Embed Size (px)
Citation preview

8/6/18
1
Validation of practice based evidence for effective management of
Chronic Migraine and Occipital Neuralgia in the Post 9/11 Combat Veteran
Karen Williams,MSN, RN, FNP-BCNeurology/Headache Clinic
Central Texas Veterans Health Care System
Patient Experience
• 54 yo male with a history of refractory headaches increased after 2004 deployment• Started in 1992 with parachute jump, hard landing, hit head to
the left, with Loss of Consciousness (LOC)- 2004- Improvised explosive Device (IED) blast with LOC• Described as Left hemi-cranial throbbing/aching associated
with photophobia/phonophobia, Nausea/Vomiting & worse with exertion. Rated as 10/10• Occurring 2-4 times per month lasting 3-6 days
~ (up to 24 days per month debilitating headache, plus a daily posterior headache)
Overview of the Headache Population
• The Headache clinic was established in November 2013 • Patient population:• Refractory headache patients- most have failed Primary Care
treatments, many have also failed Neurology, all seeking alternatives• Common types of headache- Migraine, Occipital Neuralgia,
Tension, Cervical degeneration• Common co-occurring diagnosis- prior hx of head and/or neck
injury, PTSD, Insomnia, Anxiety/Depression, Musculoskeletal pain,
Conceptual Framework
• The Headache Clinic utilizes a Chronic Care Model
• Incorporate multiple modalities: • Traditional and Alternative • Medication• Botox• Occipital blocks• Acupuncture• Cefaly/Alpha-stim• Relaxation techniques• Aromatherapy (Peppermint
oil)• Patient education (continual)
Study Purpose• Headache clinic utilizes:
o Onabotulinum A (BOTOX) every 12 weeks o Occipital blocks every 4-8 weeks as neededo Treating combat veteran with a history of:• traumatic brain injury(TBI) • neck trauma/whiplash with chronic migraine (CM) • occipital neuralgia
o Based on the available evidence /anecdotally this seemed to be very effective
o Validation through empirical practice based evidence was needed

8/6/18
2
Study Disclaimer• This study:• Was been reviewed and approved by the Central Texas Veterans
Health Care System (CTVHCS) Institutional Review Board and University of Alabama at Tuscaloosa • This material is the result of work supported by resources at the
Central Texas Veterans Health Care System• Does not necessarily express the views of the Department of
Veterans Affairs or the United States Government nor does mention of trade names, commercial products, or organizations imply endorsement by the U.S. Government
Background
• CM in the post 9/11 combat veteran with a history of TBI- is 20% or more: even after 11 years of treatment (Couch & Stewart 2016; Patil et al., 2011)
• General population CM rate is 4 - 5% (Munakata et al., 2009)
• CM causes: reduced work and quality of life, increase in ER and primary visits (Munakata et al., 2009)
• Young population: average age of post 9/11 combat with CM 29-30 years of age (Altalib et al., 2016)
Knowledge Gap
• Current treatments- medications for prevention (Topiramate) and Onabotulinum Toxin A (BOTOX)(Yerry, Kuehn, & Finkel, 2015)
• Treatments failure- wear off of Botox before 12 weeks and do not fully address the occipital neuralgia• Occipital neuralgia is common after traumatic brain injury (TBI)/neck
trauma and may be part of the CM (Ducic, Sinkin, & Crutchfield, 2015; Zaremski, Herman, Clugston, Hurley, & Ahn, 2015)
• Occipital Blocks have been an effective treatment for occipital neuralgia and short term relief of CM (Cuadrado et.al, 2016; Gul, Ozon, Karadas, Koc, &; Inan, 2016)
(Onabotulinumtoxin A “Botox”) Injection Paradigm 31 injections into 7 muscle groups
Blumenfeld et. al, Headache 2010;50:1406-1418. 10
11
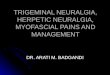
The sensory distribution of the trigeminal nerve (cranial nerve V) and its three divisions (V1, V2, V3) are show along with branches of the cervical spinal nerves that innervate cutaneous regions of the head and neck.
Image courtesy of UpToDate
Cutaneous innervation of the head and neck
12
Occipital Nerve
Anatomy

8/6/18
3
Occipital Block Injection Sites
13
GON aiming slightly up maintaining a subcutaneous courseLOC aiming lateral and up, maintaining a subcutaneous course
Occipital block consisted of 1 to 1 ratio of 1% Lidocaine &0.5% Bupivacaine, 1 mL into the greater and 0.5 mL into the lesser
Methodology
• Retrospective review of post 9/11 combat veterans – seen in the headache clinic between Jan 1, 2014- Dec 31, 2015• History of TBI or neck trauma/whiplash• Findings of CM & Occipital Neuralgia• Treated with Botox and Occipital Blocks• 282 patient charts reviewed > 137 Dx w/CM & Occipital neuralgia
> 107 excluded (did not fit all the criteria) > 30 were included
Data Collection• Number of self-reported headache days per month (28 days)
o The month prior to treatment in the headache clinico 6 months after treatment in the headache clinicoMean and 95% confidence interval for # of Headache days/month for pre and post
intervention for each subject was computedo Binomial mixed regression model- to determine if the mean # of headache days is
significantly lower post intervention• Dependent Variables: headache days per month (28 days)• Independent variables: age, gender, head or neck trauma, headache
types (migraine, tension, occipital neuralgia, medication overuse), comorbid diseases (mood disorders of anxiety, depression or PTSD, musculoskeletal pain, insomnia), prior headache treatments and treatments in the headache clinic of Botox and occipital blocks
18
65
Patient age[27, 34.1] (34.1, 41.2] (41.2, 48.3]
Num
ber o
f Vet
eran
s in
each
age
rang
e
0
2
4
6
8
10
12
14
16
18
20
60%
20%17%
3%
Veteran ages ranged from 27 to 55.4 years of age. 80% were between the ages of 27 and 41.2 years
1 1
4
3
1
3 3
2
7
2 2
1
0
1
2
3
4
5
6
7
8
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2014
Num
ber o
f Vet
eran
s
Year of Headache Onset
Headaches started after the head or neck trauma
23
19
14
9
56
PRIOR PREVENTATIVE MEDICATION TREATMENTS Topiramate Divalproex TCA Inderal Verapamil Gabapentin
Number in the graphic represents the number of veterans who had taken the medication for migraine prevention prior to treatment in the headache clinic. 13 veterans had trials of 3 or more medications.

8/6/18
4
20
10
Gender Distribution of Patients Treated
# of Males # of Females Some patients were diagnosed with PTSD & Anxiety or Depression PTSD = Post-traumatic Stress DisorderMSK = Musculoskeletal Disorder
25
65
21 21
0
5
10
15
20
25
30
PTSD Anxiety Depression MSK Insomnia
Vete
ran
Medical Diagnosis
Comorbid Conditions
Results
• Mean number of headache days in the month prior to treatment was 24.1 (22.0, 25.7)*• Mean number of headache days in the month post-treatment was 12.9
(9.7, 16.4)*• Mean difference in number of headache days (pre-treatment minus
post-treatment) was 11.2 (8.2, 14.2)*• Findings were clinically and statistically significant
*Numbers in parenthesis are the 95% Confidence Interval
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
Num
ber o
f Hea
dach
e da
ys
Veterans
Pre-Post Headache Frequency
Headaches Pre Headaches Post
*6 patients did not have a reduction in number of headache days, but did have a reduction in severity of headaches
Limitations/Needs
• Results are promising in treating CM and Occipital neuralgia with Botox and Occipital Blocks• Limitations: • Inability to have treatment and control group• small sample size (N=30) • self report for only one month pre and post treatment
• Needs:• Long term study• Larger cohort controlled for confounders• Additional studies for CM/Occipital neuralgia treatment in the veteran
population
Final Thoughts
• Post 9/11 combat veterans, with a history of TBI or neck trauma/whiplash with findings of CM and occipital neuralgia, who have not had satisfactory relief of their CM with conventional medical treatment, may have a reduction in the number of days of headache after treatment with occipital blocks and Botox• In other words: it may reduce the headache
burden and improve quality of life

8/6/18
5
Karen [email protected]
Central Texas Veterans Health Care System1901 Veterans Memorial Drive
Temple, TX 76504
References• Altalib, H. H., Fenton, B. T., Sico, J., Goulet, J. L., Bathulapalli, H., Mohammad, A., . . .
Haskell, S. (2016). Increase in migraine diagnoses and guideline-concordant treatment in veterans, 2004-2012. Cephalalgia: An International Journal of Headache. Advance on Line Publication. doi:0333102416631959
• Blumenfeld, A, Silberstein SD, Dodick DW, Aurora SK, Turkel CC, Binder WJ. Method of injection of OnabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache: The Journal of Head and Face Pain. 2010;50(9):1406-1418. https://doi.org/10.1111/j.1526- 4610.2010.01766.x. doi: 10.1111/j.1526-4610.2010.01766.x
• Couch, J. R., & Stewart, K. E. (2016). Headache prevalence at 4–11 years after deployment-related traumatic brain injury in veterans of Iraq and Afghanistan wars and comparison to controls: A matched case-controlled study. Headache: The Journal of Head and Face Pain, 56(6), 1004-1021. doi:10.1111/head.12837
References• Cuadrado, M. L., Aledo-Serrano, A., Navarro, P., Lopez-Ruiz, P., Fernandez-de-Las-Penas, C.,
Gonzalez-Suarez, I., . . . Fernandez-Perez, C. (2016). Short-term effects of greater occipital nerve blocks in chronic migraine: A double-blind, randomised, placebo-controlled clinical trial. Cephalalgia : An International Journal of Headache, doi:0333102416655159
• Ducic, I., Sinkin, J. C., & Crutchfield, K. E. (2015). Interdisciplinary treatment of post-concussion and post-traumatic headaches. Microsurgery, 35(8), 603-607. doi:10.1002/micr.22503
• DoD Worldwide Number for TBI. (2016, Aug). Retrieved from http://dvbic.dcoe. mil/files/tbi-numbers/DoD-TBI-Worldwide-Totals_2000-2016_Feb-17-2017_v1.0_2017-04-06.pdf
• Finkel, A. G., Yerry, J. A., Klaric, J. S., Ivins, B. J., Scher, A., & Choi, Y. S. (2016). Headache in military service members with a history of mild traumatic brain injury: A cohort study of diagnosis and classification. Cephalalgia: An International Journal of Headache. Advance online publication. doi:0333102416651285
• Gul, H. L., Ozon, A. O., Karadas, O., Koc, G., & Inan, L. E. (2016). The efficacy of greater occipital nerve blockade in chronic migraine: A placebo-controlled study. Acta NeurologicaScandinavica, n/a. doi:10.1111/ane.12716
References• Headache Classification Committee of the International Headache Society, (IHS). (2013). The
international classification of headache disorders, 3rd edition (beta version). Cephalalgia : An International Journal of Headache, 33(9), 629-808. doi:10.1177/0333102413485658
• Management of Concussion-mild Traumatic Brain Injury (mTBI). Retrieved from http://www. Healthquality.va.gov/guidelines/Rehab/mtbi
• Munakata, J., Hazard, E., Serrano, D., Klingman, D., Rupnow, M. F. T., Tierce, J., . . . Lipton, R. B. (2009). Economic Burden of Transformed Migraine: Results from the American Migraine Prevalence and Prevention (AMPP) study. Headache: The Journal of Head and Face Pain, 49, 498-508. doi:10.1111/j.1526-4610.2009.01369.x
• National Center for Veterans Analysis and Statistics. (2016, May). Profile of Post - 9/11 Veterans: 2014. Retrieved from http://www.va.gov/vetdata/Veteran_Population.asp
References
• Patil, V. K., St. Andre, J. R., Crisan, E., Smith, B. M., Evans, C. T., Steiner, M. L., & Pape, T. L. (2011). Prevalence and treatment of headaches in veterans with mild traumatic brain injury.Headache: The Journal of Head & Face Pain, 51, 1112-1121. doi:10.1111/j.1526-4610.2011.01946.x
• Theeler, B. J., & Erickson, J. C. (2009). Mild head trauma and chronic headaches in returning US soldiers. Headache: The Journal of Head and Face Pain, 49, 529-534. doi:10.1111/j.1526-4610.2009.01345.x
• Theeler, B. J., Flynn, F. G., & Erickson, J. C. (2012). Chronic daily headache in U.S. soldiers after concussion. Headache: The Journal of Head and Face Pain, 52, 732-738. doi:10.1111/j.1526-4610.2012.02112.x
• Vos, T., Flaxman, A. D., Naghavi, M., Lozano, R., Michaud, C., Ezzati, M., . . . Atkinson, C. (2013). Years Lived with Disability (YLDs) for 1160 Sequelae of 289 Diseases and Injuries 1990-2010: A Systematic Analysis for the Global Burden of Disease Study 2010. Lancet, 380 North American Edition (9859), 2163-2196. doi:10.1016/S0140-6736(12)61729-2

8/6/18
6
References• Yerry, J. A., Kuehn, D., & Finkel, A. G. (2015). Onabotulinum toxin A for the treatment of
headache in service members with a history of mild traumatic brain injury: A cohort study.Headache: The Journal of Head & Face Pain, 55, 395-406. doi:10.1111/head.12495
• Zaremski, J. L., Herman, D. C., Clugston, J. R., Hurley, R. W., & Ahn, A. H. (2015). Occipital neuralgia as a sequela of sports concussion: A case series and review of the literature.Current Sports Medicine Reports (American College of Sports Medicine), 14(1), 16-19. doi:10.1249/JSR