Embed Size (px)
Citation preview
Pharmacokinetics: A Refresher
Pharmacokinetics: A RefresherCurtis L. Smith, Pharm.D., BCPS Ferris State University Grand Ledge,
Michigan© 2008 American College of Clinical Pharmacy
1-187

Pharmacokinetics: A Refresher
Learning Objectives:
1. Identify and provide examples using basic pharmacokinetic concepts commonly used in clinical practice, including elimination rate constant, volume of distribution (Vd), clearance, and bioavailability.
2. Describe specifi c pharmacokinetic characteristics
of commonly used therapeutic agents.
3. Defi ne important issues as they relate to drug
concentration sampling and interpretation.
Self-Assessment Questions: Answers to these questions may be found at the end of this chapter.
1. J.H. is a 65-year-old woman (65 kg) who was recently started on tobramycin and piperacillin/ tazobactam for treatment of hospital-acquired pneumonia. After the fi rst dose of tobramycin 120 mg (infused from noon to 1:00 pm), serum tobramycin concentrations are drawn. They are 4.4 mg/L at 3:00 pm and 1.2 mg/L at 7:00 pm. Which one of the following statements is true regarding the tobramycin? A. There are suffi cient data to determine the
half-life (t
1/2
© 2008 American College of Clinical Pharmacy
1-188
congestive heart failure and is fl uid overloaded due to her diminished renal function and nonadherence with her angiotensin-converting enzyme inhibitor and diuretic. A few days into her hospitalization, her SCr is down to 1.1 mg/dL, and she has been restarted on her furosemide and enalapril. Which one of the following probably happened to the gentamicin half-life in R.O. during her hospitalization? A. Her clearance increased, which increased
her Vd and decreased her t1/2. B. Her clearance increased, which increased
her elimination rate constant and decreased her t1/2. C. Her Vd decreased, which increased
her clearance and decreased her t1/2. D. Her Vd decreased, which increased
her elimination rate constant and increased her t1/2.
4. A patient who is receiving vancomycin 1000 mg IV (for 1 hour) every 24 hours has serum concentrations drawn 1 and 23 hours postinfusion, which are 40 mg/L and 3 mg/L, respectively. Which one of the following regimens would be best for this patient? A. Maintain the dose at 1000 mg IV every 24
hours. B. Lower the dose, but keep the interval at every
24 hours. ) but not the VD. B. There are suffi cient data to determine
C. Keep the dose at 1000 mg, but shorten the
interval to every 12 hours. D. Lower the dose, and shorten the interval to C. every 12 hours.
5. A 40-year-old, 60-kg woman who smokes presents to the emergency department at 2:00 pm with an acute exacerbation of asthma. She takes theophylline sustained release 300 mg 2 times/day, with the last dose taken at 9:00 that morning. Her theophylline concentration soon after presenting to the emergency department is 7.0 mg/L. She is stabilized and is to be sent home on theophylline sustained release. Which one of the following options is the best regimen for this patient? A. Theophylline sustained release 300 mg by
mouth (PO) every 12 hours. B. Theophylline sustained release 600 mg PO
every 12 hours. C. Theophylline sustained release 400 mg PO
every 8 hours. D. Theophylline sustained release 600 mg PO
every 8 hours. both There the are t
1/2
insuffi and VD.
cient data to determine D. either There the are t
suffi 1/2
or cient the VD.
data to determine the V
d
but not the t
1/2
.
2. P.L. is a 60-year-old woman (60 kg) who was recently started on gentamicin and clindamycin. After the fi rst gentamicin dose of 110 mg (infused from 6:00 to 6:30 pm), serum gentamicin concentrations are drawn. They are 3.6 mg/L at 7:30 pm and 0.9 mg/L at 11:30 pm. Which one of the following best describes this patient’s gentamicin pharmacokinetic parameters? A. B. The t
1/2
is about 2 hours. C. The The t
maximum 1/2
is about concentration
3 hours.
is about 3.8 mg/L. D. The V
d
is about 11.6 L.
3. R.O. is a 74-year-old woman started on gentamicin 100 mg intravenously (IV) every 24 hours for pyelonephritis. On admission, her serum creatinine (SCr) is 1.8 mg/dL. She also has

Pharmacokinetics: A Refresher
© 2008 American College of Clinical Pharmacy
1-189 6. L.R. is a 49-year-old patient with diabetes and
of the following statistical tests will need to be renal failure. He was recently in a car accident
employed to assess the relationship? and sustained head trauma. He is currently receiving phenytoin 100 mg IV 3 times/day, and his most recent concentration was 5.6 mcg/mL. You are asked to suggest a new dose to achieve a concentration within the therapeutic range.
A. One-way analysis of variance. B. Analysis of covariance. C. Multiple logistic regression. D. Spearman rank correlation.
Current laboratory results include sodium 145, potassium 3.9, clearance 101, carbon dioxide 26, blood urea nitrogen (BUN) 95, SCr 5.4, glucose 230, and albumin (Alb) 2.8. Which one of the following choices is your recommendation? A. Increase the dose to 200 mg IV 3 times/day. B. Increase the dose to 200 mg IV 2 times/day. C. Decrease the dose to 100 mg IV 2 times/
day. D. Keep the dose the same.
10. N.T. is a 24-year-old woman currently receiving valproic acid for tonic-clonic seizures. Her most recent trough valproic acid concentration was 22 mg/L. Her most recent Alb concentration was 4.1 g/dL. Based on this serum concentration, which one of the following recommendations would you make concerning her dose? A. Continue with the current dose; the concentration is close enough to the therapeutic range.
7. You are asked how the TDx (fl uorescence polarization immunoassay) and EMIT (enzyme multiplied immunotechnique) assays compare with each other. Which one of the following statements is most accurate?
B. Assess compliance and increase her dose; the concentration is below the therapeutic range. C. Decrease her dose; the concentration is
slightly above the therapeutic range. D. Assess compliance and then check a free A. Although both are immunoassays, one labels
valproic acid concentration and adjust antibody, whereas the other labels antigen.
accordingly. B. Although both are immunoassays, one uses antibody as a marker, whereas the other uses a radioisotope. C. Although both are immunoassays, one uses an enzyme label, whereas the other uses a fl uorescent label. D. They are both names for the same assay
technique.
8. An elderly patient is seen in the morning medicine clinic for a routine follow-up. Medication history includes digoxin 0.25 mg/day PO, furosemide 40 mg/day PO, and potassium chloride 10 mEq/ day PO. All doses were last taken at 8:00 am today at home. The patient has vague complaints of stomach upset, which began 2 days ago, but is otherwise in no apparent distress. A serum digoxin concentration drawn today at 10:00 am is 2.5 mcg/L. Which one of the following statements best describes what should be done next? A. Admit the patient for administration of
digoxin Fab. B. Tell the patient to skip tomorrow’s dose of
digoxin and begin 0.125 mg/day PO. C. Administer a dose of activated charcoal. D. Do nothing today regarding the digoxin.
9. A research group is analyzing the relationship between various patient demographics (e.g., age, height, weight, Alb, creatinine clearance [CrCl]) and phenytoin pharmacokinetics. Which one

Pharmacokinetics: A Refresher

Patient Cases 1. H.R. is receiving vancomycin for a methicillin-resistant Staphylococcus aureus bacteremia. H.R. has chronic renal failure. A 1-g IV dose of vancomycin is given at noon on March 21. A concentration drawn at 2:00 pm on March 21 is 23.8 mcg/mL. A concentration drawn at 2:00 pm on March 24 is 12.1 mcg/mL. If you were to give a dose at 4:00 pm on March 24 and your goal trough concentration is 10–15 mg/L, when would you need to give the next dose? A. 1 day after the dose on the 24th. B. 3 days from the dose on the 24th. C. 6 days from the dose on the 24th. D. There is not enough information to calculate when to redose.
2. After the administration of 100 mg of a drug IV and 200 mg of the same drug PO, the areas under the curves
are 50 mg/L/hour and 25 mg/L/hour. Which one of the following is the bioavailability of this drug? A. 25%. B. 37.5%. C. 50%. D. 100%.
3. An infusion of 20 mg/hour of theophylline is started. What would the serum concentration be at 48 hours if
the t
1/2
of the drug were 4 hours and the V
d
were 0.5 L/kg (your patient weighs 65 kg)? A. 3.6 mg/L. B. 5.0 mg/L. C. 18.2 mg/L. D. 30.4 mg/L.
I. BASIC PHARMACOKINETIC RELATIONSHIPS
A.
Absorption F = Doseiv * AUCevDoseev * AUCiv
B.
Distribution Rapid IV (or oral) bolus: V d
=
F * dose Cp0
Continuous IV infusion at steady state: Vd
© 2008 American College of Clinical Pharmacy
1-190
R k * CContinuous IV infusion before steady state: Vd
=0
ss
=
C R * 0
k(1 − e−kt) and C =
R0 V d
* k(1 − e−kt)

Pharmacokinetics: A Refresher
Multiple IV (or oral) bolus at steady state: V
d
=
F * Dose C ss
max * (1 − e− k
τ )Multiple IV (or oral) infusion at steady state: Vd
© 2008 American College of Clinical Pharmacy
1-191
1 −
e− kt
′
C max −
(C min
* e − kt
′
)Css
max =
F * Dose V d
* (1 −e − k
τ ) Css
min =
F * Dose V d
* (1 −e − k
τ )
* e− k
τ

C.
Clearance Clearance = k =d
=
F * Dose k*
Dose AUC
Cl Vk =
(ln C 1 −
ln C 2
) (t 1 −
t 2
)t1/2
=
0.693 k
Continuous IV infusion at steady state: Clearance =
C RContinuous IV infusion before steady state: Clearance =0
ss
R
0 C
* (1 −e − k
τ )Multiple IV (or oral) bolus at steady state: Clearance =
F * C
Dose/ss-avg
τ
τ =
(ln C max −
ln C min
) kC1
= C0
* e−kt
II. ABSORPTION
A.
First-pass Effect 1. Blood perfusing virtually all the gastrointestinal tissues passes through the liver via the
hepatic portal vein. a. Fifty percent of the rectal blood supply bypasses the liver (middle and inferior
hemorrhoidal veins). b. Drugs absorbed in the buccal cavity bypass the liver. 2. Drugs affected most by the fi rst-pass effect are those with a high hepatic extraction ratio.
Pharmacokinetics: A Refresher
3. Examples:
Amitriptyline Desipramine Diltiazem Doxepin Imipramine Isosorbide dinitrate
© 2008 American College of Clinical Pharmacy
1-192 Labetolol Lidocaine Metoprolol Morphine Nicardipine Nifedipine
Nitroglycerin Pentazocine Propoxyphene Propranolol Verapamil
B.
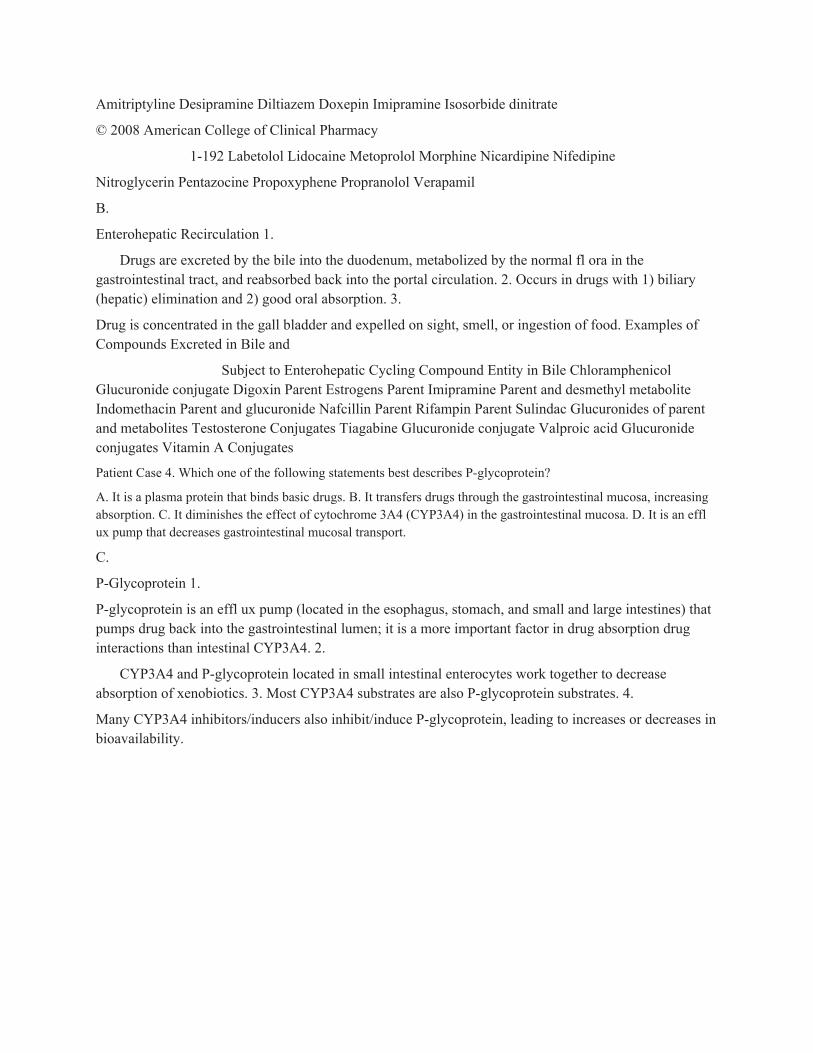
Enterohepatic Recirculation 1.
Drugs are excreted by the bile into the duodenum, metabolized by the normal fl ora in the gastrointestinal tract, and reabsorbed back into the portal circulation. 2. Occurs in drugs with 1) biliary (hepatic) elimination and 2) good oral absorption. 3.
Drug is concentrated in the gall bladder and expelled on sight, smell, or ingestion of food. Examples of Compounds Excreted in Bile and
Subject to Enterohepatic Cycling Compound Entity in Bile Chloramphenicol Glucuronide conjugate Digoxin Parent Estrogens Parent Imipramine Parent and desmethyl metabolite Indomethacin Parent and glucuronide Nafcillin Parent Rifampin Parent Sulindac Glucuronides of parent and metabolites Testosterone Conjugates Tiagabine Glucuronide conjugate Valproic acid Glucuronide conjugates Vitamin A Conjugates
Patient Case 4. Which one of the following statements best describes P-glycoprotein?
A. It is a plasma protein that binds basic drugs. B. It transfers drugs through the gastrointestinal mucosa, increasing absorption. C. It diminishes the effect of cytochrome 3A4 (CYP3A4) in the gastrointestinal mucosa. D. It is an effl ux pump that decreases gastrointestinal mucosal transport.
C.
P-Glycoprotein 1.
P-glycoprotein is an effl ux pump (located in the esophagus, stomach, and small and large intestines) that pumps drug back into the gastrointestinal lumen; it is a more important factor in drug absorption drug interactions than intestinal CYP3A4. 2.
CYP3A4 and P-glycoprotein located in small intestinal enterocytes work together to decrease absorption of xenobiotics. 3. Most CYP3A4 substrates are also P-glycoprotein substrates. 4.
Many CYP3A4 inhibitors/inducers also inhibit/induce P-glycoprotein, leading to increases or decreases in bioavailability.
Pharmacokinetics: A Refresher
5.
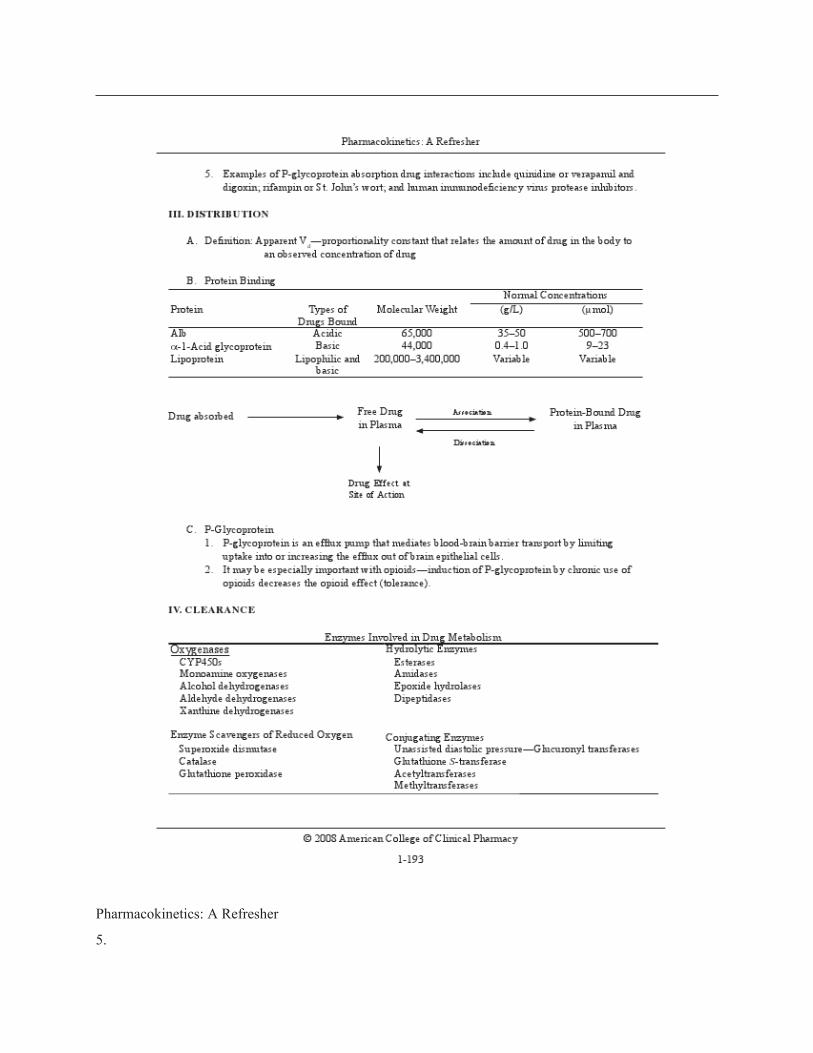
Examples of P-glycoprotein absorption drug interactions include quinidine or verapamil and digoxin; rifampin or St. John’s wort; and human immunodefi ciency virus protease inhibitors.
III. DISTRIBUTION
A. Defi nition: Apparent an observed Vd
—proportionality concentration of constant drug
© 2008 American College of Clinical Pharmacy
1-193
that relates the amount of drug in the body to
B.
Protein Binding Normal Concentrations Protein Types of
Drugs Bound
Molecular Weight (g/L) (μmol)
Alb Acidic 65,000 35–50 500–700 α-1-Acid glycoprotein Basic 44,000 0.4–1.0 9–23 Lipoprotein Lipophilic and
basic
200,000–3,400,000 Variable Variable
Drug absorbed
Free DrugAssociation
Protein-Bound Drug in Plasma
in PlasmaDissociation
Drug Effect at Site of Action
C.
P-Glycoprotein 1.
P-glycoprotein is an effl ux pump that mediates blood-brain barrier transport by limiting uptake into or increasing the effl ux out of brain epithelial cells. 2.
It may be especially important with opioids—induction of P-glycoprotein by chronic use of opioids decreases the opioid effect (tolerance).
IV. CLEARANCE
Enzymes Involved in Drug Metabolism Oxygenases Hydrolytic Enzymes
CYP450s Esterases Monoamine oxygenases Amidases Alcohol dehydrogenases Epoxide hydrolases Aldehyde dehydrogenases Dipeptidases Xanthine dehydrogenases

Enzyme Scavengers of Reduced Oxygen
Conjugating Enzymes Superoxide dismutase Unassisted diastolic pressure—Glucuronyl transferases Catalase Glutathione S-transferase Glutathione peroxidase Acetyltransferases
Methyltransferases
Patient Case 5. A renal transplant patient currently receiving cyclosporine is diagnosed with a community-acquired pneumonia. The patient is admitted to the hospital and started on ceftriaxone and a macrolide. Which one of the
following macrolides would be the least likely to interact with cyclosporine? A. Erythromycin. B. Clarithromycin. C. Azithromycin. D. All of the macrolides inhibit CYP3A4.
A.
Cytochrome P450 1. Introduction
a. A group of heme-containing enzymes responsible for Phase 1 metabolic reactions b. Characteristic absorbance of light at 450 nm (thus CYP450) c.
Primarily located in the membranes of the smooth endoplasmic reticulum in 1) liver; 2) small intestine; and 3) brain, lung, and kidney d. Encoded by a supergene family; separate genes code for different isoenzymes e.
Drugs will generally have a high affi nity for one particular CYP450 but also may use secondary pathways. f. Nomenclature CYP 3 A 4
specifi c enzyme
subfamily (> 70% identical) family (> 40% identical)
GENE for mammalian cytochrome
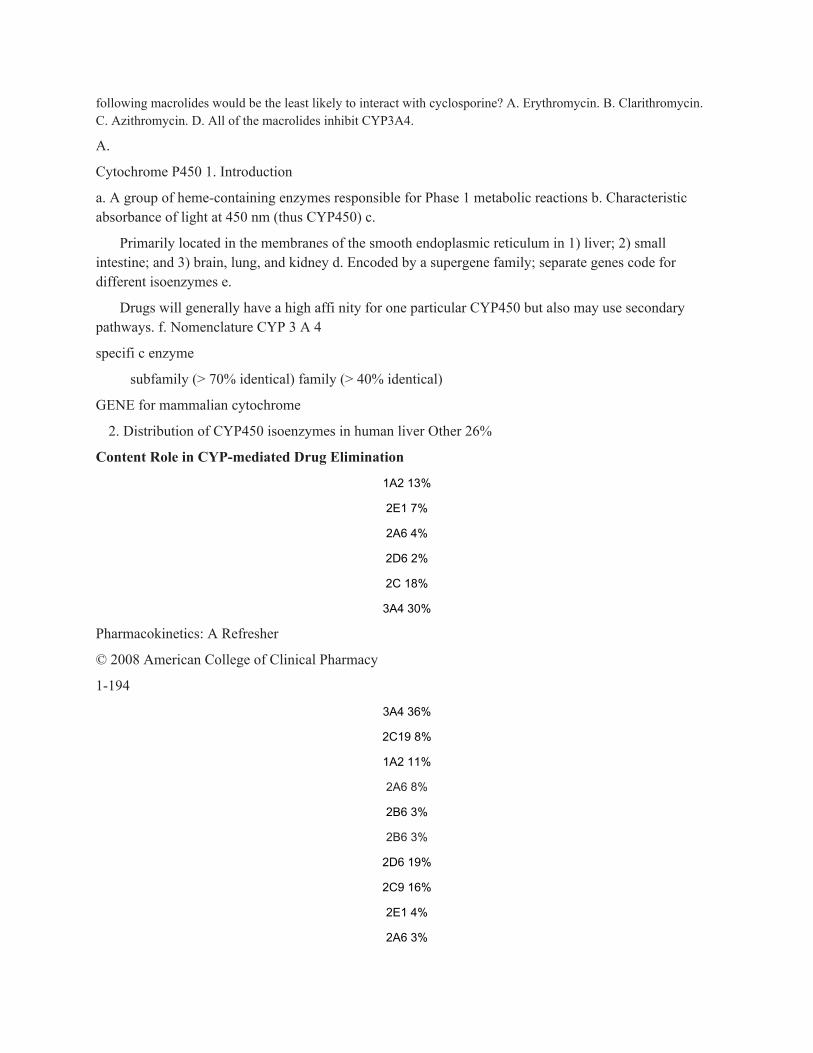
2. Distribution of CYP450 isoenzymes in human liver Other 26%
Content Role in CYP-mediated Drug Elimination
1A2 13%
2E1 7%
2A6 4%
2D6 2%
2C 18%
3A4 30%
Pharmacokinetics: A Refresher
© 2008 American College of Clinical Pharmacy
1-194
3A4 36%
2C19 8%
1A2 11%
2A6 8%
2B6 3%
2B6 3%
2D6 19%
2C9 16%
2E1 4%
2A6 3%

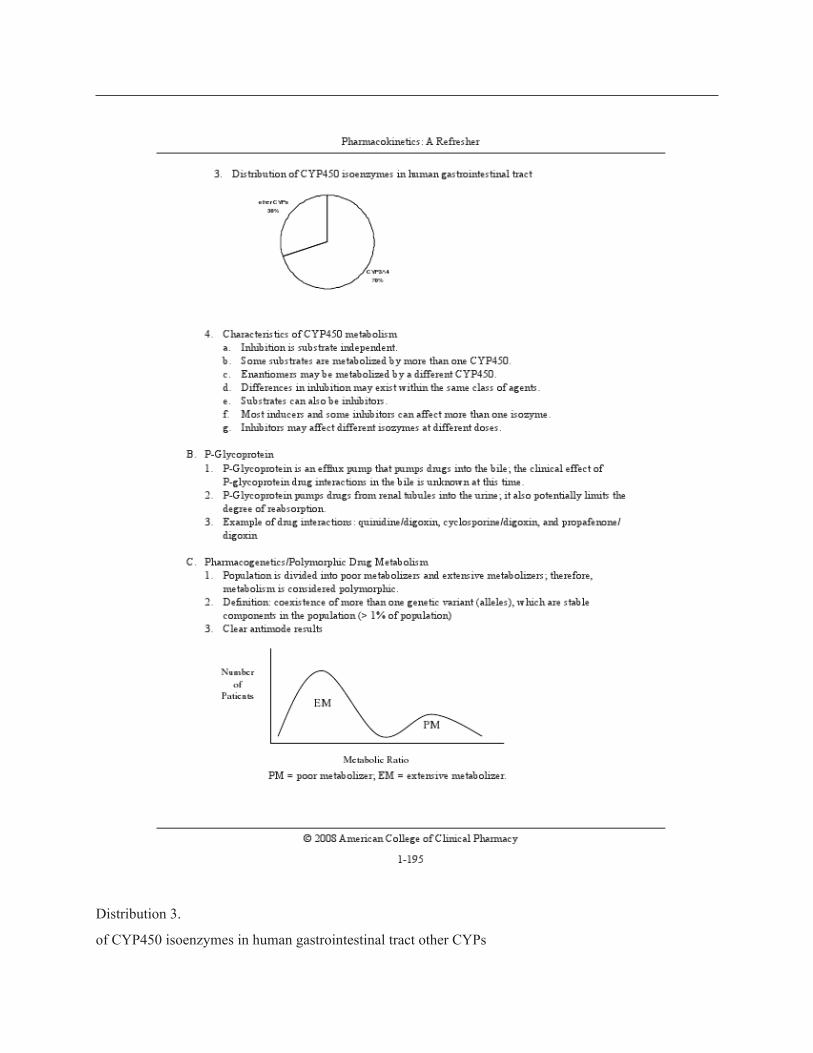
Distribution 3.
of CYP450 isoenzymes in human gastrointestinal tract other CYPs
30%
4. Characteristics of CYP450 metabolism
a. Inhibition is substrate independent. b. Some substrates are metabolized by more than one CYP450. c. Enantiomers may be metabolized by a different CYP450. d. Differences in inhibition may exist within the same class of agents. e. Substrates can also be inhibitors. f. Most inducers and some inhibitors can affect more than one isozyme. g. Inhibitors may affect different isozymes at different doses. B.
P-Glycoprotein 1.
P-Glycoprotein is an effl ux pump that pumps drugs into the bile; the clinical effect of P-glycoprotein drug interactions in the bile is unknown at this time. 2.
P-Glycoprotein pumps drugs from renal tubules into the urine; it also potentially limits the degree of reabsorption. 3.
Example of drug interactions: quinidine/digoxin, cyclosporine/digoxin, and propafenone/ digoxin
C.
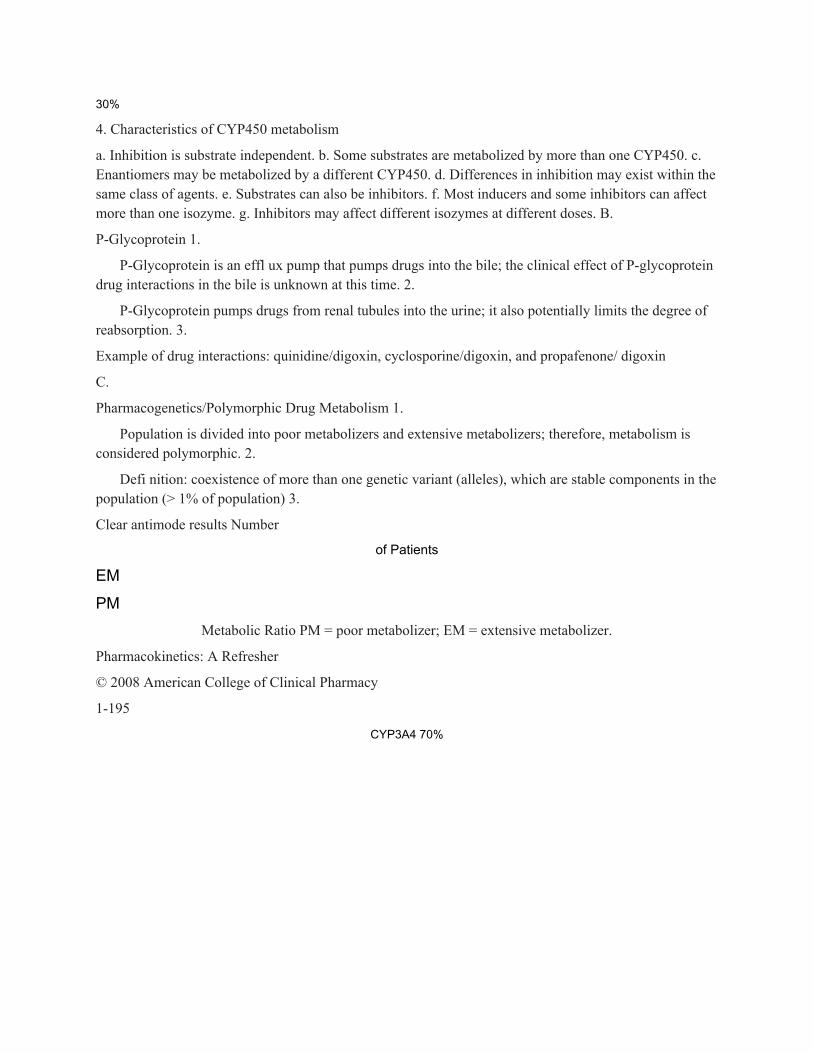
Pharmacogenetics/Polymorphic Drug Metabolism 1.
Population is divided into poor metabolizers and extensive metabolizers; therefore, metabolism is considered polymorphic. 2.
Defi nition: coexistence of more than one genetic variant (alleles), which are stable components in the population (> 1% of population) 3.
Clear antimode results Number
of Patients
EM
PMMetabolic Ratio PM = poor metabolizer; EM = extensive metabolizer.
Pharmacokinetics: A Refresher
© 2008 American College of Clinical Pharmacy
1-195
CYP3A4 70%
Pharmacokinetics: A Refresher
4.
Phenotype: expression of the trait a.
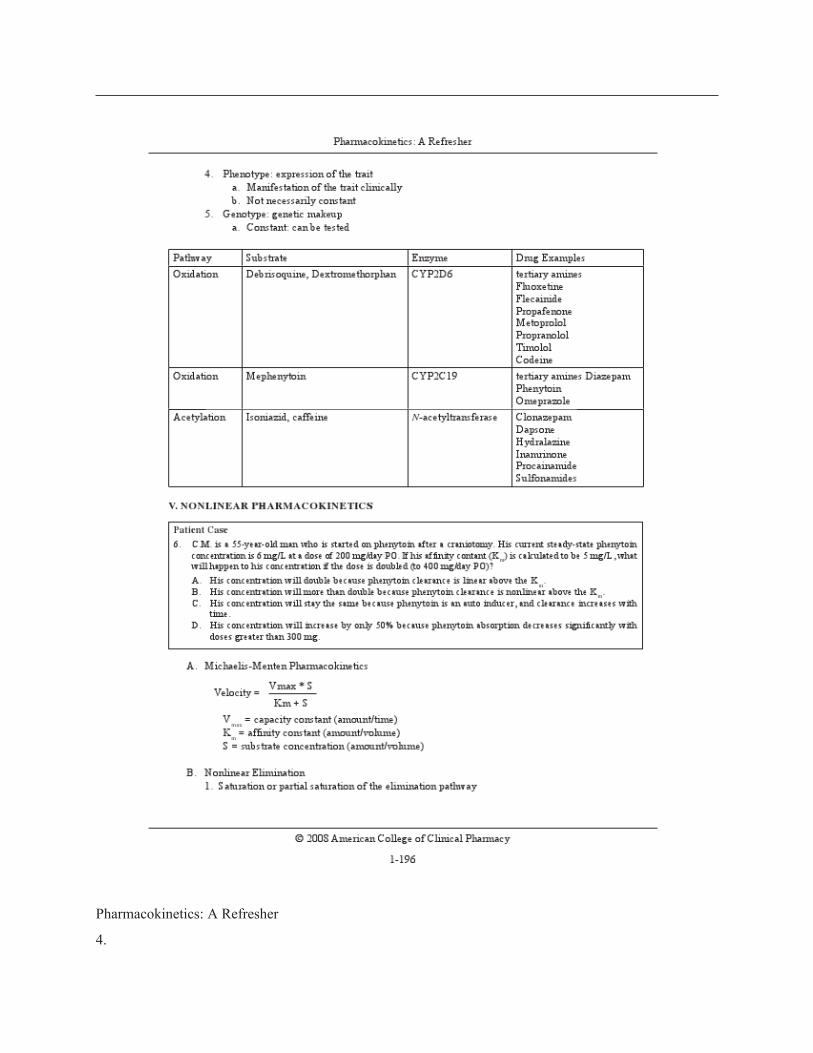
Manifestation of the trait clinically b. Not necessarily constant 5. Genotype: genetic makeup a. Constant: can be tested Pathway Substrate Enzyme Drug Examples Oxidation Debrisoquine, Dextromethorphan CYP2D6 tertiary amines
Fluoxetine Flecainide Propafenone Metoprolol Propranolol Timolol Codeine Oxidation Mephenytoin CYP2C19 tertiary amines Diazepam
Phenytoin Omeprazole Acetylation Isoniazid, caffeine N-acetyltransferase Clonazepam
Dapsone Hydralazine Inamrinone Procainamide Sulfonamides
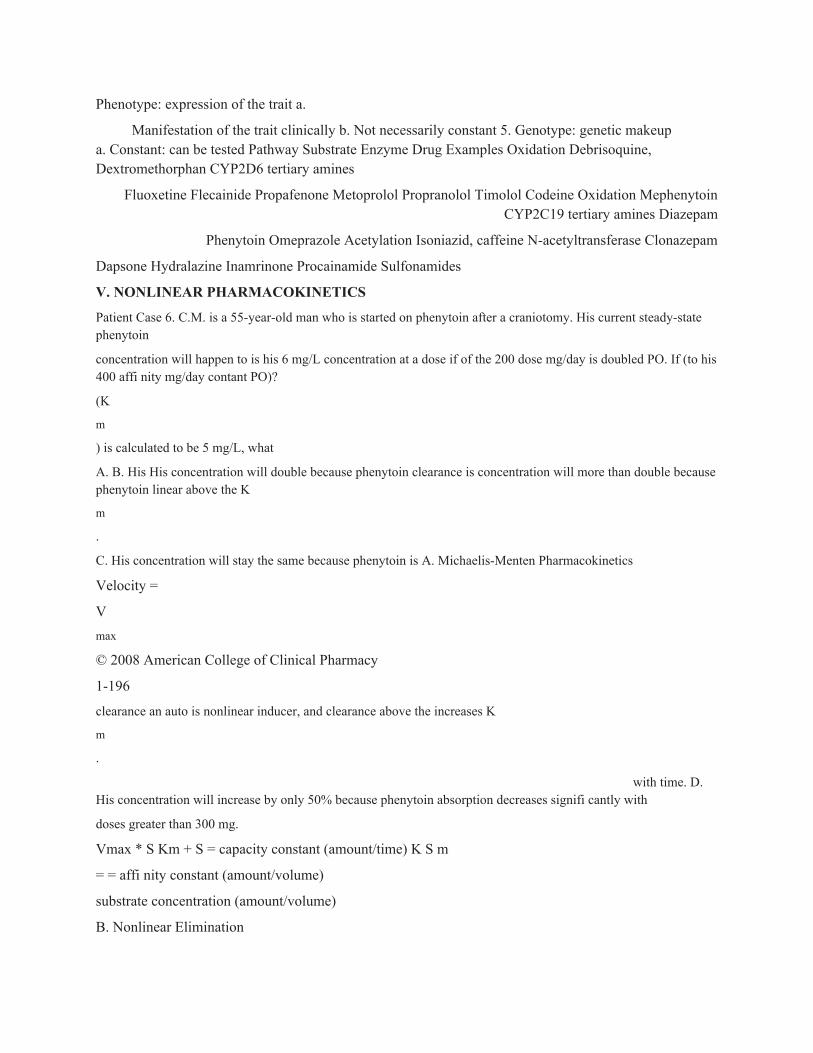
V. NONLINEAR PHARMACOKINETICS
Patient Case 6. C.M. is a 55-year-old man who is started on phenytoin after a craniotomy. His current steady-state phenytoin
concentration will happen to is his 6 mg/L concentration at a dose if of the 200 dose mg/day is doubled PO. If (to his 400 affi nity mg/day contant PO)?
(K
m
) is calculated to be 5 mg/L, what
A. B. His His concentration will double because phenytoin clearance is concentration will more than double because phenytoin linear above the K
m
.
C. His concentration will stay the same because phenytoin is A. Michaelis-Menten Pharmacokinetics
Velocity =
Vmax
© 2008 American College of Clinical Pharmacy
1-196
clearance an auto is nonlinear inducer, and clearance above the increases K
m
.
with time. D. His concentration will increase by only 50% because phenytoin absorption decreases signifi cantly with
doses greater than 300 mg.
Vmax * S Km + S = capacity constant (amount/time) K S m
= = affi nity constant (amount/volume)
substrate concentration (amount/volume)
B. Nonlinear Elimination

1.
Saturation or partial saturation of the elimination pathway





























