yes, " completeSchedule N, Part II . . . . . . . . . . . . . . . . . . . . . .
33 Did the organization own 100% of an entity disregarded as separate from the organization under Regulations
sections 301 7701-2 and 301 7701-3? If "Yes," complete Schedule R, PartI . . . . . . . .
34 Was the organization related to any tax-exempt or taxable entity? If "Yes,"complete Schedule R, Part II, III, orIV,
and Part V, line 1 . . . . . . . . . . . . . . . . . . . . . . . .
35a Did the organization have a controlled entity within the meaning of section 512(b)(13)?
b If'Yes'to line 35a, did the organization receive any payment from or engage in any transaction with a controlled
entity within the meaning of section 512 (b)(13 )? If "Yes,"complete Schedule R, Part V, line 2 . . . S
36 Section 501(c)( 3) organizations. Did the organization make any transfers to an exempt non-charitable related
organization? If "Yes,"complete Schedule R, Part V, line 2 . . . . . . . . . . . . . IN
37 Did the organization conduct more than 5 % of its activities through an entity that is not a related organization
and that is treated as a partnership for federal income tax purposes? If "Yes," complete Schedule R, Part VI S
38 Did the organization complete Schedule 0 and provide explanations in Schedule 0 for Part VI, lines 1 lb and 19?Note . All Form 990 filers are required to complete Schedule 0 .
23 Yes
24a Yes
24b N o
24c No
24d No
25a N o
25b No
26 N o
27 N o
28a N o
28b Yes
28c N o
29 No
30 N o
31 No
32 No
33 No
34 Yes
35a Yes
35b Yes
36 1 Yes
No
Form 990 (2013)
Form 990 (2013) Page 5
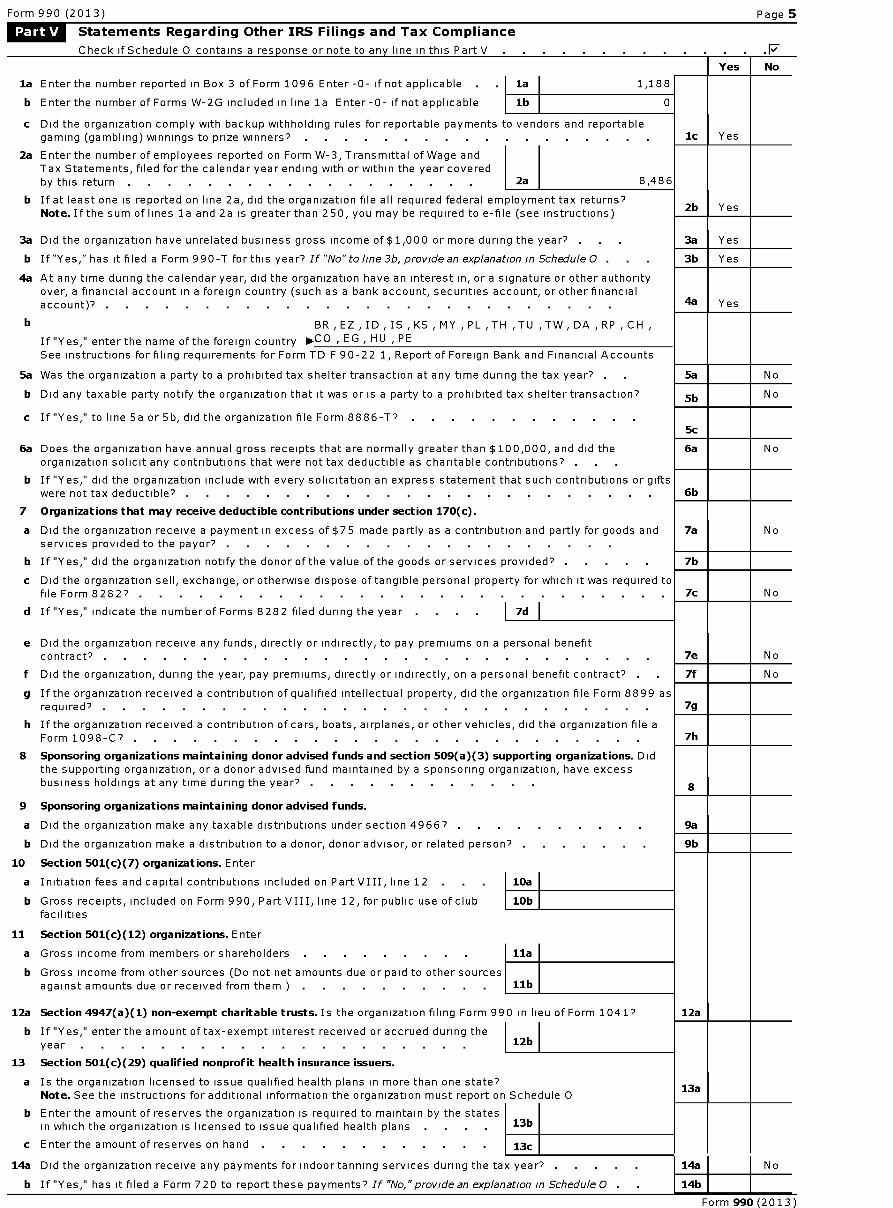
-Statements Regarding Other IRS Filings and Tax ComplianceMEWCheck if Schedule 0 contains a res p onse or note to an y line in this Part V .F
Yes No
la Enter the number reported in Box 3 of Form 1096 Enter -0- if not applicable . la 1,188
b Enter the number of Forms W-2G included in line la Enter-0- if not applicable lb 0
c Did the organization comply with backup withholding rules for reportable payments to vendors and reportablegaming (gambling) winnings to prize winners? . . . . . . . . . . . . . . . . . 1c Yes
2a Enter the number of employees reported on Form W-3, Transmittal of Wage andTax Statements, filed for the calendar year ending with or within the year coveredby this return . . . . . . . . . . . . . . . . . 2a 8,486
b If at least one is reported on line 2a, did the organization file all required federal employment tax returns?Note . If the sum of lines la and 2a is greater than 250 you may be required to e-file (see instructions)
2b Yes,
3a Did the organization have unrelated business gross income of $1,000 or more during the year? . . 3a Yes
b If "Yes," has it filed a Form 990-T for this year? If 'No" to line 3b, provide an explanation in Schedule O . . . 3b Yes
4a At any time during the calendar year, did the organization have an interest in, or a signature or other authorityover, a financial account in a foreign country (such as a bank account, securities account, or other financialaccount)? . . . . . . . . . . . . . . . . . . . . . . . . . 4a Yes
b BR,EZ,ID,IS,KS,MY,PL,TH,TU,TW,DA,RP,CH,
If "Yes," enter the name of the foreign country O-CO , EG , HU , PE
See instructions for filing requirements for Form TD F 90-22 1, Report of Foreign Bank and Financial Accounts
5a Was the organization a party to a prohibited tax shelter transaction at any time during the tax year? . . 5a No
b Did any taxable party notify the organization that it was or is a party to a prohibited tax shelter transaction? 5b No
c If "Yes," to line 5a or 5b, did the organization file Form 8886-T?
6a Does the organization have annual gross receipts that are normally greater than $100,000, and did theorganization solicit any contributions that were not tax deductible as charitable contributions? . .
b If "Yes," did the organization include with every solicitation an express statement that such contributions or giftswere not tax deductible? . . . . . . . . . . . . . . . . . . . . . . . .
7 Organizations that may receive deductible contributions under section 170(c).
a Did the organization receive a payment in excess of $75 made partly as a contribution and partly for goods andservices provided to the payor? .
b If "Yes," did the organization notify the donor of the value of the goods or services provided? . .
c Did the organization sell, exchange, or otherwise dispose of tangible personal property for which it was required tofile Form 82827 . . . . . . . . . . . . . . . . . . . . . . . . . . .
d If "Yes," indicate the number of Forms 8282 filed during the year . I 7d
e Did the organization receive any funds, directly or indirectly, to pay premiums on a personal benefitcontract? . . . . . . . . . . . . . . . . . . . . . . . . . . . .
f Did the organization, during the year, pay premiums, directly or indirectly, on a personal benefit contract? . .
g If the organization received a contribution of qualified intellectual property, did the organization file Form 8899 asrequired? .
h If the organization received a contribution of cars, boats, airplanes, or other vehicles, did the organization file aForm 1098-C? .
8 Sponsoring organizations maintaining donor advised funds and section 509(a )( 3) supporting organizations. Didthe supporting organization, or a donor advised fund maintained by a sponsoring organization, have excessbusiness holdings at any time during the year? .
9 Sponsoring organizations maintaining donor advised funds.
a Did the organization make any taxable distributions under section 4966? . .
b Did the organization make a distribution to a donor, donor advisor, or related person? . .
10 Section 501(c)( 7) organizations. Enter
a Initiation fees and capital contributions included on Part VIII, line 12 . 10a
b Gross receipts, included on Form 990, Part VIII, line 12, for public use of club 10bfacilities
11 Section 501(c)( 12) organizations. Enter
a Gross income from members or shareholders . . . . . . . . 11a
b Gross income from other sources (Do not net amounts due or paid to other sourcesagainst amounts due or received from them ) . . . . . . . . . 11b
12a Section 4947( a)(1) non-exempt charitable trusts. Is the organization filing Form 990 in lieu of Form 1041?
b If "Yes," enter the amount of tax-exempt interest received or accrued during theyear . . . . . . . . . . . . . . . . . . . 12b
13 Section 501(c)( 29) qualified nonprofit health insurance issuers.
a Is the organization licensed to issue qualified health plans in more than one state?Note . See the instructions for additional information the organization must report on Schedule 0
b Enter the amount of reserves the organization is required to maintain by the statesin which the organization is licensed to issue qualified health plans 13b
c Enter the amount of reserves on hand 13c
5c
6a N o
6b
7a N o
7b
7c N o
7e N o
7f N o
7g
7h
8
9a
9b
12a
13a
14a Did the organization receive any payments for indoor tanning services during the tax year? . . . 14a No
b If "Yes," has it filed a Form 720 to report these payments? If "No,"provide an explanation in Schedule 0 . 14b
Form 990 (2013)

Form 990 (2013) Page 6
Governance , Management, and Disclosure For each "Yes" response to lines 2 through 7b below, and for a"No" response to lines 8a, 8b, or 1Ob below, describe the circumstances, processes, or changes in Schedule 0.See instructions.Check if Schedule 0 contains a response or note to any line in this Part VI .F
Section A . Governing Body and Management
Yes No
la Enter the number of voting members of the governing body at the end of the taxla 23
year
If there are material differences in voting rights among members of the governingbody, or if the governing body delegated broad authority to an executive committeeor similar committee, explain in Schedule 0
b Enter the number of voting members included in line la, above, who areindependent . . . . . . . . . . . . . . . . . . lb 21
2 Did any officer, director, trustee, or key employee have a family relationship or a business relationship with anyother officer, director, trustee, or key employee? 2 No
3 Did the organization delegate control over management duties customarily performed by or under the direct3 No
supervision of officers, directors or trustees, or key employees to a management company or other person?
4 Did the organization make any significant changes to its governing documents since the prior Form 990 wasfiled? . . . . . . . . . . . . . . . . . . . . . . . . . . 4 No
5 Did the organization become aware during the year of a significant diversion of the organization's assets? 5 No
6 Did the organization have members or stockholders? 6 No
7a Did the organization have members, stockholders, or other persons who had the power to elect or appoint one ormore members of the governing body? . . . . . . . . . . . . . . . . . . . 7a Yes
b Are any governance decisions of the organization reserved to (or subject to approval by) members, stockholders, 7b Yesor persons other than the governing body?
8 Did the organization contemporaneously document the meetings held or written actions undertaken during theyear by the following
a The governing body? . . . . . . . . . . . . . . . . . . . . . . . . 8a Yes
b Each committee with authority to act on behalf of the governing body? 8b Yes
9 Is there any officer, director, trustee, or key employee listed in Part VII, Section A, who cannot be reached at theorganization's mailing address? If "Yes,"provide the names and addresses in Schedule 0 . . . . . . 9 No
Section B. Policies ( This Section B requests information about p olicies not required b y the Internal Revenue Code.)Yes No
10a Did the organization have local chapters, branches, or affiliates? 10a Yes
b If "Yes," did the organization have written policies and procedures governing the activities of such chapters,affiliates, and branches to ensure their operations are consistent with the organization's exempt purposes? 10b Yes
11a Has the organization provided a complete copy of this Form 990 to all members of its governing body before filingthe form? . . . . . . . . . . . . . . . . . . . . . . . . . . . 11a Yes
b Describe in Schedule 0 the process, if any, used by the organization to review this Form 990
12a Did the organization have a written conflict of interest policy? If "No,"go to line 13 . 12a Yes
b Were officers, directors, or trustees, and key employees required to disclose annually interests that could giverise to conflicts? . . . . . . . . . . . . . . . . . . . . . . . . . 12b Yes
c Did the organization regularly and consistently monitor and enforce compliance with the policy? If "Yes," describein Schedule 0 how this was done . 12c Yes
13 Did the organization have a written whistleblower policy? 13 Yes
14 Did the organization have a written document retention and destruction policy? . 14 Yes
15 Did the process for determining compensation of the following persons include a review and approval byindependent persons, comparability data, and contemporaneous substantiation of the deliberation and decision?
a The organization's CEO, Executive Director, or top management official 15a Yes
b Other officers or key employees of the organization 15b Yes
If "Yes" to line 15a or 15b, describe the process in Schedule 0 (see instructions)
16a Did the organization invest in, contribute assets to, or participate in a joint venture or similar arrangement with ataxable entity during the year? . . . . . . . . . . . . . . . . . . . . . 16a No
b If "Yes," did the organization follow a written policy or procedure requiring the organization to evaluate itsparticipation in joint venture arrangements under applicable federal tax law, and take steps to safeguard theorganization's exempt status with respect to such arrangements? . . . . . . . . . . 16b
Section C. Disclosure
17 List the States with which a copy of this Form 990 is required to be filed-
18 Section 6104 requires an organization to make its Form 1023 (or 1024 if applicable), 990, and 990-T (501(c)(3 )s only) available for public inspection Indicate how you made these available Check all that apply
fl Own website fl Another's website F Upon request fl Other (explain in Schedule O )
19 Describe in Schedule 0 whether (and if so, how) the organization made its governing documents, conflict ofinterest policy, and financial statements available to the public during the tax year
20 State the name, physical address, and telephone number of the person who possesses the books and records of the organization-Edward L Tyrrell FACHE 6565 Fannin GB240Houston,TX 77030 (832)667-6160
Form 990 (2013)
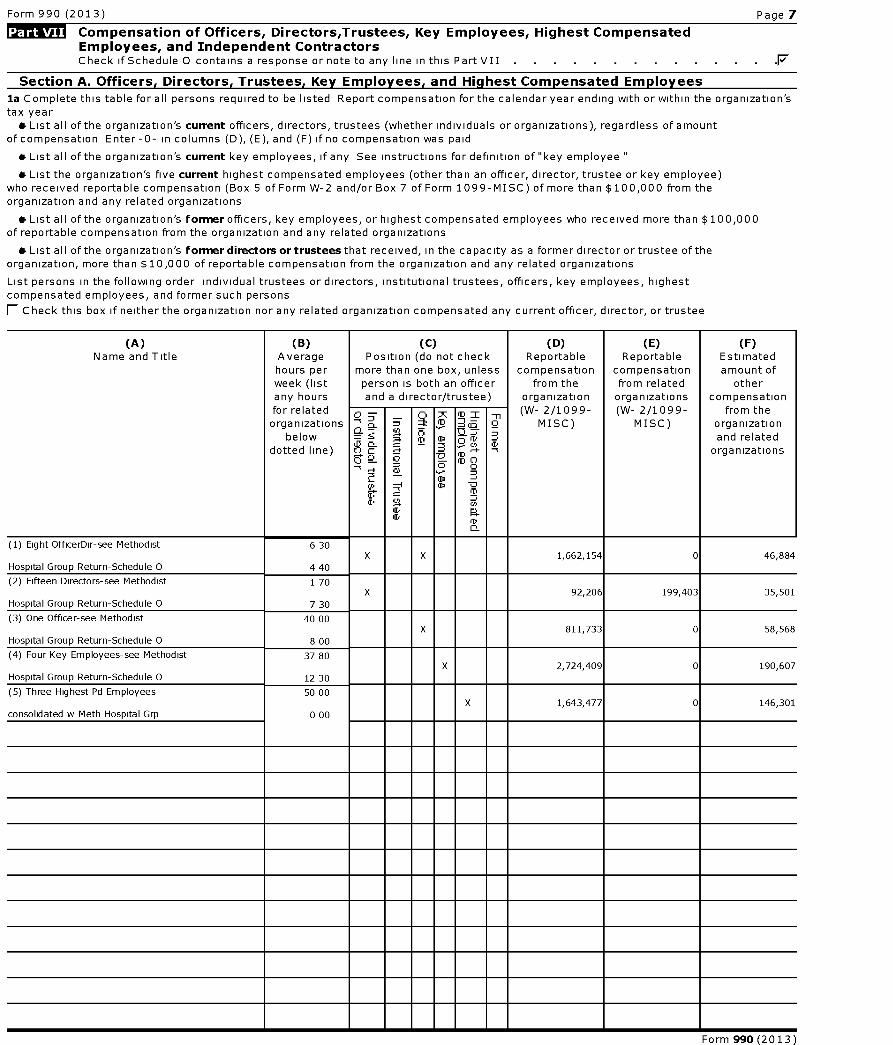
Form 990 (2013) Page 7
Compensation of Officers, Directors ,Trustees, Key Employees, Highest CompensatedEmployees , and Independent ContractorsCheck if Schedule 0 contains a response or note to any line in this Part VII .F
Section A. Officers, Directors, Trustees, Kev Employees, and Highest Compensated Employees
la Complete this table for all persons required to be listed Report compensation for the calendar year ending with or within the organization'stax year* List all of the organization's current officers, directors, trustees (whether individuals or organizations), regardless of amount
of compensation Enter-0- in columns (D), (E), and (F) if no compensation was paid
* List all of the organization's current key employees, if any See instructions for definition of "key employee "
* List the organization's five current highest compensated employees (other than an officer, director, trustee or key employee)who received reportable compensation (Box 5 of Form W-2 and/or Box 7 of Form 1099-MISC) of more than $100,000 from theorganization and any related organizations
* List all of the organization 's former officers, key employees, or highest compensated employees who received more than $100,000of reportable compensation from the organization and any related organizations
* List all of the organization's former directors or trustees that received, in the capacity as a former director or trustee of theorganization, more than $10,000 of reportable compensation from the organization and any related organizations
List persons in the following order individual trustees or directors, institutional trustees, officers, key employees, highestcompensated employees, and former such persons
1 Check this box if neither the organization nor any related organization compensated any current officer, director, or trustee
(A) (B) (C) (D) ( E) (F)Name and Title Average Position (do not check Reportable Reportable Estimated
hours per more than one box, unless compensation compensation amount ofweek (list person is both an officer from the from related otherany hours and a director/trustee) organization organizations compensationfor relatedorganizations
belowdotted line)
cSaS
7
o
m_ Q(o
0r
mc)
T
LD
(W- 2/1099-MISC)
(W- 2/1099-MISC)
from theorganizationand related
organizations
ID
J.
V
(1) Eight OfficerDir-see Methodist 6 30X X 1,662,154 0 46,884
Hospital Group Return-Schedule 0 4 40
(2) Fifteen Directors-see Methodist 1 70X 92,206 199,403 35,501
Hospital Group Return-Schedule 0 7 30
(3) One Officer-see Methodist 40 00X 811,733 0 58,568
Hospital Group Return-Schedule 0 8 00
(4) Four Key Employees-see Methodist 37 80X 2,724,409 0 190,607
Hospital Group Return-Schedule 0 12 30
(5) Three Highest Pd Employees 50 00X 1,643,477 0 146,301
consolidated w Meth Hospital Grp 0 00
Form 990 (2013)
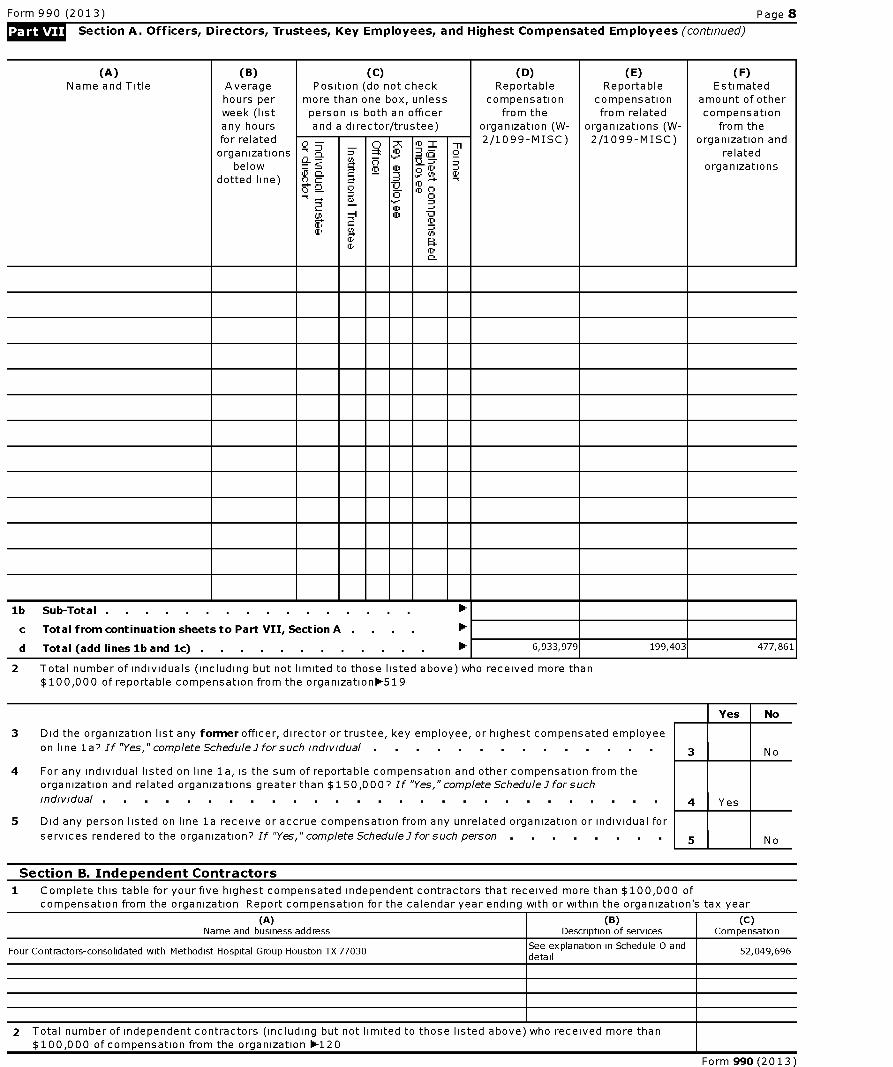
Form 990 (2013) Page 8
Section A. Officers, Directors , Trustees, Key Employees, and Highest Compensated Employees (continued)
(A)Name and Title
(B)Averagehours perweek (listany hours
(C)Position (do not check
more than one box, unlessperson is both an officerand a director/trustee)
(D)Reportable
compensationfrom the
organization (W-
( E)Reportable
compensationfrom related
organizations (W-
(F)Estimated
amount of othercompensation
from thefor relatedorganizations
belowdotted line)
0--
C:SL
a
747.
;3
m_
;rl
!
M=
boo
fD
ur
T
a
2/1099-MISC) 2/1099-MISC) organization andrelated
organizations
lb Sub-Total . . . . . . . . . . . . . . . .
c Total from continuation sheets to Part VII, Section A . . . .
d Total ( add lines lb and 1c) . . . . . . . . . . . . 0- 6,933,979 199,403 477,861
Total number of individuals (including but not limited to those listed above) who received more than$100,000 of reportable compensation from the organization-519
No
Did the organization list any former officer, director or trustee, key employee, or highest compensated employee
on line la? If "Yes," complete Schedule Jfor such individual . . . . . . . . . . . . . 3 No
4 For any individual listed on line la, is the sum of reportable compensation and other compensation from theorganization and related organizations greater than $150,0007 If "Yes," complete Schedule -7 for such
individual . . . . . . . . . . . . . . . . . . . . . . . . . . .
Did any person listed on line la receive or accrue compensation from any unrelated organization or individual for
services rendered to the organization? If "Yes," complete Schedule Jfor such person . . . . . . . 5 No
Section B. Independent Contractors
1 Complete this table for your five highest compensated independent contractors that received more than $100,000 ofcompensation from the organization Report compensation for the calendar year ending with or within the organization's tax year
(A)Name and business address
(B)Description of services
(C)Compensation
Four Contractors-consolidated with Methodist Hospital Group Houston TX 77030See explanation in Schedule 0 anddetail
52,049,696
2 Total number of independent contractors (including but not limited to those listed above) who received more than$100,000 of compensation from the organization 0-120
Form 990 (2013)
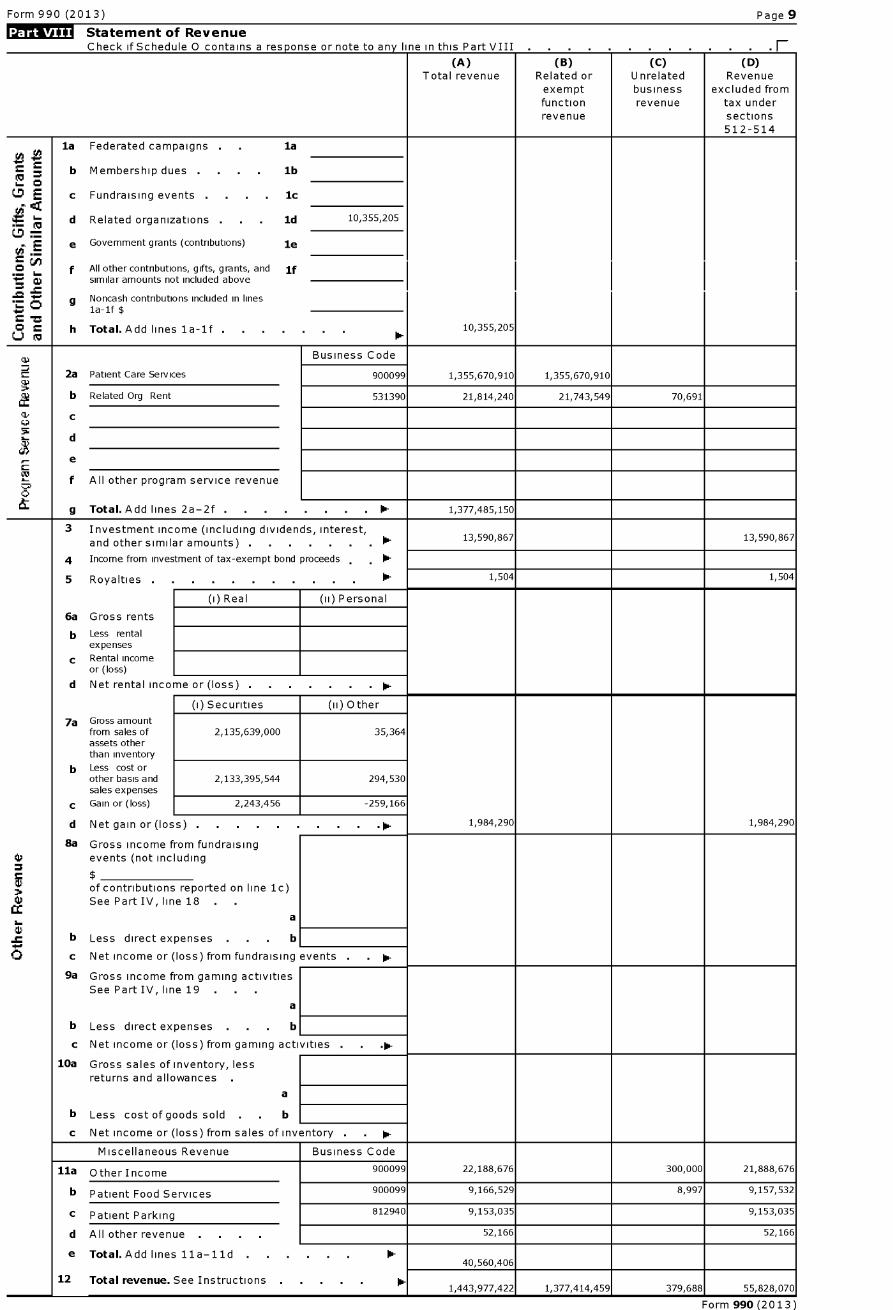
Form 990 (2013) Page 9
Statement of RevenueCheck if Schedule 0 contains a response or note to any line in this Part VIII F
(A) (B) (C) (D)Total revenue Related or Unrelated Revenue
exempt business excluded fromfunction revenue tax underrevenue sections
512-514
la Federated campaigns . laZ
r = b Membership dues . . . . lb6- 0
0 E c Fundraising events . . . . 1c
d Related organizations . ld 10,355,205
tJ'E e Government grants ( contributions) le
V f All other contributions, gifts, grants, and if^ similar amounts not included above
g Noncash contributions included in linesla-If $
h Total . Add lines la -1f . 10,355,205
Business Code
2a Patient Care Services 900099 1,355,670,910 1,355,670,910
a2S
b Related Org Rent 531390 21,814,240 21,743,549 70,691
4 C
d
e
f All other program service revenue
g Total . Add lines 2a -2f . . . . . . . . 0- 1,377,485,150
3 Investment income ( including dividends , interest,10-and other similar amounts ) .
13,590,867 13,590,867
4 Income from investment of tax- exempt bond proceeds , . 0-
5 Royalties . . . . . . . . . . . 0- 1,504 1,504
(i) Real (ii) Personal
6a Gross rents
b Less rentalexpenses
c Rental incomeor (loss)
d Net rental inco me or ( loss) . . lim-
(i) Securities (ii) Other
7a Gross amountfrom sales of 2,135,639,000 35,364assets otherthan inventory
b Less cost orother basis and 2,133,395,544 294,530sales expenses
c Gain or (loss) 2,243,456 -259,166
d Net gain or ( loss) . lim- 1,984,290 1,984,290
8a Gross income from fundraisingW events ( not including
$
of contributions reported on line 1c)See Part IV, line 18
a
s b Less direct expenses . b
c Net income or (loss) from fundraising events . . 0-
9a Gross income from gaming activitiesSee Part IV , line 19 . .
a
b Less direct expenses . b
c Net income or (loss) from gaming acti vities . . .0-
10a Gross sales of inventory, lessreturns and allowances .
a
b Less cost of goods sold . b
c Net income or (loss ) from sales of inventory . lim-
Miscellaneous Revenue Business Code
11a Other Income 900099 22,188,676 300,000 21,888,676
b Patient Food Services 900099 9,166,529 8,997 9,157,532
c Patient Parking 812940 9,153,035 9,153,035
d All other revenue . . . 52,166 52,166
e Total.Add lines 11a-11d 10-40,560,406
12 Total revenue . See Instructions 0- 11,443,977,422 1,377,414,459 379,688 55,828,070
Form 990 (2013)
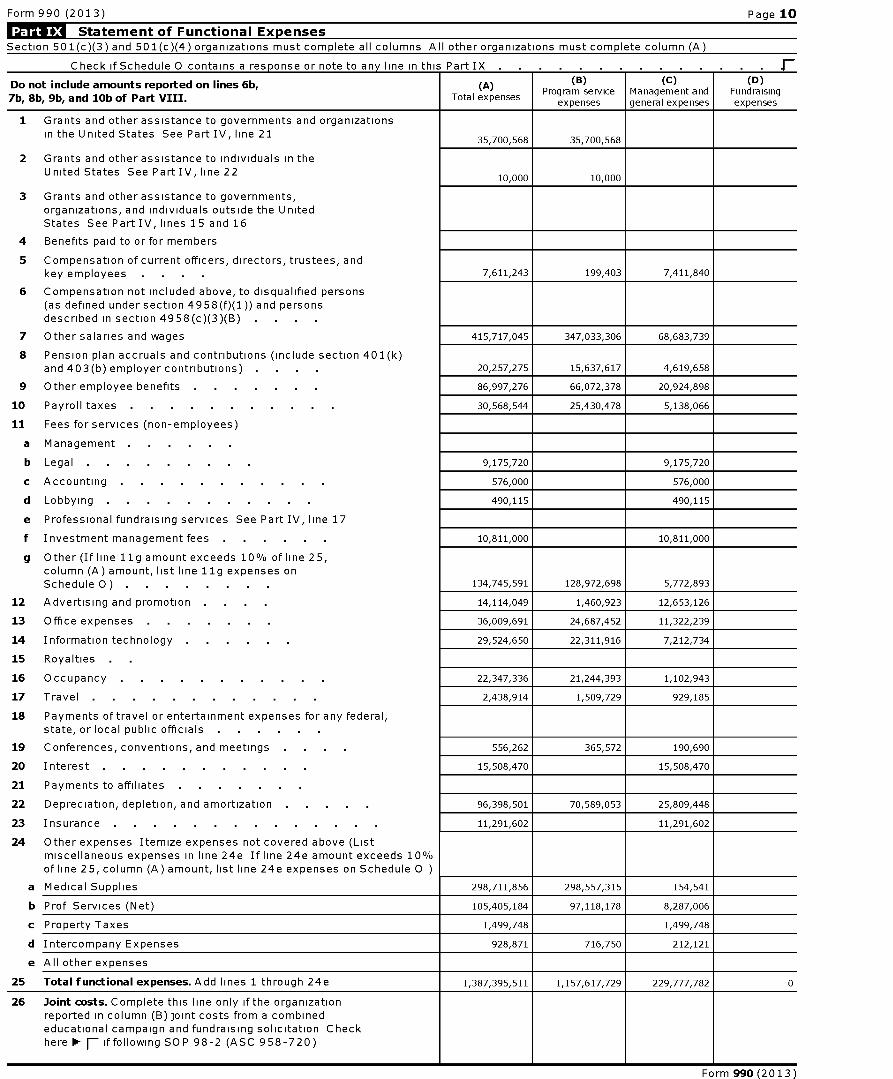
Form 990 (2013) Page 10
Statement of Functional Expenses
Section 501(c)(3) and 501(c)(4) organizations must complete all columns All other organizations must complete column (A)
Check if Schedule 0 contains a response or note to any line in this Part IX . . . . . . . . . . . . . .
Do not include amounts reported on lines 6b,
7b, 8b, 9b, and 10b of Part VIII .
( A)
Total expenses
(B)Program service
expenses
(C)Management andgeneral expenses
(D)Fundraisingexpenses
1 Grants and other assistance to governments and organizations
in the United States See Part IV, line 2135,700,568 35,700,568
2 Grants and other assistance to individuals in theUnited States See Part IV, line 22
10,000 10,000
3 Grants and other assistance to governments,organizations , and individuals outside the UnitedStates See Part IV, lines 15 and 16
4 Benefits paid to or for members
5 Compensation of current officers, directors , trustees, and
key employees 7,611,243 199,403 7,411,840
6 Compensation not included above, to disqualified persons(as defined under section 4958(f)(1)) and personsdescribed in section 4958( c)(3)(B)
7 Other salaries and wages 415,717,045 347,033,306 68,683,739
8 Pension plan accruals and contributions ( include section 401(k)and 403(b) employer contributions ) 20 ,257,275 15,637,617 4,619,658
9 Other employee benefits 86 ,997,276 66,072,378 20,924,898
10 Payroll taxes 30,568,544 25,430,478 5,138,066
11 Fees for services ( non-employees)
a Management . .
b Legal 9,175 ,720 9,175,720
c Accounting 576,000 576,000
d Lobbying 490,115 490,115
e Professional fundraising services See Part IV, line 17
f Investment management fees 10,811 ,000 10,811,000
g Other ( If line 11g amount exceeds 10 % of line 25,
column ( A) amount, list line 11g expenses on
Schedule 0 ) . 134,745,591 128,972,698 5,772,893
12 Advertising and promotion 14,114,049 1,460,923 12,653,126
13 Office expenses 36,009,691 24,687,452 11,322,239
14 Information technology 29,524,650 22,311,916 7,212,734
15 Royalties
16 Occupancy 22,347,336 21,244,393 1,102,943
17 Travel 2,438,914 1,509,729 929,185
18 Payments of travel or entertainment expenses for any federal,state, or local public officials
19 Conferences , conventions , and meetings 556,262 365,572 190,690
20 Interes t 15, 508,470 15, 508,470
21 Payments to affiliates
22 Depreciation , depletion, and amortization 96,398,501 70,589,053 25,809,448
23 Insurance . . . . . . . . . . . . . 11,291,602 11,291,602
24 Other expenses Itemize expenses not covered above (Listmiscellaneous expenses in line 24e If line 24e amount exceeds 10%of line 25, column ( A) amount, list line 24e expenses on Schedule 0
a Medical Supplies 298,711,856 298,557,315 154,541
b Prof Services (Net) 105,405,184 97,118,178 8,287,006
c Property Taxes 1,499,748 1,499,748
d Intercompany Expenses 928,871 716,750 212,121
e All other expenses
25 Total functional expenses. Add lines 1 through 24e 1,387,395,511 1,157,617,729 229,777,782 0
26 Joint costs. Complete this line only if the organizationreported in column ( B) joint costs from a combinededucational campaign and fundraising solicitation Checkhere F- if following SOP 98-2 (ASC 958-720)
Form 990 (2013)
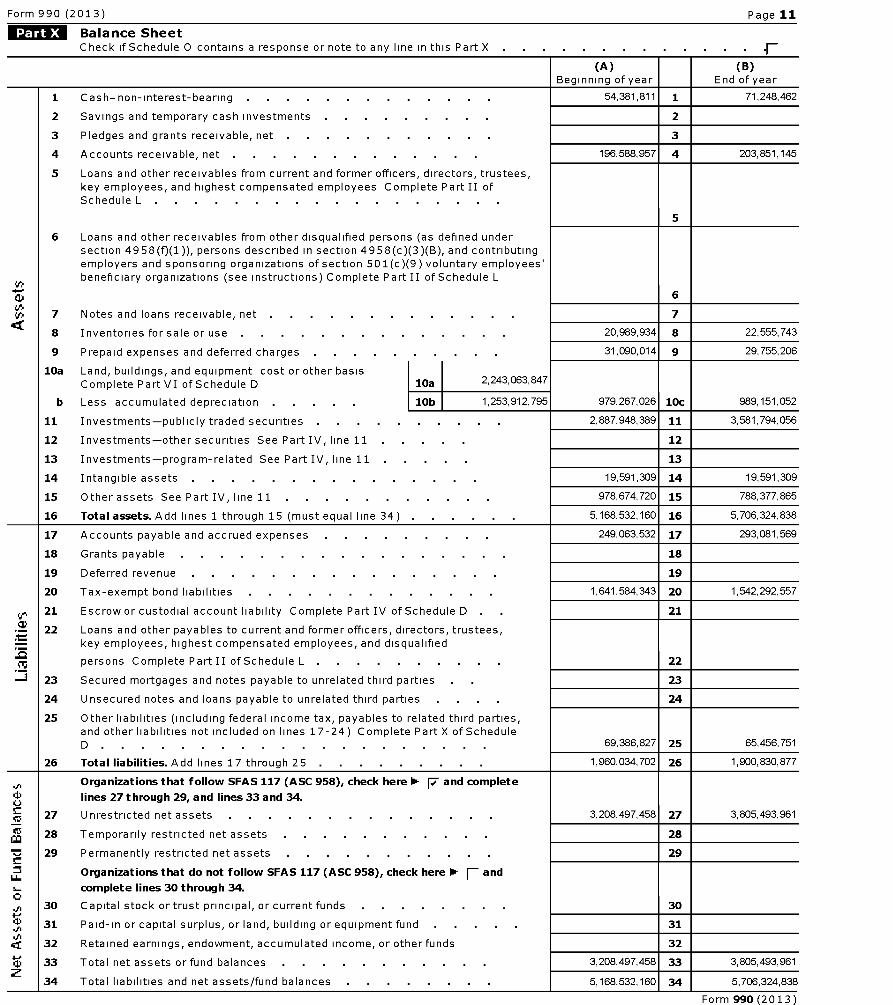
Form 990 (2013) Page 11
Balance SheetCheck if Schedule 0 contains a response or note to any line in this Part X F
(A) (B)Beginning of year End of year
1 Cash-non-interest-bearing 54,381,811 1 71,248,462
2 Savings and temporary cash investments 2
3 Pledges and grants receivable, net 3
4 Accounts receivable, net . . . . . . . . . . . . 196,588,957 4 203,851,145
5 Loans and other receivables from current and former officers, directors, trustees,key employees, and highest compensated employees Complete Part II ofSchedule L . .
5
6 Loans and other receivables from other disqualified persons (as defined undersection 4958(f)(1)), persons described in section 4958(c)(3)(B), and contributingemployers and sponsoring organizations of section 501(c)(9) voluntary employees'beneficiary organizations (see instructions) Complete Part II of Schedule L
6
7 Notes and loans receivable, net 7'cc
8 Inventories for sale or use 20,989,934 8 22,555,743
9 Prepaid expenses and deferred charges . 31,090,014 9 29,755,206
10a Land, buildings, and equipment cost or other basisComplete Part VI of Schedule D 10a 2,243,063,847
b Less accumulated depreciation . . . . 10b 1 ,253,912,795 979,267,026 10c 989,151,052
11 Investments-publicly traded securities . 2,887,948,389 11 3,581,794,056
12 Investments-other securities See Part IV, line 11 12
13 Investments-program-related See Part IV, line 11 13
14 Intangible assets . . . . . . . . . . . . . . 19,591,309 14 19,591,309
15 Other assets See Part IV, line 11 978, 674, 720 15 788, 377, 865
16 Total assets . Add lines 1 through 15 (must equal line 34) . 5,168,532,160 16 5,706,324,838
17 Accounts payable and accrued expenses . . . . . . . . 249,063,532 17 293,081,569
18 Grants payable . . . . . . . . . . . . . . . . 18
19 Deferred revenue . . . . . . . . . . . . . . . 19
20 Tax-exempt bond liabilities . . . . . . . . . . . . 1,641,584,343 20 1,542,292,557
21 Escrow or custodial account liability Complete Part IV of Schedule D . 21
22 Loans and other payables to current and former officers, directors, trustees,key employees, highest compensated employees, and disqualified
persons Complete Part II of Schedule L . 22
23 Secured mortgages and notes payable to unrelated third parties 23
24 Unsecured notes and loans payable to unrelated third parties 24
25 Other liabilities (including federal income tax, payables to related third parties,and other liabilities not included on lines 17-24) Complete Part X of ScheduleD . 69, 386, 827 25 65, 456, 751
26 Total liabilities . Add lines 17 through 25 . 1,960,034,702 26 1,900,830,877
Organizations that follow SFAS 117 (ASC 958), check here 1- F and complete
lines 27 through 29, and lines 33 and 34.
C5 27 Unrestricted net assets . . . . . . . . . . . . . 3,208,497,458 27 3,805,493,961
Mca 28 Temporarily restricted net assets 28
r29 Permanently restricted net assets 29
_Organizations that do not follow SFAS 117 (ASC 958), check here 1 andFW_complete lines 30 through 34.
30 Capital stock or trust principal, or current funds 30
31 Paid-in or capital surplus, or land, building or equipment fund 31
32 Retained earnings, endowment, accumulated income, or other funds 32
33 Total net assets or fund balances . . . . . . . . . . 3,208,497,458 33 3,805,493,961
34 Total liabilities and net assets/fund balances . . . . . . . 5,168,532,160 34 5,706,324,838
Form 990 (2013)
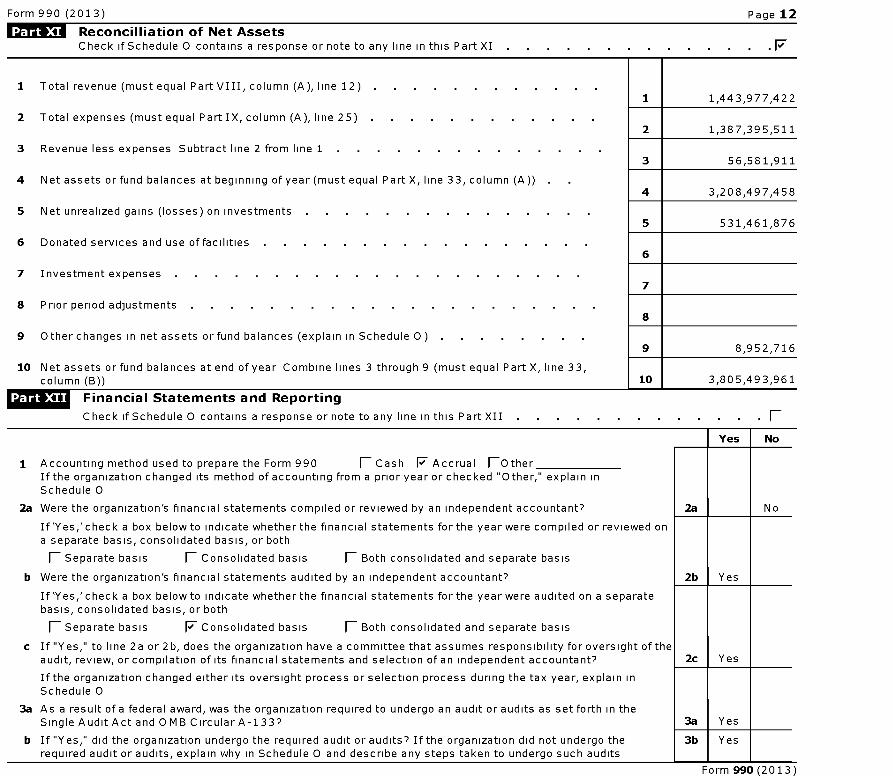
Form 990 (2013) Page 12
« Reconcilliation of Net AssetsCheck if Schedule 0 contains a response or note to any line in this Part XI . F
1 Total revenue (must equal Part VIII, column (A), line 12) . .
2 Total expenses (must equal Part IX, column (A), line 25) . .
3 Revenue less expenses Subtract line 2 from line 1
4 Net assets or fund balances at beginning of year (must equal Part X, line 33, column (A))
5 Net unrealized gains (losses) on investments
6 Donated services and use of facilities
7 Investment expenses . .
8 Prior period adjustments . .
9 Other changes in net assets or fund balances (explain in Schedule 0)
10 Net assets or fund balances at end of year Combine lines 3 through 9 (must equal Part X, line 33,column (B))
1 1,443,977,422
2 1,387,395,511
3 56,581,911
4 3,208,497,458
5 531,461,876
6
7
8
9 8,952,716
10 3,805,493,961
Financial Statements and Reporting
Check if Schedule 0 contains a response or note to any line in this Part XII (-
Yes No
1 Accounting method used to prepare the Form 990 fl Cash 17 Accrual (OtherIf the organization changed its method of accounting from a prior year or checked " Other," explain inSchedule 0
2a Were the organization 's financial statements compiled or reviewed by an independent accountant? 2a
If'Yes,'check a box below to indicate whether the financial statements for the year were compiled or reviewed ona separate basis, consolidated basis, or both
fl Separate basis fl Consolidated basis fl Both consolidated and separate basis
b Were the organization 's financial statements audited by an independent accountant? 2b Yes
If'Yes,'check a box below to indicate whether the financial statements for the year were audited on a separatebasis, consolidated basis, or both
fl Separate basis F Consolidated basis fl Both consolidated and separate basis
c If "Yes," to line 2a or 2b, does the organization have a committee that assumes responsibility for oversight of theaudit, review , or compilation of its financial statements and selection of an independent accountant? 2c Yes
If the organization changed either its oversight process or selection process during the tax year, explain inSchedule 0
3a As a result of a federal award, was the organization required to undergo an audit or audits as set forth in the
No
Single Audit Act and 0 MB Circular A-1 33? 3a Yes
b If "Yes," did the organization undergo the required audit or audits? If the organization did not undergo the 3b Yesrequired audit or audits, explain why in Schedule 0 and describe any steps taken to undergo such audits
Form 990 (2013)
efile GRAPHIC p rint - DO NOT PROCESS As Filed Data - DLN: 93493321108274
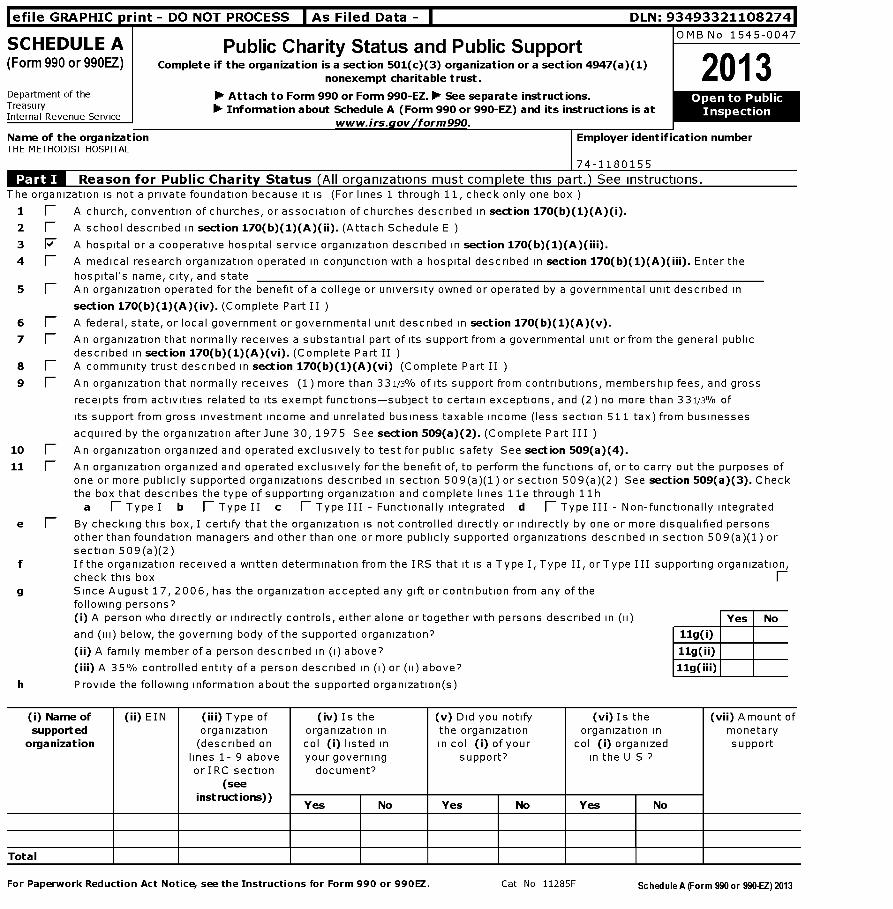
SCHEDULE A Public Charity Status and Public SupportOMB No 1545-0047
(Form 990 or 990EZ) Complete if the organization is a section 501(c)(3) organization or a section 4947(a)(1)2013nonexempt charitable trust.
Department of the I Oil Attach to Form 990 or Form 990-EZ . Oil See separate instructions. Ope nTreasury Oil Information about Schedule A (Form 990 or 990-EZ) and its instructions is at Inspe ctInternal Revenue Service
www.irs.gov form 990.
Name of the organization Employer identification numberTHE METHODIST HOSPITAL
Reason for Public Charity Status (All organizations must complete this part.) See instructions.The organization is not a private foundation because it is (For lines 1 through 11, check only one box )
1 1 A church, convention of churches, or association of churches described in section 170(b)(1)(A)(i).
2 fl A school described in section 170(b)(1)(A)(ii). (Attach Schedule E )
3 F A hospital or a cooperative hospital service organization described in section 170(b)(1)(A)(iii).
4 1 A medical research organization operated in conjunction with a hospital described in section 170(b)(1)(A)(iii). Enter the
hospital's name, city, and state5 1 An organization operated for the benefit of a college or university owned or operated by a governmental unit described in
section 170 ( b)(1)(A)(iv ). (Complete Part II )
6 1 A federal, state, or local government or governmental unit described in section 170(b)(1)(A)(v).
7 1 An organization that normally receives a substantial part of its support from a governmental unit or from the general publicdescribed in section 170 ( b)(1)(A)(vi ). (Complete Part II )
8 fl A community trust described in section 170 ( b)(1)(A)(vi ) (Complete Part II )
9 1 An organization that normally receives (1) more than 331/3% of its support from contributions, membership fees, and gross
receipts from activities related to its exempt functions-subject to certain exceptions, and (2) no more than 331/3% of
its support from gross investment income and unrelated business taxable income (less section 511 tax) from businesses
acquired by the organization after June 30, 1975 See section 509( a)(2). (Complete Part III )
10 1 An organization organized and operated exclusively to test for public safety See section 509(a)(4).
11 1 An organization organized and operated exclusively for the benefit of, to perform the functions of, or to carry out the purposes ofone or more publicly supported organizations described in section 509(a)(1) or section 509(a)(2) See section 509( a)(3). Checkthe box that describes the type of supporting organization and complete lines Ile through 11 h
a fl Type I b fl Type II c fl Type III - Functionally integrated d fl Type III - Non -functionally integrated
e (- By checking this box, I certify that the organization is not controlled directly or indirectly by one or more disqualified personsother than foundation managers and other than one or more publicly supported organizations described in section 509 ( a)(1 ) orsection 509(a)(2)
f If the organization received a written determination from the IRS that it is a Type I, Type II, orType III supporting organization,check this box F
g Since August 17, 2006, has the organization accepted any gift or contribution from any of thefollowing persons?(i) A person who directly or indirectly controls , either alone or together with persons described in (ii) Yes No
and (iii) below, the governing body of the supported organization? 11g(i)
(ii) A family member of a person described in (i) above? 11g(ii)
(iii) A 35% controlled entity of a person described in (i) or (ii) above? 11g(iii)
h Provide the following information about the supported organization(s)
(i) Name of (ii) EIN (iii) Type of (iv) Is the (v) Did you notify (vi) Is the (vii) Amount ofsupported organization organization in the organization organization in monetary
organization (described on col (i) listed in in col (i) of your col (i) organized supportlines 1- 9 above your governing support? in the U S ?or IRC section document?
(seeinstructions))
Yes No Yes No Yes No
Total
For Paperwork Reduction Act Notice, see the Instructions for Form 990 or 990EZ . Cat No 11285F ScheduleA(Form 990 or 990-EZ)2013
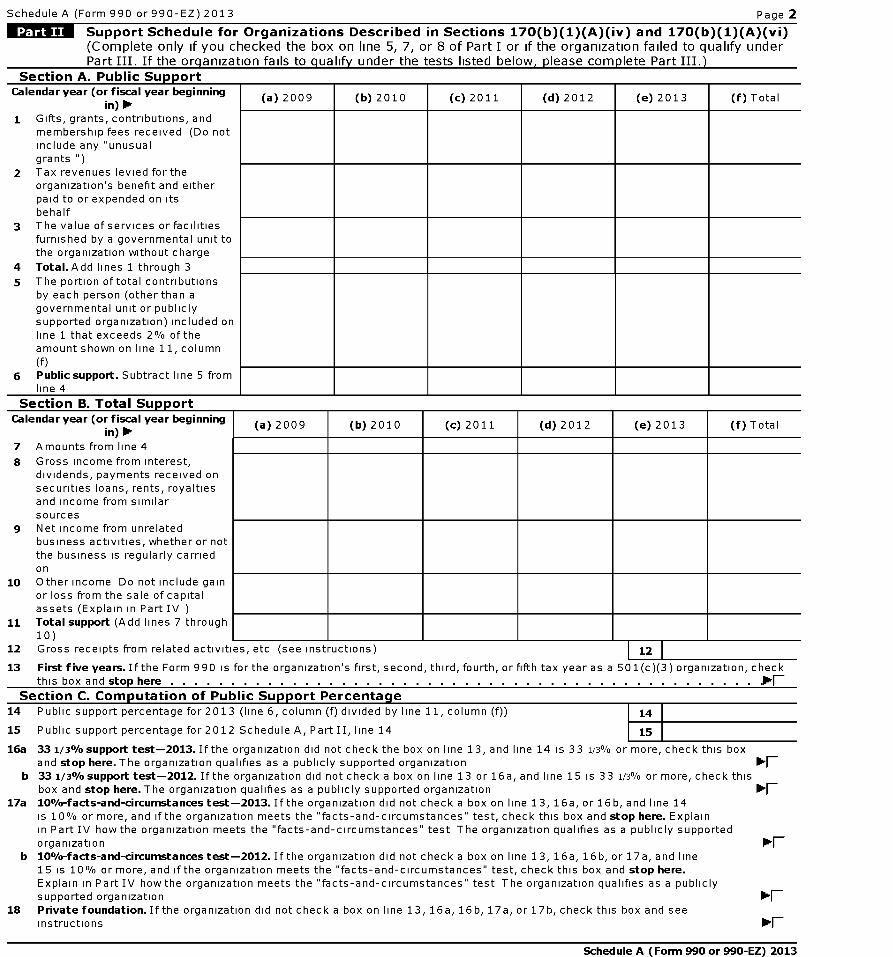
Schedule A (Form 990 or 990-EZ) 2013 Page 2
MU^ Support Schedule for Organizations Described in Sections 170(b)(1)(A)(iv) and 170(b)(1)(A)(vi)(Complete only if you checked the box on line 5, 7, or 8 of Part I or if the organization failed to qualify underPart III. If the organization fails to qualify under the tests listed below, please complete Part III.)
Section A . Public SupportCalendar year ( or fiscal year beginning (a) 2009 (b) 2010 (c) 2011 (d) 2012 (e) 2013 (f) Total
in) 111111 Gifts, grants, contributions, and
membership fees received (Do notinclude any "unusualgrants ")
2 Tax revenues levied for theorganization's benefit and eitherpaid to or expended on itsbehalf
3 The value of services or facilitiesfurnished by a governmental unit tothe organization without charge
4 Total .Add lines 1 through 3
5 The portion of total contributionsby each person (other than agovernmental unit or publiclysupported organization) included online 1 that exceeds 2% of theamount shown on line 11, column(f)
6 Public support . Subtract line 5 fromline 4
Section B. Total SupportCalendar year ( or fiscal year beginning (a) 2009 (b) 2010 (c) 2011 (d) 2012 (e) 2013 (f) Total
in) ►7 Amounts from line 4
8 Gross income from interest,dividends, payments received onsecurities loans, rents, royaltiesand income from similarsources
9 Net income from unrelatedbusiness activities, whether or notthe business is regularly carriedon
10 Other income Do not include gainor loss from the sale of capitalassets (Explain in Part IV )
11 Total support (Add lines 7 through10)
12 Gross receipts from related activities, etc (see instructions) 12
13 First five years. If the Form 990 is for the organization's first, second, third, fourth, or fifth tax year as a 501(c)(3) organization, checkthis box and stop here . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ^.
Section C. Com p utation of Public Support Percenta g e14 Public support percentage for 2013 (line 6, column (f) divided by line 11, column (f)) 14
15 Public support percentage for 2012 Schedule A, Part II, line 14 15
16a 331 / 3%support test-2013. If the organization did not check the box on line 13, and line 14 is 33 1/3% or more, check this boxand stop here . The organization qualifies as a publicly supported organization
b 331 / 3%support test-2012 . If the organization did not check a box on line 13 or 16a, and line 15 is 33 1/3% or more, check thisbox and stop here . The organization qualifies as a publicly supported organization
17a 10%-facts-and -circumstances test - 2013. If the organization did not check a box on line 13, 16a, or 16b, and line 14is 10% or more, and if the organization meets the "facts-and-circumstances" test, check this box and stop here . Explainin Part IV how the organization meets the "facts-and-circumstances" test The organization qualifies as a publicly supportedorganization
b 10%-facts-and-circumstances test -2012 . If the organization did not check a box on line 13, 16a, 16b, or 17a, and line15 is 10% or more, and if the organization meets the "facts- and-circumstances" test, check this box and stop here.Explain in Part IV how the organization meets the "facts-and-circumstances" test The organization qualifies as a publiclysupported organization
18 Private foundation . If the organization did not check a box on line 13, 16a, 16b, 17a, or 17b, check this box and seeinstructions
Schedule A (Form 990 or 990-EZ) 2013
Schedule A (Form 990 or 990-EZ) 2013 Page 3
IMMITM Support Schedule for Organizations Described in Section 509(a)(2)(Complete only if you checked the box on line 9 of Part I or if the organization failed to qualify underPart II. If the organization fails to qualify under the tests listed below, please complete Part II.)
Section A . Public SupportCalendar year ( or fiscal year beginning (a) 2009 (b) 2010 (c) 2011 (d) 2012 (e) 2013 (f) Total
in) 111111 Gifts, grants, contributions, and
membership fees received (Do notinclude any "unusual grants ")
2 Gross receipts from admissions,merchandise sold or servicesperformed, or facilities furnished inany activity that is related to theorganization's tax-exemptpurpose
3 Gross receipts from activities thatare not an unrelated trade orbusiness under section 513
4 Tax revenues levied for theorganization's benefit and eitherpaid to or expended on itsbehalf
5 The value of services or facilitiesfurnished by a governmental unit tothe organization without charge
6 Total . Add lines 1 through 5
7a Amounts included on lines 1, 2,and 3 received from disqualifiedpersons
b Amounts included on lines 2 and 3received from other thandisqualified persons that exceedthe greater of$5,000 or 1% of theamount on line 13 for the year
c Add lines 7a and 7b
8 Public support (Subtract line 7cfrom line 6 )
Section B. Total SuuuortCalendar year ( or fiscal year beginning (a) 2009 (b) 2010 (c) 2011 (d) 2012 (e) 2013 (f) Total
in) ►9 Amounts from line 6
10a Gross income from interest,dividends, payments received onsecurities loans, rents, royaltiesand income from similarsources
b Unrelated business taxableincome (less section 511 taxes)from businesses acquired afterJune 30, 1975
c Add lines 10a and 10b
11 Net income from unrelatedbusiness activities not includedin line 10b, whether or not thebusiness is regularly carried on
12 Other income Do not includegain or loss from the sale ofcapital assets (Explain in PartIV )
13 Total support . (Add lines 9, 1Oc,11, and 12 )
14 First five years. If the Form 990 is for the organization's first, second, third, fourth, or fifth tax year as a 501(c)(3) organization,check this box and stop here
Section C. Computation of Public Support Percentage
15 Public support percentage for 2013 (line 8, column (f) divided by line 13, column (f)) 15
16 Public support percentage from 2012 Schedule A , Part III, line 15 16
Section D . Com p utation of Investment Income Percenta g e
17 Investment income percentage for 2013 (line 10c, column (f) divided by line 13, column (f)) 17
18 Investment income percentage from 2012 Schedule A, Part III, line 17 18
19a 331 / 3% support tests-2013. If the organization did not check the box on line 14, and line 15 is more than 33 1/3%, and line 17 is notmore than 33 1/3%, check this box and stop here . The organization qualifies as a publicly supported organization lk'F-
b 331 / 3% support tests-2012. If the organization did not check a box on line 14 or line 19a , and line 16 is more than 33 1/3% and line 18is not more than 33 1/3%, check this box and stop here . The organization qualifies as a publicly supported organization lk'F-
20 Private foundation . If the organization did not check a box on line 14, 19a, or 19b, check this box and see instructions
Schedule A (Form 990 or 990-EZ) 2013
Schedule A (Form 990 or 990-EZ) 2013 Page 4
Supplemental Information . Provide the explanations required by Part II, line 10; Part II, line 17a or17b; and Part III, line 12. Also complete this part for any additional information. (See instructions).
Facts And Circumstances Test
I Return Reference I Explanation I
Schedule A (Form 990 or 990-EZ) 2013
l efile GRAPHIC p rint - DO NOT PROCESS As Filed Data - DLN: 93493321108274
SCHEDULE C Political Campaign and Lobbying Activities OMB No 1545-0047
(Form 990 or 990-EZ )For Organizations Exempt From Income Tax Under section 501(c) and section 527 2013
Department of the Treasury 1- Complete if the organization is described below. 0- Attach to Form 990 or Form 990-EZ.
Internal Revenue Service0- See separate instructions . 0- Information about Schedule C (Form 990 or 990-EZ) and its •
instructions is at www.irs. gov form 990.
If the organization answered "Yes" to Form 990, Part IV , Line 3, or Form 990-EZ, Part V, line 46 (Political Campaign Activities), then• Section 501(c)(3) organizations Complete Parts I-A and B Do not complete Part I-C• Section 501(c) (other than section 501(c)(3)) organizations Complete Parts I-A and C below Do not complete Part I-B• Section 527 organizations Complete Part I-A only
If the organization answered "Yes" to Form 990, Part IV , Line 4, or Form 990-EZ , Part VI, line 47 ( Lobbying Activities), then• Section 501(c)(3) organizations that have filed Form 5768 (election under section 501(h)) Complete Part II-A Do not complete Part II-B• Section 501(c)(3) organizations that have NOT filed Form 5768 (election under section 501(h)) Complete Part II-B Do not complete Part II-A
If the organization answered "Yes" to Form 990, Part IV , Line 5 ( Proxy Tax) or Form 990-EZ, Part V, line 35c (Proxy Tax), then* Section 501(c)(4), (5), or (6) organizations Complete Part IIIName of the organization Employer identification numberTHE METHODIST HOSPITAL
74-1180155
Complete if the organization is exempt under section 501(c) or is a section 527 organization.
1 Provide a description of the organization's direct and indirect political campaign activities in Part IV
2 Political expenditures 0- $
3 Volunteer hours
Complete if the organization is exempt under section 501(c)(3).
1 Enter the amount of any excise tax incurred by the organization under section 4955 0- $
2 Enter the amount of any excise tax incurred by organization managers under section 4955 0- $
3 If the organization incurred a section 4955 tax, did it file Form 4720 for this year? fl Yes fl No
4a Was a correction made? fl Yes fl No
b If "Yes," describe in Part IV
rMWINT-Complete if the organization is exempt under section 501 ( c), except section 501(c)(3).
1 Enter the amount directly expended by the filing organization for section 527 exempt function activities 0- $
2 Enter the amount of the filing organization's funds contributed to other organizations for section 527exempt function activities 0- $
3 Total exempt function expenditures Add lines 1 and 2 Enter here and on Form 1120-PO L, line 17b 0- $
4 Did the filing organization file Form 1120-POL for this year? fl Yes fl No
5 Enter the names, addresses and employer identification number (EIN) of all section 527 political organizations to which the filingorganization made payments For each organization listed, enter the amount paid from the filing organization's funds Also enter theamount of political contributions received that were promptly and directly delivered to a separate political organization, such as aseparate segregated fund or a political action committee (PAC) If additional space is needed, provide information in Part IV
(a) Name (b) Address ( c) EIN (d ) Amount paid fromfiling organization's
funds If none, enter -0-
(e) Amount of politicalcontributions received
and promptly anddirectly delivered to a
separate politicalorganization If none,
enter -0-
i-or raperworK rteauction Act Notice, see the instructions Tor corm 99U or yyu -tc. Cat No 50084S Schedule C ( Form 990 or 990 - EZ) 2013
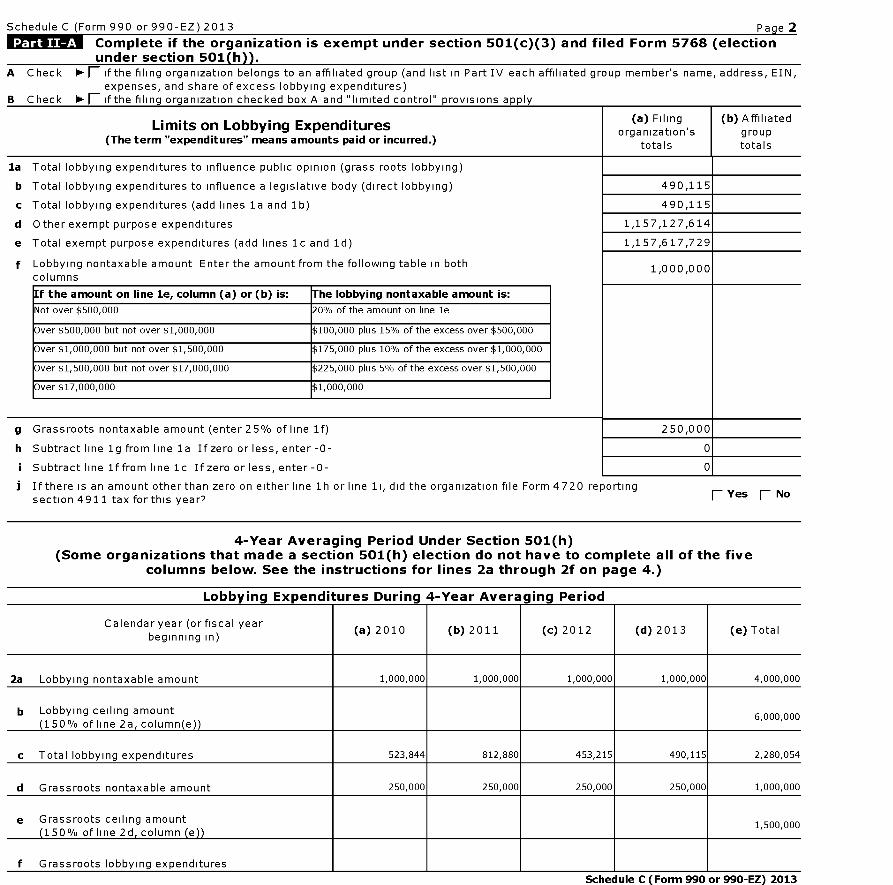
Schedule C (Form 990 or 990-EZ) 2013 Page 2
Complete if the organization is exempt under section 501 ( c)(3) and filed Form 5768 ( electionunder section 501(h)).
A Check - (- if the filing organization belongs to an affiliated group (and list in Part IV each affiliated group member's name, address, EIN,expenses, and share of excess lobbying expenditures)
B Check - (- if the filing organization checked box A and "limited control" provisions apply
Limits on Lobbying Expenditures(a) Filing (b) Affiliated
(The term "expenditures " means amounts paid or incurred .)organization's group
totals totals
la Total lobbying expenditures to influence public opinion (grass roots lobbying)
b Total lobbying expenditures to influence a legislative body (direct lobbying)
c Total lobbying expenditures (add lines la and 1b)
d Other exempt purpose expenditures
e Total exempt purpose expenditures (add lines 1c and 1d)
f Lobbying nontaxable amount Enter the amount from the following table in bothcolumns
If the amount on line le, column ( a) or (b ) is: The lobbying nontaxable amount is:
Not over $500,000 20% of the amount on line le
Over $500,000 but not over $1,000,000 $100,000 plus 15% of the excess over $500,000
Over $1,000,000 but not over $1,500,000 $175,000 plus 10% of the excess over $1,000,000
Over $1,500,000 but not over $17,000,000 $225,000 plus 5% of the excess over $1,500,000
Over $17,000,000 $1,000,000
490,115
490,115
1,157,127,614
1,157,617,729
g Grassroots nontaxable amount (enter 25% of line 1f)
h Subtract line 1g from line la If zero or less, enter-0-
i Subtract line 1f from line 1c If zero or less, enter-0-
] If there is an amount otherthan zero on either line 1h or line li, did the organization file Form 4720 reportingsection 4911 tax for this year?
1,000,000
250,000
0
0
F- Yes F- No
4-Year Averaging Period Under Section 501(h)(Some organizations that made a section 501(h) election do not have to complete all of the five
columns below. See the instructions for lines 2a through 2f on page 4.)
Lobbvina Exoenditures During 4-Year Averaaina Period
Calendar year (or fiscal year(a) 2010 (b) 2011 (c) 2012 (d) 2013 (e) Total
beginning in)
2a Lobbying nontaxable amount 1,000,000 1,000,000 1,000,000 1,000,000 4,000,000
b Lobbying ceiling amount(150% of line 2a, column(e))
6,000,000
c Total lobbying expenditures 523,844 812,880 453,215 490,115 2,280,054
d Grassroots nontaxable amount 250,000 250,000 250,000 250,000 1,000,000
e Grassroots ceiling amount 1,500,000150% of line 2d column e
f Grassroots lobbying expenditures
Schedule C (Form 990 or 990-EZ) 2013
Schedule C (Form 990 or 990-EZ) 2013 Pa g e 3Complete if the organization is exempt under section 501 ( c)(3) and has NOTfiled Form 5768 ( election under section 501(h)).
For each "Yes " response to lines la through li below, provide in Part IV a detailed description of the lobbying(a) (b)
activity. Yes No Amount
1 During the year, did the filing organization attempt to influence foreign, national, state or locallegislation, including any attempt to influence public opinion on a legislative matter or referendum,through the use of
a Volunteers?
b Paid staff or management (include compensation in expenses reported on lines 1c through 1i)?
c Media advertisements?
d Mailings to members, legislators, or the public?
e Publications, or published or broadcast statements?
f Grants to other organizations for lobbying purposes?
g Direct contact with legislators, their staffs, government officials, or a legislative body?
h Rallies, demonstrations, seminars, conventions, speeches, lectures, or any similar means?
i Other activities?
j Total Add lines 1c through 1i
2a Did the activities in line 1 cause the organization to be not described in section 501(c)(3)?
b If "Yes," enter the amount of any tax incurred under section 4912
c If "Yes," enter the amount of any tax incurred by organization managers under section 4912
d If the filing organization incurred a section 4912 tax, did it file Form 4720 for this year?
Complete if the organization is exempt under section 501(c)(4), section 501(c)(5), or section501(c)(6).
1 Were substantially all (90% or more) dues received nondeductible by members?
2 Did the organization make only in-house lobbying expenditures of $2,000 or less?
3 Did the organization agree to carry over lobbying and political expenditures from the prior year?
No
Complete if the organization is exempt under section 501(c)(4), section 501(c)(5), or section501(c)(6) and if either (a) BOTH Part III-A, lines 1 and 2, are answered "No" OR (b) Part III-A,line 3, is answered "Yes."
1 Dues, assessments and similar amounts from members 1
2 Section 162(e) nondeductible lobbying and political expenditures ( do not include amounts of politicalexpenses for which the section 527(f) tax was paid).
a Current year 2a
b Carryover from last year 2b
c Total 2c
3 Aggregate amount reported in section 6033(e)(1 )(A) notices of nondeductible section 162(e) dues 3
4 If notices were sent and the amount on line 2c exceeds the amount on line 3, what portion of the excessdoes the organization agree to carryover to the reasonable estimate of nondeductible lobbying andpolitical expenditure next year? 4
5 Taxable amount of lobbying and political expenditures (see instructions) 5
Supplemental Information
Provide the descriptions required for Part I-A, line 1, Part I-B, line 4, Part I-C, line 5, Part II-A (affiliated group list), Part II-A, line 2, andPart II-B. line 1 Also. comDlete this Dart for any additional information
Return Reference I Explanation
Schedule C (Form 990 or 990-EZ) 2013
Schedule D (Form 990) 2013
Schedule C (Form 990 or 990-EZ) 2013 Page 4
lefile GRAPHIC print - DO NOT PROCESS As Filed Data - DLN: 93493321108274
SCHEDULE D Supplemental Financial StatementsOMB No 1545-0047
(Form 990)Complete if the organization answered "Yes," to Form 990,0- 2013
Part IV, line 6, 7, 8, 9, 10, 11a, 11b, 11c, 11d , 11e, 11f , 12a, or 12b
Department of the Treasury 0- Attach to Form 990. 0- See separate instructions . 1- Information about Schedule D (Form 990) •II. -
Internal Revenue Service and its instructions is at www.irs.gov /form990 . . -
Name of the organization Employer identification numberTHE METHODIST HOSPITAL
74-1180155Organizations Maintaining Donor Advised Funds or Other Similar Funds or Accounts. Complete if theorg anization answered "Yes" to Form 990 , Part IV , line 6.
(a) Donor advised funds (b) Funds and other accounts
1 Total number at end of year
2 Aggregate contributions to (during year)
3 Aggregate grants from ( during year)
4 Aggregate value at end of year
5 Did the organization inform all donors and donor advisors in writing that the assets held in donor advisedfunds are the organization ' s property , subject to the organization ' s exclusive legal control? F Yes I No
6 Did the organization inform all grantees , donors, and donor advisors in writing that grant funds can beused only for charitable purposes and not for the benefit of the donor or donor advisor, or for any other purposeconferring impermissible private benefit? fl Yes fl No
MRSTI-Conservation Easements . Complete if the organization answered "Yes" to Form 990, Part IV , line 7.
1 Purpose ( s) of conservation easements held by the organization ( check all that apply)
1 Preservation of land for public use ( e g , recreation or education ) 1 Preservation of an historically important land area
1 Protection of natural habitat 1 Preservation of a certified historic structure
fl Preservation of open space
2 Complete lines 2a through 2d if the organization held a qualified conservation contribution in the form of a conservationeasement on the last day of the tax year
a Total number of conservation easements
b Total acreage restricted by conservation easements
c Number of conservation easements on a certified historic structure included in (a)
d Number of conservation easements included in (c) acquired after 8/17/06, and not on ahistoric structure listed in the National Register
Held at the End of the Year
2a
2b
2c
2d
3 N umber of conservation easements modified, transferred, released, extinguished , or terminated by the organization during
the tax year 0-
4 N umber of states where property subject to conservation easement is located 0-
5 Does the organization have a written policy regarding the periodic monitoring , inspection , handling of violations, andenforcement of the conservation easements it holds? fl Yes fl No
6 Staff and volunteer hours devoted to monitoring , inspecting , and enforcing conservation easements during the year
0-
7 Amount of expenses incurred in monitoring , inspecting , and enforcing conservation easements during the year
0- $
8 Does each conservation easement reported on line 2(d) above satisfy the requirements of section 170(h)(4)(B)(i)and section 170(h)(4)(B)(ii)? F Yes 1 No
9 In Part XIII, describe how the organization reports conservation easements in its revenue and expense statement, andbalance sheet, and include, if applicable, the text of the footnote to the organization's financial statements that describesthe organization's accounting for conservation easements
Organizations Maintaining Collections of Art, Historical Treasures, or Other Similar Assets.Complete if the oraanization answered "Yes" to Form 990. Part IV. line 8.
la If the organization elected, as permitted under SFAS 116 (ASC 958), not to report in its revenue statement and balance sheetworks of art, historical treasures, or other similar assets held for public exhibition, education, or research in furtherance of publicservice, provide, in Part XIII, the text of the footnote to its financial statements that describes these items
b If the organization elected, as permitted under SFAS 116 (ASC 958), to report in its revenue statement and balance sheetworks of art, historical treasures, or other similar assets held for public exhibition, education, or research in furtherance of publicservice, provide the following amounts relating to these items
(i) Revenues included in Form 990, Part VIII, line 1 $
(ii)Assets included in Form 990, Part X $
2 If the organization received or held works of art, historical treasures, or other similar assets for financial gain, provide thefollowing amounts required to be reported under SFAS 116 (ASC 958) relating to these items
a Revenues included in Form 990, Part VIII, line 1 $
b Assets included in Form 990, Part X $
For Paperwork Reduction Act Notice, see the Instructions for Form 990. Cat No 52283D Schedule D ( Form 990) 2013
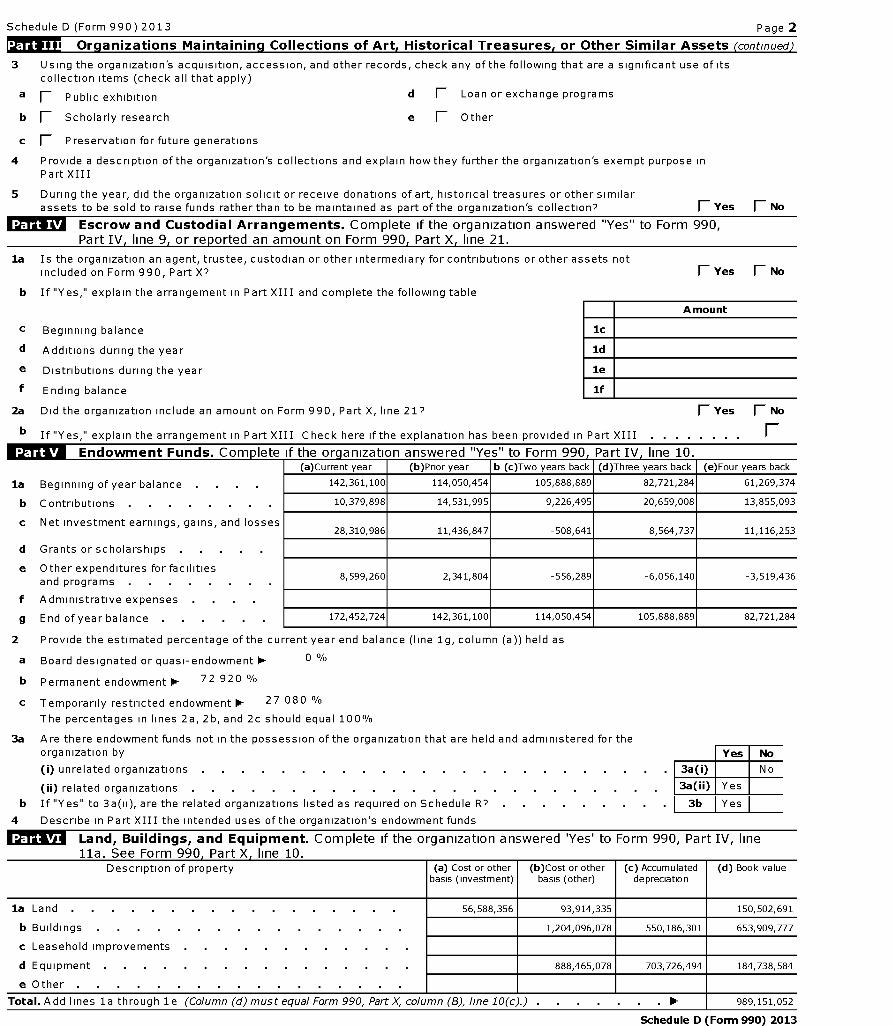
Schedule D (Form 990) 2013 Page 2
r:FTnFW Organizations Maintaining Collections of Art, Historical Treasures, or Other Similar Assets (continued)
3 Using the organization's acquisition, accession, and other records, check any of the following that are a significant use of itscollection items (check all that apply)
a F_ Public exhibition d fl Loan or exchange programs
b 1 Scholarly research e (- Other
c F Preservation for future generations
4 Provide a description of the organization's collections and explain how they further the organization's exempt purpose inPart XIII
5 During the year, did the organization solicit or receive donations of art, historical treasures or other similarassets to be sold to raise funds rather than to be maintained as part of the organization's collection? 1 Yes 1 No
Escrow and Custodial Arrangements . Complete if the organization answered "Yes" to Form 990,Part IV, line 9, or reported an amount on Form 990, Part X, line 21.
la Is the organization an agent, trustee, custodian or other intermediary for contributions or other assets notincluded on Form 990, Part X7 1 Yes F No
b If "Yes," explain the arrangement in Part XIII and complete the following table
c Beginning balance 1c
d Additions during the year ld
e Distributions during the year le
f Ending balance if
A mount
2a Did the organization include an amount on Form 990, Part X, line 21? fl Yes fl No
b If "Yes," explain the arrangement in Part XIII Check here if the explanation has been provided in Part XIII . . . . . . . . F
MWAF-Endowment Funds . Com p lete if the or anization answered "Yes" to Form 990 , Part IV, line 10.
la Beginning of year balance .
b Contributions
c Net investment earnings, gains, and losses
d Grants or scholarships
e Other expenditures for facilitiesand programs
f Administrative expenses .
g End of year balance
(a)Current year (b)Prior year b (c)Two years back (d)Three years back (e)Four years back
142, 361,100 114, 050, 454 105, 888, 889 82, 721, 284 61, 269, 374
10,379,898 14,531,995 9,226,495 20,659,008 13,855,093
28,310,986 11,436,847 -508,641 8,564,737 11,116,253
8,599,260 2,341,804 -556,289 -6,056,140 -3,519,436
172,452,724 142,361,100 114,050,454 105,888,889 82,721,284
2 Provide the estimated percentage of the current year end balance (line 1g, column (a)) held as
a Board designated or quasi-endowment 0- 0 %
b Permanent endowment 0- 72 920 %
c Temporarily restricted endowment 0- 27 080 %
The percentages in lines 2a, 2b, and 2c should equal 100%
3a Are there endowment funds not in the possession of the organization that are held and administered for theorganization by Yes No
(i) unrelated organizations . . . . . . . . . . . . . . . . . . . . . . . . 3a(i) No
(ii) related organizations . . . . . . . . . . . . . . . . . . . . . . 3a(ii) Yes
b If "Yes" to 3a(ii), are the related organizations listed as required on Schedule R? . . I 3b I Yes
4 Describe in Part XIII the intended uses of the organization's endowment funds
Land , Buildings , and Equipment . Complete if the organization answered 'Yes' to Form 990, Part IV, line1 1 a See Form 990 Part X line 1(l
Description of property (a) Cost or otherbasis (investment)
(b)Cost or otherbasis (other)
(c) Accumulateddepreciation
(d) Book value
la Land 56,588,356 93,914,335 150,502,691
b Buildings 1,204,096,078 550,186,301 653,909,777
c Leasehold improvements . .
d Equipment 888,465,078 703,726,494 184,738,584
e Other
Total . Add lines la through 1 e (Column (d) must equal Form 990, Part X, column (B), line 10(c).) . . 0- 989,151,052
Schedule D (Form 990) 2013
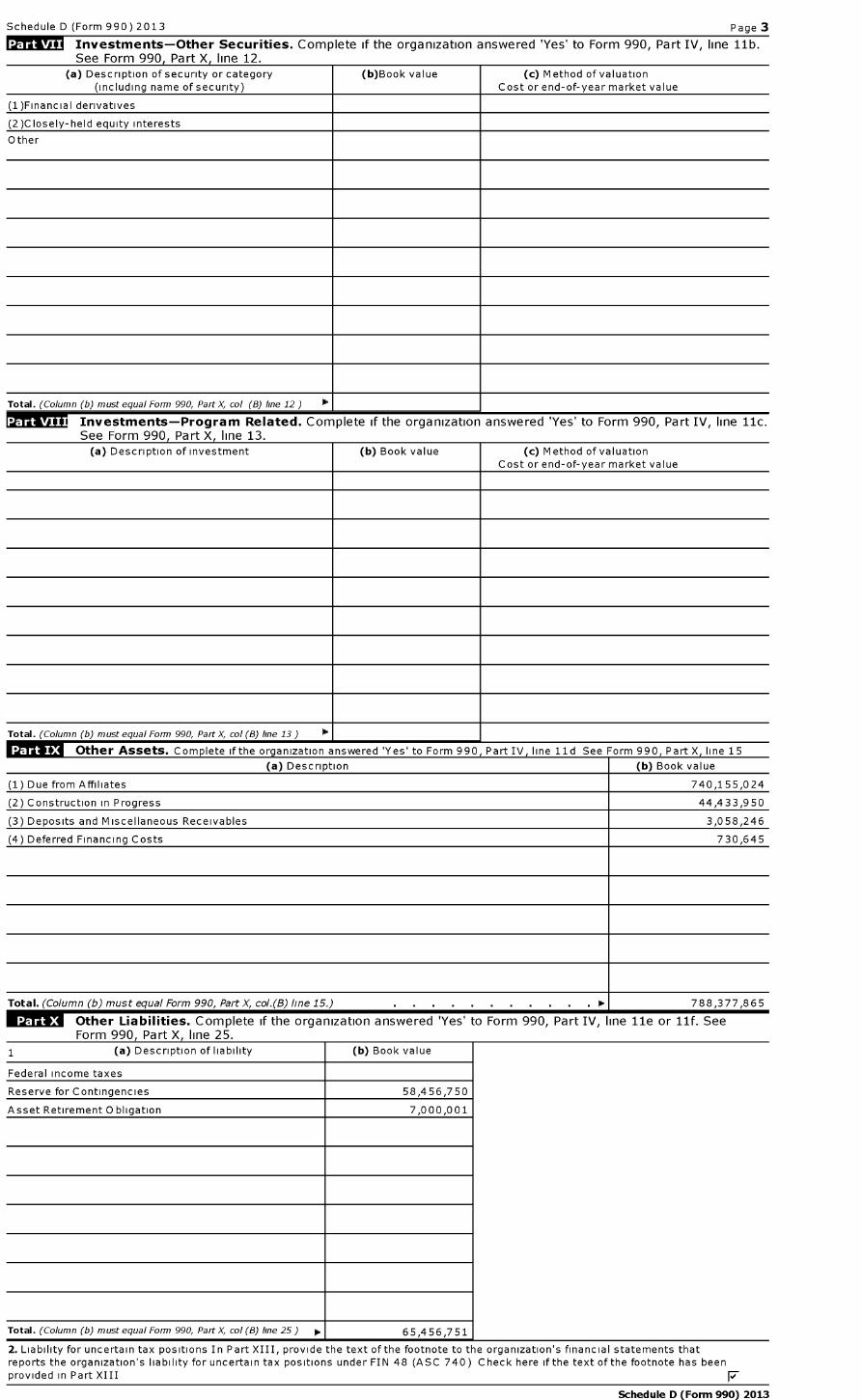
Schedule D (Form 990) 2013 Page 3
Investments-Other Securities . Complete if the organization answered 'Yes' to Form 990, Part IV, line 11b.See Form 990 , Part X line 12.
(a) Description of security or category (b)Book value (c) Method of valuation(including name of security) Cost or end-of-year market value
(1 )Financial derivatives
(2)Closely-held equity interests
Other
Total . (Column (b) must equal Form 990, Part X, col (B) line 12) 0. 11
Related . Complete if the organization answered 'Yes' to Form 990, Part IV, line 11c.See Form 990, Part X, line 13.
(a) Description of investment (b) Book value (c) Method of valuationCost or end-of-year market value
Total . (Column (b) must equal Form 990, Part X, col (8) line 13 ) 0.1
Other Assets . Complete if the organization answered 'Yes' to Form 990, Part IV, line 1ld See Form 990, Part X, line 15
(a) Description (b) Book value
(1) Due from Affiliates 740,155,024
(2) Construction in Progress 44,433,950
(3) Deposits and Miscellaneous Receivables 3,058,246
(4) Deferred Financing Costs 730,645
Total . (Column (b) must equal Form 990, Part X, co/.(8) line 15.) . 0.1 788,377,865
Other Liabilities . Complete if the organization answered 'Yes' to Form 990, Part IV, line 11e or 11f. See
Schedule D (Form 990) 2013
2. Liability for uncertain tax positions In Part XIII, provide the text of the footnote to the organization ' s financial statements thatreports the organization ' s liability for uncertain tax positions under FIN 48 (A SC 740 ) Check here if the text of the footnote has beenprovided in Part XIII F
Schedule D (Form 990) 2013 Page 4
Reconciliation of Revenue per Audited Financial Statements With Revenue per Return Complete ifthe org anization answered 'Yes' to Form 990 , Part IV line 12a.
1 Total revenue, gains, and other support per audited financial statements . 1
2 Amounts included on line 1 but not on Form 990, Part VIII, line 12
a Net unrealized gains on investments . 2a
b Donated services and use of facilities . 2b
c Recoveries of prior year grants 2c
d Other (Describe in Part XIII ) 2d
e Add lines 2a through 2d . . . . . . . . . . . . . . . . . . . . 2e
3 Subtract line 2e from line 1 . . . . . . . . . . . . . . . . . . . . 3
4 Amounts included on Form 990, Part VIII, line 12, but not on line 1
a Investment expenses not included on Form 990, Part VIII, line 7b . 4a
b Other (Describe in Part XIII ) . . . . . . . . . . 4b
c Add lines 4a and 4b . . . . . . . . . . . . . . . . . . . . . . 4c
5 Total revenue Add lines 3 and 4c. (This must equal Form 990, Part I, line 12 ) . . . . . 5
« Reconciliation of Expenses per Audited Financial Statements With Expenses per Return . Completeif the org anization answered 'Yes' to Form 990 , Part IV line 12a.
1 Total expenses and losses per audited financial statements . . . . . . . . . . 1
2 Amounts included on line 1 but not on Form 990, Part IX, line 25
a Donated services and use of facilities . 2a
b Prior year adjustments 2b
c Other losses . . . . . . . . . . . . . . . 2c
d Other (Describe in Part XIII ) . . . . . . . . . . . 2d
e Add lines 2a through 2d . . . . . . . . . . . . . . . . . . . . . 2e
3 Subtract line 2e from line 1 . . . . . . . . . . . . . . . . . . . . 3
4 Amounts included on Form 990, Part IX, line 25, but not on line 1:
a Investment expenses not included on Form 990, Part VIII, line 7b 4a
b Other (Describe in Part XIII ) . . . . . . . . . . . 4b
c Add lines 4a and 4b . . . . . . . . . . . . . . . . . . . . . . 4c
5 Total expenses Add lines 3 and 4c. (This must equal Form 990, Part I, line 18 ) . . . . . 5
UT1174M Supplemental Information
Provide the descriptions required for Part II, lines 3, 5, and 9, Part III, lines la and 4, Part IV, lines lb and 2b,Part V, line 4, Part X, line 2, Part XI, lines 2d and 4b, and Part XII, lines 2d and 4b Also complete this part to provide any additionalinformation
Return Reference Explanation
Part V, Line 4 Houston Methodist Hospital Foundation, a related organization of The Methodist Hospital doingbusiness as Houston Methodist Hospital, holds permanently restricted net assets which consist of 77individual endowment accounts Unless otherwise directed by the donor, gifts received for endowmentaccounts are invested consistent with Houston Methodist Hospital's approved investment policyUnless otherwise directed by the donor, the Foundation has a policy of annually appropriating acertain percentage of each endowment account, which is then available to be spent consistent withdonor intent In order to preserve the real value of a donor's gift and to sustain funding consistent withdonor intent, the annual appropriation rate is set to strike a reasonable balance between long-termobjectives of preserving and growing each endowment fund for the future and providing stable, year-to-year appropriation amounts
Part X, Line 2 Houston Methodist Hospital's financial statements are included in the consolidated financialstatements of Houston Methodist (HM), which are audited by an independent accountant HM did notrecognize any adjustments related to uncertain tax positions as of December 31, 2013
Schedule D (Form 990) 2013
Schedule D (Form 990) 2013
Schedule D (Form 990) 2013 Page 5
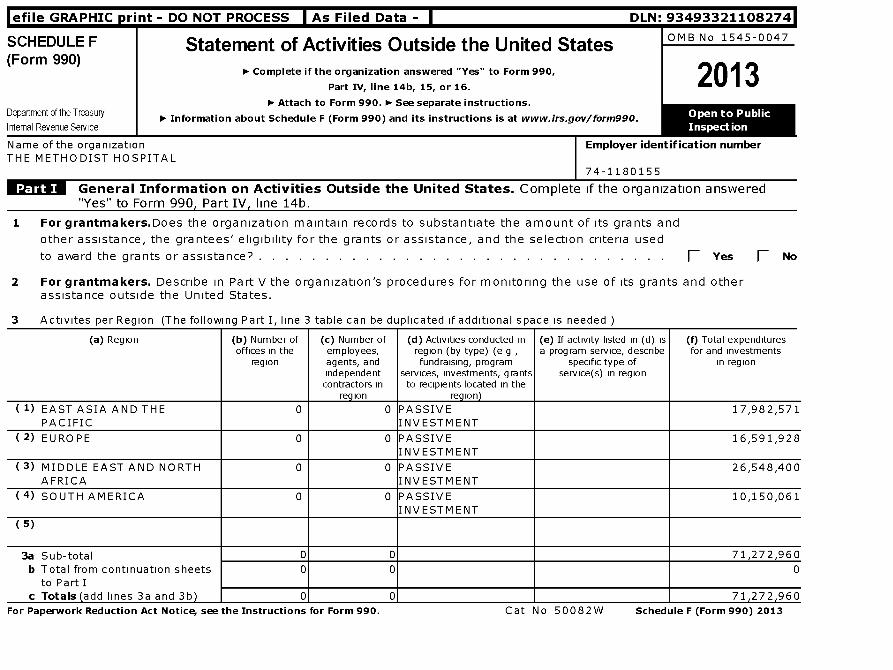
lefile GRAPHIC print - DO NOT PROCESS As Filed Data - DLN: 93493321108274
SCHEDULE F(Form 990)
Department of the Treasury
Internal Revenue Service
Statement of Activities Outside the United Statesn Complete if the organization answered "Yes" to Form 990,
Part IV, line 14b, 15, or 16.
n Attach to Form 990. ► See separate instructions.
n Information about Schedule F (Form 990) and its instructions is at www.irs.gov/form990.
Name of the organizationTHE METHODIST HOSPITAL
OMB No 1545-0047
2013
Employer identification number
74-1180155
General Information on Activities Outside the United States . Complete if the organization answered"Yes" to Form 990, Part IV, line 14b.
1 For grantmakers.Does the organization maintain records to substantiate the amount of its grants and
other assistance, the grantees' eligibility for the grants or assistance, and the selection criteria used
to award the grants or assistance? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . fl Yes fl No
2 For grantmakers . Describe in Part V the organization's procedures for monitoring the use of its grants and otherassistance outside the United States.
3 Activites per Region (The following Part I, line 3 table can be duplicated if additional space is needed )
(a) Region (b) Number of ( c) Number of ( d) Activities conducted in (e) If activity listed in ( d) is (f) Total expendituresoffices in the employees, region (by type) ( e g , a program service, describe for and investments
region agents , and fundraising , program specific type of in regionindependent services, investments , grants service ( s) in regioncontractors in to recipients located in the
reg ion re g ion )
( 1) EAST ASIA AND THE 0 0 PASSIVE 17,982,571PACIFIC INVESTMENT
( 2) EUROPE 0 0 PASSIVE 16,591,928INVESTMENT
(3) MIDDLE EAST AND NORTH 0 0 PASSIVE 26,548,400AFRICA INVESTMENT
(4) SOUTH AMERICA 0 0 PASSIVE 10,150,061INVESTMENT
(5)
3a Sub-total 0 0 71,272,960
b Total from continuation sheets 0 0 0to Part I
c Totals ( add lines 3a and 3b ) 0 0 71 , 272 , 960
For Paperwork Reduction Act Notice, see the Instructions for Form 990 . Cat N o 50082W Schedule F (Form 990) 2013
Schedule F (Form 990) 2013 Page 2
Grants and Other Assistance to Organizations or Entities Outside the United States . Complete if the organization answered "Yes" to Form 990,Part IV, line 15, for any recipient who received more than $5,000. Part II can be duplicated if additional space is needed.
1(a) Name oforganization
(b) IRS codesection
and EIN ( ifapplicable)
( c) Region ( d) Purpose ofgrant
(e) Amount ofcash grant
(f) Manner ofcash
disbursement
(g) Amountof non-cashassistance
( h) Descriptionof non-cashassistance
( i) Method ofvaluation
(book, FMV,appraisal, other)
( 1)
(2)
(3)
(4)
2 Enter total number of recipient organizations listed above that are recognized as charities by the foreign country, recognized astax-exempt by the IRS, or for which the grantee or counsel has provided a section 501(c)(3) equivalency letter . . . .
Enter total number of other organizations or entities .
Schedule F (Form 990) 2013
Schedule F (Form 990) 2013 Page 3
Grants and Other Assistance to Individuals Outside the United States . Complete if the organization answered "Yes" to Form 990, Part IV, line 16.Part III can be duplicated if additional space is needed.
(a) Type of grant orassistance
(b) Region (c) Number ofrecipients
(d) Amount ofcash grant
(e) Manner of cashdisbursement
(f) Amount ofnon-cashassistance
(g) Descriptionof non-cashassistance
(h) Method ofvaluation
(book, FMV,a pp raisal , other )
( 1)
(2)
(3)
(4)
(5)
(6)
(7)
(8)
(9)
( 10)
( 11)
( 12)
( 13)
( 14)
( 15)
( 16)
( 17)
( 18)
Schedule F (Form 990) 2013
Schedule F (Form 990) 2013 Page 4
Foreign Forms
1 Was the organization a U S transferor of property to a foreign corporation during the tax year? If "Yes,"theorganization may be required to file Form 926, Return by a U.S. Transferor of Property to a Foreign Corporation (seeInstructions for Form 926) F- Yes F N o
2 Did the organization have an interest in a foreign trust during the tax year? If "Yes," the organization may berequired to file Form 3520, Annual Return to Report Transactions with Foreign Trusts and Receipt of Certain ForeignGifts, and/or Form 3520-A, Annual Information Return of Foreign Trust With a U . S. Owner (see Instructions forForms 3520 and 3520-A) F- Yes F N o
3 Did the organization have an ownership interest in a foreign corporation during the tax year? If "Yes," theorganization may be required to file Form 5471, Information Return of U.S. Persons with Respect to Certain ForeignCorporations. (see Instructions for Form 5471) F- Yes F N o
4 Was the organization a direct or indirect shareholder of a passive foreign investment company or a qualifiedelecting fund during the tax year? If " Yes,"the organization may be required to fi le Form 8621 , Information Returnby a Shareholder of a Passive Foreign Investment Company or Qualified Electing Fund. (see Instructions for Form8621 ) F- Yes F No
5 Did the organization have an ownership interest in a foreign partnership during the tax year? If "Yes," theorganization may be required to file Form 8865, Return of U.S. Persons with Respect to Certain Foreign Partnerships.(see Instructions for Form 8865) F- Yes F N o
6 Did the organization have any operations in or related to any boycotting countries during the tax year? If "Yes,"the organization may be required to file Form 5713, International Boycott Report (see Instructions for Form5713). F- Yes F No
Schedule F ( Form 990) 2013
Additional Data
Software ID:
Software Version:
EIN: 74 -1180155
Name : THE METHODIST HOSPITAL
Schedule F (Form 990) 2013 Page 5
Supplemental InformationProvide the information required by Part I, line 2 (monitoring of funds); Part I, line 3, column (f) (accountingmethod; amounts of investments vs. expenditures per region); Part II, line 1 (accounting method); Part III(accounting method); and Part III, column (c) (estimated number of recipients), as applicable. Also completethis part to provide any additional information (see instructions).
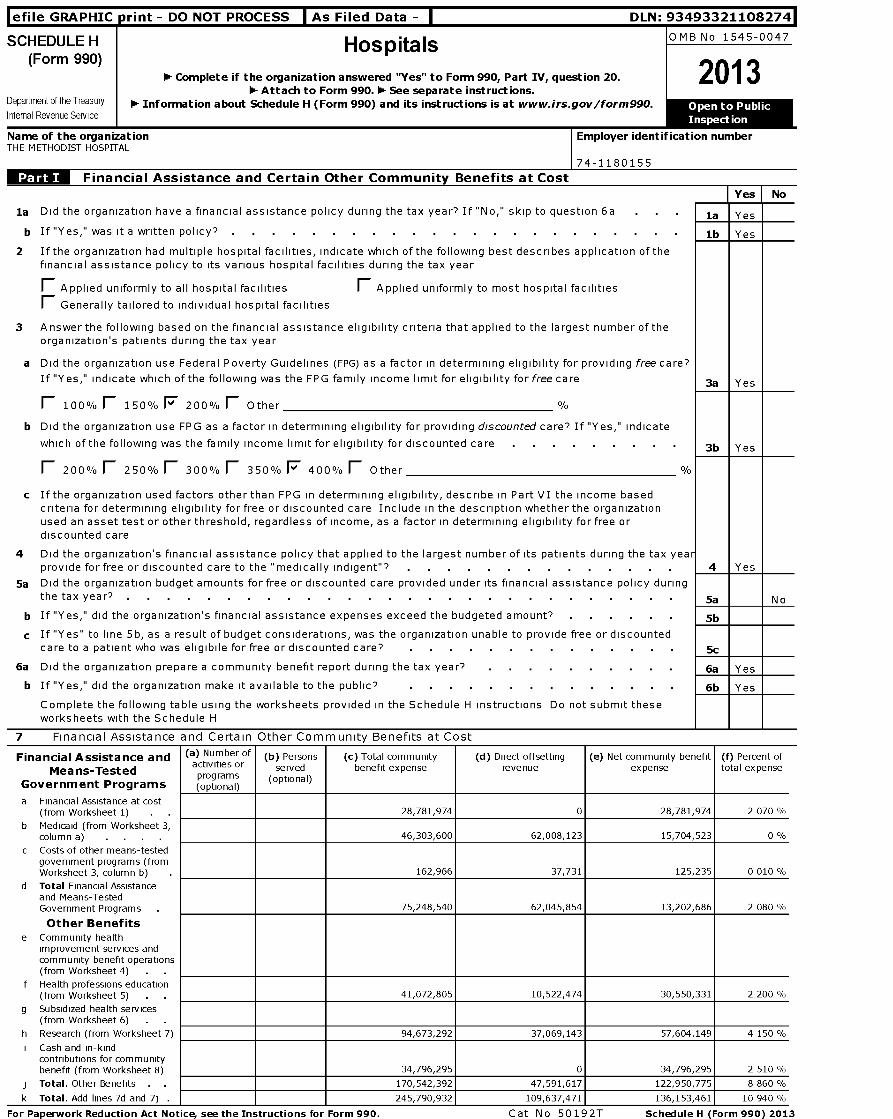
l efile GRAPHIC print - DO NOT PROCESS As Filed Data - DLN: 93493321108274
SCHEDULE H HospitalsOMB No 1545-0047
(Form 990)
20131- Complete if the organization answered "Yes" to Form 990, Part IV , question 20.1- Attach to Form 990. 1- See separate instructions.
Department of the Treasury 0- Information about Schedule H (Form 990) and its instructions is at www.irs.gov/form990. OpenInternal Revenue Service
I Inspection
Name of the organizationTHE METHODIST HOSPITAL
Employer identification number
74-1180155
Financial Assistance and Certain Other Community Benefits at CostYes I No
la Did the organization have a financial assistance policy during the tax year? If "No," skip to question 6a la Yes
b If "Yes," was it a written policy? . . . . . . . . . . . . . . . . . . . . . lb Yes
2 If the organization had multiple hospital facilities , indicate which of the following best describes application of thefinancial assistance policy to its various hospital facilities during the tax year
F Applied uniformly to all hospital facilities F Applied uniformly to most hospital facilities
F Generally tailored to individual hospital facilities
3 Answer the following based on the financial assistance eligibility criteria that applied to the largest number of theorganization ' s patients during the tax year
a Did the organization use Federal Poverty Guidelines ( FPG) as a factor in determining eligibility for providing free care?
If "Yes," indicate which of the following was the FPG family income limit for eligibility for free care 3a Yes
F 100% F 150% F 2000/o F Other %
b Did the organization use FPG as a factor in determining eligibility for providing discounted care? If "Yes ," indicate
which of the following was the family income limit for eligibility for discounted care 3b Yes
F 200% F 250% F 300% F 350% F 4000/o F Other %
c If the organization used factors other than FPG in determining eligibility, describe in Part VI the income basedcriteria for determining eligibility for free or discounted care Include in the description whether the organizationused an asset test or other threshold, regardless of income, as a factor in determining eligibility for free ordiscounted care
4 Did the organization's financial assistance policy that applied to the largest number of its patients during the tax yearprovide for free or discounted care to the "medically indigent"? 4 Yes
5a Did the organization budget amounts for free or discounted care provided under its financial assistance policy duringthe tax year? 5a No
b If "Yes," did the organization's financial assistance expenses exceed the budgeted amount? 5b
c If "Yes" to line 5b, as a result of budget considerations, was the organization unable to provide free or discountedcare to a patient who was eligibile for free or discounted care? 5c
6a Did the organization prepare a community benefit report during the tax year? 6a Yes
b If "Yes," did the organization make it available to the public? 6b Yes
Complete the following table using the worksheets provided in the Schedule H instructions Do not submit theseworksheets with the Schedule H
7 Financial Assistance and Certain Other Community Benefits at Cost
Financial Assistance and (a) Number of b Persons( )
c Total community( )
d Direct offsetting( ) g
a Net community benefit()
f Percent of( )
Means-Testedactivities or served benefit expense revenue expense total expense
Government Programsprograms(optional)
(optional)
a Financial Assistance at cost(from Worksheet 1) . 28,781,974 0 28,781,974 2 070 %
b Medicaid (from Worksheet 3,column a) . . . 46,303,600 62,008,123 -15,704,523 0 %
c Costs of other means-testedgovernment programs (fromWorksheet 3, column b) 162,966 37,731 125,235 0 010 %
d Total Financial Assistanceand Means-TestedGovernment Programs 75,248,540 62,045,854 13,202,686 2 080 %
Other Benefitse Community health
improvement services andcommunity benefit operations(from Worksheet 4) .
f Health professions education(from Worksheet 5) . 41,072,805 10,522,474 30,550,331 2 200 %
g Subsidized health services(from Worksheet 6) .
h Research (from Worksheet 7) 94,673,292 37,069,143 57,604,149 4 150 %
i Cash and in-kindcontributions for communitybenefit (from Worksheet 8) 34,796,295 0 34,796,295 2 510 %
j Total . Other Benefits . 170,542,392 47,591,617 122,950,775 8 860 %
k Total . Add lines 7d and 7j 245,790,932 109,637,471 136,153,461 10 940
For Paperwork Reduction Act Noticee see the Instructions for Form 990 . Cat N o 50192T Schedule H (Form 990) 2013
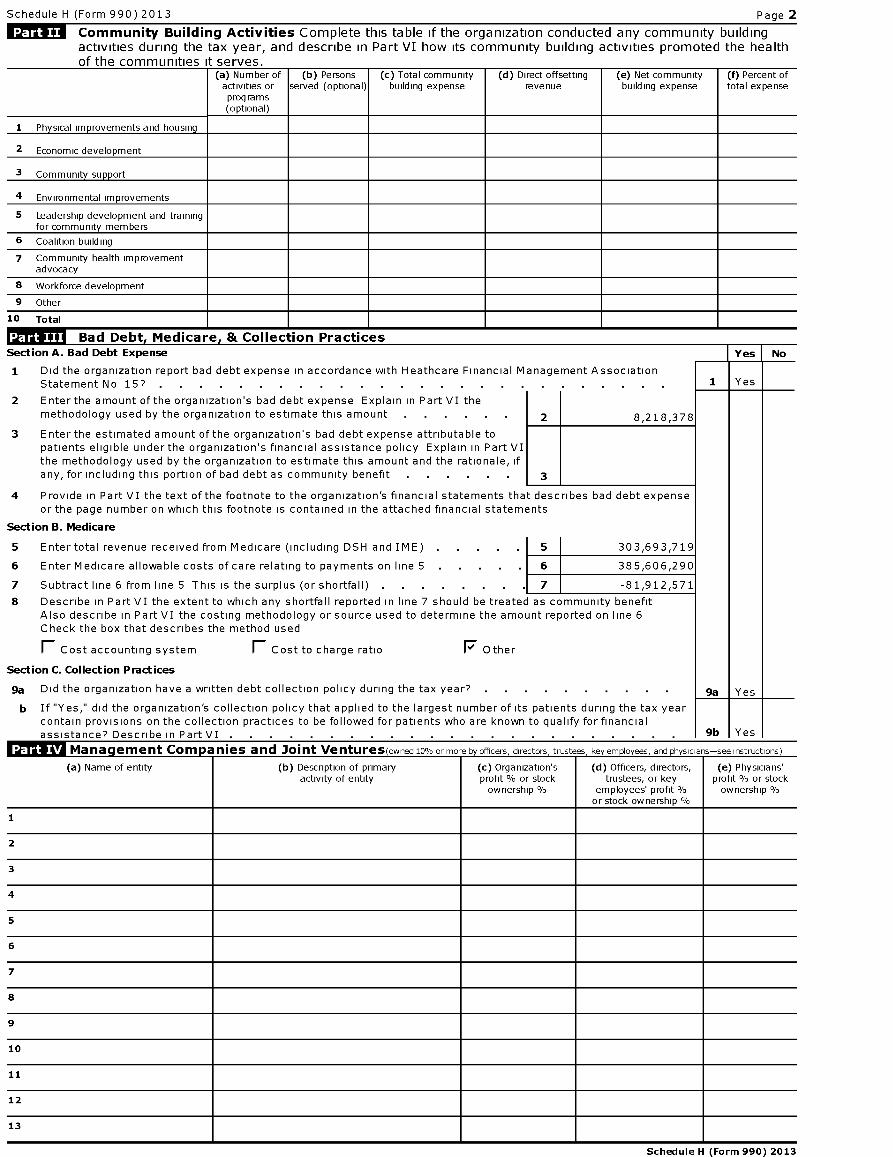
Schedule H (Form 990) 2013 Page 2
Community Building Activities Complete this table if the organization conducted any community buildingactivities during the tax year, and describe in Part VI how its community building activities promoted the healthof the communities it serves-
(a) Number ofactivities orprograms(optional)
(b) Personsserved (optional)
(c) Total communitybuilding expense
(d) Direct offsettingrevenue
(e) Net communitybuilding expense
(f) Percent oftotal expense
1 Ph y sical im p rovements and housin g
2 Economic development
3 Community su pp ort
4 Environmental improvements
5 Leadership development and trainingfor community members
6 Coalition building
7 Community health improvementadvocacy
8 Workforce development
9 Other
10 Total
Ill: Bad Debt , Medicare , & Collection PracticesSection A. Bad Debt Expense Yes No
1 Did the organization report bad debt expense in accordance with Heathcare Financial Management AssociationStatement No 15? . . . . . . . . . . . . . . . . . . . . 1 Yes
2 Enter the amount of the organization's bad debt expense Explain in Part VI themethodology used by the organization to estimate this amount 2 8,218,378
3 Enter the estimated amount of the organization's bad debt expense attributable topatients eligible under the organization's financial assistance policy Explain in Part VIthe methodology used by the organization to estimate this amount and the rationale, ifany, for including this portion of bad debt as community benefit 3
4 Provide in Part VI the text of the footnote to the organization's financial statements that describes bad debt expenseor the page number on which this footnote is contained in the attached financial statements
Section B. Medicare
5 Entertotal revenue received from Medicare (including DSH and IME) . 5 303,693,719
6 Enter Medicare allowable costs of care relating to payments on line 5 . 6 385,606,290
7 Subtract line 6 from line 5 This is the surplus (or shortfall) . 7 -81,912,571
8 Describe in Part VI the extent to which any shortfall reported in line 7 should be treated as community benefitAlso describe in Part VI the costing methodology or source used to determine the amount reported on line 6Check the box that describes the method used
r- Cost accounting system F Cost to charge ratio F Other
Section C. Collection Practices
9a Did the organization have a written debt collection policy during the tax year? .
b If "Yes," did the organization 's collection policy that applied to the largest number of its patients during the tax yearcontain provisions on the collection practices to be followed for patients who are known to qualify for financialassistance? Describe in Part VI 9b Yes. . . . . . . . . . . . . . . . . . . . . . .
MITUT Mananernent Comnanies and Joint VenturesrnvunPri ,n° nr mnra hvnfrarc rLrartnrc triictaac kavamnlnvaac and nhvananc-s inctrnrtinncl
(a) Name of entity (b) Description of primaryactivity of entity
(c) Organization'sprofit % or stockownership %
(d) Officers, directors,trustees, or key
employees' profit %or stock ownership
(e) Physicians'profit % or stockownership
1
2
3
4
5
6
7
8
9
10
11
12
13
Schedule H (Form 990) 2013
Schedule H (Form 990) 2013 Page 2
Facility Information
Section A . Hospital Facilities -^ s CD -m
0
(list in order of size from largest tosmallest-see instructions) o CL 0 aHow many hospital facilities did the 5 -0 (organization operate during the tax year? a
1 U
Name, address, primary website address,and state license number a Other (Describe) Facility reporting group
See Additional Data Table
Schedule H (Form 990) 2013
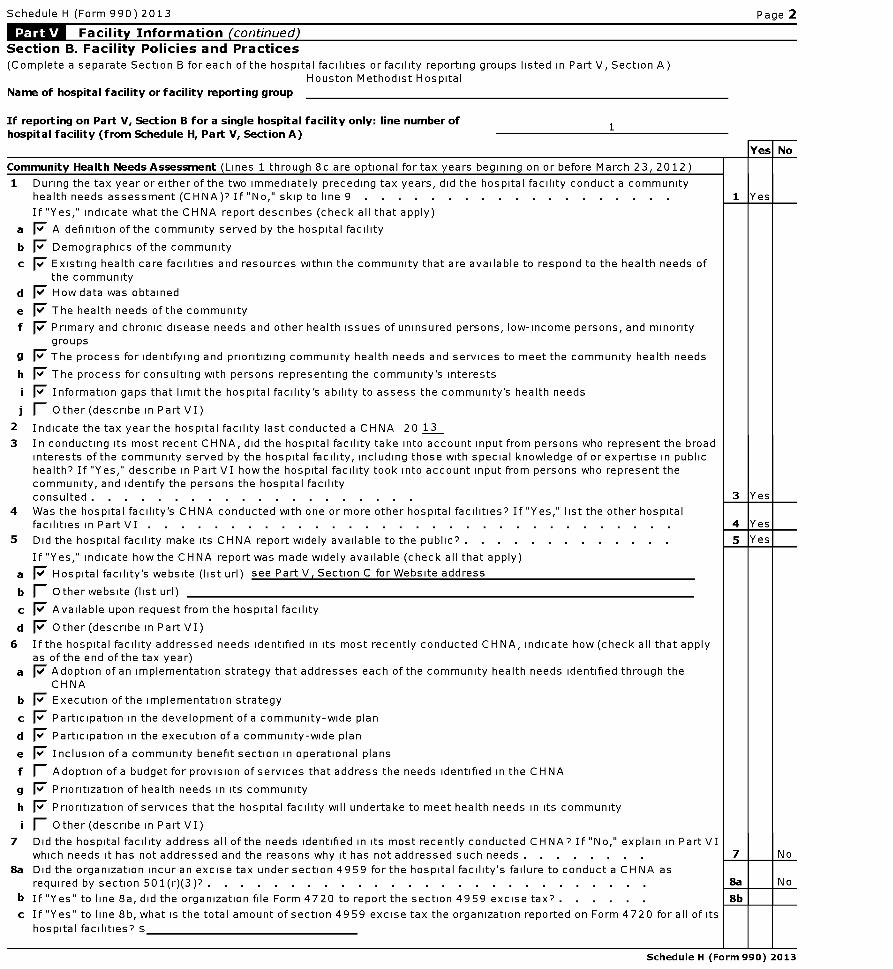
Schedule H (Form 990) 2013 Page 2
Facility Information (continued)Section B. Facility Policies and Practices(Complete a separate Section B for each of the hospital facilities or facility reporting groups listed in Part V, Section A)
Houston Methodist Hospital
Name of hospital facility or facility reporting group
If reporting on Part V, Section B for a single hospital facility only: line number ofhospital facility (from Schedule H, Part V, Section A)
1
1
a
b
c
d
e
f
9
h
2
3
4
5
a
b
c
d
6
a
b
c
d
e
f
9
h
7
8a
b
c
munity Health Needs Assessment ( Lines 1 through 8c are optional for tax years begining on or before March 23, 2012)
During the tax year or either of the two immediately preceding tax years , did the hospital facility conduct a communityhealth needs assessment (CHNA)? If "No," skip to line 9 . . . . . . . . . . . . . . . . . . .
If "Yes," indicate what the CHNA report describes ( check all that apply)
F A definition of the community served by the hospital facility
F Demographics of the community
7 Existing health care facilities and resources within the community that are available to respond to the health needs ofthe community
F' How data was obtained
F' The health needs of the community
7 Primary and chronic disease needs and other health issues of uninsured persons, low- income persons , and minoritygroups
I The process for identifying and prioritizing community health needs and services to meet the community health needs
I The process for consulting with persons representing the community's interests
I Information gaps that limit the hospital facility's ability to assess the community's health needs
I Other ( describe in Part VI)
Indicate the tax year the hospital facility last conducted a CHNA 20 13
In conducting its most recent CHNA, did the hospital facility take into account input from persons who represent the broadinterests of the community served by the hospital facility, including those with special knowledge of or expertise in publichealth? If "Yes ," describe in Part VI how the hospital facility took into account input from persons who represent thecommunity , and identify the persons the hospital facilityconsulted . . . . . . . . . . . . . . . . . . . .
Was the hospital facility's CHNA conducted with one or more other hospital facilities? If "Yes," list the other hospitalfacilities in Part VI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Did the hospital facility make its CHNA report widely available to the public? . . . . . . . . . . . . .
If "Yes," indicate how the CHNA report was made widely available ( check all that apply)
F Hospital facility's website ( list url ) see Part V , Section C for Website address
Other website ( list url)
F' Available upon request from the hospital facility
F' Other ( describe in Part VI)
If the hospital facility addressed needs identified in its most recently conducted CHNA, indicate how (check all that applyas of the end of the tax year)7' Adoption of an implementation strategy that addresses each of the community health needs identified through the
CHNA
F Execution of the implementation strategy
F Participation in the development of a community - wide plan
I Participation in the execution of a community - wide plan
I Inclusion of a community benefit section in operational plans
1' Adoption of a budget for provision of services that address the needs identified in the CHNA
F Prioritization of health needs in its community
F Prioritization of services that the hospital facility will undertake to meet health needs in its community
1' Other ( describe in Part VI)
Did the hospital facility address all of the needs identified in its most recently conducted CHNA? If "No," explain in Part VIwhich needs it has not addressed and the reasons why it has not addressed such needs . . . . . . . .
Did the organization incur an excise tax under section 4959 for the hospital facility's failure to conduct a CHNA asrequired by section 501 (r)(3)? . . . . . . . . . . . . . . . . . . . . . . . . . . .
If "Yes" to line 8a, did the organization file Form 4720 to report the section 4959 excise tax? . . . . . .
If "Yes" to line 8b, what is the total amount of section 4959 excise tax the organization reported on Form 4720 for all of its
hospital facilities? $
No
1 Yes
3 Yes
4 Yes
8a N o
Schedule H (Form 990) 2013
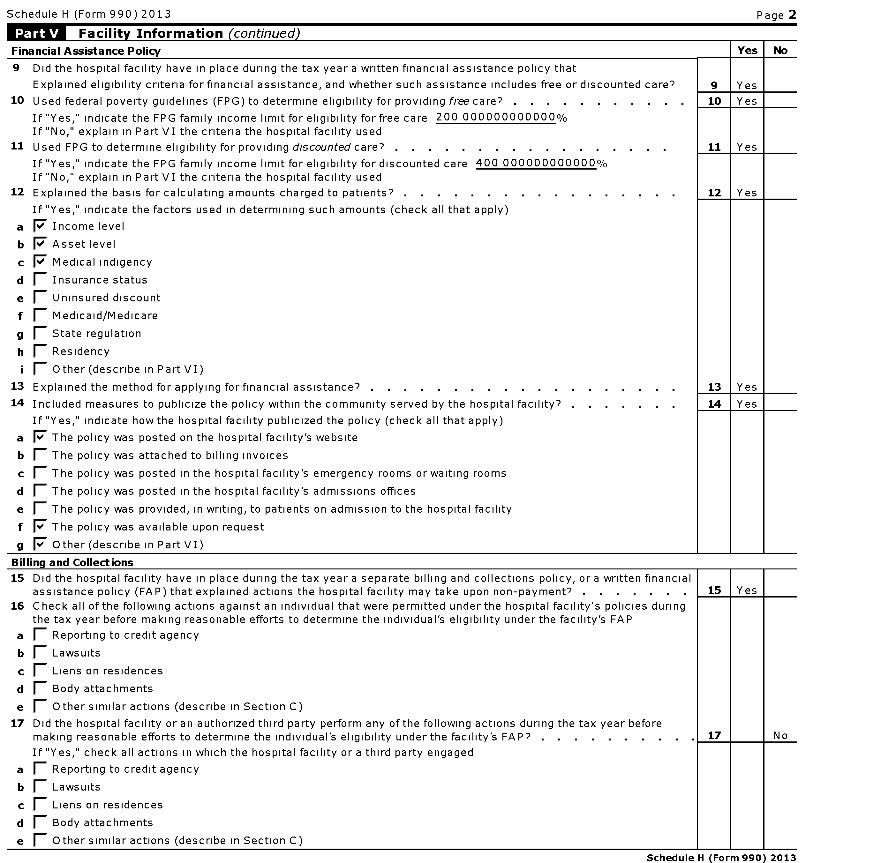
Schedule H (Form 990) 2013 Page 2
Facility Information (continued)
Financial Assistance Policy Yes No
9 Did the hospital facility have in place during the tax year a written financial assistance policy that
Explained eligibility criteria for financial assistance, and whether such assistance includes free or discounted care? 9 Yes
10 Used federal poverty guidelines (FPG) to determine eligibility for providing free care? . . . . . . . . . . . 10 Yes
If "Yes," indicate the FPG family income limit for eligibility for free care 200 000000000000 %
If "No," explain in Part VI the criteria the hospital facility used
11 Used FPG to determine eligibility for providing discounted care? . . . . . . . . . . . . . . . . . 11 Yes
If "Yes," indicate the FPG family income limit for eligibility for discounted care 400 000000000000 %
If "No," explain in Part VI the criteria the hospital facility used
12 Explained the basis for calculating amounts charged to patients? . . . . . . . . . . . . . . . . . 12 Yes
If "Yes," indicate the factors used in determining such amounts (check all that apply)
a F' Income level
b F' Asset level
c F' Medical indigency
d F' Insurance status
e F' Uninsured discount
f F' Medicaid/Medicare
g F' State regulation
h F' Residency
i F' Other (describe in Part VI)
13 Explained the method for applying for financial assistance? . . . . . . . . . . . . . . . . . . . 13 Yes
14 Included measures to publicize the policy within the community served by the hospital facility? . . . . . . . 14 Yes
If "Yes," indicate how the hospital facility publicized the policy (check all that apply)
a I The policy was posted on the hospital facility's website
b 1 The policy was attached to billing invoices
c 1 The policy was posted in the hospital facility's emergency rooms or waiting rooms
d 1 The policy was posted in the hospital facility's admissions offices
e 1 The policy was provided, in writing, to patients on admission to the hospital facility
f F The policy was available upon request
g I Other (describe in Part VI)
Billing and Collections
15 Did the hospital facility have in place during the tax year a separate billing and collections policy, or a written financialassistance policy (FAP) that explained actions the hospital facility may take upon non-payment? . . . . . . . 15 Yes
16 Check all of the following actions against an individual that were permitted under the hospital facility's policies duringthe tax year before making reasonable efforts to determine the individual's eligibility under the facility's FAP
a F' Reporting to credit agency
b F' Lawsuits
c F' Liens on residences
d F' Body attachments
e F' Other similar actions (describe in Section C)
17 Did the hospital facility or an authorized third party perform any of the following actions during the tax year beforemaking reasonable efforts to determine the individual's eligibility under the facility's FAP? . . . . . . . 17 No
If "Yes," check all actions in which the hospital facility or a third party engaged
a F' Reporting to credit agency
b F' Lawsuits
c F' Liens on residences
d F' Body attachments
e F' Other similar actions (describe in Section C)
Schedule H (Form 990) 2013
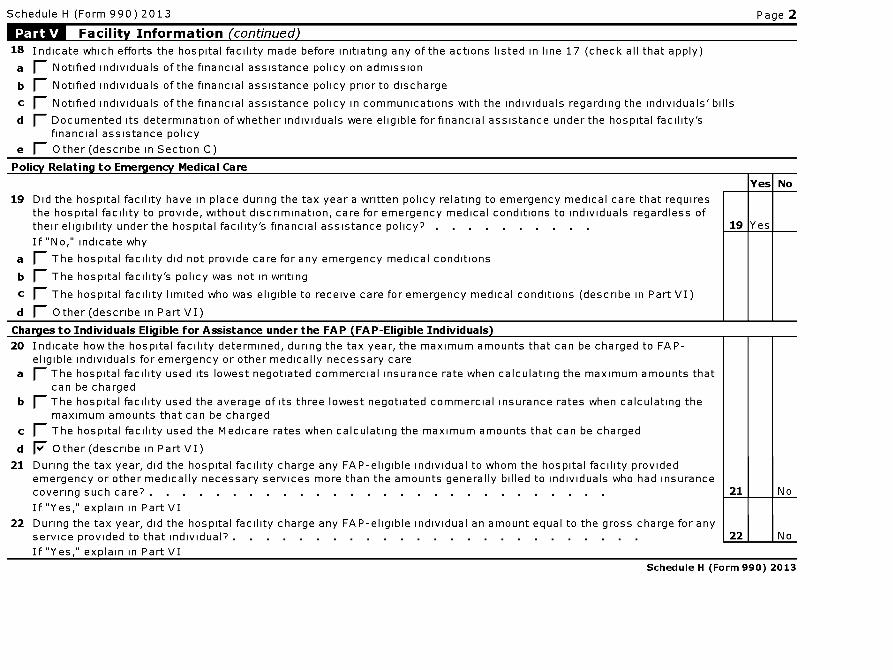
Schedule H (Form 990) 2013 Page 2
Facility Information (continued)
18 Indicate which efforts the hospital facility made before initiating any of the actions listed in line 17 (check all that apply)
a F Notified individuals of the financial assistance policy on admission
b F Notified individuals of the financial assistance policy prior to discharge
c F Notified individuals of the financial assistance policy in communications with the individuals regarding the individuals' bills
d F- Documented its determination of whether individuals were eligible for financial assistance under the hospital facility'sfinancial assistance policy
e 1 Other (describe in Section C)
Policy Relating to Emergency Medical Care
19 Did the hospital facility have in place during the tax year a written policy relating to emergency medical care that requiresthe hospital facility to provide, without discrimination, care for emergency medical conditions to individuals regardless oftheir eligibility under the hospital facility's financial assistance policy? . . . . . . . . . .
If "No," indicate why
1 The hospital facility did not provide care for any emergency medical conditions
1 The hospital facility's policy was not in writing
1 The hospital facility limited who was eligible to receive care for emergency medical conditions ( describe in Part VI)
1 Other ( describe in Part VI)
No
Charges to Individuals Eligible for Assistance under the FAP (FAP-Eligible Individuals)
20 Indicate how the hospital facility determined, during the tax year, the maximum amounts that can be charged to FA P-eligible individuals for emergency or other medically necessary care
a F- The hospital facility used its lowest negotiated commercial insurance rate when calculating the maximum amounts thatcan be charged
b F- The hospital facility used the average of its three lowest negotiated commercial insurance rates when calculating themaximum amounts that can be charged
c 1 The hospital facility used the Medicare rates when calculating the maximum amounts that can be charged
d I Other (describe in Part VI)
21 During the tax year, did the hospital facility charge any FAP-eligible individual to whom the hospital facility providedemergency or other medically necessary services more than the amounts generally billed to individuals who had insurancecovering such care? . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21 No
If "Yes," explain in Part VI
22 During the tax year, did the hospital facility charge any FAP-eligible individual an amount equal to the gross charge for anyservice provided to that individual? . . . . . . . . . . . . . . . . . . . . . . . . . 22 No
If "Yes," explain in Part VI
Schedule H (Form 990) 2013
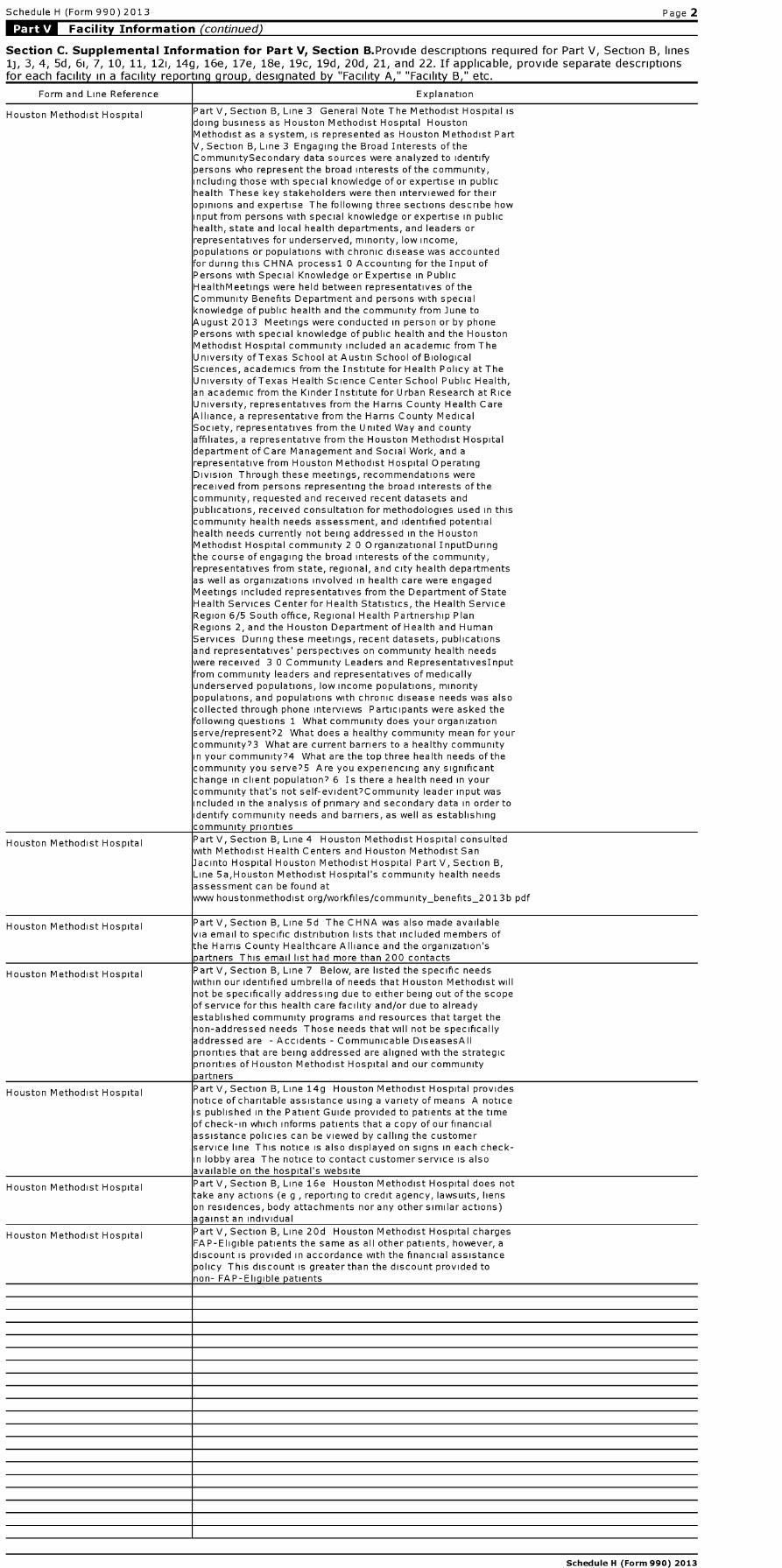
Schedule H (Form 990) 2013 Page 2
Facility Information (continued)
Section C. Supplemental Information for Part V, Section B.Provide descriptions required for Part V, Section B, lines1j, 3, 4, 5d, 61, 7, 10, 11, 121, 14g, 16e, 17e, 18e, 19c, 19d, 20d, 21, and 22. If applicable, provide separate descriptionsfor each facility in a facility re p ortin g g rou p, desig nated by "Facility A , " "Facility B , " etc.
Form and Line Reference Explanation
Houston Methodist Hospital Part V, Section B, Line 3 General Note The Methodist Hospital isdoing business as Houston Methodist Hospital HoustonMethodist as a system, is represented as Houston Methodist Part
Section B, Line 3 Engaging the Broad Interests of theCommunitySecondary data sources were analyzed to identifypersons who represent the broad interests of the community,ncluding those with special knowledge of or expertise in publichealth These key stakeholders were then interviewed for theiropinions and expertise The following three sections describe hownput from persons with special knowledge or expertise in publichealth, state and local health departments, and leaders orrepresentatives for underserved, minority, low income,populations or populations with chronic disease was accountedfor during this CHNA processl 0 Accounting for the Input ofPersons with Special Knowledge or Expertise in PublicHealthMeetings were held between representatives of theCommunity Benefits Department and persons with specialknowledge of public health and the community from June tougust 2013 Meetings were conducted in person or by phone
Persons with special knowledge of public health and the HoustonMethodist Hospital community included an academic from TheUniversity of Texas School at Austin School of BiologicalSciences, academics from the Institute for Health Policy at TheUniversity of Texas Health Science Center School Public Health,an academic from the Kinder Institute for U rban Research at RiceUniversity, representatives from the Harris County Health CareAlliance, a representative from the Harris County MedicalSociety, representatives from the United Way and countyaffiliates, a representative from the Houston Methodist Hospitaldepartment of Care Management and Social Work, and arepresentative from Houston Methodist Hospital OperatingDivision Through these meetings, recommendations werereceived from persons representing the broad interests of thecommunity, requested and received recent datasets andpublications, received consultation for methodologies used in thiscommunity health needs assessment, and identified potentialhealth needs currently not being addressed in the HoustonMethodist Hospital community 2 0 Organizational InputDuringthe course of engaging the broad interests of the community,representatives from state, regional, and city health departmentsas well as organizations involved in health care were engagedMeetings included representatives from the Department of StateHealth Services Center for Health Statistics, the Health ServiceRegion 6/5 South office, Regional Health Partnership PlanRegions 2, and the Houston Department of Health and HumanServices During these meetings, recent datasets, publicationsand representatives' perspectives on community health needswere received 3 0 Community Leaders and Representativeslnputfrom community leaders and representatives of medicallyunderserved populations, low income populations, minoritypopulations, and populations with chronic disease needs was alsocollected through phone interviews Participants were asked thefollowing questions 1 What community does your organizationserve/represent?2 What does a healthy community mean for yourcommunity?3 What are current barriers to a healthy communityn your community?4 What are the top three health needs of thecommunity you serve?5 Are you experiencing any significantchange in client population? 6 Is there a health need in yourcommunity that's not self-evident?Community leader input wasncluded in the analysis of primary and secondary data in order todentify community needs and barriers, as well as establishingcommunit y p riorities
Houston Methodist Hospital Part V, Section B, Line 4 Houston Methodist Hospital consultedwith Methodist Health Centers and Houston Methodist SanJacinto Hospital Houston Methodist Hospital Part V, Section B,Line 5a,Houston Methodist Hospital's community health needsassessment can be found atwww houstonmethodist org/workfiles/community_benefits_2013b pdf
Houston Methodist Hospital Part V, Section B, Line 5d The CHNA was also made availablevia email to specific distribution lists that included members ofthe Harris County Healthcare Alliance and the organization'sp artners This email list had more than 200 contacts
Houston Methodist Hospital Part V, Section B, Line 7 Below, are listed the specific needswithin our identified umbrella of needs that Houston Methodist willnot be specifically addressing due to either being out of the scopeof service for this health care facility and/or due to alreadyestablished community programs and resources that target thenon-addressed needs Those needs that will not be specificallyaddressed are - Accidents - Communicable DiseasesAllpriorities that are being addressed are aligned with the strategicpriorities of Houston Methodist Hospital and our communitypartners
Houston Methodist Hospital Part V, Section B, Line 14g Houston Methodist Hospital providesnotice of charitable assistance using a variety of means A notices published in the Patient Guide provided to patients at the timeof check-in which informs patients that a copy of our financialassistance policies can be viewed by calling the customerservice line This notice is also displayed on signs in each check-in lobby area The notice to contact customer service is alsoavailable on the hos p ital's website
Houston Methodist Hospital Part V, Section B, Line 16e Houston Methodist Hospital does nottake any actions (e g , reporting to credit agency, lawsuits, lienson residences, body attachments nor any other similar actions)against an individual
Houston Methodist Hospital Part V, Section B, Line 20d Houston Methodist Hospital chargesFAP-Eligible patients the same as all other patients, however, adiscount is provided in accordance with the financial assistancepolicy This discount is greater than the discount provided tonon- FAP-Eli g ible p atients
Schedule H (Form 990) 2013
Schedule H (Form 990) 2013 Page 2
MVIVI-Facility Information (continued)
Section D . Other Health Care Facilities That Are Not Licensed, Registered , or Similarly Recognized as aHospital Facility(list in order of size, from largest to smallest)
How many non-hospital health care facilities did the organization operate during the tax year?
Name and address Typ e of Facility ( describe )
1
2
3
4
5
6
7
8
9
10
Schedule H (Form 990) 2013
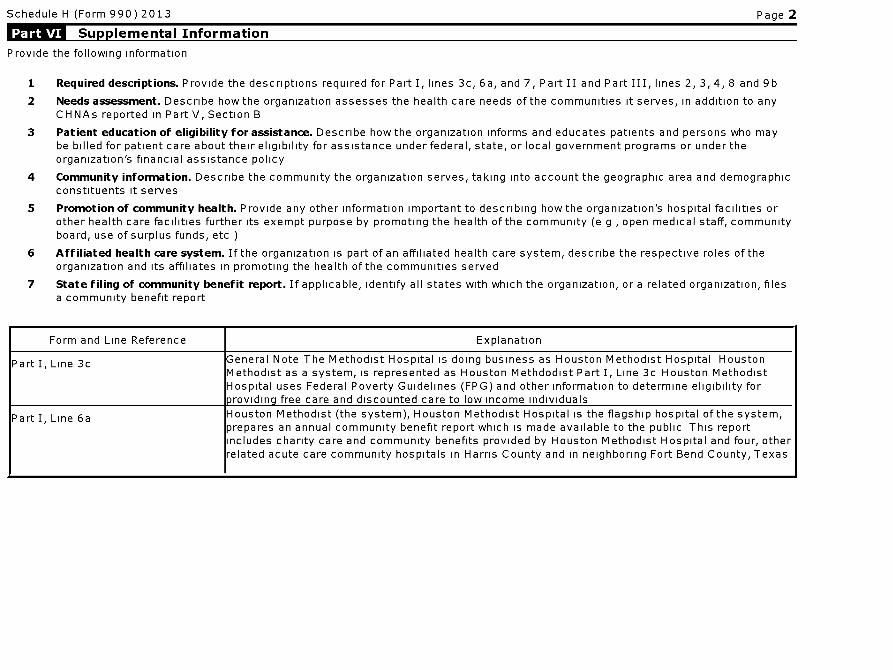
Schedule H (Form 990) 2013 Page 2
Supplemental Information
Provide the following information
1 Required descriptions. Provide the descriptions required for Part I, lines 3c, 6a, and 7, Part II and Part III, lines 2, 3, 4, 8 and 9b
2 Needs assessment . Describe how the organization assesses the health care needs of the communities it serves, in addition to anyCHNAs reported in Part V, Section B
3 Patient education of eligibility for assistance . Describe how the organization informs and educates patients and persons who maybe billed for patient care about their eligibility for assistance under federal, state, or local government programs or under theorganization's financial assistance policy
4 Community information . Describe the community the organization serves, taking into account the geographic area and demographicconstituents it serves
5 Promotion of community health . Provide any other information important to describing how the organization's hospital facilities orother health care facilities further its exempt purpose by promoting the health of the community (e g , open medical staff, communityboard, use of surplus funds, etc )
6 Affiliated health care system . If the organization is part of an affiliated health care system, describe the respective roles of theorganization and its affiliates in promoting the health of the communities served
7 State filing of community benefit report . If applicable, identify all states with which the organization, or a related organization, filesa community benefit report
Form and Line Reference Explanation
Part I, Line 3c General Note The Methodist Hospital is doing business as Houston Methodist Hospital HoustonMethodist as a system, is represented as Houston Methdodist Part I, Line 3c Houston MethodistHospital uses Federal Poverty Guidelines (FPG) and other information to determine eligibility forp rovidin g free care and discounted care to low income individuals
Part I, Line 6a Houston Methodist (the system), Houston Methodist Hospital is the flagship hospital of the system,prepares an annual community benefit report which is made available to the public This reportincludes charity care and community benefits provided by Houston Methodist Hospital and four, otherrelated acute care community hospitals in Harris County and in neighboring Fort Bend County, Texas
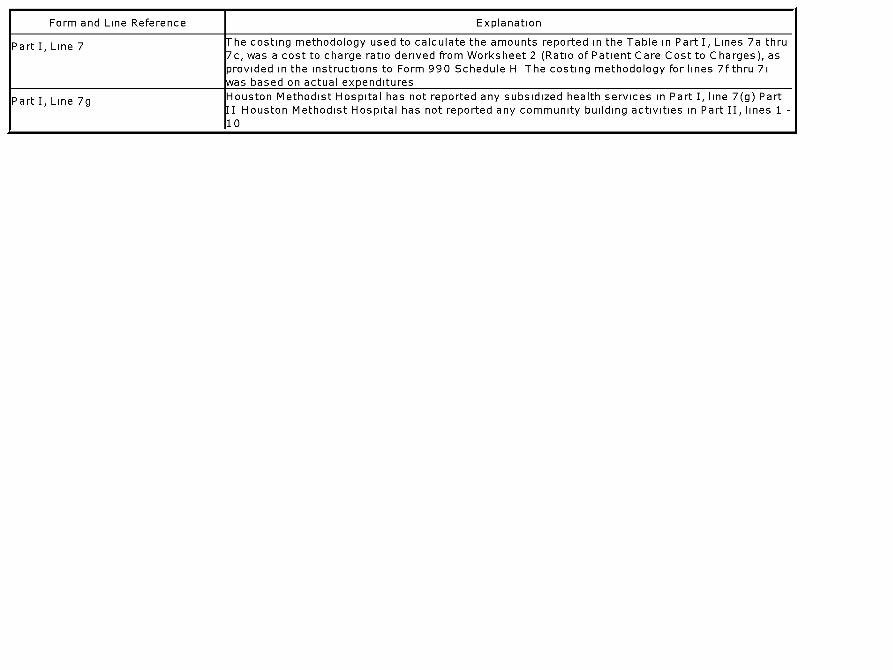
Form and Line Reference Explanation
Part I, Line 7 he costing methodology used to calculate the amounts reported in the Table in Part I, Lines 7a thru7c, was a cost to charge ratio derived from Worksheet 2 (Ratio of Patient Care Cost to Charges), asprovided in the instructions to Form 990 Schedule H The costing methodology for lines 7fthru 7iwas based on actual ex p enditures
Part I, Line 7g Houston Methodist Hospital has not reported any subsidized health services in Part I, line 7(g) PartII Houston Methodist Hospital has not reported any community building activities in Part II, lines 1 -10
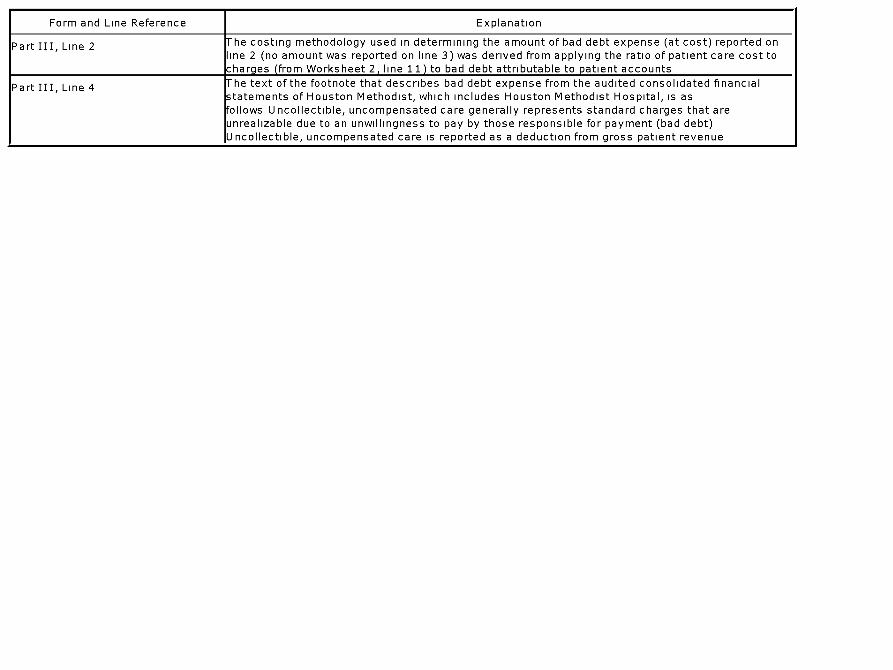
Form and Line Reference Explanation
Part III, Line 2 he costing methodology used in determining the amount of bad debt expense (at cost) reported online 2 (no amount was reported on line 3) was derived from applying the ratio of patient care cost tocharg es ( from Worksheet 2 , line 11 ) to bad debt attributable to p atient accounts
Part III, Line 4 he text of the footnote that describes bad debt expense from the audited consolidated financialstatements of Houston Methodist, which includes Houston Methodist Hospital, is asfollows Uncollectible, uncompensated care generally represents standard charges that areunrealizable due to an unwillingness to pay by those responsible for payment (bad debt)Uncollectible, uncompensated care is reported as a deduction from gross patient revenue
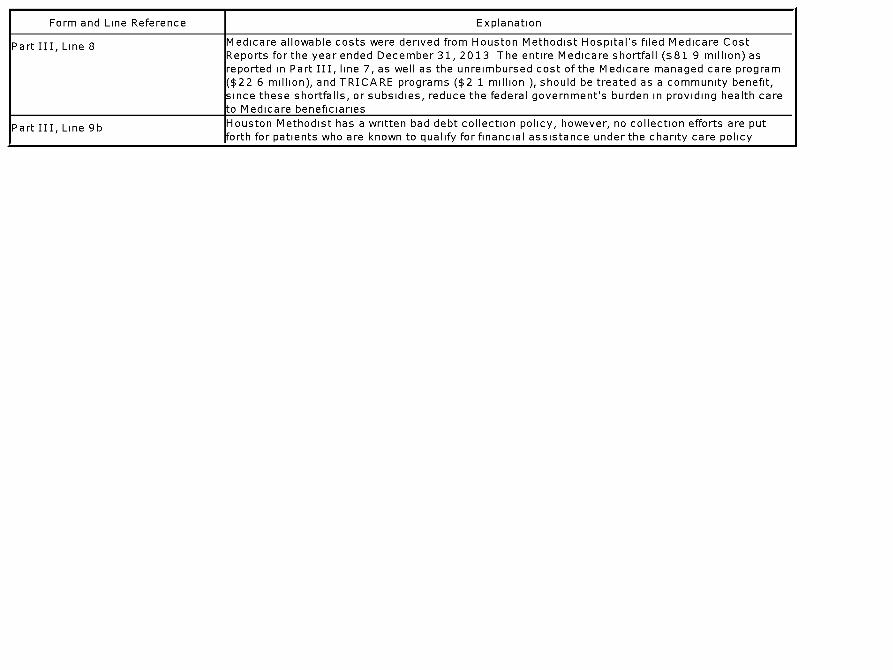
Form and Line Reference Explanation
Part III, Line 8 Medicare allowable costs were derived from Houston Methodist Hospital's filed Medicare CostReports for the year ended December 31, 2013 The entire Medicare shortfall ($81 9 million) asreported in Part III, line 7, as well as the unreimbursed cost of the Medicare managed care program($22 6 million), and TRICARE programs ($2 1 million ), should be treated as a community benefit,since these shortfalls, or subsidies, reduce the federal government's burden in providing health careto Medicare beneficiaries
Part III, Line 9b Houston Methodist has a written bad debt collection policy, however, no collection efforts are putforth for patients who are known to qualify for financial assistance under the charity care policy
Form and Line Reference Explanation
Part VI, Line 2 Houston Methodist utilized several different methods to identify its Community Health priorities(health care needs) of the communities it serves These methods include but are not limited to thereview of the Texas Institute of Health Policy research community data, Harris County Public Health& Environmental Services community data, Texas State Data Center and Office of the StateDemographer, Texas Department of State Health Services, Texas Cancer Registry, Center forDisease Control and Prevention, community advisory group committee reports for nonprofit clinicsand agencies (e g , Harris County Healthcare Alliance Primary Health Needs Assessment), TexasDepartment of Public Health selected health data, and community health status report for Harris,Liberty, Fort Bend, Chambers, Brazoria, Galveston and Montgomery counties Additionally, HoustonMethodist performs an annual Community Health Needs Assessment that evaluates the population ofHouston Methodist Hospital service area by looking at demographics, current health characteristicsin the community and access to healthcare Resources used to assess the health priorities for theCommunity Health Needs Assessment include but are not limited to Behavioral Risk FactorSurveillance System, The State of Health 2012, Health of Houston Survey and many other sources
Part VI, Line 3 Financial Assistance is provided in multiple locations within Houston Methodist, at the point ofregistration, during case management and at the time of collections post discharge Every check-inlocation has information posted in both English and Spanish stating how the patient can accessfinancial assistance Additionally, this information is posted on the Houston Methodist website and isincluded in the patient guide provided to the patient at the time of registration Houston Methodistfinancial counselors actively seek all uninsured inpatients and outpatients with scheduled servicesfor a personal visit During these visits, the financial counselors will screen the patient for financialassistance and will provide the patient with the financial assistance application The patient will thenbe provided a list of resources with contact information should the patient require further assistancein completing the application Houston Methodist utilizes an eligibility partner to work closely withpatients to qualify for State and Federal assistance programs (e g , Medicaid, SC HIP, Crime Victims,etc ) This eligibility partner will meet with all uninsured inpatients to discuss State and Federalassistance programs, where the patient is not eligible for these programs, Houston Methodist'sinternal financial assistance program is introduced Houston Methodist's case management unitworks closely with the patient during patient discharge management to ensure the patient isintroduced to all resources that may be needed post discharge (e g , home health, skilled nursing,etc ) The case management unit works with the patient to qualify the patient and to gain access tothese resources Additionally, the case management unit works closely with the financial counselorswhen the patient is identified as having a need for financial assistance Houston Methodist's patientaccounting unit works closely with all uninsured patients post discharge during the billing andcollections process Houston Methodist's collections personnel will verbally screen patients forfinancial assistance during collection calls, where applicable, the patient will be sent a financialassistance application either in English or Spanish Additionally, all billing statements provide thepatient with a phone number for customer service to obtain payment options Houston Methodistutilizes outside collection assistance, for both early out and bad debt collections Each collectionagency must adhere to Houston Methodist's financial assistance policy and philosophy during allcommunication and collection events with Houston Methodist patients Houston Methodist financialassistance application is reviewed periodically, additionally, Houston Methodist personnel areprovided with educational inservices in the administering of the financial assistance policy asneeded
Form and Line Reference Explanation
Part VI, Line 4 Houston Methodist Hospital is a Texas non-profit corporation which owns and operates a tertiarycare hospital and related medical office buildings, research, outpatient and other facilities in and nearthe Texas Medical Center in Houston, Texas Houston Methodist Hospital's primary services area iscomprised of8 counties - Brazoria, Chambers, Fort Bend, Galveston, Harris, Liberty, Montgomery andWallerwith a population estimated at more than 6 3 million for 2014 Harris County has the largestpopulation with an estimated 4 4 million as of January, 2014 From 2010 to 2014 the population hasincreased at a rate of 7% The population is expected to grow 9% in the next five years The specificmake-up of the service area includes Caucasian 38%, Hispanic 37%, African American 16%, Asian7% and other 2% Economically, the average household income is $75,945 Chambers County hasundergone the most growth in average household income (75%) from 2000 2014 to $84,917 HarrisCounty, comparatively, experienced the least growth in average household income from 2000-2014(21%) and projects a slight decrease in average household income growth to 2018 (-1%) to$72,349 Fort Bend County currently has the highest average household income at $93,471 andprojects to expand to nearly $99,000 by 2018 Liberty County currently has the lowest averagehousehold income at $58,326 and projects an expansion to $59,046 in 2018- still making it thecounty with the lowest average household income Examining the service area at the insurance level,the area consists of 80% insured and 20% uninsured
Part VI, Line 5 Houston Methodist Hospital, an acute care complex with 824 operating beds, 73 operating rooms,1,862 affiliated physicians and 6,101 employees, is the flagship of Houston Methodist Affiliated withthe Texas Annual Conference of the United Methodist Church, Houston Methodist Hospital worksclosely with local church leaders to bring compassion and spirituality to all of its endeavors and tohelp meet the health needs of the community it serves Houston Methodist Hospital's primaryacademic affiliates are Weill Cornell Medical College and NewYork Presbyterian Hospital HoustonMethodist Hospital also has affiliations with the University of Houston, Rice University, BaylorCollege of Medicine and others Houston Methodist Hospital is a teaching hospital and as part of itsteaching program it sponsored 239 medical residents in 33 accredited programs and 5 non-accredited programs in 2013 Governing BodyHouston Methodist Hospital is governed by a board ofdirectors comprised of members of the community where it is located Houston Methodist Hospital'sboard of directors includes members from the community as well as the system's President/CEO,Houston Methodist Hospital's medical staff president and the bishop of the Texas Annual Conferenceof the United Methodist Church Community CouncilsHouston Methodist Hospital also has communityinvolvement through advisory councils comprised of community members, including members of theHouston Methodist Board of Directors, who volunteer to create health-related programs forHoustonians One example is the Houston Methodist DeBakey Heart & Vascular Center Council,which is a group of Houston's leaders who advise the center on how it can best serve our patients andour community The group is comprised of opinion leaders whose experience in business and non-profit boards help shape our future direction and use of resources One way the council directs theseresources to promote the health of the community is through the Save a Life CPR/AED TrainingSessions For the last six years, the Houston Methodist DeBakey Heart & Vascular Center haspartnered with the Houston Texans, American Red Cross, and Texas Arrhythmia Institute to offermass CPR/AED training days to the Houston community The effort is spearheaded by the DeBakeyHeart & Vascular Center's council members and has successfully trained more than 3,800individuals since its inception Other councils include the Neurological Institute National Council andthe Center for Performing Arts Medicine Advisory Council Medical Staff ModelHouston MethodistHospital has an open medical staff model The open model gives patients access to physicians of allaffiliations Health EducationThe Houston Methodist Institute for Academic Medicine performsclinical and translational education with a patient-centered and interprofessional team basedapproach We continually maximize the effectiveness of our innovative teaching and learningprograms with evidence-based methodology grounded in educational research This approach,combined with a collaborative environment of learners from around the globe, creates the mosteffective educational experience for health and translational research professionals HoustonMethodist's mission of leading medicine is grounded in a commitment to translational,interdisciplinary and transformative research and education Our mission is to innovate in health caretechnology and train current and future clinicians and translational researchers in cutting edge healthcare advances The Institute for Academic Medicine supports research and education programs atHouston Methodist by providing the platform technologies and research programs, administrativesupport, staff, and facilities that are needed to rapidly translate discoveries made in the laboratoryand the clinic into new diagnostics, therapies and treatments The Office of Continuing MedicalEducation provides local, national and international education concentrated in areas where ourclinicians and scientists have recognized excellence and where our community has the greatestneed Since 2005, Houston Methodist Hospital has trained physicians in various medical andsurgical specialties Methodist sponsored 33 ACGME-accredited and 5 non-accredited programs in2013 The Houston Methodist Institute for Technology, Innovation and Education (MITIE) is acomprehensive, state-of-the-art education and research center for physicians who wish to acquirenew procedural skills and integrate new technologies into their practices Its research mission is toenhance the use of image guided technology to guide procedures, incorporate robotic surgery into theimage guided platform and develop new technology and procedural techniques Houston MethodistHospital also offers a medical laboratory science program with a 12-month track for professionals inpathology and laboratory medicine, an administrative fellowship and internship program for futurehealth care leaders, professional development programs for nursing, a pharmacy residency programand a postgraduate residency for cardiovascular surgery physician assistants Houston MethodistHospital has created the Finger Fellowship Program in Sustainable Health to allow young people toexperience the nexus of health science, policy, and community This fellowship gives exceptionalyoung people an opportunity to pursue individualized interdisciplinary research and to use thatexperience to lead improvements in health at the national, state or local level Medical ResearchTheHouston Methodist Research Institute, a subsidiary of Houston Methodist Hospital, was establishedin 2004 to conduct essential translational research In 2013 it was home to 270 principalinvestigators and credentialed researchers, 1,300 staff and trainees, and more than 640 ongoingclinical trials The Houston Methodist Research Institute is directly tied to clinicians and patients tohelp move the best in medical technology to the patient faster - for better prevention, diagnosis andtreatment of disease The Houston Methodist Research Institute is one way Houston MethodistHospital integrates its services, by bringing the research conducted in the laboratory to the patient'sbedside The discoveries made by our researchers quickly filter down to our hospitals in the form ofnew treatments and improved procedures Use of Surplus Fundsln 2013 Houston Methodist Hospital,through the Houston Methodist system's external charity care program, provided a total of $34 8million for services to the medically needy through external organizations that are already meetingthe health care needs that Houston Methodist has identified as priorities Patients qualified for ourinternal charity care were often identified through referrals by physicians, hospital staff, otherpatients and community agencies Houston Methodist Hospital provided $28 9 million in financialassistance for internal charity care based on the IRS definition of cost An internal charity careprogram provides services to the indigent at Houston Methodist Hospital and through affiliatedorganizations The majority of patients who qualified for charity care were educated about the programthrough signs posted throughout the hospital Other patients were referred by their physicians,hospital staff, other patients and through funded community agencies Surplus funds are also usedeach year to strengthen community service outreach to support low-income and uninsured patientsto help them attain access to comprehensive health care Services provided include primary healthcare, emergency and routine care, immunizations, dental care, psychological and case managementservices, well child examinations, sick visits, health education, health screenings, well woman examsand in-kind lab services and X-rays Houston Methodist Hospital's support allowed theseorganizations to enhance their services to low-income patients with diverse health needs Methodistprovided direct funding and/or in-kind services including lab tests, X-rays, immunizations, humanresources consultation and other services With Houston Methodist Hospital's support, agencies likeecino Health Centers and Good Neighbor Healthcare Centerwere positioned to meet Federally
Qualified Health Center designee qualifications, thereby allowing them to qualify for enhancedMedicare and Medicaid reimbursement Programs at Houston Methodist Hospital helped improveawareness of stroke signs, risk factors and prevention through the Stride4Stroke communityawareness campaign, which was in its seventh year in 2013 Programs addressed health disparitiesthrough our presence in minority communities and through outreach to women For further informationregarding what Houston Methodist Hospital is doing to benefit the community it serves, see theresponse to Part VI, Line 6
Form and Line Reference Explanation
Part VI, Line 6 Located in the heart of the Texas Medical Center , Houston Methodist Hospital is the flagship hospitalof Houston Methodist and serves patients from all over the world Houston Methodist includesHouston Methodist Sugar Land Hospital in Fort Bend County , Houston Methodist San Jacinto Hospitalin Baytown , Houston Methodist Willowbrook Hospital in northwest Houston and Houston MethodistWest Hospital which opened in December 2010 Houston Methodist Hospital shares the greatermission of Houston Methodist to provide high quality , cost-effective health care that delivers the bestvalue to the people we serve in a spiritual environment of caring in association with internationallyrecognized teaching and research Houston Methodist Hospital is among the country ' s largest non-profit health care providers In 2013, Houston Methodist Hospital treated 36,310 inpatients and301,478 outpatients It received 61,043 emergency room visits Houston Methodist Hospitalpromotes the health of the community and the mission of Houston Methodist by delivering the highestquality and safest health care to our patients Quality initiatives range from hand hygiene programs(with exceptionally good results), to patient fall and infection reduction programs Houston MethodistHospital was the first hospital in the Texas Medical Center to require its employees , vendors andvolunteers to receive the seasonal flu shot to protect our patients, those typically most vulnerable tocomplications from the flu Houston Methodist Hospital is the academic medical center in HoustonMethodist , bringing the community an institution dedicated to patient care, research and educationBy serving as a leading academic medical center, it provides the community quality patient care,leading research that can be quickly translated into treatments and the training of our country'sfuture doctors While all Houston Methodist hospitals provide quality patient care, Houston MethodistHospital expands the vision to include research and a comprehensive residency program Aside frompromoting the health of our community by delivering exceptional leading care to our patients, HoustonMethodist makes significant contributions through community benefits programs as describedbelow Community Benefit Activities and Health Servicesln 2013, Houston Methodist provided $56 2million for services to the medically needy through external organizations that are already meetingthe health care needs that Houston Methodist has identified as priorities Houston Methodistsupported the following grassroots agencies across the Greater Houston area, including thosecommunities served by our community hospitals -Access Health -Avondale House-Baylor College ofMedicine-Bering Omega Community Services-Boys and Girls Country of Houston, Inc -Breath of LifeChildren's Center , Inc -Casa De Esperanza de los Ninos , Inc -Chinese Community Center, Inc -CHRISTUS Home Care-El Centro de Corazon /Eastwood Health Clinic-Eye Care for Kids Foundation-Good Neighbor Healthcare Center-Harris County Clinical Services, Inc - Healthcare for the Homeless- Houston-HOPE Clinic-Houston Area Women ' s Center-Interfaith Community Clinic-Krist SamaritanCenters for Counseling and Education - Legacy Community Clinic-Matagorda Episcopal HospitalOutreach Program-Northwest Assistance Ministries-San Jose Clinic-Service Organization of GreaterHouston-Shalom Mobile Health Ministry-Star of Hope-The Center, Inc - The Centerfor Hearing andSpeech-The Rose-The Women 's Home-TOMAGWA Health Care Ministries-Vecino HealthCentersThis support allowed these organizations to leverage dollars and enhance their services tolow-income patients with diverse health needs Houston Methodist provided direct funding and/or in-kind services including lab tests, X-rays , immunizations , human resources consultation and otherservices With Methodist's support , agencies like Good Neighbor Healthcare Center were positionedto meet Federally Qualified Health Center designee qualifications , thereby allowing them to qualify forenhanced Medicare and Medicaid reimbursement EducationHouston Methodist Hospital's primaryacademic partner is Weill Cornell Medical College in NewYork The two institutions share bestpractices and collaborate on research , education and clinical care More than 350 Methodistphysicians have Weill Cornell faculty positions , and Houston Methodist Hospital sponsors more than250 of its own medical residents in various specialties - ranging from neurosurgery to pathology toobstetrics /gynecology - and hosts several more from other medical institutions In addition, HoustonMethodist Hospital collaborates with many other academic and medical institutions to promote thehealth of the community, including NewYork-Presbyterian Hospital, Rice University , Baylor Collegeof Medicine , University of Houston , Texas A&M University , Texas Children ' s Hospital, University ofT exas Health Science Center, Texas Woman's University and Prairie ViewA&M, amongothers Community InvolvementHouston Methodist Hospital actively develops awareness initiatives,sponsorships and programs that promote health and wellness, prevention and early detectionHouston Methodist Hospital staff and volunteers can be seen at health screenings , exercise andnutrition promotions , stress management clinics and other health promotion activities throughout theyear For example , Houston Methodist Hospital participated in the Houston Methodist's fourth annualStride4Stroke 5K Walk /Run The walk / run is part of the Houston Methodist ' s community strokeawareness campaign aimed at increasing stroke awareness and education in the community Morethan 2,800 employees and community participants joined this effort to raise public awareness andfunds for an event that clearly has an impact on the community Houston Methodist ConcussionCenter provides comprehensive services and a dedicated team of concussion specialists to educateathletes, especially student-athletes, about the importance of concussion awareness Through thecenter, student athletes have access to ImPACT (Immediate, Post Concussion Assessment andCognitive Testing ) testing, at their schools or at the Concussion Center ImPACT is the firstcomputerized concussion evaluation system In addition to providing clinical care, the concussioncenter staff educates the community about signs and symptoms , dangers and proper medicalmanagement The Center conducts outreach activities which benefit more than 1,000 Houston-arearesidents monthly The Nantz National Alzheimer Center at Houston Methodist Hospital advancesresearch and treatment of Alzheimer ' s disease, one of the biggest threats to the elderly population inour country It is projected that as many as 16 million people will have Alzheimer's by 2050 Thecenter, dedicated to finding a cure for Alzheimer ' s, addresses one of the biggest health crisesaffecting Americans today Houston Methodist Hospital promotes the health of the community byfulfilling Houston Methodist's mission through exceptional, high-quality patient care , education andresearch, affiliations with academic and medical partners for improved community health care, charitycare and community involvement Houston Methodist Hospital also cooperates with local entities toidentify community needs Members of Houston Methodist Hospital's executive team are on theboards of local organizations like the Greater Houston Health Care Alliance that advocate foreducational , environmental and health care issues that affect public policy and internationalcompanies that do business in Houston Houston Methodist ' s employees have a longstandingtradition of supporting efforts to improve the health and well-being of our community Our employeesdonate time , talent and mone y to man y g reat communit y causes
Continuation of Part VI, Line 6 Houston Methodist created a program called I CARE in Action , which provides employees paid timeto volunteer at approved community organizations The program encourages employees to becomeinvolved in the local communities Houston Methodist serves and provides the expertise and passionof Houston Methodist employees to assist others Hospital administration also allocates hours tocoordinate and support voluntary employee projects to meet specific community needs HoustonMethodist employees participated in or provided a service for the following - United Way Campaign-employee contributions - American Heart Association's Houston Heart Walk and Stroke Continuum ofCare-sponsorship , employees participated in Walk -National Multiple Sclerosis 150 Bike Tour(Houston-to - Austin )- sponsored employees participated in Bike Ride -Komen Race for the Cure-sponsorship , employees participated in Walk and volunteered-ADA Diabetes Walk-contributions /Walk-Stride4Stroke 5K Run/Walk-contributions/volunteers /Walk/Run-PAWS -corporatesponsorship-Star of Hope - donations - employees giving of their time to volunteer-Save a LifeCommunity Heart Training Day-Houston Methodist sponsored in conjunction w/American Red Cross&Texas Arrhythmia Institute-Adopt - a-Child / Family holiday program-employee participation-giftgiving and volunteer employee blood drive ( donations of blood, plasma and platelets)-Career Day-T alks-employee volunteering - Houston Food Bank-Texas Medical Center Food Drive - Corporatesponsorship - employees giving of their time to volunteer -Houston Area Women's Shelter - corporatesponsorship - Medical Bridges - hospital donations , corporate sponsorship and employees volunteeringtheir time-Habitat for H umanity-employees volunteering their time-San Jose Clinic-Art for Heart-corporate sponsorship and employees volunteering their time-DeBakey High School-Africanmerican Health Coalition-Texas Woman's University - The House of Amos-hospital donated
supplies-Houston Museum of Natural Science-employees volunteering their time Houston MethodistHospital operates a thriving volunteer program that offers members of the outside community anopportunity to participate in a number of patient-oriented activities including hospital visits,collecting and /or creating items to distribute to patients and wayfinding help for patients and familiesvisiting the complex for doctors' appointments and tests Identifying Community HealthIssuesHouston Methodist Hospital identified its community health priorities for 2013 using severalmethods including , but not limited to, review of the Texas Institute for Health Policy Researchcommunity data, Texas Department of Public Health selected health data, community health statusreports for Harris, Liberty , Fort Bend and Montgomery counties and community advisory groupscommittee reports for nonprofit clinics and agencies The review indicated that chronic diseases,including heart disease and stroke, are acute in our service area, exceeding the overall mortalityrates in Texas and peer counties Because stroke was identified as a primary killer and health careissue for people in our region , Houston Methodist in 2006 created the Stride4Stroke initiative toraise awareness about stroke and to raise funds for community stroke education A 5K Run /Walk eachspring allows members of the community to participate alongside hospital employees HoustonMethodist has initiated community education efforts by training and providing nurse-educators to thecommunity for public events , particularly in minority communities and for outreach to womenHouston Methodist also works to assist smaller hospitals in the community in developing their ownstroke programs and achievement of Primary Stroke Center status, while we offer a venue forcomprehensive stroke care to those patients from community hospitals that are not equipped to offermore than basic stroke care Another initiative has sought to increase early detection and communityawareness of cancer Houston Methodist Hospital annually stages a Men ' s Health Expo forcommunity awareness and education on men's health issues Houston Methodist Hospital alsosponsors and/or coordinates a number of events spotlighting women's health issues HoustonMethodist Hospital sponsored the Komen Race /Walk and Pink Ribbons campaign to promote breastcancer awareness as well as to communicate the importance of early detection of breast cancerSummaryAs a system, Houston Methodist made significant contributions through its communitybenefits and charity care program which have been a resource for patients in the community Basedon IRS cost definitions Houston Methodist provided $205 3 million in Charity Care and Certain otherCommunity Benefits for the year ended December 31, 2013 In addition , based on IRS costdefinitions Houston Methodist provided $186 6 million in care to Medicare, Medicare Managed Careand TRICARE program beneficiaries for the year ended December 31, 2013 Part VI, line 7 TX
l efile GRAPHIC p rint - DO NOT PROCESS As Filed Data - DLN: 93493321108274
Schedule I OMB No 1545-0047
(Form 990 ) Grants and Other Assistance to Organizations,Governments and Individuals in the United States 2013
Complete if the organization answered "Yes," to Form 990, Part IV, line 21 or 22.
Department of the Treasury ► Attach to Form 990 •
Internal Revenue Service ► Information about Schedule I (Form 990) and its instructions is at www.irs.gov/form990 .
Name of the organization Employer identification number
THE METHODIST HOSPITAL74-1180155
jlj^l General Information on Grants and Assistance
1 Does the organization maintain records to substantiate the amount of the grants or assistance, the grantees' eligibility for the grants or assistance, andthe selection criteria used to award the grants or assistance? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . F Yes 1 No
2 Describe in Part IV the organization's procedures for monitoring the use of grant funds in the United States
Grants and Other Assistance to Governments and Organizations in the United States . Complete if the organization answered "Yes" toForm 990, Part IV, line 21, for any recipient that received more than $5,000. Part II can be duplicated if additional space is needed.
(a) Name and address oforganization
or government
(b) EIN (c ) IRC Codesection
if applicable
( d) Amount of cashgrant
(e) Amount of non-cash
assistance
(f ) Method ofvaluation
(book, FMV,appraisal,other )
( g) Description ofnon-cash assistance
(h) Purpose of grantor assistance
See Additional Data Table
2 Entertotal number of section 501(c)(3) and government organizations listed in the line 1 table . ► 72
3 Enter total number of other organizations listed in the line 1 table . . 4
For Paperwork Reduction Act Noticee see the Instructions for Form 990 . Cat No 50055P Schedule I (Form 990) 2013
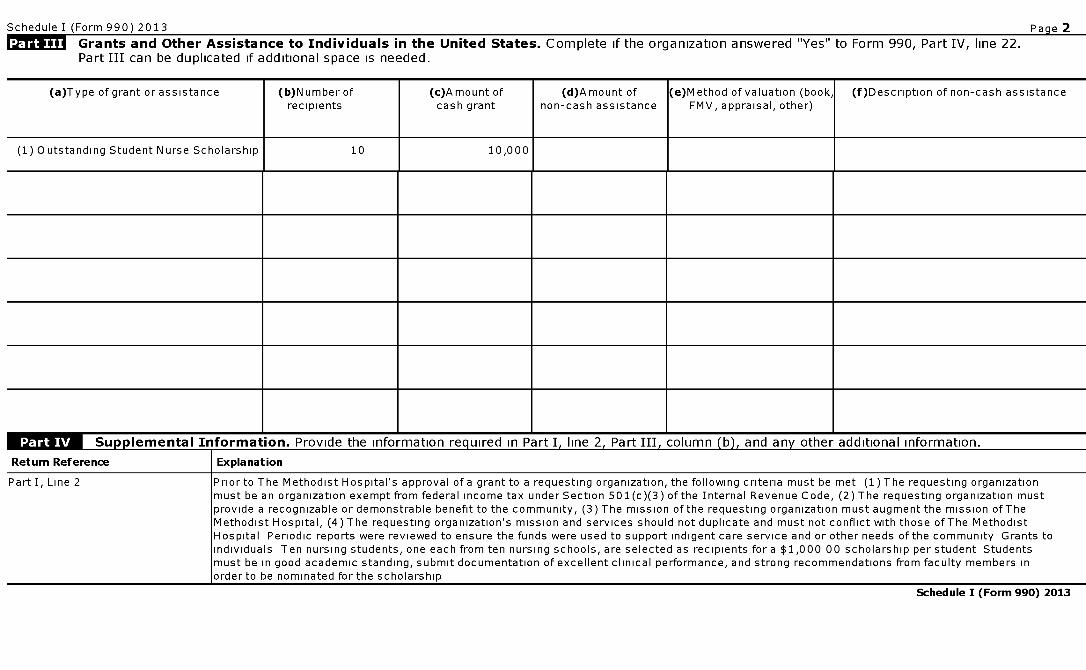
Schedule I (Form 990) 2013
Grants and Other Assistance to Individuals in the United States . Complete if the organization answered "Yes" to Form 990, Part IV, line 22.Part III can be duplicated if additional space is needed.
Pacie 2
(a)Type of grant or assistance (b)N umber ofrecipients
(c)A mount ofcash grant
(d)Amount ofnon-cash assistance
(e)Method of valuation (book,FMV, appraisal, other)
(f)Description of non-cash assistance
(1) Outstanding Student Nurse Scholarship 10 10,000
n 1 M Suuulemental Information . Provide the information reauired in Part I. line 2. Part III. column W. and any other additional information.
Return Reference I Explanation
Part I, Line 2 Prior to The Methodist Hospital's approval of a grant to a requesting organization, the following criteria must be met (1) The requesting organizationmust be an organization exempt from federal income tax under Section 501(c)(3) of the Internal Revenue Code, (2) The requesting organization mustprovide a recognizable or demonstrable benefit to the community, (3) The mission of the requesting organization must augment the mission of TheMethodist Hospital, (4) The requesting organization's mission and services should not duplicate and must not conflict with those of The MethodistHospital Periodic reports were reviewed to ensure the funds were used to support indigent care service and or other needs of the community Grants toindividuals Ten nursing students, one each from ten nursing schools, are selected as recipients for a $1,000 00 scholarship per student Studentsmust be in good academic standing, submit documentation of excellent clinical performance, and strong recommendations from faculty members inorder to be nominated for the scholarship
Schedule I (Form 990) 2013
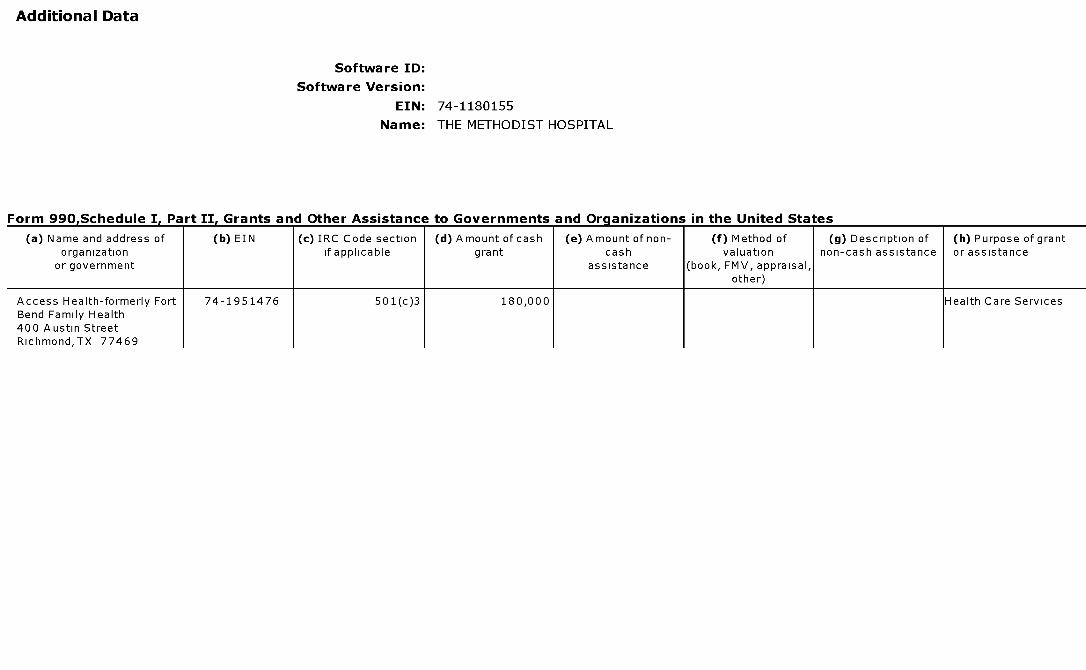
Additional Data
Software ID:
Software Version:
EIN: 74 -1180155
Name : THE METHODIST HOSPITAL
Form 990,Schedule I, Part II, Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Access Health-formerly Fort 74-1951476 501(c)3 180,000 Health Care ServicesBend Family Health400 Austin StreetRichmond,TX 77469
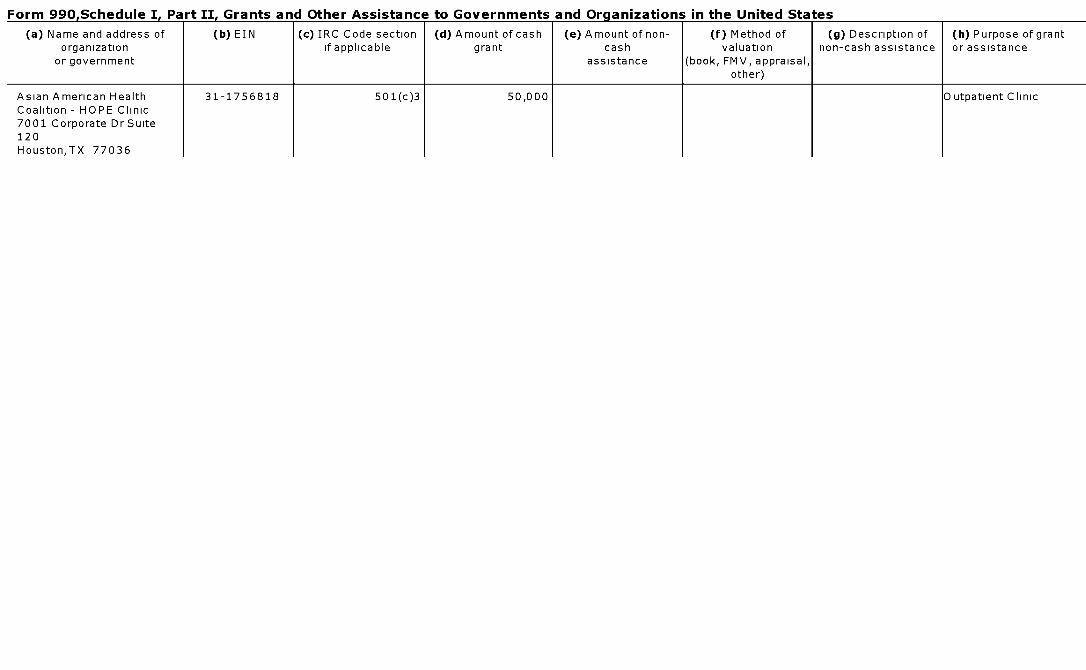
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Asian American Health 31-1756818 501(c)3 50,000 Outpatient ClinicCoalition - HOPE Clinic7001 Corporate Dr Suite120Houston,TX 77036
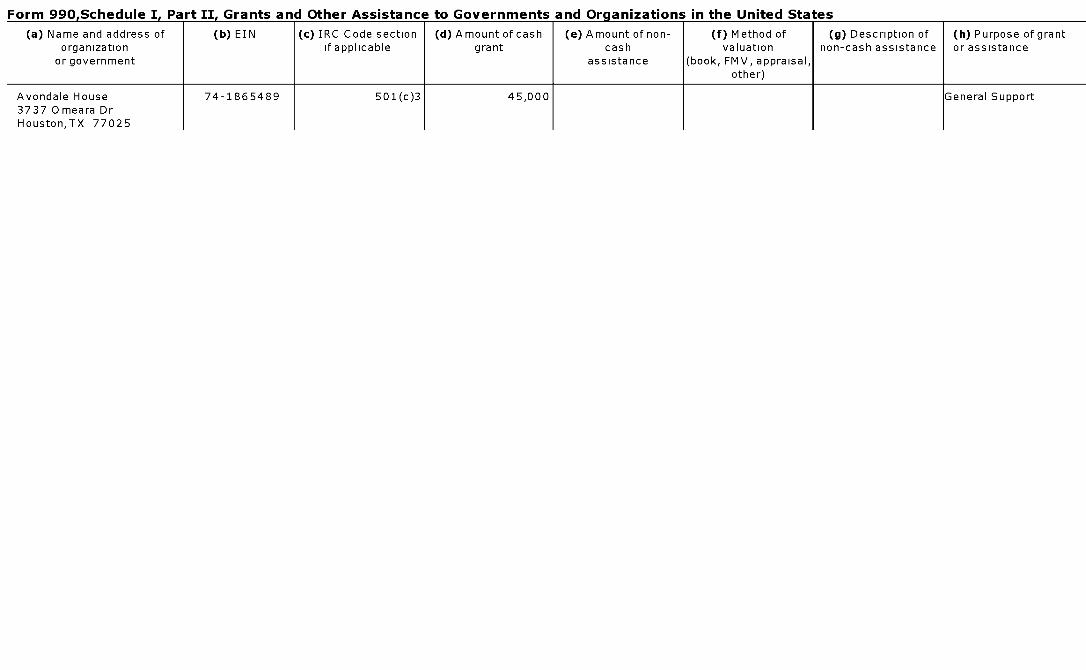
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of ( b) EIN (c ) IRC Code section ( d) Amount of cash (e) Amount of non- (f ) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Avondale House 74-1865489 501(c) 3 45,000 General Support3737 Omeara DrHouston,TX 77025
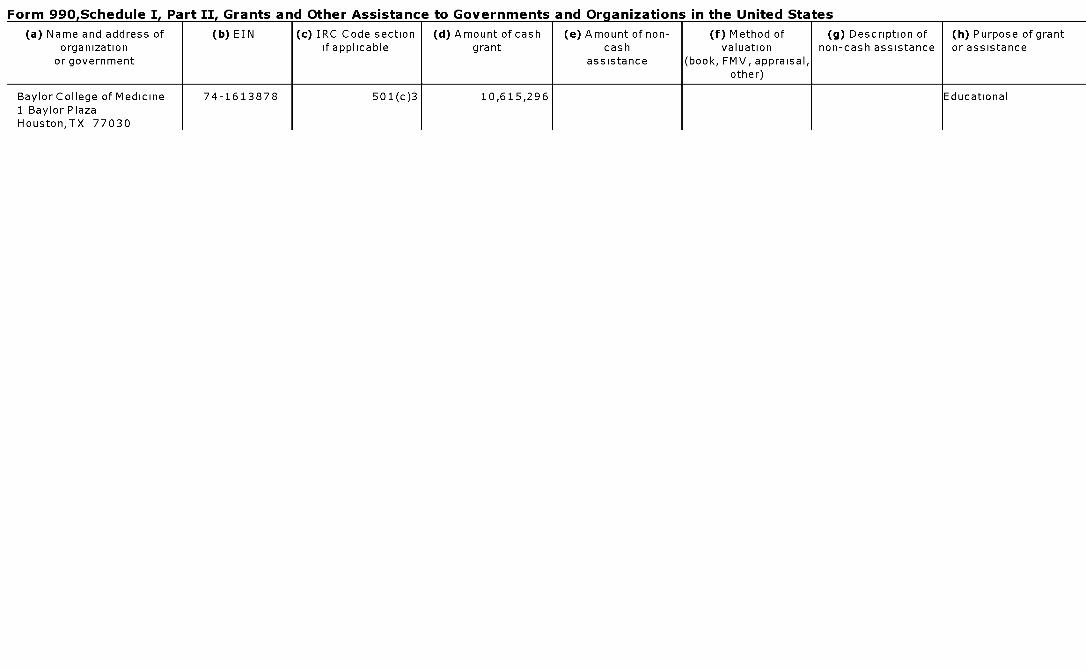
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Baylor College of Medicine 74-1613878 501(c)3 10,615,296 Educational1 Baylor PlazaHouston,TX 77030
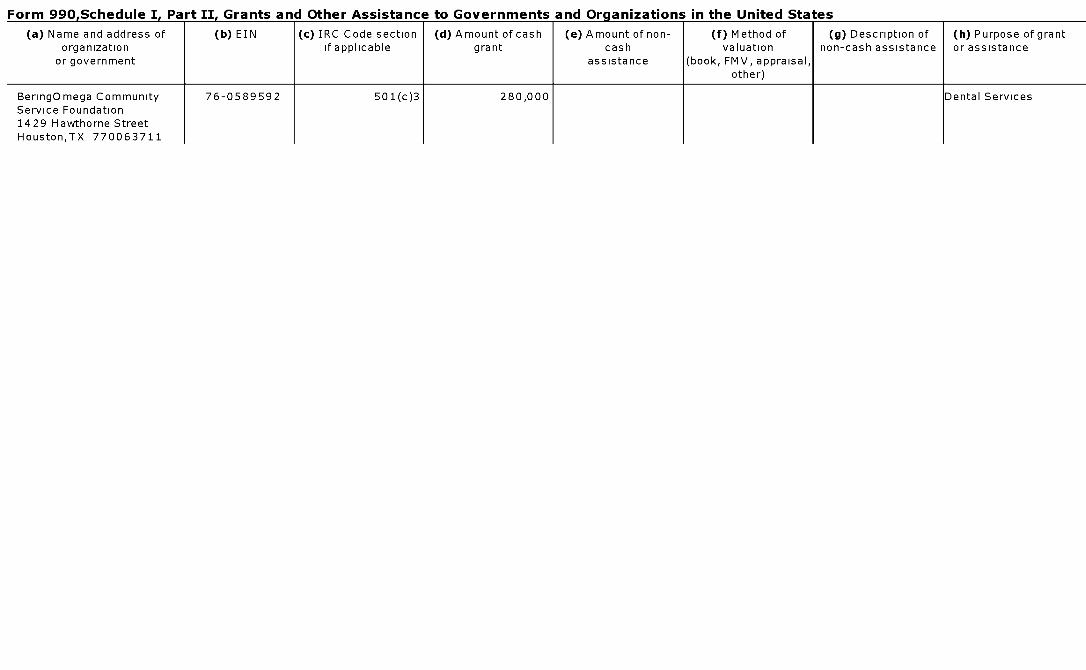
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of ( b) EIN (c ) IRC Code section (d) Amount of cash (e) Amount of non- (f ) Method of ( g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non - cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
BeringOmega Community 76-0589592 501(c ) 3 280,000 Dental ServicesService Foundation1429 Hawthorne StreetHouston,TX 770063711
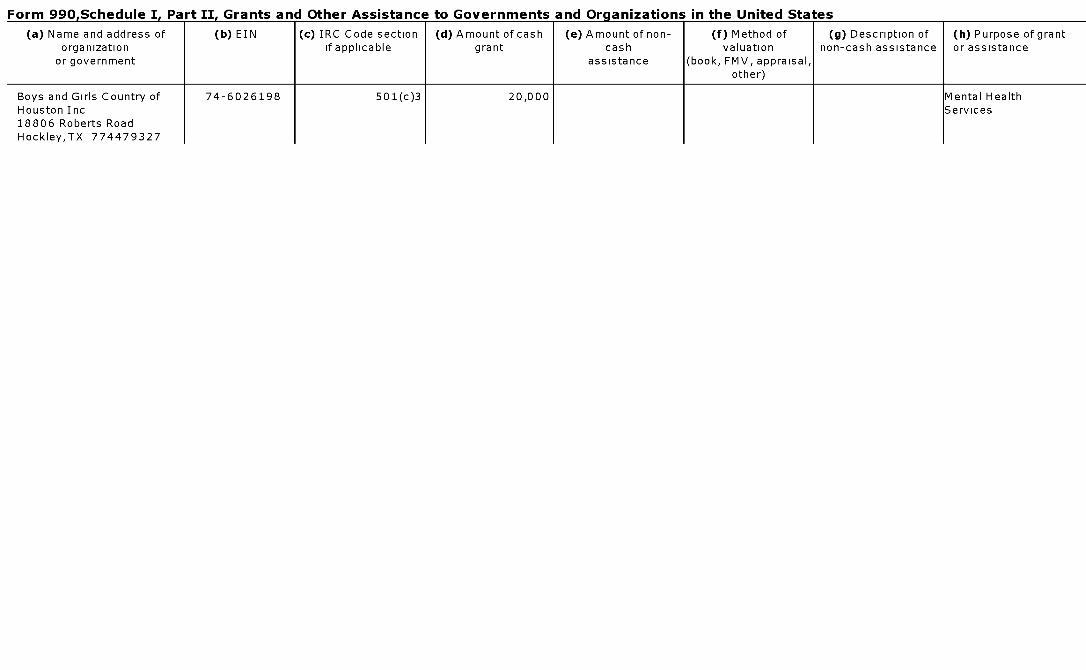
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c ) IRC Code section ( d) Amount of cash ( e) Amount of non- (f) Method of ( g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non - cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Boys and Girls Country of 74-6026198 501(c) 3 20,000 Mental HealthHouston Inc Services18806 Roberts RoadHockley,TX 774479327
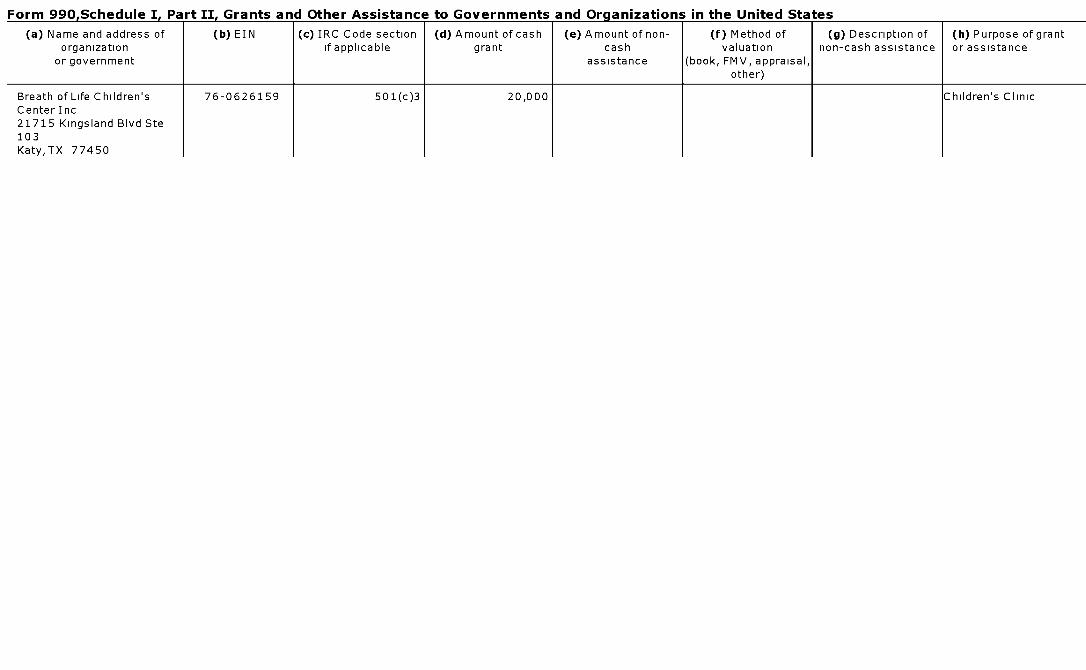
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c ) IRC Code section (d) Amount of cash (e) Amount of non- (f ) Method of ( g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Breath of Life Children ' s 76-0626159 501(c ) 3 20,000 Children 's ClinicCenter Inc21715 Kingsland Blvd Ste103Katy,TX 77450
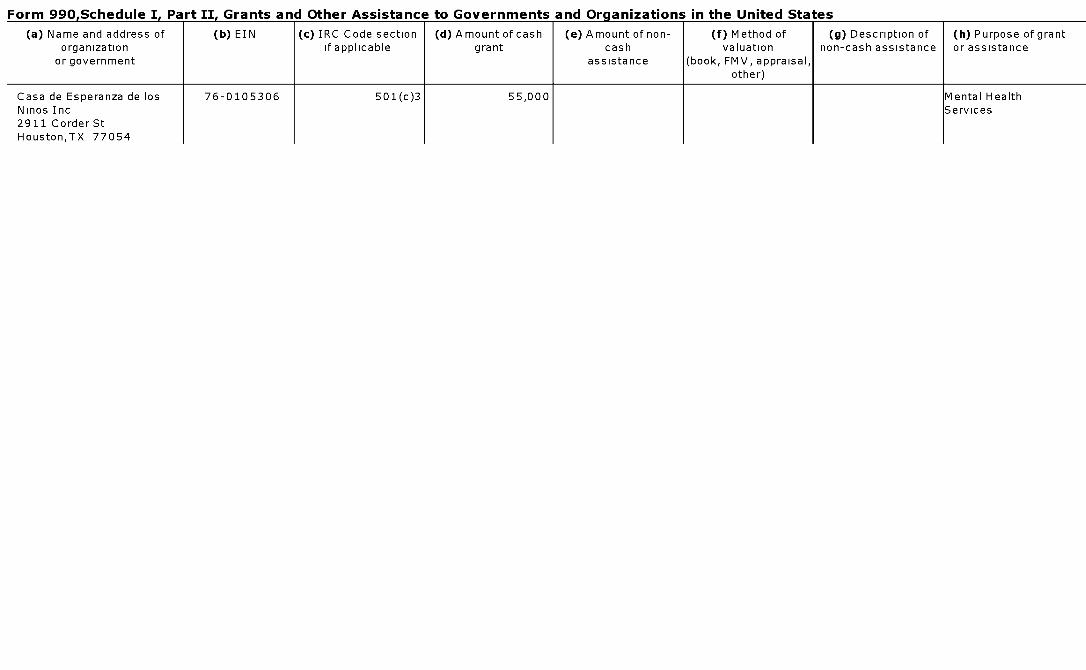
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Casa de Esperanza de los 76-0105306 501(c)3 55,000 Mental HealthNinos Inc Services2911 Corder StHouston,TX 77054
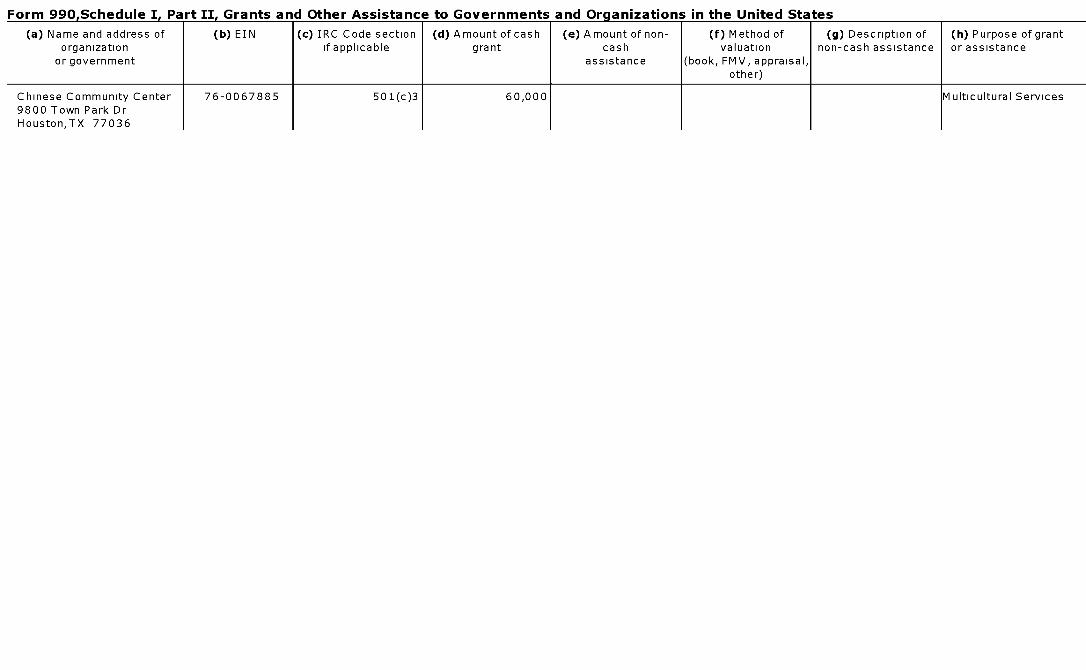
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Chinese Community Center 76-0067885 501(c)3 60,000 Multicultural Services9800 Town Park DrHouston,TX 77036
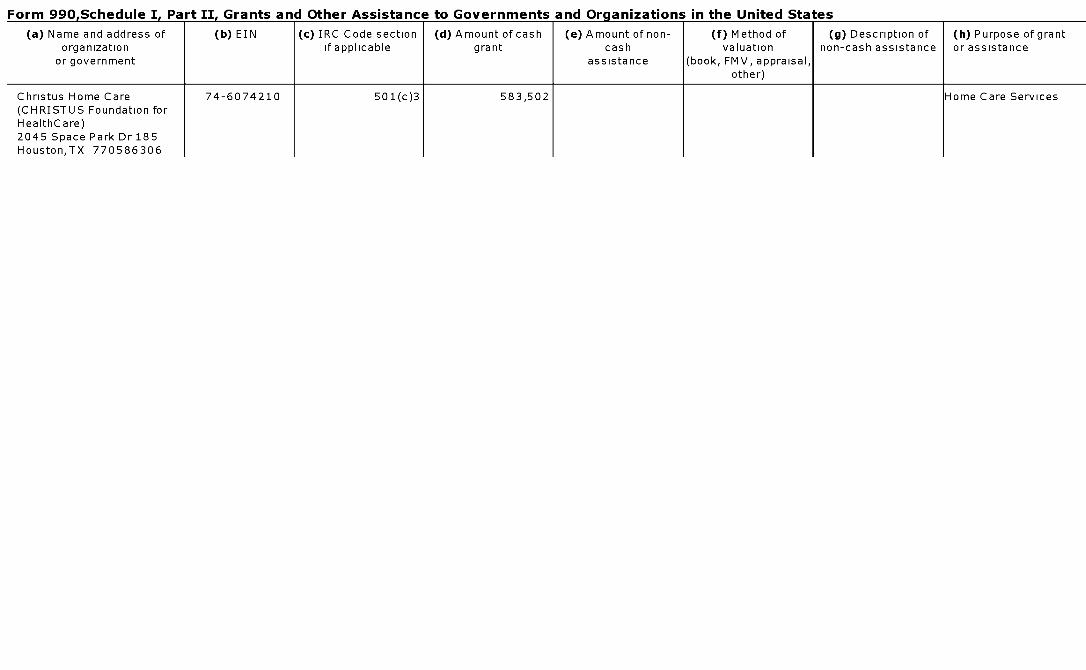
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Christus Home Care 74-6074210 501(c)3 583,502 Home Care Services(CHRISTUS Foundation forHealthCare)2045 Space Park Dr 185Houston,TX 770586306
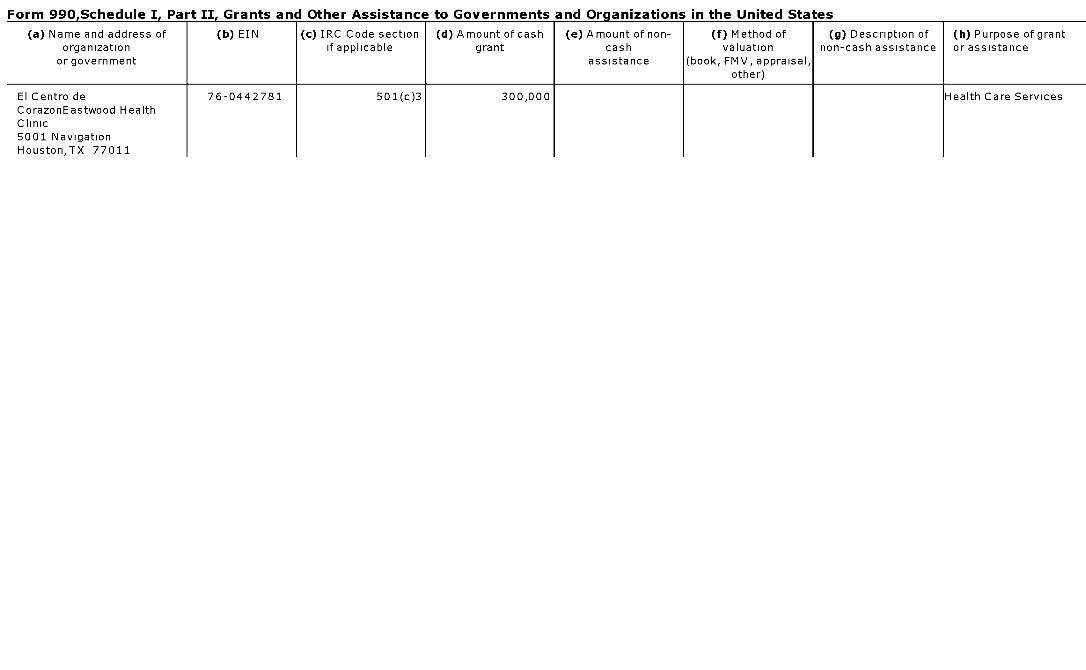
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
El Centro de 76-0442781 501(c)3 300,000 Health Care ServicesCorazonEastwood HealthClinic5001 NavigationHouston,TX 77011
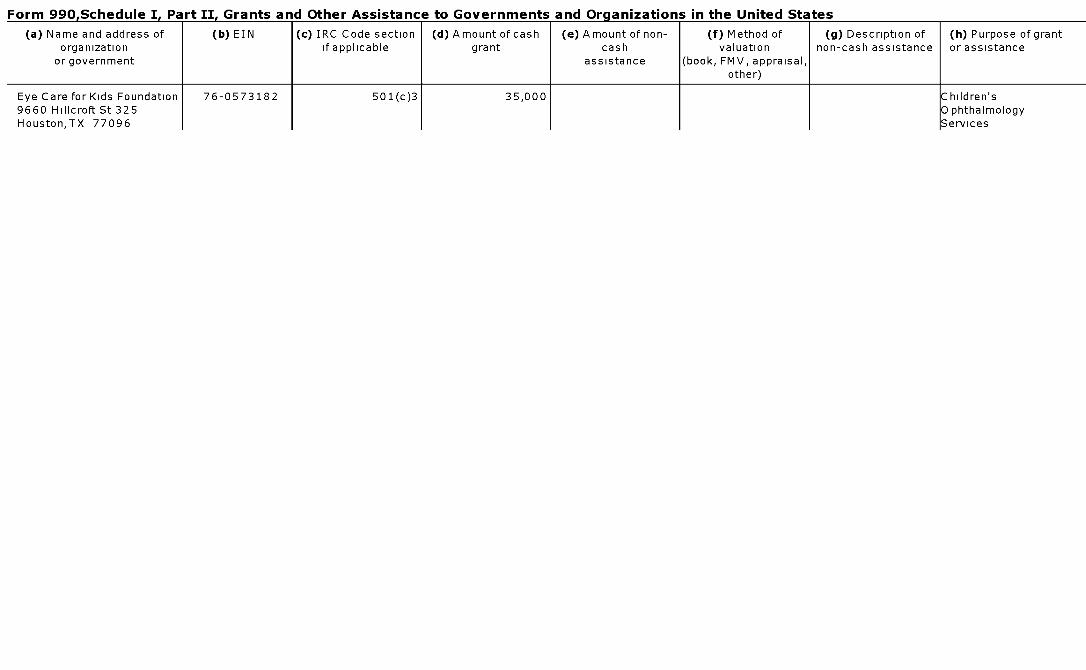
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Eye Care for Kids Foundation 76-0573182 501(c)3 35,000 Children's9660 Hillcroft St 325 OphthalmologyHouston,TX 77096 Services
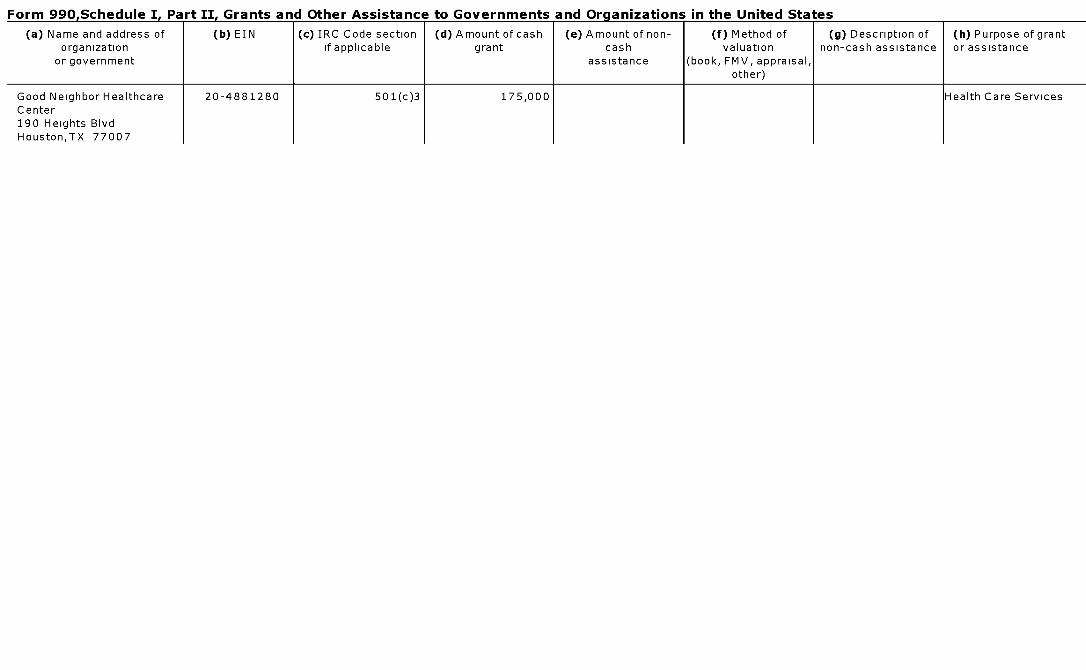
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Good Neighbor Healthcare 20-4881280 501(c)3 175,000 Health Care ServicesCenter190 Heights BlvdHouston,TX 77007
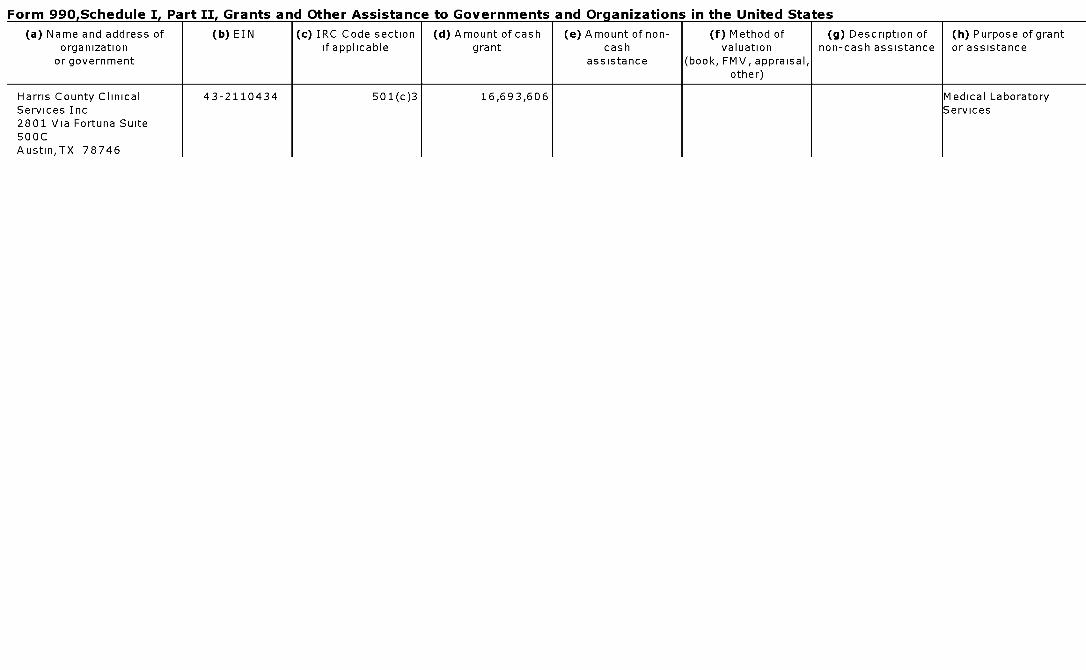
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Harris County Clinical 43-2110434 501(c)3 16,693,606 Medical LaboratoryServices Inc Services2801 Via Fortuna Suite500CAustin,TX 78746
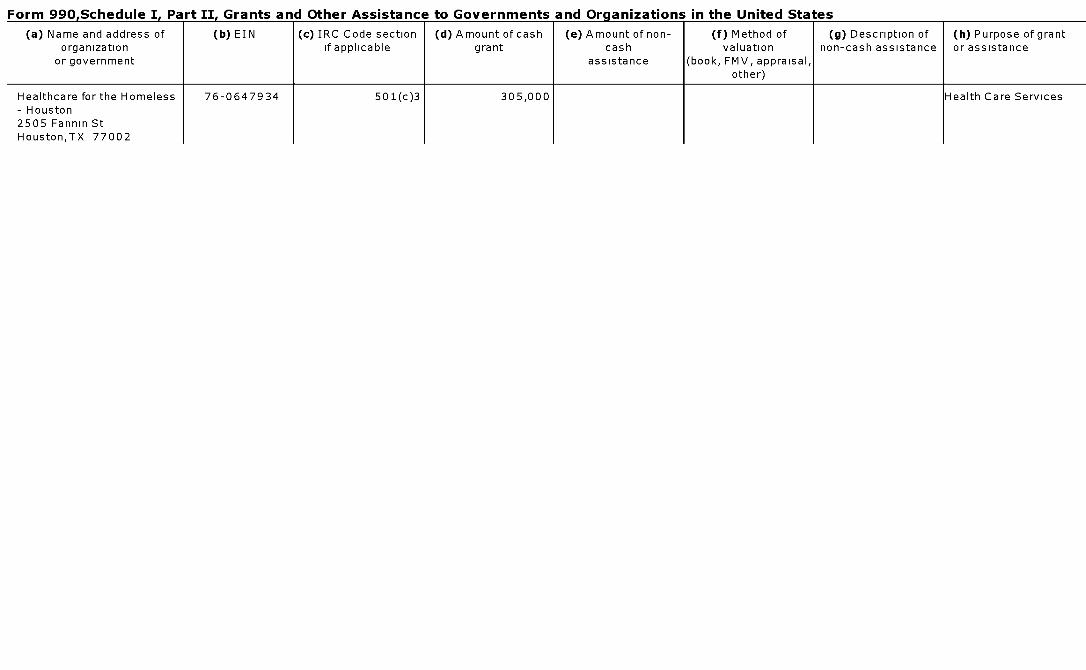
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Healthcare for the Homeless 76-0647934 501(c)3 305,000 Health Care Services- Houston2505 Fannin StHouston,TX 77002
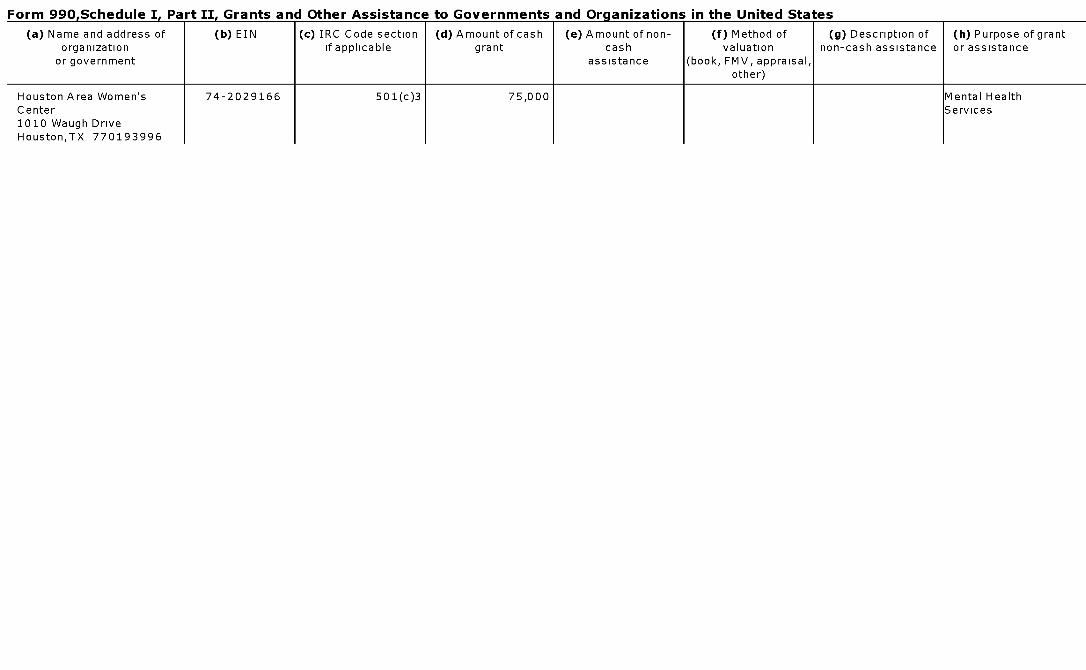
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Houston Area Women's 74-2029166 501(c)3 75,000 Mental HealthCenter Services1010 Waugh DriveHouston,TX 770193996
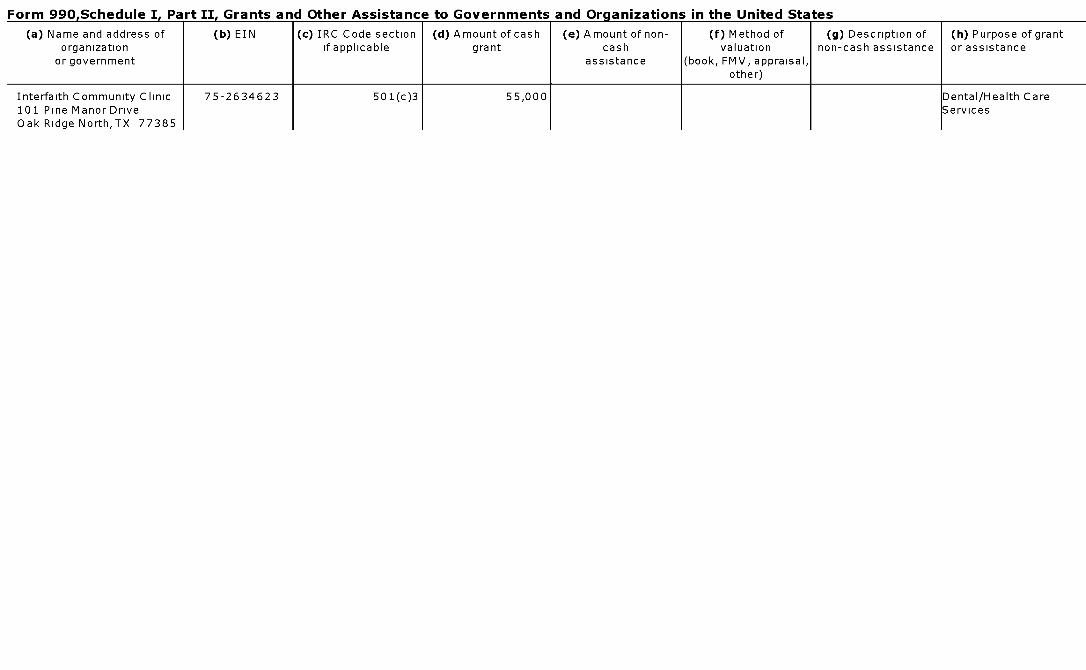
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Interfaith Community Clinic 75-2634623 501(c)3 55,000 Dental/Health Care101 Pine Manor Drive ServicesOak Ridge North,TX 77385
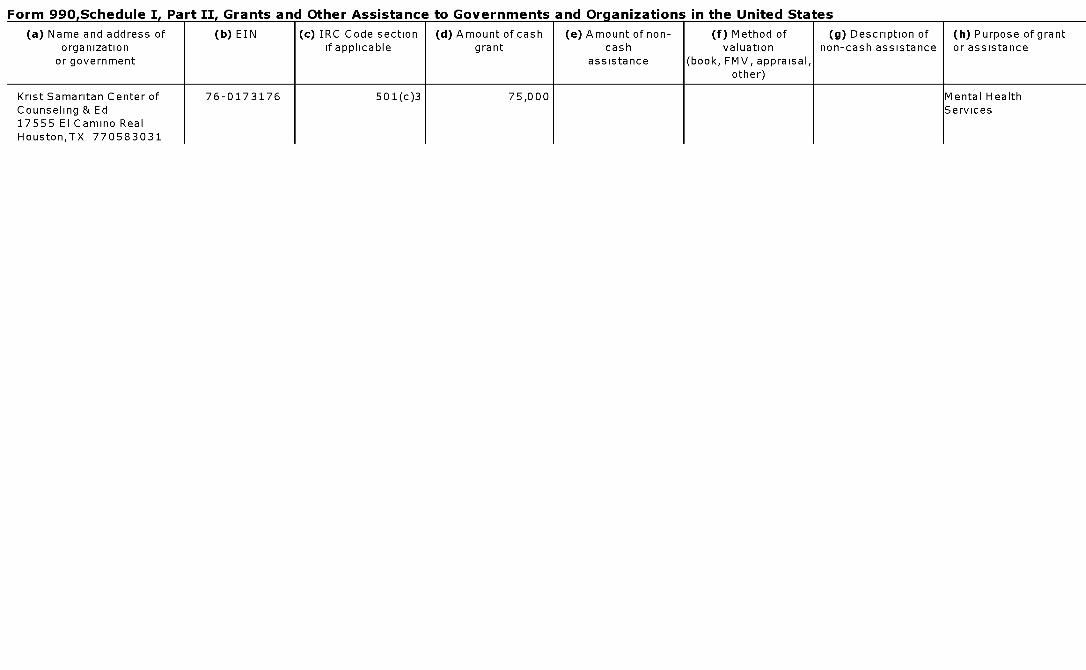
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of ( b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Krist Samaritan Center of 76-0173176 501(c)3 75,000 Mental HealthCounseling & Ed Services17555 El Camino RealHouston,TX 770583031
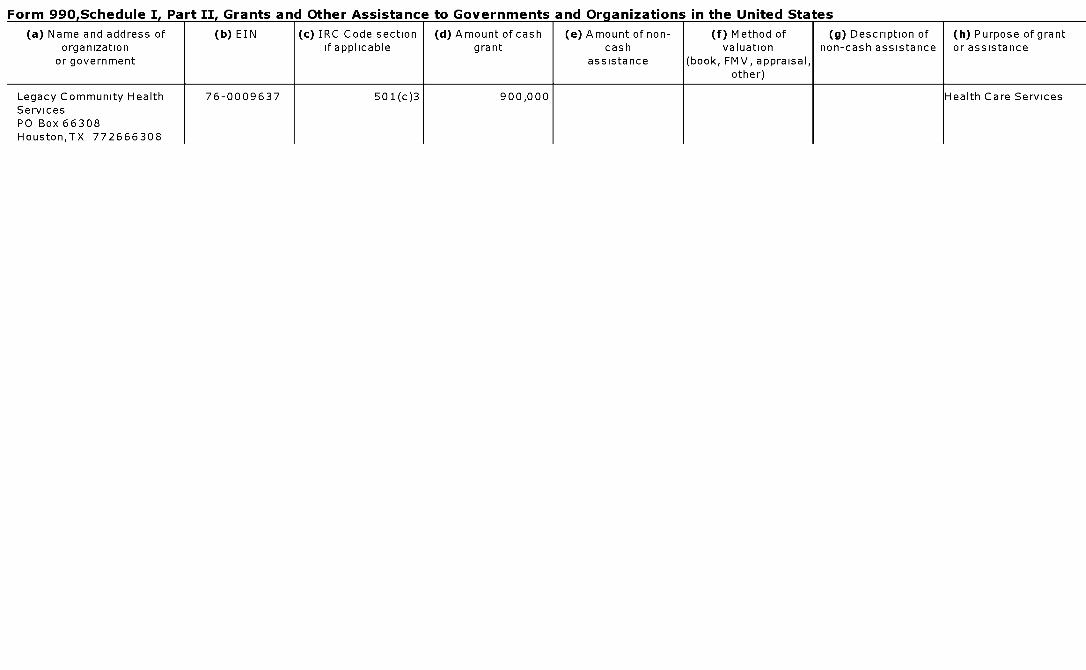
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Legacy Community Health 76-0009637 501(c)3 900,000 Health Care ServicesServicesPO Box 66308Houston,TX 772666308
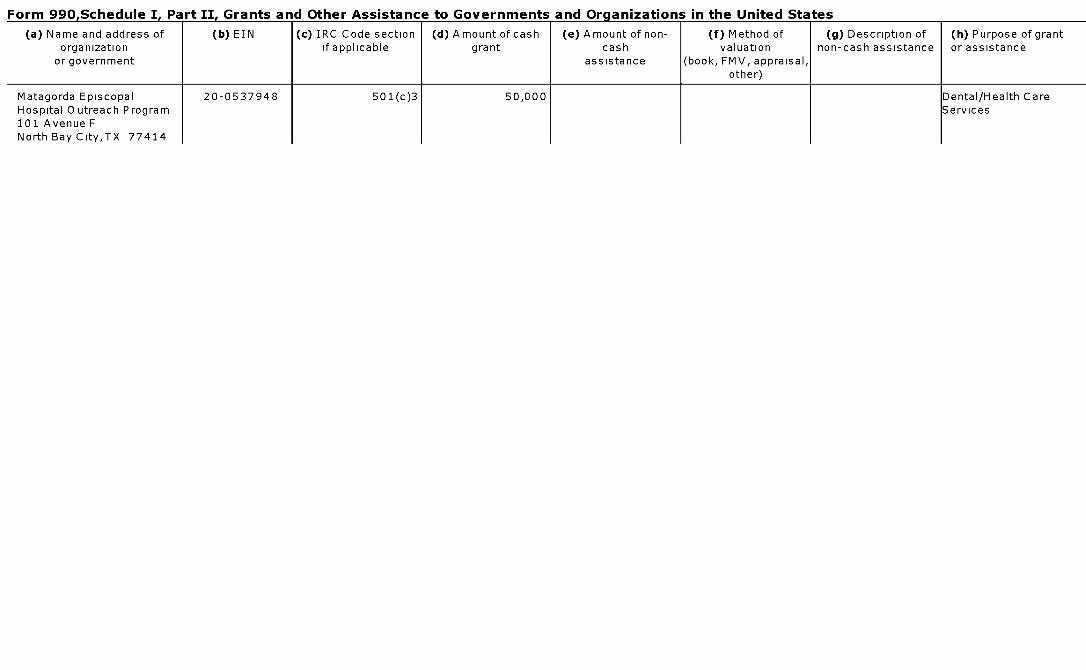
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of ( b) EIN (c ) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Matagorda Episcopal 20 -0537948 501 (c)3 50,000 Dental/Health CareHospital Outreach Program Services101 Avenue FNorth Bay City,TX 77414
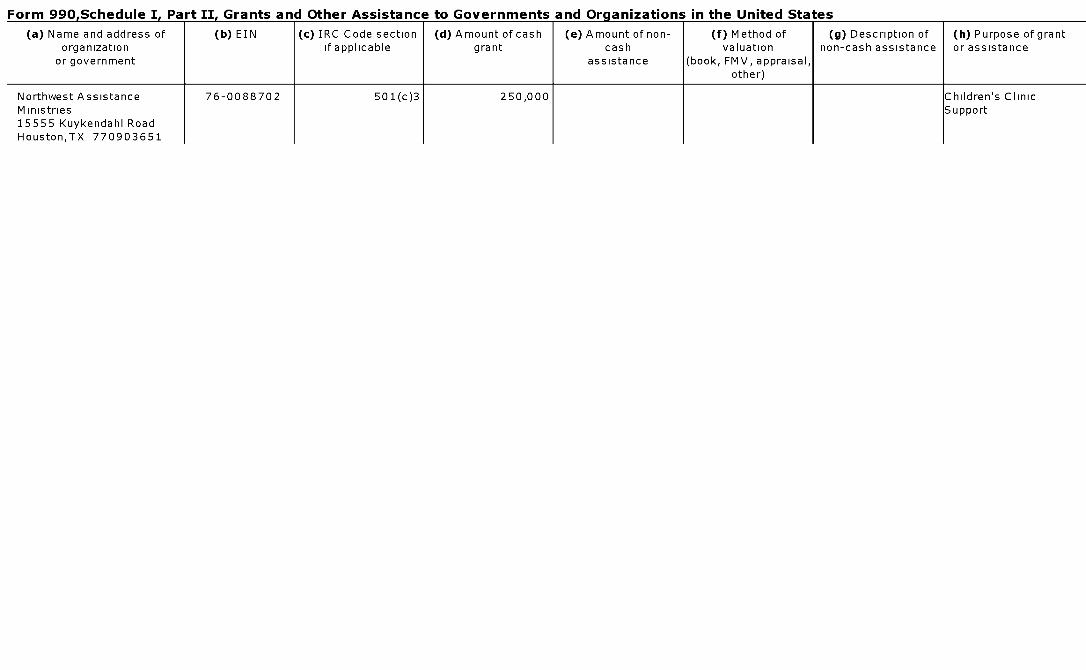
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Northwest Assistance 76-0088702 501(c)3 250,000 Children's ClinicMinistries Support15555 Kuykendahl RoadHouston,TX 770903651
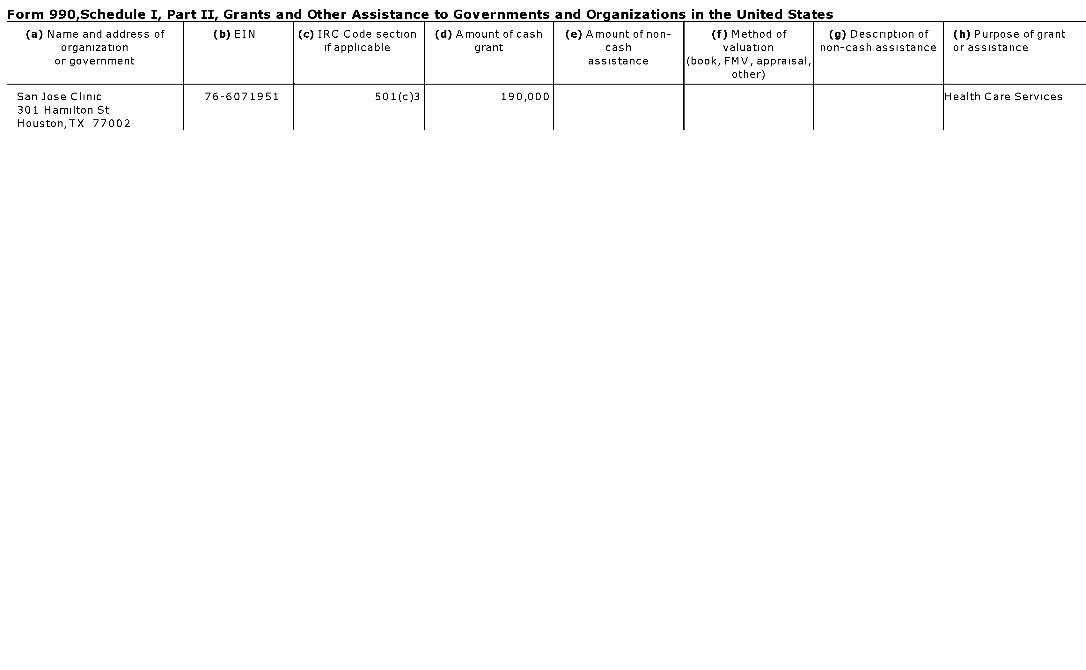
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
San Jose Clinic 76-6071951 501(c)3 190,000 Health Care Services301 Hamilton StHouston,TX 77002
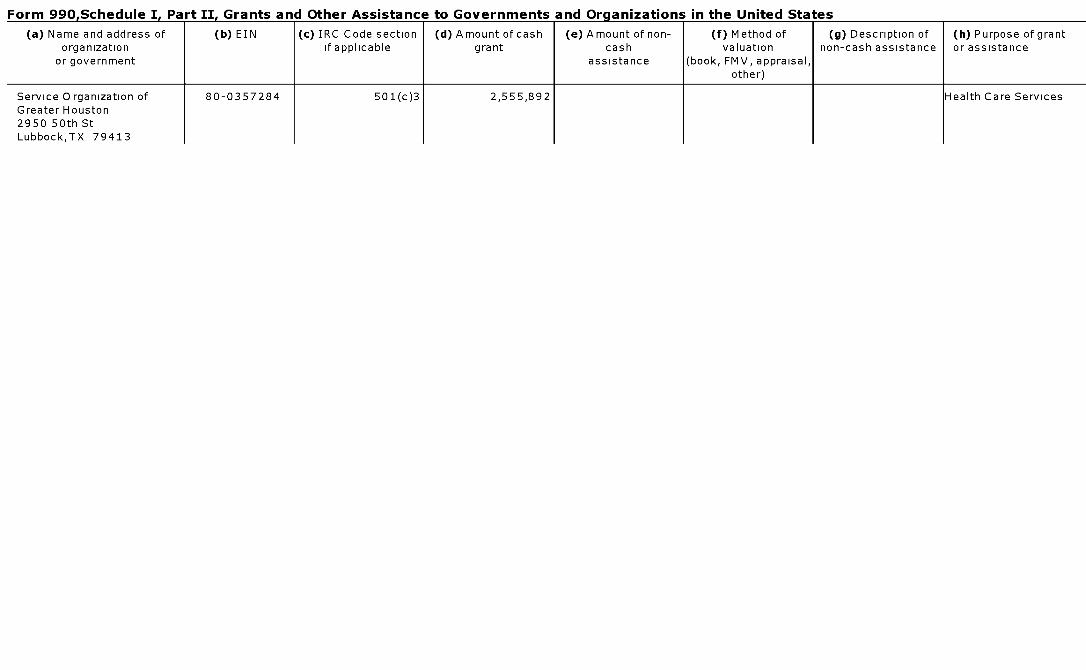
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Service Organization of 80-0357284 501(c)3 2,555,892 Health Care ServicesGreater Houston2950 50th StLubbock,TX 79413
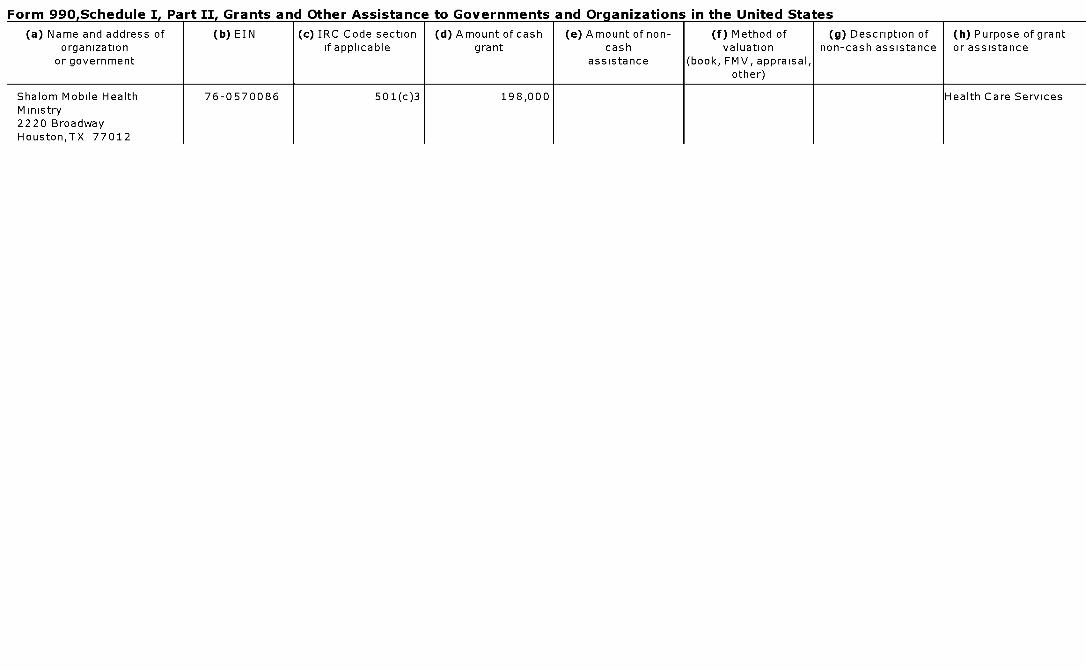
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Shalom Mobile Health 76-0570086 501(c)3 198,000 Health Care ServicesMinistry2220 BroadwayHouston,TX 77012
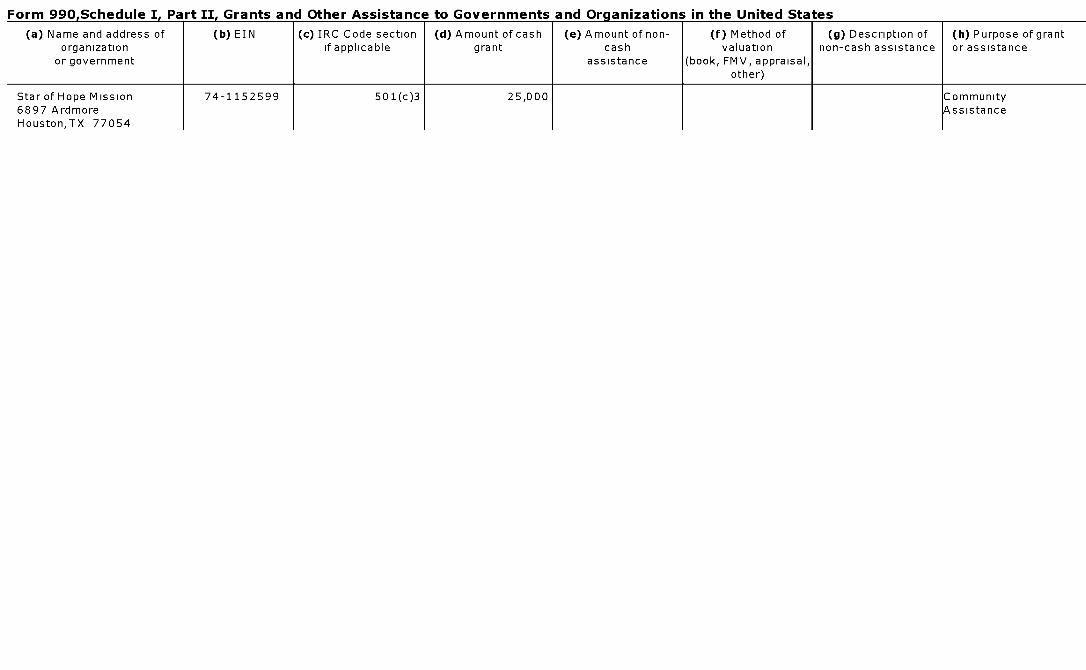
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Star of Hope Mission 74-1152599 501(c)3 25,000 Community6897 Ardmore AssistanceHouston,TX 77054
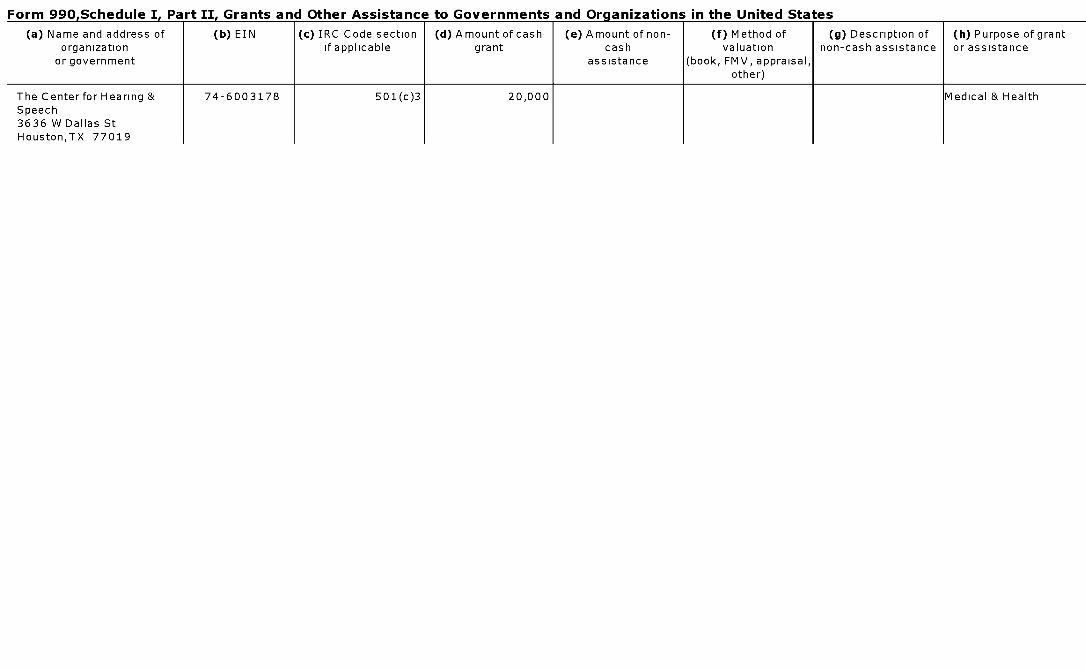
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
The Center for Hearing & 74-6003178 501(c)3 20,000 Medical & HealthSpeech3636 W Dallas StHouston,TX 77019
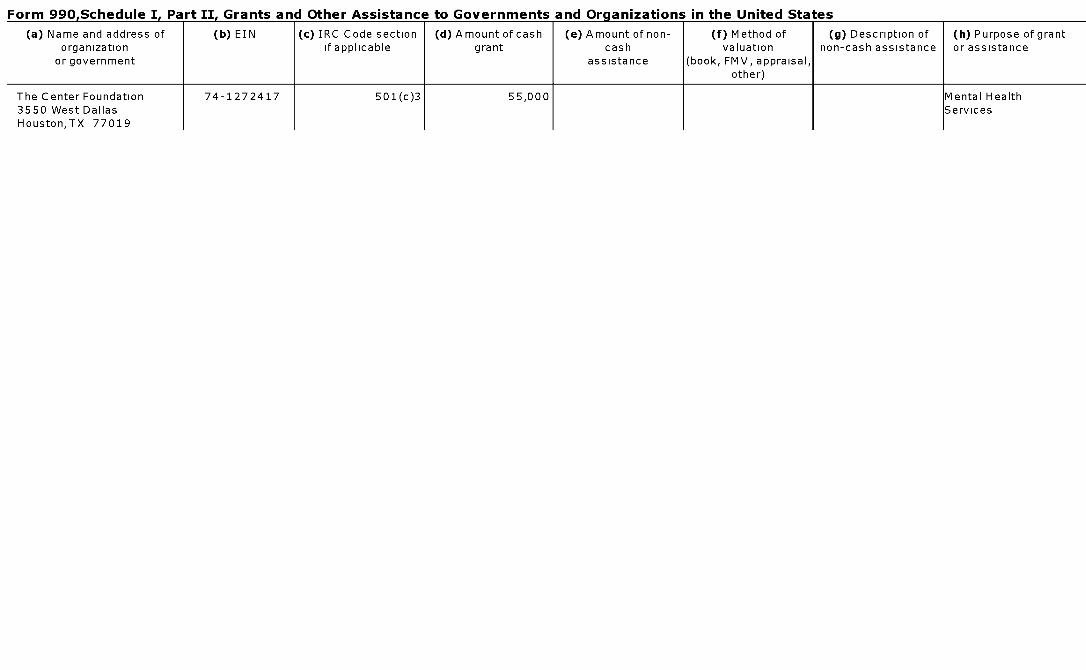
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of ( b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
The Center Foundation 74-1272417 501(c)3 55,000 Mental Health3550 West Dallas ServicesHouston,TX 77019
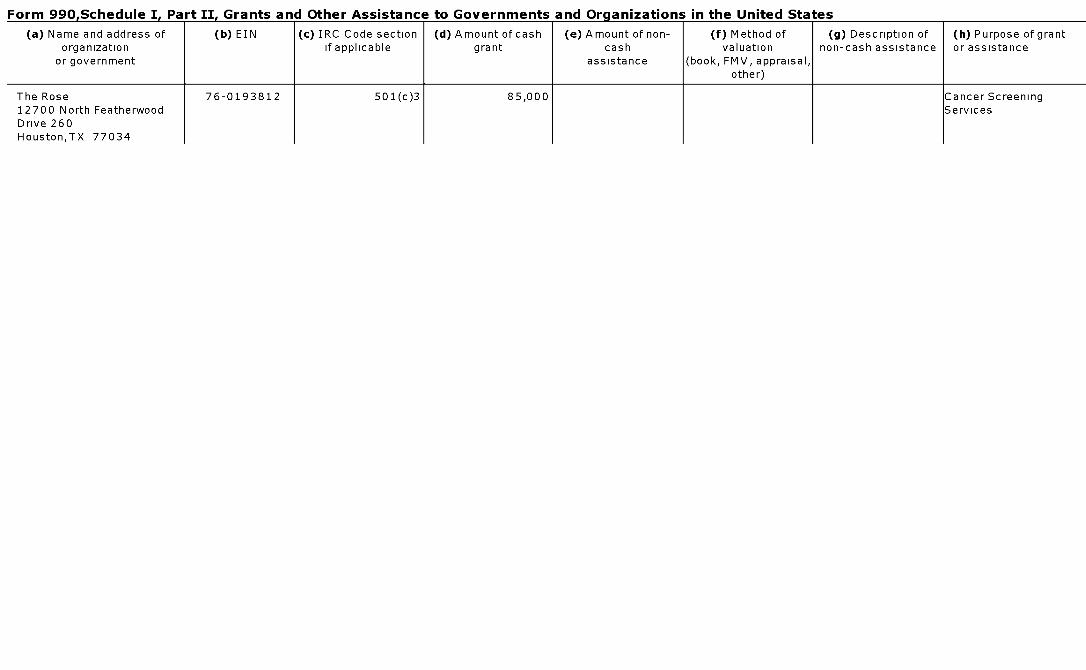
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c ) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
The Rose 76-0193812 501( c)3 85,000 Cancer Screening12700 North Featherwood ServicesDrive 260Houston,TX 77034
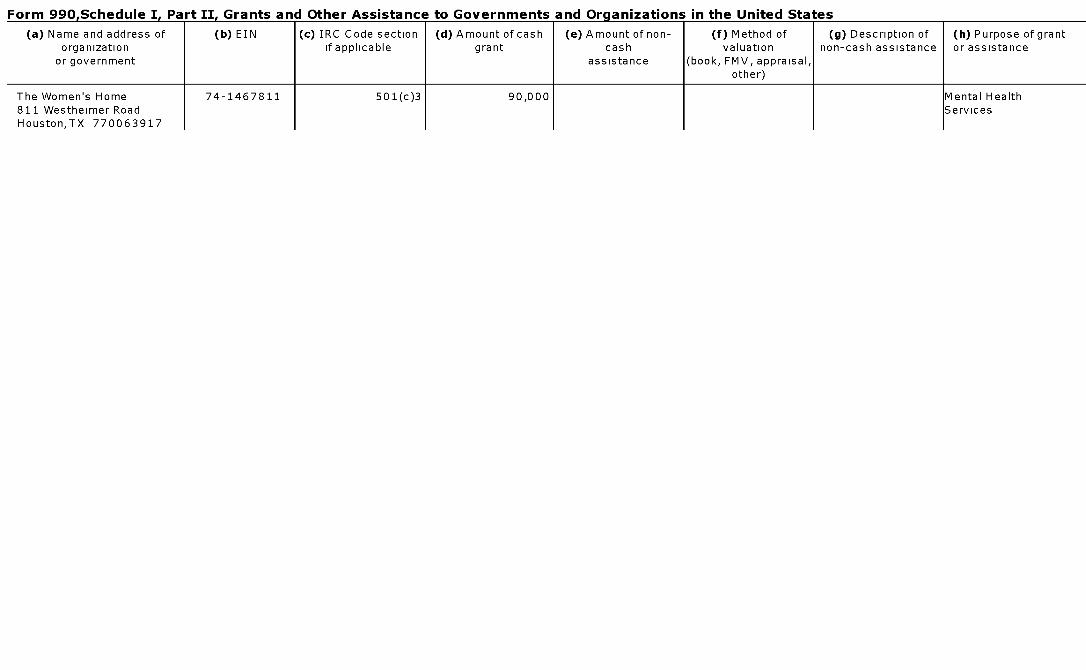
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
The Women's Home 74-1467811 501(c)3 90,000 Mental Health811 Westheimer Road ServicesHouston,TX 770063917
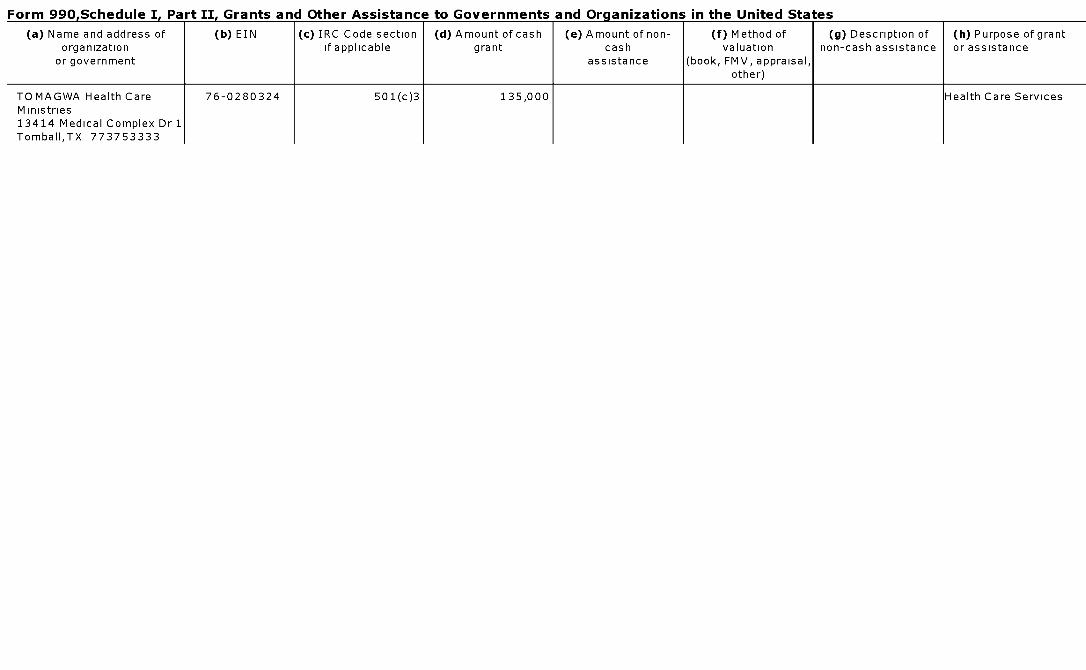
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
TOMAGWA Health Care 76-0280324 501(c)3 135,000 Health Care ServicesMinistries13414 Medical Complex Dr 1Tomball,TX 773753333
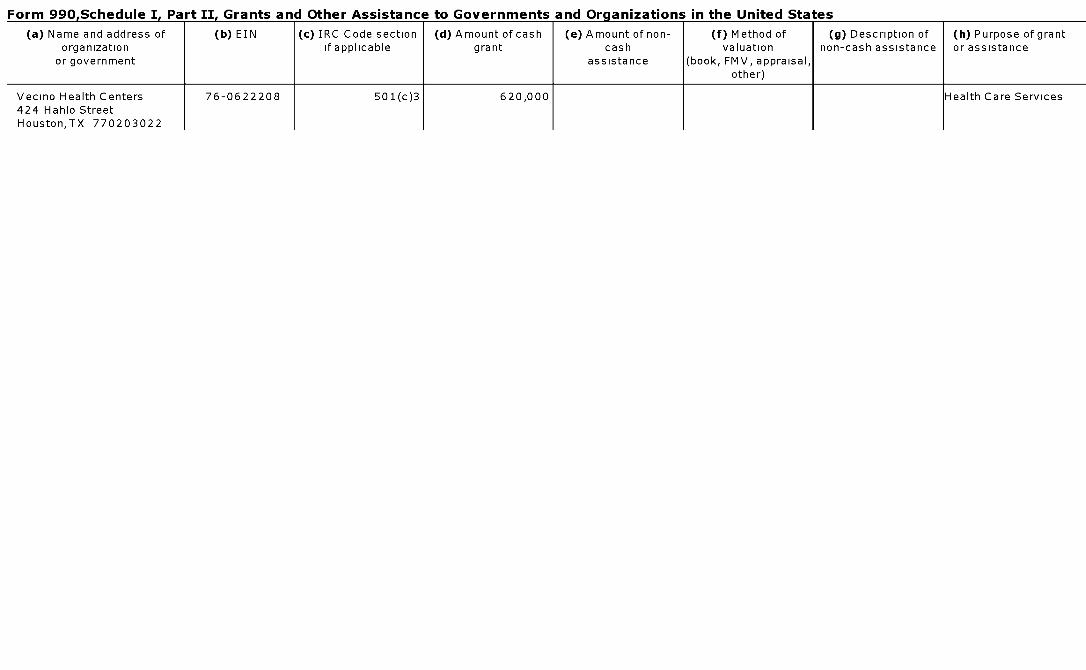
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Vecino Health Centers 76 - 0622208 501(c)3 620,000 Health Care Services424 Hahlo StreetHouston,TX 770203022
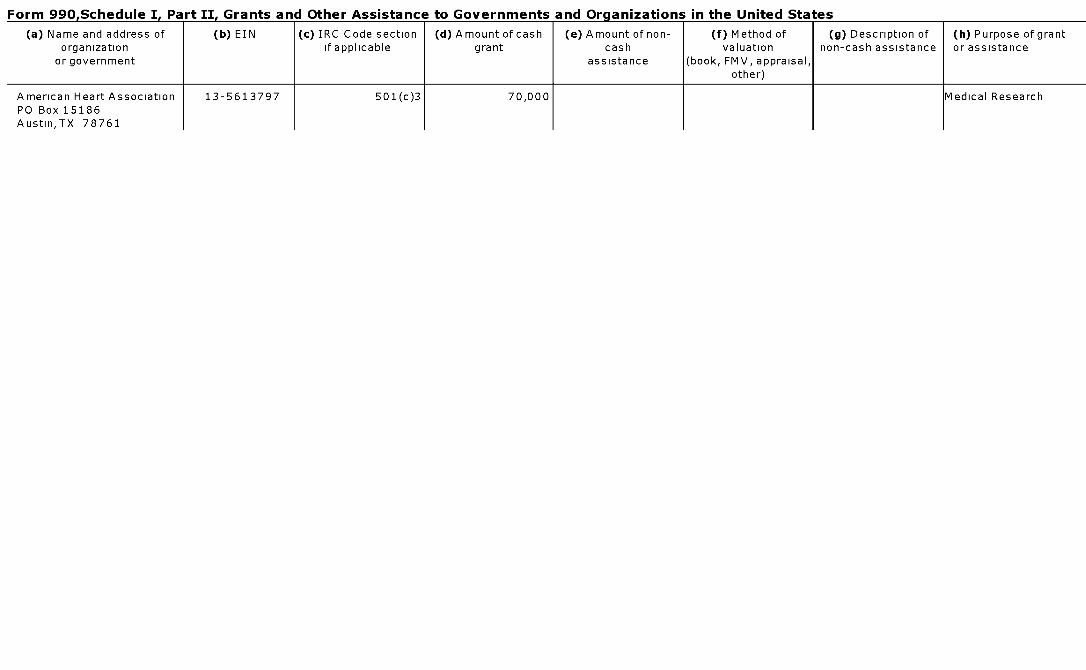
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
American Heart Association 13-5613797 501(c)3 70,000 Medical ResearchPO Box 15186Austin,TX 78761
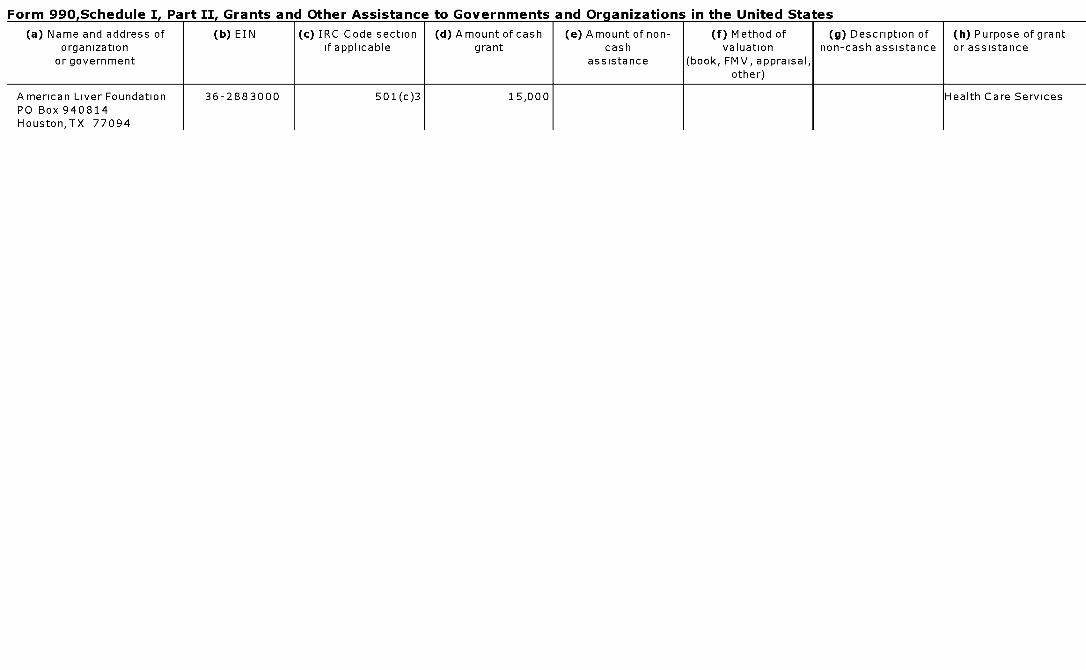
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
American Liver Foundation 36-2883000 501(c)3 15,000 Health Care ServicesPO Box 940814Houston,TX 77094
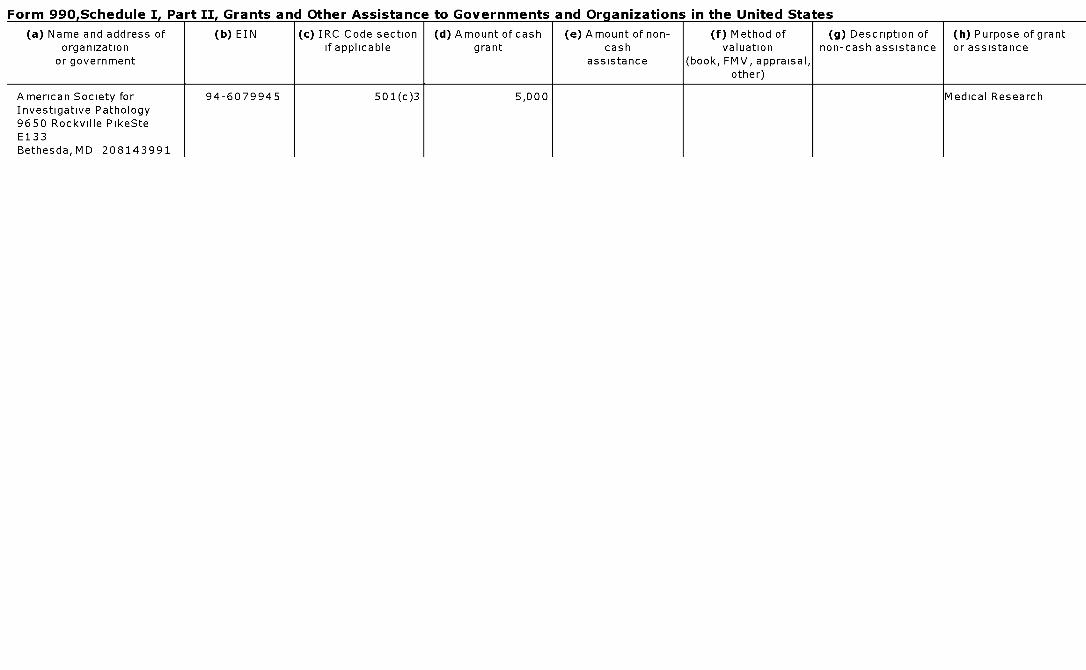
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
American Society for 94-6079945 501(c)3 5,000 Medical ResearchInvestigative Pathology9650 Rockville PikeSteE133Bethesda,MD 208143991
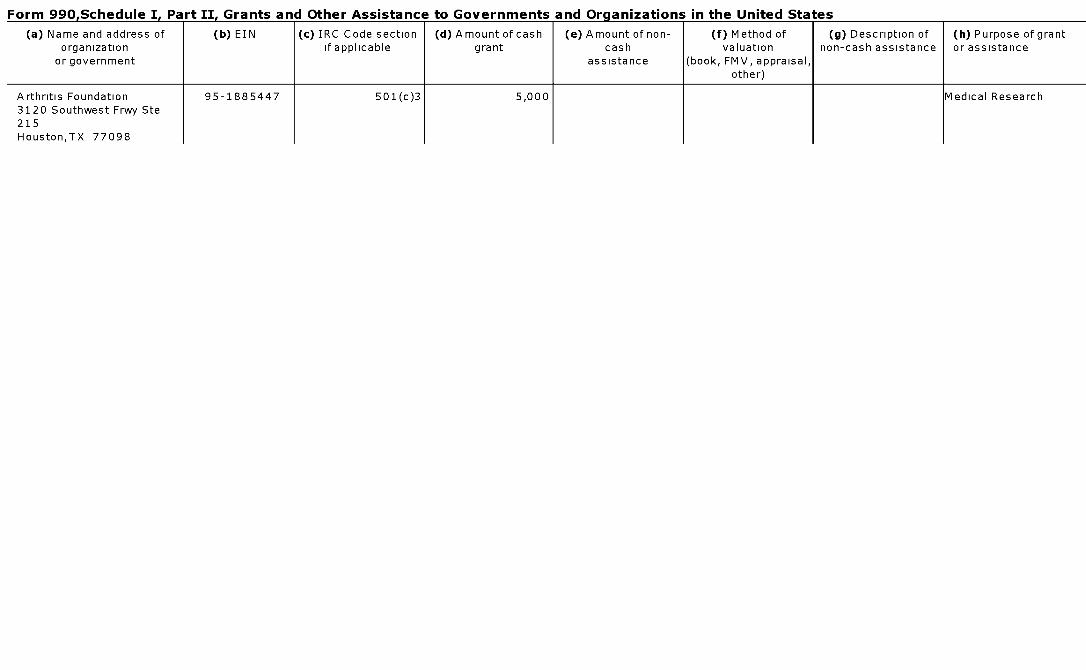
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Arthritis Foundation 95-1885447 501(c)3 5,000 Medical Research3120 Southwest Frwy Ste215Houston,TX 77098
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Association of Fundraising 13-2590764 501(c)3 10,000 AssistanceProfessional-GreaterHouston ChapterPO Box 59Bellaire,TX 77405
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c ) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Avon Walk for Breast Cancer 13-6128447 501(c )3 5,000 Medical Research777 Third AveNewYork,NY 10017
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Bilateral US-ARAB Chamber 32-0099085 501(c)6 15,000 Community Service2323 S Shepherd Dr Ste1150Houston,TX 77019
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of ( b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Boy Scouts of America 74-1109732 501(c)3 10,000 Community ServicePO Box 924528Houston,TX 772924528
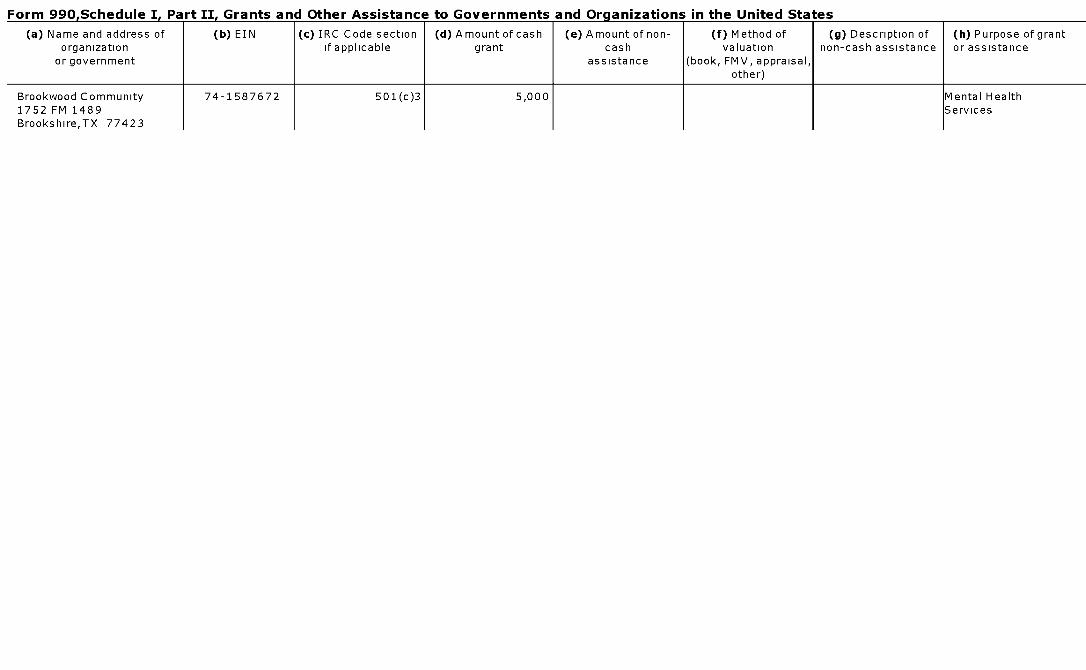
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Brookwood Community 74-1587672 501(c)3 5,000 Mental Health1752 FM 1489 ServicesBrookshire,TX 77423
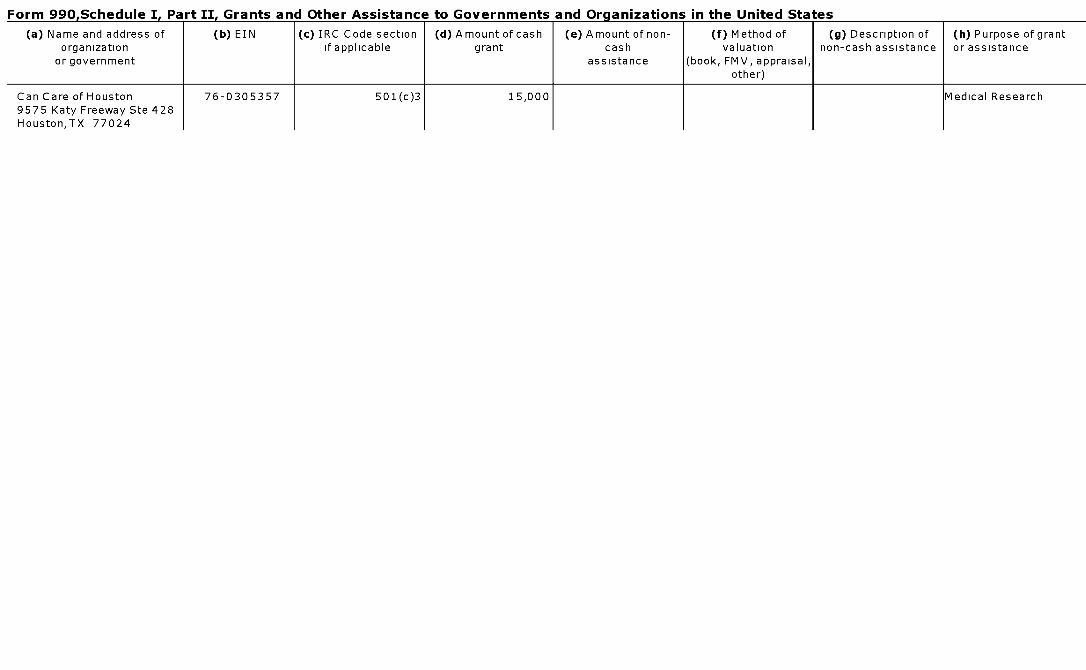
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Can Care of Houston 76-0305357 501(c)3 15,000 Medical Research9575 Katy Freeway Ste 428Houston,TX 77024
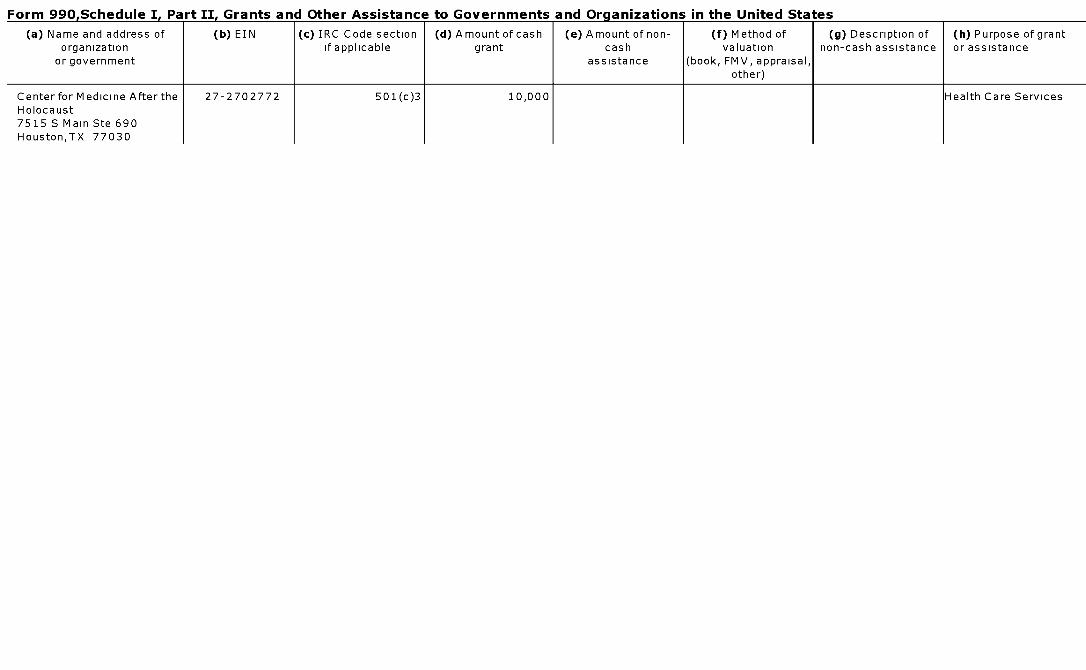
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Center for Medicine After the 27-2702772 501(c)3 10,000 Health Care ServicesHolocaust7515 S Main Ste 690Houston,TX 77030
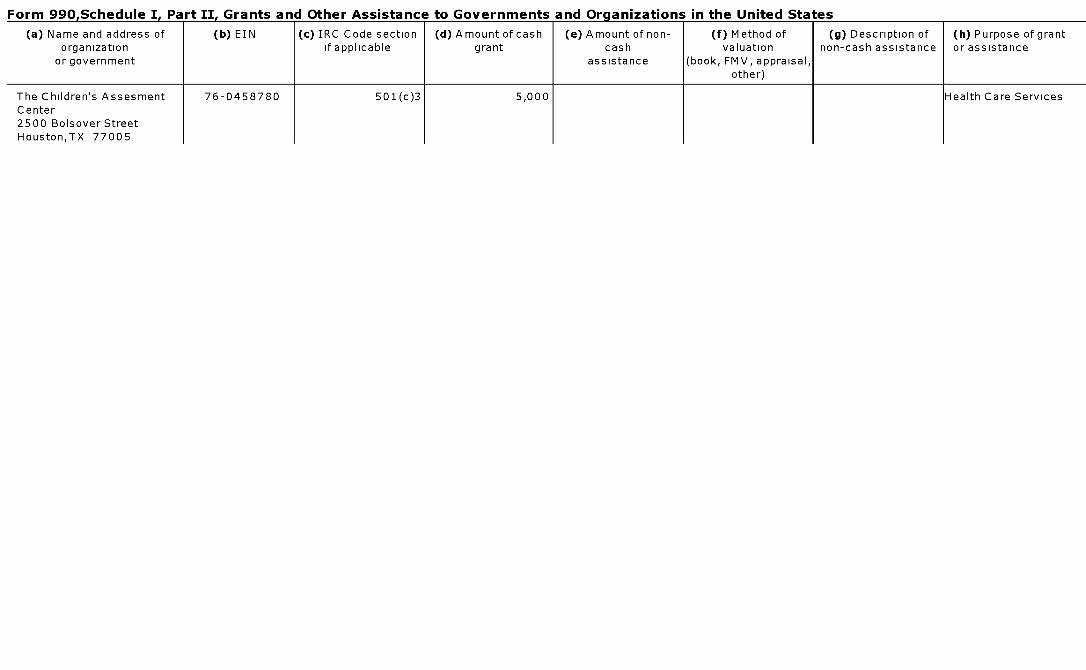
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
The Children's Assesment 76-0458780 501(c)3 5,000 Health Care ServicesCenter2500 Bolsover StreetHouston,TX 77005
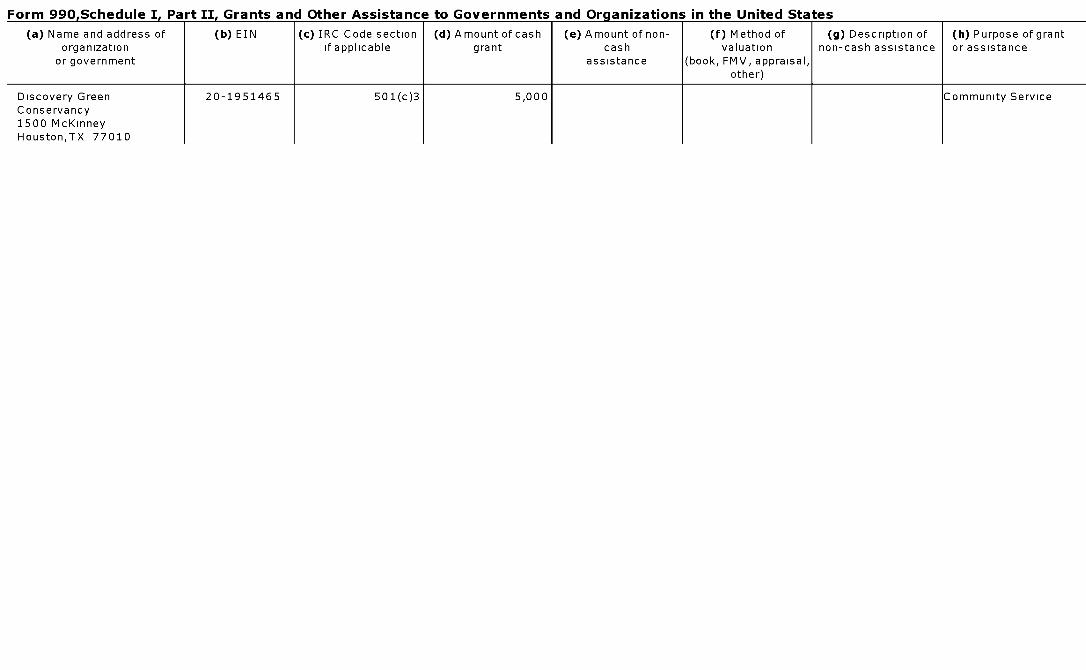
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Discovery Green 20-1951465 501(c)3 5,000 Community ServiceConservancy1500 McKinneyHouston,TX 77010
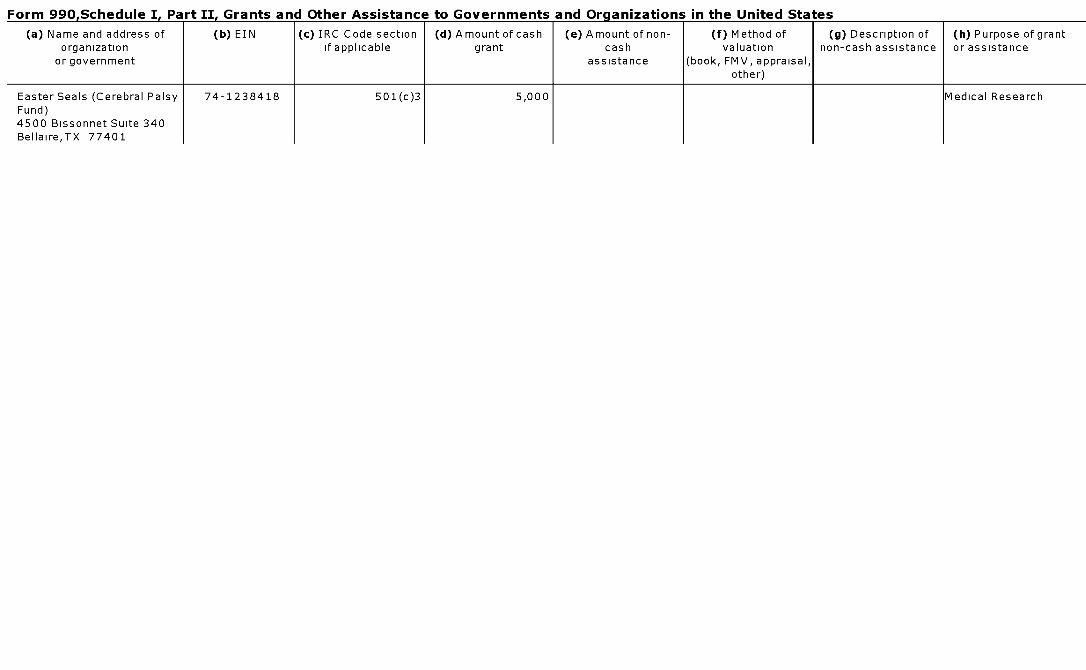
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Easter Seals (Cerebral Palsy 74-1238418 501(c)3 5,000 Medical ResearchFund)4500 Bissonnet Suite 340Bellaire,TX 77401
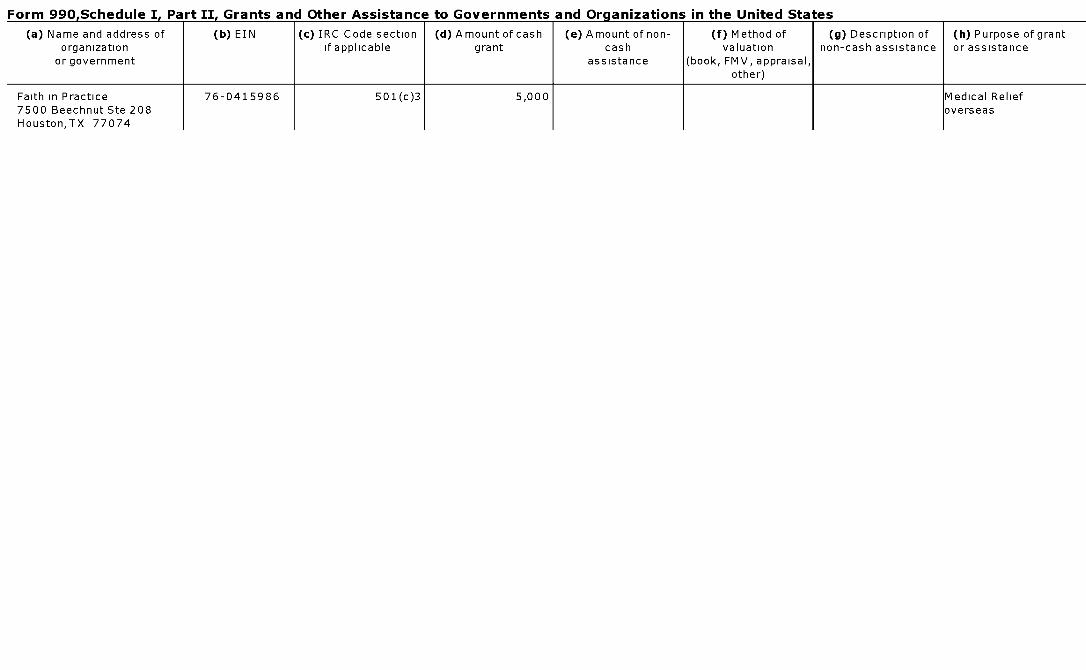
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of ( b) EIN (c ) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Faith in Practice 76-0415986 501(c )3 5,000 Medical Relief7500 Beechnut Ste 208 overseasHouston,TX 77074
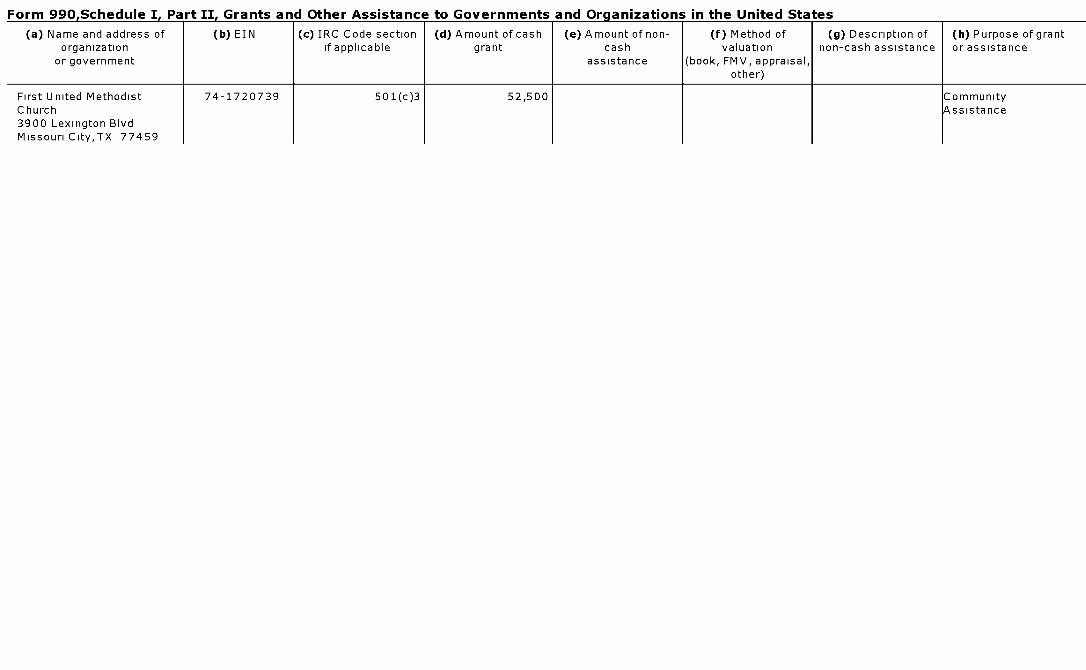
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c ) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
First United Methodist 74-1720739 501(c)3 52,500 CommunityChurch A ssistance3900 Lexington BlvdMissouri City ,TX 77459
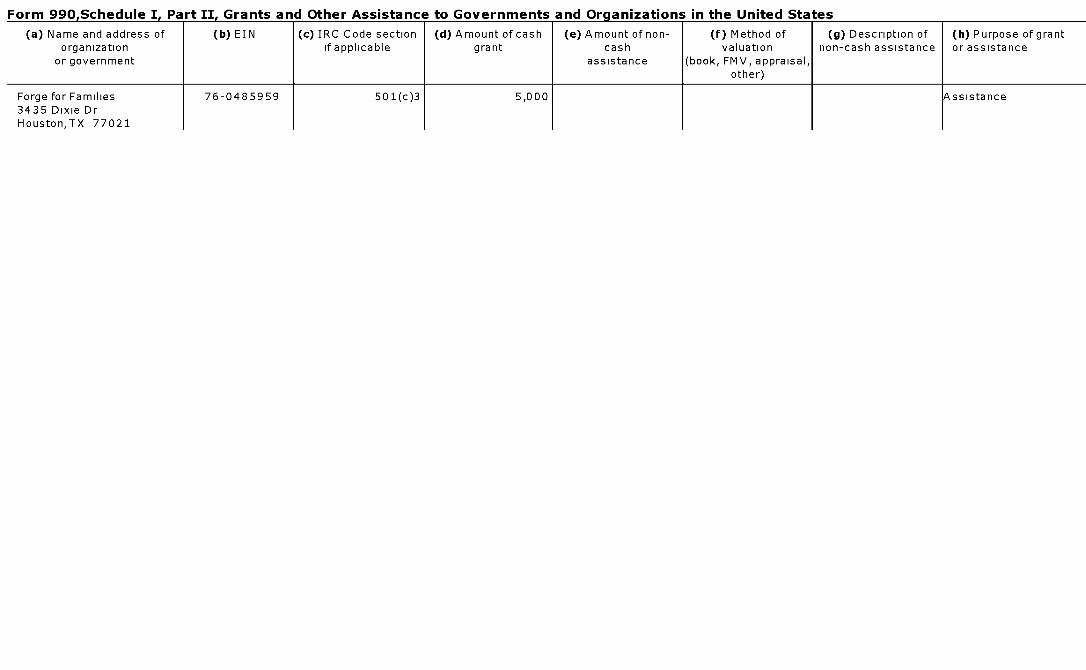
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Forge for Families 76-0485959 501(c)3 5,000 Assistance3435 Dixie DrHouston,TX 77021
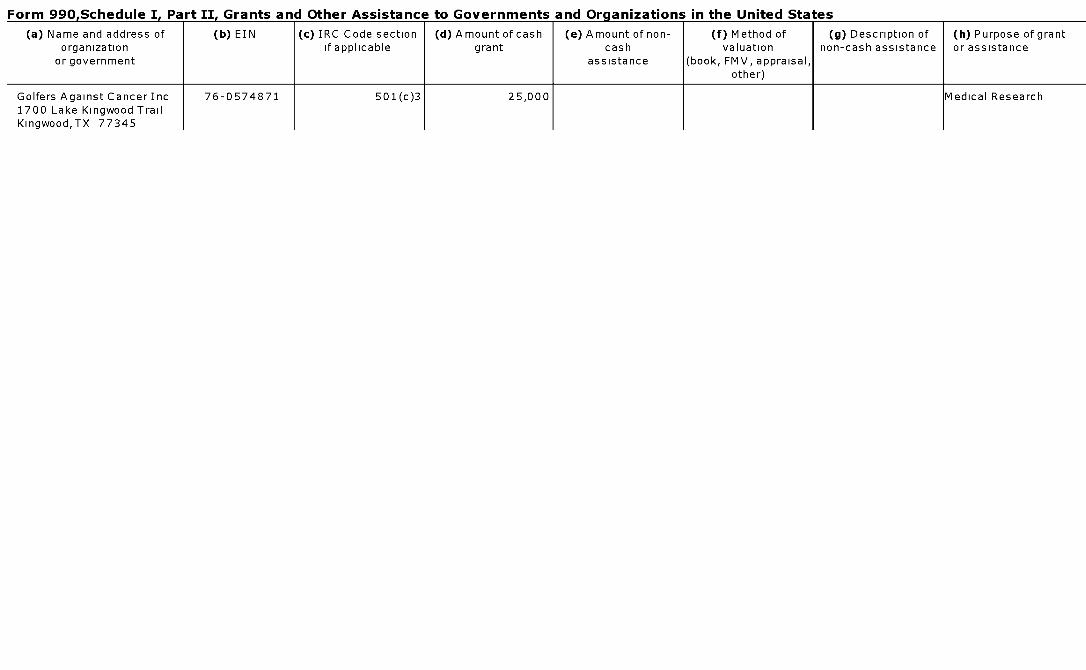
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Golfers Against Cancer Inc 76-0574871 501(c)3 25,000 Medical Research1700 Lake Kingwood TrailKingwood,TX 77345
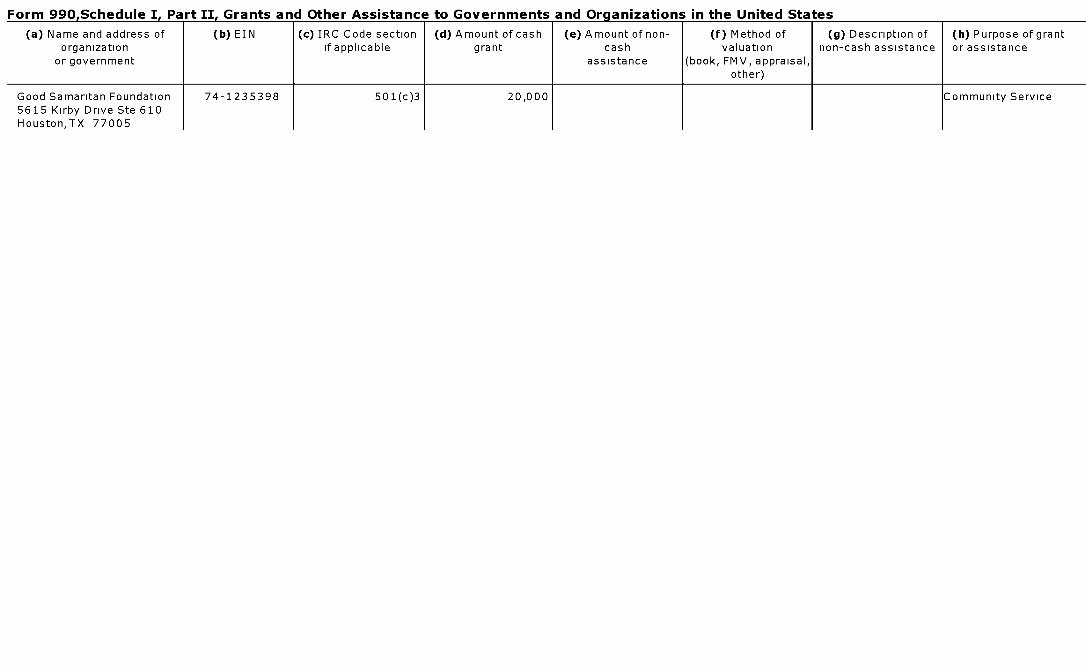
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Good Samaritan Foundation 74-1235398 501(c)3 20,000 Community Service5615 Kirby Drive Ste 610Houston,TX 77005
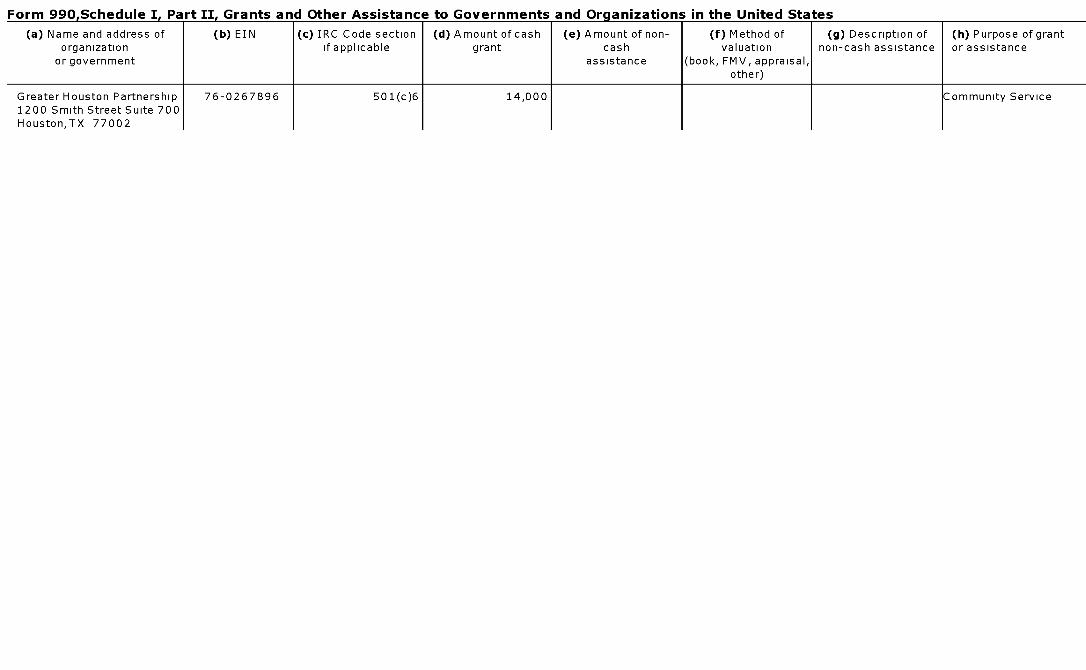
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Greater Houston Partnership 76-0267896 501(c)6 14,000 Community Service1200 Smith Street Suite 700Houston,TX 77002
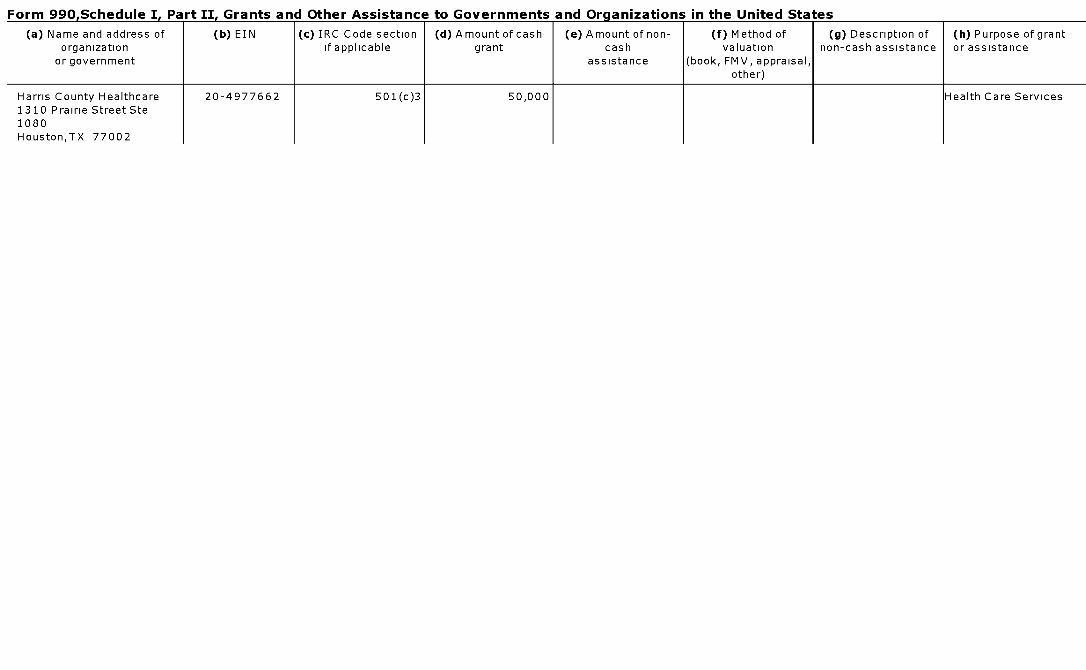
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Harris County Healthcare 20-4977662 501(c)3 50,000 Health Care Services1310 Prairie Street Ste1080Houston,TX 77002
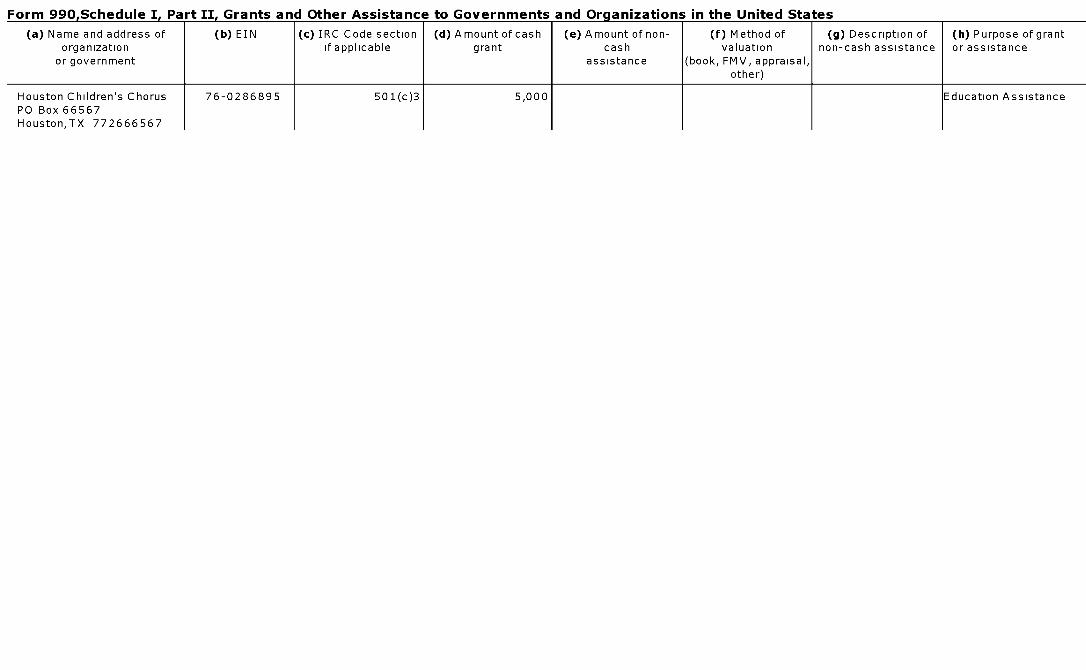
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Houston Children's Chorus 76-0286895 501(c)3 5,000 Education AssistancePO Box 66567Houston,TX 772666567
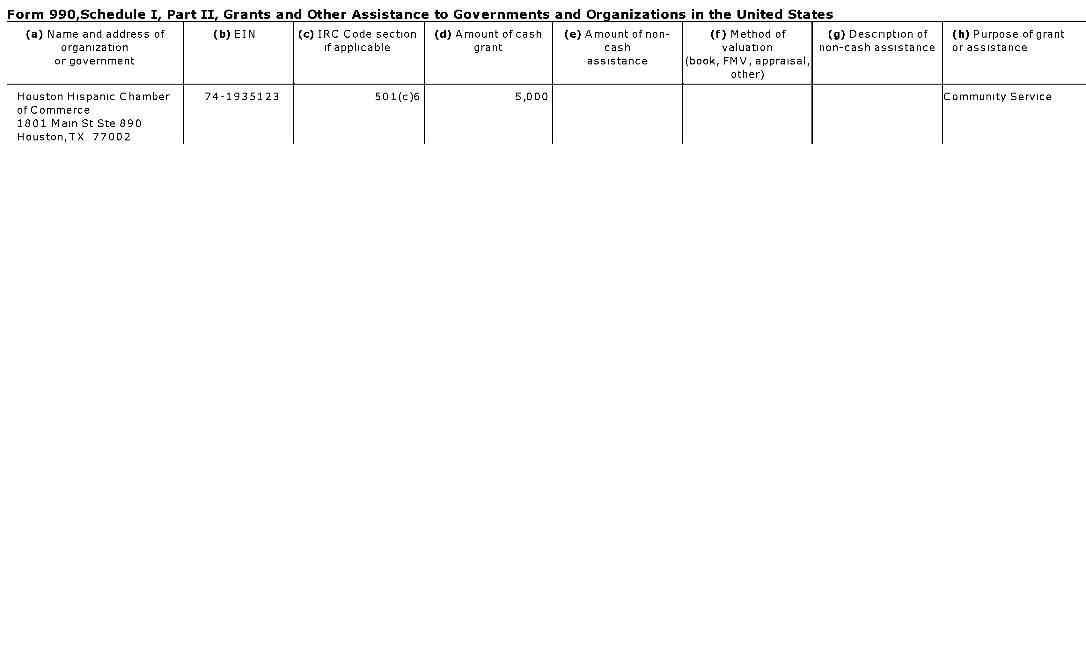
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Houston Hispanic Chamber 74-1935123 501(c)6 5,000 Community Serviceof Commerce1801 Main St Ste 890Houston,TX 77002
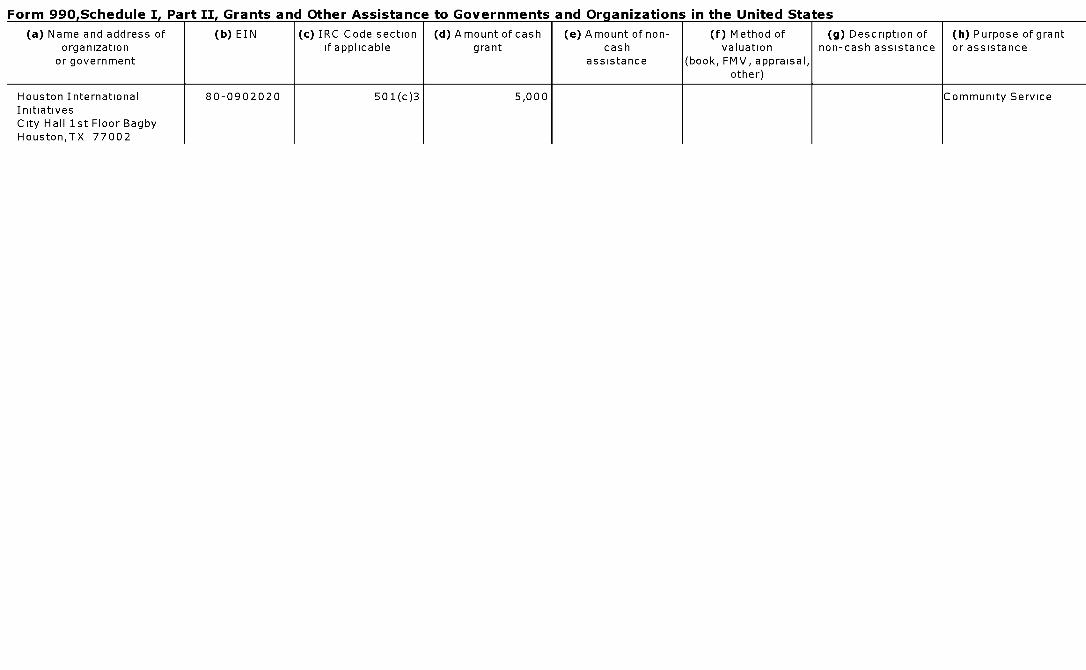
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Houston International 80-0902020 501(c)3 5,000 Community ServiceInitiativesCity Hall 1st Floor BagbyHouston,TX 77002
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Interface-Samaritan 74-1734082 501(c)3 10,000 Mental HealthCounseling Centers Inc Services4803 San FelipeHouston,TX 77045
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Jewish Federation of Greater 74-1109654 501(c)3 5,000 Community ServiceHouston5603 S BraeswoodHouston,TX 770963907
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Lifeline Chaplancy Inc- 20-2193278 501(c)3 5,000 Community ServiceCompassionate Touch Inc1415 Southmore BlvdHouston,TX 77004
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Local Infant Formula for 76-0296548 501(c)3 5,000 Baby needs forEmergencies(LIFE) Disasters2002 S Wayside 113Houston,TX 77023
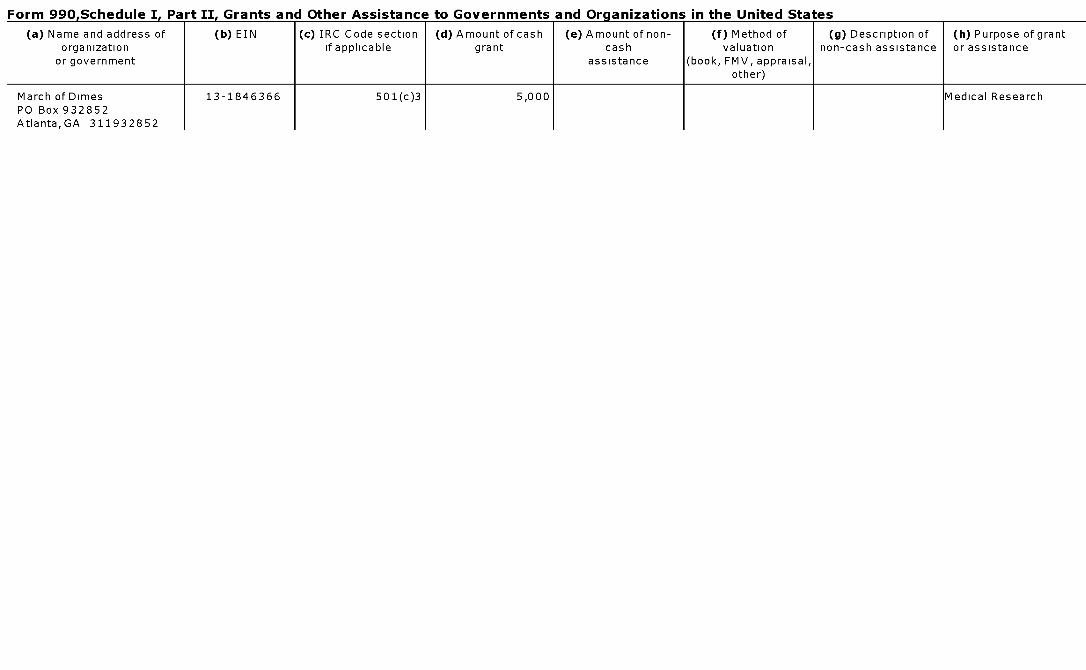
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
March of Dimes 13-1846366 501(c)3 5,000 Medical ResearchPO Box 932852Atlanta,GA 311932852
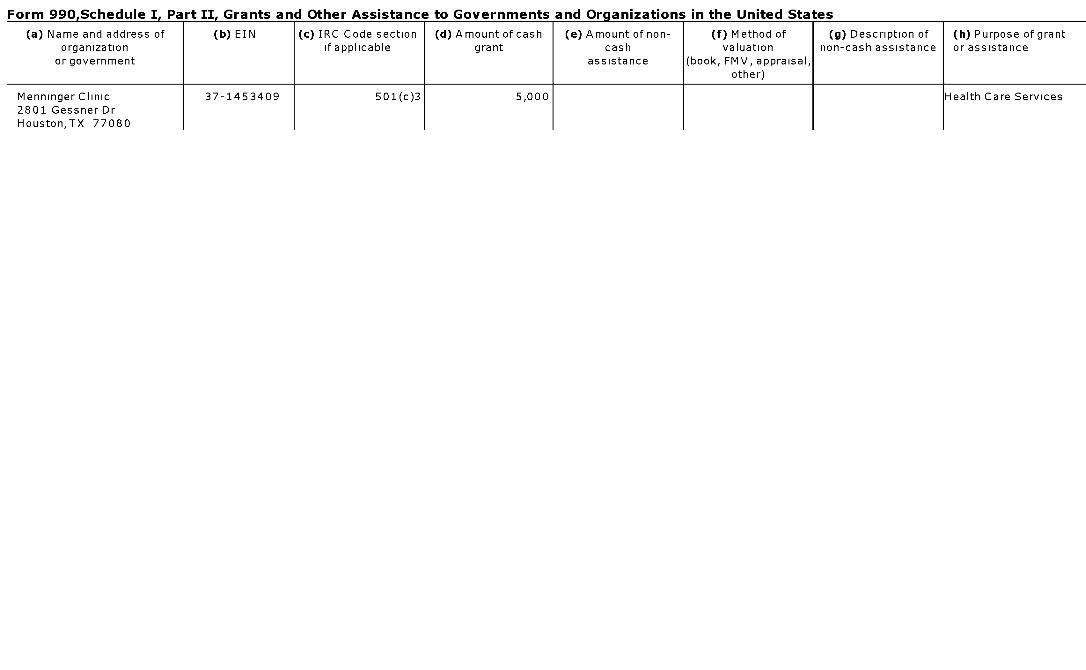
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
MenningerClinic 37-1453409 501(c)3 5,000 Health Care Services2801 Gessner DrHouston,TX 77080
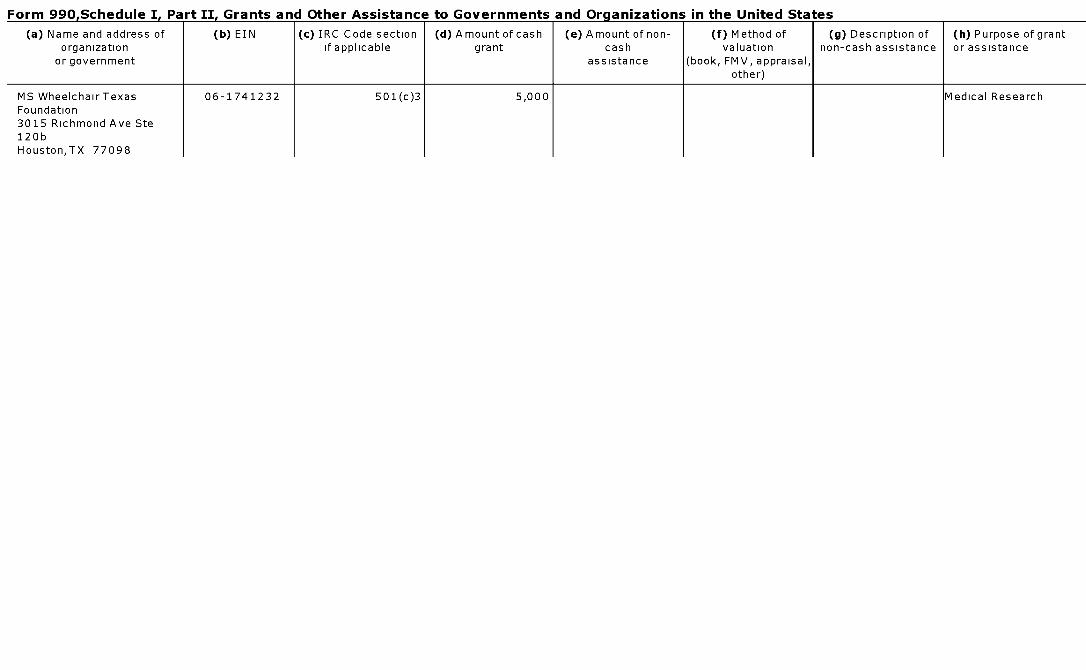
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
MS WheelchairTexas 06-1741232 501(c)3 5,000 Medical ResearchFoundation3015 Richmond Ave Ste120bHouston,TX 77098
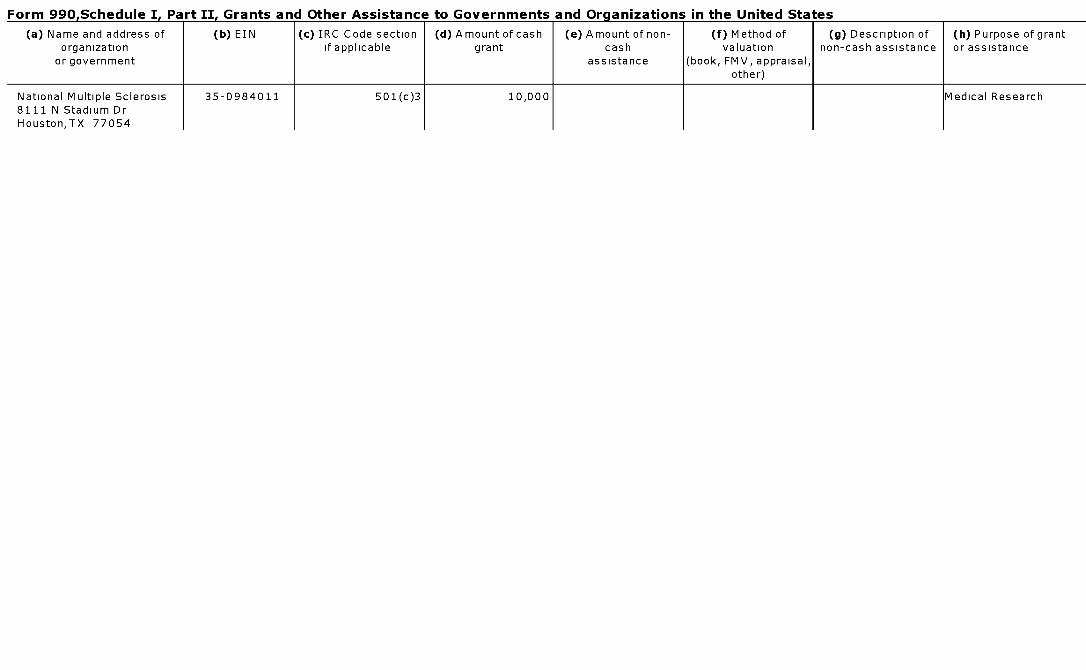
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
National Multiple Sclerosis 35-0984011 501(c)3 10,000 Medical Research8111 N Stadium DrHouston,TX 77054
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Nehemiah Center 76-0437157 501(c)3 15,000 Community5015 Fannin St AssistanceHouston,TX 77004
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c ) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Neighborhood Centers Inc 23-7062976 501(c)3 5,000 Community InitiativesPO Box 271389Houston,TX 77277
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Nora's Gift Foundation 62-1763895 501(c)3 10,000 CommunityPO Box 8350 AssistanceHouston,TX 772888350
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
PAWS Houston 26-0054032 501(c)3 5,000 Rehabilitative Support5201 Memorial DrSte 1162Houston,TX 77007
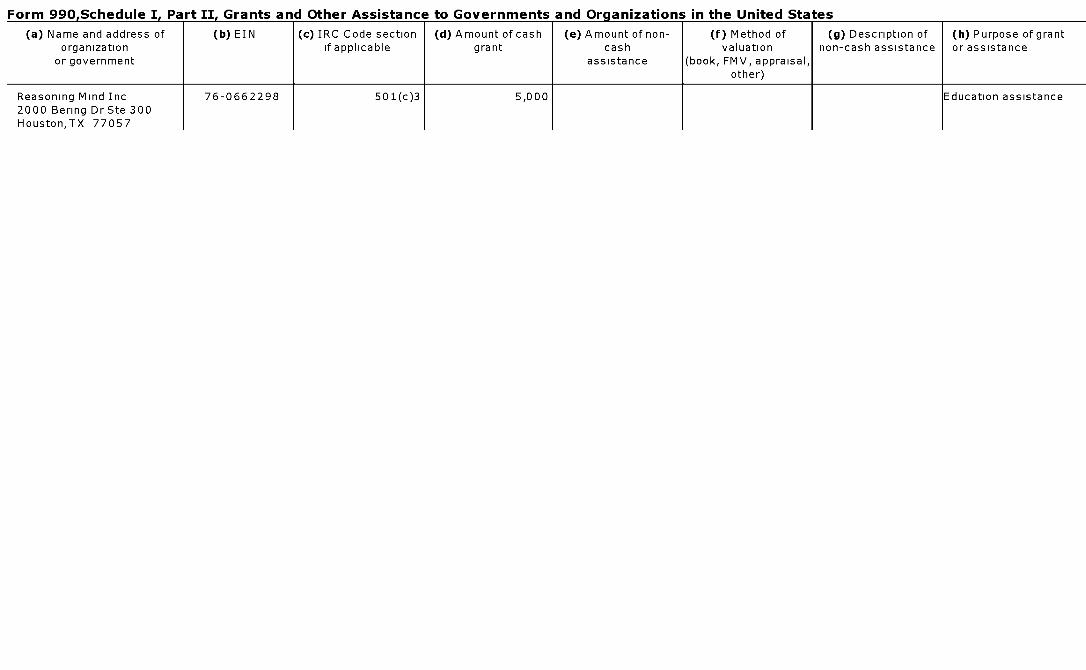
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Reasoning Mind Inc 76-0662298 501(c)3 5,000 Education assistance2000 Bering Dr Ste 300Houston,TX 77057
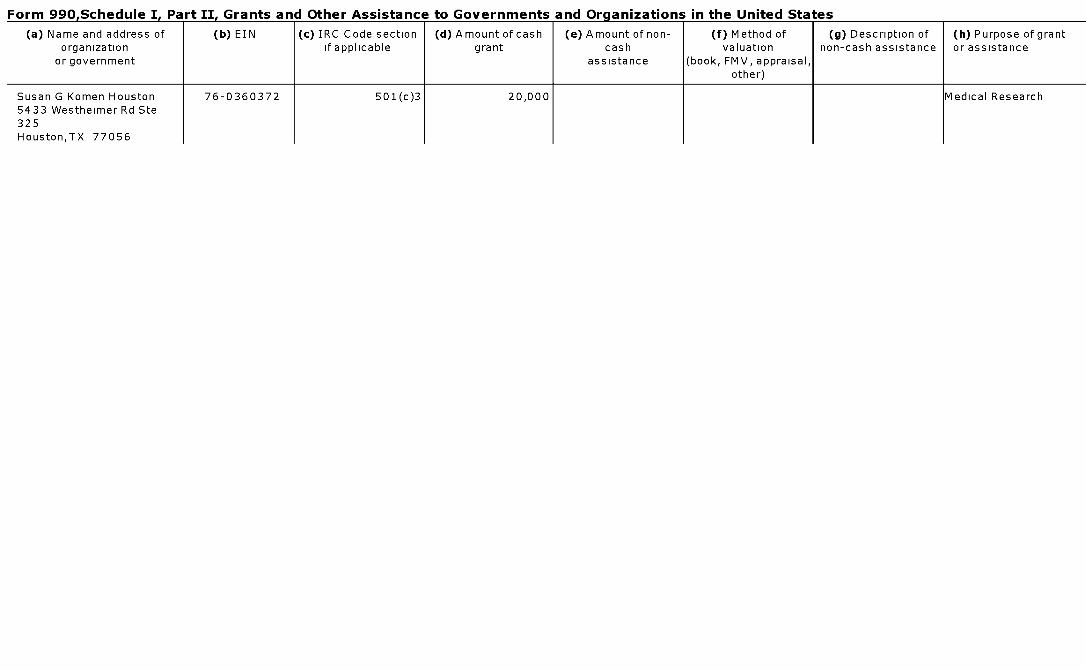
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Susan G Komen Houston 76-0360372 501(c)3 20,000 Medical Research5433 Westheimer Rd Ste325Houston,TX 77056
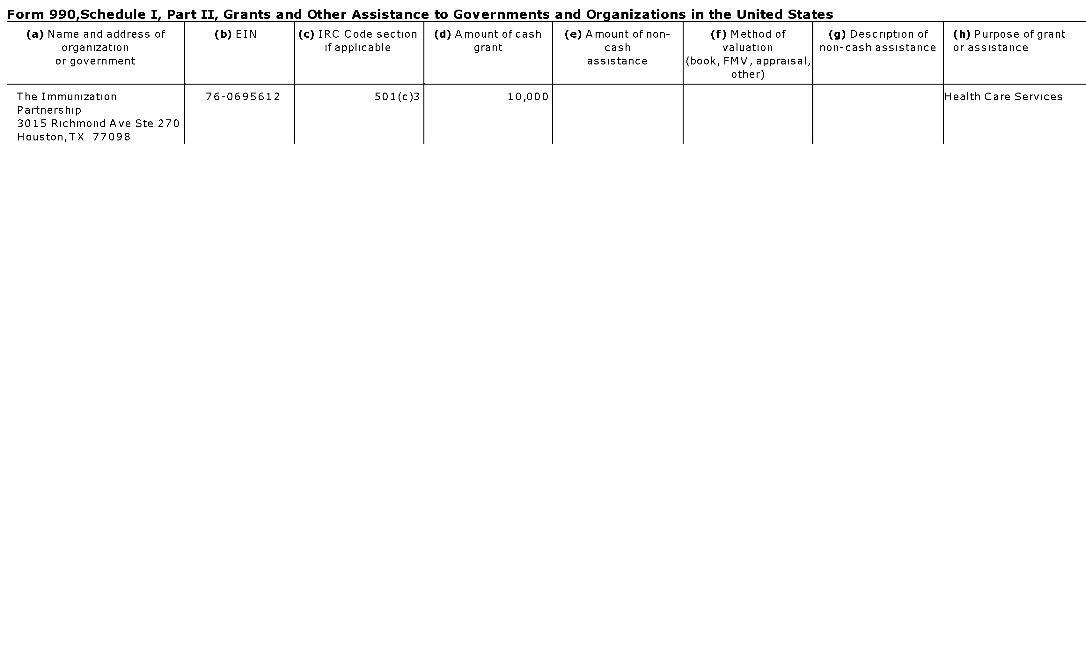
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
The Immunization 76-0695612 501(c)3 10,000 Health Care ServicesPartnership3015 Richmond Ave Ste 270Houston,TX 77098
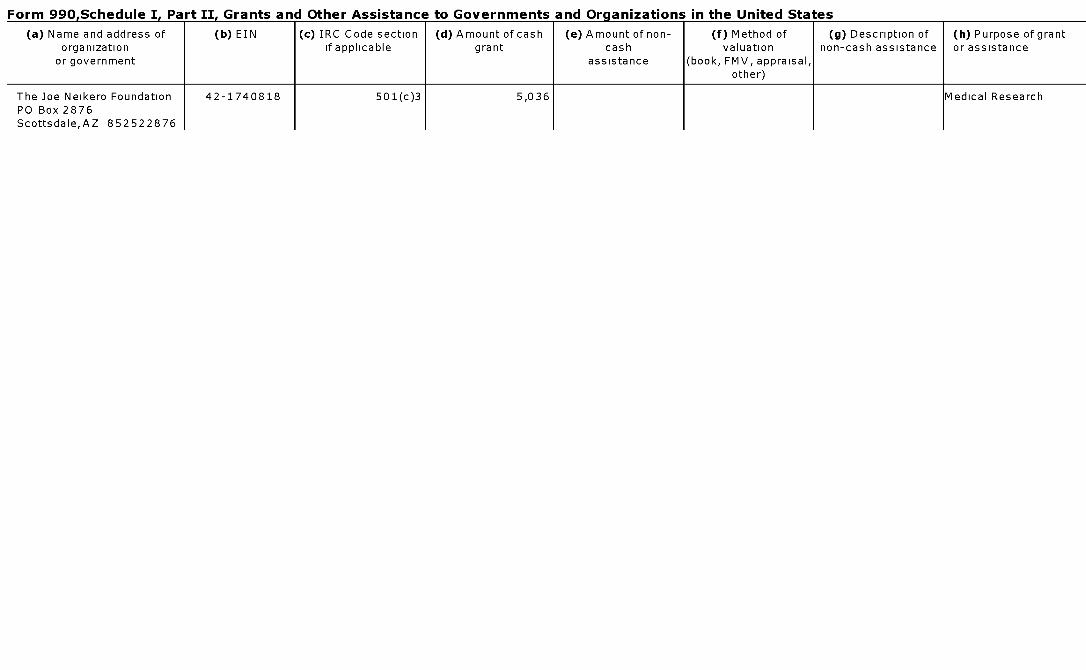
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
The Joe Neikero Foundation 42-1740818 501(c)3 5,036 Medical ResearchPO Box 2876Scottsdale,AZ 852522876
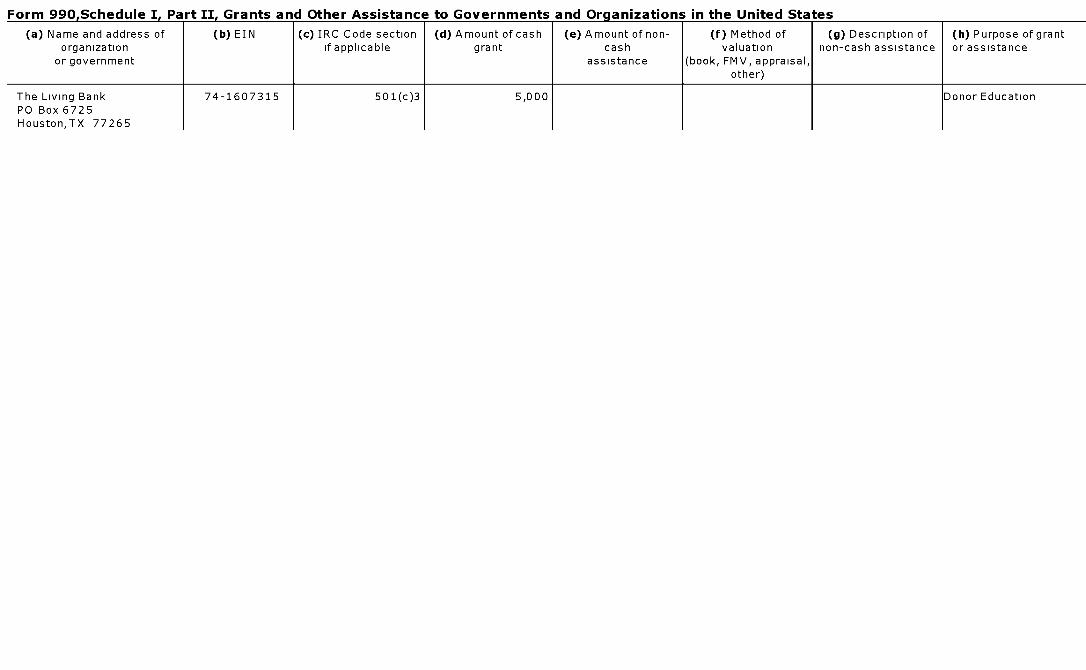
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
The Living Bank 74-1607315 501(c)3 5,000 Donor EducationPO Box 6725Houston,TX 77265
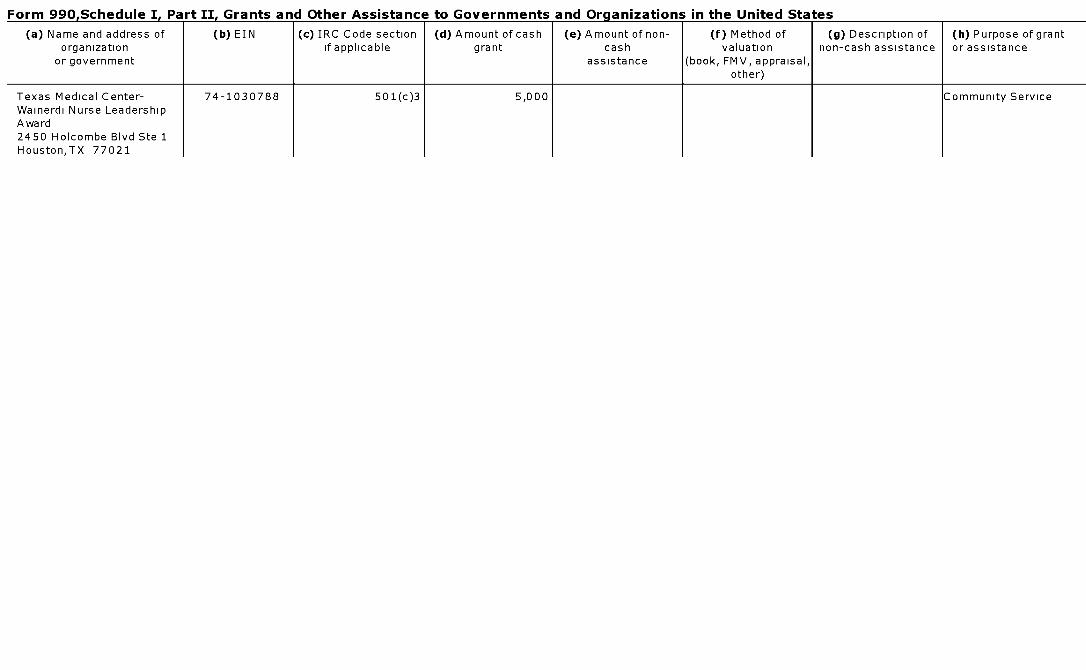
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Texas Medical Center- 74-1030788 501(c)3 5,000 Community ServiceWainerdi Nurse LeadershipAward2450 Holcombe Blvd Ste 1Houston,TX 77021
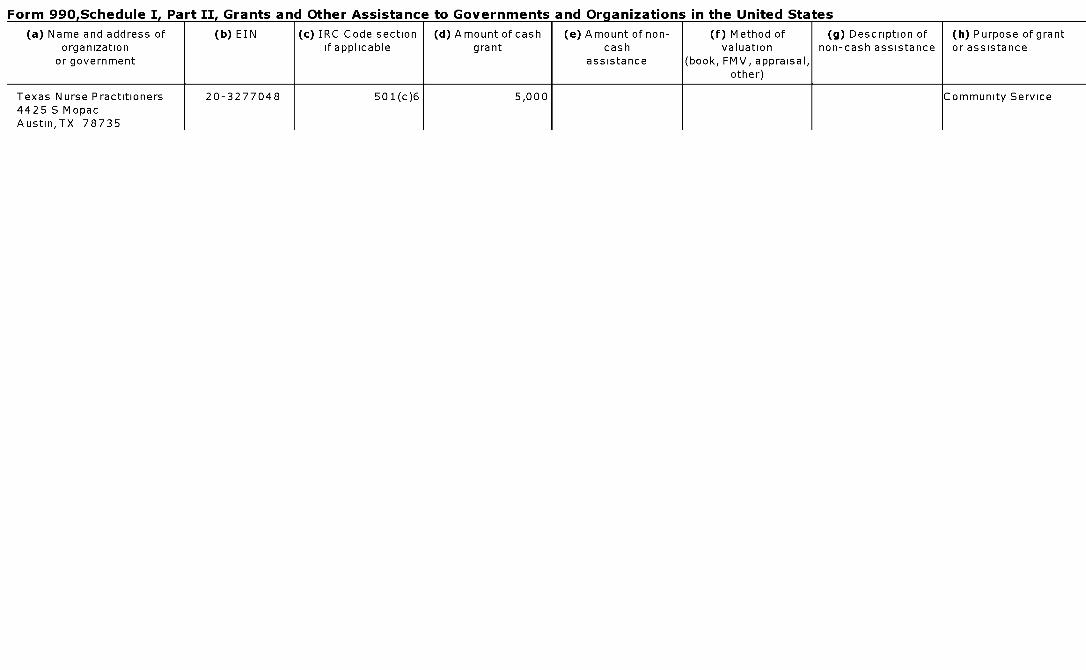
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
Texas Nurse Practitioners 20-3277048 501(c)6 5,000 Community Service4425 S MopacAustin,TX 78735
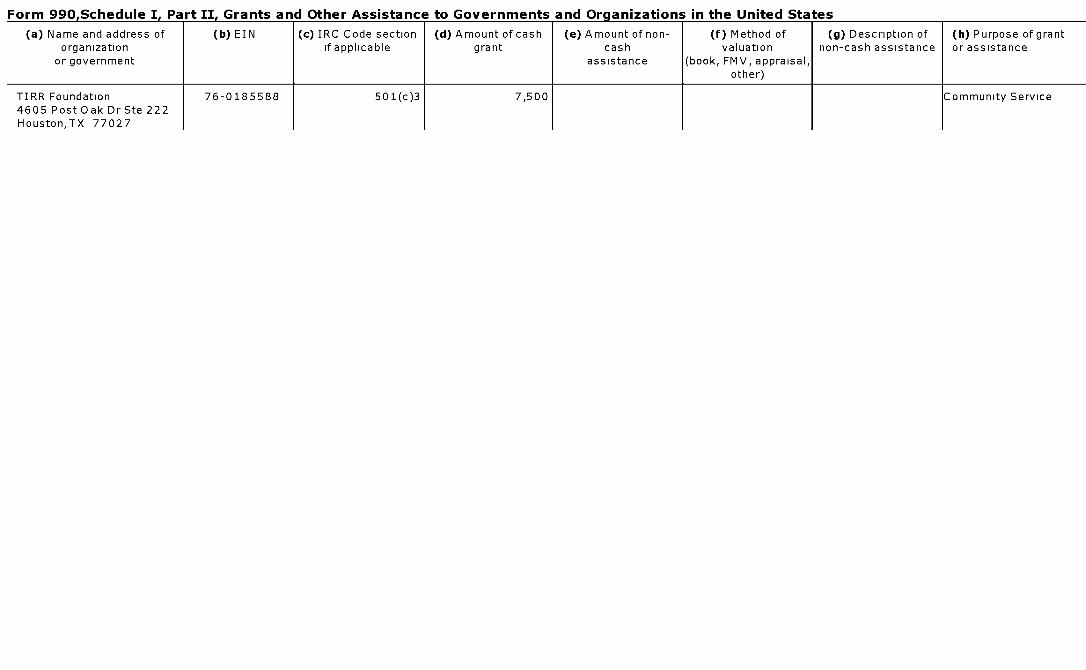
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
TIRR Foundation 76-0185588 501(c)3 7,500 Community Service4605 Post Oak Dr Ste 222Houston,TX 77027
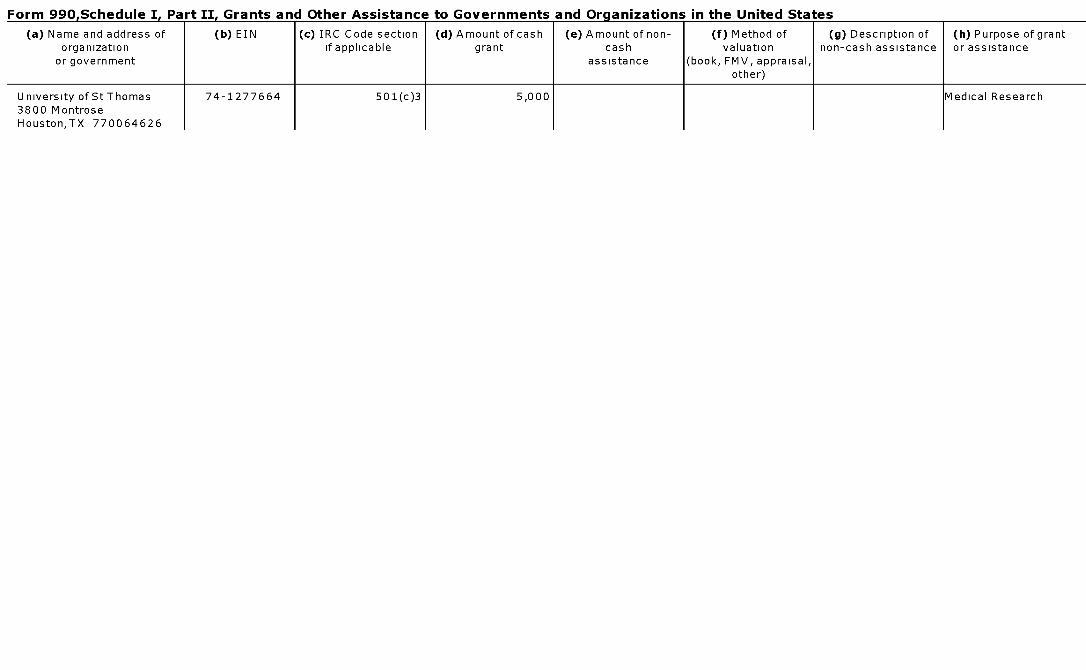
Form 990.Schedule I. Part II. Grants and Other Assistance to Governments and Organizations in the United States
(a) Name and address of (b) EIN (c) IRC Code section (d) Amount of cash (e) Amount of non- (f) Method of (g) Description of (h) Purpose of grantorganization if applicable grant cash valuation non-cash assistance or assistance
or government assistance (book, FMV, appraisal,other)
University of St Thomas 74-1277664 501(c)3 5,000 Medical Research3800 MontroseHouston,TX 770064626
l efile GRAPHIC p rint - DO NOT PROCESS As Filed Data - DLN: 93493321108274
Schedule J Compensation Information OMB No 1545-0047
(Form 990)For certain Officers, Directors, Trustees, Key Employees, and Highest
2013Compensated Employees1- Complete if the organization answered "Yes" to Form 990, Part IV, line 23.
Department of the Treasury 1- Attach to Form 990. 1- See separate instructions. 'Internal Revenue Service 1- Information about Schedule J (Form 990) and its instructions is at www.irs.gov /form990.
Name of the organization Employer identification numberTHE METHODIST HOSPITAL
74-1180155
EFROOK Questions Re g arding Com pensation
Yes No
la Check the appropiate box(es ) if the organization provided any of the following to or for a person listed in Form990, Part VII , Section A, line la Complete Part III to provide any relevant information regarding these items
1 First-class or charter travel 1 Housing allowance or residence for personal use
F Travel for companions 1 Payments for business use of personal residence
1 Tax idemnification and gross-up payments 1 Health or social club dues or initiation fees
1 Discretionary spending account 1 Personal services ( e g , maid, chauffeur, chef)
b If any of the boxes in line la are checked , did the organization follow a written policy regarding payment orreimbursement or provision of all of the expenses described above? If "No ," complete Part III to explain lb Yes
2 Did the organization require substantiation prior to reimbursing or allowing expenses incurred by alldirectors , trustees, officers, including the CEO/Executive Director, regarding the items checked in line la? 2 Yes
3 Indicate which , if any, of the following the filing organization used to establish the compensation of theorganization 's CEO/Executive Director Check all that apply Do not check any boxes for methodsused by a related organization to establish compensation of the CEO /Executive Director, but explain in Part III
F Compensation committee 1 Written employment contract
F Independent compensation consultant F Compensation survey or study
1 Form 990 of other organizations F Approval by the board or compensation committee
4 During the year, did any person listed in Form 990, Part VII, Section A, line la with respect to the filing organizationor a related organization
a Receive a severance payment or change-of-control payment? 4a No
b Participate in, or receive payment from, a supplemental nonqualified retirement plan? 4b Yes
c Participate in, or receive payment from, an equity-based compensation arrangement? 4c No
If "Yes" to any of lines 4a-c, list the persons and provide the applicable amounts for each item in Part III
Only 501 ( c)(3) and 501 ( c)(4) organizations only must complete lines 5-9.
5 For persons listed in Form 990, Part VII, Section A, line la, did the organization pay or accrue anycompensation contingent on the revenues of
a The organization? 5a No
b Any related organization? 5b No
If "Yes," to line 5a or 5b, describe in Part III
6 For persons listed in Form 990, Part VII, Section A, line la, did the organization pay or accrue anycompensation contingent on the net earnings of
a The organization? 6a No
b Any related organization? 6b No
If "Yes," to line 6a or 6b, describe in Part III
7 For persons listed in Form 990, Part VII, Section A, line la, did the organization provide any non-fixedpayments not described in lines 5 and 6? If "Yes," describe in Part III 7 Yes
8 Were any amounts reported in Form 990, Part VII, paid or accured pursuant to a contract that wassubject to the initial contract exception described in Regulations section 53 4958-4(a)(3)? If "Yes," describein Part III 8 No
9 If "Yes" to line 8, did the organization also follow the rebuttable presumption procedure described in Regulationssection 53 4958-6(c)? 9
For Paperwork Reduction Act Notice, see the Instructions for Form 990. Cat No 50053T Schedule 3 ( Form 990) 2013
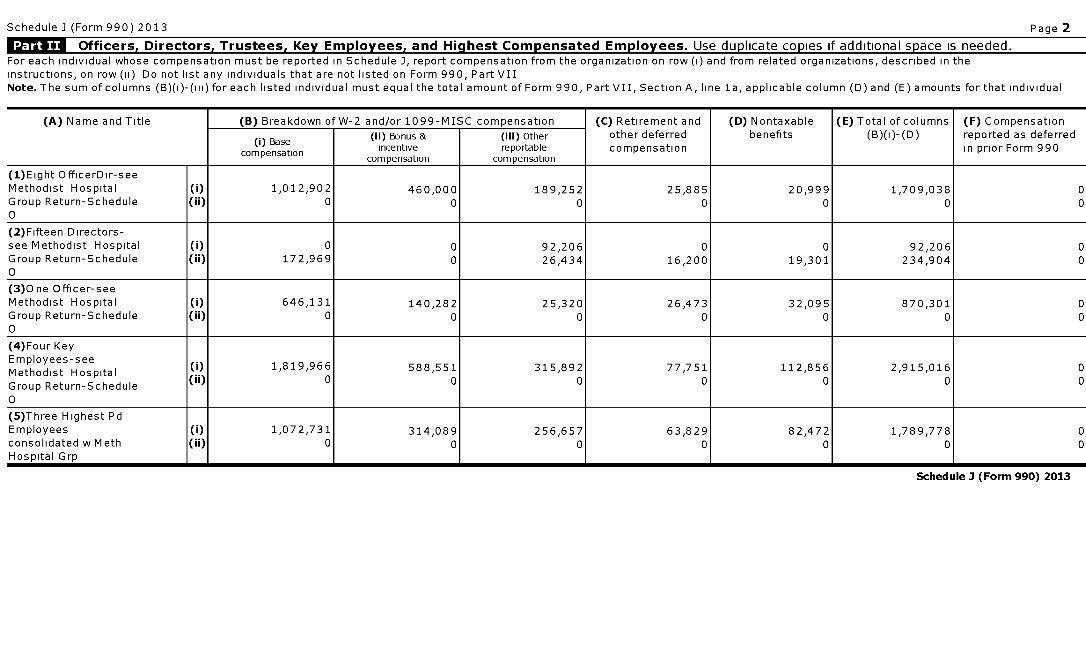
Schedule J (Form 990) 2013 Page 2
Officers , Directors , Trustees , Key Employees, and Highest Compensated Employees . Use duplicate copies if additional space is needed.For each individual whose compensation must be reported in Schedule J, report compensation from the organization on row (i) and from related organizations, described in theinstructions, on row (ii) Do not list any individuals that are not listed on Form 990, Part VIINote . The sum of columns (B)(1)-(iii) for each listed individual must equal the total amount of Form 990, Part VII, Section A, line la, applicable column (D) and (E) amounts for that individual
(A) Name and Title (B) Breakdown of W-2 and/or 1099-MISC compensation (C) Retirement and (D) Nontaxable (E) Total of columns (F) Compensation
(i) Base (ii) Bonus & (iii) Other other deferred benefits (B)(1)-(D) reported as deferred
compensationincentive reportable compensation in prior Form 990
compensation compensation
(1)Eight OfficerDir-seeMethodist Hospital 0) 1,012,902 460,000 189,252 25,885 20,999 1,709,038 0Group Return-Schedule (ii) 0 0 0 0 0 0 00
(2)Fifteen Directors-see Methodist Hospital (i) 0 0 92,206 0 0 92,206 0Group Return-Schedule (ii) 172,969 0 26,434 16,200 19,301 234,904 00
(3)One Officer-seeMethodist Hospital 0) 646,131 140,282 25,320 26,473 32,095 870,301 0Group Return-Schedule (ii) 0 0 0 0 0 0 00
(4)Four KeyEmployees-seeMethodist HospitalMeth 0) 1,819,966 588,551 315,892 77,751 112,856 2,915,016 0
Group Return-Schedule (ii) 0 0 0 0 0 0 0
0
(5)Three Highest PdEmployees 0) 1,072,731 314,089 256,657 63,829 82,472 1,789,778 0consolidated w Meth (ii) 0 0 0 0 0 0 0Hospital Grp
Schedule 3 (Form 990) 2013

Schedule J (Form 990) 2013 Page 3
Supplemental InformationProvide the information, explanation, or descriptions required for Part I, lines la, 1b, 3, 4a, 4b, 4c, 5a, 5b, 6a, 6b, 7, and 8, and for Part IIAlso complete this part for any additional information
Return Reference Explanation
Part I, Line la Travel for Companions Methodist requires all employees including officers to provide written substantiation of all expenses related to their businesstravel through the provision of detailed receipts in order to receive approval from their direct superiors for reimbursement in accordance with our corporatepolicy on travel and other business expenses In 2013, President/CEO had 1 trip approved for attendance at an out of state meeting where it was deemedappropriate by the Chair of our Board that the attendance of the President/CEO's spouse (and the related expenses for her travel to these meetings) wasintegral to conducting effective Methodist business at these meetings Part I, Line 4a Explanation The Methodist Hospital System has a formalseverance plan Eligible employees include all staff including hourly staff up through senior vice presidents provided they work at least 20 hours per weekand are not otherwise covered by a physician employment agreement The plan only provides salary and benefits in the event an eligible employee isinvoluntarily terminated due to the elimination of their position or if their current position is significantly impacted by an organizational restructuring orchange in requirement and a comparable position is not available within the organization The eligible person must also sign a termination agreement inorder to receive salary continuation and benefits under the plan to which they would not normally be eligible to receive under a voluntary resignationPursuant to Treasury Reg Section 1 6033-2(D)(5), The Methodist Hospital has elected to report information about contributions, gifts & grants,compensation and other information about Officers, Directors, Trustees, Key Employees, Former Employees, certain other highly paid employees, certainprofessional contractors and certain other contractors on a consolidated basis for all of the members of the group, including the parent organization, on theGroup Return of Methodist Hospital Group, EIN 35-2410801
Part I, Line 4b The Methodist Hospital has a Supplemental Executive Retirement Plan, a non-qualified employer funded plan Contributions are made annually into a taxdeferred account and are considered taxable upon vesting (i e completion of three years of vesting service) Once vested, each year's subsequentcontribution is taxable within the calendar year in which the deposit was made Account balances cannot be accessed until retirement or termination(whichever occurs first) and may be subject to non-revocable distribution options selected upon employment
Part I, Line 7 This organization provides variable compensation opportunity through an annual management incentive plan Executives at the Vice President level andabove may be eligible to participate The annual incentive program is based on system and operating entity level performance in the areas of qualityimprovement outcomes, patient satisfaction and financial performance In addition, a portion of the payout percentage is based on goals that are specificto the participants' management roles at the division or department level including but not limited to such metrics as operating results, quality and safetyimprovements, customer satisfaction measures, growth and innovation initiatives Determination of a participant's percentage of the potential bonuspayout (paid as a percent of base salary) is based on whether the individual attains agreed upon goals for their area of responsibility as determined bytheir immediate supervisor
Schedule J, PART II Pursuant to Treasury Reg Section 1 6033-2(D)(5), The Methodist Hospital has elected to report information about contributions, gifts & grants,compensation and other information about Officers, Directors, Trustees, Key Employees, Former Employees, certain other highly paid employees, certainprofessional contractors and certain other contractors on a consolidated basis for all of the members of the group, including the parent organization, on theGroup Return of Methodist Hospital Group, EIN 35-2410801
Schedule 3 (Form 990) 2013
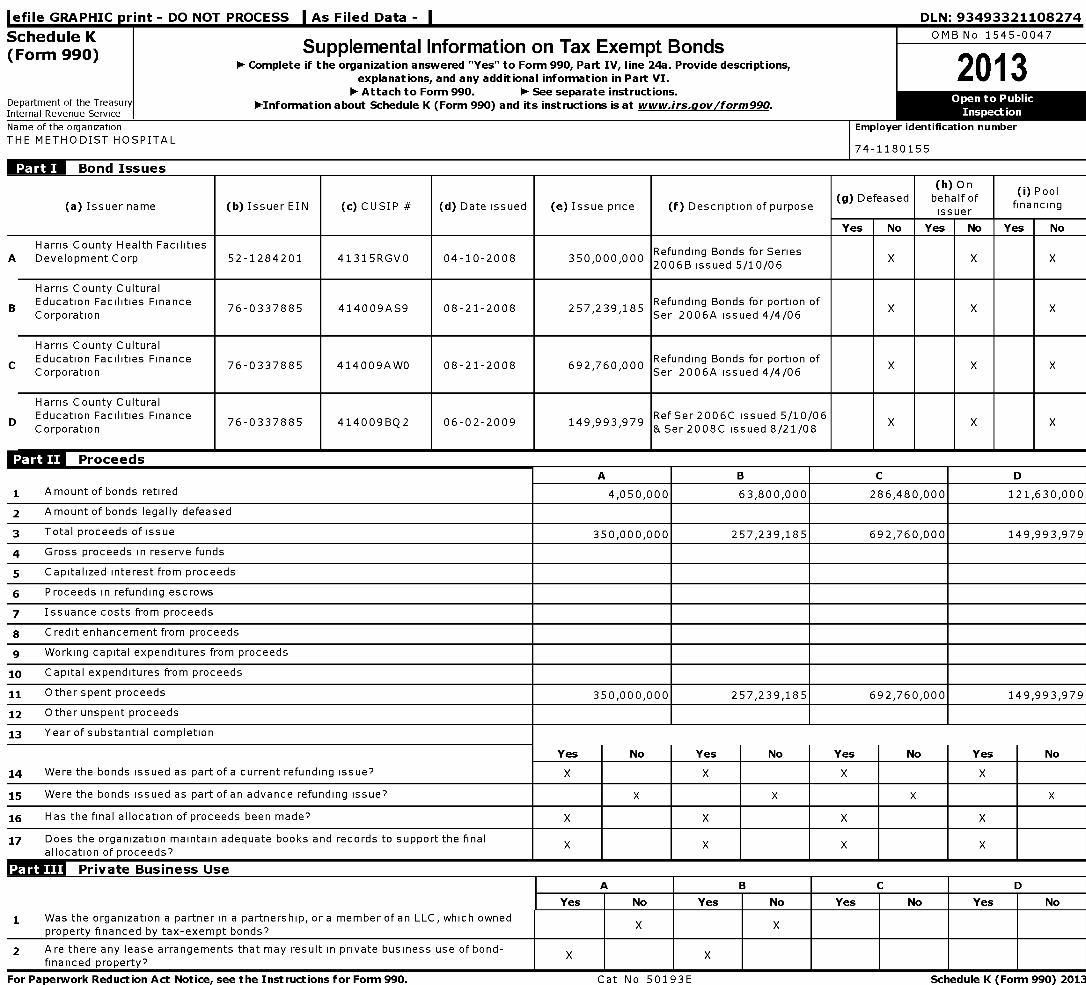
l efile GRAPHIC print - DO NOT PROCESS As Filed Data - DLN: 93493321108274
Schedule K OMB No 1545-0047
(Form 990) Supplemental Information on Tax Exempt Bonds1- Complete if the organization answered "Yes" to Form 990, Part IV, line 24a. Provide descriptions,
2013explanations, and any additional information in Part VI.1- Attach to Form 990. 1- See separate instructions.
Department of the Treasury 1-Information about Schedule K (Form 990) and its instructions is at www.irs.gov/form990 .Internal Revenue Service
Name of the organization Employer identification number
THE METHODIST HOSPITAL74-1180155
Bond Issues
(h) On(i) Pool
(a) Issuer name ( b) Issuer EIN (c) CUSIP # ( d) Date issued (e) Issue price (f) Description of purpose(g) Defeased behalf of
financingissuer
Yes No Yes No Yes No
Harris County Health FacilitiesRefunding Bonds for Series
A Development Corp 52-1284201 41315RGVO 04-10-2008 350,000,00020066 issued 5/10/06
X X X
Harris County CulturalB Education Facilities Finance
76-0337885 414009AS9 08-21-2008 257,239,185Refunding Bonds for portion of
X X XCorporation Ser 2006A issued 4/4/06
Harris County CulturalC Education Facilities Finance
76-0337885 414009AWO 08-21-2008 692,760,000Refunding Bonds for portion of
X X XCorporation Ser 2006A issued 4/4/06
Harris County CulturalD Education Facilities Finance
76-0337885 414009BQ2 06-02-2009 149,993,979Ref Ser 2006C issued 5 /10/06
X X XCorporation & Ser 2008C issued 8/21/08
n all Proceeds
A B C D
1 Amount of bonds retired 4,050,000 63,800,000 286,480,000 121,630,000
2 Amount of bonds legally defeased
3 Total proceeds of issue 350,000,000 257,239,185 692,760,000 149,993,979
4 Gross proceeds in reserve funds
5 Capitalized interest from proceeds
6 Proceeds in refunding escrows
7 Issuance costs from proceeds
8 Credit enhancement from proceeds
9 Working capital expenditures from proceeds
10 Capital expenditures from proceeds
11 Other spent proceeds 350,000,000 257,239,185 692,760,000 149,993,979
12 Other unspent proceeds
13 Year of substantial completion
Yes No Yes No Yes No Yes No
14 Were the bonds issued as part of a current refunding issue? X X X X
15 Were the bonds issued as part of an advance refunding issue? X X X X
16 Has the final allocation of proceeds been made? X X X X
17 Does the organization maintain adequate books and records to support the finalallocation of proceeds?
X X X X
f iii Private Business Use
A B C D
Yes No Yes No Yes No Yes No
1 Was the organization a partner in a partnership, or a member of an LLC, which ownedproperty financed by tax-exempt bonds?
X X
2 Are there any lease arrangements that may result in private business use of bond-X X
financed property?
For Paperwork Reduction Act Notice, see the Instructions for Form 990. Cat No 50193E Schedule K (Form 990) 2013
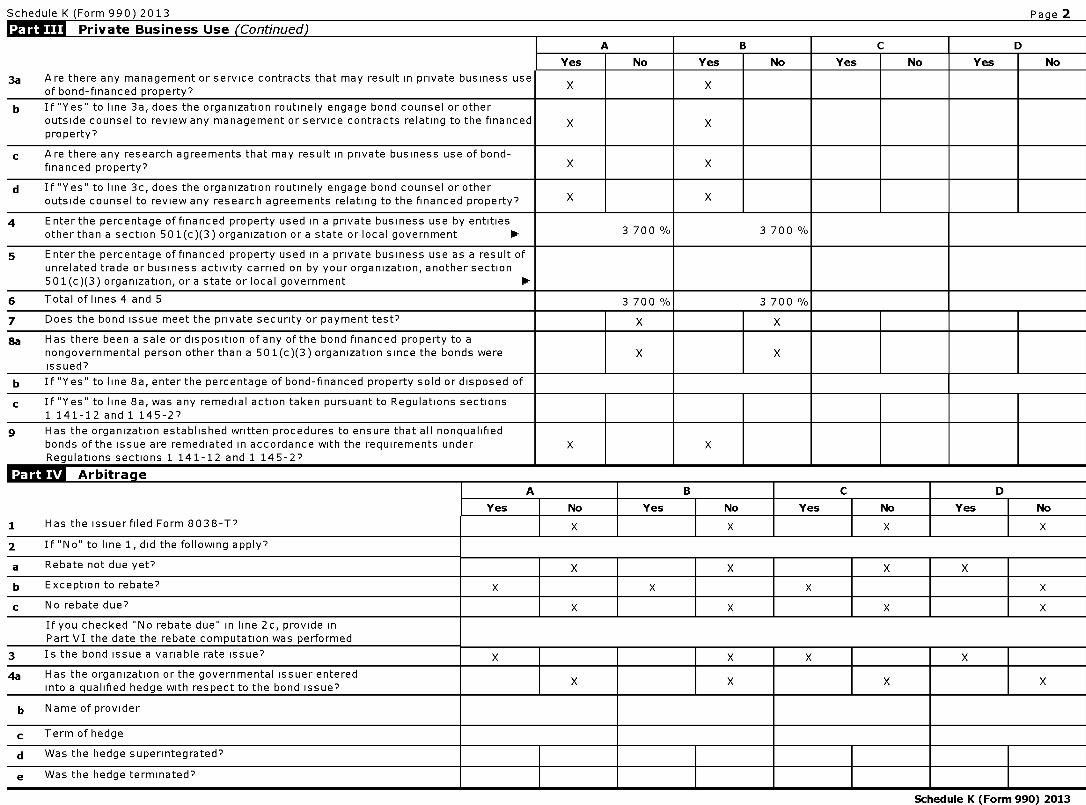
Schedule K (Form 990) 2013 Pa g e 2
Private Business Use (Continued)
A B C D
Yes No Yes No Yes No Yes No
3a Are there any management or service contracts that may result in private business useof bond-financed property?
X X
b If "Yes" to line 3a, does the organization routinely engage bond counsel or otheroutside counsel to review any management or service contracts relating to the financed X Xproperty?
c Are there any research agreements that may result in private business use of bond-financed property? X X
d If "Yes" to line 3c, does the organization routinely engage bond counsel or otheroutside counsel to review any research agreements relating to the financed property? X X
4 Enter the percentage of financed property used in a private business use by entitiesother than a section 501(c)(3) organization or a state or local government 0- 3 700 % 3 700 %
5 Enter the percentage of financed property used in a private business use as a result ofunrelated trade or business activity carried on by your organization, another section501(c)(3) organization, or a state or local government 0-
6 Total of lines 4 and 5 3 700 % 3 700 %
7 Does the bond issue meet the private security or payment test? X X
ga Has there been a sale or disposition of any of the bond financed property to anongovernmental person other than a 501(c)(3) organization since the bonds were X Xissued?
b If "Yes" to line 8a, enter the percentage of bond-financed property sold or disposed of
c If "Yes" to line 8a, was any remedial action taken pursuant to Regulations sections1 141-12 and 1 145-27
g Has the organization established written procedures to ensure that all nonqualifiedbonds of the issue are remediated in accordance with the requirements under X XRegulations sections 1 141-12 and 1 145-2?
ArbitrageA B C D
Yes No Yes No Yes No Yes No
1 Has the issuerfiled Form 8038-T? X X X X
2 If "No" to line 1, did the following apply?
a Rebate not due yet? X X X X
b Exception to rebate? X X X X
c No rebate due? X X X X
If you checked No rebate due" in line 2c, provide inPart VI the date the rebate computation was performed
3 Is the bond issue a variable rate issue? X X X X
4a Has the organization or the governmental issuer enteredinto a qualified hedge with respect to the bond issue?
X X X X
b Name of provider
c Term of hedge
d Was the hedge superintegrated?
e Was the hedge terminated?
Schedule K (Form 990) 2013
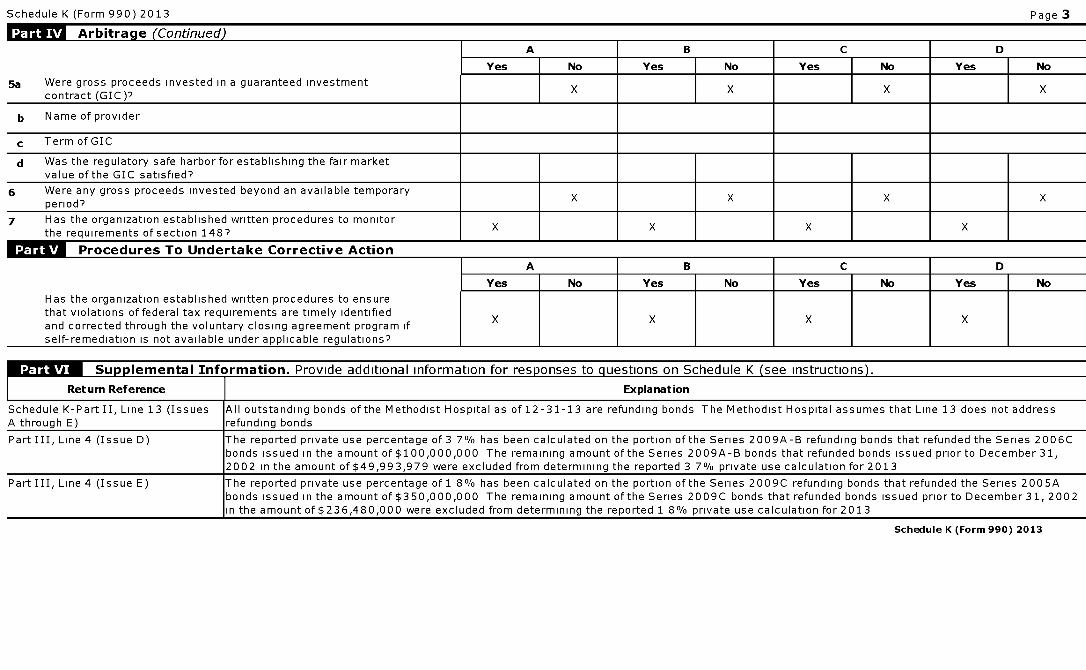
Schedule K (Form 990 ) 2013 Page 3
Arbitrage (Continued)A B C D
Yes No Yes No Yes No Yes No
5a Were gross proceeds invested in a guaranteed investmentX X X X
contract (GIC)7
b Name of provider
c Term of GIC
d Was the regulatory safe harbor for establishing the fair marketvalue of the GIC satisfied?
6 Were any gross proceeds invested beyond an available temporaryperiod?
X X X X
7 Has the organization established written procedures to monitorthe requirements of section 148?
X X X X
Procedures To Undertake Corrective ActionA
Has the organization established written procedures to ensurethat violations of federal tax requirements are timely identifiedand corrected through the voluntary closing agreement program ifself-remediation is not available under arDlicable regulations?
D
I Yes I No I Yes I No I Yes I No I Yes I No
X
Su lemental Information . Provide additional information for res ponses to q uestions on Schedule K ( see instructions ) .
Return Reference Explanation
Schedule K-Part II, Line 13 (Issues All outstanding bonds of the Methodist Hospital as of 12-31-13 are refunding bonds The Methodist Hospital assumes that Line 13 does not addressA through E) refunding bonds
Part III, Line 4 (Issue D) The reported private use percentage of 3 7% has been calculated on the portion of the Series 2009A-B refunding bonds that refunded the Series 2006Cbonds issued in the amount of $100,000,000 The remaining amount of the Series 2009A-B bonds that refunded bonds issued prior to December 31,2002 in the amount of $49,993,979 were excluded from determining the reported 3 7% private use calculation for 2013
Part III, Line 4 (Issue E) The reported private use percentage of 1 8% has been calculated on the portion of the Series 2009C refunding bonds that refunded the Series 2005Abonds issued in the amount of $350,000,000 The remaining amount of the Series 2009C bonds that refunded bonds issued prior to December 31, 2002in the amount of $236,480,000 were excluded from determining the reported 1 8% private use calculation for 2013
Schedule K (Form 990) 2013
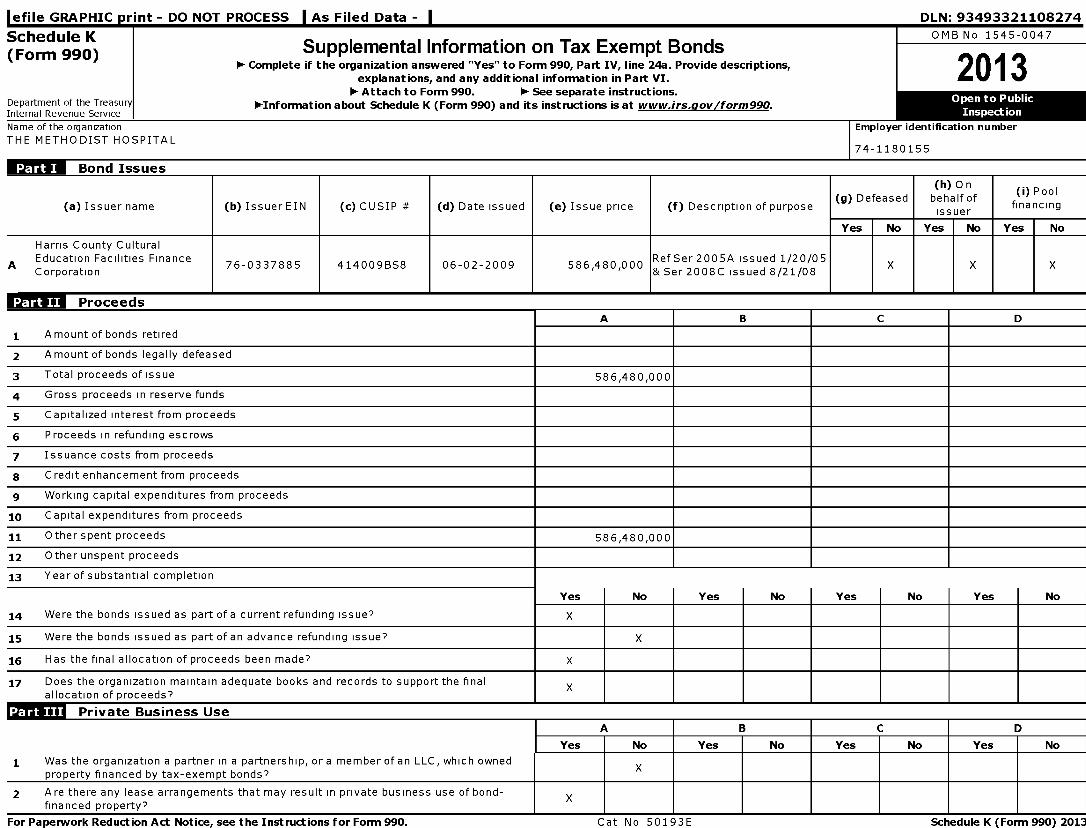
l efile GRAPHIC print - DO NOT PROCESS As Filed Data - DLN: 93493321108274
Schedule K OMB No 1545-0047
(Form 990) Supplemental Information on Tax Exempt Bonds1- Complete if the organization answered "Yes" to Form 990, Part IV, line 24a. Provide descriptions,
2013explanations, and any additional information in Part VI.1- Attach to Form 990. 1- See separate instructions.
Department of the Treasury 1-Information about Schedule K (Form 990) and its instructions is at www.irs.gov/form990 .Internal Revenue Service
Name of the organization Employer identification number
THE METHODIST HOSPITAL74-1180155
Bond Issues
(h) On(i) Pool
(a) Issuer name ( b) Issuer EIN (c) CUSIP # ( d) Date issued ( e) Issue price (f) Description of purpose(g) Defeased behalf of
financingissuer
Yes No Yes No Yes No
Harris County CulturalA Education Facilities Finance
76-0337885 414009B58 06-02-2009 586,480,000RefSer2005A issued 1/20/05
X X XCorporation & Ser 2008C issued 8/21/08
n OOG Proceeds
A B C D
1 A mount of bonds retired
2 Amount of bonds legally defeased
3 Total proceeds of issue 586,480,000
4 Gross proceeds in reserve funds
5 Capitalized interest from proceeds
6 Proceeds in refunding escrows
7 Issuance costs from proceeds
8 Credit enhancement from proceeds
9 Working capital expenditures from proceeds
10 Capital expenditures from proceeds
11 Other spent proceeds 586,480,000
12 Other unspent proceeds
13 Year of substantial completion
Yes No Yes No Yes No Yes No
14 Were the bonds issued as part of a current refunding issue? X
15 Were the bonds issued as part of an advance refunding issue? X
16 Has the final allocation of proceeds been made? X
17 Does the organization maintain adequate books and records to support the finalallocation of proceeds?
X
I T I I I Private Business Use
A B C D
Yes No Yes No Yes No Yes No
1 Was the organization a partner in a partnership, or a member of an LLC, which ownedproperty financed by tax-exempt bonds?
X
2 Are there any lease arrangements that may result in private business use of bond- Xfinanced property?
For Paperwork Reduction Act Notice, see the Instructions for Form 990. Cat No 50193E Schedule K (Form 990) 2013
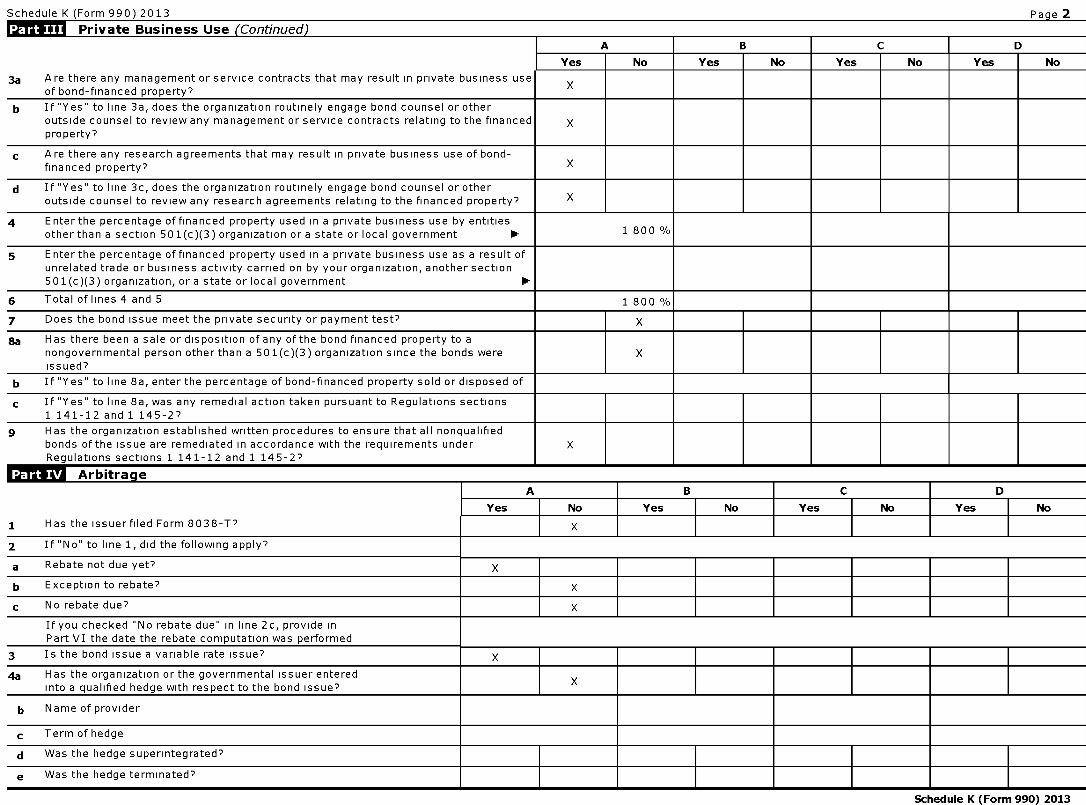
Schedule K (Form 990) 2013 Pa g e 2
Private Business Use (Continued)
A B C D
Yes No Yes No Yes No Yes No
3a Are there any management or service contracts that may result in private business useof bond-financed property?
X
b If "Yes" to line 3a, does the organization routinely engage bond counsel or otheroutside counsel to review any management or service contracts relating to the financed Xproperty?
c Are there any research agreements that may result in private business use of bond-financed property? X
d If "Yes" to line 3c, does the organization routinely engage bond counsel or otheroutside counsel to review any research agreements relating to the financed property? X
4 Enter the percentage of financed property used in a private business use by entitiesother than a section 501(c)(3) organization or a state or local government 0- 1 800 %
5 Enter the percentage of financed property used in a private business use as a result ofunrelated trade or business activity carried on by your organization, another section501(c)(3) organization, or a state or local government 0-
6 Total of lines 4 and 5 1 800 %
7 Does the bond issue meet the private security or payment test? X
ga Has there been a sale or disposition of any of the bond financed property to anongovernmental person other than a 501(c)(3) organization since the bonds were Xissued?
b If "Yes" to line 8a, enter the percentage of bond-financed property sold or disposed of
c If "Yes" to line 8a, was any remedial action taken pursuant to Regulations sections1 141-12 and 1 145-27
g Has the organization established written procedures to ensure that all nonqualifiedbonds of the issue are remediated in accordance with the requirements under XRegulations sections 1 141-12 and 1 145-2?
ArbitrageA B C D
Yes No Yes No Yes No Yes No
1 Has the issuerfiled Form 8038-T? X
2 If "No" to line 1, did the following apply?
a Rebate not due yet? X
b Exception to rebate? X
c No rebate due? X
If you checked No rebate due" in line 2c, provide inPart VI the date the rebate computation was performed
3 Is the bond issue a variable rate issue? X
4a Has the organization or the governmental issuer enteredinto a qualified hedge with respect to the bond issue?
X
b Name of provider
c Term of hedge
d Was the hedge superintegrated?
e Was the hedge terminated?
Schedule K (Form 990) 2013
Schedule K (Form 990) 2013 Page 3
Arbitrage (Continued )
A B C D
Yes No Yes No Yes No Yes No
5a Were gross proceeds invested in a guaranteed investment Xcontract (GIC)7
b Name of provider
c Term of GIC
d Was the regulatory safe harbor for establishing the fair marketvalue of the GIC satisfied?
6 Were any gross proceeds invested beyond an available temporaryperiod?
X
7 Has the organization established written procedures to monitorthe requirements of section 148?
X
ff^illll Procedures To Undertake Corrective ActionA I B I C I D
I Yes I No I Yes I No I Yes I No I Yes I No
Has the organization established written procedures to ensurethat violations of federal tax requirements are timely identified Xand corrected through the voluntary closing agreement program ifself-remediation is not available under aoolicable regulations?
Supplemental Information . Provide additional information for responses to questions on Schedule K (see instructions).
IReturn Reference Explanation
Schedule K (Form 990) 2013
l efile GRAPHIC p rint - DO NOT PROCESS As Filed Data - DLN: 93493321108274
Schedule L Transactions with Interested Persons OMB No 1545-0047
(Form 990 or 990-EZ ) 0- Complete if the organization answered
2O13"Yes" on Form 990, Part IV , lines 25a , 25b, 26, 27, 28a , 28b, or 28c,or Form 990-EZ, Part V, line 38a or 40b.
Department of the Treasury 0- Attach to Form 990 or Form 990-EZ. 0- See separate instructions . Open
Internal Revenue Service 1-Information about Schedule L (Form 990 or 990 -EZ) and its instructions is at Inspe ctionwww.irs .gov/form990 .
Name of the organizationTHE METHODIST HOSPITAL
Employer identification number
1 74-1180155
L^l Excess Benefit Transactions (section 501(c)(3) and section 501(c)(4) organizations only).Cmmnlata iftha nrnanvatinn ancwarad "Yac" nn Fnrm 99O Part TV Iina 75a nr 75h nr Fnrm 990-F7 Part V lino 40h
1 (a) Name of disqualified person (b) Relationship between disqualified (c) Description of transaction (d) Corrected?person and organization Yes No
2 Enter the amount of tax incurred by organization managers or disqualified persons during the year under section4958 . . . . . . . . . . . . . . . . . . . . . . . . . . . ► $
3 Enter the amount of tax, if any, on line 2, above, reimbursed by the organization . ► $
Loans to and / or From Interested Persons.Complete if the organization answered "Yes" on Form 990-EZ, Part V, line 38a, or Form 990, Part IV, line 26, or if the
(a) Name of (b) (c) (d) Loan tointerested Relationship Purpose of or from theperson with loan organization?
organization
To I From
(e)Original ( f)Balance (g) Inprincipal due default?amount
Yes I No
(h)A pprovedby
boardor
committee?
Yes F No
(i)Writtenagreement?
Yes I No
Total ► $
Grants or Assistance Benefitting Interested Persons.Complete if the organization answered "Yes" on Form 990, Part IV, line 27.
(a) Name of interested (b) Relationship between (c) Amount of assistance (d) Type of assistance (e) Purpose of assistanceperson interested person and the
organization
For Paperwork Reduction Act Noticee see the Instructions for Form 990 or 990 -EZ. Cat No 50056A Schedule L (Form 990 or 990 - EZ) 2013
Schedule L (Form 990 or 990-EZ) 2013 Page 2
Business Transactions Involving Interested Persons.
Complete if the organization answered "Yes" on Form 990, Part IV, line 28a, 28b, or 28c.(a) Name of interested person (b) Relationship
between interestedperson and theorganization
(c) Amount oftransaction
(d) Description of transaction (e) Sharingof
organization'srevenues?
Yes No
(1) Laura Beth Nelson Daughter-G Nelson 25,000 Employment No
Supplemental Information
Return Reference I Explanation
Schedule L (Form 990 or 990-EZ) 2013
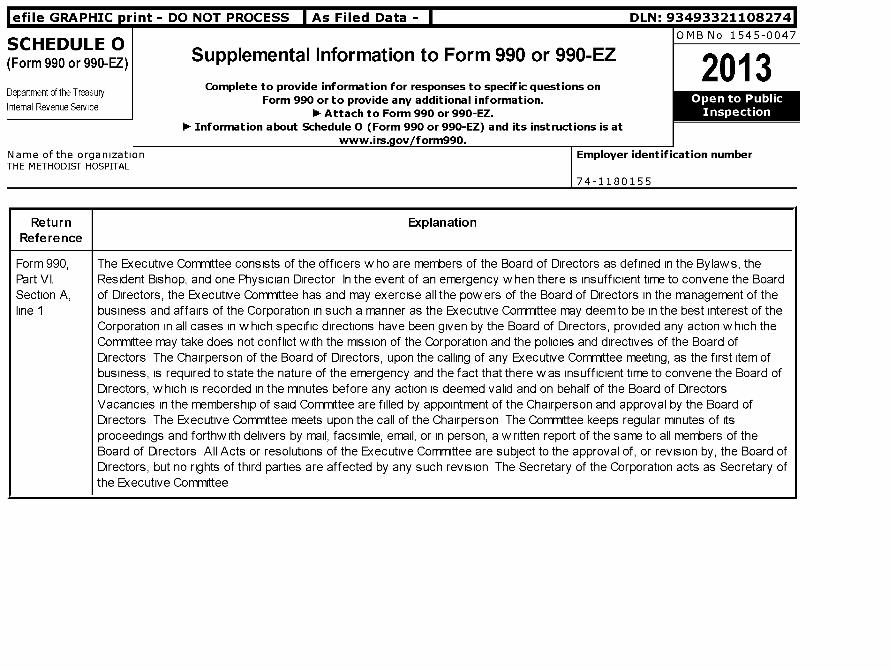
efile GRAPHIC p rint - DO NOT PROCESS As Filed Data - DLN: 93493321108274
SCHEDULE 0OMB No 1545 0047
(Form 990 or 990-EZ) Supplemental Information to Form 990 or 990-EZ2013
Department of the Treasury Complete to provide information for responses to specific questions onForm 990 or to provide any additional information . Open
Internal Revenue Service1- Attach to Form 990 or 990-EZ. Inspection
1- Information about Schedule 0 (Form 990 or 990-EZ) and its instructions is atwww.irs.gov/form990.
Name of the organization Employer identification numberTHE METHODIST HOSPITAL
74-1180155
ReturnReference
Explanation
Form 990, The Executive Committee consists of the officers who are members of the Board of Directors as defined in the Bylaws, thePart VI, Resident Bishop, and one Physician Director In the event of an emergency w hen there is insufficient time to convene the BoardSection A, of Directors, the Executive Committee has and may exercise all the powers of the Board of Directors in the management of theline 1 business and affairs of the Corporation in such a manner as the Executive Committee may deem to be in the best interest of the
Corporation in all cases in which specific directions have been given by the Board of Directors, provided any action which theCommittee may take does not conflict with the mission of the Corporation and the policies and directives of the Board ofDirectors The Chairperson of the Board of Directors, upon the calling of any Executive Committee meeting, as the first item ofbusiness, is required to state the nature of the emergency and the fact that there was insufficient time to convene the Board ofDirectors, which is recorded in the minutes before any action is deemed valid and on behalf of the Board of DirectorsVacancies in the membership of said Committee are filled by appointment of the Chairperson and approval by the Board ofDirectors The Executive Committee meets upon the call of the Chairperson The Committee keeps regular minutes of itsproceedings and forthwith delivers by mail, facsimile, email, or in person, a written report of the same to all members of theBoard of Directors All Acts or resolutions of the Executive Committee are subject to the approval of, or revision by, the Board ofDirectors, but no rights of third parties are affected by any such revision The Secretary of the Corporation acts as Secretary ofthe Executive Committee
Return Reference Explanation
Form 990, Part VI, Section A,line 7a
The Texas Annual Conference of the South Central Jurisdiction of the United Methodist Church ("Conference")elects the Board of Directors
ReturnReference
Explanation
Form 990, Part The Conference has the authority to approve any amendments to the following provisions of The Methodist Hospital's BylawsVI, Section A, or the Articles of Incorporation i) the provision that the Conference elects all Directors of this organization from nomineesline 7b recommended by the committee on Nominations of the Conference based on nominations made by the Board of Directors, (u)
the provision that a sufficient number of Directors be members of The United Methodist Church to comply with the membershiprequirements set forth in the Book of Discipline of The United Methodist Church, (vi) the provision that four Methodist Ministers,including the Resident Bishop be members of the Board of Directors, (iv) the provision that the Board of Directors shall consistof no more than twenty-six and no fewer than fifteen members, or (v) the provision that amend the purpose clauses (Article IIand VI) of the Articles of Incorporation of the Corporation or the dissolution clause (Article VII) of the Articles of Incorporationof the Corporation
Return ExplanationReference
Form 990, Part VI, Management, including certain Officers, works diligently to complete the Form 990 and attached schedules ("return") in aSection B, line 11 thorough manner The return is prepared by a Paid Preparer Prior to filing the return, a copy of the Form 990 is made
availabe to Board members (including required schedules), and management team members are available to answer anyBoard Members' questions
ReturnReference
Explanation
Form 990, Part All Individuals serving in a significant decision making capacity complete a Conflict of Interest (COI) questionnaire annually AVI, Section B, comprehensive evaluation and thorough review of all disclosures is performed by a 6-member COI Committee comprised ofline 12c executives, management, and staff The results of the COI disclosures are reported to the Audit & Compliance Committee and
Houston Methodist Hospital Board of Directors, including the actions being taken to protect the integrity of decision-making Inaddition, disclosure results are also communicated to management and to affected committee chairs to promote transparencyand to ensure that actions are taken and restrictions are imposed where appropriate Conflicted individuals may not vote orexert self-serving influence on the disclosed matter
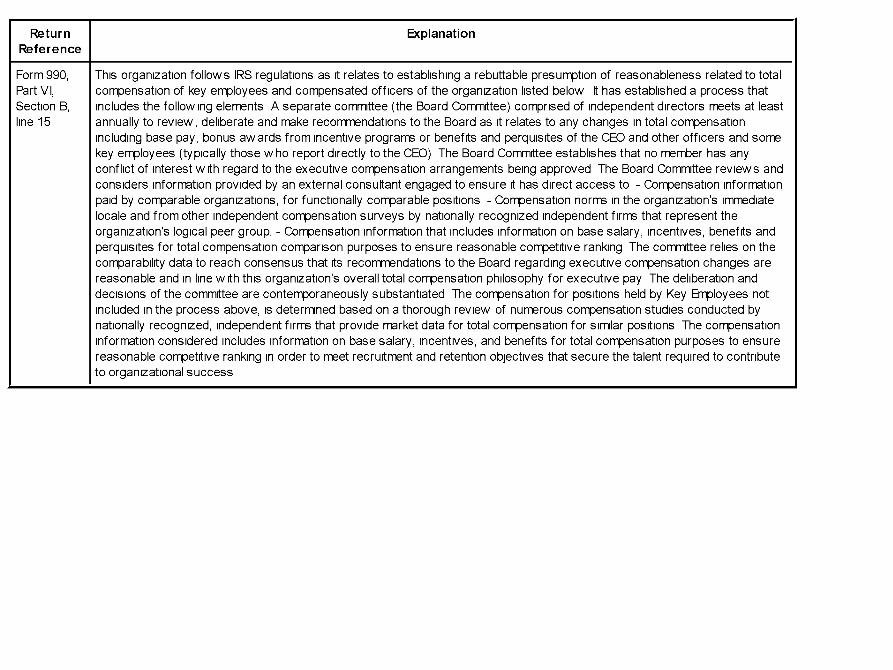
ReturnReference
Explanation
Form 990, This organization follows IRS regulations as it relates to establishing a rebuttable presumption of reasonableness related to totalPart VI, compensation of key employees and compensated officers of the organization listed below It has established a process thatSection B, includes the following elements A separate committee (the Board Committee) comprised of independent directors meets at leastline 15 annually to review, deliberate and make recommendations to the Board as it relates to any changes in total compensation
including base pay, bonus awards from incentive programs or benefits and perquisites of the CEO and other officers and somekey employees (typically those who report directly to the CEO) The Board Committee establishes that no member has anyconflict of interest with regard to the executive compensation arrangements being approved The Board Committee reviews andconsiders information provided by an external consultant engaged to ensure it has direct access to - Compensation informationpaid by comparable organizations, for functionally comparable positions - Compensation norms in the organization's immediatelocale and from other independent compensation surveys by nationally recognized independent firms that represent theorganization's logical peer group, - Compensation information that includes information on base salary, incentives, benefits andperquisites for total compensation comparison purposes to ensure reasonable competitive ranking The committee relies on thecomparability data to reach consensus that its recommendations to the Board regarding executive compensation changes arereasonable and in line with this organization's overall total compensation philosophy for executive pay The deliberation anddecisions of the committee are contemporaneously substantiated The compensation for positions held by Key Employees notincluded in the process above, is determined based on a thorough review of numerous compensation studies conducted bynationally recognized, independent firms that provide market data for total compensation for similar positions The compensationinformation considered includes information on base salary, incentives, and benefits for total compensation purposes to ensurereasonable competitive ranking in order to meet recruitment and retention objectives that secure the talent required to contributeto organizational success
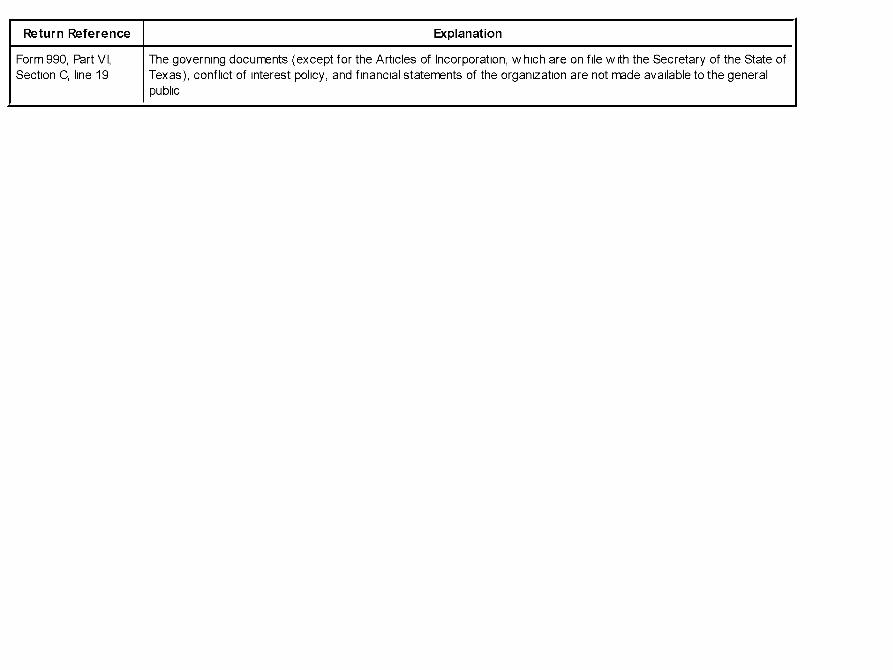
Return Reference Explanation
Form 990, Part VI, The governing documents (except for the Articles of Incorporation, which are on file w ith the Secretary of the State ofSection C, line 19 Texas), conflict of interest policy, and financial statements of the organization are not made available to the general
public
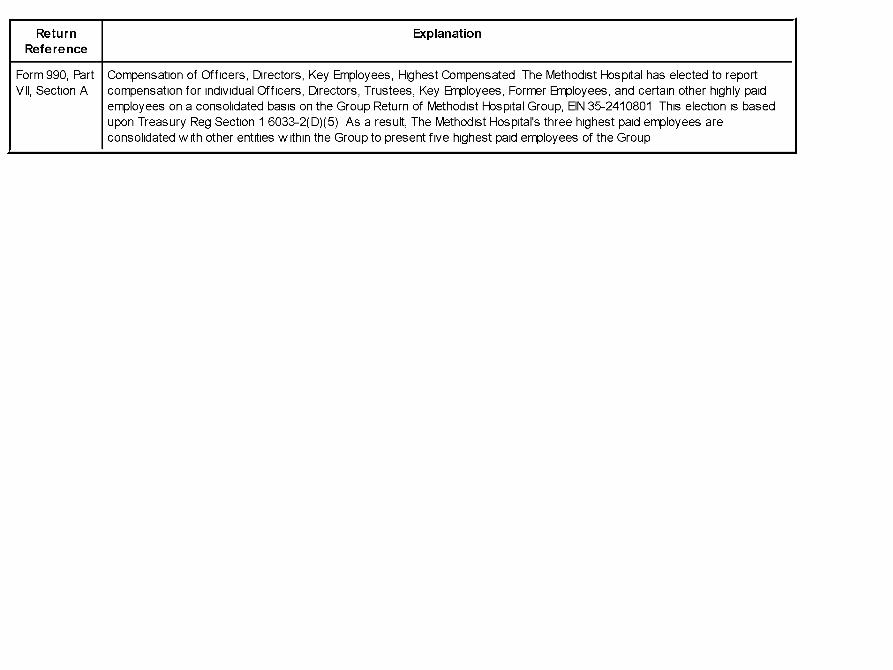
ReturnReference
Explanation
Form 990, Part Compensation of Officers, Directors, Key Employees, Highest Compensated The Methodist Hospital has elected to reportVII, Section A compensation for individual Officers, Directors, Trustees, Key Employees, Former Employees, and certain other highly paid
employees on a consolidated basis on the Group Return of Methodist Hospital Group, EIN 35-2410801 This election is basedupon Treasury Reg Section 1 6033-2(D)(5) As a result, The Methodist Hospital's three highest paid employees areconsolidated with other entities within the Group to present five highest paid employees of the Group
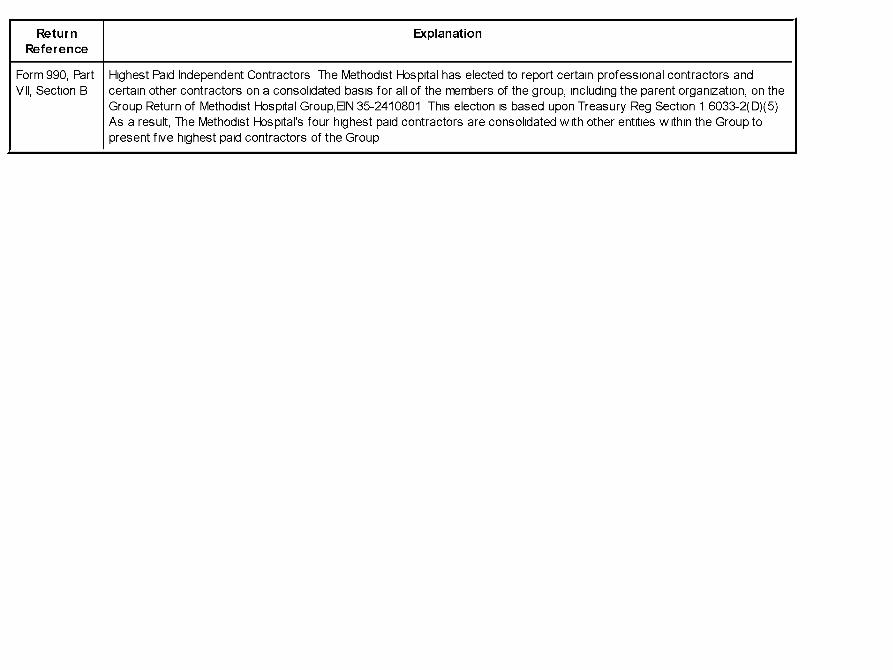
ReturnReference
Explanation
Form 990, Part Highest Paid Independent Contractors The Methodist Hospital has elected to report certain professional contractors andVII, Section B certain other contractors on a consolidated basis for all of the members of the group, including the parent organization, on the
Group Return of Methodist Hospital Group,EIN 35-2410801 This election is based upon Treasury Reg Section 1 6033-2(D)(5)As a result, The Methodist Hospital's four highest paid contractors are consolidated with other entities within the Group topresent five highest paid contractors of the Group
Return Reference Explanation
Form 990, Part XI, line 9 Transfer from Houston Methodist Hospital Foundation 975,684 Transfer to other Entity 7,977,032
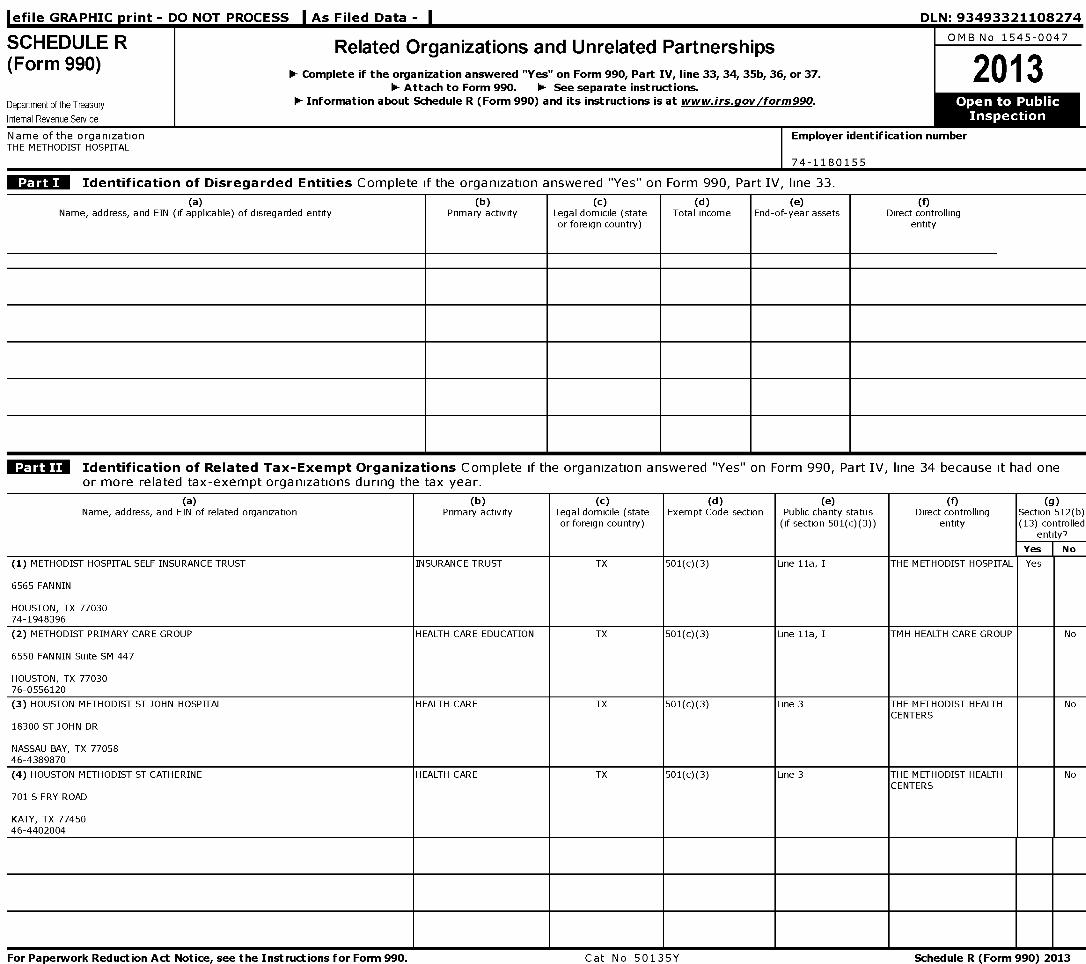
l efile GRAPHIC p rint - DO NOT PROCESS
SCHEDULE R(Form 990)
Department of the Treasury
Internal Revenue Service
As Filed Data -
Related Organizations and Unrelated Partnerships
1- Complete if the organization answered "Yes" on Form 990, Part IV, line 33, 34, 35b, 36, or 37.1- Attach to Form 990. 1- See separate instructions.
1- Information about Schedule R (Form 990) and its instructions is at www.irs.gov/form990 .
DLN:93493321108274
OMB No 1545-0047
2013
Name of the organization Employer identification numberTHE METHODIST HOSPITAL
74-1180155
Identification of Disregarded Entities Complete if the organization answered "Yes" on Form 990, Part IV, line 33.
(a)Name, address, and EIN (if applicable) of disregarded entity
(b)Primary activity
(c)Legal domicile (stateor foreign country)
(d)Total income
(e)End-of-year assets
(f)Direct controlling
entity
Identification of Related Tax-Exempt Organizations Complete if the organization answered "Yes" on Form 990, Part IV, line 34 because it had oneor more related tax-exempt organizations during the tax year.
(a) ( b) (c) (d) (e) (f) (g)Name, address, and EIN of related organization Primary activity Legal domicile (state Exempt Code section Public charity status Direct controlling Section 512(b)
or foreign country) (if section 501(c)(3)) entity (13) controlledentity?
Yes No
(1) METHODIST HOSPITAL SELF INSURANCE TRUST INSURANCE TRUST TX 501(c)(3) Line I la, I THE METHODIST HOSPITAL Yes
6565 FANNIN
HOUSTON, TX 7703074-1948396
(2) METHODIST PRIMARY CARE GROUP HEALTH CARE EDUCATION TX 501(c)(3) Line I la, I TMH HEALTH CARE GROUP No
6550 FANNIN Suite SM 447
HOUSTON, TX 7703076-0556120
(3) HOUSTON METHODIST ST JOHN HOSPITAL HEALTH CARE TX 501(c)(3) Line 3 THE METHODIST HEALTH NoCENTERS
18300 ST JOHN DR
NASSAU BAY, TX 7705846-4389870
(4) HOUSTON METHODIST ST CATHERINE HEALTH CARE TX 501(c)(3) Line 3 THE METHODIST HEALTH NoCENTERS
701 S FRY ROAD
KATY, TX 7745046-4402004
For Paperwork Reduction Act Notice, see the Instructions for Form 990. Cat No 50135Y Schedule R (Form 990) 2013
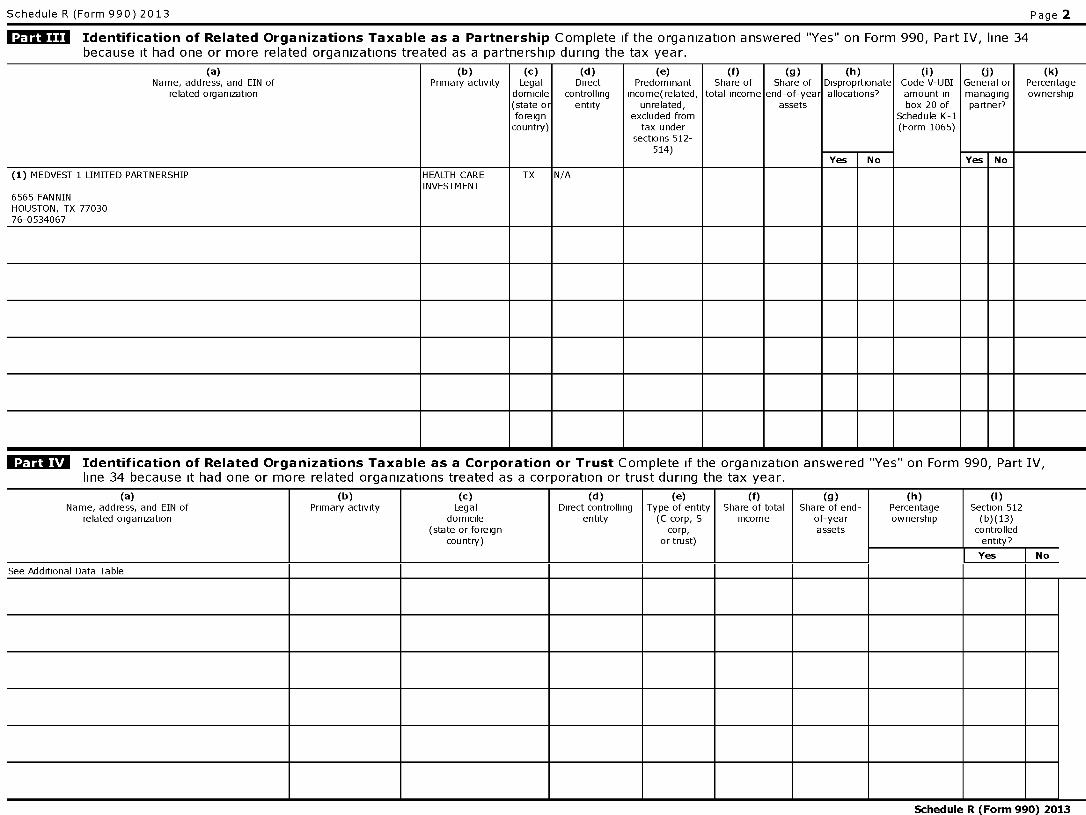
Schedule R (Form 990) 2013 Page 2
Identification of Related Organizations Taxable as a Partnership Complete if the organization answered "Yes" on Form 990, Part IV, line 34because it had one or more related organizations treated as a partnership during the tax year.
(a)Name, address, and EIN of
related organization
(b)Primary activity
(c)Legal
domicile(state orforeigncountry)
(d)Direct
controllingentity
(e)Predominant
income(related,unrelated,
excluded fromtax under
sections 512-514)
(f)Share of
total income
(g)Share of
end-of-yearassets
(h)Disproprtionateallocations?
(i)Code V-UBIamount inbox 20 of
Schedule K-1(Form 1065)
U)General ormanagingpart ner?
(k)Percentageownership
Yes No Yes No
(1) MEDVEST 1 LIMITED PARTNERSHIP
6565 FANNINHOUSTON, TX 7703076-0534067
HEALTH CAREINVESTMENT
TX N/A
Identification of Related Organizations Taxable as a Corporation or Trust Complete if the organization answered "Yes" on Form 990, Part IV,line 34 because it had one or more related organizations treated as a corporation or trust during the tax year.
(a)Name, address, and EIN of
related organization
(b)Primary activity
(c)Legal
domicile(state or foreign
country)
(d)Direct controlling
entity
(e)Type of entity
(C corp, Scorp,
or trust)
(f)Share of total
income
(g)Share of end-
of-yearassets
(h)Percentageownership
(i)Section 512
(b)(13)controlledentity?
Yes No
See Additional Data Table
Schedule R (Form 990) 2013
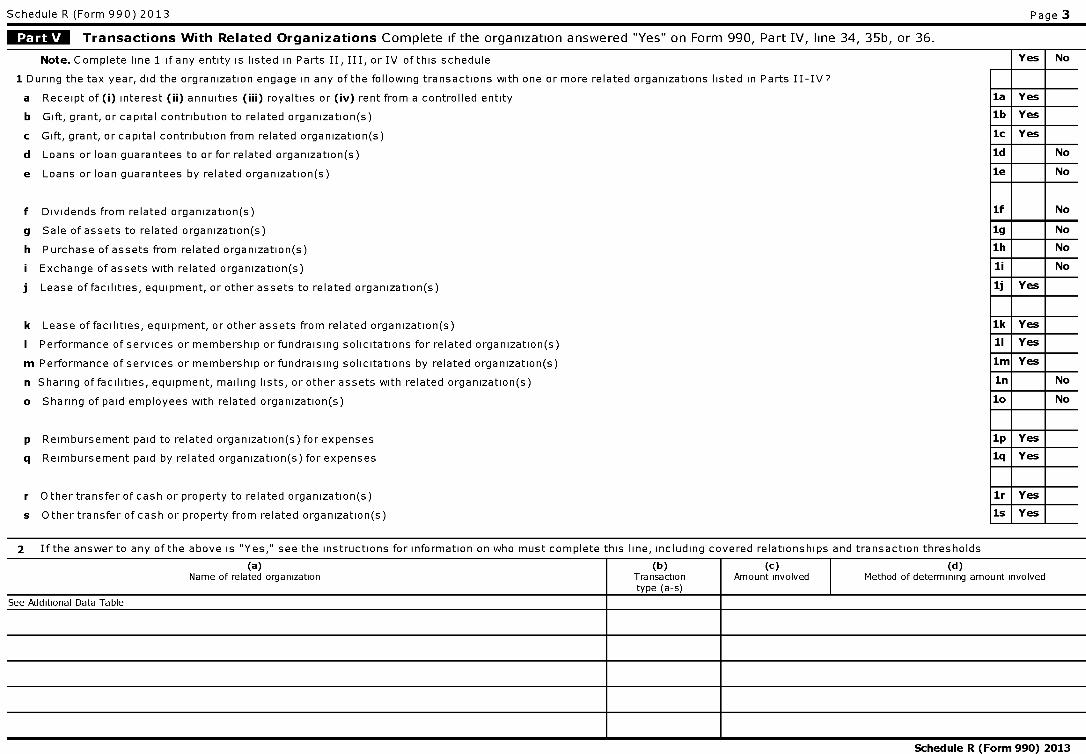
Schedule R (Form 990) 2013
ff^ Transactions With Related Organizations Complete if the organization answered "Yes" on Form 990, Part IV, line 34, 35b, or 36.
Note . Complete line 1 if any entity is listed in Parts II, III, or IV of this schedule
1 During the tax year, did the orgranization engage in any of the following transactions with one or more related organizations listed in Parts II-IV?
a Receipt of (i) interest (ii) annuities (iii) royalties or (iv) rent from a controlled entity
b Gift, grant, or capital contribution to related organization(s)
c Gift, grant, or capital contribution from related organization(s)
d Loans or loan guarantees to or for related organization(s)
e Loans or loan guarantees by related organization(s)
f Dividends from related organization(s)
g Sale of assets to related organization(s)
h Purchase of assets from related organization(s)
i Exchange of assets with related organization(s)
j Lease of facilities, equipment, or other assets to related organization(s)
k Lease of facilities, equipment, or other assets from related organization(s)
I Performance of services or membership or fundraising solicitations for related organization(s)
m Performance of services or membership or fundraising solicitations by related organization(s)
n Sharing of facilities, equipment, mailing lists, or other assets with related organization(s)
o Sharing of paid employees with related organization(s)
p Reimbursement paid to related organization(s) for expenses
q Reimbursement paid by related organization(s) for expenses
r Other transfer of cash or property to related organization(s)
s Other transfer of cash or property from related organization(s)
Page 3
YesFNo
la Yes
lb Yes
1c Yes
ld No
le No
if No
1g No
1h No
li No
1j Yes
1k Yes
11 Yes
1m Yes
in No
10 No
1p Yes
1q Yes
lr Yes
is Yes
2 If the answer to any of the above is "Yes," see the instructions for information on who must complete this line, including covered relationships and transaction thresholds
(a)Name of related organization
(b)Transactiontype (a-s)
(c)Amount involved
(d)Method of determining amount involved
See Additional Data Table
Schedule R (Form 990) 2013
Schedule R (Form 990) 2013 Page 4
Unrelated Organizations Taxable as a Partnership Complete if the organization answered "Yes" on Form 990, Part IV, line 37.Provide the following information for each entity taxed as a partnership through which the organization conducted more than five percent of its activities (measured by total assets or grossrevenue) that was not a related organization See instructions regarding exclusion for certain investment partnerships
(a)Name, address, and EIN of entity
(b)Primary activity
(c)Legal
domicile(state orforeigncountry)
(d)Predominant
income(related,unrelated,
excluded fromtax under
sections 512-
(e)Are all partners
section501(c)(3)
organizations?
(f)Share of
totalincome
(g)Share of
end-of-yearassets
(h)Disproprtionateallocations?
(i)Code V7UBIamount inbox 20
of ScheduleK-1
(Form 1065)
U)General ormanagingpart ner?
(k)Percentageownership
514)Yes No Yes No Yes No
Schedule R (Form 990) 2013
Schedule R (Form 990) 2013 Page 5
Supplemental Information
Provide additional information for responses to auestions on Schedule R (see instructions
Return Reference Explanation
Schedule R (Form 990) 201
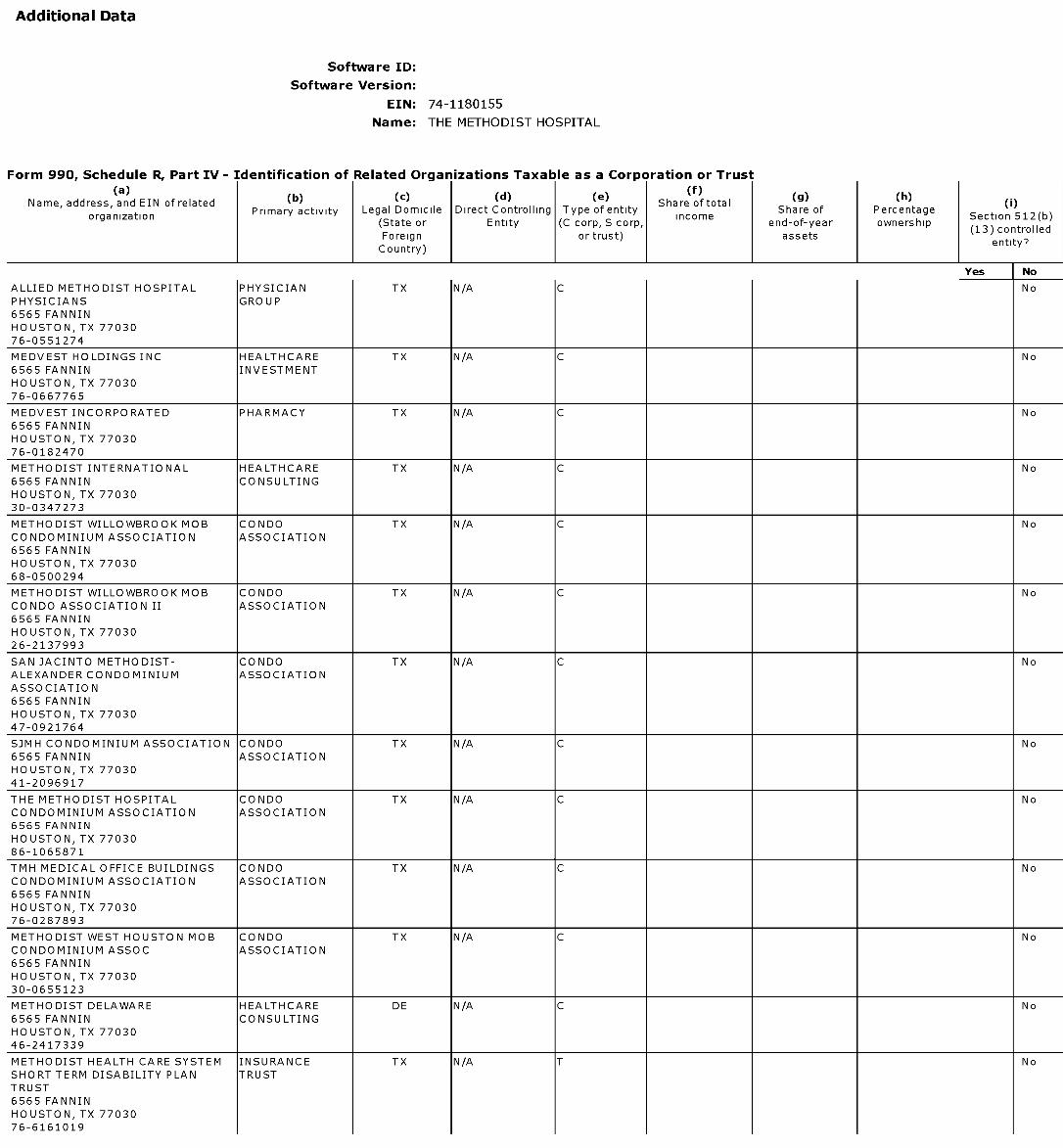
Additional Data
Software ID:
Software Version:
EIN: 74 -1180155
Name : THE METHODIST HOSPITAL
Form 990, Schedule R, Part IV - Identification of Related Organizations Taxable as a Corporation or Trust
( (b) (c) (d) (e) (9) (h)Name, address, and EIN of related Share of total 0)Primary activity Legal Domicile Direct Controlling Type of entity Share of Percentage
organization(State or Entity (C corp, S corp,
incomeend-of-year ownership
Section 512(b)(13) controlled
Foreign or trust) assetsentity?
Country)
Yes No
ALLIED METHODIST HOSPITAL PHYSICIAN TX N/A C NoPHYSICIANS GROUP6565 FANNINHOUSTON, TX 7703076-0551274
MEDVEST HOLDINGS INC HEALTHCARE TX N/A C No6565 FANNIN INVESTMENTHOUSTON, TX 7703076-0667765
MEDVEST INCORPORATED PHARMACY TX N/A C No6565 FANNINHOUSTON, TX 7703076-0182470
METHODIST INTERNATIONAL HEALTHCARE TX N/A C No6565 FANNIN CONSULTINGHOUSTON, TX 7703030-0347273
METHODIST WILLOWBROOK MOB CONDO TX N/A C NoCONDOMINIUM ASSOCIATION ASSOCIATION6565 FANNINHOUSTON, TX 7703068-0500294
METHODIST WILLOWBROOK MOB CONDO TX N/A C NoCONDO ASSOCIATION II ASSOCIATION6565 FANNINHOUSTON, TX 7703026-2137993
SAN JACINTO METHODIST- CONDO TX N/A C NoALEXANDER CONDOMINIUM ASSOCIATIONASSOCIATION6565 FANNINHOUSTON, TX 7703047-0921764
SJMH CONDOMINIUM ASSOCIATION CONDO TX N/A C No6565 FANNIN ASSOCIATIONHOUSTON, TX 7703041-2096917
THE METHODIST HOSPITAL CONDO TX N/A C NoCONDOMINIUM ASSOCIATION ASSOCIATION6565 FANNINHOUSTON, TX 7703086-1065871
TMH MEDICAL OFFICE BUILDINGS CONDO TX N/A C NoCONDOMINIUM ASSOCIATION ASSOCIATION6565 FANNINHOUSTON, TX 7703076-0287893
METHODIST WEST HOUSTON MOB CONDO TX N/A C NoCONDOMINIUM ASSOC ASSOCIATION6565 FANNINHOUSTON, TX 7703030-0655123
METHODIST DELAWARE HEALTHCARE DE N/A C No6565 FANNIN CONSULTINGHOUSTON, TX 7703046-2417339
METHODIST HEALTH CARE SYSTEM INSURANCE TX N/A T NoSHORT TERM DISABILITY PLAN TRUSTTRUST6565 FANNINHOUSTON, TX 7703076-6161019
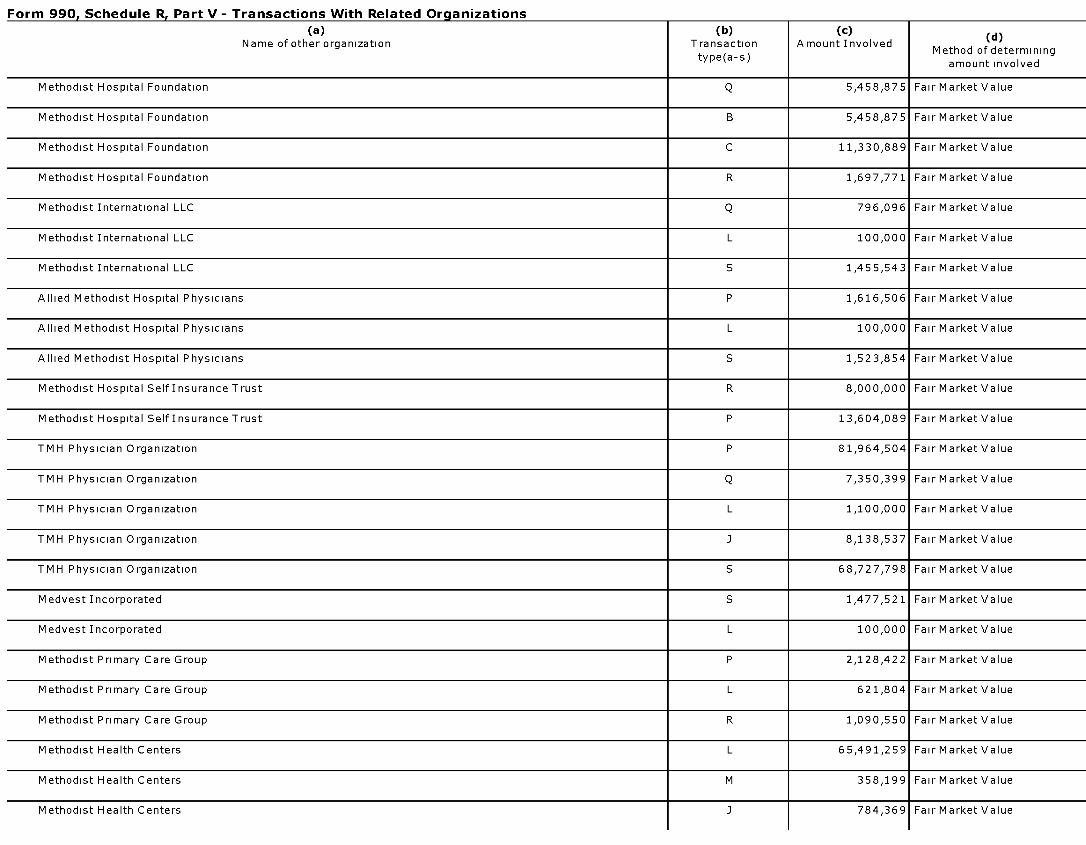
Form 990. Schedule R. Part V - Transactions With Related Organizations
(a)Name of other organization
(b)Transactiontype(a-s)
(c)Amount Involved
(d)
Method of determiningamount involved
Methodist Hospital Foundation Q 5,458,875 Fair Market Value
Methodist Hospital Foundation B 5,458,875 Fair Market Value
Methodist Hospital Foundation C 11,330,889 Fair Market Value
Methodist Hospital Foundation R 1,697,771 Fair Market Value
Methodist International LLC Q 796,096 Fair Market Value
Methodist International LLC L 100,000 Fair Market Value
Methodist International LLC S 1,455,543 Fair Market Value
Allied Methodist Hospital Physicians P 1,616,506 Fair Market Value
Allied Methodist Hospital Physicians L 100,000 Fair Market Value
Allied Methodist Hospital Physicians S 1,523,854 Fair Market Value
Methodist Hospital Self Insurance Trust R 8,000,000 Fair Market Value
Methodist Hospital Self Insurance Trust P 13,604,089 Fair Market Value
TMH Physician Organization P 81,964,504 Fair Market Value
TMH Physician Organization Q 7,350,399 Fair Market Value
TMH Physician Organization L 1,100,000 Fair Market Value
TMH Physician Organization J 8,138,537 Fair Market Value
TMH Physician Organization S 68,727,798 Fair Market Value
Medvest Incorporated S 1,477,521 Fair Market Value
Medvest Incorporated L 100,000 Fair Market Value
Methodist Primary Care Group P 2,128,422 Fair Market Value
Methodist Primary Care Group L 621,804 Fair Market Value
Methodist Primary Care Group R 1,090,550 Fair Market Value
Methodist Health Centers L 65,491,259 Fair Market Value
Methodist Health Centers M 358,199 Fair Market Value
Methodist Health Centers 3 784,369 Fair Market Value
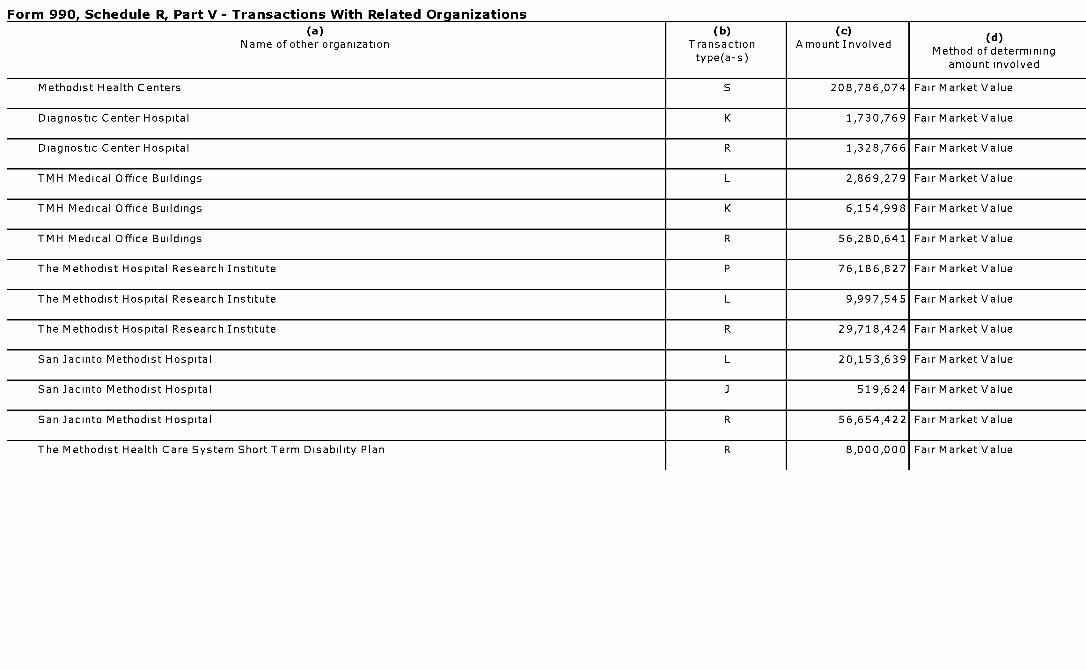
Form 990. Schedule R. Part V - Transactions With Related Organizations
(a)Name of other organization
(b)Transactiontype(a-s)
(c)Amount Involved
(d)
Method of determiningamount involved
Methodist Health Centers S 208,786,074 Fair Market Value
Diagnostic Center Hospital K 1,730,769 Fair Market Value
Diagnostic Center Hospital R 1,328,766 Fair Market Value
TMH Medical Office Buildings L 2,869,279 Fair Market Value
TMH Medical Office Buildings K 6,154,998 Fair Market Value
TMH Medical Office Buildings R 56,280,641 Fair Market Value
The Methodist Hospital Research Institute P 76,186,827 Fair Market Value
The Methodist Hospital Research Institute L 9,997,545 Fair Market Value
The Methodist Hospital Research Institute R 29,718,424 Fair Market Value
San Jacinto Methodist Hospital L 20,153,639 Fair Market Value
San Jacinto Methodist Hospital J 519,624 Fair Market Value
San Jacinto Methodist Hospital R 56,654,422 Fair Market Value
The Methodist Health Care System Short Term Disability Plan R 8,000,000 Fair Market Value

AUDITED CONSOLIDATED FINANCIAL STATEMENTS
Houston MethodistDecember 31, 2013 and 2012
AUDITED CONSOLIDATED FINANCIAL STATEMENTS
HOUSTON METHODIST
December 31, 2013 and 2012
Contents
Independent Auditors' Report 1
Consolidated Balance Sheets 3
Consolidated Statements of Operations and Changes in Net Assets 4
Consolidated Statements of Cash Flows 6
Notes to Consolidated Financial Statements 8
Deloitte .
INDEPENDENT AUDITORS' REPORT
To the Board of Directors ofHouston MethodistHouston. Texas
Deloitte & Touche LLP1111 Bagby StreetSuite 4500Houston , TX 77002-4196USA
Tel +1 713 982 2000Fax +1 713 982 2001wvwv deloitte corn
We halv e audited the accompany ing consolidated financial statements of Houston Methodist (Methodist).
which comprise the consolidated balance sheets as of December 31. 2013 and 2012. and the relatedconsolidated statements of operations and changes in net assets and cash flows for the N ears then ended.and the related notes to the consolidated financial statements
Management's Responsibility for the Consolidated Financial Statements
Management is responsible for the preparation and fair presentation of these consolidated financialstatements in accordance with accounting principles generallN accepted in the United States of America.this includes the design. implementation. and maintenance of internal control releN ant to the preparationand fair presentation of consolidated financial statements that are free from material misstatement. whetherdue to fraud or error
Auditors' Responsibility
Our responsibilit\ is to express an opinion on these consolidated financial statements based on our auditsWe conducted our audits in accordance ww ith auditing standards generally accepted in the United States ofAmerica Those standards require that ww e plan and perform the audit to obtain reasonable assurance aboutww hether the consolidated financial statements are free from material misstatement
An audit in olh es performing procedures to obtain audit eN idence about the amounts and disclosures in theconsolidated financial statements The procedures selected depend on the auditor's judgment. including the
assessment of the risks of material misstatement of the consolidated financial statements. ww hether due tofraud or error In making those risk assessments. the auditor considers internal control releN ant toMethodist's preparation and fair presentation of the consolidated financial statements in order to design
audit procedures that are appropriate in the circumstances. but not for the purpose of expressing an opinionon the effectiv eness of Methodist's internal control Accordingly. we express no such opinion An auditalso includes eN aluating the appropriateness of accounting policies used and the reasonableness ofsignificant accounting estimates made bN management. as well as eN aluating the oN erall presentation of theconsolidated financial statements
We belies e that the audit eN idence ww e haN e obtained is sufficient and appropriate to pros ide a basis for our
audit opinion
Member ofDeloitte Touche Tohmatsu Limited
Opinion
In our opinion. the consolidated financial statements referred to aboN e present fair1N. in all materialrespects. the financial position of Methodist as of December 3 1. 2013 and 2012. and the results of itsoperations and its cash flows for the N ears then ended in accordance with accounting principles general1N
accepted in the United States of America
March 31. 2014
-2-
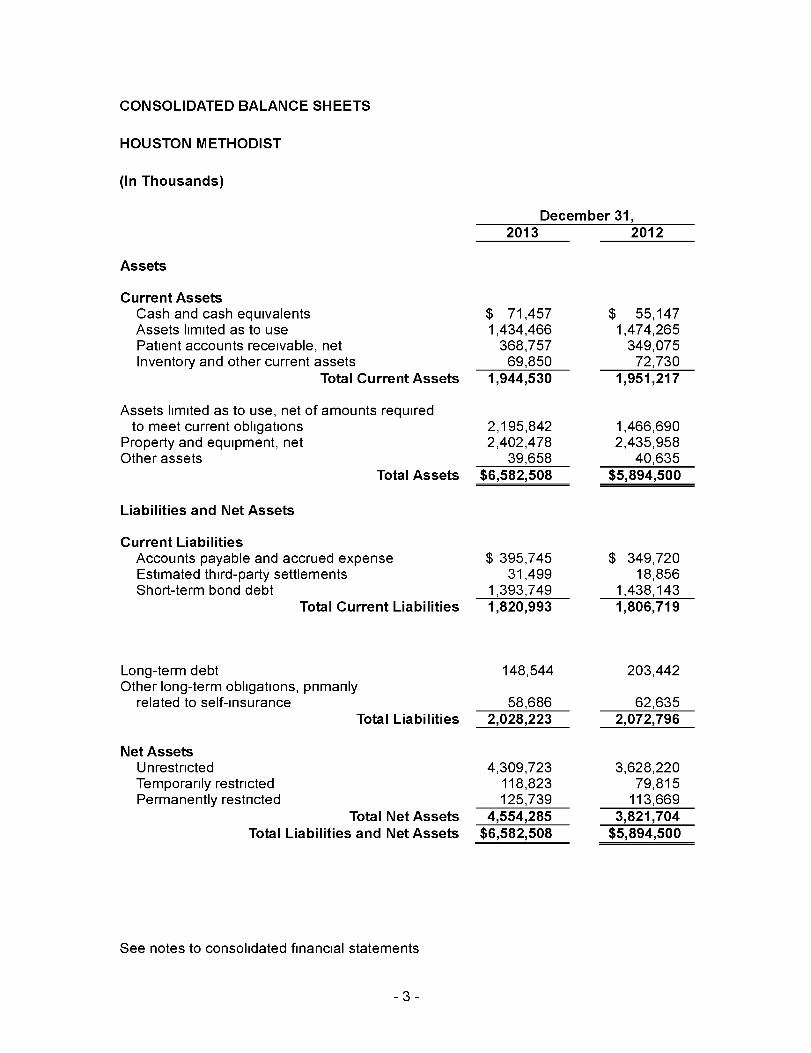
CONSOLIDATED BALANCE SHEETS
HOUSTON METHODIST
(In Thousands)
December 31,2013 2012
Assets
Current AssetsCash and cash equivalents $ 71,457 $ 55,147Assets limited as to use 1,434,466 1,474,265Patient accounts receivable, net 368,757 349,075Inventory and other current assets 69,850 72,730
Total Current Assets 1,944,530 1,951,217
Assets limited as to use, net of amounts requiredto meet current obligations 2,195,842 1,466,690
Property and equipment, net 2,402,478 2,435,958Other assets 39,658 40,635
Total Assets $6,582,508 $5,894,500
Liabilities and Net Assets
Current LiabilitiesAccounts payable and accrued expense $ 395 ,745 $ 349,720Estimated third - party settlements 31,499 18,856Short-term bond debt 1,393,749 1,438,143
Total Current Liabilities 1,820 , 993 1,806,719
Long-term debt 148,544 203,442Other long-term obligations , primarily
related to self- insurance 58,686 62,635Total Liabilities 2,028 , 223 2,072,796
Net AssetsUnrestricted 4,309,723 3,628,220Temporarily restricted 118,823 79,815Permanently restricted 125,739 113,669
Total Net Assets 4,554 , 285 3 , 821,704Total Liabilities and Net Assets $6,582,508 $5,894,500
See notes to consolidated financial statements
-3-
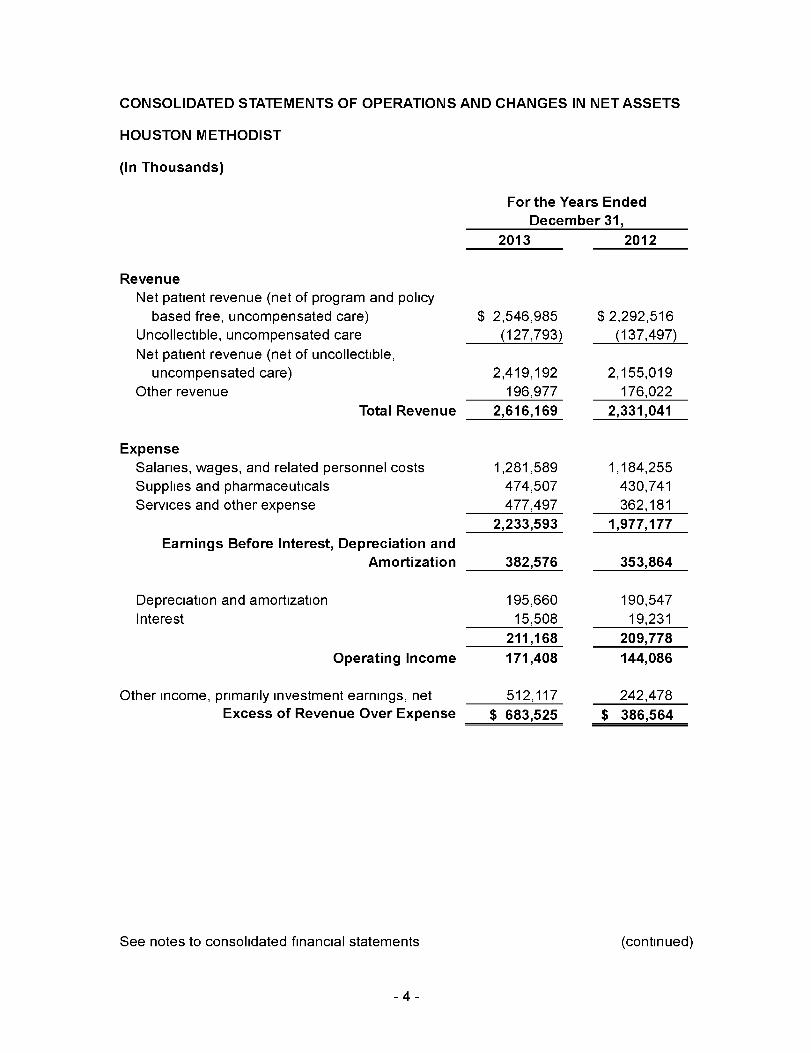
CONSOLIDATED STATEMENTS OF OPERATIONS AND CHANGES IN NET ASSETS
HOUSTON METHODIST
(In Thousands)
For the Years Ended
December 31,
2013 2012
Revenue
Net patient revenue (net of program and policy
based free, uncompensated care) $ 2,546,985 $ 2,292,516
Uncollectible, uncompensated care (127,793) (137,497)
Net patient revenue (net of uncollectible,
uncompensated care) 2,419,192 2,155,019
Other revenue 196,977 176,022
Total Revenue 2,616,169 2,331,041
ExpenseSalaries, wages, and related personnel costs 1,281,589 1,184,255
Supplies and pharmaceuticals 474,507 430,741
Services and other expense 477,497 362,181
2,233 ,593 1 ,977,177
Earnings Before Interest , Depreciation and
Amortization 382,576 353,864
Depreciation and amortization 195,660 190,547
Interest 15,508 19,231
211,168 209,778
Operating Income 171,408 144,086
Other income, primarily investment earnings, net 512,117 242,478
Excess of Revenue Over Expense $ 683 ,525 $ 386,564
See notes to consolidated financial statements (continued)
-4-
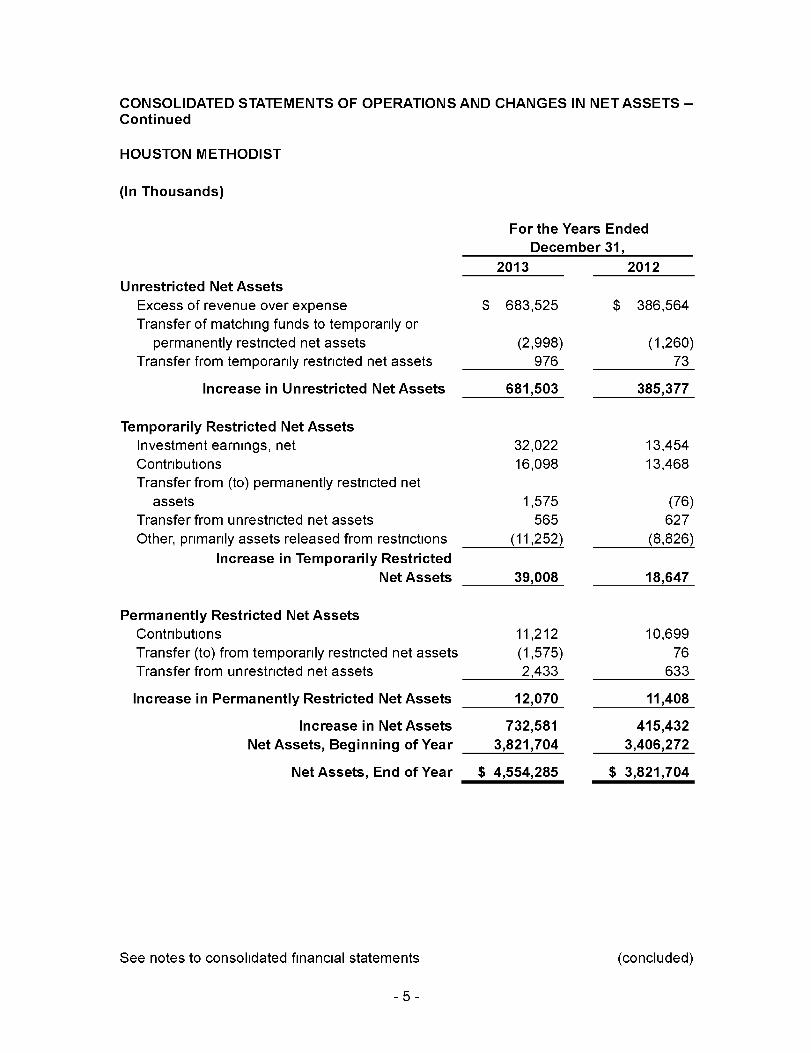
CONSOLIDATED STATEMENTS OF OPERATIONS AND CHANGES IN NET ASSETS -Continued
HOUSTON METHODIST
(In Thousands)
For the Years Ended
December 31,
2013 2012
Unrestricted Net Assets
Excess of revenue over expense $ 683,525 $ 386,564
Transfer of matching funds to temporarily or
permanently restricted net assets (2,998) (1,260)
Transfer from temporarily restricted net assets 976 73
Increase in Unrestricted Net Assets 681,503 385,377
Temporarily Restricted Net Assets
Investment earnings, net 32,022 13,454
Contributions 16,098 13,468
Transfer from (to) permanently restricted net
assets 1,575 (76)
Transfer from unrestricted net assets 565 627
Other, primarily assets released from restrictions (11,252) (8,826)
Increase in Temporarily Restricted
Net Assets 39,008 18,647
Permanently Restricted Net Assets
Contributions 11,212 10,699
Transfer (to) from temporarily restricted net assets (1,575) 76
Transfer from unrestricted net assets 2,433 633
Increase in Permanently Restricted Net Assets 12,070 11,408
Increase in Net Assets 732,581 415,432
Net Assets , Beginning of Year 3 ,821,704 3,406,272
Net Assets, End of Year $ 4,554,285 $ 3 , 821,704
See notes to consolidated financial statements (concluded)
-5-
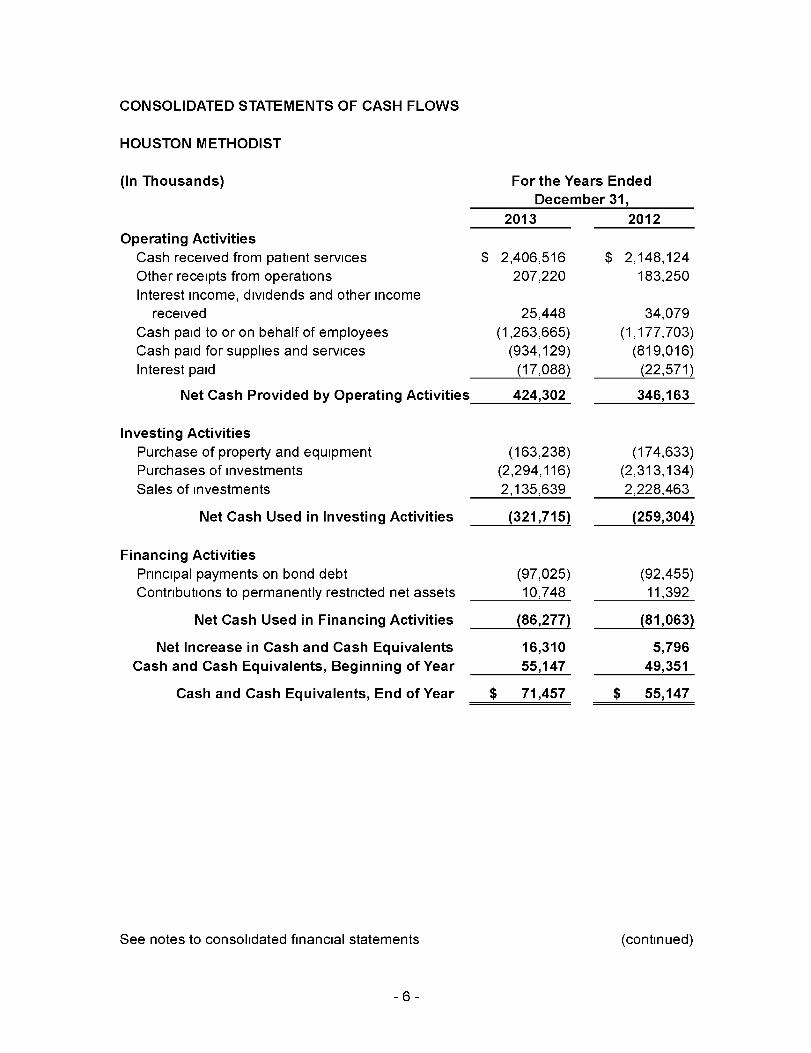
CONSOLIDATED STATEMENTS OF CASH FLOWS
HOUSTON METHODIST
(In Thousands)
Operating ActivitiesCash received from patient services
Other receipts from operations
Interest income, dividends and other income
received
Cash paid to or on behalf of employees
Cash paid for supplies and services
Interest paid
Net Cash Provided by Operating Activities
Investing Activities
Purchase of property and equipment
Purchases of investments
Sales of investments
Net Cash Used in Investing Activities
Financing Activities
Principal payments on bond debt
Contributions to permanently restricted net assets
Net Cash Used in Financing Activities
For the Years Ended
December 31,
2013 2012
$ 2,406,516
207,220
$ 2,148,124
183,250
25,448
(1,263,665)
(934,129)
(17,088)
424,302
(163,238)
(2,294,116)
2,135,639
(321,715)
(97,025)
10,748
(86,277)
Net Increase in Cash and Cash Equivalents 16,310
Cash and Cash Equivalents, Beginning of Year 55,147
Cash and Cash Equivalents, End of Year $ 71,457
See notes to consolidated financial statements
34,079
(1,177,703)
(819,016)
(22,571)
346,163
(174,633)
(2,313,134)
2,228,463
(259,304)
(92,455)
11,392
(81,063)
5,796
49,351
$ 55,147
(continued)
-6-
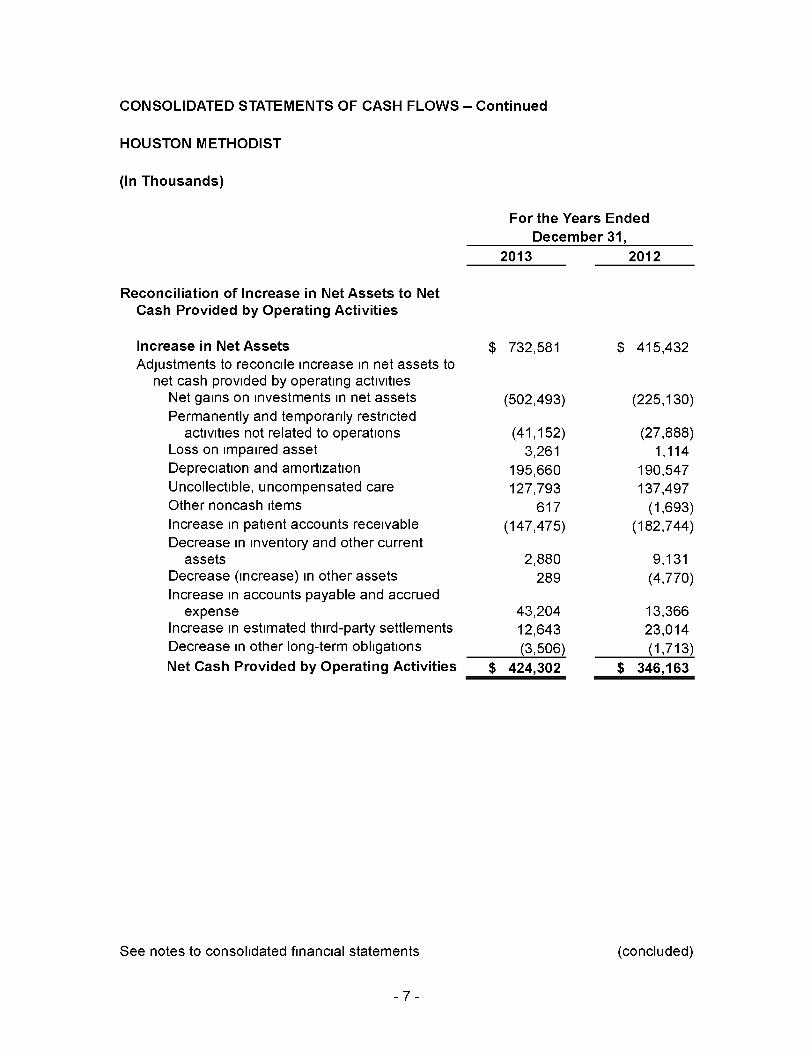
CONSOLIDATED STATEMENTS OF CASH FLOWS - Continued
HOUSTON METHODIST
(In Thousands)
For the Years Ended
December 31,
2013 2012
Reconciliation of Increase in Net Assets to NetCash Provided by Operating Activities
Increase in Net Assets $ 732,581 $ 415,432Adjustments to reconcile increase in net assets to
net cash provided by operating activitiesNet gains on investments in net assets (502,493) (225,130)Permanently and temporarily restricted
activities not related to operations (41,152) (27,888)Loss on impaired asset 3,261 1,114Depreciation and amortization 195,660 190,547Uncollectible, uncompensated care 127,793 137,497Other noncash items 617 (1,693)Increase in patient accounts receivable (147,475) (182,744)Decrease in inventory and other current
assets 2,880 9,131Decrease (increase) in other assets 289 (4,770)Increase in accounts payable and accrued
expense 43,204 13,366Increase in estimated third-party settlements 12,643 23,014Decrease in other long-term obligations (3,506) (1,713)
Net Cash Provided by Operating Activities $ 424,302 $ 346,163
See notes to consolidated financial statements (concluded)
-7-

NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODISTDecember 31, 2013 and 2012
NOTE A- MISSION AND ORGANIZATION
The mission of Houston Methodist (Methodist) is to provide high-quality, cost-effectivehealth care that delivers the best value to the people it serves in a spiritual environmentof caring in association with internationally recognized teaching and research Methodistoperates a large academic medical center hospital, a research institute, a physicianorganization, four community hospitals, and various medical office buildings in Houston,Texas, and the surrounding area
Methodist is a not-for-profit, nonmember corporation organized and existing under the
laws of the State of Texas It is exempt from federal income taxes The consolidatedfinancial statements include the accounts of Methodist and its wholly owned and/orcontrolled affiliates
NOTE B - SIGNIFICANT ACCOUNTING POLICIES
Use of Estimates - The preparation of consolidated financial statements in conformitywith accounting principles generally accepted in the United States of America requiresmanagement to make estimates and assumptions that affect the reported amounts ofassets and liabilities, disclosure of contingent assets and liabilities at the date of theconsolidated financial statements and the reported amounts of revenue and expenseduring the reporting period Actual results could differ from those estimates Significantestimates include the allowances for uncollectible accounts and contractuals, estimated
third-party settlements, self-insurance reserves and valuation of investments
Cash and Cash Equivalents - Investments with maturities of three months or lesswhen purchased are classified as cash equivalents, excluding amounts classified asassets limited as to use
Accounts Receivable - Accounts receivable are reported in the consolidated balancesheets net of an estimated allowance for uncollectible, uncompensated care of$126 3 million and $108 5 million as of December 31, 2013 and 2012, respectivelyCurrent operations are charged with a provision for uncollectible, uncompensated carebased on experience, eligibility, and any other circumstances, which may affect the abilityof patients to meet their obligations Methodist routinely obtains assignment of (or isotherwise entitled to receive) patients' benefits payable under their health insuranceprograms, plans, or policies (e g , Medicare, Medicaid, health maintenanceorganizations, and commercial insurance policies)
Patient accounts receivable are stated at net realizable value Accounts receivable arereduced by an allowance for contractual adjustments, based on expected payment ratesfrom payors under current reimbursement methodologies, and also by an allowance fordoubtful accounts In evaluating the collectibility of accounts receivable, Methodistanalyzes historical trends for each of its major payor sources of revenue to estimate anappropriate allowance for doubtful accounts and provision for uncollectible accountsManagement regularly reviews data about these major payor sources of revenue in
-8-
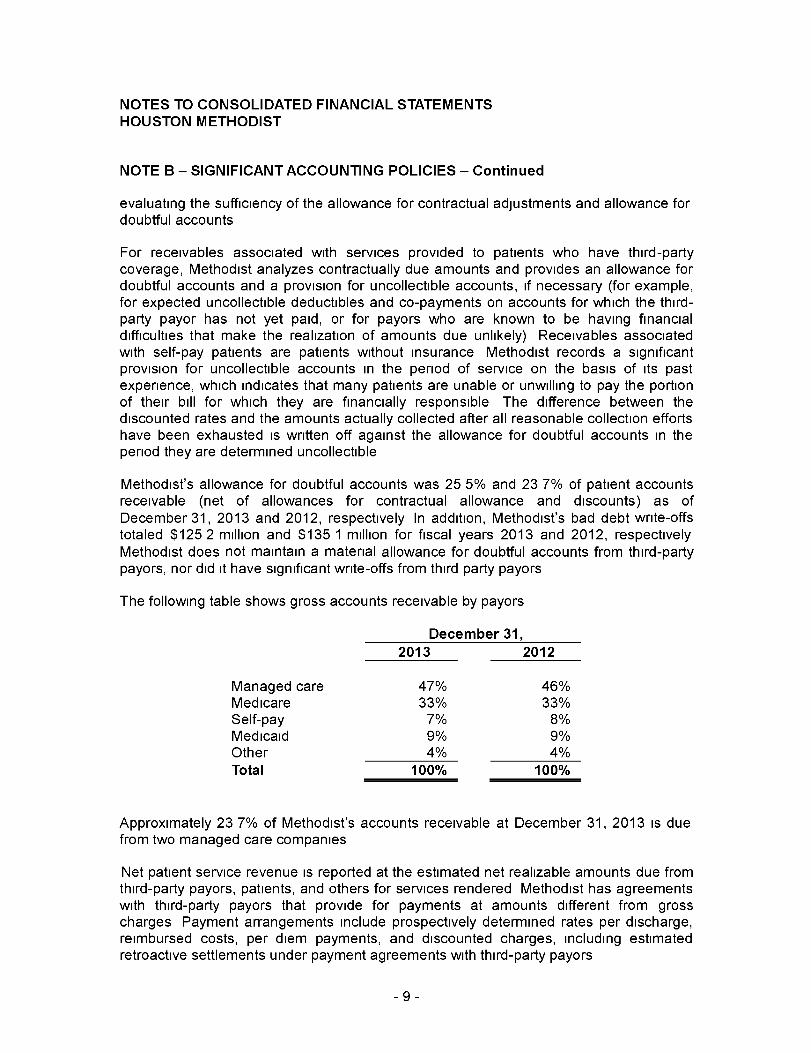
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE B - SIGNIFICANT ACCOUNTING POLICIES - Continued
evaluating the sufficiency of the allowance for contractual adjustments and allowance fordoubtful accounts
For receivables associated with services provided to patients who have third-partycoverage, Methodist analyzes contractually due amounts and provides an allowance fordoubtful accounts and a provision for uncollectible accounts, if necessary (for example,for expected uncollectible deductibles and co-payments on accounts for which the third-party payor has not yet paid, or for payors who are known to be having financialdifficulties that make the realization of amounts due unlikely) Receivables associatedwith self-pay patients are patients without insurance Methodist records a significantprovision for uncollectible accounts in the period of service on the basis of its pastexperience, which indicates that many patients are unable or unwilling to pay the portionof their bill for which they are financially responsible The difference between thediscounted rates and the amounts actually collected after all reasonable collection effortshave been exhausted is written off against the allowance for doubtful accounts in theperiod they are determined uncollectible
Methodist's allowance for doubtful accounts was 25 5% and 23 7% of patient accountsreceivable (net of allowances for contractual allowance and discounts) as ofDecember 31, 2013 and 2012, respectively In addition, Methodist's bad debt write-offstotaled $125 2 million and $135 1 million for fiscal years 2013 and 2012, respectivelyMethodist does not maintain a material allowance for doubtful accounts from third-partypayors, nor did it have significant write-offs from third party payors
The following table shows gross accounts receivable by payors
December 31,
2013 2012
Managed care 47% 46%Medicare 33% 33%Self-pay 7% 8%Medicaid 9% 9%Other 4% 4%
Total 100% 100%
Approximately 23 7% of Methodist' s accounts receivable at December 31, 2013 is duefrom two managed care companies
Net patient service revenue is reported at the estimated net realizable amounts due fromthird-party payors, patients, and others for services rendered Methodist has agreementswith third-party payors that provide for payments at amounts different from grosscharges Payment arrangements include prospectively determined rates per discharge,reimbursed costs, per diem payments, and discounted charges, including estimatedretroactive settlements under payment agreements with third-party payors
-9-
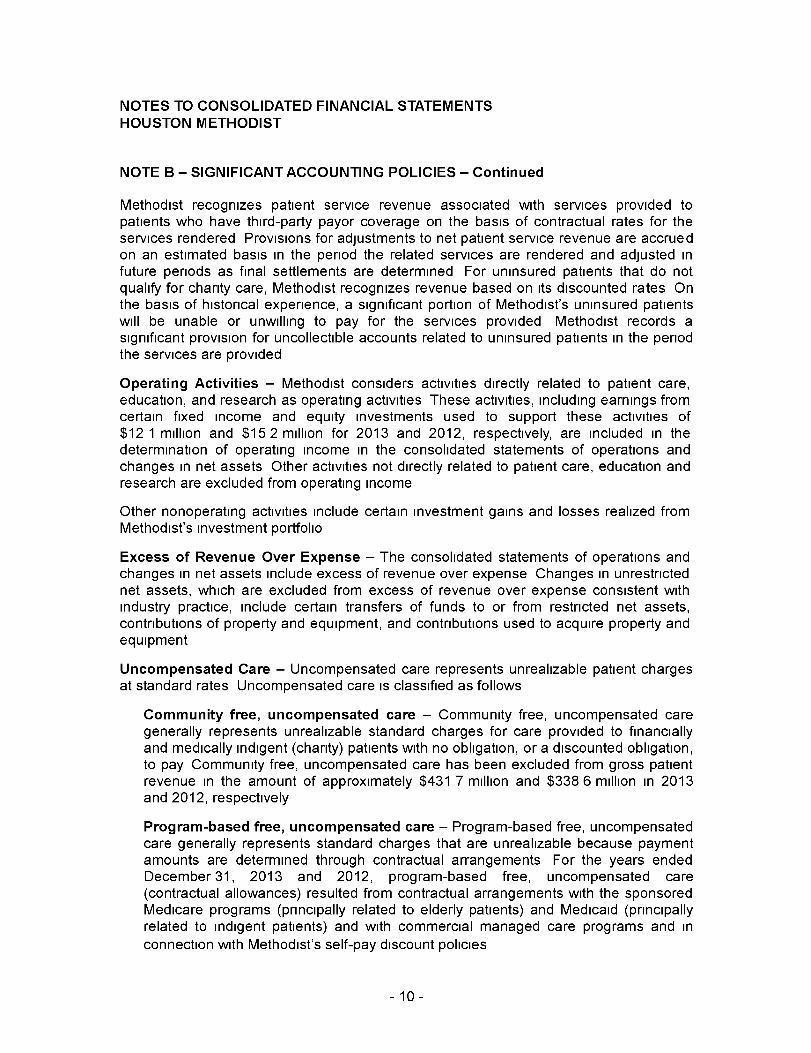
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE B - SIGNIFICANT ACCOUNTING POLICIES - Continued
Methodist recognizes patient service revenue associated with services provided topatients who have third-party payor coverage on the basis of contractual rates for theservices rendered Provisions for adjustments to net patient service revenue are accruedon an estimated basis in the period the related services are rendered and adjusted infuture periods as final settlements are determined For uninsured patients that do notqualify for charity care, Methodist recognizes revenue based on its discounted rates Onthe basis of historical experience, a significant portion of Methodist's uninsured patientswill be unable or unwilling to pay for the services provided Methodist records asignificant provision for uncollectible accounts related to uninsured patients in the periodthe services are provided
Operating Activities - Methodist considers activities directly related to patient care,education, and research as operating activities These activities, including earnings fromcertain fixed income and equity investments used to support these activities of$12 1 million and $15 2 million for 2013 and 2012, respectively, are included in thedetermination of operating income in the consolidated statements of operations andchanges in net assets Other activities not directly related to patient care, education andresearch are excluded from operating income
Other nonoperating activities include certain investment gains and losses realized fromMethodist's investment portfolio
Excess of Revenue Over Expense - The consolidated statements of operations andchanges in net assets include excess of revenue over expense Changes in unrestrictednet assets, which are excluded from excess of revenue over expense consistent withindustry practice, include certain transfers of funds to or from restricted net assets,contributions of property and equipment, and contributions used to acquire property andequipment
Uncompensated Care - Uncompensated care represents unrealizable patient chargesat standard rates Uncompensated care is classified as follows
Community free , uncompensated care - Community free, uncompensated caregenerally represents unrealizable standard charges for care provided to financiallyand medically indigent (charity) patients with no obligation, or a discounted obligation,to pay Community free, uncompensated care has been excluded from gross patientrevenue in the amount of approximately $431 7 million and $338 6 million in 2013and 2012, respectively
Program -based free, uncompensated care - Program-based free, uncompensatedcare generally represents standard charges that are unrealizable because paymentamounts are determined through contractual arrangements For the years endedDecember 31, 2013 and 2012, program-based free, uncompensated care(contractual allowances) resulted from contractual arrangements with the sponsoredMedicare programs (principally related to elderly patients) and Medicaid (principallyrelated to indigent patients) and with commercial managed care programs and in
connection with Methodist's self-pay discount policies
-10-
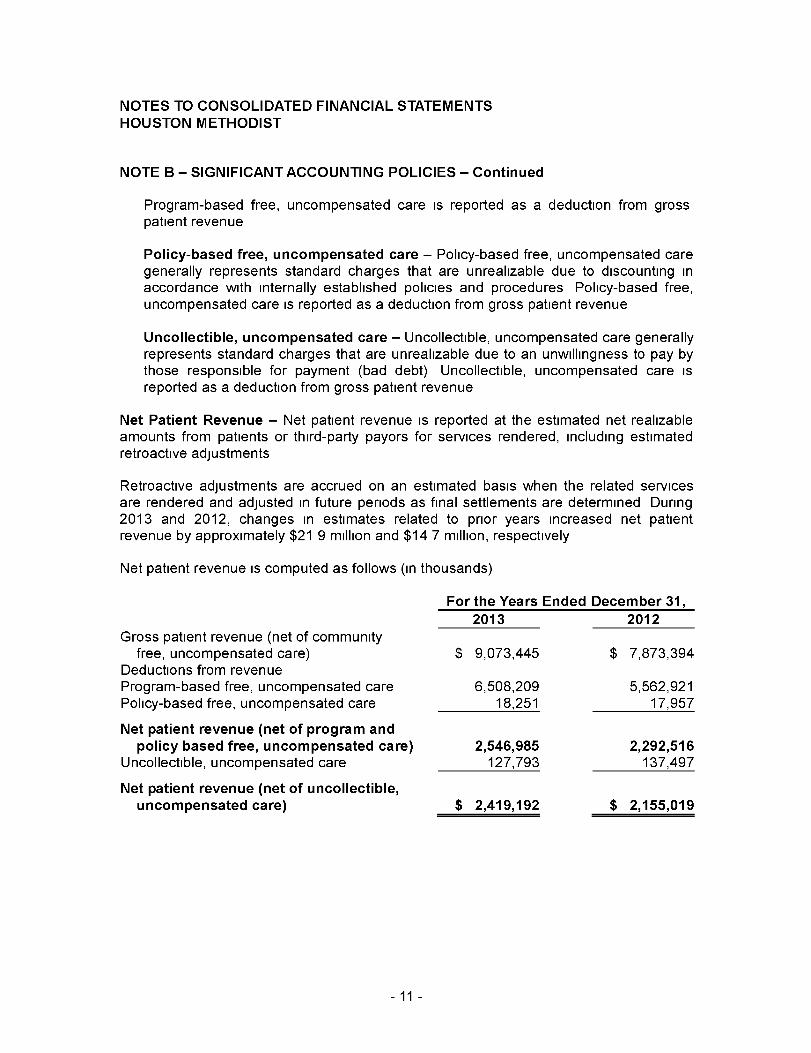
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE B - SIGNIFICANT ACCOUNTING POLICIES - Continued
Program-based free, uncompensated care is reported as a deduction from grosspatient revenue
Policy- based free , uncompensated care - Policy-based free, uncompensated caregenerally represents standard charges that are unrealizable due to discounting inaccordance with internally established policies and procedures Policy-based free,uncompensated care is reported as a deduction from gross patient revenue
Uncollectible, uncompensated care - Uncollectible, uncompensated care generallyrepresents standard charges that are unrealizable due to an unwillingness to pay bythose responsible for payment (bad debt) Uncollectible, uncompensated care isreported as a deduction from gross patient revenue
Net Patient Revenue - Net patient revenue is reported at the estimated net realizableamounts from patients or third-party payors for services rendered, including estimatedretroactive adjustments
Retroactive adjustments are accrued on an estimated basis when the related servicesare rendered and adjusted in future periods as final settlements are determined During2013 and 2012, changes in estimates related to prior years increased net patientrevenue by approximately $21 9 million and $14 7 million, respectively
Net patient revenue is computed as follows (in thousands)
Gross patient revenue (net of community
For the Years Ended December 31,
2013 2012
free, uncompensated care) $ 9,073,445Deductions from revenueProgram-based free, uncompensated care 6,508,209Policy-based free, uncompensated care 18,251
Net patient revenue ( net of program andpolicy based free , uncompensated care) 2,546,985
Uncollectible, uncompensated care 127,793
Net patient revenue ( net of uncollectible,uncompensated care) $ 2,419,192
$ 7,873,394
5,562,92117.957
2,292,516137,497
$ 2,155, 019
- 11 -
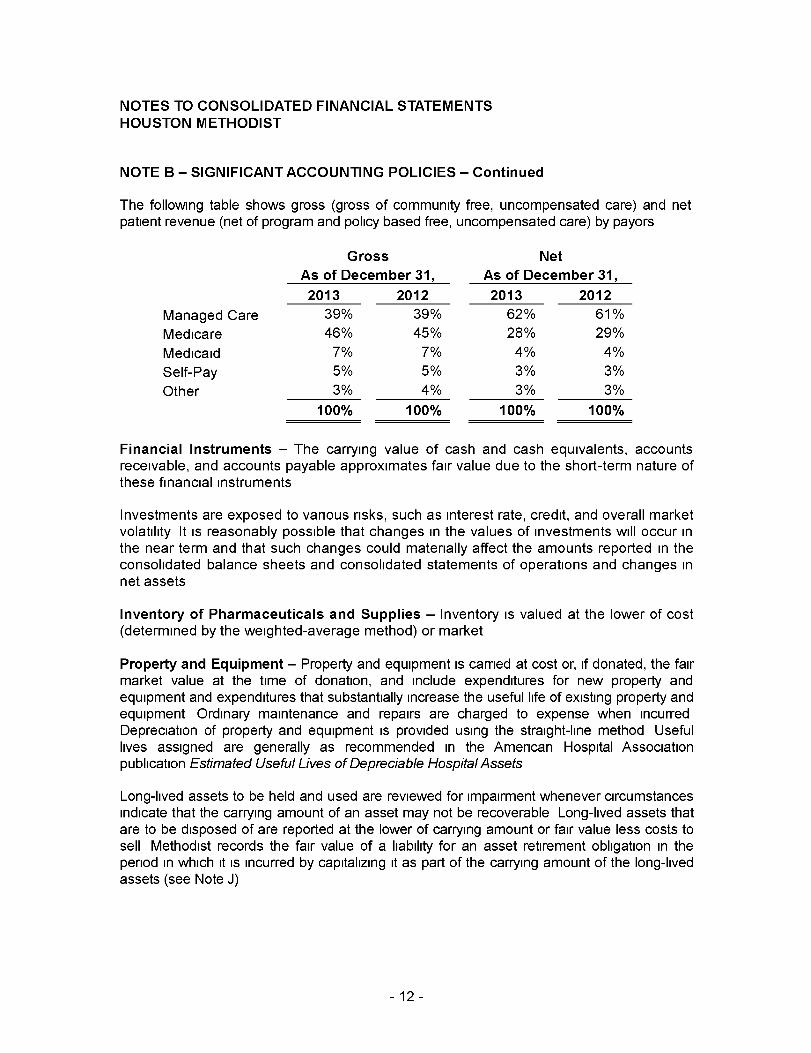
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE B - SIGNIFICANT ACCOUNTING POLICIES - Continued
The following table shows gross (gross of community free, uncompensated care) and netpatient revenue (net of program and policy based free, uncompensated care) by payors
Gross Net
As of December 31, As of December 31,
2013 2012 2013 2012
Managed Care 39% 39% 62% 61%
Medicare 46% 45% 28% 29%
Medicaid 7% 7% 4% 4%
Self-Pay 5% 5% 3% 3%
Other 3% 4% 3% 3%
100% 100% 100% 100%
Financial Instruments - The carrying value of cash and cash equivalents, accountsreceivable, and accounts payable approximates fair value due to the short-term nature ofthese financial instruments
Investments are exposed to various risks, such as interest rate, credit, and overall marketvolatility It is reasonably possible that changes in the values of investments will occur inthe near term and that such changes could materially affect the amounts reported in theconsolidated balance sheets and consolidated statements of operations and changes innet assets
Inventory of Pharmaceuticals and Supplies - Inventory is valued at the lower of cost(determined by the weighted-average method) or market
Property and Equipment - Property and equipment is carried at cost or, if donated, the fairmarket value at the time of donation, and include expenditures for new property andequipment and expenditures that substantially increase the useful life of existing property andequipment Ordinary maintenance and repairs are charged to expense when incurredDepreciation of property and equipment is provided using the straight-line method Usefullives assigned are generally as recommended in the American Hospital Associationpublication Estimated Useful Lives of Depreciable Hospital Assets
Long-lived assets to be held and used are reviewed for impairment whenever circumstancesindicate that the carrying amount of an asset may not be recoverable Long-lived assets thatare to be disposed of are reported at the lower of carrying amount or fair value less costs tosell Methodist records the fair value of a liability for an asset retirement obligation in theperiod in which it is incurred by capitalizing it as part of the carrying amount of the long-livedassets (see Note J)
-12-
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE B - SIGNIFICANT ACCOUNTING POLICIES - Continued
Other Assets - Other assets consist primarily of goodwill ($23 4 million) and deferredfinancing costs Methodist tests for impairment of goodwill on an annual basis, or morefrequently if indicators of impairment are present Methodist did not record any goodwillimpairments for the years ended 2013 or 2012 Premiums collected in connection withthe issuance of fixed rate bonds, the cost of issuing fixed rate bonds, and premiums paidto insure variable rate demand bonds are capitalized and amortized over the term of therespective bond issue
Paid Time Off (Vacation , Holiday and Sick Leave ) Benefits - The cost of employees'paid time off benefits is recorded at the time benefits are earned
Professional and General Liability Self-Insurance - Methodist has a separate,revocable self-insurance trust for which funding has been actuarially determined for thepayment of professional and general liability losses, related expenses, and the cost ofadministering the trust
The assets of the revocable trust are reported in assets limited as to use in theconsolidated balance sheets Income from the trust assets are reported in other revenuein the consolidated statements of operations and changes in net assets Professionaland general liability losses and administrative costs are reported in services and otherexpense in the consolidated statements of operations and changes in net assets
Unconditional Pledges and Unrestricted Contributions - Unrestricted contributionsand pledges are recorded as other income (losses), primarily investment earnings(losses), net in the consolidated statements of operations and changes in net assets inthe period of the contribution or pledge commitment Donor-restricted pledges andcontributions are recorded as temporarily or permanently restricted net assets when thepledge or contribution is made Pledges receivable are reported at their net presentvalue, discounted at rates ranging from 1 0% to 3 4% As of December 31, 2013 and2012, the amount of the discount was $5 9 million and $10 9 million, respectively
Temporarily and Permanently Restricted Net Assets - Temporarily restricted netassets are those limited as to use by donors to a specific time period or purposePermanently restricted net assets are those that have been restricted by donors to bemaintained in perpetuity Temporarily restricted net assets released from restriction arerecorded as increases in unrestricted net assets when costs are incurred for theirrestricted purposes Temporarily and permanently restricted net assets are primarilyrestricted for patient care, research and education
-13-
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE B - SIGNIFICANT ACCOUNTING POLICIES - Continued
Methodist's permanently restricted net assets consist of individual endowment accountsUnless otherwise directed by the donor, gifts received for endowment accounts areinvested consistent with Methodist's board-approved investment policy Unless otherwisedirected by the donor, Methodist has a policy of annually appropriating a certainpercentage of each endowment account, which is then available to be spent consistentwith donor intent In order to preserve the real value of a donor's gift and to sustainfunding consistent with donor intent, the annual appropriation rate is set to strike areasonable balance between long-term objectives of preserving and growing eachendowment fund for the future and providing stable, year-to-year appropriation amountsFrom time to time, the fair value of assets associated with a permanently restrictedendowment account may fall below the applicable endowments gift amount(s) due tounfavorable investment returns
As of December 31, 2013, the fair value of assets associated with permanently restrictedendowment accounts did not fall below the applicable endowment gift amount(s) for anyof the endowments As of December 31, 2013, the endowment accounts included intemporarily restricted net assets totaled $46 7 million This amount was increased in2013 by investment gains totaling $28 3 million and reduced by expenditures consistentwith donor intent totaling $2 5 million
As of December 31, 2012, the fair value of assets associated with permanently restrictedendowment accounts that fell below the applicable endowment gift amount(s) totaled$139,000 As of December 31, 2012, the endowment accounts included in temporarilyrestricted net assets totaled $21 5 million This amount was increased in 2012 byinvestment gains totaling $11 7 million and reduced by expenditures consistent withdonor intent totaling $1 9 million
Income Taxes - Methodist and most of its affiliates are 501(c)(3) organizations generallyexempt from income taxes As a result of its unrelated business taxable income activityand taxable subsidiary operations, there are net operating losses of approximately$127 5 million that are available to offset net taxable income through 2025 Substantiallyall of the related deferred tax assets of $44 2 million have been offset by a valuationallowance The income tax provision and related tax assets and liabilities are immaterialMethodist did not recognize any adjustments related to uncertain tax positions as ofDecember 31, 2013
-14-
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE B - SIGNIFICANT ACCOUNTING POLICIES - Continued
Subsequent Events - Methodist has evaluated subsequent events through March 31,
2014, which is the date the consolidated financial statements were issued Effective
February 1, 2014, Methodist acquired a controlling interest in Christus St John Hospital
in the Clear Lake area south of Houston and Methodist acquired the operating assets of
Christus St Catherine Hospital in west Houston The real property and improvements of
the Christus St Catherine Hospital are now held in a joint operating company with
Methodist holding a controlling interest The majority interest in the joint operating
companies is owned by Methodist and the minority interest is owned by Christus St
John Hospital will be operated as a Methodist acute care hospital and St Catherine
Hospital will be repurposed as a long term care facility
NOTE C - SERVICES PROVIDED TO THE COMMUNITY
Under legislation passed in the state of Texas, not-for-profit hospitals are required toprovide a mandated amount of "Charity Care" and "Community Benefits," as defined bythe legislation Methodist was in compliance with the legislation, providing an estimatedtotal of $744 1 million and $703 8 million in combined Charity Care and CommunityBenefits based on estimated unreimbursed costs for the years ended December 31,2013 and 2012, respectively, which exceeded the mandated amounts
Through its controlled corporations, Methodist has a program to address specific healthcare needs that are not being met in the local community Estimated charity careunreimbursed cost under this program for the years ended December 31, 2013 and2012, totaled $174 7 million and $177 9 million, respectively The method to estimatecharity patient care costs is based on the cost to charge ratio, as defined by state ofTexas statutory legislation, and then multiplying that ratio by the gross patient chargesassociated with providing care to financially or medically indigent patients, reduced byany payments received
Methodist contributed to the advancement of medical science through direct financialsupport of research and medical education during 2013 and 2012 Approximately$115 3 million and $110 3 million in 2013 and 2012, respectively, was incurred in directand indirect expense for Methodist's internally funded research and educationalprograms, support of its multiyear primary affiliations with Weill Medical College atCornell University and New York-Presbyterian Hospital, and its support of other affiliates,including Baylor College of Medicine Methodist also provided financial support foreducation in several allied health professions
-15-
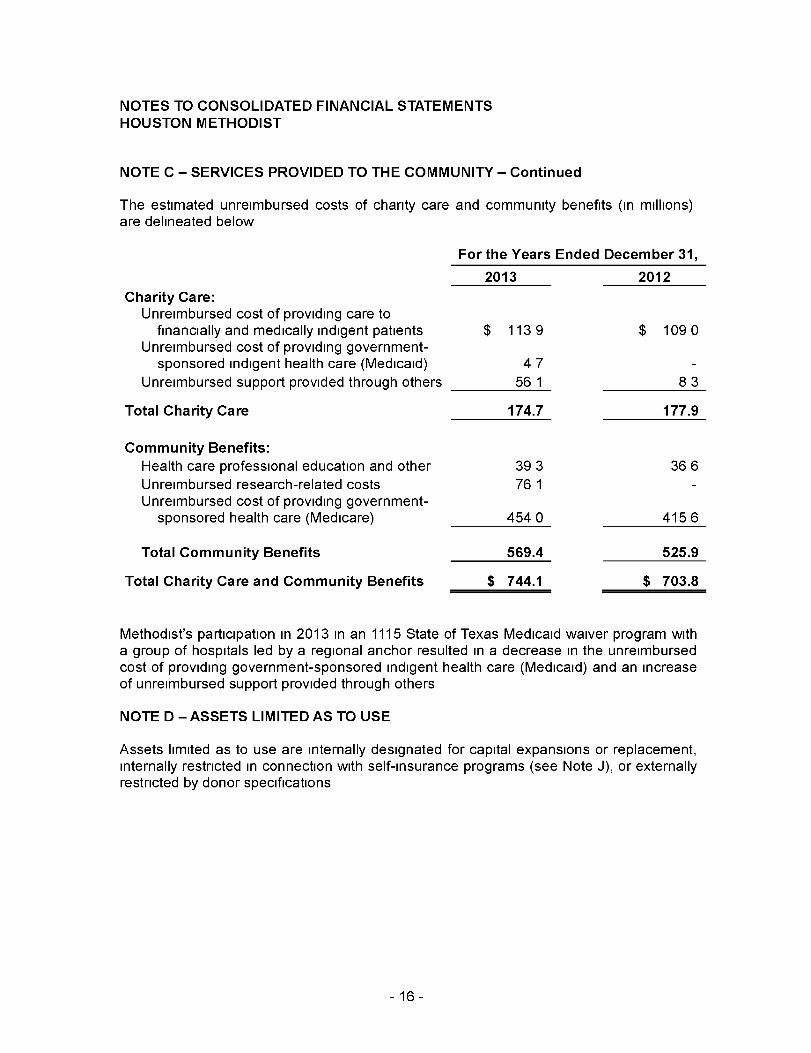
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE C - SERVICES PROVIDED TO THE COMMUNITY - Continued
The estimated unreimbursed costs of charity care and community benefits (in millions)are delineated below
For the Years Ended December 31,
2013 2012
Charity Care:Unreimbursed cost of providing care to
financially and medically indigent patients $ 1139 $ 109 0Unreimbursed cost of providing government-
sponsored indigent health care (Medicaid) 47 -
Unreimbursed support provided through others 56 1 83
Total Charity Care 174.7 177.9
Community Benefits:
Health care professional education and other 39 3 36 6
Unreimbursed research-related costs 76 1 -Unreimbursed cost of providing government-
sponsored health care (Medicare) 454 0 415 6
Total Community Benefits 569.4 525.9
Total Charity Care and Community Benefits $ 744.1 $ 703.8
Methodist's participation in 2013 in an 1115 State of Texas Medicaid waiver program witha group of hospitals led by a regional anchor resulted in a decrease in the unreimbursedcost of providing government-sponsored indigent health care (Medicaid) and an increaseof unreimbursed support provided through others
NOTE D - ASSETS LIMITED AS TO USE
Assets limited as to use are internally designated for capital expansions or replacement,internally restricted in connection with self-insurance programs (see Note J), or externallyrestricted by donor specifications
-16-
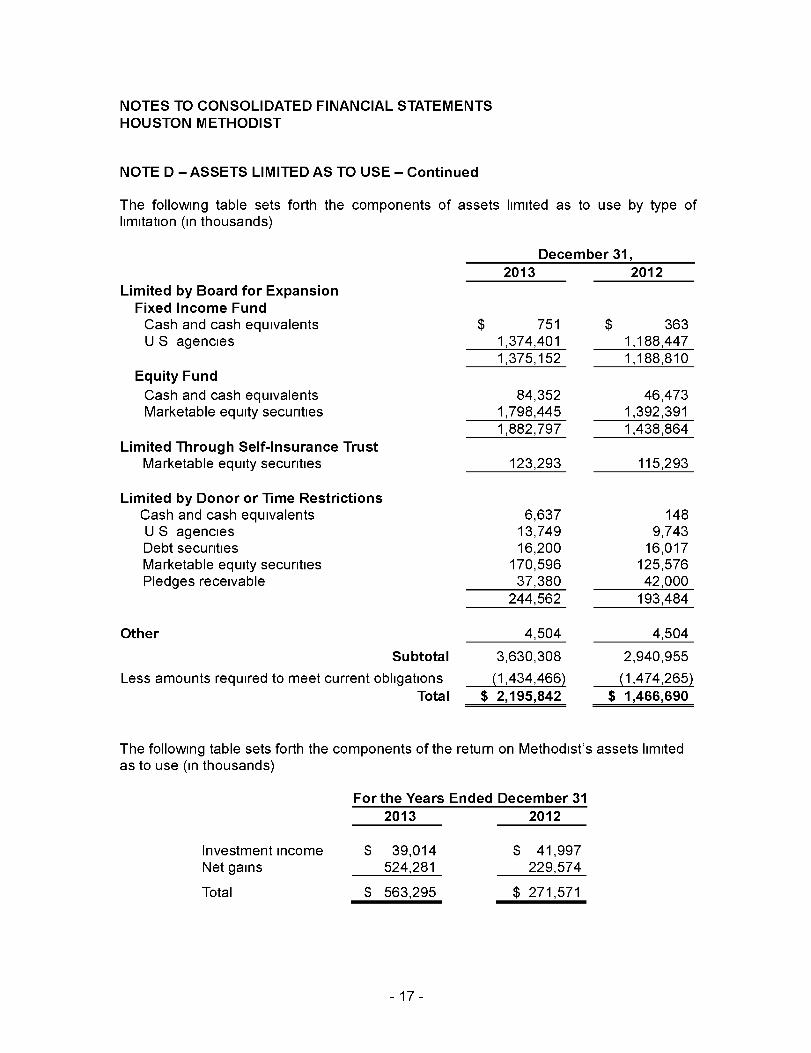
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE D - ASSETS LIMITED AS TO USE - Continued
The following table sets forth the components of assets limited as to use by type oflimitation (in thousands)
Limited by Board for ExpansionFixed Income FundCash and cash equivalentsUS agencies
Equity Fund
Cash and cash equivalentsMarketable equity securities
Limited Through Self-Insurance TrustMarketable equity securities
Limited by Donor or Time RestrictionsCash and cash equivalentsUS agenciesDebt securitiesMarketable equity securitiesPledges receivable
Other
Subtotal
Less amounts required to meet current obligations
Total
December 31,
2013 2012
$ 7511,374,4011.375.152
$ 3631,188,4471.188.810
84,3521,798,445
46,4731,392,391
1,882,797 1,438,864
123,293 115,293
6,63713,74916,200
170,59637,380
244,562
1489,743
16,017125,57642,000
193,484
4,504
3,630,308
(1,434,466)
$ 2,195,842
4,504
2,940,955
(1,474,265)
$ 1,466,690
The following table sets forth the components of the return on Methodist's assets limitedas to use (in thousands)
For the Years Ended December 312n1s
Investment incomeNet gains
Total
$ 39,014524,281
$ 563,295
2012
$ 41,997229,574
$ 271,571
-17-
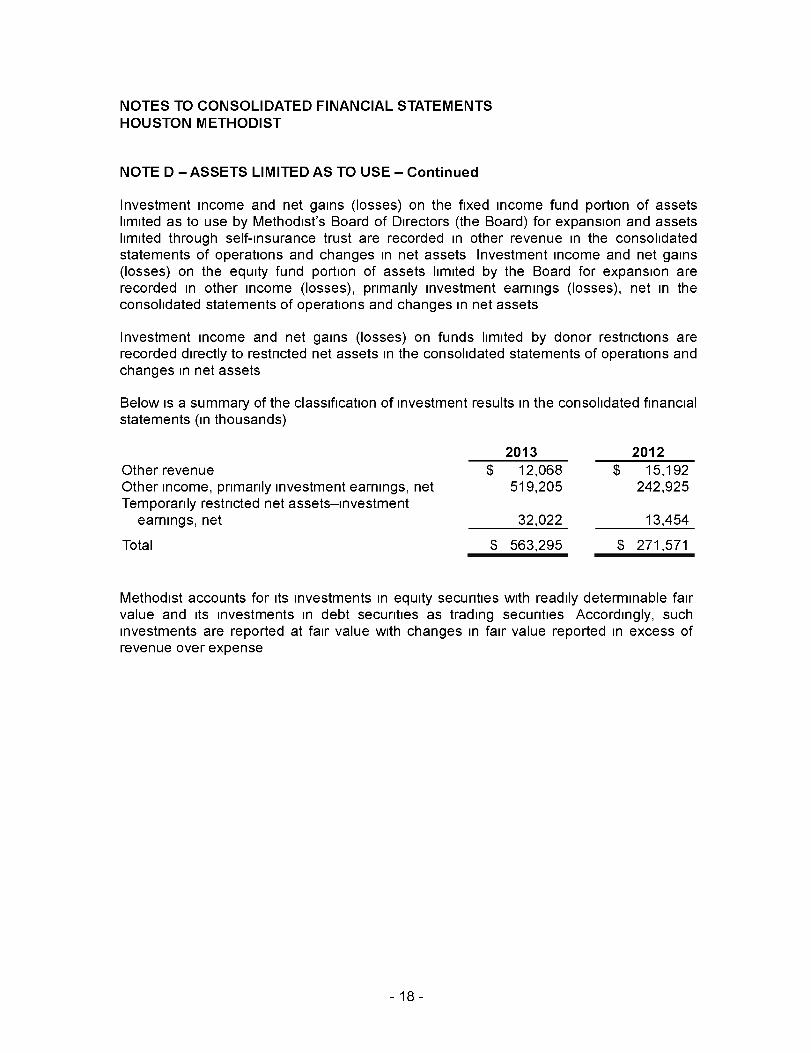
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE D - ASSETS LIMITED AS TO USE - Continued
Investment income and net gains (losses) on the fixed income fund portion of assetslimited as to use by Methodist's Board of Directors (the Board) for expansion and assetslimited through self-insurance trust are recorded in other revenue in the consolidatedstatements of operations and changes in net assets Investment income and net gains(losses) on the equity fund portion of assets limited by the Board for expansion arerecorded in other income (losses), primarily investment earnings (losses), net in theconsolidated statements of operations and changes in net assets
Investment income and net gains (losses) on funds limited by donor restrictions arerecorded directly to restricted net assets in the consolidated statements of operations andchanges in net assets
Below is a summary of the classification of investment results in the consolidated financialstatements (in thousands)
Other revenueOther income, primarily investment earnings, netTemporarily restricted net assets-investment
earnings, net
Total
2013 2012
$ 12,068519,205
32,022
$ 563,295
$ 15,192242,925
13,454
$ 271,571
Methodist accounts for its investments in equity securities with readily determinable fairvalue and its investments in debt securities as trading securities Accordingly, suchinvestments are reported at fair value with changes in fair value reported in excess ofrevenue over expense
-18-
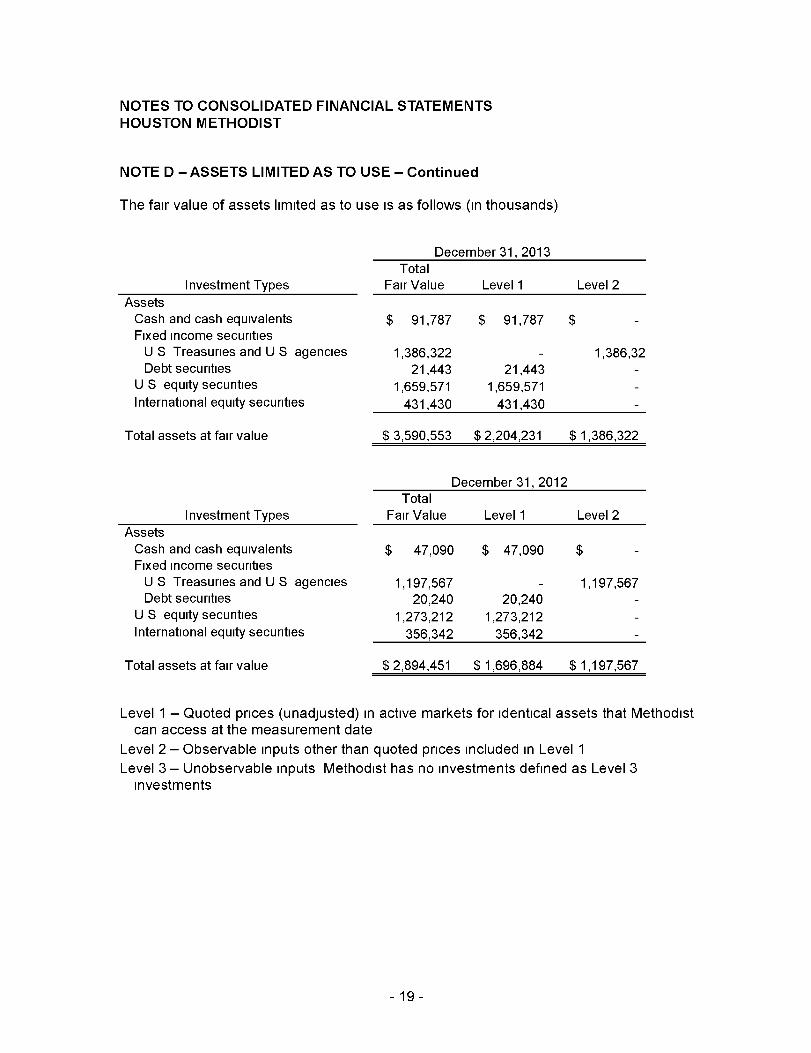
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE D - ASSETS LIMITED AS TO USE - Continued
The fair value of assets limited as to use is as follows (in thousands)
December 31, 2013Total
Investment Types Fair Value Level 1 Level 2
AssetsCash and cash equivalentsFixed income securitiesU S Treasuries and U S agenciesDebt securities
U S equity securities
International equity securities
$ 91,787 $ 91,787 $ -
1,386,322 - 1,386,3221,443 21,443 -
1,659,571 1,659,571 -
431,430 431,430 -
Total assets at fair value
Investment TypesAssetsCash and cash equivalentsFixed income securitiesU S Treasuries and U S agenciesDebt securities
U S equity securitiesInternational equity securities
Total assets at fair value
$ 3,590,553 $ 2,204,231 $ 1,386,322
December 31, 2012Total
Fair Value Level 1 Level 2
$ 47,090 $ 47,090 $ -
1,197,567 - 1,197,56720,240 20,240 -
1,273,212 1,273,212 -356,342 356,342 -
$ 2,894,451 $ 1,696,884 $ 1,197,567
Level 1 - Quoted prices (unadjusted) in active markets for identical assets that Methodistcan access at the measurement date
Level 2 - Observable inputs other than quoted prices included in Level 1
Level 3 - Unobservable inputs Methodist has no investments defined as Level 3investments
-19-
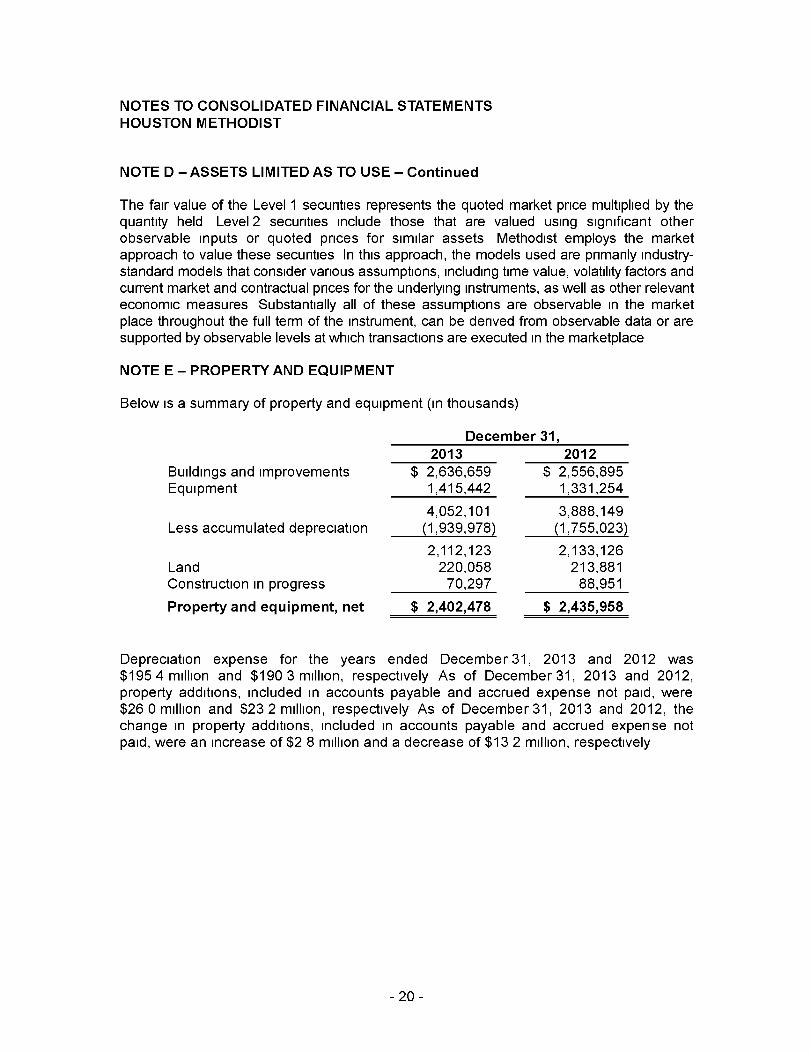
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE D - ASSETS LIMITED AS TO USE - Continued
The fair value of the Level 1 securities represents the quoted market price multiplied by thequantity held Level 2 securities include those that are valued using significant otherobservable inputs or quoted prices for similar assets Methodist employs the marketapproach to value these securities In this approach, the models used are primarily industry-standard models that consider various assumptions, including time value, volatility factors andcurrent market and contractual prices for the underlying instruments, as well as other relevanteconomic measures Substantially all of these assumptions are observable in the marketplace throughout the full term of the instrument, can be derived from observable data or aresupported by observable levels at which transactions are executed in the marketplace
NOTE E - PROPERTY AND EQUIPMENT
Below is a summary of property and equipment (in thousands)
December 31,
2013 2012
Buildings and improvements $ 2,636,659Equipment 1,415,442
Less accumulated depreciation
LandConstruction in progress
Property and equipment, net
4,052,101(1,939,978)
2,112,123220,05870,297
$ 2,402,478
$ 2,556,8951,331,254
3,888,149(1,755,023)
2,133,126213,88188,951
$ 2,435,958
Depreciation expense for the years ended December3l, 2013 and 2012 was
$1954 million and $1903 million, respectively As of December 31, 2013 and 2012,property additions, included in accounts payable and accrued expense not paid, were$26 0 million and $23 2 million, respectively As of December 31, 2013 and 2012, thechange in property additions, included in accounts payable and accrued expense notpaid, were an increase of $2 8 million and a decrease of $13 2 million, respectively
-20-
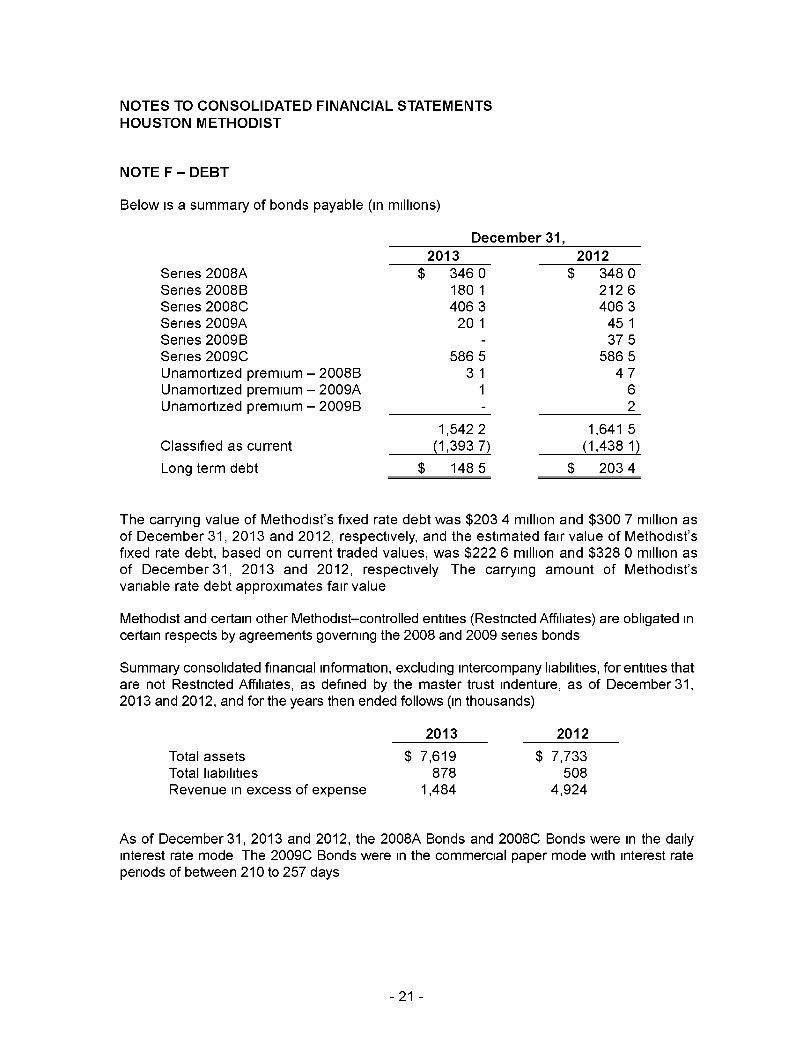
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE F - DEBT
Below is a summary of bonds payable (in millions)
Series 2008ASeries 2008BSeries 2008CSeries 2009ASeries 2009BSeries 2009CUnamortized premium - 2008BUnamortized premium - 2009AUnamortized premium - 2009B
Classified as current
December 31,
2013 2012
$ 3460 $ 34801801 21264063 4063201 451
- 3755865 586531 47
1 6- 2
1,5422 1,641 5(1,3937) (1,438 1)
Long term debt $ 1485 $ 2034
The carrying value of Methodist's fixed rate debt was $203 4 million and $300 7 million asof December 31, 2013 and 2012, respectively, and the estimated fair value of Methodist'sfixed rate debt, based on current traded values, was $222 6 million and $328 0 million asof December 31, 2013 and 2012, respectively The carrying amount of Methodist'svariable rate debt approximates fair value
Methodist and certain other Methodist-controlled entities (Restricted Affiliates) are obligated incertain respects by agreements governing the 2008 and 2009 series bonds
Summary consolidated financial information, excluding intercompany liabilities, for entities thatare not Restricted Affiliates, as defined by the master trust indenture, as of December 31,2013 and 2012, and for the years then ended follows (in thousands)
2013 2012
Total assets $ 7,619 $ 7,733Total liabilities 878 508Revenue in excess of expense 1 ,484 4,924
As of December 31, 2013 and 2012, the 2008A Bonds and 2008C Bonds were in the dailyinterest rate mode The 2009C Bonds were in the commercial paper mode with interest rateperiods of between 210 to 257 days
-21 -
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE F - DEBT - Continued
While bonds are in the daily rate or commercial paper mode, they may be tendered bybondholders ("put") on business days for full payment of principal and interest TheSeries 2008B Bonds were issued on August 21, 2008 in the fixed rate serial mode
To provide assurance of its ability to purchase tendered 2008A Bonds, 2008C Bonds and2009C Bonds, Methodist intends to maintain unencumbered cash, cash equivalents,immediately saleable fixed income obligations (e g , high-grade, fixed incomeinvestments), readily saleable equity investments and committed bank lines or similarbank facilities with a market value at least equal to the maximum aggregate purchaseprice that could become due on all bonds in a daily rate mode, weekly rate mode, orcommercial paper rate mode Methodist had a three year $100 million revolving line ofcredit with a large commercial bank, which was not drawn and expired on October 13,2013
Consistent with the put feature of Methodist's 2008A Bonds, 2008C Bonds and 2009CBonds , these bonds have been classified as current liabilities The 2008B Bonds and2009A Bonds have been classified as long-term liabilities, other than amounts due in2014, which have been classified as current liabilities , as indicated below
The 2008A Bonds, 2008C Bonds and 2009C Bonds may be converted to fixed rateobligations or other variable rate modes (e g , weekly, commercial paper) at the option ofMethodist
The Restricted Affiliates have covenanted to abide by guidelines regarding repayment,financial performance and organizational changes defined in agreements and indenturesrelated to the 2008 and 2009 series bonds Management believes Methodist is incompliance with debt covenants
The 2008A Bonds were issued in two subseries of $175 million each and have a finalmaturity date of December 1, 2041 Principal payments on the two subseries of 2008ABonds of $2 0 million began in 2012, with remaining principal payments scheduled from2013 through 2041 The 2008B Bonds were issued in seven series ranging from$31 3 million to $38 5 million Principal payment on the first 2008B Bond series of$31 3 million began in 2012, with payments on the other six series scheduled from 2013through 2018
-22-
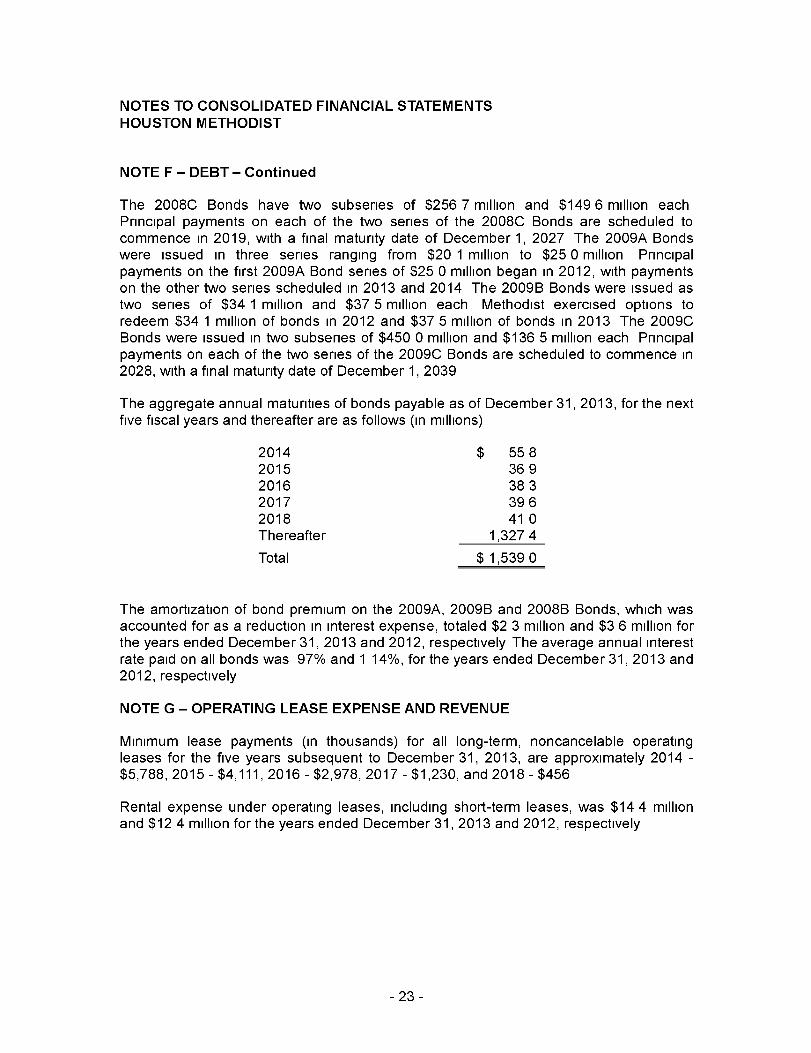
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE F - DEBT - Continued
The 2008C Bonds have two subseries of $256 7 million and $149 6 million eachPrincipal payments on each of the two series of the 2008C Bonds are scheduled tocommence in 2019, with a final maturity date of December 1, 2027 The 2009A Bondswere issued in three series ranging from $20 1 million to $25 0 million Principalpayments on the first 2009A Bond series of $25 0 million began in 2012, with paymentson the other two series scheduled in 2013 and 2014 The 2009B Bonds were issued astwo series of $34 1 million and $37 5 million each Methodist exercised options toredeem $34 1 million of bonds in 2012 and $37 5 million of bonds in 2013 The 2009CBonds were issued in two subseries of $450 0 million and $136 5 million each Principalpayments on each of the two series of the 2009C Bonds are scheduled to commence in2028, with a final maturity date of December 1, 2039
The aggregate annual maturities of bonds payable as of December 31, 2013 , for the nextfive fiscal years and thereafter are as follows ( in millions)
2014 $ 5582015 3692016 3832017 3962018 41 0Thereafter 1,3274
Total $1,5390
The amortization of bond premium on the 2009A, 2009B and 2008B Bonds, which wasaccounted for as a reduction in interest expense, totaled $2 3 million and $3 6 million forthe years ended December 31, 2013 and 2012, respectively The average annual interestrate paid on all bonds was 97% and 1 14%, for the years ended December 31, 2013 and2012, respectively
NOTE G - OPERATING LEASE EXPENSE AND REVENUE
Minimum lease payments (in thousands) for all long-term, noncancelable operatingleases for the five years subsequent to December 31, 2013, are approximately 2014 -$5,788, 2015 - $4,111, 2016 - $2,978, 2017 - $1,230, and 2018 - $456
Rental expense under operating leases, including short-term leases, was $14 4 millionand $12 4 million for the years ended December 31, 2013 and 2012, respectively
-23-
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE G - OPERATING LEASE EXPENSE AND REVENUE - Continued
Rental revenue (in thousands) for operating leases for the five years subsequent toDecember 31, 2013, is approximately 2014 - $27,403, 2015 - $20,683, 2016 - $14,143,2017 - $9,590, 2018 - $4,716, and years after 2018 - $2,545 This revenue primarilyrelates to the leasing of medical office buildings (MOBs) space to physician practices atmarket rates The approximate carrying value of the MOBs is $203 8 million withaccumulated depreciation of $146 4 million as of December 31, 2013
NOTE H - RETIREMENT PLANS
Most Methodist corporations participate in a noncontributory, defined contribution planThe amounts incurred during 2013 and 2012 totaled $31 0 million and $29 6 million,respectively, and are included in salaries, wages, and related personnel costs in theconsolidated statements of operations and changes in net assets
Additionally, Methodist has a tax-sheltered annuity plan that includes an employer matchcalculated at 50% of an employee's contribution up to 4% of pay The contributions forthe employer match on the tax-sheltered annuity plan totaled $12 7 million and$11 8 million during 2013 and 2012, respectively These amounts are included insalaries, wages, and related personnel costs in the consolidated statements ofoperations and changes in net assets
Certain executives participate in a Supplemental Executive Retirement Plan Theexpense associated with this plan was $1 5 million and $1 1 million during 2013 and2012, respectively These amounts are included in salaries, wages, and relatedpersonnel costs in the consolidated statements of operations and changes in net assets
NOTE I - FUNCTIONAL EXPENSES
The functional classification of expense was as follows (in thousands)
Patient care, research and medical educationGeneral and administrative
Total operating expense
For the Years Ended December 31,
2013 2012
$ 1,940,474504,287
$ 2,444,761
NOTE J - COMMITMENTS AND CONTINGENCIES
$ 1,791,776395,179
$ 2,186,955
Methodist arranges for the issuance of bank letters of credit in connection with itsfinancial obligations, such as claims administration funding and support of frontedinsurance programs As of December31, 2013, outstanding letters of credit totaled$9 0 million and expire after a one-year term
-24-
NOTES TO CONSOLIDATED FINANCIAL STATEMENTSHOUSTON METHODIST
NOTE J - COMMITMENTS AND CONTINGENCIES - Continued
Methodist is party to a number of pending or threatened lawsuits arising out of, orincidental to, the ordinary course of business for which it carries professional and generalliability coverage and other insurance coverages In the opinion of management, uponconsultation with legal counsel, none of the pending or threatened lawsuits will have amaterial effect upon the financial position or results of operations of Methodist, and areproperly reserved for
Laws and regulations governing the Medicare and Medicaid programs and certain otherthird-party programs are complex and subject to interpretation As a result, there is areasonable possibility that recorded estimates of third-party settlements will change by amaterial amount in the near term Methodist's intent is to be in compliance with allapplicable laws and regulations, and it is not aware of any significant pending orthreatened investigations involving allegations of potential wrongdoing Compliance withsuch laws and regulations can be subject to future review and interpretation Changes inthe Medicare and Medicaid programs and a reduction of funding could have an adverseeffect on Methodist
Methodist accounts for asset retirement obligations in accordance with authoritativeguidance which clarifies that an entity is required to recognize a liability for the fairmarket value of a conditional asset retirement obligation when incurred if the liability'sfair value can be reasonably estimated The corresponding cost is capitalized as part ofthe carrying amount of the related long-lived asset The liability is accreted to its presentvalue each period and the capitalized cost is depreciated over the useful life of therelated asset
The asset retirement obligation, totaling $7 0 million and $7 3 million as of December 31,2013 and 2012, respectively, has been classified as a long-term liability This liability wasreduced by $216,000 and $282,000 in payments, increased by $243,000 and $253,000in accretion expense and reduced by a $327,000 and $271,000 change in estimate forthe years ended December31, 2013 and 2012, respectively The change in estimatewas recorded as a decrease in the carrying value of Methodist's various building facilitiesas of December 31, 2013 and 2012
-25-





























