Embed Size (px)
Citation preview

University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 39
University J Dent Scie 2015; No. 1, Vol. 3
ABSTRACT: Aim and Objectives: To determine the results of using the free vascularized fibular flap for comprehensive reconstruction of mandibular continuity defects. Materials and Methods: The study group consisted of patients who reported to the Department of Oral and Maxillofacial Surgery, Army Dental Centre (R&R) from the year May 2010 to Mar 2014. underwent reconstruction of continuity defects of the mandible using a fibular vascularized free flap Indication for mandibular resection were squamous cell carcinoma of the floor of the mouth and alveolar ridge in 4 cases, ameloblastoma of the mandible in 8 cases, odontogenic keratocyst in 2 cases and 1 case of osteosarcoma of the mandible and 3 cases of patients with post traumatic mandibular defects sustained due to Gunshot wound (GSW) . The type of reconstruction performed was primary reconstruction in 12 patients and secondary in 6 patients. Results: There were 18 patients including 13 males and 5 females with mean age of 40 years. Of those, 2 completely failed, due to venous thrombosis. Donor site morbidity was low; there was some compromise in the ankle function but none of the patient complaint of foot drop. Simple problems with wound healing such as dehiscence and delayed wound healing developed in 3 patients, which usually required only local antiseptic treatment. After the operation patient began oral feeding and walking with some aid in fourth week and became completely ambulant in 8 weeks. Conclusion: In this small series the free fibula flap was a versatile and reliable option for microvascular reconstruction of large mandibular defects. It provided a large quantity of bone, which could be easily shaped and passively adapt to the remaining mandible and for an implant-based prosthetic restoration.
1S.K. Roy, Professor & Head, Dept of Oral and Maxillofacial Surgery Army Dental Centre (R&R), 2Delhi Cantt-110010, Ajay P Desai, Assistant Professor, Dept of Oral and Maxillofacial Surgery
3Army Dental Centre (R&R), Delhi Cantt-110010, P.K. Chattopadhyay, Associate Professor, Dept of Oral and Maxillofacial Surgery Army Dental Centre (R&R), Delhi Cantt-110010 4V. Langer, Associate Professor, Dept of Plastic & Reconstructive Surgery, AH (R&R),
5Delhi Cantt-110010, I.D. Roy, Associate Professor, Dept of Oral and Maxillofacial Surgery Army 6Dental Centre (R&R), Delhi Cantt-110010, Col. Ravinder S. Semi, Assistant Professor, Dept of Oral and
Maxillofacial Surgery Army Dental Centre (R&R), Delhi Cantt-1100107Col. Serat Rehman, Assistant Professor, Dept of Oral and Maxillofacial SurgeryArmy Dental Centre (R&R), Delhi Cantt-110010
INTRODUCTION : Mandibular reconstruction continues to
be one of the most common surgical challenges faced by oral
and maxillofacial surgeons. The advent of microvascular
surgery has made it possible to reconstruct complex
maxillofacial region in a single stage. This technique allows
for larger resections and reconstruction, which allows patients
to return to normal function in a much shorter period when
compared with multistage local, regional pedicled flaps and
nonvascularized free bone flaps [1]. Multiple studies have
shown the clear superiority of microvascular reconstruction
of the mandible when compared with ''traditional'' methods.
Tissue loss resulting from cancer ablation, debridement of
infected tissues or secondary to trauma provides the surgeon
with various reconstructive challenges. Although
reconstruction of soft tissue defects of head and neck requires
a fasciocutaneous or musculocutaneous flap, composite
tissue loss that includes bone should be managed with a flap
that contains vascularized bone. The goal of reconstructive
surgery in tissue loss is to repair the defect, early return to
function with least complications [2]. Until the advent of free
tissue transfer, reconstruction of the defects of mandible and
midface was sub optimal. Plating across the defects with or
without nonvascularized bone flaps usually results in plate
exposure, particularly in irradiated patients. The fibula free
flap provides a strong long segment of bone and can include a
large fasciocutaneous component as well. As such this
versatile flap may be harvested as an osteocutaneous flap or a
purely osseous flap. It is now the most popular method of
mandibular reconstruction. The free fibula flap provides a
successful bone flap with an acceptably low complication rate
[1, 2]. Fibular bone allows to plan osteotomies in relation to
the orientation of the bone and its vascular pedicle. Thick
cortical bone readily accepts plates and screws for a secure
interosseous fixation and osteointegrated implants may be
placed in this bone safely. Another advantage of the free
fibular flap is that in case of the insufficient bone height for the
prosthetic rehabilitation either a double barrel or distraction
osteogenesis (DO) can be carried out [3]. Optimization of the
height di? erential between the native mandible and the ?bula
in selected patients may be achieved by placing the ?bula
approximately 1 cm superior to the inferior border of the
mandible [4]. Moreover, the free vascularized flaps are not
MICROVASCULAR RECONSTRUCTION OF MANDIBLE BY FREE FIBULAR FLAP
Journal of Dental Sciences
University
Key words: Fibula Flap. Autogenous flap. Reconstruction. Mandible.
Source of support : NillConflict of interest : None
Maxillofacial Reconstruction and Technics

expensive as compared to other methods and may provide
cost saving for selected patients. Among other alternatives
like scapular and iliac crest flaps, fibular flap has many
advantages for mandibular reconstruction and represents the
first choice for the head and neck surgeon [5]. In the field of
contemporary head and neck reconstructive surgery, free
vascularized tissue transfer is becoming a gold standard. The
current study was designed to determine the results of using
the free vascularized fibular flap for comprehensive
reconstruction of mandibular defects.
METHODOLOGY : This case series was conducted at
Department of Oral and Maxillofacial Surgery in association
with Department of Plastic and Reconstructive Surgery for
over a period of more than 4 years from May 2010 to Mar
2014.
The patients having mandibular defects or those needing
mandibular resection were selected. Medically fit patients of
either gender with an age range of 21-60 years were the
subjects of this study.
Patients, with abnormalities of the lower leg vascular
anatomy i.e. impaired circulation of the leg, with extensive
leg trauma and those who were diabetic and had significant
venous stasis or peripherial oedema, poor circulation or
healing, or cutaneous ulcers were excluded from the study.
An informed consent was obtained from them or their
parents/guardians for including their data in research. The
procedure, purpose with risks and benefits and treatment
alternatives were discussed with them. Baseline
investigations were carried out. Laboratory studies based on
patient history, coagulation status were done. Chest
radiography and CT scan was done to assess the presence of
chronic obstructive pulmonary disease and metastasis in case
of malignant lesions. Pre-operative Doppler examination or
MR angiography was done to assess the patency of the
peronneal vessels (Fig-1). Likewise routine examination of
patients with trauma or those who required secondary
reconstruction was carried out.
Ablative surgery of the tumor was done in the case of primary
reconstruction, while a recipient site was prepared for
secondary reconstruction especially for the vascular
anastomosis (Fig-2). Depending upon the case either the
facial artery or lingual artery was used for the anastomosis.
For better pedicle orientation contralateral fibula was selected
as the donor tissue. To reduce the operative time,
simultaneous harvesting of the free fibular flap was done by
the reconstructive surgeon keeping in mind the dimension of
the defect present or produced. Depending on the requirement
either osseous or osteomycutaneous free fibular flap was
harvested to reconstruct either the bone or composite defect
(Fig-3).
A tourniquet inflated to 350mm was used during harvesting.
As per requirement approx. 16 cms long incision was placed
on the lateral surface through the skin, superficial fascia to
expose the soleous and peroneous longus muscle. Skin
pedicle when required was marked as per the requirement.
Dissection was carried to expose the lateral surface of the
peroneous muscle. Peroneous muscle was traced to expose
the fibula, peroneal vessel was identified at lower 1/3rd of the
fibula. Proximally 6 cms of bone was preserved to avoid
injury to the peroneal nerve. Distally 8 cms of bone was left to
support the ankle. Hemostasis was achieved, suction drain
placed closure was done in layers by 3-0 vicryl sutures.
Fibular flap was contoured to the shape of mandible by
performing multiple closing osteotomies as per indication.
The rigid fixation of the flap to the native bone was achieved
using miniplates (Fig-4). The protocol followed was a 6 holed
miniplate at the wedge osteotomy in body region and a curved
4-holed orbital miniplate with gap at the angle osteotomy as
per requirement. Anastomosis was carried out using
operating microscope with the recipient vessel either the
facial or lingual vessels. Venous filling and arterial pulsation
was found proximal to the anastomosis following the
procedure. As per the institutional protocol a three drug
antibiotic regimen was followed i.e. Inj cefotaxime1 gm 8
hrly, Inj amikacin 500mg 12 hrly, Inj clindamycin 600mg iv 8
hrly, Inj LMWH 2500IU 12 hourly, Inj Morphine 1mg/ hrly
after 3 hours (stopped 2 days postoperatively), Inj ketorolac
30 mg IV 8 hourly, Inj ranitidine (50mg) IV 8 hrly, Tab
Chymoral forte 2 TDS 6 hourly, Tab Paracetamol 6 hourly.
Postoperatively, patients' recovery was uneventful. Patients
were placed on nasogastric tube feed in the early
postoperative period. The patients were allowed to ambulate
in a non-weight bearing fashion on the second postoperative
day. The first postoperative visit was generally scheduled 1-2
weeks after release from the hospital. Flap and skin flap
viability were assessed. Postoperatively the patency of the
anastomosed vessel was confirmed with Doppler
examination (Fig-6). The recipient site was closely
monitored for early identification of any vascular
compromise. After healing of the donor site physical therapy
was instituted to restore ankle function. Adequate measures
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 40
University J Dent Scie 2015; No. 1, Vol. 3

were taken to avoid complications at donor and recipient sites.
Early operative intervention was considered for flap salvage
due to venous or arterial thrombosis or if twisting of the
pedicle had occurred.
Operative time, hospitalization period, donor site morbidity,
duration of NG tube feeding, postoperative complications
such as infection dehiscence, skin necrosis were noted. The
collected data was analyzed by SPSS statistical version 11.
The variables under study were age, sex, diagnosis, operative
time, donor site morbidity, and flap survival, duration of NG
tube feeding and postoperative complications (infection,
dehiscence, skin necrosis, and delayed wound healing or
fistula formation). Simple descriptive statistics were used.
Numerical variables like age, operative time, duration NG
tube feeding were analyzed using mean and standard
deviation and for qualitative variables like diagnosis, donor
site morbidity, flap survival and postoperative complications,
frequency distribution tables were made for them.
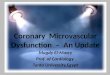
RESULTS : This study was carried out on 18 patients who
underwent reconstruction with fibula free flap for mandibular
defects (Table-1). Among these, 13 patients were males
(72.2%) and 5 were females (27.8%) with the male female
ratio was 2.6:1. The age of the patients presented with some
lesion or defect ranged between 24-55 years with the mean
age of 38.72 years.
Resection followed by primary reconstruction was done in 12
patients (70%) and secondary reconstruction was done in 6
patients (30%). Out of the 6 patients who were secondarily
reconstructed one had odontogenic keratocystic, one had
squamous cell carcinoma of the alveolar ridge one had
ameloblastoma and three cases of GSW. Out of the 12 patients
where primary reconstruction was done 7 had
ameloblastoma, 1 had OKC. 1 had osteosarcoma and 3 cases
had Ca-alveolus.
The range of operation time was 6-8 hours with average time
of 6.4 ±0.4 hours. The range of hospital stay was 14-29 days
and average stay was 18.8 ±.4.77 days. The range of duration
of NG tube was 12-25 days and average duration was 15.6 +
4.2 days.
Donor site morbidity included wound scarring in 3 patients
(16.7%). All patients were ambulated within 5 weeks. Major
donor site complications were uncommon. Skin flaps, when
used, were survived well. Range of motion of the foot was a
little limited due to scarring and muscle resection but none of
the patients complained of ankle instability. Prolonged pain
was rare at donor site. Recipient site complications included
vascular complication in 2 flaps (11.76%).100% salvaged
following venous thrombosis by an urgent operative
intervention. Thrombectomy and revision of the thrombosed
vessels were performed. Wound infection occurred in 1
patient (5.5%), which were managed by local antiseptic
measures. Dehiscence of the wound occurred in 3 patients
(16.6%) and was resutured after the control of infection.
There was some delayed wound healing in 2 patients
(11.76%). One patient with osteosarcoma (5.5%) had plate
exposure was subsequently managed with local flap
advancement and primary closure. Due to the unfavorable
condition of the recipient bed and the formation of the fistula
two flaps failed one in patient with Ca alveolus and one
patient with GSW (Table-2). Out of 18 patients, 16 patients
(88%) had successful flap survival. Follow-up ranged from 8-
24 months. Six patients complained of trismus which might
be due to surgical manipulation and/or resection of the
masticatory muscles and disturbance in mandibular integrity.
Patients were counseled regarding jaw opening exercises to
minimize the impact of this complication. Patients were also
referred for the prosthodontic rehabilitation or for the
radiation therapy if indicated. DISCUSSION
Mandibular reconstruction continues to be one of the most
difficult challenges in reconstructive surgery. It plays a major
role in airway protection, support for the tongue, muscles of
the floor of the mouth, lower jaw dentition, articulation,
deglutition and respiration [6].
The goals of mandibular reconstruction are:
i) Establishment of mandibular continuity with
acceptable cosmetic result.
ii) Early return to function either by providing a stable
denture base or providing dental implants.
iii) Correction of soft tissue defect.
Therefore, a surgeon has to balance his procedure to achieve
best possible cosmetic appearance with reliable function. The
functions of chewing, swallowing, speech articulation and
oral competence must be addressed. In order to achieve it, one
must restore bony continuity, facial contour, tongue mobility
and speech. Dental rehabilitation must also be kept in mind.
Mandibular reconstruction represents a challenge to the oral
and maxillofacial surgeon and has been revolutionized by the
modern microvascular techniques. Non vascularized bone
flaps from various donor sites including the iliac crest, rib
and calvarial bones have been used for mandibular
reconstruction, either alone or in conjunction with pedicled
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 41
University J Dent Scie 2015; No. 1, Vol. 3

soft tissue flaps [7, 8, 9]. It is worth to mention that the flap
healing is significantly dependent on the quality of the
vascularity of the recipient bed.
The majority of patients requiring mandibular
reconstruction present with unfavorable recipient bed either
at the time of resection with contamination from the oral
cavity or subsequently because of adjuvant radiation
therapy. All these factors contribute significantly to failure
of conventional bone flaps [10,11]
The use of free bone flaps for mandibular reconstruction has
the obvious advantage of being a well-vascularized tissue that
can withstand the hostile environment of the oral cavity. The
donor site complication is a serious problem when planning a
free tissue transfer. Given the above condition in our case
series we still carried out secondary reconstruction in 06 of the
cases. Most of the cases where secondary reconstruction was
done were in early part of the study, where 3 patients one
ameloblastoma, one case of OKC and one case of Ca-alveolus
did not agree for harvesting of free fibular flap and in 3 cases
of GSW where there was gross contamination of the wound
with multiple splinters which could have compromised the
survival of the flap. In these cases the primary reconstruction
was done using a reconstruction plate, this acted as a guide
during our subsequent secondary reconstruction. The
problems faced during the secondary reconstruction was
severe scarring caused in the previously operated site leading
to difficulty in locating the vascular pedicle for anastomosis.
So care should be taken to preserve the vascular bed at the
time of primary reconstruction in those cases.
In this study the fibula free flap harvest appears to be
associated with acceptable donor site morbidity and
preservation of good foot and ankle function in most
individuals.
The average operative time was 6 hours and 40 minutes. It
also depends upon that whether the defect was primarily
reconstructed or it was done as a second stage procedure. This
is consistent with those in larger series [12]. The advantages
of revascularized free flap are achieved at the cost of the
procedure that is longer than other conventional
reconstructive procedures. Foster and co-workers also
concluded that additional operative time is required for a free
flap reconstruction [13].
Average hospital stay was 14-28 days with an average of
18.37 + 4.52 days. This time was a little longer than those,
which are mentioned, in recent patient series [13,14]
The range of NG tube dependencies was 14-36 days with an
average of 21.6 + 7.31 days. This wide range was due to the
fact that those patients who had failure of their flaps had
extended period of NG tube dependency. However, in
recently published studies the NG tube dependency is less in
patients who underwent revascularized free tissue transfer as
compared to the pedicle flaps [15].
Tosoco and co-workers evaluated 18 patients of free fibular
flap reconstruction of the mandible which were resected for
central giant cell granuloma. In this study they also
prosthodontically rehabilitated the patients via implants.
They had best functional and esthetic results [16].
In the present study, the functional results were assessed as
regards deglutition, oral competence, and speech. Regarding
deglutition, 56% of our patients resumed normal diet and
44% patients tolerated only soft diet. None of our patients
was feeding tube dependent.
Hidalgo and Rekow reported 51% normal diet, 42% soft
diet and 7% feeding tube dependent [17]. Rivas et al reported
78% normal diet and 22% soft diet. The causes of diet
limitations in our patients were malocclusion, restricted
tongue mobility and insufficient dentition [18]. Chana et al
recommended simultaneous placement of osseointegrated
implants for ideal function, however, none of our patients
had osseointegrated implants, but two patients had dental
rehabilitation in the form of removable denture [19].
Peled reconstructed 13 patients (9 males, 4 females) of
discontinuity defects of the mandible with free fibular flap
[1]. Wound healing disturbance at the donor site occurred in 4
cases. Two flaps were lost with the success rate of 84%. In this
study there were two complete flap failures, one due to
unfavorable recipient bed of the patient with GSW and other
due to venous thrombosis. There was an overall success rate
of 88%, which is comparable to previously published studies.
Our success rate is comparable to study by Kroll et al who
reported 90% success rate that included 93 patients [20].
Hidalgo and Rekow salvaged 3 of 4 failing flaps to improve
what would have otherwise been 93% success rate to 98%
[17]. We had 1 free flap failure due to venous thrombosis,
salvage surgery attempted was not successful. Frequent
clinical observation of the flap, Doppler examination of the
pedicle by a trained staff would help in improving our chances
of early detection of free flap compromiseCONCLUSION
Within the last three decades major advances have been
made in the field of microvascular and reconstructive
surgery. In mandibular reconstruction the challenge is to
restore airway support, oral incompetence, articulation,
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 42
University J Dent Scie 2015; No. 1, Vol. 3

mastication, deglutition and acceptable cosmesis; thus,
allowing the patient to resume role in the society.
In this series the free fibula flap was a versatile and reliable
option for microvascular reconstruction of large mandibular
defects.
It provided a large quantity of bone, which could easily be
shaped and passively adapt to the remaining mandible.
In conclusion, we believe that vascularized fibula flap is a
versatile and reliable method of reconstruction of lateral as
well as antero-lateral mandibular defects. However, it is a
technically demanding surgery with high learning curve.
REFERENCES :
1. Peled M, El-Naaj IA, Lipin Y, Ardekian L. The use of free
fibula flap for functional mandibular reconstruction. J
Oral Maxillofac Surg 2005; 63:220-4.
2. Fonseca RJ. Reconstruction of the maxillofacial cancer
patient. In: Quereshy FA, Powers MP, editors. Oral and
maxillofacial surgery. Philadelphia: WB Saunders;
2000: 361
3. Shen Y, , Li J, Shi J, Ow A. Long-term results of
partial double-barrel vascularized fibula flap in
symphysis for extensive mandibular reconstruction. J
Oral Maxillofac Surg 2012;70:983-91
4. Rui Fernandes. Fibula Free Flap in Mandibular
Reconstruction. Atlas Oral Maxillofacial Surg Clin N
Am 2006; 143–150
5. Genden E, Haughey BH. Mandibular reconstruction by
vascularised free tissue transfer. Am. J. Otolaryngol
1996;17:219-27.
6. Nath S, Joshi KD, Shakya S, Shrestha S, Koirala U
Mandibular reconstruction. Kathmandu University
Medical Journal 2006;16:497-500. .
7. Soutar D, Scheker LR, Tanner NSB, MaGregor IA: the
radial forearm flap: A versatile method for intraoral
reconstruction. Br J Plas Surg. 1983; 36:1,
8. Serafin D, Villarrreal – Rios A, Feorgiade N: A rib
containing free flap to reconstruct mandibular defects.
Br J Plas Surg 1977;30: 263
9. Daniel RK: Mandibular reconstruction with free tissue
transfer. Ann Plas Surg 1978; 1: 346.
10. DeFries H.O., Marble H.B. and Sell K.W.:
Reconstruction of the mandible. Use of a homoflap
combined with autogenous bone and marrow. Arch.
Otolaryngol 1971; 93: 426-32.
11. Soutar D.S.: Mandibular reconstruction with
Sun J
vascularized bone. In Soutar D.S. and Tiwari R.
(editors): Excision and reconstruction in head and neck
cancer. Ediburgh Churchill Livingstone1994; 59
12. Rosenthal E, Carroll W, Dobbs M, Wax M, Peters G.
Simplifying head and neck micro-vascular
reconstruction. Head Neck 2004;26:930-6.
13. Foster RD, Anthony JP, Sharma A, Pogrel MA.
Vascularized bone flaps versus nonvascularized bone
flaps for mandibular reconstruction: an outcome
analysis of primary bony union and endosseous implant
success. Head Neck 1999; 21:66-71
14. Kroll SS, Evans GR, Goldberg D, Wang BG, Reece GP,
Miller MJ, et al. A comparison of resource cast and
reconstruction with free and pectoralis major flaps.
Plast Reconstr Surg 1997; 99:1282-6.
15. Chepeha DB, Annich G, Pynnonen MA, Beck J, Wolf
GT, Teknos TN, et al. Pectolaris major myocutaneous
flap vs. revascularized free tissue transfer:
complications, gastotomy tube dependency, and
hospitalization. Arch Otolaryngol Head and Neck Surg
2004;130:181-6.
16. Tosco P, Tanteri G, Iaquinta C, Fasolis M, Roccia F,
Berrone S, et al. Surgical treatment and reconstruction
for central giant cell granuloma of the jaws: a review of
18 cases. J Craniomaxillofac Surg 2009; 37:380-7
17. Hidalgo D.A. and Rekow A.: A series of 60 consecutive
fibula free flap mandible reconstruction. Plast. Reconstr.
Surg 1995;96: 585-96.
18. Rivas B., Carrillo J.F. and Granados M.: Oromandibular
reconstruction for oncological purposes. Ann. Plast.
Surg 2000; 44: 29-35.
19. Chana J.S., Chang Y.M., Wei F.C., Shen Y.F., Chan C.P.,
Lin H.N., Tsai C.Y. and Jeng S.F. Segmental
mandibulectomy and immediate free fibula
osteocutaneous flap reconstruction with endosteal
implant ideal treatment method for mandibular
ameloblastoma. Plast. Reconstr. Surg 2004; 113 : 80-87.
Kroll S.S., Schusterman M.A., Reece G.P., Miller M.J.,
Evans G.R., Robb G.L. and Baldwin B.J.: Choice of
flap and incidence of free flap success. Plast. Reconstr.
Surg 1996;98: 459-63.
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 43
University J Dent Scie 2015; No. 1, Vol. 3

Fig-1 Preoperative MR angiography.
Fig-2 Ablative surgery for the tumor and the resected specimen
Fig-3 Harvesting of the Free fibular Graft
Fig-4 Osteotomized Fibular graft
Fig-5 Reconstructed mandible with Fibular graft
Fig-6 Postoperative Doppler examination
Table 1 - Database of the patients.
Table 2 Relative percentage of the postoperative complications
Corresponding Author:
Dr. Ajay P. Desai
Dept of Oral & Maxillofacial Surgery, Army Dental
Centre (R&R), Delhi Cantt-110010
Email : [email protected]
University Journal of Dental Sciences, An Official Publication of Aligarh Muslim University, Aligarh. India 44
University J Dent Scie 2015; No. 1, Vol. 3