Upload
thycoon
View
401
Download
20
Embed Size (px)
Citation preview
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
1/272
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
2/272
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
3/272
Manual ofNeuro-ophthalmology
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
4/272
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
5/272
Manual of
Neuro-ophthalmology
Amar AgarwalMS FRCS FRCOphth
Athiya AgarwalMD DO
Dr Agarwals Group of Eye Hospitals and Eye Research Centre19, Cathedral Road, Chennai - 600 086, India
JAYPEE BROTHERS MEDICAL PUBLISHERS (P) LTD
New Delhi Ahmedabad Bengaluru Chennai HyderabadKochi Kolkata Lucknow Mumbai Nagpur
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
6/272
Published by
Jitendar P VijJaypee Brothers Medical Publishers (P) Ltd
Corporate Office4838/24, Ansari Road, Daryaganj, New Delhi 110 002, IndiaPhone: +91-11-43574357
Registered OfficeB-3, EMCA House, 23/23B Ansari Road, Daryaganj, New Delhi 110 002, IndiaPhones: +91-11-23272143, +91-11-23272703, +91-11-23282021, +91-11-23245672Rel: +91-11-32558559 Fax: +91-11-23276490, +91-11-23245683e-mail: [email protected] our website: www.jaypeebrothers.com
Branches
2/B, Akruti Society, Jodhpur Gam Road SatelliteAhmedabad 380 015 Phones: +91-79-26926233, Rel: +91-79-32988717Fax: +91-79-26927094 e-mail: [email protected]
202 Batavia Chambers, 8 Kumara Krupa Road, Kumara Park East
Bengaluru 560 001 Phones: +91-80-22285971, +91-80-22382956, +91-80-22372664Rel: +91-80-32714073 Fax: +91-80-22281761 e-mail: [email protected] 282 IIIrd Floor, Khaleel Shirazi Estate, Fountain Plaza, Pantheon Road
Chennai600 008 Phones: +91-44-28193265, +91-44-28194897, Rel: +91-44-32972089Fax: +91-44-28193231 e-mail: [email protected]
4-2-1067/1-3, 1st Floor, Balaji Building, Ramkote Cross RoadHyderabad 500 095 Phones: +91-40-66610020, +91-40-24758498 Rel:+91-40-32940929Fax:+91-40-24758499, e-mail: [email protected]
No. 41/3098, B & B1, Kuruvi Building, St. Vincent RoadKochi 682 018, Kerala Phones: +91-484-4036109, +91-484-2395739, +91-484-2395740e-mail: [email protected]
1-A Indian Mirror Street, Wellington Square
Kolkata 700 013 Phones: +91-33-22651926, +91-33-22276404, +91-33-22276415Rel: +91-33-32901926 Fax: +91-33-22656075, e-mail: [email protected] Lekhraj Market III, B-2, Sector-4, Faizabad Road, Indira Nagar
Lucknow 226 016 Phones: +91-522-3040553, +91-522-3040554e-mail: [email protected]
106 Amit Industrial Estate, 61 Dr SS Rao Road, Near MGM Hospital, ParelMumbai 400012 Phones: +91-22-24124863, +91-22-24104532, Rel: +91-22-32926896Fax: +91-22-24160828, e-mail: [email protected]
KAMALPUSHPA 38, Reshimbag, Opp. Mohota Science College, Umred RoadNagpur 440 009 (MS) Phone: Rel: +91-712-3245220, Fax: +91-712-2704275e-mail: [email protected]
USA Office
1745, Pheasant Run Drive, Maryland Heights (Missouri), MO 63043, USAPh: 001-636-6279734 e-mail: [email protected], [email protected]
Manual of Neuro-ophthalmology
2008, Jaypee Brothers Medical Publishers
All rights reserved. No part of this publication should be reproduced, stored in a retrieval system,or transmitted in any form or by any means: electronic, mechanical, photocopying, recording, orotherwise, without the prior written permission of the authors and the publisher.
This book has been published in good faith that the material provided by authors is original.Every effort is made to ensure accuracy of material, but the publisher, printer and authors willnot be held responsible for any inadvertent error(s). In case of any dispute, all legal matters
are to be settled under Delhi jurisdiction only.
First Edition: 2009
ISBN 978-81-8448-411-3
Typeset at JPBMP typesetting unit
Printed at Ajanta
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
7/272
This book is dedicatedto a lovely couple
Marguerite Mcdonald and Stephen Klyce
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
8/272
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
9/272
Amar Agarwal MS FRCS FRCOPHTHDr. Agarwals Group of Eye Hospitalsand Eye Research Centre19, Cathedral RoadChennai-600 086, [email protected]
Athiya Agarwal MD DODr. Agarwals Group of Eye Hospitalsand Eye Research Centre19, Cathedral RoadChennai-600 086, [email protected]
Garrett Smith MD
Moran Eye CenterSalt Nake City, UTAHUSA
Jeyalakshmi Govindan DO DNBConsultant OphthalmologistDr. Agarwals Eye Hospital19, Cathedral Road
Chennai, India
Nick Mamalis MDMoran Eye CenterSalt Nake City, UTAHUSA
P Ramesh MBBS DMRD DNB MNAMS FRCRDirector, Liberty ScansChennai, India
Priya Narang MSNarang Eye HospitalAhmedabad, Gujarat, India
Contributors
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
10/272
viii Manual of Neuro-ophthalmology
Reena M Choudhry MD DO DNB FRCSIcare Eye Hospital and Postgraduate InstituteNoida, Uttar PradeshIndia
Sameer Narang MSNarang Eye HospitalAhmedabad, GujaratIndia
Saurabh Choudhry MD DO DNB
Icare Eye Hospital and Postgraduate Institute
Noida, Uttar PradeshIndia
S Soundari DO DNB FRCSConsultant OphthalmologistDr. Agarwals Eye Hospital19, Cathedral RoadChennai
India
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
11/272
Neuro-ophthalmology is a complex subspecialty which requires keenskills of clinical observation, attention to detail, and intricate thoughtprocesses in order to formulate the appropriate diagnostic andtherapeutic plan for the patient. What makes the field even morechallenging is our limited knowledge of the intricate neurologicalpathways between the eye and the brain; many of which are still
being discovered, as long as our understanding is evolving.To concisely and accurately explain the basics of neuro-
ophthalmology is a difficult task, as it requires a thoroughunderstanding of the subject as well as a natural gift for simplifyingand organizing the material so that it appeals to a wide audience.Through the process of teamwork, the Agarwals have succeeded increating an outstanding book for neuro-ophthalmology that will proveto be an excellent reference for a full spectrum of readers, from medicalstudents to practising ophthalmologists.
Prof Amar Agarwal once explained to me that for any challengingsituation, The battle is in the brain. Whether the task is climbingMount Everest or writing a complete library of ophthalmology texts,the true challenge is in mind. Having the drive and determination tosucceed, no matter the situation, is the mark of a true pioneer, and acharacteristic of one of my strongest mentors, Prof Amar Agarwal.
Uday Devgan MD FACS
Chief of OphthalmologyOlive View-UCLA Medical Center
UCLA School of MedicinePrivate Ophthalmic Practice
Maloney Vision InstituteLos Angeles, California, USA
Foreword
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
12/272
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
13/272
Understanding Neuro-ophthalmology is a challenge. It took us a longtime to comprehend the basics in this field when we were residents.That is the notion why we have writtenManual of Neuro-ophthalmology.The idea is that you dear reader can go through the text and figuresand never have difficulty in understanding this subject like we did.
We would like to thank our consultant Dr S Soundari for helpingus. Shri JP Vij and his full team of M/s Jaypee Brothers MedicalPublishers have always supported our writing endeavors. Our sincerethanks to them. Finally, dear reader we hope this book will changeyour outlook to Neuro-ophthalmology.
Amar Agarwal
Athiya Agarwal
Preface
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
14/272
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
15/272
1. Supranuclear Pathways for Eye Movements ..................................... 1
Athiya Agarwal, Amar Agarwal2. Supranuclear Disorders of Eye Movements ....................................17
Athiya Agarwal, Amar Agarwal3. Nystagmus .............................................................................................32
Athiya Agarwal, Amar Agarwal4. The Pupil................................................................................................54
Athiya Agarwal, Amar Agarwal5. Visual Pathway ..................................................................................... 73
Athiya Agarwal6. Anatomy of the Optic Nerve ............................................................ 103
Athiya Agarwal7. Oculomotor Nerve ............................................................................. 109
Athiya Agarwal8. Lesions of the Oculomotor Nerve ................................................... 118
Athiya Agarwal9. Trochlear Nerve and its Lesions ..................................................... 123
Athiya Agarwal10. Abducent Nerve and its Lesions ..................................................... 132
Athiya Agarwal11. Trigeminal Nerve .............................................................................. 140
Athiya Agarwal12. Facial Nerve and its Lesions ............................................................ 145
Athiya Agarwal
13. Congenital Optic Nerve Anomalies................................................ 150Priya Narang, Sameer Narang, Amar Agarwal
14. Optic Nerve Tumors ......................................................................... 157
Nick Mamalis, Garrett Smith15. Abnormalities of Optic Nerve Head .............................................. 185
Reena M Choudhry, Saurabh Choudhry, Amar Agarwal16. Ocular Myopathies ............................................................................ 197
S Soundari17. Miscellaneous .................................................................................... 204
Jeyalakshmi Govindan, S Soundari18. Examination of a Neuro-ophthalmology Case .............................. 219
S Soundari19. Imaging in Neuro-ophthalmology .................................................. 226
P Ramesh
Index ..................................................................................................... 253
Contents
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
16/272
1
Supranuclear
Pathways for EyeMovements
Athiya Agarwal, Amar Agarwal
INTRODUCTION
One is always confused about supranuclear pathways. We understandthe pathways of the III, IV and VI cranial nerve nuclei. We would beable to trace it from the brain to the superior orbital fissure, but wefail to remember that these pathways we are discussing are theinfranuclear pathways which extend from the cranial nerve nuclei tothe ocular muscle. We need to also understand the anatomy of the
supranuclear pathways.1,2
SUPRANUCLEAR AND INFRANUCLEAR PATHWAYS
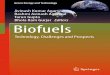
Anatomical pathways, which extend from the cortical centers of thebrain to the cranial nerve nuclei, are called the supranuclear pathways.From the cranial nerve nuclei to theocular muscle exist the infranuclearpathways (Fig. 1.1).
In peripheral nerves, the nerve starts from the brain and reaches
the anterior horn cell in the spinal cord. This is the upper motorneuron. From the anterior horn cell of the spinal cord, the nerve movesto the peripheral muscle. This is the lower motor neuron. If there is alower motor neuron disease the limb is flaccid and if there is an uppermotor neuron disease the limb is spastic.
The cranial nerve nuclei are like peripheral nerve nuclei. From thecortex of the brain the nerve extends to the cranial nerve nuclei andthis is the upper motor neuron (UMN) pathway. From the cranialnerve nuclei the nerve extends to the ocular muscle and this is thelower motor neuron (LMN) pathway. In peripheral nerves if theanterior horn cell gets involved as in poliomyelitis, the patient has aLMN disease and so the limb is flaccid. The anterior horn cell is akinto the cranial nerve nuclei of cranial nerves. So, if the cranial nervenuclei gets involved the lesion produced will be a LMN lesion.
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
17/272
2 Manual of Neuro-ophthalmology
Fig. 1.1: Supranuclear pathway
SUPRANUCLEAR EYE MOVEMENT SYSTEMS
There are five supranuclear eye movement systems. They are:1. Saccadic system2. Pursuit system3. Vergence system
4. Non-optic reflex system5. Position maintenance system.
SACCADIC SYSTEM
The saccadic system is otherwise known as the fast eye movementsystem or rapid eye movement system. This is because the saccadicsystem controls the fast eye movements. These are commandmovements. For example if we say, look to the right, the eyes turn to
the right. This occurs rapidly and is a rapid eye movement. The system,which controls this command pathway, is the saccadic system.The saccadic system originates from the frontal lobe of the brain.
The impulses then move to the mesencephalic system and so theanatomical pathway subserving the fast eye movements is the
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
18/272
Supranuclear Pathways for Eye Movements 3
frontomesencephalic pathway. When you watch someone watching a gameof tennis or table tennis, you will notice the eyes move rapidly fromone end of the court or table to the other. The eyes keep on dartingfrom one end to the other. These are fast eye movements controlled
by the frontomesencephalic pathway.
Horizontal Saccades
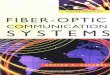
The saccades can in turn be horizontal or vertical. In horizontalsaccades, the eyes move horizontally and in vertical saccades, theeyes move up and down. Let us now understand the pathway of thehorizontal saccades (Fig. 1.2).
Fig. 1.2: Horizontal saccade pathwayLR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; Occ.Lobe-Occipital Lobe; Fron.lobe- Frontal lobe; III- III Cranial nerve nucleus; VI- VI Cranialnerve nucleus; PGC- Pontine gaze center; MLF- Medial longitudinal fasciculus;UMN Pathway- Upper motor neuron pathway; LMN Pathway- Lower motor neuronpathway
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
19/272
4 Manual of Neuro-ophthalmology
If the eyes have to look to the right, then the command for thismovement is given by the left frontal lobe in area 8 of the cortex. Thenerves cross over to the opposite side and reach the right pontinegaze center. From here the nerves pass to the same side (in this casethe right) VI nerve nuclei. From the right pontine gaze center nervesalso pass to the opposite III nerve nuclei. In this case this will be theleft III nerve nuclei. All the cranial nerve nuclei are connected witheach other through the medial longitudinal fasciculus or mediallongitudinal bundle. In other words from the right pontine gaze center,the nerves pass through the medial longitudinal bundle to the left IIIcranial nerve nuclei. Till here is the supranuclear pathway. This iswhy this is also called the frontomesencephalic pathway.
From the right VI nerve nucleus nerves then pass to the lateralrectus muscle of the right eye. From the left III nerve nucleus nervespass to the left medial rectus muscle. These are the infranuclearpathways and both the eyes move to the right.
At this stage it is important to understand a bit more on themedial longitudinal bundle. As just explained, the nerves pass fromthe pontine gaze center to the VI and III nerve nuclei through themedial longitudinal bundle. If there is a lesion in the medial
longitudinal bundle, these fibers are cut and there would not be acorrelation between the III nerve and the VI nerve. This leads to thecondition called internuclear ophthalmoplegia.
Vertical Saccades
The pathway for the vertical saccades is still doubtful. Vertical saccadesdepend on simultaneous bilateral activity within the frontal lobes inArea 8 (Fig. 1.3). This means that the horizontal saccades are
unilaterally controlled whereas the vertical saccades are bilaterallycontrolled.
If one has to look up or down, impulses travel from both the frontallobes in Area 8. The impulse travels via the basal ganglia to the pretectalarea or the pretectal center for vertical gaze. This is the vertical gazecenter. From the vertical gaze center impulses pass to the III nervenuclei. Till here is the supranuclear pathway. Now, the infranuclearpathway starts and impulses go via the III cranial nerve to the verticalmuscles and the patient looks up or looks down.
Because of the fact that vertical saccades require bilateral corticalactivity, cerebral hemisphere lesions rarely produce deficits in thevertical saccades. Such deficits are seen only with massive hemisphericlesions producing bilateral damage to both frontomesencephalic
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
20/272
Supranuclear Pathways for Eye Movements 5
pathways. Disturbances of vertical saccades are much more commonwith midbrain disorders.
Characteristic of the Saccade
The characteristic of the saccades is shown in Table 1.1 compared tothe other supranuclear eye movements. From the onset of the stimulus,which is voluntary to the beginning of the recorded saccade, the latentperiod is about 200 to 250 msec. The velocity of the fast eye movementis 30 to 700 degrees/second.
Fig. 1.3: Vertical saccade pathwayLE- Left eye; RE- Right eye; Occ.Lobe- Occipital Lobe; III- III Cranial nerve nucleus;VI- VI Cranial nerve nucleus; PGC- Pontine gaze center; MLF- Medial longitudinalfasciculus; UMN Pathway- Upper motor neuron pathway; LMN Pathway- Lower
motor neuron pathway
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
21/272
6 Manual of Neuro-ophthalmology
PURSUIT SYSTEM
The smooth pursuit system is utilized when the eyes follow targetsthat move smoothly and relatively slowly. It maintains a fixed
relationship between the movements of the eyes and the target. Assmooth pursuit movements directly relate eye position to targetposition, they are also termed as following or tracking movements. Asthese movements are slow, they are called slow eye movements. Imaginea person walking and you are watching that person. When your eyesfollow the movement of the person, they will be using the pursuitsystem. The pathway for the pursuit system starts from the occipitallobe and hence is known as the occipitomesencephalic pathway. Thereare different pathways for horizontal pursuits and for vertical pursuits.
Horizontal Pursuit System Pathway
If a target is moving to the right (Fig. 1.4), the first step is that theeyes have to visualize the object. So the pathway starts from the retina
Fig. 1.4: Horizontal pursuit pathway (slow phase)LR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; Occ.Lobe-Occipital Lobe; Fron.lobe- Frontal lobe; III- III Cranial nerve nucleus; VI- VI Cranialnerve nucleus; PGC- Pontine gaze center; MLF- Medial longitudinal fasciculus;UMN Pathway- Upper motor neuron pathway; LMN Pathway- Lower motor neuronpathway
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
22/272
Supranuclear Pathways for Eye Movements 7
of both eyes. The impulses pass through the optic nerve, optic chiasma,and optic tract and reach the right occipital lobe in area 19. This areasubserves the pursuit movements. It is important to note that theoccipital areas mediate horizontal pursuit movements to the ipsilateralside. In other words, the right occipital lobe mediates horizontalpursuit movements to the right.
From the occipital lobe, impulses go to the same side pontine gazecenter. In this case, impulses from the right occipital lobe go to theright Pontine gaze center. From here impulses go to the right VI nervenucleus and the left III nerve nucleus. Till here is the supranuclearpathway. From the right VI nerve nucleus and the left III nerve nucleusimpulses go via the infranuclear pathway to the lateral rectus and the
medial rectus. The characteristics of the pursuits are shown inTable 1.1.
Corrective Saccade
When the target is moving away from the field of vision the eyeswhich were moving slowly to that side have to come back to theiroriginal position. A fast eye movement does this, in other words asaccade. This is the corrective saccade. If a stream of cars are going in
front of our vision, then we keep on following one car and when itgoes out of the field of vision our eyes would come and fixate back tothe car in the center of our field of vision. This would be done by thecorrective saccade.
As the impulses from the target moving to the right reaches theoccipital lobe (Area 19) and the object is going out of the field of
Table 1.1: Characteristics of eye movements
Type Stimulus Latency Velocity Amplitude Conjugacy (msec) (Deg./Sec) (Degrees)
1. Saccade Volition, reflex 200 30-700 0.5-9.0 Conjugate2. Pursuit Target motion 125 < 50 0-90 Conjugate3. Vergence Accommodative, 160 < 20 Age Disjugate
fusional dependent4. Vestibulo- Head movement
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
23/272
8 Manual of Neuro-ophthalmology
vision the occipital lobe sends impulses to the ipsilateral frontal lobeto perform the corrective saccade. In this case the right occipital lobe(Fig. 1.5) sends impulses to the right frontal lobe (Area 8). This meansthere has to be a communication between the occipital lobe and thefrontal lobe. From the right occipital lobe impulses pass to the frontallobe via the parietal lobe.
From the right frontal lobe, impulses then pass to the left pontinegaze center which in turn sends impulses to the left VI nerve nucleusand the right III nerve nucleus. This is the supranuclear pathway.Then, the infranuclear pathway takes over and impulses go to therespective lateral and medial recti and the eyes move to the left as afast eye movement. This is the corrective saccade.
Fig. 1.5: Corrective saccade (Horizontal pursuit pathway for the fast phase)LR- lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; Occ.Lobe-Occipital Lobe; Fron.lobe- Frontal lobe; III- III Cranial nerve nucleus; VI- VI Cranialnerve nucleus; PGC- Pontine gaze center; MLF- Medial longitudinal fasciculus;UMN Pathway- Upper motor neuron pathway; LMN Pathway- Lower motor neuronpathway
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
24/272
Supranuclear Pathways for Eye Movements 9
One can illustrate this with an optokinetic drum, which is a drumwith black and white stripes. The drum is rotated and the eyes fixateon it. When the stripes go away from the field of vision, the correctivesaccade occurs. This leads to a type of nystagmus known as opto-kinetic nystagmus.
Parietal Lobe Lesion
If the person has a parietal lobe lesion, then there is a problem (Fig.1.6). When the corrective saccade has to work the impulse would notpass beyond the parietal lobe. Thus, this would lead to a deficit in thecorrective saccade. So a deep parietal lobe lesion causes loss or decreaseof the fast phase of the optokinetic nystagmus, when movement ofthe drum is towards the side of the lesion.
Fig. 1.6: Parietal lobe lesionLR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; Occ.Lobe-Occipital Lobe; Fron.lobe- Frontal lobe; III- III Cranial nerve nucleus; VI- VI Cranialnerve nucleus; PGC- Pontine gaze center; MLF- Medial longitudinal fasciculus;UMN Pathway- Upper motor neuron pathway
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
25/272
10 Manual of Neuro-ophthalmology
Vertical Pursuit System
Vertical pursuit movements are generated by simultaneous bilateralstimulation of area 19 of the occipital lobe (Fig. 1.7). The axons of the
occipital lobe descend to the pretectal area. From the pretectal areaimpulses travel to the III nerve nuclei. Till here is the supranuclear orUMN pathway. Then from the III nerve nuclei, impulses pass to thevertical muscles via the infranuclear pathway. The pretectal area orpretectal center is the center for vertical gaze, analogous to the pontinegaze center, which is the center for horizontal gazes.
Fig. 1.7: Vertical pursuit pathwayLE- Left eye; RE- Right eye; III- III Cranial nerve nucleus; VI- VI Cranial nervenucleus; PGC- Pontine gaze center; MLF- Medial longitudinal fasciculus; UMNPathway- Upper motor neuron pathway; LMN Pathway- Lower motor neuronpathway
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
26/272
Supranuclear Pathways for Eye Movements 11
VERGENCE SYSTEM
The role of the vergence system is to keep the image of a target onappropriate points (corresponding elements) of the two retinas by
controlling the visual axes of the eyes. Thus, vergence is utilizedwhenever a target falls on noncorresponding retinal elements. Forexample, if a target is moved towards the eyes, they must turn towardeach other (converge) to keep the target on the fovea of each eye.Conversely, as the target is moved further away, the eyes must turnout (diverge) (Actually, divergence does not occur in our eyes.)Vergence is thus a disconjugate (nonparallel) movement of the eyes,in contrast to most other eye movements which are conjugate (parallel).There are two types of vergence. They can be voluntarywhen wecommand our eyes to converge or reflexwhen we bring an objector tape towards our nose and the eyes converge while fixating on theobject. The characteristics of the vergence movements are shown inTable 1.1.
Voluntary Vergence
The center for voluntary vergence is situated in area 8 of the frontallobe (Fig. 1.8). If one wants to converge then a command movementis sent from area 8. These are bilateral impulses and they go to thepretectal area via the basal ganglia. Here there is the convergencearea. From the convergence area, impulses go bilaterally to the IIIand VI nerve nuclei. Till here is the supranuclear pathway. From theIII nerve nuclei impulses go to the medial recti to converge. From theVI nerve nuclei inhibitory impulses go to the lateral recti so that theeyes can converge. Thus both the eyes converge.
Pursuit or Reflex Vergence
In this, the impulses originate from the retina of the two eyes (Fig.1.9). If a pen is held in front of our eyes and moved towards the noseand if we keep looking at the pen, then the impulses from the twoeyes will make the eyes converge by the pursuit vergence pathway.From the retina impulses will go via the optic nerve and tract to area19 of the occipital lobe. This is a bilateral impulse. From here it goesto the pretectal area where it reaches the convergence area. From
here impulses pass bilaterally to the III and VI nerve nuclei. This isthe supranuclear pathway. Then positive impulses go to the medialrecti and inhibitory impulses to the lateral recti and the eyes convergewhile looking at the object.
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
27/272
12 Manual of Neuro-ophthalmology
Fig. 1.8: Voluntary vergence pathway
LR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; Occ.Lobe-Occipital Lobe; Fron.lobe- Frontal lobe; III- III Cranial nerve nucleus; VI- VI Cranialnerve nucleus; PGC- Pontine gaze center; MLF- Medial longitudinal fasciculus;UMN Pathway- Upper motor neuron pathway; LMN Pathway- Lower motor neuronpathway
NON-OPTIC REFLEX SYSTEM
The non-optic reflex system integrates eye movements and the bodymovements. There are basically three systems in this: (i) semicircularcanals, (ii) neck receptors, and (iii) the cerebellum. The characteristicsare shown in Table 1.1.
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
28/272
Supranuclear Pathways for Eye Movements 13
Fig. 1.9: Pursuit or reflex vergence pathway
LR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; III- III Cranialnerve nucleus; VI- VI Cranial nerve nucleus; PGC- Pontine gaze center; MLF-Medial longitudinal fasciculus; UMN Pathway- Upper motor neuron pathway; LMNPathway- Lower motor neuron pathway
Semicircular Canals
If a lateral semicircular canal is stimulated, the non-optic reflex systemstarts to work. If the head is rotated to the left (Fig. 1.10), the lateralsemicircular canal is stimulated. If we tilt our head to the left, theeyes should generally keep looking straight ahead (the ultimate aimof the whole process). For the eyes to look straight ahead when we
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
29/272
14 Manual of Neuro-ophthalmology
Fig. 1.10: Non-optic reflex system pathwayLR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; III- III Cranial
nerve nucleus; VI- VI Cranial nerve nucleus; PGC- Pontine gaze center; MLF-Medial longitudinal fasciculus; VN- Vestibular nucleus; UMN Pathway- Uppermotor neuron pathway; LMN Pathway- Lower motor neuron pathway
have tilted our head to the left the eyes will move to the right. Trythis on yourself by tilting your head to the left. You will note youreyes move to the right so that you keep on looking straight ahead.
When the semicircular canal is stimulated, impulse goes to the sameside (in this case left side) vestibular nucleus. From the left vestibularnucleus, impulses go to the opposite side pontine gaze center whichin turn send impulses to the right VI nerve nuclei and left III nervenucleus. This is the supranuclear pathway. Then the infranuclear
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
30/272
Supranuclear Pathways for Eye Movements 15
pathway takes over to the right lateral rectus and left medial rectusand the eyes turn towards the right. This constitutes the vestibularinfluence on eye movements.
Neck Receptors
Contributory information also comes from the proprioceptive organsof the neck muscles via the spinovestibular tract.
Cerebellum
The role of the cerebellum is not very clear. There is a prominentflocculo-oculomotor tract, which is the only direct cerebellar
connection with the eye nerve nuclei. This pathway connects with theopposite III nerve nuclei and the same side VI nerve nuclei (exactlyopposite the semicircular canal connection, which connects with thesame side III nerve and opposite side VI nerve nuclei). Thus, the eyestend to move in the opposite direction. This pathway may help explainthe reason why nystagmus in cerebellar disease is in the oppositedirection to that occurring in vestibular disease.
POSITION MAINTENANCE SYSTEM
The function of the position maintenance system is to maintain anobject of interest on the fovea or to maintain a specific gaze position.It is the most complex of eye movements and works efficiently onlywhen the person is alert. It becomes seriously disturbed when thepersons level of consciousness is depressed. The micromovementsystems use the same substrates as its macrocounterparts, but thedetails of the pathways are not yet known.
The micro eye movements are known as microsaccades or flicksand micropursuits or drifts. The microsystem is continuously activein maintaining the target precisely on the fovea, presumable whileother eye movement systems are active as well. Hence, it is the ultimatemonitor of eye movements, coordinating all the other eye movementsystems and determining the precise position of the eye with respectto the target as well as to the head and body. Stated simply, when anobject moves more rapidly than the smooth pursuit system can followit, a saccadic compensation is made to maintain the eye position relative
to the moving target. The pursuit system has been overcome by theposition maintenance system.
Take an example of your catching a ball. At that time when theball is in the air, your saccadic and pursuit systems work so that your
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
31/272
16 Manual of Neuro-ophthalmology
eyes are on the ball. Sometimes, there would be an overshooting ofeither of the systems and at that time the micromovements ofmicrosaccades and micropursuits take over so that you finally catchthe ball.
SUMMARY
Thus, there are basically five supranuclear pathways, which controleye movements. It is important to know them if one wants tounderstand supranuclear lesions.
REFERENCES
1. Sunita Agarwal, Athiya Agarwal, et al. Textbook of Ophthalmology 4th vol;Jaypee, India 2003.2. Amar Agarwal. Handbook of Ophthalmology; Slack USA 2005.
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
32/272
2
Supranuclear
Disorders ofEye Movements
Athiya Agarwal, Amar Agarwal
INTRODUCTION
If paralysis of an eye muscle occurs due to a lesion in the muscle,nerve or the nerve nucleus, all the functions of the muscle are involved.For example, if an infranuclear lesion occurs in the medial rectus, thepatient will neither be able to adduct the eye nor be able to performconvergence as the medial rectus is paralyzed. If the lesion was asupranuclear lesion, then the patient would not be able to perform
convergence but would be able to adduct the eye. The supranuclearlesions are lesions above the cranial nerve nucleus.1,2
PSEUDO-OPHTHALMOPLEGIA
In supranuclear lesions, only those activities controlled by theparticular region involved are impaired and other movements eventhough carried out by the same muscle remain normal. This paralysisof one type of movement and not of another is called pseudo-
ophthalmoplegia.
CLASSIFICATION
Depending on the supranuclear pathway, we can classify the supranuclearlesions as: Saccadic disorders Pursuit disorders Vergence disorders
Non-optic reflex system disorders (Flow chart 2.1).
SACCADIC DISORDERS
Saccadic disorders can in turn be divided into two groups (Flow chart 2.1): Conjugate palsies Dissociated palsies.
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
33/272
18 Manual of Neuro-ophthalmology
Flow chart 2.1: Supranuclear pathway lesions
In dissociated palsies, there is a misalignment of the eyes as theconjugate movements become dissociated, whereas in conjugate palsies
both the eyes fail to look in one direction. In dissociated palsies, oneeye fails to move in a particular direction, whereas the other eyemoves in that direction.
CONJUGATE PALSIES
Depending on the site of lesion, conjugate palsies can be grouped andclassified (Flow chart 2.2). The site of lesion could be in the frontallobe, basal ganglia, etc. In other words an area subserving the saccadicpathway if involved would lead to conjugate palsies.
Lesions of the Frontal Cortex
Overactivity
Epileptic seizures arising in the appropriate area of the frontal cortexcause what are called frontal adversive attacks. In these episodes, theattack commences with the head and eyes being forcibly deviatedaway from the discharging frontal cortex. If the left frontal cortex hasan overactivity due to a discharging focus and area 8 is involved, thesaccadic system overworks and the eyes look to the opposite sidethat is to the right (Fig. 2.1).
The side of the body to which the deviation has occurred maythen be involved by focal motor activity and ultimately the attackmay progress to a generalized seizure (Fig. 2.2).
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
34/272
Supranuclear Disorders of Eye Movements 19
Flow chart 2.2: Conjugate palsies
Fig. 2.1: Frontal lobe overactivity: Frontal adversive seizureLR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; Occ.Lobe-Occipital Lobe; Fron.lobe- Frontal lobe; III- III Cranial nerve nucleus; VI- VI Cranialnerve nucleus; PGC- Pontine gaze center; MLF- Medial longitudinal fasciculus
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
35/272
20 Manual of Neuro-ophthalmology
Fig. 2.2: Frontal adversive attackOcc.Lobe- Occipital Lobe; Fron.lobe- Frontal lobe; PGC- Pontine gaze center
Unilateral Underactivity
Damage to the frontal eye field by a vascular lesion may render thepatient unable to look to the opposite side. This deficit is rarely seenas rapid compensation occurs and the eye movements appear to benormal within hours. However, residual evidence may be found inthe patient having difficulty in maintaining gaze in that direction orin the development of some nystagmus caused by this weakness when
attempting to do so. If the patient is subsequently comatose oranesthetized, the eyes will deviate towards the damaged side of thecortex, because of the unopposed activity of the intact opposite frontallobe.
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
36/272
Supranuclear Disorders of Eye Movements 21
If the left side of the frontal area is damaged (Fig. 2.3), the intactarea 8 on the right side acts. This in turn pushes the eyes to the leftside, in other words, to the side of the lesion. The left hemispherecauses a right hemiparesis and the eyes thus look away from the para-lyzed limbs.
Bilateral Underactivity
Bilateral lesions of the frontomesencephalic pathway cause saccadic
palsy in both directions with preservation of pursuit and other eyemovements. Bidirectional saccadic palsy necessitates utilization of headmovements for refixation. The eyes remain locked on the originalobject of regard during a rapid head movement. This is called spasmof fixation. Bilateral saccadic palsies could be congenital or acquired. If
Fig. 2.3: Frontal lobe underactivityOcc.Lobe- Occipital Lobe; Fron.Lobe- Frontal lobe; PGC- Pontine gaze center
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
37/272
22 Manual of Neuro-ophthalmology
acquired it could be due to multiple sclerosis, Wilsons disease,Huntingtons chorea or lipidosis.
The most striking feature of this condition is the head thrusts utilizedto accomplish refixations. The head moves in the direction of theeccentric new target, as there is a saccadic palsy present. When thehead moves, the intact vestibulo-ocular system (non-optic reflexsystem) gets activated and the eyes are driven away from the attemp-ted direction of gaze. So, the patient closes the eyelids thus reducingthe vestibulo-ocular reflex gain and so reduces the amount of headthrust required. Head rotation overshoots the intended target,enabling the deviated eyes to fixate upon the object.
Lesions of the Basal Ganglia
Overactivity
The basal ganglia is predominantly concerned with movements in thevertical plane. Overactivity in the basal ganglia leads to the oculogyriccrisis. This usually consists of a fixed deviation of the eyes in anupward direction. During this crisis, the patient is incapacitated andany attempt to recover control of the eyes results merely in a feeble
jerky displacement from the position of spasmodic displacement. Thehead is frequently turned in the same direction as the eyes. This occursin postencephalitic parkinsonism, posthead injury state, neurosyphilisor brain tumors.
Underactivity: Progressive Supranuclear Palsy
In progressive supranuclear palsy there is loss of nerve cells, vasculardegenerations and glial reactions in the basal ganglia and midbrain.
The first manifestation of progressive supranuclear palsy is an inabilityto make vertical saccades, particularly downward saccades. At thispoint, the patients bang their shins, eat off only the top part of theirplates and complain of being unable to read (they cannot look down!).As the disease progresses, horizontal fast movements becomeinvolved as well. Eventually all fast eye movements are affected andthe pursuit movements become cogwheel.
Lesions of the Collicular Area
Parinauds Syndrome
There are several manifestations of lesions in the collicular area. Thesigns are thought to be caused by pressure and distortion of
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
38/272
Supranuclear Disorders of Eye Movements 23
underlying structures in the midbrain and not by damage to specificpathways traversing the colliculi. The general name for the clinicalpicture produced is known as Parinauds syndrome. Any combinationof impaired upward gaze, impaired downward gaze, pupillaryabnormalities or loss of accommodation reflex can occur. In general,loss of upward gaze associated with dilated pupils that are fixed tolight suggests a lesion at the level of the superior colliculus. Loss ofdownward gaze, normal pupillary reactions to light and loss ofconvergence suggest that the lesion is slightly lower in the area of theinferior colliculus. It could be due to lesions of the pineal gland,multiple sclerosis, vascular diseases or Wernickes encephalopathy.
A special type of nystagmus is present called retractory nystagmus.
This is a very rare sign of disease in the collicular area and consists ofan inward and outward movement of both eyes when the patientattempts to look upwards. Presumably, it is produced by all theextraocular muscles acting simultaneouslyjerking the globe back intothe orbit or attempted upward gazein an attempt to overcome theinability to look upwards.
DISSOCIATED PALSIES
In dissociated palsies, one eye moves in one direction whereas theother eye cannot move in the same direction. Thus, there is adissociation in the gaze movements. These canbe: Internuclear ophthalmoplegia One and one-half syndrome Dissociated vertical palsies.
Internuclear Ophthalmoplegia
Introduction
Lesions affecting the pathways by which the various ocular nuclei arelinked together, i.e. lesions of the medial longitudinal fasciculus (MLF)or medial longitudinal bundle produces internuclear ophthalmoplegia.The MLF connects the III nerve and the VI nerve nuclei. If a lesionoccurs in this there is prevention of the harmonious coordination ofthese nuclei in producing conjugate movements. So, one eye carriesout a voluntary movement of gaze whereas the other eye does not,thus leading to failure of the conjugate (both eyes moving in the samedirection) movement. This leads to a misalignment of the eyes andthus to diplopia. This feature differentiates the internuclear palsiesfrom the other supranuclear lesions.
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
39/272
24 Manual of Neuro-ophthalmology
Etiology
Depending on the lesion being unilateral or bilateral, various causesof internuclear ophthalmoplegia are present (Flow chart 2.3). The
common causes are vascular lesions or multiple sclerosis.
Classification
Internuclear ophthalmoplegia (INO) are grouped into three types.They can be type I, type II or type III INO.
Type I-INO In type I INO, the lesion is near the III cranial nervenuclei including also the convergence area (Fig. 2.4). Essentially thereis paralysis of both medial recti. The impulses coming from the pontine
gaze center go to the VI nerve and III nerve nuclei. As the connectionsto the VI nerve nuclei are not affected no disturbance is present inlateral rectus movements. The eyes are divergent due to bilateralinvolvement of the medial recti and there is loss of convergence. Itoccurs in hypertensive brainstem lesions and multiple sclerosis.Divergence may be complicated by skew deviation of the eyes inwhich one eye may be up and out and the other eye looks down andout. There may be a see saw nystagmus present in which the eyes jerkup and down alternately (Fig. 2.5).
Type II-INO In this relatively common variety of INO, the MLF isdamaged and the medial recti fail to move synchronously with thelateral recti (Fig. 2.6) on attempted lateral gaze to either side. Yetwhen each eye is tested alone, the medial recti function is evident butincomplete. Test this by covering the abducting eye and making theadducting eye follow the finger. In type II-INO convergence is normal
Flow chart 2.3: Etiology of inter nuclear ophthalmoplegia
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
40/272
Supranuclear Disorders of Eye Movements 25
Fig. 2.4: Site of lesions in internuclear ophthalmoplegiaIII- III Cranial nerve nucleus; VI- VI Cranial nerve nucleus; PGC- Pontine gazecenter; MLF- Medial longitudinal fasciculus
Fig. 2.5: Type I internuclear ophthalmoplegia
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
41/272
26 Manual of Neuro-ophthalmology
as the convergence area is not affected (Fig. 2.4). This occurs in multiple
sclerosis, pontine glioma or in encephalitis.Type III-INO The third variety of INO occurs in multiple sclerosis.
In this type of INO (Fig. 2.7), none of the eye abducts completelywhile adduction is complete. The relay to the VI cranial nerve nucleiis affected on both sides (Fig. 2.4). If you test the eye individually byclosing the other eye, the eye would abduct differentiating this froman infranuclear lesion (VI nerve palsy).
One and One-Half Syndrome
One and one-half syndrome is also known as paralytic pontineexotropia. In the primary position the eye which is opposite the sideof lesion is exotropic. The eye on the same side of the lesion looksstraight ahead. The lesion is in the pontine paramedian reticular
Fig. 2.6: Type II internuclear ophthalmoplegia
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
42/272
Supranuclear Disorders of Eye Movements 27
formation (pontine gaze centerPGC) or VI nerve nucleus and
ipsilateral medial longitudinal fasciculus. From figure 2.8 one willunderstand that only the VI nerve on the side opposite the side of thelesion will work. The patient is not able to gaze with either eyetowards the side of the lesion and is not able to adduct the eye on theside of the lesion (Fig. 2.9). This is why this is called one and one-halfsyndrome as one side gaze is absent and on the other side half thegaze movement only is present.
Dissociated Vertical Palsies
A dissociated palsy may affect the elevators of one eye in a supranuclearpalsy due to a localized lesion close to the nuclei below the pointwhere the corticofugal pathway for elevation of the eyes bifurcatesinto the branches which go to both III nerve nuclei. In this event,
Fig. 2.7: Type III internuclear ophthalmoplegia
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
43/272
28 Manual of Neuro-ophthalmology
Fig. 2.8: One and one-half syndrome- Site of lesionIII- III Cranial nerve nucleus; VI- VI Cranial nerve nucleus; PGC- Pontine gazecenter; MLF- Medial longitudinal fasciculus
Fig. 2.9: One and one-half syndrome
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
44/272
Supranuclear Disorders of Eye Movements 29
conjugate vertical movements are dissociated, one eye being incap-able of elevation in voluntary movements but moving up normally inBells phenomenon.
PURSUIT DISORDERS
Overactivity
If there is an overactivity of the parieto-occipital cortex (read verticalpursuit pathway), seizures originating in the occipital cortex causedeviation of the eyes to the same side. But in this situation, themovements will be accompanied by visual hallucinations. These usuallyconsist of flashing lights and colored blobs. A generalized convulsion
may ensue but focal motor activity, other than the eye movements isnot a feature of a focal seizure arising in the occipital lobe.
Underactivity
Damage to the parieto-occipital cortex leads to the patient not able tofollow a target on the side of the lesion. If the patient has a rightoccipital lobe lesion, then the patient would not be able to follow thetargets to the right side. Damage to the parieto-occipital cortex is
often associated with either parietal lobe difficulties, which may maketesting impossible. Similarly, if a homonymous hemianopia coexists(as it often does if the lesion is a vascular one), the patient may beunable to follow an object because it keeps vanishing into thehemianopic field. In these cases, it is essential to keep the object to befollowed just inside the midline, in the intact half of the patientsvision and to move it slowly.
VERGENCE DISORDERS
Paralysis of Convergence
Paralysis of convergence occurs if the lesion is in the pretectal areaaffecting the convergence area (read vergence pathways in Chapter 1).It is characterized by a failure of convergence with crossed diplopiaof the concomitant type. When the eyes view a near object, togetherwith the absence of any limitation of movement on either eyeinductions or inversions in any part of the field.
Paralysis of Divergence
Paralysis of divergence is characterized by the appearance of aconvergent strabismus with uncrossed diplopia when the eyes view adistant object.
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
45/272
30 Manual of Neuro-ophthalmology
NON-OPTIC REFLEX SYSTEM DISORDERS
Vestibular System Disorders
The vestibular apparatus (semicircular canals) controls the non-opticreflex system. Any lesion affecting the semicircular canals, VIII nerveor the vestibular nuclei will seriously affect the push-pull effect of thevestibular control of eye movements.
The right-sided vestibular elements, normally push the eyes tothe left. If there is a lesion in the right vestibular apparatus, it willlead to weakness of the eye movements to the left side. On attemptinggaze to this side, the intact normal vestibular mechanism on the leftside, coupled with the weakness of the damaged right side will force
the eyes to drift back to the midline. To solve this problem, there willbe a quick jerk of the eyes to the left side; i.e. to the side opposite theside of the lesion. The quick jerk in this case will be occurring to theleft side and the lesion was in the right side. Nystagmus is alwaystalked in relation to the fast phase of the nystagmus. In this case(right side vestibular lesion), the slow phase was on the right sideand to correct it a quick jerk or fast phase occurred towards the leftside. Thus, the nystagmus is away from the side of the lesion in a vestibular
disease (Fig. 2.10).With destruction of the labyrinth by Mnires disease, nystagmus
does not occur, because of central compensation for the absence ofany input. A similar situation exists after acute labyrinthine destructionwhen the initial imbalance settles. Similarly, in slowly occurringdamage to the VIII nerve (an acoustic nerve tumor) compensationoften prevents development of nystagmus. When it does occur in thissituation, it reflects brainstem or cerebellar damage from the extensionof the tumor into the cerebellopontine angle.
With central lesions of the vestibular apparatus (multiple sclerosis,vascular accidents) compensation cannot occur and the nystagmusand associated symptoms of vestibular damage tend to persist.
Cerebellar Disorder
The exact mechanism of cerebellar nystagmus is not known. Whennystagmus occurs it is opposite that found in a vestibular lesion. In a
right-sided vestibular lesion, the slow phase of the nystagmus is tothe right and the fast phase to the left. This means the nystagmus is tothe left, in other words opposite the side of the lesion. In cerebellardisease, the fast phase of the nystagmus is on the same side of thelesion. So, if there is a right-sided cerebellar lesion, the fast phase of
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
46/272
Supranuclear Disorders of Eye Movements 31
Fig. 2.10: Vestibular lesionLR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; Occ.Lobe-Occipital Lobe; Fron.lobe- Frontal lobe; III- III Cranial nerve nucleus; VI- VI Cranialnerve nucleus; PGC- Pontine gaze center; MLF- Medial longitudinal fasciculus;
VN- Vestibular nucleus
the nystagmus is towards the right side. This could be due to theflocculo-oculomotor pathway, which works in the reverse of thevestibular pathway. The left vestibular pathway pushes the eyes tothe right whereas the left flocculo-oculomotor pathway from the leftcerebellum pushes the eyes to the left.
REFERENCES
1. Sunita Agarwal, Athiya Agarwal, et al. Textbook of Ophthalmology 4th vol;Jaypee, India 2003.
2. Amar Agarwal. Handbook of Ophthalmology; Slack USA 2005.
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
47/272
3 Nystagmus
Athiya Agarwal, Amar Agarwal
DEFINITION
Nystagmus is a rhythmic to and fro oscillation of the eyes.
GENERAL CONSIDERATIONS
The specific neurophysiologic mechanism of nystagmus is not wellunderstood. Like all eye movements, nystagmus involves all or moreof the five known supranuclear pathways1,2 namely:
Saccadic system pathway Pursuit system pathway Vergence system pathway Non-optic reflex system pathway Position maintenance system pathway.
In nystagmus, generally the movement in slow phase is in onedirection and the fast phase in the opposite direction. The fast phaseof nystagmus is mediated by the saccadic system under all conditions.
One or more of the other systems mediates the slow phase. It isimportant to remember that nystagmus is given its direction based on thefast phase. This means that if we say a nystagmus is to the right, itmeans that the fast phase of the nystagmus is to the right. But actually,the important point of nystagmus is the slow phase. So actually,nystagmus should be given its direction depending on the slow phasebutthis is not done. An abnormality in the slow phase is more significant.But, alas, convention makes us talk only of the fast phase.
The eye position at any given moment results from all the impulsesfed into the III, IV and VI cranial nerve nuclei, from the supranuclearmechanism, the gaze systems and the gaze centers. Normally the inputis balanced and the eye movements are smoothly coordinated.Nystagmus develops when the normal balance is interrupted by a
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
48/272
Nystagmus 33
change of stimulus in a gaze system, frequently the vestibular system.Thus, in jerk nystagmus, a defect in one system results in eye deviation(slow phase) and repetitive attempts at correction of that deviation(by fast phases).
In many kinds of nystagmus, the patient has the subjectiveexperience that the world is moving or oscillopsia. Oscillopsia orperception of motion of the visual field associated with nystagmusseems to be present primarily during the slow phase of nystagmus,during which time the environment appears to move in the directionof the fast phase.You can demonstrate this for yourself by followingyour finger slowly back and forth horizontally in front of you. Noticethat the background appears to move in a direction opposite to your
slow eye movement (if the slow phase of nystagmus is to the left, thefield appears to move to the right).
During saccades (the fast phases of the nystagmus) the backgrounddoes not appear to move. Try making saccades by looking rapidlyfrom one corner of the room to the other. The background will not beperceived because of an elevated visual threshold. This elevation ofvisual threshold actually occurs prior to the start of the saccades.Some investigators believe that a discharge associated with the
oculomotor activity of the saccade causes an increase of threshold inthe visual afferent system. Other evidence suggests that the elevationof visual threshold occurs in the retina as a response to the forms andcontour in the visual environment.
Environmental motion perceived during nystagmus occurspredominantly during the slow phase, but in a direction that happensto coincide with the direction of the fast phase. Consequently, a patientwith a large amplitude right-beating nystagmus (fast phase to theright) might state that the room appears to be moving to the right.During the fast phase of the nystagmus and during all saccades, visualperception is suppressed.
TERMINOLOGY
Before we proceed further we should understand what certain termsmean in nystagmus.
Pendular Nystagmus
In this there is an undulatory movement of equal speed and amplitudein both directions.
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
49/272
34 Manual of Neuro-ophthalmology
Jerky Nystagmus
Jerky nystagmus demonstrates a biphasic rhythm wherein a slowmovement in one direction is followed by a rapid saccadic return to
the original position.
Micronystagmus
Micronystagmus is a term applied to a nystagmus, which is subclinical,so that it is incapable of being detected with ordinary clinical tests
because of its extremely small amplitude. The diagnosis is apparentby the fixation pattern, which shows a regular jerky type of nystagmuswith fast and slow phases of extremely small amplitude within the
parafoveal areas so that it may be revealed only by a carefulexamination with the visuoscope or direct ophthalmoscope.
Null Zone
The field of gaze in which the intensity of nystagmus is minimal istermed the null zone.
Neutral Zone
It is that eye position in which a reversal of direction of jerkynystagmus occurs and in which any of several bidirectional waveforms,pendular nystagmus or no nystagmus may be present.
Alexanders Law
Jerky nystagmus usually increases in amplitude with gaze in thedirection of the fast component. This is called Alexanders law.
GRADES
Nystagmus is divided into three grades.
Grade IJerky nystagmus is evident only in the direction of the fastphase, i.e. on conjugate deviation to one side.
Grade IIWhen in addition, it is evident in the primary position.
Grade IIIWhen it is evident in all positions of the eyes.
EXAMINATION OF A CASE OF NYSTAGMUS
There are certain points one should check when one is examining acase of nystagmus. They are:
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
50/272
Nystagmus 35
Is the nystagmus pendular or jerky? The fast phase of the nystagmus is on which side? Grade of nystagmus Symptoms of nystagmus Is squint present or not and if present, the type of squint? Is the nystagmus affected by heads position? Is the nystagmus worse with the eyes open or with them closed? Is the nystagmus affected by convergence? How wide are the ocular excursions?
CLASSIFICATION
Nystagmus can be divided into various groups (Flow chart 3.1). Ocular nystagmus Vestibular nystagmus Cerebellar nystagmus Central nystagmus Miscellaneous.
OCULAR NYSTAGMUS
Ocular nystagmus is due to a defect or embarrassment of central vision,which renders fixation difficult or impossible. It can in turn be eitherphysiological or pathological. The physiological nystagmus can in turn
be either deviational nystagmus or optokinetic nystagmus.
Flow chart 3.1:Types of nystagmus
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
51/272
36 Manual of Neuro-ophthalmology
Deviational Nystagmus
Deviational nystagmus is also called end-point nystagmus. It is a jerkynystagmoid movement of a physiological type when the fixation of
the axes are deviated beyond the limits of the field of binocular fixationand an effort is made to keep them there. It would generally happenif a person looks in the extreme lateral gaze. The fast phase is in thedirection of deviation. It would also occur if a person is tired or ifthere is a paresis of a muscle.
Optokinetic Nystagmus
Introduction
If a target moving in one direction is shown to a person, then the eyesmove in the direction of the target and when the target goes out ofthe limit of gaze, the eyes rapidly comes back to the center to refixatea new target. This is optokinetic nystagmus.
Clinical Test
A simple way to perform the optokinetic nystagmus (OKN) test is tohold a tailors tape in both our hands. One should stand one meteraway from the patient. Keep one hand stationary and with the otherhand move the tape. The patient looks at the tape. As the tape movesin one direction, the patient follows the movement of the tape by aslow eye movement (pursuit). Then there is a fast eye movement(corrective saccade) to bring back the eyes to refixate on the tape.
Kestenbaums Newspaper Method
The same result can be done with a sheet of a large newspaper movedslowly in front of the eyes in a direction perpendicular to the lines ofthe newspaper.
Barries Ruler Test
One can use a ruler about 12 inches long to perform the OKN test.The ruler is held with its long edge horizontal and with its short edgevertical and moved to the right and left of the eye.
Optokinetic Nystagmus Drum
The best method to test OKN is to use the OKN drum. This is aspecial drum, which rotates. The drum has black and white stripespainted on it. As the drum rotates the patient fixates on the stripes.
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
52/272
Nystagmus 37
There is a slow phase towards the direction of movement of the drumand when the stripes go out of the field of view, the eyes have a fastphase so that they come back to the center and refixate new stripesonce again.
Pathway
Optokinetic nystagmus has two parts: a slow phase (pursuit), and afast phase (saccadic). Let us imagine a tape or target moving in frontof the patients eyes from left to right. When the target moves fromleft to right the eyes fixate the target and the image reaches the retina.From here it goes to the optic nerve, optic chiasma, optic tract andthen reaches the right occipital cortex in area 19 (Fig. 3.1). This areasubserves the pursuit movements. It is important to note that the
Fig. 3.1: Slow phase of optokinetic nystagmus (OKN)LR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; Occ.lobe-Occipital lobe; Fron.lobe- Frontal lobe; III- III nerve nuclei; VI- VI nerve nuclei;PGC- Pontine gaze center; MLF- Medial longitudinal fasciculus
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
53/272
38 Manual of Neuro-ophthalmology
occipital areas mediate horizontal pursuit movements to the ipsilateralside. In other words, the right occipital lobe mediates horizontalpursuit movements to the right.
From the occipital lobe, impulses go to the same side pontine gazecenter. In this case, the impulses from the right occipital lobe go tothe right pontine gaze center. From here impulses go to the right VInerve nucleus and the left III nerve nucleus. Till here is the supranuclearpathway. From the right VI nerve nucleus and the left III nerve nucleusimpulses go via the infranuclear pathway to the lateral rectus and themedial rectus. Thus, the patients eyes move in the direction of thetarget.
When the moving target goes away from the field of vision the
eyes which were moving slowly to that side have to come back totheir original position. A fast eye movement does this, in other wordsa saccade. This is the corrective saccade. If a stream of cars are goingin front of our vision, then we keep on following one car and when itgoes out of the field of vision our eyes would come and fixate back tothe car in the center of our field of vision. This would be done by thecorrective saccade. As the impulses from the target moving to theright reaches the occipital lobe (area 19) and the object is going out of
the field of vision, the occipital lobe sends impulses to the ipsilateralfrontal lobe to perform the corrective saccade. In this case the rightoccipital lobe (Fig. 3.2) sends impulses to the right frontal lobe (area8). This means there has to be a communication between the occipitallobe and the frontal lobe. From the right occipital lobe impulses passto the frontal lobe via the parietal lobe.
From the right frontal lobe, impulses then pass to the left pontinegaze center which in turn sends impulses to the left VI nerve nucleusand the right III nerve nucleus. This is the supranuclear pathway.Then, the infranuclear pathway takes over and impulses got to therespective lateral and medial recti and the eyes move to the left as afast eye movement. This is the corrective saccade.
One can illustrate this with an optokinetic drum, which is a drumwith black and white stripes. The drum is rotated and the eyes fixateon it. When the stripes go away from the field of vision, the correctivesaccade occurs. This leads to a type of nystagmus known as optoki-netic nystagmus.
Parietal Lobe Lesion
If the person has a parietal lobe lesion, then there is a problem (Fig.3.3). When the corrective saccade has to work the impulse would not
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
54/272
Nystagmus 39
Fig. 3.2:Fast phase of optokinetic nystagmus (OKN)LR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; Occ.lobe-Occipital lobe; III- III nerve nuclei; VI- VI nerve nuclei; PGC- Pontine gaze center;MLF- Medial longitudinal fasciculus
Fig. 3.3:Parietal lobe lesionLR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; Occ.lobe-Occipital lobe; Fron.lobe- Frontal lobe; III- III nerve nuclei; VI- VI nerve nuclei;PGC- Pontine gaze center; MLF- Medial longitudinal fasciculus
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
55/272
40 Manual of Neuro-ophthalmology
pass beyond the parietal lobe. Thus, this would lead to a deficit in thecorrective saccade. So a deep parietal lobe lesion causes loss or decreaseof the fast phase of the OKN, when movement of the drum is towardsthe side of the lesion.
Type of OKN Abnormalities
There are four types of OKN abnormalities from type I to type IV(Table 3.1). The problems in OKN could occur if the lesion is in thepursuit system starting from the retina, optic nerve to the occipitallobe or in the saccadic system. There also could be a combination of
both systems involved.
Inverse OKN
An inverse OKN, wherein in horizontal movements the more rapidexcursion occurs in the direction of the moving object, can be seen incases of congenital nystagmus of ocular origin or in amblyopic
Table 3.1: Types of optokinetic abnormalities
Features Type I Type II Type III Type IV
Slow phase fast phase Combination complex abnormality abnormality (I and II)
Pursuit Affected Normal Affected Normal
Saccade Normal Affected Normal Normal
Neuroanatomiccorrelation
Posteriorhemisphericlesions on sideof OKNabnormality
Frontomesen-cephalic lesionon side of OKNdeviation
Extensivedeephemisphericlesion on sideof SOKabnormality
Occipitallesion on sideof OKNabnormality.Disconnectionsyndromepossibleinvolvingsplenium ofthe corpuscallosum
Frequentlyassociatedsignscontralateralto lesion
Hemianopia Hemiparesis Hemianopia,Hemiparesis
Hemianopsia
Oculardeviation
Normal Eyes tonicallydeviated indirection ofmoving targets
Same astype I
Same astype I
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
56/272
Nystagmus 41
nystagmus. The inversion is due to the fact that a pre-existingnystagmus takes precedence over the optokinetic phenomenon andmay thus augment it or interfere with it.
Pathological Ocular Nystagmus
Amaurotic Nystagmus
Nystagmus of pendular or rarely jerky type may occur in those whohave been blind for a long time. The nystagmus is sometimes constantand at other times it appears only when the attention is aroused.
Amblyopic Nystagmus
This is due to a defect in central vision in both eyes, which precludesthe normal development of the fixation reflex.
Spasmus Nutans
In this the nystagmus occurs with head nodding. It is also called Dunkelnystagmus. It generally occurs within the first year of life. The causeappears to be difficulty in maintaining fixation, which is frequentlyassociated with inadequate light. There is also insufficient controldue to instability of the motor cortical centers in early life.
Miners Nystagmus
This is an acquired occupational disease of the nervous system withspecial manifestations in the ocular motor apparatus, occurring inworkers in coalmines (Fig. 3.4). Basically it is due to lack ofillumination. In the early stages which is the latent stage slightnystagmus starts. Then in the acute stage trembling of the head andhands occurs with marked nystagmus and a pathognomic attitude ofthe head being thrown back. Then the psychopathic stage starts inwhich there are cramps, tremors, headaches and insomnia. Thenystagmus is generally pendular in type in the primary position butfrequently changes to the jerky type on lateral gaze. The treatment ofthis condition is to give the patient surface work and improve thegeneral health.
Latent Nystagmus
In this condition, nystagmus is not normally present when both eyesare open but is elicited on covering either eye. In the classical case thenystagmus appears on closing one eye. Bilateral jerky nystagmus is
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
57/272
42 Manual of Neuro-ophthalmology
seen with the fast phase towards the uncovered eye. Another conditionis called manifest latent nystagmus, which occurs in patients withamblyopia or strabismus who although viewing with both eyes openare fixing monocularly. Again the fast phase is towards the directionof the intended viewing eye. The phenomenon of latent nystagmus isparticularly evident when the visual acuity of the two eyes are unequal.Sometimes if one eye has a very poor vision on covering the bettereye instead of nystagmus, a conjugate deviation of both eyes occurstowards the side of the closed eye. This is calledthe latent deviationof Kestenbaum. One is not sure of the reason for latent nystagmus. It
could be due to lack of coordination of the supranuclear centers. Itcould also be due to the fact that the nystagmus was latent but kept incheck by convergence so that abolition of the impulse to binocularconvergence allowed it to become manifest.
Fig. 3.4:Miners nystagmus
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
58/272
Nystagmus 43
VESTIBULAR NYSTAGMUS
Vestibular Apparatus
The semicircular canals are three fine tubes arranged in the ear. Thelateral semicircular canal is tilted up 30 degrees. Normally the eyes atrest are in the primary position (Fig. 3.5). Impulses go from eachsemicircular canal to the respective vestibular nuclei. From here, theimpulse goes to the opposite pontine gaze center, which in turnconnects to the same side VI nerve nucleus and opposite side III nervenucleus. The impulses thus reach the medial and lateral recti and theeyes are balanced and in the primary position.
Caloric Test
The most easily understood form of vestibular nystagmus is whenperforming the caloric test. The patient lies on a couch with the head
Fig. 3.5: Caloric test eyes at rest in primary positionLR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; III- III nervenuclei; VI- VI nerve nuclei; VN Vestibular nuclei; PGC- Pontine gaze center;MLF- Medial longitudinal fasciculus
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
59/272
44 Manual of Neuro-ophthalmology
back at 60 degrees to bring the lateral semicircular canals to the verticalposition. This is because it is easier to produce convection currents ina vertical column of fluid. The test should not be performed if theeardrum is perforated. Water is taken at 30 degrees centigrade and44 degrees centigrade. Normal temperature is 37 degrees centigrade.One takes the water at 7 degrees centigrade higher and lower thanthe normal temperature. The water is run into each ear in turn. Athermostat is used to keep the temperature steady. 250 ml of water isallowed to flow over 40 seconds in the standardized test. While thewater is running the patient looks at a point straight ahead. Thisproduces vertigo and easily observed nystagmus as the canals arestimulated or inhibited and the eyes are pushed or pulled on either
side. The duration of the nystagmus is timed. The normal duration is2 minutes and 15 seconds.
When warm water is passed in the left ear (44C), it stimulates theleft semicircular canal. This in turn increases the discharge to the leftvestibular nucleus and thus the right pontine gaze center. This in turnleads to the eyes deviating to the right (Fig. 3.6). The slow phase of
Fig. 3.6:Caloric test with warm waterLR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; III- III nervenuclei; VI- VI nerve nuclei; VN Vestibular nuclei; PGC- Pontine gaze center;MLF- Medial longitudinal fasciculus
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
60/272
Nystagmus 45
Fig. 3.7:Caloric test with cold waterLR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; III- III nervenuclei; VI- VI nerve nuclei; VN Vestibular nuclei; PGC- Pontine gaze center;MLF- Medial longitudinal fasciculus
nystagmus is thus away from the ear, which is irrigated with warmwater. The eyes try to come back to the original position with a fastphase towards the left and thus a vestibular nystagmus is created.
When cold water (30C) is passed through the left ear impulsesare inhibited in that side. So the normal right semicircular canal worksand pushes the eyes with a slow phase to the left (Fig. 3.7). The fastphase then occurs to the right.
Remember nystagmus is always talked of in regard to the fast
phase. A mnemonic to remember the direction of the fast phase inthe caloric test isCOWS (cold opposite, warm same). This meanscold water calorics produce a fast phase to the opposite side and
warm water calorics produce a fast phase to the same side.
Vertical Vestibular Nystagmus
Vertical vestibular nystagmus can be elicited by bilateral caloricstimulation with the patient recumbent and his or her head flexed 30degrees above the horizontal plane. Bilateral cold water caloricsproduce vertical nystagmus with the fast phase up and the slow phase
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
61/272
46 Manual of Neuro-ophthalmology
down. Bilateral warm water calorics produce vertical nystagmus withthe fast phase down and the slow phase up. The mnemonic to
remember this is: Cold Slows Things Down. This means that thecold water produces the slow phase in the downward direction.
Lesions
Vestibular nystagmus could be produced with either a central lesionor a peripheral lesion. It is very important to differentiate betweenthe two. The caloric test can differentiate between canal paresis(peripheral lesion) and directional preponderance (central lesion).
Canal Paresis (Peripheral Lesion)
If the semicircular canal or the VIII nerve are damaged an incompleteor defective response to both hot or cold water in the affected earwill be found. In a normal caloric response (Fig. 3.8) hot and coldwater produce a nystagmus for about 2 minutes. If the patient has aleft canal paresis (Fig. 3.9) then neither hot nor cold water will producea good nystagmus in the affected ear. The duration of the nystagmus
Fig. 3.8:Normal caloric response
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
62/272
Nystagmus 47
will be less, for example, it could be just 1 minute. In peripheral lesions,the nystagmus is unidirectional and is horizontal and not vertical. Itis enhanced by removal of ocular fixation and may be positional.
Directional Preponderance (Central Lesion)
The central connections of the vestibular nerve are such that coldwater in one ear has the same effect as hot water in the other. If it isfound that nystagmus cannot be induced to one side it indicates thatthe vestibular nucleus of the appropriate side is defective (Fig. 3.10).This is known as directional preponderance. In left directionalpreponderance both the stimuli necessary to produce nystagmus tothe right fail, that means cold in the left ear and hot in the right ear.This proves that the nerve endings are normal but the brainstemmechanism for gaze to the left is defective. Central vestibularnystagmus is bidirectional and is not influenced by removal of ocularfixation. There is likely to be associated saccadic and pursuit eyemovement disorders.
Fig. 3.9:Left canal paresis. Neither hot nor cold stimuliproduce a full effect in the left ear, i.e. local lesion
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
63/272
48 Manual of Neuro-ophthalmology
There are some situations in which both canal paresis anddirectional preponderance may be combined. This is oftenencountered when an acoustic nerve tumor or other posterior fossa
lesion is displacing the brainstem.
Rotational Nystagmus
Rotation of the head can also produce a rotational nystagmus. If alateral semicircular canal is stimulated, the vestibular system starts towork. If the head is rotated to the left (Fig. 3.11), the left lateralsemicircular canal is stimulated. If we tilt our head to the left, theeyes should generally keep looking straight ahead (the ultimate aimof the whole process). For the eyes to look straight ahead when wehave tilted our head to the left the eyes will move to the right. Trythis on yourself by tilting your head to the left. You will note youreyes move to the right so that you keep on looking straight ahead.
Fig. 3.10:Left directional preponderance. Both the two stimuli necessary to producenystagmus to the right fail, that means cold in the left ear and hot in the right ear.This proves that the nerve endings are normal but the brainstem mechanism forgaze to the left is defective
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
64/272
Nystagmus 49
When the semicircular canal is stimulated, impulse goes to the sameside (in this case left side) vestibular nucleus. From the left vestibular
nucleus, impulses go to the opposite side pontine gaze center whichin turn sends impulses to the right VI nerve nuclei and left III nervenucleus. This is the supranuclear pathway. Then the infranuclearpathway takes over to the right lateral rectus and left medial rectusand the eyes turn towards the right. This constitutes the vestibularinfluence on eye movements.
On cessation of the rotation the right semicircular canal takes overproducing a deviation of the eyes to the left. Thus, the slow phase isto the left and this is the postrotational nystagmus (Fig. 3.12).
Remember when we use the direction of nystagmus, it is always saidaccording to its fast phase.
Fig. 3.11:Rotational nystagmusLR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; III- III nervenuclei; VI- VI nerve nuclei; VN Vestibular nuclei; PGC- Pontine gaze center;MLF- Medial longitudinal fasciculus
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
65/272
50 Manual of Neuro-ophthalmology
Fig. 3.12:Postrotational nystagmus
LR- Lateral rectus; MR- Medial rectus; LE- Left eye; RE- Right eye; III- III nervenuclei; VI- VI nerve nuclei; VN Vestibular nuclei; PGC- Pontine gaze center;MLF- Medial longitudinal fasciculus
Dolls Head Phenomenon
The rotational nystagmus provides a simple method for testing
vestibular responses in an infant or comatose patient. If an infant orcomatose patient is held at arms length and the head tilted slightlytowards the examiner and rotated to the patients left, the infant willdevelop a slow tonic deviation to the right and a corrective saccadeto the left. This is the dolls head phenomenon. This is extremelyhelpful in confirming the diagnosis of congenital oculomotor apraxiain infants. In this disorder, the saccadic mechanism is defective. Duringrotation of the head, the child will have the slow phase movement of
the eyes opposite the direction of rotation of the head, but the eyeswill not have a fast phase saccadic return.If you are not able to perform the caloric test in your office, you
could ask the adult patient to spin around several times while you
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
66/272
Nystagmus 51
note the postrotational nystagmus when the spinning is stopped. Thenormal patient who is spun to the left will develop postrotationalnystagmus to the right once the spinning is stopped. In other wordsthe slow phase will be towards the left and the fast phase towardsthe right. The environment will appear to move in the direction ofthe fast phase.
CEREBELLAR NYSTAGMUS
The exact mechanism of cerebellar nystagmus is not known. Whennystagmus occurs it is opposite that found in a vestibular lesion. In aright-sided vestibular lesion, the slow phase of the nystagmus is to
the right and the fast phase to the left. This means the nystagmus is tothe left, in other words opposite the side of the lesion. In cerebellardisease, the fast phase of the nystagmus is on the same side of thelesion. So, if there is a right sided-cerebellar lesion, the fast phase ofthe nystagmus is towards the right side. This could be due to theflocculo-oculomotor pathway, which works in the reverse of thevestibular pathway. The left vestibular pathway pushes the eyes tothe right whereas the left flocculo-oculomotor pathway from the leftcerebellum pushes the eyes to the left.
CENTRAL NYSTAGMUS
In central nystagmus, the nystagmus is of the jerky type. It isoccasionally present when the eyes are at rest, but usually developsonly when they are deviated to one or the other direction. Thenystagmus is symmetrical. This means that the movement starts atthe same angle of eccentricity and has approximately the same
excursion whether the gaze is directed to one or the other side.
MISCELLANEOUS
Voluntary Nystagmus
Voluntary nystagmus is habit learned and retained. The movementsare pendular and minute and in a horizontal direction.
Hysterical NystagmusHysterical nystagmus is just like voluntary nystagmus but theoscillations are quicker.
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
67/272
52 Manual of Neuro-ophthalmology
Idiopathic Congenital Nystagmus
In this there is congenital nystagmus without any known cause. Thisincludes all forms of nystagmus noted at birth or within the prenatal
period. It is usually horizontal but may be vertical, circular or elliptical.It may be pendular or jerky. Certain important points about congenitalnystagmus are: It is binocular and there is similar amplitude in both eyes There is no oscillopsia and it is abolished in sleep It is dampened by convergence and increased by a fixation effort.
As it is dampened by convergence the child usually has good nearacuity and can do well in school
It is uniplanar. This is the hallmark of congenital nystagmus. Planeof the nystagmus, usually horizontal remains unchanged in allpositions of gaze including the vertical gaze. This phenomenon isseen only in three entitiescongenital nystagmus, peripheralvestibular nystagmus and periodic alternating nystagmus
One can frequently identify a null zone of gaze in which thenystagmus is least marked and the visual acuity is the best
The patient may manifest a head turn to keep the eyes in the nullzone or alternatively have a muscle surgery to create the same
effect High astigmatism is frequently found which can be treated by
contact lenses.
Nystagmus Blockage Syndrome
In this there is reduction of nystagmus or blockage of the nystagmusin some particular gaze. The nystagmus diminishes or disappears withthe willed act of forced convergence while fixating a distant target.
This should not be confused with the dampening of congenitalnystagmus during convergence on a near target.
SYMPTOMS
The various symptoms of nystagmus are oscillopsia, diplopia, tiltingof the head or head nodding.
TREATMENT
The treatment can be treating the cause, use of prisms or surgery inwhich Fadens operation is done. The methods to treat nystagmusare shown in flow chart 3.2. The treatment can be general treatmentwhere the cause is treated or specific treatment, which can be medical
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
68/272
Nystagmus 53
or surgical. In medical treatment one can improve the visual acuity byusing prisms base out to simulate fusional convergence. One can useprisms to eliminate anomalous head postures also. For a head turn tothe left, the neutral zone is in dextroversion and a prism base out
before the right eye and base in before the left eye will shift the eyesconjugately along with the neutral zone towards the primary position.One can also use occlusion in which partial occlusion of the sound eyewith a neutral density filter to decrease visual acuity in the fixatingeye to a level below that of the amblyopic eye but not dark enough toelicit the nystagmus is used. Surgically one can perform Fadensoperation in which the required muscle creating the nystagmus issutured to the sclera at the equator.
REFERENCES
1. Sunita Agarwal, Athiya Agarwal, et al. Textbook of Ophthalmology 4th vol;Jaypee, India 2003.
2. Amar Agarwal. Handbook of Ophthalmology; Slack USA 2005.
Flow chart 3.2: Treatment of nystagmus
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
69/272
4 The Pupil
Athiya Agarwal, Amar Agarwal
NORMAL PUPIL
The pupil is an aperture present in the center of the iris and controlsthe amount of light entering the eye and reaching the retina. There isgenerally only one pupil but in some cases one can have more thanone pupil and this condition is called polycoria.
PUPILLARY PATHWAYS
Introduction
When light is shone in one eye, both the pupils constrict.1,2 Constrictionof the pupil to which light is shone is called direct light reflex and thatof the other pupil is called consensual (indirect) light reflex. If both pupilsare illuminated simultaneously, the response summates. This meansthe constriction of each pupil is greater than the constriction notedwhen only one pupil is illuminated. Rods and cones initiate the lightreflex.
Pupilloconstrictor Light Reflex Pathway
Afferent
The outer segments of the rods and cones are the receptors for boththe visual pathway and the light reflex. When light is flashed on theeyes, the pupillary fibers run in the optic nerve. From there they crossin the optic chiasma and reach the optic tract (Fig. 4.1). From the optic
tract they leave the visual pathway fibers (which continue to the lateralgeniculate body) and reach the pretectal nucleus. This is an ill-definedcollection of small cells anterior to the lateral margin of the superiorcolliculus. Internuncial fibers connect each pretectal nucleus with the
7/29/2019 9788184484113 - Agarwal - Manual of Neuro Ophthalmogy
70/272
The Pupil 55
Edinger-Westphal nucleus of both sides. Half of the postsynaptic fibersfrom the pretectal area cu