Embed Size (px)
Citation preview
1/16/2014
1
Prehospital Response to the Marathon Bombings: Boston, MA
Adam Darnobid, MDFellow in EMSDepartment of Emergency MedicineUniversity of Massachusetts Medical School
2014 NAEMSP ANNUAL MEETING, TUSCON, AZ
Ricky Kue, MD, MPH, FACEPAssociate Medical DirectorBoston EMS, Police and Fire DepartmentsAssistant Professor of Emergency MedicineBoston University School of Medicine
David Hirsch, MD, MPH, FACEPEMS Medical DirectorCapital Area of New HampshireConcord Emergency Medical AssociatesConcord Hospital
The 117th Running of the Boston Marathon
Boston EMS: Who we are…
Municipal 3rd service EMS and bureau of the Boston Public Health Commission
Two‐tiered system: Basic Life Support (BLS) and Advanced Life Support (ALS)
111,074 incidents in CY2012
Over 138,000 responses
Average >300 calls/day
>81,000 transports
378 department members 358 uniformed staff
251 EMTs 58 Paramedics
1/16/2014
2
117th Boston Marathon
Multi‐Day Event
ICS Implemented
Zone Concept
9 BLS / 4 ALS
11 Bicycles
Medical Stations / Proceed Out Teams
Dispatch Operations
Coordination Centers: UCC, MEMA, MIC
Finish Area Footprint
Marathon Medical OperationsOperations managed by BAA and ARC medical tents
Surges require triage and management outside of tents
Data regularly sent to field command staff, hospitals, and race physicians during event
PURPOSE – Reduce surge to area hospitals (and EMS) by managing runner related illnesses and conditions at the medical tents
Medical “Stay and play” mentality
Runners Max. TempIncident Totals
Transport Totals
Hospital Totals
Incidence RateTransports
(% of Incidents)
2010 22,540 61 1,320 42 68 5.86% 3.18%
2011 21,554 61 1,324 55 87 6.14% 4.15%
2012 22,426 87 2,181 241 260 9.73% 11.05%
1/16/2014
3
VOLUNTEERS47Medical doctors110 Registered nurses 60Massage therapists65 Physical therapists50Medical records personnel60 Athletic trainers25 Non‐medical assistants5 Chiropractors
TOOLS OF THE TRADE7,200 Band‐Aids3,000 Ice bags400 IV bags of saline314 Rolls of medical tape200 Cots46 Rectal thermometers15Massage tables
(Source: Runner’s World)
ICU Section◦ “Heat” Teams
◦ CWI therapy based on Marine Corps Marathon
Medical Section◦ iStat® POC testing –hyponatremia
◦ 12‐Lead ECG with Cardiology
Podiatry / Physical Therapy
EMS◦ Critical care treatment area
◦ Airway, nebs, ACLS, meds, etc.
◦ Transport staging area
9:22AM Wheel Chair Participants Start Race
9:32 AM
Elite Women Start Race
10:00 AM
General Start (3 waves)
11:59 AM Female Winner Crosses Finish Line
12:10 AM
Male Winner Crosses Finish Line
2:30‐3PMLargest wave of amateur runners cross finish line
1/16/2014
4
Another typical Marathon Monday…Perfect marathon weather: 50s and dry.
Marathon Maladies: Hypohydration
Muscle Cramps, Blisters
Heat Exhaustion/Stroke
Hypothermia
Hyponatremia
Patient Tracking 523 Patients Seen
193 Active, 330 Discharged
8 Transports (some non‐marathon related)
David Hirsch, MD, MPH, FACEP
Marathon VideoInsert video clip here
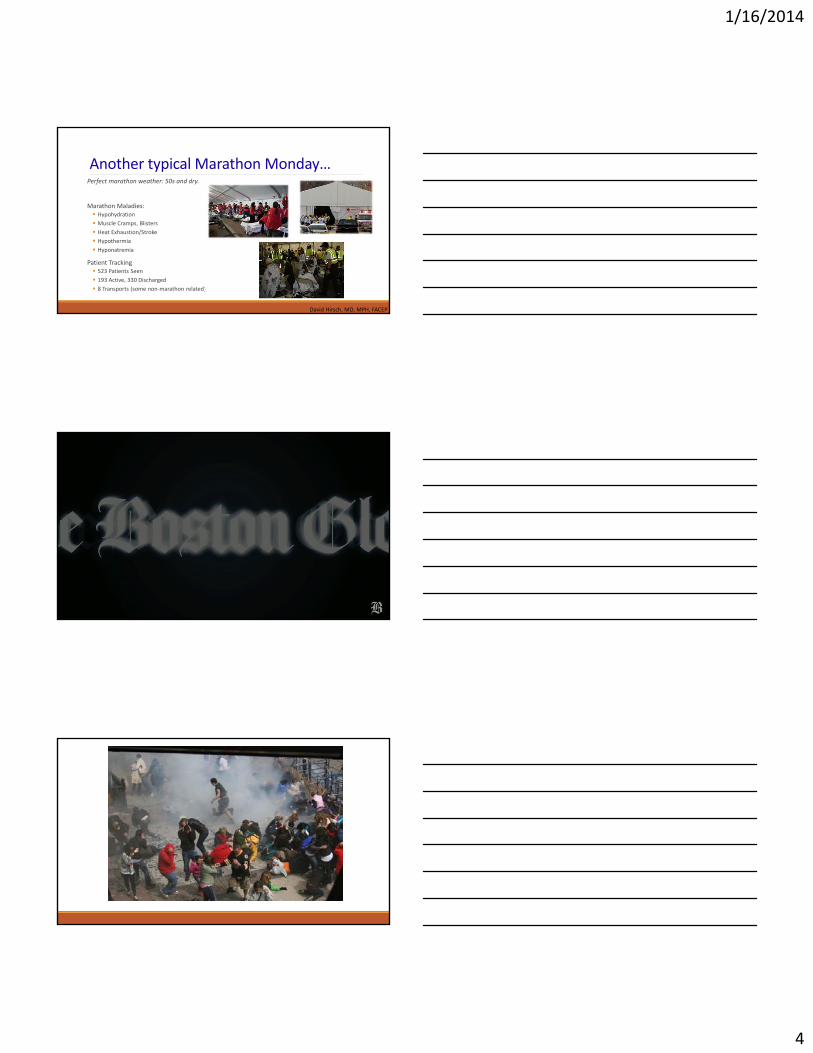
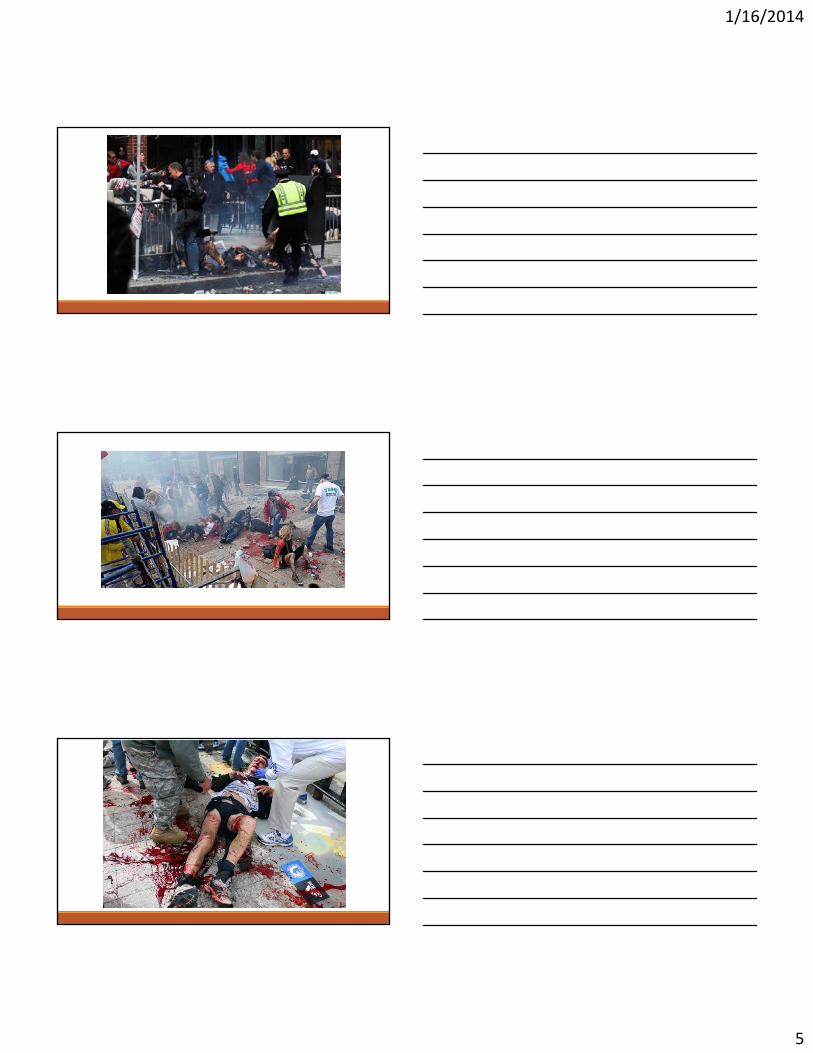
The Initial Scene
1/16/2014
5
1/16/2014
6
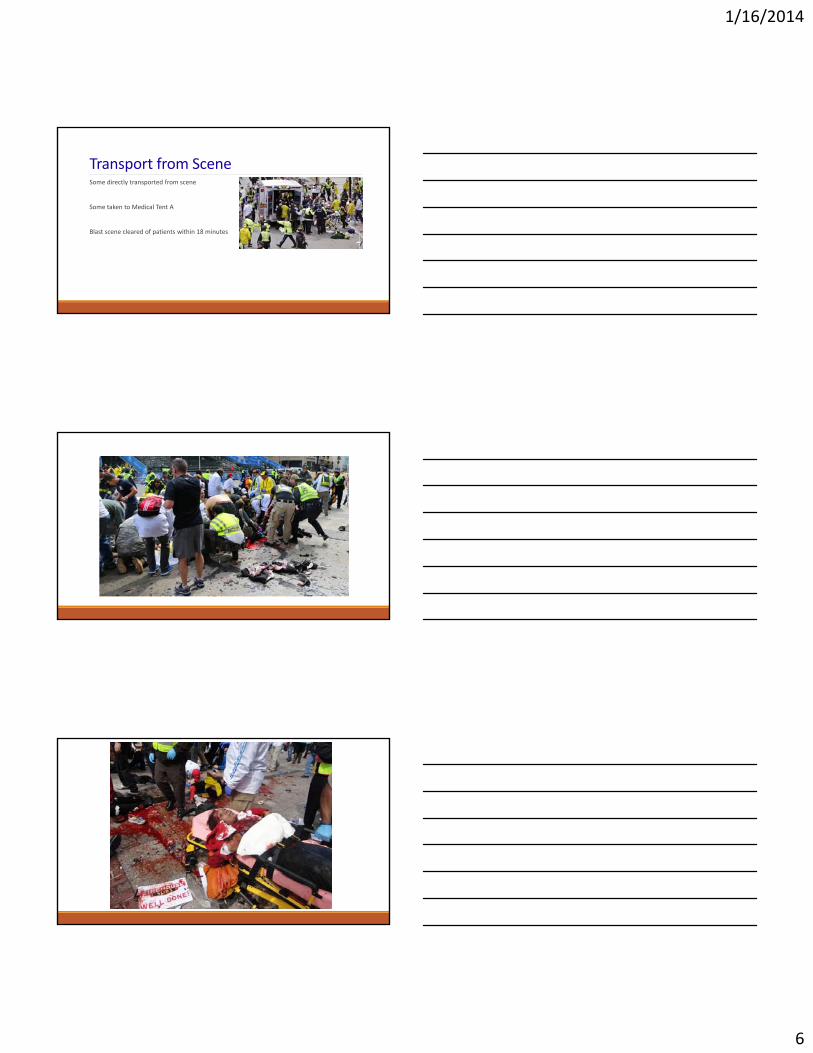
Transport from SceneSome directly transported from scene
Some taken to Medical Tent A
Blast scene cleared of patients within 18 minutes
1/16/2014
7
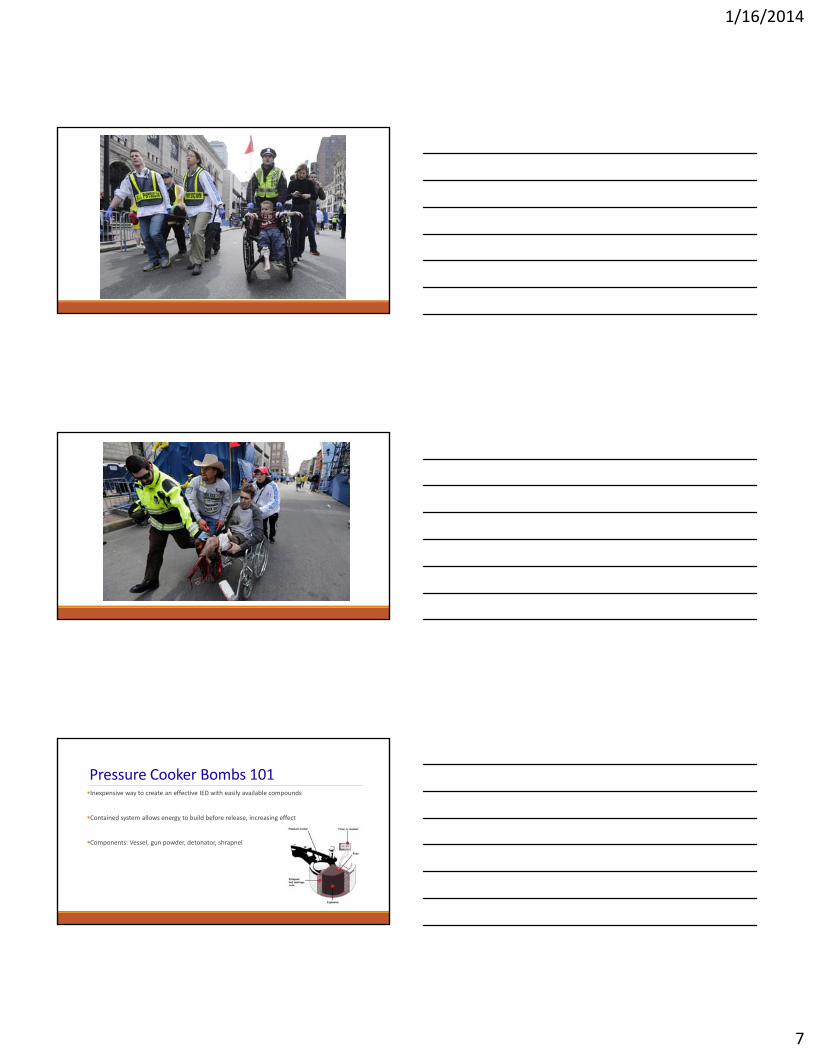
Pressure Cooker Bombs 101Inexpensive way to create an effective IED with easily available compounds
Contained system allows energy to build before release, increasing effect
Components: Vessel, gun powder, detonator, shrapnel
1/16/2014
8
ExplosivesLow Order
subsonic explosion
lack over‐pressurization wave
e.g.: gun powder, petroleum based
High Order
supersonic explosion
Creates a blast/over‐pressure wave
e.g.: ammonium nitrate fuel oil (ANFO), TNT, dynamite, plastic
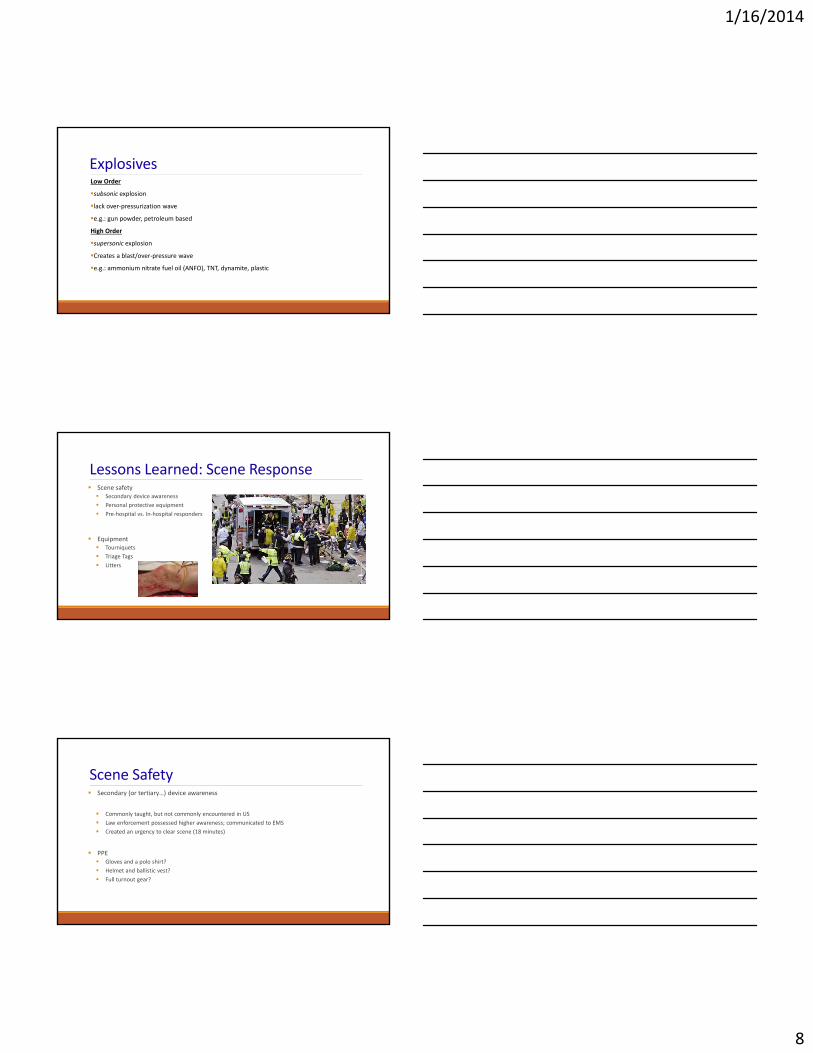
Lessons Learned: Scene Response Scene safety Secondary device awareness
Personal protective equipment
Pre‐hospital vs. In‐hospital responders
Equipment Tourniquets
Triage Tags
Litters
Scene Safety Secondary (or tertiary…) device awareness
Commonly taught, but not commonly encountered in US
Law enforcement possessed higher awareness; communicated to EMS
Created an urgency to clear scene (18 minutes)
PPE Gloves and a polo shirt?
Helmet and ballistic vest?
Full turnout gear?
1/16/2014
9
Responders at the ScenePre‐hospital vs. In‐hospital Responders◦ Different levels of training and awareness
◦ Different equipment
◦ Different mindset and priorities
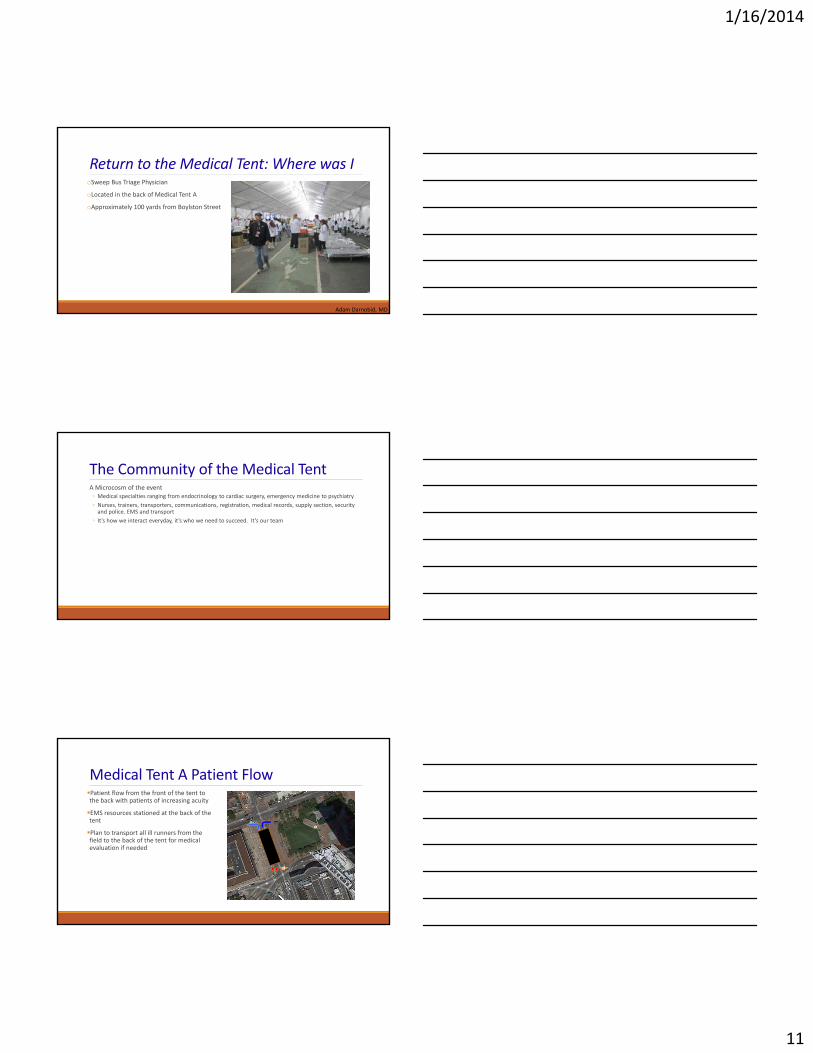
Equipment: X‐A‐B‐C’sCombat Application Tourniquet (C‐A‐T) SOFT‐Tw Tourniquet

1/16/2014
10
Equipment: Triage Tag Systems
Equipment: Rapid Extrication/Transport
1/16/2014
11
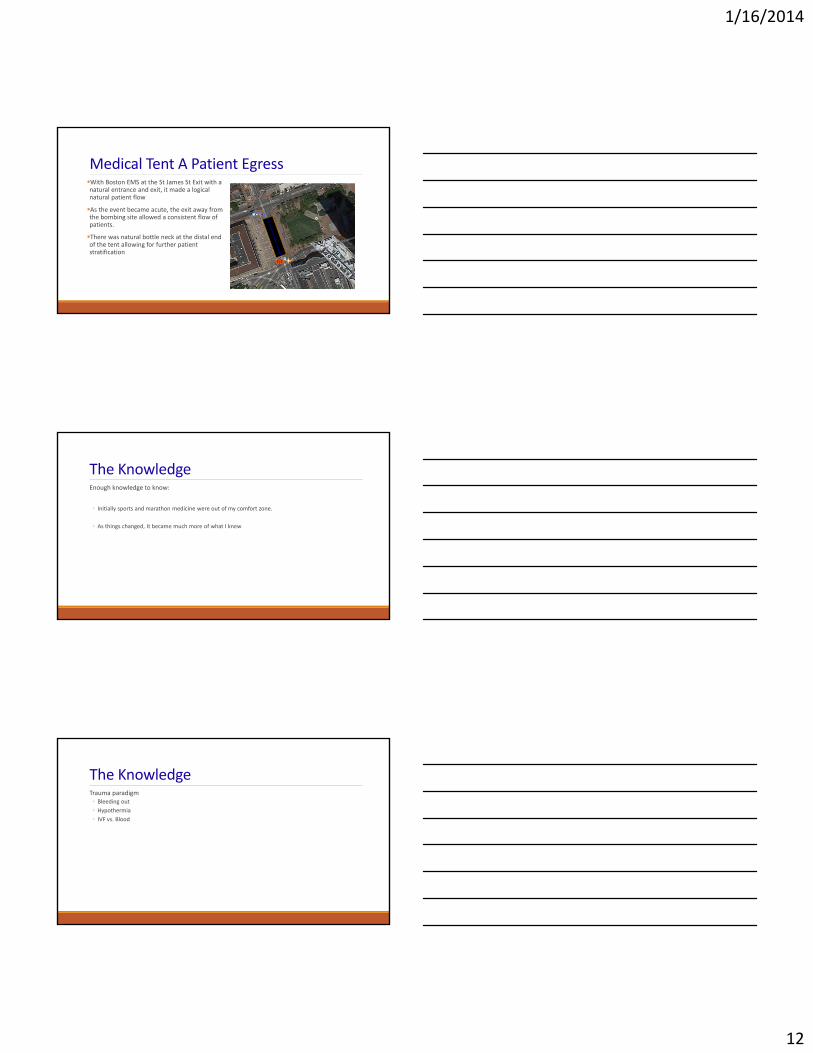
Return to the Medical Tent: Where was IoSweep Bus Triage Physician
oLocated in the back of Medical Tent A
oApproximately 100 yards from Boylston Street
Adam Darnobid, MD
The Community of the Medical TentA Microcosm of the event◦ Medical specialties ranging from endocrinology to cardiac surgery, emergency medicine to psychiatry
◦ Nurses, trainers, transporters, communications, registration, medical records, supply section, security and police. EMS and transport
◦ It’s how we interact everyday, it’s who we need to succeed. It’s our team
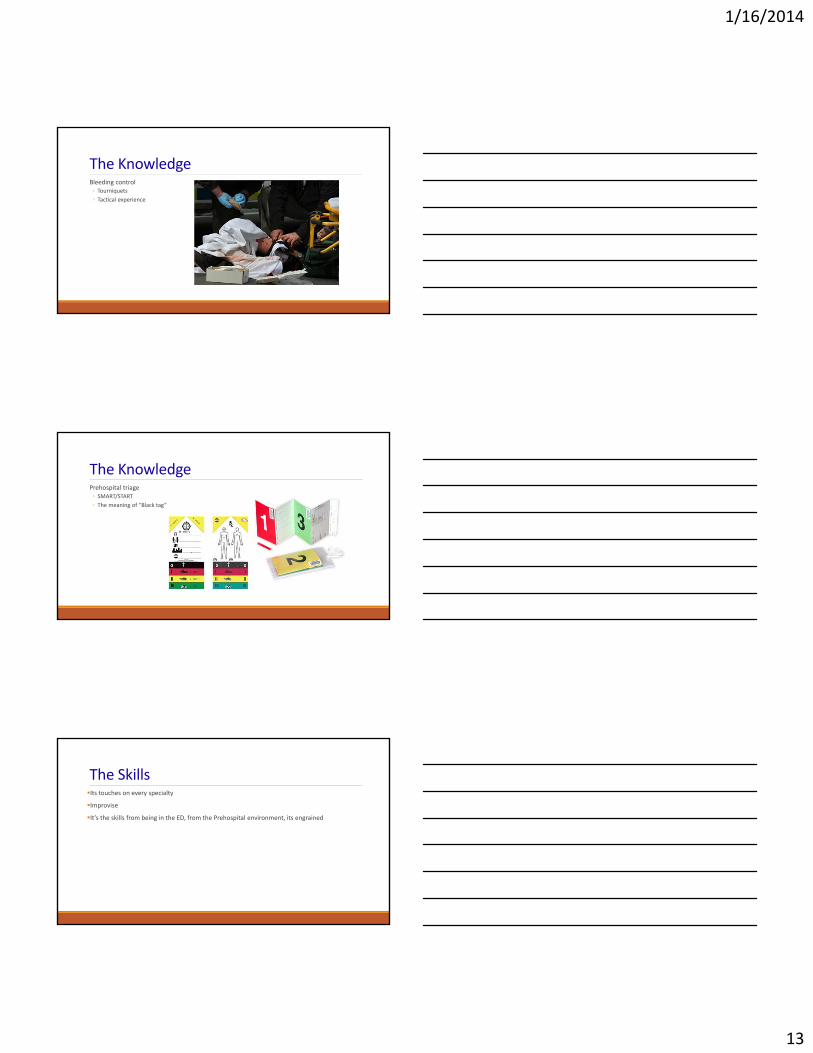
Medical Tent A Patient FlowPatient flow from the front of the tent to the back with patients of increasing acuity
EMS resources stationed at the back of the tent
Plan to transport all ill runners from the field to the back of the tent for medical evaluation if needed
1/16/2014
12
Medical Tent A Patient EgressWith Boston EMS at the St James St Exit with a natural entrance and exit, it made a logical natural patient flow
As the event became acute, the exit away from the bombing site allowed a consistent flow of patients.
There was natural bottle neck at the distal end of the tent allowing for further patient stratification
The KnowledgeEnough knowledge to know:
◦ Initially sports and marathon medicine were out of my comfort zone.
◦ As things changed, It became much more of what I knew
The KnowledgeTrauma paradigm◦ Bleeding out
◦ Hypothermia
◦ IVF vs. Blood
1/16/2014
13
The KnowledgeBleeding control◦ Tourniquets
◦ Tactical experience
The KnowledgePrehospital triage◦ SMART/START
◦ The meaning of “Black tag”
The SkillsIts touches on every specialty
Improvise
It’s the skills from being in the ED, from the Prehospital environment, its engrained
1/16/2014
14
The Skills
“You have the skills and the knowledge, now you just need to do it”
Intersection of EMS and the PhysicianA unique setting where not every (or any) doctor could have performed
Communication and the exchange of information needs to happen in a unique fashion
This isn’t the emergency department or hospital setting. Its prehospital medicine in its own environment with its own challenges
The EMS Response:“Chance favors the prepared mind…” ‐Louis Pasteur
Ricky Kue, MD, MPH, FACEP
1/16/2014
15
MBHSR MCI PHASE DESIGNATIONS
Phase 1 ‐ 1 to 10 potential victims
Phase 2 ‐ 11 to 30 potential victims
Phase 3 ‐ 31 to 50 potential victims
Phase 4 ‐ 50 to 200 potential victims
Phase 5 ‐ Greater than 200 potential victims
Phase 6 ‐ Incident or Event Requiring Sustained EMS Operations (longer than twenty‐four hours)
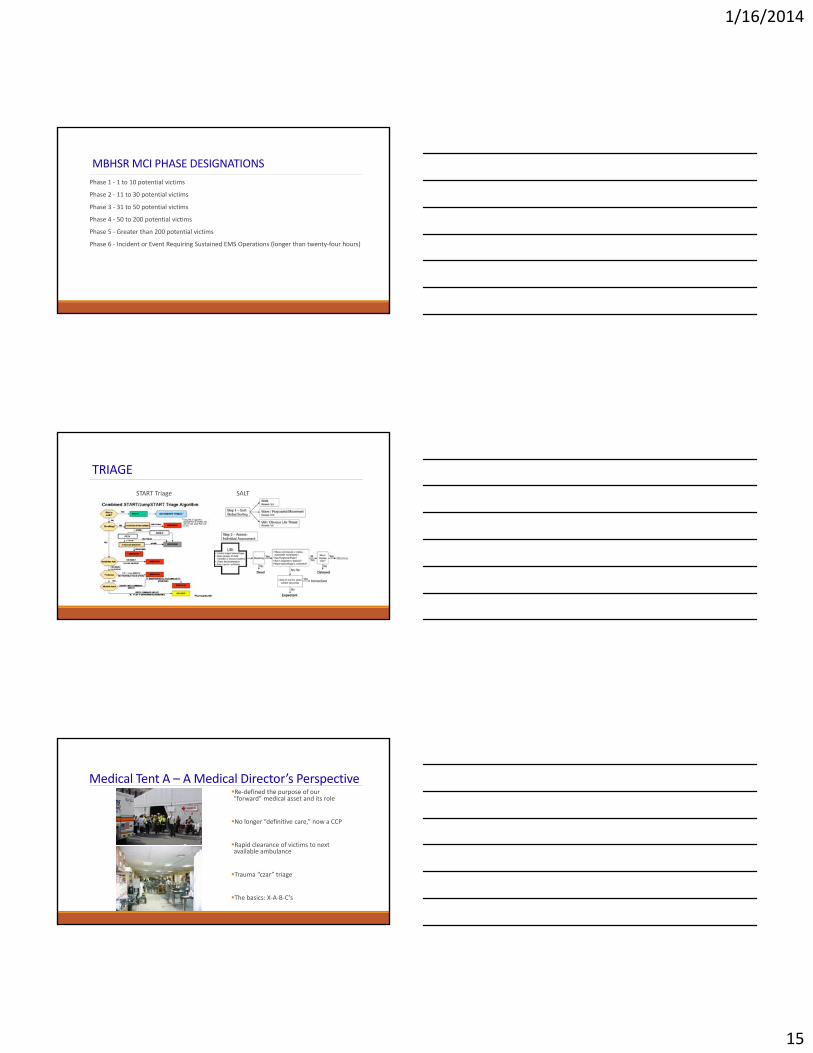
TRIAGE
START Triage SALT
Medical Tent A – A Medical Director’s Perspective Re‐defined the purpose of our “forward” medical asset and its role
No longer “definitive care,” now a CCP
Rapid clearance of victims to next available ambulance
Trauma “czar” triage
The basics: X‐A‐B‐C’s
1/16/2014
16
Training
• Urban Shield (2011, 2012)• MBTA Green Line Crash
(Nov. 2012)
• Flu Public Health Emergency (Jan. 2013)
• Tour Bus Crash (Feb. 2013)• “Nemo” Blizzard (Feb. 2013)
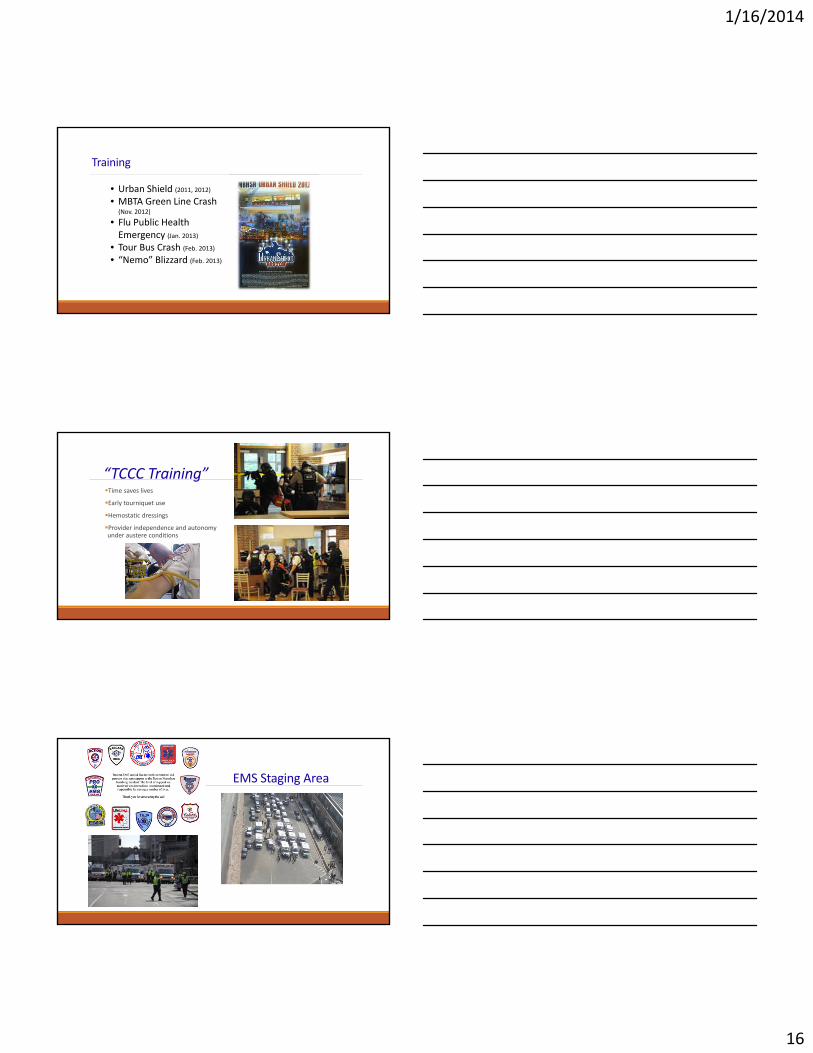
“TCCC Training”Time saves lives
Early tourniquet use
Hemostatic dressings
Provider independence and autonomy under austere conditions
EMS Staging Area
1/16/2014
17
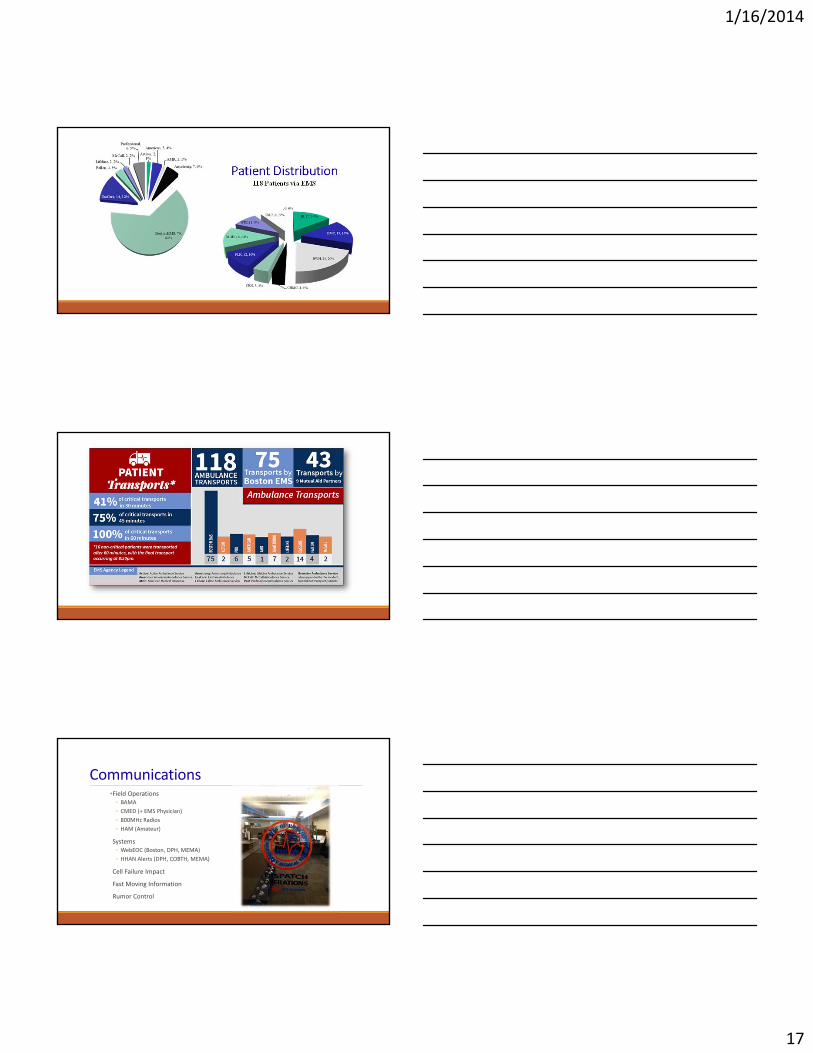
Patient Distribution118 Patients via EMS
Communications•Field Operations◦ BAMA
◦ CMED (+ EMS Physician)
◦ 800MHz Radios
◦ HAM (Amateur)
Systems◦ WebEOC (Boston, DPH, MEMA)
◦ HHAN Alerts (DPH, COBTH, MEMA)
Cell Failure Impact
Fast Moving Information
Rumor Control
1/16/2014
18
Hospital Distribution and Inter‐facility Communication
•Boston EMS Dispatch Operations
•Boston Area Ambulance Mutual Aid Network (BAMA)
•Central Medical Emergency Direction (CMED)
•Disaster Radio Network
•Consortium of Boston Teaching Hospitals (COBTH)*
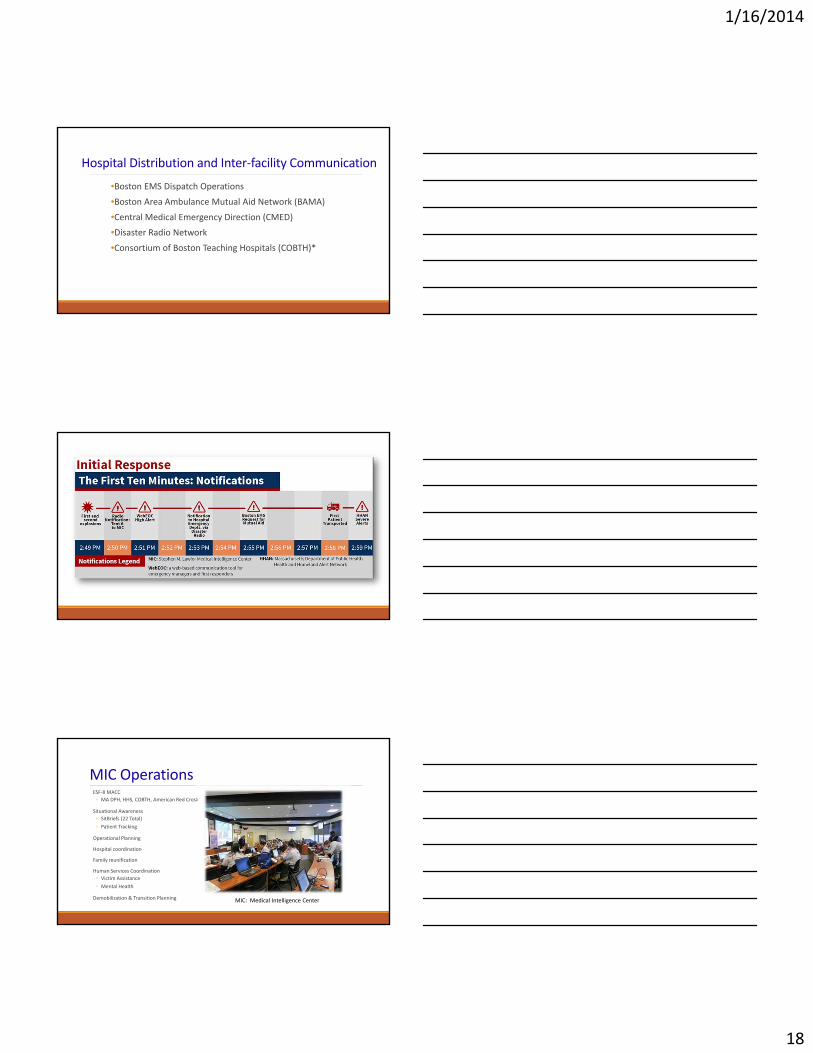
MIC OperationsESF‐8 MACC
◦ MA DPH, HHS, COBTH, American Red Cross
Situational Awareness
◦ SitBriefs (22 Total)
◦ Patient Tracking
Operational Planning
Hospital coordination
Family reunification
Human Services Coordination
◦ Victim Assistance
◦ Mental Health
Demobilization & Transition Planning MIC: Medical Intelligence Center
1/16/2014
19
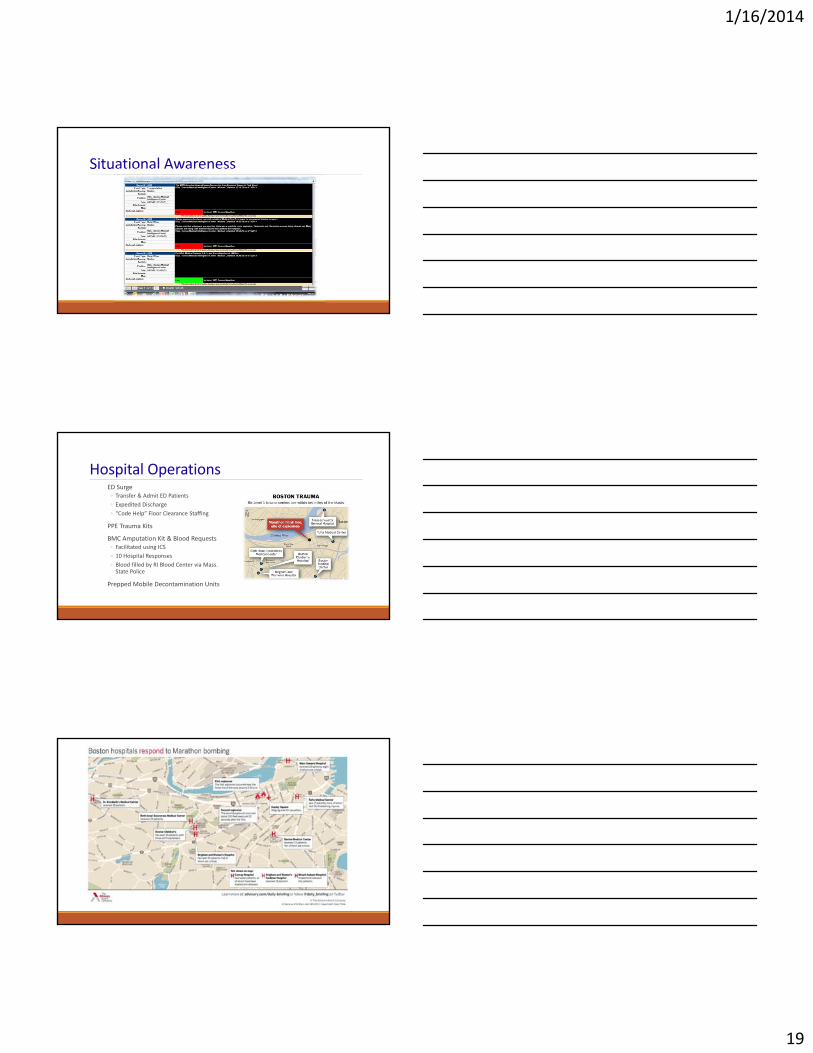
Situational Awareness
Hospital OperationsED Surge ◦ Transfer & Admit ED Patients
◦ Expedited Discharge
◦ “Code Help” Floor Clearance Staffing
PPE Trauma Kits
BMC Amputation Kit & Blood Requests◦ Facilitated using ICS
◦ 10 Hospital Responses
◦ Blood filled by RI Blood Center via Mass. State Police
Prepped Mobile Decontamination Units
1/16/2014
20
And then, the longest day…
Sean Collier26 Y/O
Richard Donohue Jr.33 Y/O
Thank you…





























