Embed Size (px)
Citation preview
eNS, Head and Neck Imaging Case 92
91
• \.omcg:a]ovirus (CMV). • Herpes simplex.
• 'lpticdruscn. • _ rhisis bulbi. • lninal detachment • ~rinopathy of prematurity. • thpcrcalcacmic states - hyperparathyroidism,
..an:oidosis, chronic renal failure.
g adult m:lle prescnted with and panlysis of upward b'"lZC.
Discussion Optic drusen arc focal accumu lations of hyali ne material in the region of the optic nerve head, which commonly calcify. Aetiology is thought to be either a dc\'clopmcnral abnor!ll;llit)' or a degenerative process and it is histopathologically separate from retinal drusen deposits that call be a nOTmallinding or associated with age related macular degeneration. Clinically. patients arc usually asymptomatk bur can present with reduced \'isu:al acuity, migraine-like headaches and pscudopapillocdema. Di:agnosis is made by the absence of ad\·ersc imaging features such as abnormal cnhanccmcnt, optic nen'C thickening, mass dlcCI or postcrior globe solid lesions. Ocular ultrasound can be particularly usefu l in evaluating, and confirming this is not anuall). papilloedema. Optic disk haemorrhage is a very rare complication. The majoriry of cases (75%) arc bilateral.
Practica l tips Bilateral calcification docs not necessarily suggest a benign disc::lsc process. The nonherirable form of retinoblastoma (66") presents at - 24 months \\irh usually unilatcnl disease; but the heritable form (33%) presents ::II - 12 months with often (66%) bil::atenl disease.
Further management Ophthalmologica l assessment is required 10 confi rm the diagnosis and check viSllal fields and acuity.
157
158
Answer 92 eNS, Head and Neck Imaging
ANSWER 92
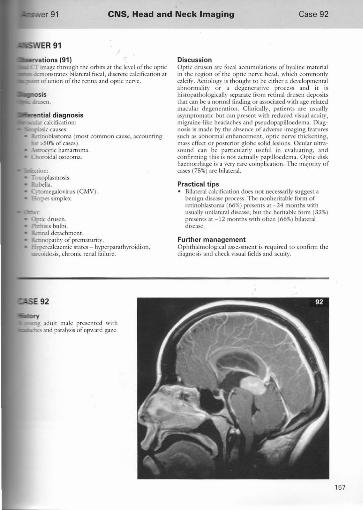
Observations (92) This midline saginal Tl post-contrast ,'vIR image demonstrates a large, slightly lobulated but well defined mass in the pineal region. The mass enhances homogeneously, compresses the superior colliculus and causes dilatation of the 3rd velUride. The most likely diagnosis is a pineal germinoma causing Parinaud's syndrome and obstructive hydrocephalus
Diagnosis Pineal germinoma.
Differential diagnosis Of pineal region masses: • Germ cdl tumours (>50%):
Germinoma Teratoma - extremely heterogeneous mass. Occurs in young children Choriocarcinoma. Embryonal cell tumour.
Pineal parenchymal tumours (25%): • Pineoeytoma - well demarcated, calcified, slow
growing tumour in1middle ,'ged adults. • . Pineoblastoma - si milar to medulloblastoma.
Allects young children. Enhances avidly :llld is nOl usually well circumscribed.
Others: • J'vlcningioma • Epidermoid or dermoid. • Arachnoid cyst - CSF density/signal • Pineal cySt - common; fluid density or signal
though contents can be proteinaceous on MlU. • Lipoma
Discussion The pineal gland is a midline structure situated behind the 3rd ventricle and responsible for biorhythm. It is calcified in most people over the age of 15 years and in almost all
elderly. Germ cell tumours arc the most common tum ofthe pineal region, accounting for over 50% of all p. masses. The most common subtype is germinoma, which histological1y similar to testicular seminoma. Pi germinomas arc well defined midline masses that arc more common in m3les than females. T hey afe norma seen in children and young adults. The lesion enh avidly. Oue to the anatomical location of the pineal these lesions compress the aqueduct ofSylvius produ hydrocephalus. The superior col1iculus of the brain ma~' also be compressed producing Parinaud's synd paralysis of upward gaze. Less common germ cd! ttl of the pineal gland include teratOmas, which are m seen in young children. Choriocarcinomas and emb~ cell tumours arc even less common and arc hi_ rn~lignant
Practical tips The pineal region is in the midline and masses in region may compress the aqueduct ofSyivius, so
~. ~t;;~~~ ~~~~~;n~~S~I~~~~~~~r~~h~l~~~~al gland exceeds I em in diameter a pathological pineal p should be suspected. Calcification in germinoma when present is ccntnIL. pincobbst'Oma pniphaal. In ~'ollng children think of teratoma (which are \heterogeneous masses), pineoblastoma and a vein Galcnancurysm In young adults, the most common solid lesion is germinoma.
Further management Surgery is difiicult due to the central location in The main rolc for surgery is in obtaining a possibly debulkins of tumour to relieve symptoms. However, serminomas arc radiosensitive and therefore radiotherapy is the of treatment.
92 Pineal germinoma.
eNS, Head and Neck Imaging Case 93
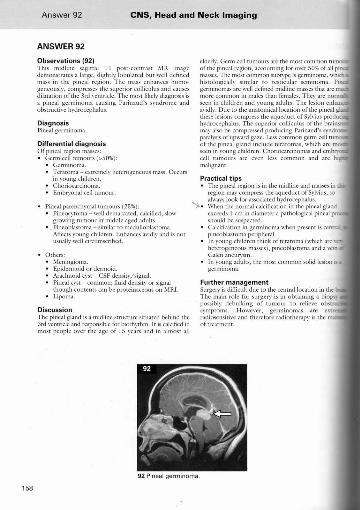
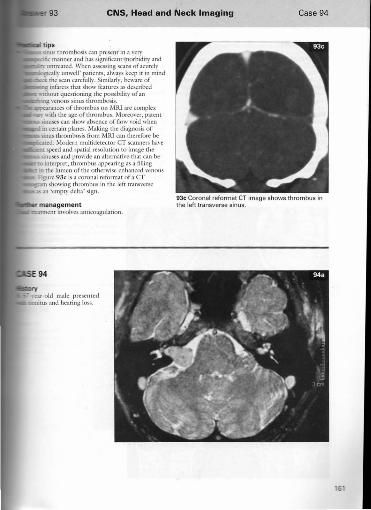
na PO and T2 weighted axial (top), T2 weighted coronal and T1 weighted sagittal (bottom) images.
159
160
Answer 93 eNS, Head and Neck Imaging
ANSWER 93
Observations (93a) Selected J\Ht images of Ihe brain demonstrate hyperintel1sity in the righr trans\'ersc sinus on the T I and T2 weighted images \\lrh an absence oCthe nomlal \'enOliS sinus flow \'aids. There is high-signal abnormality seen withi n the right mastoid air cells on T2 weighred images, which is intermediate signal on Tl imaging - this is likely to indicate infection/innammato~' change, Appearances arc consistenr wirh a diagnosis of \'enous sinus thrombosis secondary to mastoiditis. No imracerebral/ccrcbellar h~\emorrhage or inlarer is demonstrated on these images.
Diagnosis Venous sinus thrombosis.
Discussion There arc a variet), of underl )'ing ellises of \'enous si nus thrombosis, which include trauma, in/ccrion, idiopathic and h)'percoagulablc states, i.e. oral contracepti\'e pill, anti phospholipid syndrome, parancoplastic tumour s)'ndromes, antithrombin III deficiency. Presenting srmptoms can often be \'ery nonspecific, meaning that diagnosis is often OI}ly made radiologically. Symptoms include headache, nausea, vomiting and drowsiness, The superior sagit tal sinus is most commonly aflccted, followed by trans\'ersc and sigmoid sinuses
IUdiological appearances :ITC:
Uncontrastcd CT may show a hypcrdcnsc \ '(nOllS
sinus due to thrombus (Figure 93b shows a thrombosed superior sagitt:J.J sinus). Contrast enhanced CT shows a filling delcct within the triangular lumen outlined by a sillall rim of (oml"$ the 'empty delta' sign.
• MRI demonstrates :lIlabscncc afOaw \·oid within vcnous sinus, with local eflects of oedema, subcom infurction, suteal effacement and haemorrhage. • [n the acute phase, thrombus can appear as
isoinrcnsc on Tl weighted imaging and hypointcnsc on 1'2 weighted imaging. TIlis hypointcnsity on T2 can sometimes be mistna. tor flow \'oid and thcn::forc phase-contrast MR.o\. which shows /low, is beneT at identification.
• I n a chronic thrombosis, the venous sinus appea hypcrimcnsc on T I and '1'2 weighted images w extracellular methaemoglobin .
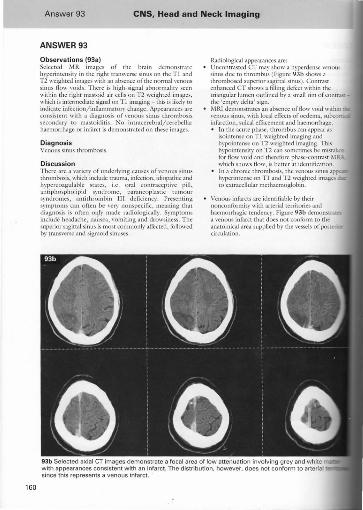
Venous infarcts arc idenrifiablc by their nonconformity \\ltb arterial territories and haemorrhagic tendency, Figure 93b demOIlstr.u a \'enous inf.,rct that docs nOt conform to the anatomical area sl1pplied by the vessels of posta. circulation,
93b Selected axia l CT images demo nstrate a focal area of low attenuation involving grey and with appearances consistent with an infarct. The distribution, however, does nol conform to arteria since this represents a venous infarct.
eNS, Head and Neck Imaging Case 94
sinus thrombosis call present in a '"cry • manner and has signific3m morbidity and umrC31cd. When assessing scans of acutely
_-call)' unwell' palicnts, alwa)'S keep it in mind the scan carefully. Similarly, beware of
g infan':t$ that show features as described :itham questioning the possibility of an
rutg wnous sinus thrombosis. J.ranccs oflhrombus o n MRl are complex
~ \\;th the age o[[hrombus. Moreover, patent sinuses can show absence of tlow \'oid when in certain planes. Making the diagnosis of smus thrombosis from MRI can therefore be
1('d. Modern Illultidctcctor CT scanners h3YC
t speed and spatial rcso]urion to image the Sinuses and provide an allcrnari"c that (an be
interpret, thrombus appearing as a filling Ul the lumen Oflhc otherwise enhanced '"CnOllS Figure 93c is a coronal reformat of a CT ~l showing thrombus in rhe lefi- tranS\'crsc ~ an ;cmpty dclt.l' sign.
93c Coronal reformat CT image shows thrombus in the left transverse sinus.
162
Answer 94 eNS. Head and Neck Imaging
ANSWER 94
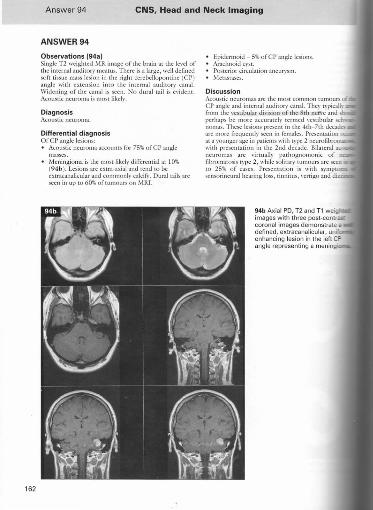
Observations 194a) Single T2 weighted Mit image of [he brain at the kycl of the internal ;ludirol)' Illcarus. There is a large , well defined soft tissue mass lesion in the Tight ccrcbcllopontinc (C P) angle with extension intO the internal auditory canal. Widening of the canal is seen. No dural tai l is c\'idclH. Acoustic neuroma is m OST likely.
Diagnosis Acousticncuroma.
Differential diagnosis orer angle lesions: • Acoustic neuroma accounts tor 75% orcp angle
masses. Meningioma is the mosllikdy diHi.:rclltial at 10% (94b ). Lesions arc extra-axial and tend 10 be cxtracanalicular and commonly calci!},. Dunl rails arc seen in up [0 6O'X.oftumours on MRJ.
Epidermoid ~ 5% ofCP angle lesions. Arachnoid CYST. Posterio r circulation aneurysm. Metastases.
Discussion Acoustic neuromas arc the most common tumours of C P angle and internal auditory (anal. They typicall~
from the \'estibular di\'ision of the 8th nefl,c and sh. p·erhaps be morc accurately termed \'cstibular sc llomas. These lesions prescll! in the 4th-7th decades arc more frequently seen in females. Prescntation at a rounger age in patients \lith type 2 neurofibro with prescntation in thc 2nd decade. Bilateral aCf' neuromas arc virtually pathognomonic of fibromatosis typc 2, whilc solimry tUlllours arc seen to 25% of cases. Presentation is with sympl scnsorincural hearing loss, tinnitus, vertigo and
94b Axial PO, T2 and T1 weig images w ith three post-contras: coronal images demonstrate a defined, extracanalicular, enhancing lesion in the angle representing a
swer 94 eNS. Head and Neck Imaging Case 95
ging features: arise ill the internal auditOry canal ( lAC). cause ~nlargcmcnt/c:rosion oftlte lAC.
LCSions extend imo rhe CP angle. L.olt'gcr tumours (>3 em) have central areas of necrosis md haemorrhage. ~ification is llOt a feature.
cr lesions arc usually imensc with uniform anccmcnt. MRI, lesions arc low sigmll on TI, high signal on
n <lnd show uniform enhancement with gadolinium.
ieal tips 'nguishing the main C P angle masses from each
Ilhcr: • Bmh acoustic neuroma and meningioma show
uniform enhancement so this is unhclphLI. • Acoustic neuroma - expands the lAC, causing
flaring of the poms acousricus. May be bright 011
T2 unlike meningioma. Makes an acute angle \\ith petrous bone.
• Mcningiolll::l - dural rail of enhancement, obtuse! anglCJwith petrOlls bone. Relatin:ly linle tissuc in the lAC compared to acoustic neuroma.
• Epidermoid vs arnchnoid cyst - both appear to follow the density and signal ofCSF on CT and T I md T2 weighted j\'IRJ. Howc\"er, the epidermoid shows increased signal on PO, FLAIR and diffusionfl weightedMI{:l .
SE 95
ory 30-ycar-old male:
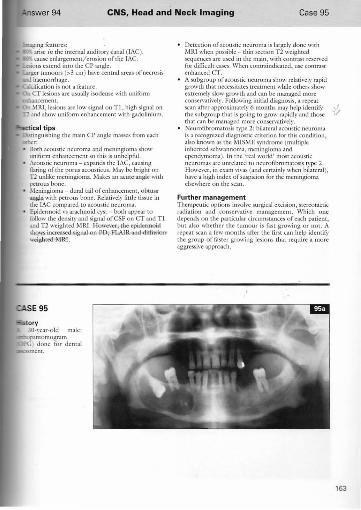
-opanlomogram ) done for denral
Detection of acoustic neuroma is largely done with M RJ when possible - thin section T2 weighted sequences are used in the main, with COntrast reserved for difficult cases. When contT:lindicated, use contrast enhanced CT. A subgroup of acoustic neuroma show rel;llively rapid growtb that necessit3tes treatment while others show extremely slow growth and can be managed morc conservatively, Follo\\;ng initial diagnosis, a repeat
~~l~~~~~~~~~~~:i:l~:~~n~ ~~o~:~~\,n;;~i~~I~I~~e~~~~~ * that can be managed more conservatively. Neurofibromatosis type 2: bil:lteral acoustic neuroma is a recognized diagnostic criterion for this condition. also known as the MlSME srndrome (multiple inherited schwan noma, meningioma and ependymoma), In the 'real world' most acoustic neuromas arc unrelated to neurofibromatosis typc 2. However, in exam "i\'as (and cenainl~' when bilateral), hal'e a high index of suspicion for the meningioma elsewhere on the scan.
Further management Therapeutic options involve surgical excision, stereotactic radiation and conservative management. Which o ne depends on the particubr circumstances of each patient, but also whether the tumour is fast growing o r not. A repeat sean a few months after the first can help identit}' the group of f.1Ster growing lesions that require a more aggressivc approach.
163
164
Answer 95 eNS, Head and Neck Imaging
ANSWER 95
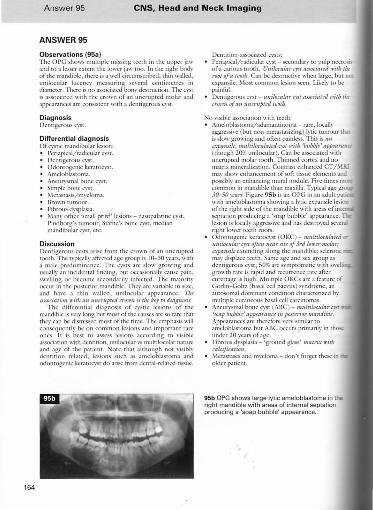
Observations (95a) The OPG shows multiple missing teeth in the upper jaw and to a lesser extent the lower jaw LOO. In the riglu body of the mandible, there is a well cin:ulllsuibcd, thin walled, unilocular lucency measuring sen:ral ccmimclrcs in diameter. 111crc is no associated bon}' dC$truClion. The Ll'St is 3ssociatcd with the crown of an unerupted molar and appcar:lIlccs afC consistent WiTh a dentigerous cyst.
Diagnosis Dentigerous cyst.
Differential diagnosis Of cYStic mandibular lesion:
P~riapical/radicular cyst. Dentigerous cySt. OdonlOgenic kcratocyst. AmcloblaSIOlll:l. Aneurysmal bone cyst. Simple bone cyst. Metastasis/ myeloma. Brown tulllour. Fibrous dysplasia. Man}' orher 'small print' lesions - nasopalatine cySt, Pindborg's tumour, Statile's bone cyst, medi:tn mandibular cyst, etc.
Discussion Dentigerous cysts arise from the ctown of an unerupted tooth. The typicall}' aftccted age group is 10-30 years, with a male predominance. The cysts arc slow growing and usually an incidental finding, but occasionally cause pain, swelling or becomc secondarily infected. The majority occur in the posterior mandible. They arc \'ariable in size, and ha\'c a thin walled, unilocular appearance. TIlt associatio" ",ilh all ll1uyupud CYOII"1 is lilt key to diaguosis.
The diAcrential diagnosis of cystic lesions of the mandible is vcry long bl
eNS, Head and Neck Imaging Case 96
l. ... 'St with demal associ,uian: tCd \Iith tooth apcx :md pain . I>crbpical cyst. tcd with unerupted tooth _ dentigerous cyst
\'Can and associated with crown ) or JStOlll3 (>30 years).
C\ost with no dcnral association: ~.n· _ OKC, simple bone cysr.
- I~ars - ameloblastoma, mct3stases o r myeloma.
<Y ·year-old patient presented with -hes and suspected sinusitis.
If brown tumour is suspected look. for other signs of hypcrpar:uhyroidism such as resorption ofthc lamina dura orthe teeth producing 'floating teeth' and generali zed dcmincmlization ofrhc mandible and ll1;uilb .
Further management Though often aS~'ll1ptomatic, dentigerolls cyst can cause pain and swelling and may predispose to pathological merure. Surgical excision (including the uncruprcd tooth) may therefore be undertaken.
Further reading Scholl R., Kcllw H , Neumann D, Lurie A ( 1999). Cysts
and c"sric lesions of the mandible: clinical and radioiogk-histopathologic review. RndioGrnplJics 19: 1107- 11 24.
165
166
Answer 96 eNS. Head and Neck Imaging
ANSWER 96
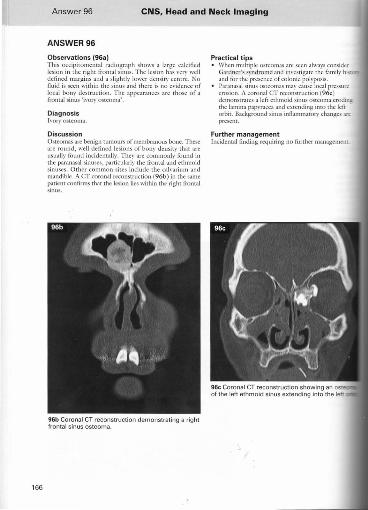
Observations (96a) This occipiwn1cnral radiograph shows a large calcified lesion in the right fromal sinus. The lesion has \'cry well defined margins and a slightly lower density cemre. No fluid is seen within the sinus and there is no evidence of local bony destruction. The appearances arc those of a frontal sinus 'iYory Ostt-oma',
Diagno'sis h 'ol)' osteoma.
Discussion Osteomas an:: benign tumours of membranous bone. These arc round, well defined lesions of bony density that arc usually found incidentally. They arc commonly found in the paranasal sinuses, p:l1"ticularly the frontal and ethmoid sinuses. Other coml11on si tes include the calvarium and mandible. A CT coronal reconstruction (96b) in the same patient confimls that the lesion lies within the right frontal sinus.
96b Coronal CT reconstruction demo nstrating a right frontal sinus osteoma.
Practica l tips • "Yhen multiple osteomas arc seen always consider
Gardner's syndrome and irwcsligarc the fami ly hist and tor the presence of colonic polyposis.
• Paran:lsal sinus osteomas may cause local pressure erosion. A coronal CT rcconsmlCtion (96c) dcmonstrJtcs a left cdulloid sinus osteoma eroding: the lamina papyracc;l and extending into the left orbit. Background sinus inOammatory changes 3«
present.
Further management Incidental finding requiring no further management
eNS. Head and Neck Imaging
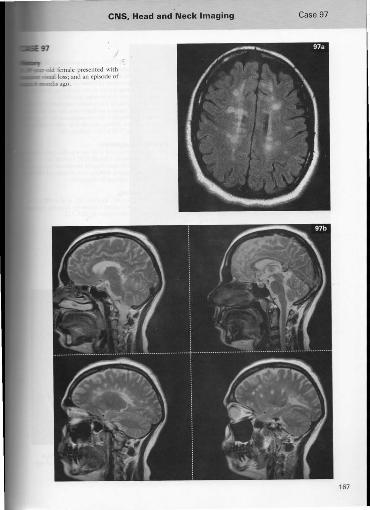
lid female presented with w.l loss; and an episode of
mthsago.
Case 97
167
168
Answer 97 eNS, Head and Neck Imaging
ANSWER 97
Observations (97a. 97b) Selected MR images ofrhc brain - FLAIR axial and T2 weighted sag;!!al - arc presented. These scans show multiple foc:!] O\'oid signal abnormalities in the pcri\'ctltricubr white matter, which 3rc orientated perpendicular to the long ax is of dIe ventricles. Further lesions invoke the corpus callosum. No associated oedema. No evidence of hydroccph:tlus. Given the clinical derails, it is likely that the patient has multiple sclerosis and is currently experiencing optic t~Cllli t is.
Diagnosis Multiple sclerosis (MS).
Differential diagnosis Of white matter lesions on MR];
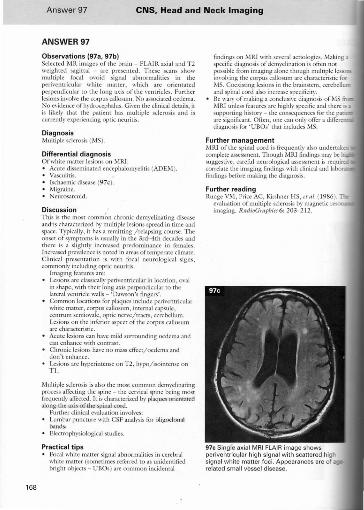
Acute disseminated cnccphalolll),clitis (ADEM ). Vasculi t is. Ischaemic disease (97c). M igraine. Ncurosarcoid.
Discussion This is the mOSt common chronic demyelinating disease and'is characterized by multiple lesions spread in tillle and space. T ypically, it has a remitting /rdapsi ng course. The onset of symptOms is usually in the 3rd-4th decades and thcre is a sli ghtly increased predominance in remales. I ncrcascd prevalence is nOTed in areas of temperate climate. Clinkal presentation is with focal neurological signs, com monly including optic neuritis.
Imagingfcaru resare: Lesions arc classicall~' ]x:ri\'entricular in location, O\'al in shape, with their long axis perpendicular to the lateral ventricle walls - 'Dawson's fin gers'. Common locations for plaques include peri\'entricular white matter, corpus callosum, internal capsule, centrum scmiovale, optic ner'I'C/ tracts, cerebellu m. Lesions on the inferior aspect ofrhe corpus ca llosulll arc characteristic.
• Acute lesions can ha,'c mild surrounding oedema and can enhance with comraSt.
• Chronic lesions ha"e no mass effect/ oedema and don'tcnhancc.
• Lesions arc hyperintense o n T2 , hypo/ isointense o n Tl.
Mull'ip1c sclerosis is also the most common demyelinating process aflccting the spine - the cervical spine being most frequently affected. It is characterized by plaques orientated alo ng the axis or the spinal cord.
Funher clinical e\'3lua[ion im'ol\'es: Lumbar punctme with CS F analysis for ol igoclon:tI bands. Electrophysiologic;).1 studies.
Practical tips Focal while matter signal ;).bnorm;).lities in cerebral white marter (sometimes referred to as unidentified bright objects - UBOs) are common incidental
fi ndings on MRl with se\'eral aetiologies. Making a specific diagnosis of dem),clination is often nor possible from imaging alone though multiple IcsiOOl. il1\'ol\;ng lhe corpus callosum arc characteristic for 1.'15. Coexisting lesions in the brainsl'cm, cerebellum and spinal cord also increase specificity. Be wary of making a conclusive diagnosis of M5 M RI unless feat ures arc highly specific and there is J.
supporting history - the consequences for the pa arc significant. O ften , one can only offer a ditlcrcn diagnosis for ' UBOs' that includes ,'v15.
Further management M RI of the spi nal cord is freq uently also undertak complete assessment. Though MRl findings may be _ suggesti\"e , careful neurological assessment is req uira. correlate the imaging findings \\~th clinical and Jahora. findings before making the diagnosis.
Further reading Runge VM, Price AC, Kirshner H5, ct at. ( 1986). n.
evaluation of multiple sclerosis by magnetic reso imaging. RfldioGrnpbiC!6: 203- 212.
97c Sing(e axial MRI FLAIR image shows periventricular high signal with scattered high signal w hite matter foci. Appearances are of related small vessel disease.
eNS, Head and Neck Imaging Case 98
169
170
ANSWER 98
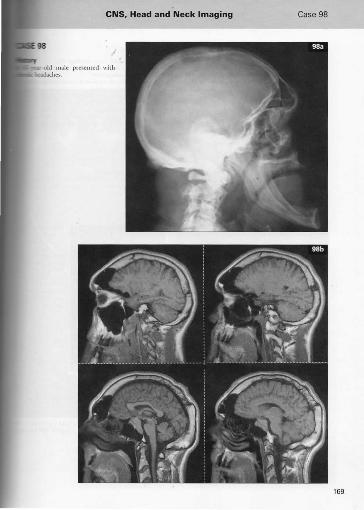
Observations 198a, 98b) This later:)l image of the skull (98a) shows elongation of the jaw (prognathism ), frontal bossing, cnlargcl1lt:nr of the frontal sinuses and thickening of the calvaria. There is marked enlargement of the pituitary fOssa with e,·idcncc of expansion bur no erosion.
Selected sagitt;'l] 1' 1 weighted illlages (98b) of the br.l.in connml the plain IiIIll findings of enlargement of the lTontal sin uses, frontal bossing ;'ind thickening of the c;l]"aria. There is a mass lesion within the pituitary fossa with appearances consistent with pituitary macroadcllol1la. Enlargemen t of the tongue is also noted.
Diagnosis Acrorncgal~' .
Discussion Excess growth hormo ne secretion by the anterior lobe of the pituitary gland results in a variety of nlllsculoskclet;ll abnOfm:l.litics.
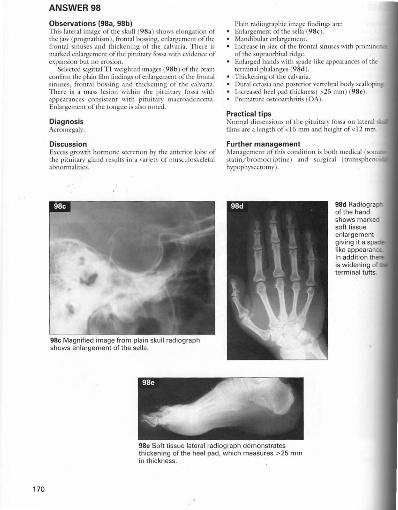
g8e Magnified image from plain skull radiograph shows enlargement of the sella.
Plain radiogr:tphic image findings :l.rc: Enlargement of the sella (98c). Mandibular enlargemcnt. Increase in sizc ofrhe frontal sinuses with promin afthc supraorbital ridge. Enlarged hands with spade -like appearances o f the terminal phalanges (98d). Thickening of the calvaria. Dur:t l ect:l.sia :l.nd posterior \"crtebr:l.1 body scallapln:Increased heel pad thickness( >25 tllm) (98c). Prcm:lture ostcO:lrthritis (OA).
Pract ical tips Normal dimcnsions of thc pitu itary fossa on lateral films arc a length of < 15 mill and height of < 12 mm.
Further management !\'ianagcmcnr of this condition is both medical (soma statin/brollloc riptine ) and surgical ( trallssphe n hypophysectomy).
98d Ra diogra of the hand shows marked soft tissue en largement giving it a sp like appearanc:e. In addition th is w iden ing of terminal tufts.
98e Soft tissue lateral radiograph demonstrates thickening of the heel pad, which measures >25 mm in thickness. .
eNS. Head and Neck Imaging Case 99
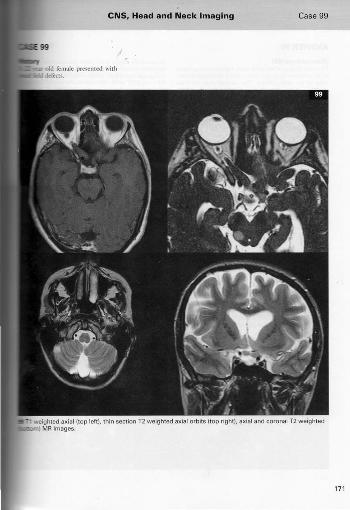
-. weighted axial (top left). thin section T2 weighted axial orbits (top right), axial and coronal T2 weighted I MR images.
171

172
Answer 99 eNS. Head and Neck Imaging
ANSWER 99
Observations (99) The axial images of the orbit show fusitorm enlargement of the posterior right optic l1en'e, which also il1\"okes both sidcs of the optic chiasm. The coronal scan confirms thickening of the posTerior aspect of bOTh optic nen'es. Axial T2 weighted images also show a round tixus of high signal in The right cerebellar hemisphere and a second lesion in the posterior aspen of right midbrain that produces convexity to the margins of the cerebral peduncle. The appearances arc likely to indicate optic nerTe glioma involving the chiasm and both opril": nen'es along with hamartomas in the cerebellum and midbrain due to neurofibromatosis type I. No cutaneous neurofibromas arc seen on these images.
Diagnosis O pTic chiasm/nen'e glioma due LO neurofibromatosis type 1 (NF l ).
Differential diagnosis ror optic nerve thickening: • Optic nen'e glioma - 80% under 20 yean, variable
enhancement, calcifjcation I""Olre, buckling of nen"e, of len asymptomatic.
• 'Meningioma of optic nem: - middlc aged women, 'tramtrack' enhancemelll, calcification in 20- 50%, st raight nen"e, visu al impairment early. Sarcoidosis. Multiplcsclcrosis Lymphoma, kukaemia and metastatic disease. Intracranial hypertension - enlarges the perineural CSFspace.
Discussion Optic nen'e glioma typically presents in childhood, only 20% manifesting beyond the age of 20. Rclati\"cly slow growing and benign ill children, lesions presenting in adults often show morc rapid malignant growth with intracranial spread. T hough often asymptom:uic, prescntaTion can bc with visual loss and strabismus. BHater:!1 tumours herald NF l . The tumour causes fusiform or tubular cnlargement of the optic nen"e sheaTh complex and shows variable enhancement with IV contrasT. The majority of lesions occurring in the orbital portion of the nen·e do not extend
intracranillly. Some optic nen'c gliomas haxc ext!: associated thickening of rhe surrounding meninges, Ie
ar.lchnoidal hyperplasia, which is often seen in patients 'Il NF - on T 2W M IU , Ihis is seen as:I ccntrallow-si tumour surrounded b~' a higher-signal rim that call M like a dilated perineural CSF space. p.
Approximately 25% of paticlHs with optic glioma NFl and it is one of the diagnostic critcri:l listcd for condition, of which two or more arc required: six or IDI
'cafe-au -lait' patches; twO or morc Lisch nodules; rn more neurofibromas or one plexiform ncurofibr axillary freckling; optic glioma; bone dyspb.si~
pseudarthrosis; fint degree relati,'c with NF l} In this the coexisting lesions in the cerebellum and midbrJin one to the overall diagnosis of NF l . These high T2 si~ toci arc seen in the brainsl'em, basal gangl ia, cerci peduncles, cerebellum and the stLprarenrorb.1 whiTe They arc usually thought of lS I
lnd often decrease in size with . to as[f(xyrom~ in the cerebmm, and telling the difference ma~' be i enlarges O\'er time or shows possibility of astrocytoma must be considered. choroid plexus calcification and hydrocephalus aqucduct stenosis arc o ther intrncranial features .
NFl is sporad ic in 50% and autosomal dominant' (chromosome 17).
Practical tips Tl weighted post-contraSt scans of the orbit sh be performed with fut suppression in view of the adjacemorbitai fur. Meningioma is the main differential diagnosis for optic ncn'e thickening and the features liSTed abomay help dis tinguish the tWO. Whenever NFl enters the diflcrential for anv
~ I""Oldiological study, al\\':lYs check for evidence of cutaneous nodules that 'clinch thc diagnosis'.
Further management Treatment depcnds on the size ofnrl1lour along \\ age and gener:!] condition ofthc patient. Options surgcry, radiotherapy and chemotherapy.
eNS. Head and Neck Imaging Case 100
173
174
Answer lOa eNS, Head and Neck Imaging
ANSWER 100
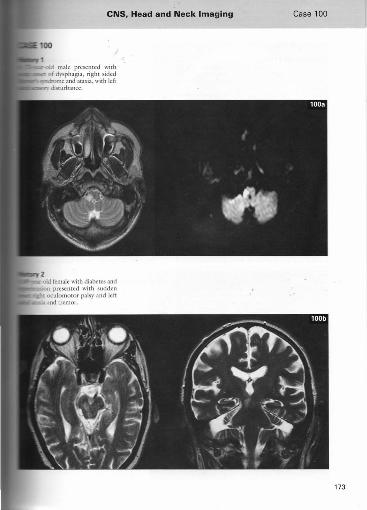
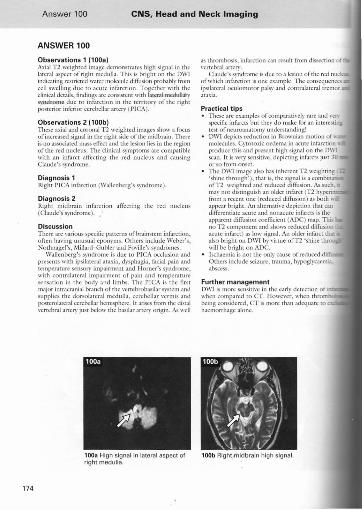
Observations 1 11008) Axial T2 weighted image demonstrates high signal in the lateral aspect of right medulla. This is bright on dIe DWI indicating restricted water molecule: diffusion probably from cell swell ing due to leutc inf:lfction. Together with the clinical details, findings arc consistent with latcrallllcdllll~'
syndrome due to in furction in the territory of the right posterior inferior cerebellar artery ( PICA).
Observations 2 (100b) These axial and coronal 1'2 weighted images show a focus ofincrcascd signal in the right side of the midbr:l.in. Then: is no associated mass dice! and the lesion lies in the region of the red nucleus. The clinical symptoms arc compatible with 3n infurct affecting the red nucleus and causing Claude's syndrome.
Diagnosis' Right PICA infarction (Wallenberg's syndrome).
Diagnosis 2 Ri ght midbrain infarction :lflccting the red nucleus (Claude's syndrome ),
Discussion There arc various specific panems ofbrainstem infarction, oftell having unusual eponyms. Othe rs include Weber's, Nodlnagel's, "<lillard-Gubler and Foville's syndromes.
Wallenberg's syndrome is due to PICA occlusion and presents with ipsilateral ataxia, d)'sphagia, fucial pain and temperanlre sensory impairment and Homer's syndrome, wi th contralateral irnpairrncnL of pain and tcmpcrature scnsation in the bod)' and limbs. The PICA is the first major intracranial branch of the vertebrobasilar system :lIld supplies the dorsolateral medulla, cerebellar ,'ermis and posterolatcral cerebellar hemisphere. It arises from the distal "ertebral :lrtery just below the basilar artery origin. As well
100a High signal in latera l aspect of right medulla.
as thrombosis, infuretion can result from dissection of ,'crtebral artery,
Claude's syndrome is due TO a lesion of the red nu of which inF.lrction is one example. T he consequences ipsil:tteral oculomotor pals}' and contralateral tremor araxia,
Practical tips • T hese arc examples of comparati\'ely rare and \'e~
specific infarcts but they do make for an interestin .... test ofne uroonatomy understanding!
• OWl depicts reduction in Brownian motion of\\ molecules, Cytotoxic oedema in acute infarction produce this and present high signal on the 0\\1 scan. It is ,'cry sensitive, depicting infurclS JUSt 30 or SO from onset.
• The DWI image also has inherent T2 weighting 'shine through' ), that is, thc signal is a combin.lD ofT2 weighted and reduced diffilsion , As such. ma~' not distinguish an older infurcr (T2 hyperi from a recent one (reduced diffusion ) as both \\ appear bright. An alternati\'e dep i~tion that can diflcrentiate acute and nonacute infurcts is the apparent diffusion coefficient (ADC) map. Th~ no T2 component and shows reduccd diffusion acute infurct) as low signaL An older infarct th.Jl: also bright on DWI b}' virtue of T2 'shine th ~
will be bright on AOC. Ischaemia is not the on l ~' cause of reduced di Others include seizurc, trauma, h}'\>oglycaemi..l. abscess.
Further management DWI is !\lore scnsiti"e in thc carl}' detection of ' when compared to CT. However, when throm being considered, cr is more than adequate to haemorrhage alone.
100b Right midbrain high signal.
eNS. Head and Neck Imaging
101
C1r-old male presented with _lIlrrollcd epilepsy_
Case 101
175
176
Answer 101 eNS, Head and Neck Imaging
ANSWER 101
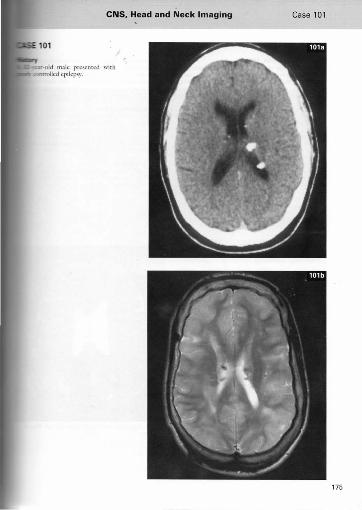
Observations 1101a. 101b) The axial CT image of the [)",in ( lOla) showsscvcliIl small calcified lesions in the subepcndymaJ region of the txxIy of the lateral \·cntricks. The T2 wciglucd MR im:agc of the brain (10 I b ) conlirms sc\'cml small subcpcndYlllalnodulcs with associated low signal representing calcification. These appearances arc consisTcm with slIbcpcndymal hamartomas. There arc abnormal widened gyri in the left paricml lobe and right frontallobc seen on Ihe MR image, which arc likely to indicate cortical h:lI11lrtom3S.
Diagnosis Tuberous sclerosis.
Discussion TuberOLis sclerosis is an inheri ted autosomal domin:llll disorder of the neuroectoderm that is characterized bv mul[isystem abnormalities. The classical triad of features arc mental retardation, seizures and adenoma scbaceum.
CNSfcarures: Subepcndymal hamartomas - most commonfy seen along the ventricular surfuce of the caudate nucleus. r ... lultiple small sy.bependymallcsions which calcify in 80%. Figure I Ol c shows another case where nodules have not calcified, but produce :I 'w:lI'y' border to the ,·entriclcw:llls. Corric:ll tubers - appearances arc of large widened :ltypical gyri with reduced attenuation ce!lues on CT. T he)' :Ire usuall}' multiple and can show rim calcification in 50%. Heterotopic grey matter is13nds - these :lppcar as 13rge hypodcnsc focal islands of tissue \\ithin the cerebral whiremattcr. Giant cell astrocytOlll:ls - occur around the foramcn of J" lonro, and can cause hydrocephalus. J\-blign:l11t potential is low.
Multisystem illvokement: • Ocular - ocular phakomas, oplic nerve gliomas. • Renal - angiomyolipoma, cysts, incre:lsed risk of ren:ll
ccllcarcinoma. Respiratory - Iymphangiomyom:ltosis-like features with cystic lung disease, spontaneous pneumothoraces ~lnd chylothorax. Cardio,"asctdar - rhabdomyoma, aonic aneurysms. Skin - :ldenoma sebaceum (red/ brown small flat skin lesions distribUled sylllmetricall ~' o\"er nose and checks), sh:lgreen p:ltches, ash lcaflcsiolls, subungual fibromas.
Practical tips The phakornatoses (neurocutaneous disorders), o f which tuberous sclerosis is an example, make great eX:l111 G1SCS because of the multitude of radiological signs to 'piece together' - know them well!
• Distinguishing lubcrs/ h:lrnarto111as from giant c astrocytomas: tubers and subependymal hamar! C:lll show some enhancement on MRI but CT is usually sensith·e enough to show this. Because cell astrocytom3S show more enh:lllcement, this be :lppreeiable on CT a.nd should a.rouse suspici
Further management Tuberous sclerosis has a high mortality with 70 before the :lgc of 24 ~'ears. A multidisciplinan approach is required with follow-up imaging im Mltl brain, renal ultr3Sonography (monitoring myolipom:ls :lnd looking for renal cell c:lTcino cchocardiography (50% of patients ha\·c rhabdom~
Further reading AJtman Nit, Purser RK, Post MJ ( 1988). Tuberou.
sclerosis: characteristics:lt CT and J\'IR imaging. Radi%gy 167: 527-532.
~-" >"'"'" .... -.~ 101c ./ ,_
.U_'~4' ~ ~ --
i, ! _, . ,.., , ,
'.~.',; f f:-'. ', .",.
eNS, Head and Neck Imaging Case 102
177
178
Answer 102 eNS, Head and Neck Imaging
ANSWER 102
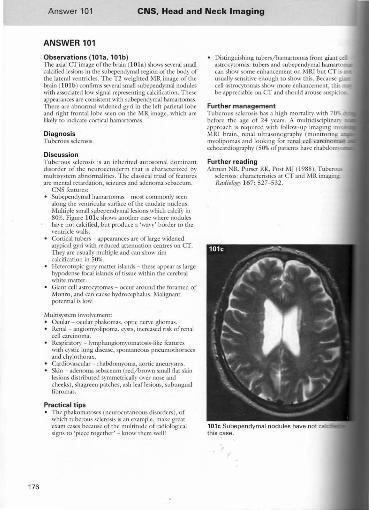
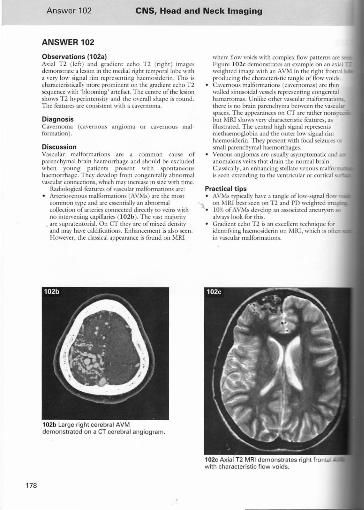
Observations (102a) Axial 1'2 (left) and gradient echo T2 (right ) images dcrnonstr,nc a lesion in the lllcdi:ll right Icmporallobc with a vcry low signal rim representing hacmosidcrin. This is ch:u :lctcristkally more prominent on the gradicm echo T2 sequence with 'blooming' artcf.tcr. The cenlre of the k-sion shows T2 hypcrimcnsity and the o\'crall shape is round. The fcamrcs are consislcnr with a C:l\'crnoma.
Diagnosis Ca\'crnoma (ca\"ernous angioma or ca'"crnous mal formation )"
Discussion Vascular malformations arc a common cause of parenchymal brain haemorrhage and should be excluded when young patients present with spontaneous haemorrhage. They de,"elop from congenitally abnormal \'ascular connections, whieh may incrcasc in size. with rimc.
R .. 1diological features of\'ascular malformations arc: Arteriovenous malformations (AVMs) afe the most common type and arc eucntially an abnormal collection of an cries connected dircctlv to ' "cins with no imen'ening capillaries ( I 02b). Thc' vast majority
• afe supratentorial. On CT thc)' arc of mixed density and mav have calcifications. Enhancement is also secn. !-Iowcver, the classical appearance is found on MRl
102b Large right cerebral AVM demonstrated on a CT cerebral angiogram.
where flow ,ooids with complcx flow patterns aTe Figurc I 0 2c demonstr.ltes an example o n an axial _ weightcd image with an AVM in the right frontal producing the characteristic (';l1lglc of now voids. C:wernous malformations (ca,"ernomas) arc thin walled sinusoidal vessels representing congenital hamartomas. Unlike other vascular malforl11 atio~
then: is no brain parenchyma Ixtwecn the \"3sculM spaces. The appearancC$ on CT arc rather nons but i\'IIU shows vcn' characteristic features, as illustrated. The celltral high signal represent's lllcthaemogiobin and the outer low signal rim haemosiderin. They presem with focal seizures (W
small parenchymal haemorrhages. Venous angiomas arc uS ll all~' asymptomatic and anomalous ,"eins that dmin rhe normal brain. Classically, an enhancing stellate venous mallo is seen extending TO the ventricular or conical
Practical tips • AVMs typically h;1\'c ;t tangle oflow-signal flo\\
":\ on ,\-IRI best seen on T2 and PD weighted ima_ • 10% of AVMs develop an :lssod:J.tcd :lllclll)'Sm OJ(
alw:l\'S look. for this. Gradient ccho T2 is an excellent technique for idcntif)'ing haclllosidcrin 011 MIU, which is oltca in vascular llultOrm:uions.
102 eNS. Head and Neck Imaging Case 103
idcrin will also be seen in an old haemorrhage KC~sarily itwoking an underlying vascular
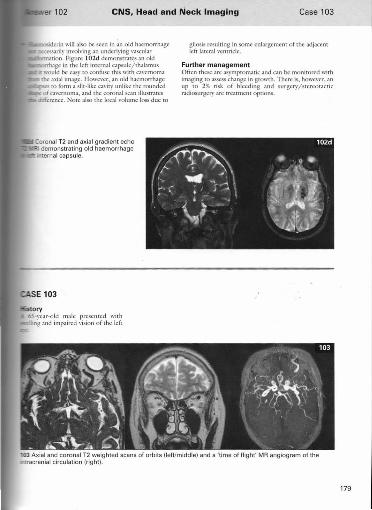
ation. Figure l02d dcmonSlrarts an old age in the kft imernal capsule/thalamus
.. would be cas}' to confuse this with c;;wcrnoma the axial image. Howe"er, all old haemorrhage
to form ::I slit-like cavity unlike the rounded of cavernoma, and the coronal scan illustr.n cs
difference. NOte also the local \'olume loss due to
gliosis resulting in some enlargemen t orlhe adjacent [cft [atcra] vcntridc.
Further management Often these arc aSYffipromatic and call be monitored with imaging to 3SSCSS change in growth. There is, however, an up to 2% risk of bleeding and surgcry/slcrcoractic radiosurgery arc treatment options.
03 Axial and coronal T2 weighted scans of orbits (left/middle) and a 'time of flight' MR angiogram of the rluacranial circulation !right),
179
180
Answer 103 eNS, Head and Neck Imaging
ANSWER 103
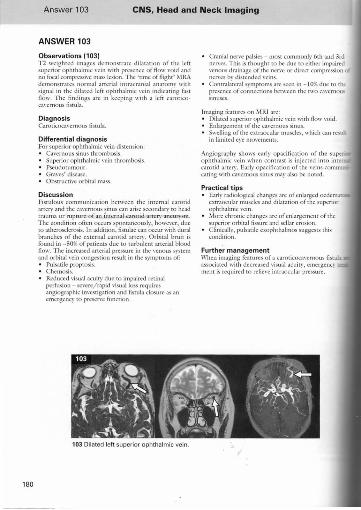
Observations (103) T2 weighted images demonstrate dilatation of the left superior ophthalmic vein \\'ith presence of flow \'oid and no focal compressi\'e mass lesion. The "time of flight' MRA demonstrates normal arteri:!l intracranial anatOIlW \\'ith signal in the dilated left ophthalmic \"cin indicatil;g f.m flow. The find ings arc in keeping with a kft caroricoC;ll'crnousfisrub.
Diagnosis CaroriCOC3'I'CrIlOUS fistub.
Differe nti a l diagnosis For superior ophthalmic rein distension: • Ca"ernous sinus thrombosis.
Superior ophthalmic "ein thrombosis. Pseudotllmour. Graves' disease. Obstructi,'c orbital mass.
Discu ssion Fistulous communication betweell the internal carotid artery and the ca"ern?us ~inus can ariS<,' secondary to head trauma or rupture 01 an mternal caroud artery aneurysm, The condition olien occurs spontaneously, however, due [0 atherosclerosis. In addition, fisllllae can occur \\ith dural branches of the external carotid artery. Orbital bruit is found in - 50% of patients due to turbulent arterial blood flow, T he increased arterial pressure in the l'e!lOllS system and orbiral "cin congestion result in the symptoms of: • Pulsatik proptosis.
Chemosis. • Reduced visual acuity due to impaired retinal
perfusion - scvere/ rapid visual loss requires angiographic im'cstigation and listula closure as an emergency (0 preserve function.
103 Dilated left superior ophthalmic vein.
Cranial nerve palsies - most commonly 6th and 3rd nervcs. This is thought to be due to either impaired \"cnous drainage of the ncn"c or direct compression Ilcr'I'CS bv distended ' "cins. Contral~tcraJ srmptoms arc secn in - 10% duc to [h~ presence of conllcniOtls between the two GI\"ernous sinuses.
Imaging features on h'IRI arc: • Dilated superior ophthalmic vcin with flow ,·oid.
Enlargement of the ea,'ernous sinus. • Swelling of the extraocular muscles, which can rcsuli
in limited ere mo,·ements.
Angiograph~' shows c;\fly opacification of the supe ophthalmic rein when contrast is injected into intc carotid artery. Earl~' opacification of the veins C011llTI
eating with cavcrnous sinus may also be noted.
Practical tips Early radiological changes arc of enlarged ocdemat extraocular muscles and dilatation of the superior ophthalmic I·cin. More chronic changes arc of eniargeillent of the superior orbital tissure and scll:ar erosion. Clinically, pulsatile exophthalmos susgeslS this condition.
Further management When imaging features of a caroticQCa"ernous fistu.b associated with decreased "isua! acuit,)" cmergency mcnt is required to relieve intraoclllar pressure.
eNS, Head and Neck Imaging Case 104
181
182
Answer 104 eNS, Head and Neck Imaging
ANSWER 104
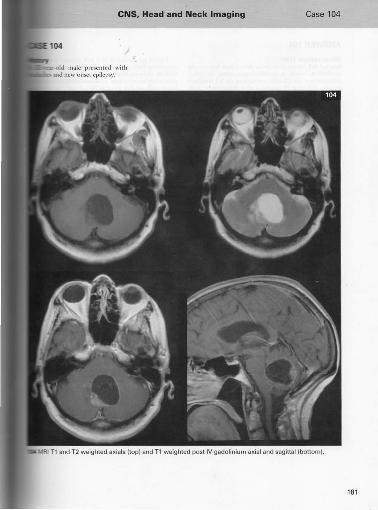
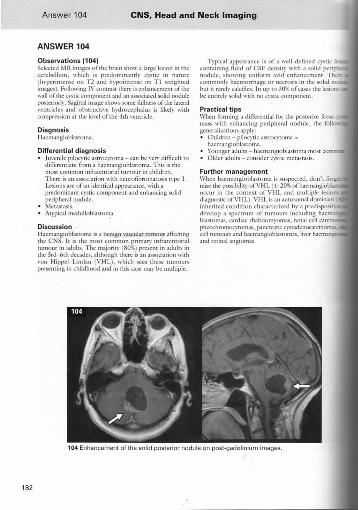
Observations (104) SeleCTed '\'IR images ofthe brain show a large lesion in the cerebellum, which is predominantly cystic in narure (hn>erimcnsc on T2 and hypoimensc on Tl weighted images). Following IV colltrnsr there is cnhancemcm oftlle \\':1.11 of the cystic component and an associan:d solid nodule posteriorly. S.1gittal image shows some filllncss of the btcral "cmridcs and ObStTUcri\'c hydrocephalus is likely with compression at thc level of the 4th '·(lUride.
Diagnosis Hacmangioblastoma.
Differential diagnosis • Juvcnilc pilocytic ;lstrocytoma - can be "cry difficult to
diflcrentiatc from a haeillangioblastonll. This is the mOSt COlllnlon infratentorialtulllour in children. There is an association wi th ncurofibromatosis typc I , Lesions arc of an ident ical appearance, with a predominant cystic component and enhancing solid peripheral nodule. Metastasis. Arypical mcdulloblastoma,
Discussion H aemangioblastoma is a benign vascular rumoull aflccting the CNS. It is the most common primary infratemorial nUllour in adults. The majority (80%) present in adults in the 3rd-6th decades, although there is an association '\ith "on H ippel- Lindau (V HL), which sees these tumours presenting in childhood and in this case may be multiple.
Typical appearance is of a well defined cystic I containing fluid of CSF density with a solid perip nodule, showing uniform a"id enhancement. Th~ commonly haemorrhage or necrosis in the solid n but it rarely calcifies. In up to 30% of cases the lesions be emird)' solid wilh no cystic component.
Practical tips When forming a differential for the posterior fossa mass with enhancing peripheral nodule, the foil generalizations apply: • Children - piloc)'tic astrocytoma>
hacmangioblutoma. • Younger adults - hacmangioblasroma most com • Older adults - consider cystic mctaS[3sis
Further management When haemangioblastoma is suspected, don't forg:... raise the possibility o f VH L (4-20% of haemangiob occur in the COllleX I of VH L and multiple lesi diagnostic ofVI-IL). VH L is an autosomal dominant inherited condition characterized
develop a spectrUl:n:~:o~rl :~"'::~m:~o~"~,~,: i~~::~~~j~i~:~: blastomas, cardiac pheochromocytomas, pancreatic I cell mmours and haemangioblaslomas, li"er and retinal angiomas.
104 Enhancement of the solid posterior nodu le on post-gadolinium images.
eNS. Head and Neck Imaging Case 105
183
184
Answer 105 eNS. Head and Neck Imaging
ANSWER 105
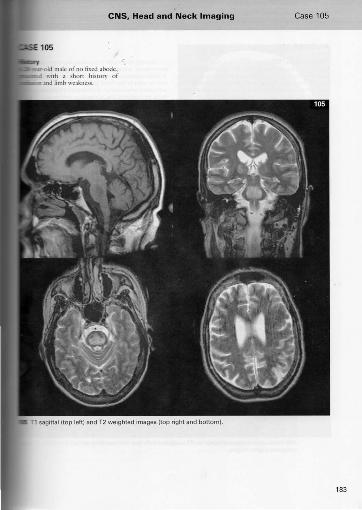
Observations (105) The selected images demonstrate diffuse cerebral atrophy exceeding that cxptctcd for the patient's young age. There is:I large focal area of signal abnonm.liry in the central pons Ih:1I is hyperintense on T2 weighted and hypointcnsc on TI wei glued sc:ms. 111crc is no associated mass effect. The signal changes would fil with central pontine myelinolysis and the clinical dCt3i1S and cerebral atrophy suggest that chronic alcohol abuse may Ix the underlying cause.
Diagnosis Central pontine myelinolysis.
Differential diagnosis • Pondnc glioma. • Inf.,rcrion.
Discussion Central ponline myelinolysis results from the destrllction of m~'c1in sheaths, dassicall~' in patients with rapidly corrected hypon:t tracmia. Cases are reported in patients with: • Chronic alcohol abuse. • Chronic liver d isease. ' • $c"ere m::alnutrition. • Wilson's disease, chronic rell::al fitilure, diabetes, acute
m)'clogcnous leukaemia .
In the c::ase demonstrated there is diffilse glob::al (erebral ::atrophic ch::ange suggestive of chronic alcohol abuse.
Clinically this results in pseudobulbar palsy, terraplc~ cOll\'uisioIlS, acute confusion and progression to comL is mOSt commonly confined to the pons but changes also be secn in the basal b>;lnglia, caudate, thalamus suocortkal white matter. Radiological presentation is fairly wdl defined low attenuation lesions on CT in central pons. On M IU, lesions aTe oflo\\' intensity on and high signal imensity on T2 imaging.
Practica l tips Standard MR/CT im::aging (::an be normal for up to days after symptolll onset, lagging considerably behind clinical presentation. Rest ricted diffusion on D however, is found wirhin 24 hours.
Further management • Early MIU appearances can be similar for a b::asibr
inElrcr and M RA (::an be useful to look for :lrteri,;d thrombus.
• Sc::arch for underlying cause if not readily app::arcOL
Further reading Ruzek KA, Campe::all NG, Miller GM (2003 ). Earf!;
diagnosis of central pontine myelinolysis with diffusion-weighted imaging. American JOllnHlJ Nmrorndiolo!JY25: 210-213.
Stadnik nv, Demaerd P, Lurpaert RR., It nl. (200.; Imaging tutori::al: differemi::al di::agnosis of bright lesions on diffusion-weighted MR images. RadioGraphies 23(1): e7.
105 Focal area of reduced Signal on T1 weighted (left) and increased signal on T2 weighted (right) images.
eNS, Head and Neck Imaging
-old fCIll:a1c patient prescnted clles.
Cases 106, 107
185
186
Answer 106 eNS, Head and Neck Imaging
ANSWER 106
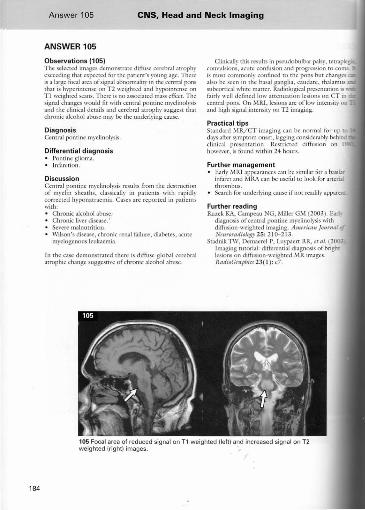
Observations (106a ) This non contrast enhanced cr image demonstrates a large midli ne mass extending into the 3rd ventricle, which hlS
both solid :lIld cystic compOllcnrs with central calcitication. There is dibtation orthe temporal and anterior horns of the "cntridcs but normal :tppcarancc to the 4th ventricle findi ngs arc in keeping with obstructive hydrocephalus at the lc,"el of the. 3rd ventricle secondary to a mass lesion. The mixed density and calcification arc \ '(1)' suggcstive of a craniopharyngioma and M IU is suggested to further e"aluate.
Diagnos is Craniopharyngioma.
Differential diagnos is or suprascllar/intrascllar mass lesion: • Pituitary macroadcnoma. • Craniopharyngioma • R.1thke cleft cysr.
Other masst:s in the sellar region include meningioma, metastases, chordoma and intenla!l'arOlid mer)' aneurysm.
Pituitary macroadenor{KI is the most common lesion involving the sellar and suprasellar regions. Microadenol1las (20%) an: defined as being less [han 10 mm in size and usu:llly present with sympl"Oms due to hormonal secretion. Macroadcnoll1as (80%) measure over 10 mill in size and arc usually endocrinologieally inaeri,'e. The~' present with symptoms secondary to mass effeer such as hydrocephalus, bitemporal hemianopia from optic chiasm compression, involvement of cranial nerves tr:wdling in the adjacent
c,wcrnolls sinus ( 3, 4, 53 and 6 ) and hypopitui resulting from compression of normal pituitary tissue
Compared to craniopharyngioma, pitu itary adenomas arc predominantly solid and show morc i uniform enhancement. Calcification is rare, craniopharyngioma. Suprasellar ex tension produca 'snowman' configuration due to w:lining at the I the diaphragm sellae. Figure I 06b shows prc- and contrast Tl weighted images of a pituitary macroa with such features.
lbthkc deft cyst is the other main diAcrcntiai di.a_ wi th 70% in\"olving sellar and suprasellar regions. benign cySt arising from remnants of Rathke's pouu can be differentiated by the following features' regular and ovoid shape, smaller size (<2 !TIl ), cystio;: 110, or minimll cnh:lllccmcnt ofthe thin wall.
Discussion Craniopharyngioma account for - 4% of int neoplasms, with a slight predominance in males, peaks ofincrcascd incidence: • Firstly in children in 1st-2nd decades, Wh("fC
account for 50% of suprasellar turnouTS. • Secondly in adults in 5th - 6th decades.
These arc benign tumours arising fro m rem 111thke's pouch. They grow from a suprasellar ori_ the base of the 3rd vemricle. lmr:lsel lar extension in 2 1%. Involvement of the bon)' sella can be seen radiographs and o n CT bOlle window imag("S demonstrate appearances or J-shaped sella , enl and then ultimately erosion and destnJcrion.
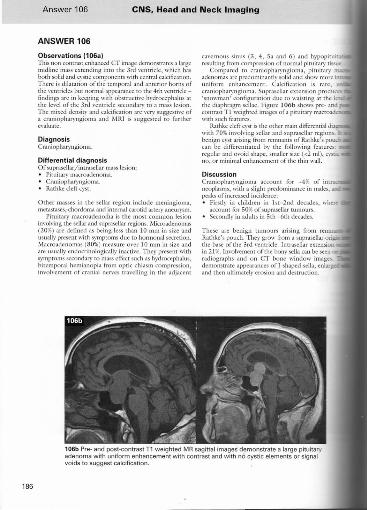
106b Pre- and post-contrast T1 weighted MR sagittal images demonstrate a large pituitary adenoma with uniform enhancement with contrast and with no cystic elements or signal voids to suggest calcification.
106 eNS, Head and Neck Imaging
IT appcar,lIlccs arc 5ho'l\'11 in this casc \\;th ,,:ystic clements and calci fi cuion (which is
-90% of cases). Following comrasl there is amen! of the solid compOllcnrs and the CYSt
.\tRI findings reflect CT features with a cystic InCn! following fluid signal (although high >my be seen on Tl weighted images depending Jttin/ blood content). The solid componcm is
on T 1 and shows cnhancclllcllI with
106c shows '1'1 sagittal pre- and post-IV contrast d T2 axial and 53gitt.l l images (left). These
.I Lu-gc suprasellar lesion with intnsclb.r extension. solid and C}'stic clements wj th enhancement of component'S and cyst wall. Complications of
'C hydrocephalus, pituitary st;}lk and optic chiasm n can be appreciated.
Practical tips Look for the complications of masslcsions in this area: • H ydrocephalus :lIld optic chiasm compression. • Lateral extension to invoke thc cavcrnous sinus (seen
in up to 10% of pituitary macro~dcnoma.s) , which can lead to thrombosis :lIld cranial nervc palsy. Lateral extension beyond the lateral wall of the internal carotid is rare wilh Rathke eleft cySt :lnd may help diflcremi:lte it frolll the other two conditions listed.
Fu rthe r management Treatment is surgical +/- posropcrath'e radiotherapy.
Further reading Choi SH , Kwon 81, Na DG, ct al. (2007). i'imitary
adenoma, craniopharyngioma, and Rathke cleft cyst ilwolving both intr.tsellar :lIld suprasellar regions: ditlcrcntiation llsing 1-Ht!. CIi"icn! Radio!ogy62: 453-462 .
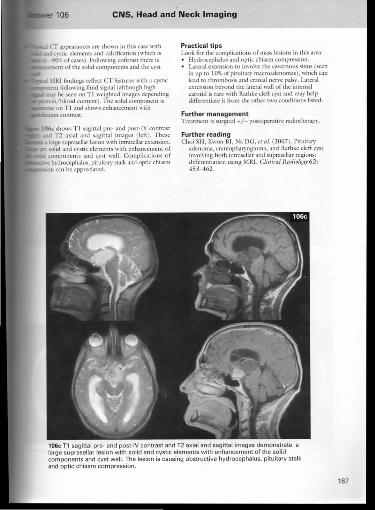
106c T1 sagittal pre· and post-IV contrast and T2 axial and sagittal images demonstrate a large suprasellar lesion w ith solid and cystic elements with enhancement of the solid components and cyst wall. The lesion is causing obstructive hydrocephalus, pituitary stalk and optic chiasm compression.
187
188
Answer 107 eNS. Head and Neck Imaging
ANSWER 107
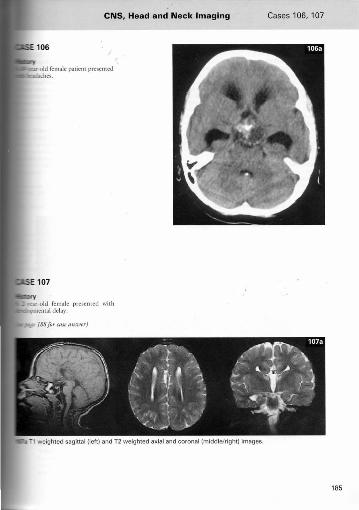
Observat ions (107a) T1 sagittal and T2 axial and coronal images of the brain dcmonsu':uc: complete :agenesis of the corpus callosum \\ith no callosal [issue identified. There is increased separation of the 13tcral \'cmodes on the a.xial images crc;uing a 'b:J.t's wing' appear-uKe. Coronal image demonstrates clc\'3tion of the 3rd ventricle .
Diagnosis Agenesis ofthc corpus callosum.
Discussion The corpus callosum usually develops by 20 \\'ccks' gestation. The genu and the body of the. corpus callosum develop first and the posterior bod)' and spleniulll develop b ter. The rostrum is the last part of the corpus callosum TO
develop. Idcntil}'i ng the parts of the corpus callosuill present call help to diflcrcntiatc octwccn dysgenesis (absent genu/splenium ) and destruction, most commonly dlll~ 10 ischaemia (genu present but may be atrophic ). Corpus callosal agenesis is usually associated with reduced intellectual function and can be associated with a varier\' of c;NS abnormalities in~ludin~ hydr~ephal.us, mid[il~e itpoma , Oandy- 'Valker cySts, mterheilltsphenc arachnOId cysts, neuronal migration disorders and Arnold- Chiari malformation.
Classical imaging appearances on CT/M IU arc with: ' Bat 's wing' appcar""Jnce of the lateral ,'entriclcs due to parallel lateral "entricles with marked separation (107b). ' High riding' 3rd ventricle - can be seen at the b 'd of the Jateml ventrieles. Enlarged foramen of t-.'ionro.
Prenatal detection can be made by US investigatic.. Diagnosis cannot usually be made before 22 wee gestation. Equivalelu image findings arc of: • Absence ofthe septum pdlucidum. • Dilated/elevated 3rd ,·cnrricle. • Enlargement of the occipitJI horns of the lateral
,·cntrides.
Practica l t ips Ditlcrentiating bcrween dysgenesis and ischacmie da is done b~' de("ermining which parts of the corpus call arc abnormal. With ischaemie injury the rostrum nill present but :ltrophic.
Fu rther management Somctimcs this fin ding is made incidentally on imaging in later lire and no fu rther in\·estigatiOD required.
Fu rther reading Babcock OS ( 1984). The normal, absent, and abno
corpus callosum: sonographic findings. Rndioio..!!! 15 1: 449-453.
Oa\'idson HO, Abraham R, Steiner RE ( 1985). of the corVllS callosum: magnetic resonance Rndiolog., 155: 371 - 373.
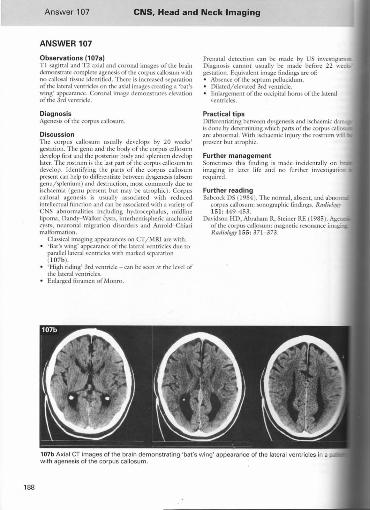
107b Axial CT images of the brain demonstrating 'bat's wing' appearance of the lateral ventricles in a with agenesis of the corpus callosum.
eNS, Head and Neck Imaging Case 108
189
190
Answer 108 eNS, Head and Neck Imaging
ANSWER 108
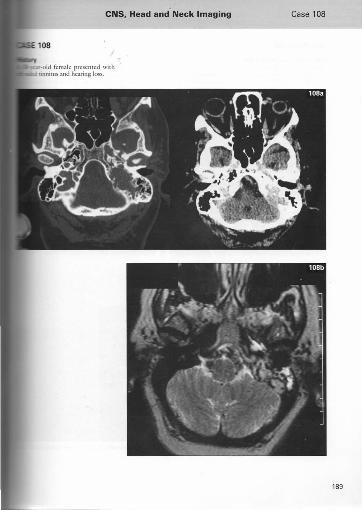
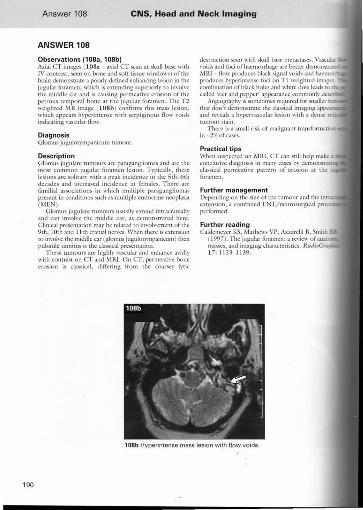
Observations (108a. 108b) Axial CT images (1 08a - axial C T scaJl at skull base with IV contrast, seen on bone and soft tissue windows) oflbe brain demonstrate a poorl}' defined enhancing lesion in the jugular foramen, which is extending superiorly to in\'ol\'e rhe middle car and is causing permeative erosion aflbe pClrous temporal bone at the juguhlf foramen. The T2 weighted MR image ( l OSb) confi rms this mass lesion, which appears hrpcrintcnsc with serpiginous flow ,ooids indicating vascular flow.
Diagnos is Glomus jugulorymp::lIlicum tumour.
Description Glolllus jugulare rulllOUrs afC paragangliomas :lIld afC rhe most common jugular foramen lesion. Trpically, these lesions arc soliury with a peak incidence in the 5th-6th decad es and increased incidence in females. There are fumi lial associations in which multiple paragangliomas present in conditions such as multiple endocrine neoplasia (MEN).
Glomus jugubre rumours usually extend imracranially and can inl"oh·e the middle car, as demonstrated here. Clinifal presentation ma), be related to illl·oll'cment oCthe 9th, 10th and 11 th cranialnervcs. When there is extension to im"oh"e the middle ear (glomus jugu10tympanicum) then pulsatile tinnitus is the classical presentation.
These tumours arc highly vascular and enhance al·idly wi th contrast on CT and MRI. O n CT , permeati\"(: bone erosion is classical, differing from the coarser lytic
destruction seen with skull base metasuses. Vasculu ,ooids and foci of haemorrhage are beller demonstnt MRI - flow produces black signal I"oids and haem produces hyperintensc foci on T I weighted images combination of black holes and white dots leads to
called 'salt and pepper' aplXlrance commonly dcscril Angiography is sometimes required for smaller
that don't demonstrate the classical imaging appe and rel"eals a hypcr\'ascular lesion with a dense mmourstain.
The re is a small risk of maligna nt transfo rmaci in -2% of cases.
Practica l tips When suspected on MRI , cr can still help make.a conclusive d iagnosis in many cases by demonstra classical permeati,", pattern of erosion at the foramen.
Further management Depending on the size of the tumour and the in extension, a combined ENT / neurosurgieal proc pcrfomled.
Further reading Caldemeyer KS, l'-'la thews vr, AzzarclJi B, Smith
( 1997). The jugular foramen: a rC\"1cwofan;a[ masses, and imaging ch:aracteristics. RadinG,.. 17: 11 23- 1139.
108b Hyperintense mass lesion with flow voids"
eNS, Head and Neck Imaging Case 109
191
192
Answer 109 eNS, Head and Neck Imaging
ANSWER 109
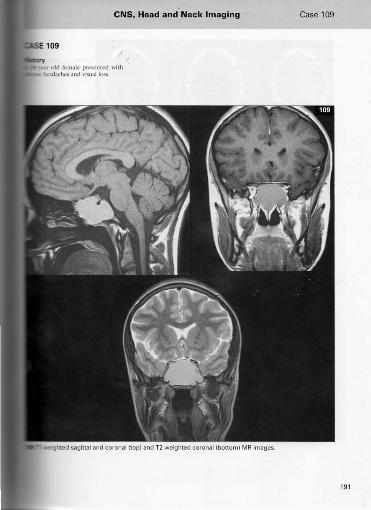
Observations (109) These sclcclcd MR im3gcs show an expanded sphenoid sinus filled with abnormal signal rather th:a11 air. The (amelUS show mild uniform hyperintcnsiry on Tl weighted and T2 weighted images. The walls of the sinus :appear slllomh and intJct with no ob\iou$ evidence of dcstmctiOIl. The findings arc consistent with a mucocele of the sphenoid si nus, the signal indicative ofprotcinaccolls fluid contents. Sagin;)'l Tl and coronll 1'2 inl:lgcs dcmonstr:I\C displacement of the optic nerves br the expanded sinus, presumably causin g compression of the atHl:rior optic pathway gi\'en the hiSTOry of\'isuaJ disrurbance.
Diagnosis Sphenoid sinus mucocele
Discussion A mucocele arises due to chronic obstruction of a sinus, which then becomes filled with mucus. This collection acts like a slow growing mass c:lUsing expansion of sinus bony walls withom frank bOil\' dl:slruction. Vessels and other srmcrures arc displaced ";ther than being encased, as with a tumour. Usually these lesions are asyrnptomaric untillhcy becomc large when the}' can cause optic nel""\'C compression, proprosis and headache. Secondary infection of the mucocele can supen'ene, but this is a rare complication. Ninet), per cent of lesions arc found in rhe frontal and ethmoid sinuses with sphenoid sinus rnucocdes being anI}' rarely seen.
Appc:ar.mccs on MRJ :lrC \'3rbbk depending 011 fluid/ protein CQrHcnt of the mucocele but impo imaging findings arc of a nondcstructi\·c, slow gra ... lesion.
Practical tips CT is good lor showing bony expansion with the absellce of bone erosion.
• ~'IlU is good for identil)'ing the exrelll/size of tile lesion and looking for complications of optic nel'\c compression (usually from postcrior ethmoid lesi<and proptosis ( usuall~' from frontal and anterior ethmoid sinuses). Tl hypcrintensity \\ithin a lesion on an~' MRI s often helps to rnpid1r limit the diAcrential diagn there are;\ limited number of things that arc brig.I:K on TI imaging, i.e. fat, blood, proteinaceous f1uiQ. paramagnetic contrast agents.
Further management Referral to ENT for consideration of endoscopic surgery.
109 Superior displacement of optic nerve (left); lateral displacement of cavernous sinus by large sinus mucocele (right).





























