Embed Size (px)
Citation preview

9/16/2012
1
Blood pressure: Pathophysiology & Clinical
Management
Shahab Noori, MD
Associate Professor of Pediatrics
Division of Neonatology
September 20, 14:00 60 min
Insult Compensated
shock
Uncompensated
shock
Irreversible
shock
BP maintained Hypotension Multiorgan failure
Progression of Shock
Rationale for recognition and treatment of hypotension: a) Prevention of progression of shock to irreversible stage
b) Association with brain injury and poor developmental outcome
20
25
30
35
40
45
50
55
Me
an
BP
(m
m H
g)
0 12 24 36 48 60 72
27-32 weeks
33-36 weeks
37-43 weeks
23-26 weeks
1. Nuntnarumit et al, Clin Perinatol; 1999:26:981
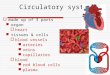
* = 90% of neonates will have a mean BP value at or above the lower limit of the confidence interval
Lower Limit of the 80% Confidence Interval of BP in Neonates ( First 3 Postnatal Days)1
Gestational- and Postnatal-Age Dependence of BP
Age (h)

9/16/2012
2
Definition of Hypotension in the VLBW Neonate
Hypotension has been defined as1:
a) Mean BP (mmHg) < gestational age (wks)
b) Mean BP ≤5th (10th) percentile for gestational and
postnatal age
c) Mean BP < 28-30 mmHg
d) “Permissive Hypotension” with no defined value
1. Noori S. et al. Clin Perinatol 2009;36:723-36
Poiseuille’s Law:
Q = P x r4
8l
P1 P2
r
l
Q =
Ohm’s Law:
R
P Q = flow
P = pressure gradient
= 3.14
r = radius
= viscosity
l = length
R = resistance
Blood Flow vs. Blood Pressure
Q =
Ohm’s Law:
R
P
Blood Flow vs. Blood Pressure
Cardiac Output = Blood Pressure
Blood Pressure = Cardiac Output x Peripheral Vascular Resistance
Blood Pressure = x Peripheral Vascular Resistance x 2 Cardiac Output
2
Peripheral Vascular Resistance

9/16/2012
3
BP = CO x SVR
Systemic Blood Pressure
Dependent Variable
Systemic Resistance
Independent variable
(Vasopressors, Lusitropes)
Systemic Flow Independent variable
(Inotropes)
Non-vital organ blood flow distribution
O2 Delivery to
Meet O2 Demand
When OBF regulation exhausted:
1. Capillary recruitment 2. O2 extraction
Systemic blood flow affected by
1. Autonomic, endocrine, paracrine, autocrine regulators of cardiac function
2. GA, PNA, shunts (PDA, PFO) 3. pH, PaCO2, PaO2, electrolytes (Ca++
i) 3. Pathology: cytokines, chemokines
PRINCIPLES OF CARDIOVASCULAR PHYSIOLOGY: BLOOD PRESSURE, BLOOD FLOW, BLOOD FLOW DISTRIBUTION, VASCULAR RESISTANCE
Resistance affected by:
1. Autonomic, endocrine, paracrine, autocrine regulators of vascular function
2. GA, PNA, shunts, vascular anatomy 3. pH, PaCO2, PaO2, electrolytes (Ca++
i) 4. 3. Pathology: cytokines, chemokines
Vital organ blood flow distribution (brain, heart,
adrenals)
Soleymani et al, J Perinatol 2010; 30:S38-S45
Adequacy of blood flow is the goal
but
cannot be ensured by clinical exam
(e.g. cap refill time) and laboratory test
(e.g. lactate)
Osborn DA et al. Arch Dis Child 2004;89:F168-73
Miletin J et al. Eur J Pediatr. 2009;168:809-13
de Boode WP. Early Hum. Dev. 2010; 86:137–141
Vast majority of studies show an
association between hypotension and
brain injury/outcome
What is the cause of poor outcome?
Hypotension
Treatment
Hypotension+treatment
Other (hypotension is a marker)

9/16/2012
4
Indicators of Hypotension during first 24 hrs and Neurodevelopmental Outcome at 24 months in Preterm Infants < 28 GA
1) Logan J W et al. Arch Dis Child 2011; 96:F321-8
After adjusting for confounders, none of the indicators of hypotension were associated with: 1) an MDI <70 or a PDI <70 2) Indicators of white matter damage or cerebral palsy
2) Logan J W et al. J Perinatol. 2011; 31:524-34
(n=945)
Challenges in Assessing Effect of Hypotension on Outcome
• Common practice of treating hypotension
• Temporal relation to other factors affecting organ perfusion (e.g. PDA)
• Dysregulated inflammation
• Lack of definition of hypotension based on vital organ blood flow
• Lack of RCT evaluating the effect of hypotension and treatment on outcome
Batton BJ et al. J Pediatr 2012; 161:65-9
Feasibility Study of Early Blood Pressure Management in Extremely Preterm Infants
• In seven NICUs and among a population of 336 only 10 were studied in 1 year! • Consent obtained in 17% of eligible infants. • All neonates with pre-eligible consents (prenatal and postnatal) were not enrolled.
Attending refused (n=13)
Of 48 not enrolled, 41 (85%) received treatment for hypotension

9/16/2012
5
Factors Affecting the Potential Impact
of Hypotension on Outcome
Duration 1-3
Loss of autoregulation 4,5
Hypercarbia 6,7
Hypoxia 2
Metabolic acidosis 3
1. Hunt et al. J Pediatr. 2004;145:588-92
2. Low JA et al. Acta Paediatr 1993;82:433-7
3. Goldstein RF et al. Pediatrics 1995;95:238-43
4. O’ Leary H. Pediatrics 2009;124:302-9
5. Wong FY et al. PLoS one 2012;7:e43165
6. Kaiser et al, Pediatr Res 2005; 58:931
7. Noori et al. APS-SPR 2011
Outcome
Average MBP
Death and any
disability
Death
Abnormal
motor
*OR (95% CI) adjusted for gestation, use of postnatal
steroids, and level of maternal education
0.84 (0.52–1.34)
0.98 (0.43–2.26)
1.18 (0.51–2.73)
First 12 h
Abnormal DQ 0.86 (0.52–1.44)
Hunt et al. J Pediatr. 2004;145:588-92
0.68 (0.42–1.09)
0.49 (0.26–0.93)
1.01 (0.48–2.10)
0.79 (0.47–1.31)
1.25 (1.03–1.51)
1.46 (1.15–1.84)
0.98 (0.74–1.30)
1.15 (0.93–1.43)
1.48 (1.07–2.04)
1.47 (1.06–2.04)
1.17 (0.77–1.77)
1.48 (1.01–2.16)
First 24 h
% Readings MBP < GA
First 12 h First 24 h
Hypotension (Mean BP < GA) and Neurodevelopmental
Outcome at 3 years
n=126
Case 1
• A set of twin were born at 26 3/7 week via c-sec with no premature rupture of membrane. Apgar scores were 71 and 85. Both received surfactant and were put on conventional mechanical ventilation. Blood pressure and capillary refill were normal in the first week.

9/16/2012
6
0
20
40
60
80
100
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72
rSO2 SPO2 Extraction
0
20
40
60
80
100
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72
rSO2 SPO2 Extraction
0
20
40
60
80
100
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72
rSO2 SPO2 Extraction
Twin
A
0
20
40
60
80
100
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56 60 64 68 72
rSO2 SPO2 Extraction
Twin
B
* * * * *
* * *
*
*
Normal HUS: Normal Normal Normal Normal Normal Normal
Normal HUS: Normal Normal G1 IVH G4 IVH
(hours)
(hours)
(%)
(%)
MCA mean velocity
(cm
/s)
(cm
/s)
0
10
20
30
40
50
60
70
80
90
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65 67 69 71 73 75
Twin A Twin B
Hours After Birth
Pa
CO
2 (
mm
Hg
)
Positive linear relationship between PaCO2 and MCA-MV
(R2=0.3, p<0.0001).
Relationship between Middle Cerebral Artery Mean
Velocity (MCA-MV) and PaCO2
(First 3 Days after Birth, GA 25.9 ± 1.4 wks, hemodynamically stable)
0
5
10
15
20
25
30
35
40
45
20 30 40 50 60 70 80
MC
A-M
V (
cm/s
)
PaCO2 (mmHg)
n= 78 data pairs in 21 subjects
Noori et al. APS-SPR 2011 (unpublished)

9/16/2012
7
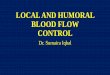
• Using piece-wise bilinear regression models, a breakpoint was identified at 51-53 mmHg of PaCO2.
• Significant increase in CBF with CO2 above low 50’s
Relationship between MCA-MV and PaCO2 in First 3 Postnatal Days
0
5
10
15
20
25
30
35
40
45
20 30 40 50 60 70 80
MC
A-M
V (
cm/s
)
PaCO2 (mmHg)
Noori et al. APS-SPR 2011 (unpublished)
R2=0.49, p <0.0001
n= 78 data pairs in 21 subjects
A slope of near or equal to 0 suggest intact cerebral autoregulation
Slope of autoregulatory plateau
CBF-MABP relationship in the neonate
Effect of Hypercapnia on Cerebral Blood Flow Autoregulation in
43 Ventilated VLBW Neonates
Kaiser et al, Pediatr Res 2005; 58:931
CBF autoregulation is affected by PaCO2
CBF and BP relationship adjusted for CO2 level
• MCA-MV had positive linear relationship with BP when adjusted for CO2
• No relationship when CO2 < 51 mmHg
• A trend for positive linear relationship when CO2 ≥ 51 mmHg
• Attenuation of CBF autoregulation with high CO2
0
10
20
30
40
50
60
70
10 15 20 25 30 35 40 45 50
MC
A-M
V (
cm/s
)
MBP (mmHg)
PaCO2 < 51 mmHg
0
10
20
30
40
50
60
70
10 15 20 25 30 35 40 45 50
MC
A-M
V (
cm/s
)
MBP (mmHg)
PaCO2 ≥ 51 mmHg R2 = 0.007
P = 0.5
R2 = 0.133
P = 0.09
Noori et al. APS-SPR 2011 (unpublished)

9/16/2012
8
Hypotension in Extremely Preterm Infants: Summary
• Hypotension is associated with poor outcome
• Adequacy of organ blood flow is the most important parameter but cannot be verified by clinical exam and laboratory tests
• “Hypotension” should be considered as one of the screening tool for adequacy of CV function
• Duration of hypotension, impairment of autoregulation and presence of co-existing derangements (hypoxemia, extremes of CO2, hsPDA, metabolic acidosis) may augment the adverse effect of hypotension
Principles of CVS Supportive Care
• Target the underlying pathophysiology
• Choose the “right” medication
• Titrate the medication to the desired effect
• Take into account the developmentally regulated
differences in CVS in neonates versus older
children
• Consider down-regulation of adrenergic
receptors
• Beware of overshooting
Pathophysiology of Shock
Blood Pressure ∝ Cardiac output x Systemic Vascular Resistance
Neuroendocrine and
paracrin regulatory
mechanisms
Heart Rate x Stroke Volume
Afterload Preload Contractility
Arrhythmia
Hypovolemia
Diastolic dysfunction
Volume overload
Poor contractility
Hyperdynamic myocardium
High afterload
Low afterload
Vasodilation
Vasoconstriction

9/16/2012
9
Adrenergic, Dopaminergic and Vasopressin Receptors
Vascular Vascular Cardiac Cardiac Vascular/Cardiac Vascular
0
++++
0
0
0
0
0
++
0
0
0
0
++++
++++
++++
0
++++*
+/++
0
0
++++
0
0
0
0
Vasoconstriction
Vasodilation
+ Inotropy
+ Chronotropy
Cond. Velocity
++++
0
0
0
0
α1 / α 2 β 2 α 1 β 1 / β 2 DA1 / DA2 V1a
Selecting the “right” medication:
Cardiovascular actions of adrenergic receptors
* = renal, mesenteric, coronary circulation > pulmonary circulation > extracranial vessels of the neck
Noori & Seri. Clin Perinatol 2012; 39:221-38.
Selecting the “right” medication:
Mechanisms of action of vasopressors, inotropes, and lusitropes
Adrenergic, Dopaminergic and Vasopressin Receptors
0
0/+
++
++
++
+++
0
0
0
+
++
++
++
++
+++
0
0
0
0
++++
++++
+++
++++
++++
0
0
0
0
0
0
++++
0
0
0
0
0
0
0
0
0
0
0
++++
0
0
Phenylephrine
Norepinephrine
Epinephrine
Dopamine
Dobutamine
Isoprenaline
Vasopressin
PDE-III Inhibitors
PDE-V Inhibitors
++++
++++
++++
++++
+/0
0
0
0
0
Vascular Vascular Cardiac Cardiac Vascular/Cardiac Vascular
α1 / α 2 β 2 α 1 β 1 / β 2 DA1 / DA2 V1a
Noori & Seri. Clin Perinatol 2012; 39:221-38.
Mean BP (mmHg)
CB
F (
ml/
10
0g
/min
)
Mean BP (mmHg)
n=17 preterm infants
Control
Pre-Dopamine Dopamine
Munro MJ. et al. Pediatrics 2004;114:1591
Avoid Excessive increase in BP
• CBF may be low in hypotensive preterm infants
• Once on vasopressor (e.g. dopamine), CBF improves BUT because of
presence of a direct correlation with blood pressure (loss of autoregulation) →
reperfusion brain injury ?

9/16/2012
10
Pathophysiology of Shock
Blood Pressure ∝ Cardiac output x Systemic Vascular Resistance
Neuroendocrine and
paracrin regulatory
mechanisms
Heart Rate x Stroke Volume
Afterload Preload Contractility
Arrhythmia
Hypovolemia
Diastolic dysfunction
Volume overload
Poor contractility
Hyperdynamic myocardium
High afterload
Low afterload
Vasodilation
Vasoconstriction
Cardiovascular
Compromise
Vasodilation
- Septic shock
- Systemic inflammatory
disease, (e.g. NEC)
- Pressor-resistant
hypotension
de Waal K, Evans N. J Pediatr 2010;156:918-22
Preterm Infants with Sepsis Have High Cardiac Output and Low SVR
• No change in flow and mild increase in SVR among survivors
• Non-survivor had a significant drop in cardiac output and a
sharp rise in SVR
n=20 (5 died), GA 27 (25-32) weeks, clinical sepsis or NEC, 15 had positive blood culture
* *

9/16/2012
11
SVRI And Cardiac Index (CI) In 30 Children with Fluid-resistant Septic Shock
Brierley J. et al. Pediatrics 2008;122:752-759
Central venous catheter-related
Community acquired
High CI > 5.5
• Hemodynamic response may vary depending on the bacteria
• Septic shock in late stages may be associated with myocardial
dysfunction
Vasodilatory Shock
• Treatment
– Volume
– Vasopressor (e.g. dopamine, epinephrine)
– Corticosteroid as a second line
*Significant hemodynamic variability among preterm infants who survive1
1. de Waal K et al. J Pediatr 2010
Cardiovascular
Compromise
Vasodilation
- Septic shock
- Systemic inflammatory
disease, (e.g. NEC)
- Pressor-resistant
hypotension
Poor Contractility
- Asphyxia
- Perinatal depression
- Septic shock (late stage)
- Dilated cardiomyopathy
- LV non-compaction
- Maladaptation after birth

9/16/2012
12
Case #2
• A preterm infant was born at 24 1/7 week (BW 805g) via vaginal delivery after prolonged rupture of membrane without signs of chorioamnionitis. Apgar scores were 21, 15, 210 and the baby required a brief chest compression. Initial ABG 7.05/92/102/-5/25 on SIMV FiO2 0.35. Switched to HFO with normal blood gases afterward.
• At 12 hrs
– ABG 7.33/37/47/-6/20 - BP 31/25 28
– CRT <2 sec - Hct 47
RVO (ml/k/min) 49 228
M-m
ode (L
V)
Short a
xis
vie
w (L
V)
Pulm
. Dop
ple
r
septum
post Wall
LV
SF 22% SF 37%
RVO (ml/k/min)
Pulm. Artery (systemic flow) Middle Cerebral Artery
A 4 hours old 25 6/7 wk preterm infants with severe
myocardial dysfunction, low systemic and cerebral blood flow
due placental abruption. Patients responds to dobutamine….
Dobutamine started Dobutamine started

9/16/2012
13
Robel-Tillig et al. Early Hum Dev. 2007;83:307
Cardiovascular Impact of Dobutamine in Neonates with Myocardial Dysfunction
Card
iac O
utp
ut
(ml/k/m
in)
SM
A –
SV
(cm
/s)
Ren
al
a. – S
V (
cm
/s)
A.
Cere
bra
l a. – S
V (
cm
/s)
Pre Dob 20 min Dob 8-10h
Pre Dob 20 min Dob 8-10h Pre Dob 20 min Dob 8-10h
Pre Dob 20 min Dob 8-10h
*
*
*
*
n=20, GA 29.4 4.4 wk, postnatal age 2 2.1 days, dobutamine 9.1 1.1 mcg/k/min
Asphyxia/Perinatal Depression
• Cause of circulatory compromise
– myocardial dysfunction (± compensatory
vasoconstriction)
• Treatment
– inotropes e.g. dobutamine
– avoid excessive fluid boluses
Cardiovascular
Compromise
Vasodilation
- Septic shock
- Systemic inflammatory
disease, (e.g. NEC)
- Pressor-resistant
hypotension
Poor Contractility
- Asphyxia
- Perinatal depression
- Septic shock (late stage)
- Dilated cardiomyopathy
- LV non-compaction
- Maladaptation after birth
High Afterload
- Maladaptation after birth
- Dilated cardiomyopathy

9/16/2012
14
Adapted from Rowland & Gutgesell, Am J Cardiol 1995
Sensitivity of Immature Myocardium to Afterload
Contr
actilit
y
Afterload
Treatment
Inotrope (e.g. dobutamine)?
Lucitrope (e.g. milrinone)?
Cardiovascular
Compromise
Vasodilation
- Septic shock
- Systemic inflammatory
disease, (e.g. NEC)
- Pressor-resistant
hypotension
High Afterload
- Maladaptation after birth
- Dilated cardiomyopathy
Hypovolemia
- Acute blood loss
- Umbilical cord avulsion
- Subgaleal hemorrhage
- insensible water loss
- Polyuria
Poor Contractility
- Asphyxia
- Perinatal depression
- Septic shock (late stage)
- Dilated cardiomyopathy
- LV non-compaction
- Maladaptation after birth

9/16/2012
15
Hemodynamic Effects of Delayed Cord Clamping in
Premature Infants
Sommers et al. Pediatrics. 2012; 129:e667-72
RCT, n=41, mean GA ~28 weeks, DCC=45 s, ICC= 5 s
• Higher SVC flow in delayed cord clamping group
• Higher RVO in delayed cord clamping group only at 48 hours
• No difference in MCA or SMA flow velocity, shortening fraction
Post Abdominal Surgery
1 month old former 23 week premie with NEC and perforation. Post-operative: Received multiple fluid boluses and escalating dose of dopamine up to 25 mcg/kg/min for persistent hypotension & metabolic acidosis BP 26/17 21 Base excess -12.8 Echo SF 48% LVO 243 ml/kg/min
Case #3
Cardiovascular
Compromise
Vasodilation
- Septic shock
- Systemic inflammatory
disease, (e.g. NEC)
- Pressor-resistant
hypotension
Diastolic Dysfunction
- Tension pneumothorax
- Cardiac tamponade
- Hypertrophic
cardiomyopathy
(e.g. IDM)
High Afterload
- Maladaptation after birth
- Dilated cardiomyopathy
Hypovolemia
- Acute blood loss
- Umbilical cord avulsion
- Subgaleal hemorrhage
- insensible water loss
- Polyuria
Poor Contractility
- Asphyxia
- Perinatal depression
- Septic shock (late stage)
- Dilated cardiomyopathy
- LV non-compaction
- Maladaptation after birth

9/16/2012
16
Case #4
• A 5.4 kg term infant, born to an insulin-dependent diabetic mother, presents with hypotension and moderate metabolic acidosis 2 hours after birth. Echocardiogram shows significant myocardial hypertrophy, dynamic left ventricular outflow tract obstruction, a closing PDA with bidirectional shunting and otherwise normal cardiac anatomy.
Normal IDM with HCM
Septum
Post Wall
Echocardiogram: M-mode
LV LV
Hypertrophic Cardiomyopathy
• Cause of circulatory failure
– diastolic dysfunction
• low preload
• hyperdynamic myocardium
– dynamic LV outflow obstruction
• Treatment
– VOLUME
– Beta-blocker (esmolol drip)
– Vasopressor
– AVOID inotropes
Cardiovascular
Compromise
Vasodilation
- Septic shock
- Systemic inflammatory
disease, (e.g. NEC)
- Pressor-resistant
hypotension
Diastolic Dysfunction
- Tension pneumothorax
- Cardiac tamponade
- Hypertrophic
cardiomyopathy
(e.g. IDM)
Shunt
- PDA
- AV malformation
High Afterload
- Maladaptation after birth
- Dilated cardiomyopathy
Hypovolemia
- Acute blood loss
- Umbilical cord avulsion
- Subgaleal hemorrhage
- insensible water loss
- Polyuria
Poor Contractility
- Asphyxia
- Perinatal depression
- Septic shock (late stage)
- Dilated cardiomyopathy
- LV non-compaction
- Maladaptation after birth

9/16/2012
17
Case # 5
• A preterm infant (twin A) was born at 31 1/7 weeks gestation (BW 1180g, 8%ile) via c-sec due to abnormal cord Doppler study. No signs of chorioamnionitis. Apgar scores were 41 and 75. The baby is on no respiratory support and blood gases are normal. However, the baby has been hypotensive despite receiving a bolus of NS. Now at 3 hours after birth, blood pressure is 34/14 (21) and capillary refill is 2-3 sec.
1) No intervention; continue close monitoring
2) Give another 10-20 ml/kg 0.9 NS bolus
3) Start dobutamine at 5 mcg/kg/min and titrate
4) Start dopamine at 5 mcg/kg/min and titrate
5) Start epinephrine at 0.05 mcg/kg/min and titrate
With regard to hemodynamic status, what would be the
best course of action:
SF 34%
LVO = 377 ml/k/min
M-mode (LV)
Short axis view (LV)
Aorta Doppler
Middle Cerebral Artery Doppler
MV 23 cm/s
15
20
25
30
35
40
3hr 9hr 33hr
MA
P (
mm
Hg)
-20
-10
0
10
20
30
40
50
60
70
80
3hr 9hr 33hr
LVO SVR MAP
% c
han
ge

9/16/2012
18
Not all “hypotensive” infant need
treatment if adequacy of organ blood
flow can be verified
Objective Assessment of Hemodynamics
Beyond BP
• Functional echocardiography
• Non-invasive continuous cardiac output
monitor
• Tissue oxygen saturation
– Near infra-red spectroscopy
– Visible light spectroscopy
Continuous Cardiac Output Monitor Based on Electrical Cardiometry
(Thoracic Electrical Biompedance)
Non-invasive
Simple to use
Need to be further validated
Aesculon ®
Aorta prior to Aortic
Valve Opening
Aorta after Aortic Valve
Opening
No Flow →
Random Orientation
Pulsatile Flow →
Alignment

9/16/2012
19
0
100
200
300
400
500
600
700
800
900
ᴏ
ᴏ ᴏ
Echo Electrical Cardiometry
LV
O (m
l/m
in)
Continuous Non-Invasive Cardiac Output Measurements in the
Neonate by Electrical Cardiometry:
A Comparison with Echocardiography
115 paired measurements in 20 healthy term neonates in first 2 days
Noori et al. Arch Dis Child 2012; 97:F340-3
Agreement between Left Ventricle Output Estimated by Echocardiography
and Electrical Cardiometry.
Noori et al. Arch Dis Child 2012; 97:F340-3
True precision = 31% which is considered clinically acceptable
115 paired measurements in 20 healthy term neonates in first 2 days
Bias 153 ± 56 ml/min
Limit of agreement = 43, 267 ml/min
NICOM consistently under-read LVO by 31 ± 8.8% (Limit of agreement = 15%, 46%)
Weisz et alNeonatology. 2012; 102:61-7
Non-invasive Cardiac Output Monitoring In Neonates Using Bioreactance:
A Comparison With Echocardiography
(ml/
min
)
97 paired measurements in 10 neonates 31-41 weeks gestation

9/16/2012
20
Fore-Sight ®
INVOS®
INVOS®
Tissue Oxygen Saturation: Near Infra-Red
Spectroscopy
Tissue Oxygen Saturation: Visible Light Spectroscopy
(T-Stat, SPECTROS)
Buccal tissue saturation is 61 to 72% in normal term neonates Correlates with LVO May be useful in detecting early stage of shock
Noori et al. J Perinatol 2011
BP or clinical assessment of flow
BP + clinical assessment of flow
+ pathophysiology
Identify underlying
pathophysiology
+
Echocardiography
+
Organ blood flow
Ensuring adequate
organ blood flow and
function
Identify possible
underlying
pathophysiology based
on the history
Level of Monitoring