Embed Size (px)
Citation preview
8th International forum for RA
(IFRA)
Welcome to an international meeting
focused on
Rheumatoid Arthritis
Saturday September 23d – Tuesday September 26th 2017
Aula Medica, Karolinska Institutet, Stockholm, Sweden
www.RAforum2017.com
Official program
Organizers: Rheumatology Karolinska (main responsible prof Lars Klareskog) together with co-
organizers prof Zhanguo Li, (Beijing) and prof Kazuhiko Yamamoto (Tokyo)
www.RAforum2017.com
Most welcome to the 8th International Forum for Rheumatoid Arthritis, this time in Stockholm. The meeting aims to present progress in RA research and outline prospects and plans for coming years. A major focus of the meeting is to present and discuss research on the causes of the dis-ease, and of the gradual development of various symptoms with the hope that such knowledge will not only help to treat the disease earlier and better, but ultimately also prevent its occur-rence. Meetings with the name RA Forum have since 2009 been organized in China (Beijing) and in 2016 in Japan (Tokyo) and the present meeting in Stockholm aims to further de-velop the scope of RA Forum, by assembling clinicians and scientists from all over the world with a special interest in the disease RA – which so far has rarely been the entire focus of internation-al meetings. We believe that this focus will allow us to make and create new contacts, visions and joint pro-jects in RA research. The meeting is organized in several sessions reaching from epidemiology to molecular sciences and includes also sessions on treatment and prevention. As a major purpose of the meeting is to discuss and define new research agenda, we have reserved time in the end of each session for dis-cussion on the presented results and implication for further research – all led by the chairper-sons of the session. We hope that this somewhat different organization of the meeting with a big role of the chairper-sons, will enable many forward-looking discussions and allow us to leave the meeting with new ideas on how to further develop research care and prevention of RA. Yu are all most welcome !! Lars Klareskog, on behalf of the rest of the organising committee With financial support from

www.RAforum2017.com
8th International Forum for RA 2017 - Program
12:30
13:00–14:00
Registrationopen
Lunch
Saturday, September 23, 2017
14:00–14:15 WelcomeandintroductiontothehistoryofandpurposeofIFRA
LarsKlareskog,ZhanguoLi,KazuhikoYamamoto
JIMWelcomeaddress
AndersEkbom,ProfessorKI,MemberoftheeditorialboardofJournalofInternalMedicine
Session 1: The good aspects of the situation today and how we arrived here
14:15–14:45
Chairs:ZhanguoLi,KazuhikoYamamoto
Fromideasinresearchtoclinicalbenefits.Thelongtermperspectives
SirRavinderMaini,KennedyInstitute,UniversityofOxford
Session 2: The unresolved clinical and scientific problems of today – and why are they unresolved?
Chairs:ToreKvien,OsloUniversityandAlisonKent,PARE/EULAR
14:50–15:15Patients’needsandcurrentscientificapproachestoRA;Notalwaysaligned.
JohanAskling,KarolinskaInstitutet,Stockholm
15:15–15:40Unresolvedproblemsasseenfromtheclinician’sperspective
MereteHetland,CopenhagenUniversity
15:40–16:05Scientificunresolvedproblemsinscience
ChrisBuckley,UniversityofBirmingham
16:05–16:30
Discussionsonneedfornovelsolutionstoadessthemostimportantunresolvedquestions
Discussionledbychairpersons
16:30–17.00 Afternoonbreakwithteaandcoffee
Session 3: Why do we get RA (1st part); What can we learn from genetic epidemiology and genomics?
Chairs:MikeBrenner,HarvardMedicalSchoolandAnneBarton,TheUniversityofManchester
17:00–17:25Polygenicburdensoncell‐specificpathwaysunderlietheriskofrheumatoidarthritis
KazuhikoYamamoto,UniversityofTokyo
17:25–17:50Rheumatoidarthritis:theroleofenvironmentandgenes
JillNorris,Denver
17:50–18:15
Combininggeneticsandepigeneticdatatodefinekeypathogenicsinglecellpopulationsinrheumatoidarthritis
SoumyaRaychadhuri,HarvardMedicalSchool,Boston,MA

www.RAforum2017.com
18:15–18:30
Selectedabstract:TheassociationbetweenHLA‐DRB1allelesandriskofrheumatoidarthritisisinfluencedbymassivegene‐geneinteractions
Lina‐MarcelaDiaz‐Gallo,KarolinskaInstitutet,Stockholm
18:30–19:00
Discussionsonstrategicthinkingconcerningcombinationsofcohortsandbiomarkersforfuturedesignofstudiesonpathogenesis,preventionandtherapy
Discussionintroducedandledbychairpersons
19:00–21:00 ReceptionatAulaMedica
Sunday, September 24, 2017
Session 4: Why do we get RA? (2nd part) The longitudinal course of RA
Chairs:AnnaRudin,GothenburgUniversityandMikeHolers,UniversityofColoradoatDenver
8:30–8:55Fromtriggeringtotargeting;thelongitudinalcourseofseropositiveRA
AncaCatrina,KarolinskaInstitutet,Stockholm
8:55–9:20AutoantibodiesandtheirglycosylationduringemergenceofRA
HansUlrichScherer,LeidenUniversity
9:20–9:45ACPAs,NETsandinflammation.Newlightonneutrophils
MarianaKaplan,NIH,Bethesda,MA
9:45–10:20
PathobiologyofRheumatoidArthritis:TowardsaMolecularDefinitionandPrecisionMedicine
CosPitzalis,London
10:20–10:50 Morningbreakwithcoffeeandfruits
Session 5: Why do we get RA? (3rd part): Microbes and RA
Chairs:ReneToes,LeidenUniversityMedicalCenterandSolbrittRantapää‐Dahlqvist,UmeåUniversity
10:50–11:15ThebacterialwaytowardsRA1:TheporphyromonasandPADpathway
KarinLundberg,KarolinskaInstitutet,Stockholm
11:15–11:40ThebacterialwaytowardsRA2:TheAggregatibacterandhypercitrullinationway.
FelipeAndrade,JohnsHopkins,Baltimore,MD
11:40–12:05RoleofthemicrobiomeinthepathogenesisofRA
XuanZhang,PekingUnionMedicalCollege
12:05–12:30DiscussionsonstrategiestounderstandthetriggersandearlystagesofRA
Discussionintroducedandledbychairpersonsfromsession4and5
12:30–13:30 Lunch

www.RAforum2017.com
Session 6: Adaptive vs. Innate immunity and mesenchymal functions as driving forces in RA
Chairs:AndyCope,King’sCollegeLondonandSteffenGay,UniversityofZürich
13:30–13:55RoleofspecificBandTcellsimmunityinRA
VivianneMalmström,KarolinskaInstitutet,Stockholm
13:55–14:20TheBcellrepertoireinRA
DanMueller,UniversityofMinnesota
14:20–14:45
EffectsofmonoclonalantibodiesfromRApatientsoninnatefunctionsofsynovialcells
BillRobinson,StanfordUniversity,CA
14:45–15:00Selectedabstract:MonoclonalACPA‐IgGfeatureextensiveFabglycosylation
KatyLloyd,KarolinskaInstitutet,Stockholm
15:00–15:15Selectedabstract:ThemutatedRNAsplicingproteinhnrnp‐a3isanovelautoantigeninsystemicrheumaticdiseasesalinktoWarburgeffectinRA
BiankaMarklein,ChariteUniversity,Berlin
15:15–15:45HowcanwecombineunderstandingofmesenchymalandimmunefunctionsinRA?
IainMcInnes,UniversityofGlasgow
15:45–16:10DiscussionsonthedrivingforcesofRA
Discussionintroducedandledbythechairpersons
16:10–16:40 Afternoonbreakwithcoffee
Session 7: Mechanisms of pain in RA
Chairs:CarlTuresson,LundUniversityandCodrutaFilip,PARE/EULAR
16:40–17:05PainandcognitioninRA,Whicharethecentralmechanisms?
GeorgSchett,ErlangenUniversityClinic
17:05–17:30
LongitudinaldevelopmentofpaininRA
JonLampa,KarolinskaInstitutet,Stockholm
17:30–17:55Antibody‐mediatedpain
CamillaSvensson,KarolinskaInstitutet,Stockholm
17:55–18:15 Discussionintroducedandledbythechairpersons
18:15–19:30
Posterswithpostercompetition,discussionclubsandotherinformalmeetingswithwineandcheese(posterscanbeputupduringSundayafternoonandhavetobetakendownaftertheendofthepostersession.)
Speakersdinner

www.RAforum2017.com
Monday, September 25, 2017
Session 8: Adaptive vs innate immunity and mesenchymal functions in RA (continued)
Chairs:LisavanBaarsen,AMCandTBC
8:30‐8:55MFAP5playsakeyroleininvasionofFL‐likesynoviocyteinRA
HujiXu,TsinghuaUniversitySchoolofClinicalMedicine,andTheSecondMilitaryMedicalUniversity,China
8:55‐9:20Genetics,TcellspecificityandTcellregulationinRA
JaneBuckner,BenaroyaResearchInstitute,Seattle,WA
9:20–9:45HowcanadaptiveimmunefunctionsinfluencestromalcellsinRA?
CarolineOspelt,UniversityofZürich
9:45–10:00
Selectedabstract:Machinelearningusingrheumiatoidarthritissynovialgeneexpressiondatadefineshistologicfeaturesthatcorrelatewithsystemicinflammationandautoantibodies
DanaOrange,RockefellerUniversity
10:00–10:20 Discussionsintroducedandledbythechairpersons
10:20–10:45 Morningbreakwithcoffee
Session 9: Genetics and function of citrullination and PAD and other post‐translational modifications in RA
Chairs:CarolineGrönwall,KarolinskaInstitutetandGerPruijn,RadboudUniversity
10:45‐11:00Introductiontopost‐translationalmodifications
GerPruijn,RadboudUniversity,Nijmegen
11:00–11:25TherolesofPADsinRA
HirofumiShoda,UniversityofTokyo
11:25–11:50Roleofosteoclastsinboneinflammation
HiroshiTakayanagi,UniversityofTokyo
11:50–12:05Selectedabstract:RA‐associatedantibodiestargetingposttranslationalmodificationhavedifferentosteoclastogenesispotential
AkilanKrishnamurthy,KarolinskaInstitutet,Stockholm
12:05–12:30 Discussionsintroducedandledbythechairpersons
12:30–13:45 Lunch
Session 10: Can we prevent RA?
Chairs:Chairs:DimitrisBoumpas,BiomedicalResearchFoundationAcademyOfAthensandLarsAlfredsson,KI
13:45–14:10Trialsforprevention:Howtodoit?
TomHuizinga,LeidenUniversityMedicalCenter
14:10–14:35ModifiableriskfactorsforRA
SaedisSaevarsdottir,KarolinskaInstitutet
14:35–15:00Howtounderstandandmeasure“subjectivesymptoms”thatmatterforthepatient?
KarimRaza,UniversityofBirmingham
15:00–15:30 Afternoonbreakwithcoffee

www.RAforum2017.com
Session 11: New ways of understanding the individual’s most urgent problems and how they change over
time; What role for e‐health
Chairs:GerdBurmester,Charité,BerlinandIngerGjertsson,UniversityofGothenburg
15:30–15:55EmergingopportunitiesfordigitalhealthresearchinRA
WillDixon,UniversityofManchester
15:55–16:20Meetingthepatientsearlywithanapp:Whatoptionsandwhatobstacles?
SofiaErnestam,KarolinskaInstitutet
16:20–17:05Whatwillhappenwith“patientreportedoutcomes”inthefuture?
ToreKvien,OsloUniversity
17:05–17:30 Discussionintroducedandledbythechairpersonsfromsession10and11
18:30 LeaveforCityHall(busseswillleavefromoutsideAulaMedica)
19:00ThereceptionintheCityHallishostedbytheStockholmCountyCouncilandtheCityofStockholm
Tuesday, September 26, 2017
Session 12: Future trials for prevention and curative treatments; Which strategies?
8:30–8:55
Chairs:MarcFeldmann,UniversityofOxfordandRonaldvanVollenhoven,KIandUniversityofAmsterdam
Tolerancetherapies–willtheybecomereal?
RanjenyThomas,UniversityofQueensland
8:55–9:20TolerizingTcells
RikardHolmdahl,KarolinskaInstitutet
9:20–9:45Antigen‐specificimmunotherapy:toleranceorimmunemodulation?
DavidWraith,UniversityofBirmingham
9:45‐10:15 Morningbreakwithcoffee
10:15–10:40Newsmarttrialdesigns
JohnIsaacs,NewcastleUniversity
10:40–11:00BioelectronicMedicine:TechnologyTargetingMolecularMechanismsforTherapy
PederOlofsson,KarolinskaInstitutet
www.RAforum2017.com
Session 13: Future strategies for prevention and treatments of RA – a collaboration between academia,
industry and health care
chairs:LarsKlareskog(KI),MarcFeldmann(UniversityofOxford)andRonaldvanVollenhoven(KIandUniversityofAmsterdam)
11:00–12:30
Discussionwithrepresentativesfromacademia,industryandhealthcareledbythechairpersons
Perspectivesfromindustry,academiaandhealthcare;Howshouldwecombineoureffortstomakethenewgenerationofcurativeandpreventivetherapiesreal?
Confirmedguests:
AnishSuri,Janssen
AaronWinkler,Pfizer
StevenNadler,BMS
12:30–12:55AlternationsintonsilmicrobiotaassociatedwithRA
ZhanguoLi,BeijingUniversity
13:00 LunchandDepartures
Practical Information
Posters:CanbeputupfromSundaylunchtimeandshallbetakendownSundayeveningafterthepostersession.
OurvenueisAulaMedica,Nobelsväg6,Solna(KarolinskaInstitutetcampus)
TogetherefromArlandaairport:Useacreditedtaxicompany,wewouldrecommendTaxiStockholm+468150000orTaxiKurir+468300000.ThereisalsoatrainservicetothecentralofStockholmfromArlanda;Arlandaexpress.
PublictransportisrunbySL,theyofferavarietyofticketswhichallmustbeboughtbeforeenteringthetrainorbus.Planyourtravelhere:https://sl.se/en
www.RAforum2017.com
Last name First name E‐mail Company /Organisation
Abdelmoaty Sally [email protected] Karolinska Institutet
Alemo Munters Li [email protected] Swedish Reumatism Association
Alfredsson Lars [email protected] Karolinska Institutet
Almgren Malin [email protected] Karolinska Institutet
Alunno Alessia [email protected] University of Perugia
Andersson Maria [email protected] AbbVie AB
Andersson Åsa [email protected] Halmstad University
Andrade Felipe [email protected] Johns Hopkins UniversityAranda‐Guillén Maribel [email protected] Karolinska Institutet
Arkema Elizabeth [email protected] Karolinska Institutet
Askling Johan [email protected] Karolinska Institutet
Azali Payam [email protected] Danderyds sjukhus Stockholm
Baharpoor Azar [email protected] Karolinska Institutet
Barton Anne [email protected] University of Manchester
Berg Louise [email protected] Karolinska Institutet
Bergman Thomas [email protected] Karolinska Institutet
Bernmalm Anna [email protected] AbbVie
Bersellini Farinotti Alex [email protected]
Karolinska Institutet
Bi Li Qi [email protected] China‐Japan Union Hospital of Jinlin
Bing Liu [email protected] Henan People's Hospital
Boddul Sanjay [email protected] Karolinska Institute
Bokarewa Maria [email protected] University of Gothenburg
Brenner Michael [email protected] Medical School/ Brigham & Women's Hospital
Brink Mikael [email protected] Umeå University
Bucher Sara sara.magnusson‐[email protected] Universitetssjukhuset Örebro
Buckley Christopher [email protected] Universities Oxford and Birmingham
Buckner Jane [email protected] Benaroya Research Institute
Bäckdahl Liselotte [email protected] Karolinska Institutet MBB
www.RAforum2017.com
Bäcklund Johan [email protected] Karolinska Institute
Cai Weiwei [email protected] Karolinska Institute
Cai Xiaoyan [email protected] Guangzhou First Municipal Hospital
Carlberg Konstantin [email protected] Scilifelab
Carlberg Renée [email protected] Bristol‐Myers Squibb
Carlens Cecilia [email protected] Karolinska Universitetssjukhuset
Cerqueira Cátia Karolinska Institutet Chatzidionysiou Katerina [email protected] Karolinska Institutet
Chemin Karine [email protected] Karolinska Institutet
Chen Jinwei [email protected] second xiangya hospital
Chen Pei [email protected] CTS MICE SERVICE CO LTD
Chen Szu‐Ying szu‐[email protected] Karolinska Institutet
Chen Weiqian [email protected] the First Affiliated Hospital, Coll
Chen Zhu [email protected] ANHUI PROVINCIAL HOSPITAL
Cope Andrew [email protected] King's College London
Cui Yang [email protected] Guangdong General Hospital
Curman Charlotte [email protected] Pfizer
De Pablo Paola [email protected] University of Birmingham
De Vries Niek [email protected] AMC/University of Amsterdam
Degerlund Helene [email protected] Roche AB
Deleskog Anna [email protected] Sandoz A/S
Dellmark Yvonne [email protected] Karolinska Universitetssjukhuset
Deng Guo‐Min [email protected] Nanjing Medical University
Diaz Lina [email protected] Karolinska Institutet
Dimitris Boumpas [email protected] BRFAA
Ding Jian [email protected] Lihuili hospital of Ningbo City
Dixon William [email protected] The University of Manchester
Dong Xiaoying [email protected] TJMU GENERAL HOSPITAL

www.RAforum2017.com
Dorph Christina [email protected] Karolinska university hospital
Dubnovitsky Anatoly [email protected] Karolinska Institutet
Edvinsson Helene [email protected] Pfizer
Egnell Maud [email protected] Eli Lilly
Ekström Tomas [email protected] Karolinska Institutet
Elfverson Hanna [email protected] Thermofisher Scientific
Emamikia Sharzad [email protected] CLINTRID
Engström‐Laurent Anna anna.engstrom‐[email protected]
Dept.Public Health and Clinical Med
Enman Yvonne [email protected] Reumatikerförbundet
Erlandsson Harris Helena [email protected] Karolinska Institutet
Ernestam Sofia [email protected] SLSO / Karolinska Institutet
Fan Xiaoyun [email protected] The Affiliated No.1 Hospital of BMC
Fasth Andreas [email protected] Novartis
Fei Guozhong [email protected] Karolinska Institutet
Felix Nathan [email protected] Janssen R&D
Fernandez Gonzalo [email protected] Karolinska Institutet
Fischer Anita [email protected] Medical University of Vienna
Fogdell‐Hahn Anna anna.fogdell‐[email protected] Karlinska Institutet
Foxryd Preben [email protected] Pfizer
Fu Xiao [email protected] Univerzita Karlova
Fu Xinli [email protected] AffiliatedHospitaShandongUniversity
Gammeltoft Gerwien Jens [email protected] Eli Lilly
Gao Guanmin [email protected] the First Affiliated Hospital of Zh
Gay Steffen [email protected] Dept Rheumatology Univ Hospital Zurich, Switzerland
Ge Changrong [email protected] Karolinska Institutet
Gerstner Christina [email protected] Karolinska Institutet
Gjertsson Inger [email protected] Göteborgs Universitet, Reumatologi
Goodyear Carl [email protected] University of Glasgow
Grönwall Caroline [email protected] Karolinska Institutet
Gu Jieruo [email protected] Third Affiliated Hospital of Sun Ya
www.RAforum2017.com
Guenter Steiner [email protected] Medical University Vienna
Gunnarsson Karin [email protected] Karolinska Univerity Hospital
Guo Jianping [email protected] Peking University
Gülfe Anders [email protected] Lund University, Rheumatology
Hafström Ingiäld [email protected] Karolinska Institutet
Hagert Cecilia [email protected] University of Turku
Hallström Magnus [email protected] Sahlgrenska Universitetssjukhuset
Hambardzumyan Karen [email protected] Karolinska Institutet
Hansson Monika [email protected] Karolinska Institutet
Harju Anders [email protected] Handelsbolag, Harpo HB 969636‐6286
He Lan [email protected] UMICE
He Yibo [email protected] Karolinska Institutet
Hedenstierna Louise [email protected] Karolinska Institutet
Heiberg Turid [email protected] Oslo University Hospital
Hellgren Karin [email protected] Rheumatology Unit Karolinska University Hospital
Hermanrud Christina [email protected] Karolinska Institutet
Hernandez Susana [email protected] Karolinska Institutet
Hetland Merete [email protected] Rigshospitalet ‐ Glostrup
Hoffmann Markus markus.hoffmann@uk‐erlangen.de University of Erlangen‐Nuremberg
Holers Michael [email protected] University of Colorado Division of Rheumatology
Hou Yong [email protected] Peking UnionMedicalCollege Hospital
Houtman Miranda [email protected] Karolinska Institutet
Hu Dawei [email protected] Renji Hospital Affiliated to Shangh
Hu Xiaobin [email protected] Hospital of traditional Medine
Huang Anbin [email protected] Wuhan Union Hospital
Huang Yanhong [email protected] Beijing Jishuitan Hospital
www.RAforum2017.com
Huizinga Tom [email protected] Leiden University Medical Center Hultgård Ekwall Anna‐Karin [email protected] Sahlgrenska Akademin
Idborg Helena [email protected] Karolinska Institutet
Ilar Anna [email protected] Karolinska Institutet
Illescas Rodriguez Vera [email protected]
Isaacs John [email protected] Newcastle University
Israelsson Lena [email protected] Karolinska Institutet
Jakobsson Per‐Johan per‐[email protected] Karolinska Institutet
James Jaime Rose [email protected] Karolinska Institute
Jenning Madeleine [email protected] Charité Universitätsmedizin Berlin
Ji Lanlan [email protected] Peking University First Hospital
Jia Ru Lin [email protected] Peking University People's Hospital
Jiajia Liu [email protected] Peking University People's Hospital
Jiang Long [email protected] Karolinska Institutet
Jimenez‐Andrade G Yanek [email protected] Karolinska Institutet
Jiping Wu [email protected] Dongguan People's Hospital
Johannesson Martina [email protected] Karolinska Institutet
Johansson Eva C. [email protected] PRP / Swedish Rheumatism Association
Johansson Linda [email protected] Umeå Universitet
Johnston Lynsey [email protected] University of Leeds
Jun Wu [email protected] Huitian Pharmaceutical Co.,Ltd
Jurczak Alexandra [email protected] Karolinska Institutet
Kampstra Sanne [email protected] Leiden University Medical Center
Kaplan Mariana [email protected] National Institutes of Health
Karlsson Marie‐Louise marie‐[email protected] Karolinska Universitetssjukhuset
Kastbom Alf [email protected] Linköping University Hospital
Kharlamova Anastasia [email protected] Karolinska Institutet
www.RAforum2017.com
Kisten Yogan [email protected] Karolinska Institutet
Klareskog Lars [email protected] Karolinska Institutet
Klein Kerstin [email protected] University Hospital Zurich
Klosinska Linder Maria [email protected]
Reumatologklin i Sunderby Sjukhus
Knutsson Susanna [email protected] Bristol‐Myers Squibb
Koen Vos [email protected] Academic Medical Center, Amsterdam
Kokkonen Heidi [email protected] Umeå University
Korotkova Marina [email protected] Karolinska Institutet
Kozhukh Genadiy [email protected] KI
Krishnamurthy Akilan [email protected] Karolinska Institutet
Krock Emerson [email protected] Karolinska Institutet
Krönke Gerhard gerhard.kroenke@uk‐erlangen.de University of Erlangen
Kvien Tore Kristian [email protected]
Dept of Rheumatology, Diakonhjemmet Hospital
Kämpe Olle [email protected] Karolinska Institutet
L Schultzberg Carin [email protected] AbbVie AB
Lampa Jon [email protected] Dept of Rheumatology, KI
Larsson Esbjörn [email protected] Eli Lilly
Le Bars Manuela [email protected] Janssen
Le Maitre Erwan [email protected] Karolinska Institutet
Lend Kristina [email protected] Karolinska Institutet
Leng Nan [email protected] XIJING HOSPITAL
Li Caifeng [email protected] Beijing Children's Hospital
Li Cunyan [email protected] The People’s Hospital of Hunan
Li Fen [email protected] THE SECOND XIANGYA HOSPITAL OF CSU
Li Hong [email protected] Linyi People’s Hospital
Li Qin [email protected] Qinghai Hospital of traditional Chi
Li Shiguang [email protected] PFIZER INVESTMENT CO., LTD
Li Taotao [email protected] Karolinska Institutet
Li Xia [email protected] Dalian Medical University
Li Xiaomei [email protected] Anhui provincial hospital
www.RAforum2017.com
Li Yinong [email protected] Affiliated Fujian Wujing Hospital
Li Yuhui [email protected] People's Hospital of Peking Univers
Li Zhanguo [email protected] UMICE
Liao Hua [email protected] Beijing Anzhen Hospital
Lindberg Tülay [email protected] Karolinska Institutet
Lindencrona Jan Alvar [email protected] Karolinska Institutet
Lindgren Inger [email protected] MedicILAB
Lindqvist Elisabet [email protected] Skånes Universitetssjukvård
Lindqvist Joakim [email protected] Karolinska Institutet
Lindroos Eva [email protected] Karolinska Institutet
Lindskog Hans [email protected] Bristol‐Myers Squibb
Ling Guanghui [email protected] The Second Xiangya Hospital
Liu Yanying [email protected] Peking University People's Hospital
Lloyd Katy [email protected] Karolinska Institutet
Lu Jing [email protected] The First Hospital of China Medica
Lu Yue Wu [email protected] BEIJING CHAOYANG HOSPITAL
Lubberts Erik [email protected] Erasmus MC, University Medical Cent
Lundberg Ingrid [email protected] Karolinska Institutet
Lundberg Karin [email protected] Karolinska Institutet
Lundblad Per [email protected] Reumabulletinen Mediahuset i Gbg AB
Lundell Anna‐Carin anna‐[email protected] Gothenburg University
Luo Jing [email protected] Shanxi Medical University
Lv Xing [email protected] China
Lydén Malin [email protected] Landstinget Kalmar län,
Lyu Liangjing [email protected] Renji Hospital
Lönnblom Erik [email protected] Karolinska Institute
Maini Ravinder [email protected] Kennedy Institute of Rheumatology
Maldonado Michael [email protected] Bristol‐Myers Squibb
Mark Linda [email protected] Sahlgrenska Academy
Marklein Bianka [email protected] Charite/ Rheumatolog. Forschungslab
Martinsson Klara [email protected] Linköping University

www.RAforum2017.com
Mathsson Alm Linda linda.mathsson‐[email protected] Thermo Fisher Scientific
Mcinnes Iain [email protected] University of Glasgow
Melasniemi Jonna [email protected] Bristol‐Myers Squibb
Mia Muhammad Sohel [email protected] Karolinska Institutet
Moberg Martin [email protected] Eli Lilly
Morado Urbina
Carlos Eduardo [email protected]
Karolinska Institutet
Mueller Daniel [email protected] University of Minnesota Medical School
Möller Petronella [email protected] Sandoz A/S
Nadler, Phd Dr. Steven [email protected] Bristol Myers Squibb
Nascimento Diana [email protected] Karolinska Institutet
Neofytou Christina [email protected] Karolinska Institutet
Neregård Petra [email protected] Centrum för reumatologi
Niklason Anders [email protected] Pfizer
Nilesh Agalave [email protected] Karolinska Institutet
Nisell Ralph [email protected] Centrum för Reumatologi
Nordström Inger [email protected] Gothenburg University
Norin Ulrika [email protected] Karolinska Institutet
Norkko Julia [email protected] Karolinska Institutet
Norris Jill [email protected] Colorado School of Public Health
Nortamo Pekka [email protected] Eli Lilly
Notarnicola Antonella [email protected] Karolinska Institutet
Nyman Ulf [email protected] Utsikten
Oke Vilija [email protected] Karolinska University Hospital
Olofsson Peder [email protected] Karolinska Institutet
Opava Christina [email protected] Karolinska institutet
Orange Dana [email protected] Rockefeller University
Ospelt Caroline [email protected] University of Zurich
Ossipova Elena Karolinska Institutet
Ota Mineto mioota‐[email protected] The University of Tokyo
Padyukov Leonid [email protected] Karolinska Institutet Palm Gustafsson Ulrika ulrika.palm‐[email protected] Bristol‐Myers Squibb
Pan Yunfeng [email protected] THE THIRD AFFILIATED HOSPITAL,SYSU
Panda Sudeepta Kumar [email protected] Karolinska Institute
www.RAforum2017.com
Parodis Ioannis [email protected]
Peng Linyi [email protected] Peking Union Medical College Hospit
Pihl Maria [email protected] Eli Lilly
Pitzalis Costantino [email protected]
William Harvey Research Institute Queen Mary University of London
Pratt Arthur [email protected] Newcastle University
Pruijn Ger [email protected] Radboud University
Qiang Guo [email protected] Shanghai Renji Hospital
Ramsköld Daniel [email protected] Karolinska Institutet
Rantapää Dahlqvist Solbritt [email protected] Umeå University
Rao Navin [email protected] Janssen Research & Development
Raychaudhuri Soumya [email protected] Brigham and Women's Hospital
Raza Karim [email protected] University of Birmingham
Reimertz Claus [email protected] Sanofi
Réthi Bence [email protected] Karolinska Institutet
Ringh Mikael [email protected] Karolinska Institutet
Robinson William [email protected] Stanford University
Rossides Marios [email protected] Karolinska Institutet
Rostvall Gloria [email protected] Karolinska Institutet
Rudin Anna [email protected] The Sahlgrenska Academy at University of Gothenburg
Rudjito Resti [email protected] Karolinska Institutet
Rydell Emil [email protected] Institutionen för Kliniska Vetenska
Saevarsdottir Saedis [email protected] Karolinska Institutet
Sahlström Peter [email protected] CMM/Charité
Salter Hugh [email protected] Anocca AB
Sandman Maria [email protected] Eli Lilly
Sardar Samra [email protected] University of Copenhagen
Saxena Amit [email protected] Karolinksa Institutet
Scheel‐Toellner Dagmar [email protected] University of Birmingham
Scherer Hans Ulrich [email protected] Leiden University Medical Center
www.RAforum2017.com
Schett Georg georg.schett@uk‐erlangen.de Universitätsklinikum Erlangen
Seddighzadeh Maria [email protected] MSD
Seidman Jade [email protected] Synergy Medical
Sener Zeynep [email protected] Karolinska Institute
Shang Mingmei [email protected] KI
Shen Hui [email protected] The First Hospital Of China Medical
Sherina Natalia [email protected] Karolinska Institutet
Shi Yunzhen [email protected] Guang Dong General Hospital
Shoda Hirofumi shoda‐[email protected] Tokyo University
Sippl Natalie [email protected] Karolinska Institutet
Sizhao Li [email protected] China‐Japan Friendship hospital
Sjöholm Louise [email protected] KI
Skougaard Nielsen Marie [email protected] The Parker Institute
Skriner Karl [email protected] Charite
Steen Johanna [email protected] Karolinska Institutet
Stenberg Jan [email protected] Biogen
Stevenaert Frederik [email protected] Janssen Pharmaceutical cies
Stolt Patrik [email protected] To be announced
Studenic Paul [email protected] Medical University of Vienna
Stålesen Ragnhild [email protected] Karolinska Institutet
Su Yin [email protected] Peking University People's Hospital
Sun Erwei [email protected] Southern Medical University
Sun Meng [email protected] Karolinska Institutet
Sun Mingshu [email protected] The Affiliated Hospital of Qingdao
Sun Xiaolin [email protected] Peking University People's Hospital
Sundberg Erik [email protected] Karolinska
Suri Anish [email protected] Janssen, J&J
Svensson Camilla [email protected] Karolinska Institutet
Svenungsson Elisabet [email protected] Karolinska Institutet
Söderbergh Annika [email protected] Örebro Universitetssjukhus
Takayanagi Hiroshi [email protected] The University of Tokyo

www.RAforum2017.com
Tang Yanchun [email protected] YTYHD HOSPITAL
Tao Jinhui [email protected] Anhui Provincial Hospital
Tengelin Sara [email protected] Sandoz A/S
Thomaidi Eleni [email protected] Universitetssjukhuset Örebro
Thomas Ranjeny [email protected] University of Queensland
Tidblad Liselotte [email protected] Karolinska Universitetssjukhuset
Tideström Margareta [email protected] Karolinska institutet
Tinna Ängeby‐Möller [email protected]
Karolinska Institutet
Tjärnlund Anna [email protected] Karolinska Institutet / UCB
Toes René [email protected] Leiden University Medical Center
Trollmo Tina [email protected] Roche AB
Tsuchiya Haruka [email protected] The University of Tokyo
Tu Shenghao [email protected] Tongji Hospital
Turcinov Sara [email protected] Karolinska Institutet
Turesson Carl [email protected] Skåne University Hospital
Urbonaviciute Vilma [email protected] Karolinska Institutet
Vaartjes Danielle [email protected] Karolinska Institutet
Waldenlind Kristin [email protected] Karolinska Institutet
Wallman Thomas [email protected] Sanofi Genzyme
Van Baarsen Lisa [email protected] Academic Medical Center
Van Schie Karin [email protected] LUMC
van Vollenhofen Ronald [email protected]
Karolinska Institutet/ University of Amsterdam
Wang Bing [email protected] Dalian Medical University
Wang Jibo [email protected] The Affiliated Hospital of QDU
Wang Yan [email protected] Karolinska Institutet
Wang Yuxuan [email protected] Peking University People's Hospital
Wenfeng Tan [email protected] Jiangsu Province Hospital
Wermeling Fredrik [email protected] Karolinska Institutet

www.RAforum2017.com
Westerlind Helga [email protected] Karolinska Institutet
Wick Cecilia [email protected] Karolinska Institutet
Wigerblad Gustaf [email protected] Karolinska Institutet
Winkler Aaron [email protected] Pfizer Inflammation and Immunology
Vinko Palada [email protected] Karolinska Institutet
Volkov Mikhail [email protected] Leiden University Medical Center
Wollheim Frank [email protected] Lund University
Wraith David [email protected] University of Birmingham
Wu Huaxiang [email protected] The 2nd Affiliated Hospital
Wu Jianxiong [email protected] Guangzhou Orthopedic Hospital
Wu Lijun [email protected] PEOPLE'S HOSPITAL OF XINJIANG UAR
Wållberg Jonsson Solveig [email protected] Umeå Universitet
Wänkkö Katarina [email protected] Reumatomogen Sunderby sjukhus
Xu Bingze [email protected] Karolinska Institute
Xu Guoli [email protected] Peking University People's Hos
Xu Haijun [email protected] AbbVie Pharmaceutical Trading(SH)
Xu Jianhua [email protected] The Affiliated No.1 Hospital of AMU
Xu Liang [email protected] Yijishan hospital of Wannan medical
Yamamoto Kazuhiko [email protected] RIKEN Center for Integrative Medical Sciences
Yan Bing [email protected] WestChinaHospitalSichuanUniversity
Yang Min [email protected] West China hospital
Yang Min [email protected] Karolinska Institutet
Yao Zhongqiang [email protected] Peking University Third Hospital
Yeremenko Nataliya [email protected] Academic Medical Center
Yongkang Wu [email protected] WestChinaHospital SichuanUniversity
www.RAforum2017.com
Zamout Petros [email protected] Reumatologkliniken, USÖ
Zeng Pingling [email protected] Karolinska Institute
Zhan Feng [email protected] Hainan General Hospital
Zhang Jing [email protected] Sichuan Provincial People’s Hospita
Zhang Juan [email protected] Lanzhou University Second Hospital
Zhang Ning [email protected] Shengjing Hospital Of China Medical
Zhang Xuan [email protected] PEKING UNION MEDICAL COLLEGE HOSPITAL
Zhang Xuewu [email protected] PEKING UNIVERSITY PEOPLE’S HOSPITAL
Zhao Jinkang [email protected] XI‐Jing Hospital
Zheng Baolin [email protected] Foshan Hospital of traditional
Zheng Zhaohui [email protected] The Affiliated No.1 Hospital of ZZU
Zhong Jianghong [email protected] Karolinska Institutet
Zhou Diana [email protected] Karolinska Sjukhuset, dep. of Medicine
Zhou Hang [email protected] Beijing Friendship Hospital
Zhou Jiaxin [email protected] Peking Union MedicalCollegeHospital
Zhu Xiaochun [email protected] The First Affiliated Hospital
Zhuoli Zhang [email protected] Peking University First Hospital
Östberg Therese [email protected] Sanofi Genzyme

1. NEW PROTEIN ARRAY TECHNOLOGY IDENTIFIES RITUXIMAB TREATED NON RESPONDER RHEUMATOID ARTHRITIS PATIENTS ARE GENERATING A NEW AUTOANTIBODY REPERTOIRE
Z. Konthur1, M. Wiemkes 2, T. Häupl2, G. Burmester1, K. Skriner2,*
1Max Planck Institute , Max Planck Institute , 2Department of Rheumatology and Clinical Immunology, CHARITÉ UNIVERSITY MEDICINE, Berlin, Germany
Objectives: Rituximab (RTX) has shown clinical efficacy but up to 40 % of RTX treated rheumatoid arthritis (RA) patients are poor responders (Ann-Rheum-Dis. 2005 Feb;64(2):246-52) and the commonly used RA biomarkers (RF/ACPA) are poor predictors for therapy response. In this study the autoantibody repertoire analysed on protein macorarrays from RA patients under RTX treatment was correlated to clinical DAS28 response.
Methods: Screening of RA sera was conducted on 37.830 unique human proteins on protein marcoarrays (http://www.engine-gmbh.de) with sera taken before and 24 weeks after treatment. The autoantibody response of different immunoglobulin classes IgD, IgA, and IgG was recorded and bioinformatically evaluated. Response was determined according to DAS28 criteria. DAS 28 scores in the responder group before treatment was from 5.4 – 7.8 and in the non-responder group 5,6 – 6,8. We analyzed 26 RA patient sera (9 responder, 7 non-responder and 10 patients with blinded response classification) investigated the data of found autoantigens in-silico and by hierarchical clustering
Results: In the cohort of 26 patients 1292 different autoantigens (IgD,IgA,IgG) were detected. Using protein array we investigated clusters of autoantigen responses that disappeared or developed during RTX treatment of RA patients. RA autoantigenic patterns before and 6 month after RTX treatment were patient-specific and no relevant autoantigenic cluster was found that was shared between patients or associated with response. However, RTX reduced the repertoire of autoantibodies after 24 weeks of treatment in the tested RA patient cohort on average by 60%. RA patients which do not respond are generating on average 63% new autoantibodies. In good responders to RTX only 5,5% (+/-3%) new autoantibodies can be detected. The IgA and IgG autoantibody repertoire in the serum after 24 weeks of RTX treatment is reduced (IgA: 41%, IgG :31%) in good responders whereas it is increased (IgA: 1,3%, IgG: 24%) in non responders to RTX.
Conclusions: After 6 month of RTX treatment the autoantibody repertoire in all good responding RA patients is reduced and non responders to RTX change their autoantibody repertoire directed against new but patient specific antigens. The fast rebuilding of functional B cells is only detected in non-responders to rituximab
RA-associated antibodies targeting post translational modification have different osteoclastogenetic potential
Akilan Krishnamurthy1, Johanna Steen1, Caroline Grönwall1, Philip Titcombe1, Gustaf Wigerblad2, Camilla Svennson2, Heidi Wähämaa1, Vivianne Malmström1, Bence Rethi1 and Anca I Catrina1 1Rheumatology unit, Karolinska University Hospital, Karolinska Institute, Stockholm, Sweden, 2 Department of Physiology and Pharmacology, Karolinska Institute, Stockholm, Sweden Background:
Some but not all antibodies against citrullinated modified proteins (ACPA) promote osteoclastogenesis and bone destruction in vitro and in vivo. We aimed to investigate the ACPA specificity pattern that is related to this effect and if this effect is limited to ACPA or encompasses also other RA-associated antibodies.
Methods:
Polyclonal ACPA IgG and IgGs others than ACPA were obtained from the peripheral blood of RA patients by purification on a G column followed by an anti-CCP2 column. Monoclonal ACPA, anti-

MDA and rheumatoid factor (RF) IgGs were generated from either single plasma cells isolated from the synovial fluid or tetramer-positive sorted single B-cell isolated from the plasma of RA patients. Osteoclasts were generated from CD14+ monocytes of healthy individuals or bone marrow cells of Fc gamma III or Fc gamma chain knockout mice, in the presence or absence of polyclonal ACPA, monoclonal antibodies (ACPA, and anti-MDA antibodies and RF) and IgG controls. TRAP positive multinucleated cells were counted and bone erosion assay was done in parallel.
Results:
Polyclonal ACPA increased osteoclastogenesis, by a fold of 1.6±0.03One out of 4 tested plasma cell derived monoclonals ACPAs and one out of the five tested tetramer positive B-cell derived monoclonals have similar effects (with a fold increase of 1.63 ±0.15 for the plasma cell derived antibody and 1.4± 0.16 for the tetramer positive B-cell derived) have similar OC effects. Two additional tetramer positive B-cell derived monoclonals inhibited osteocalstogenesis while the remaining had no significant effect. All monoclonal ACPA were relatively highly cross-reactive to several citrullinated epitopes but not to native arginine peptides. Anti-MDA monoclonals antibodies displaying somatic hypermutations and low reactivity had significant in vitro functional properties and enhanced osteoclastogenesis (fold increase of for one antibody 4.0±0.76 and fold increase of for the second one 2.3±0.2), while the natural antibody related high-reactivity anti-MDA antibody did not. Anti MDA antibodies had no cross reactivity to other antigen modifications such as citrullination or carbamylation. Monoclonal RF had no direct effect on ostecoalstogenesis but were able to significantly increase ACPA-mediated osteoclastogenesis (fold increase of 1.68 ±0.03 for ACPA alone and for the combination of ACPA and RF 3.15±0.24). Dimeric Fab fragments of polyclonal ACPA increased OC numbers by a fold of 1.78, suggesting that epitope recognition is involved in the observed osteocalstogenetic effect of ACPA. Interestingly however while ACPA increased osteoclastogenesis from bone marrow precursors of wild type mice, it had no effect on the bone marrow precursors of the Fc gamma chain knockout and Fc gamma III mice bone marrow samples, implying a more complex mechanism than epitope recognition alone that involves Fc receptors.
Conclusion:
We demonstrate that RA-associated antibodies targeting different post translational modifications have the capacity to increase osteoclastogenesis while others have not. The mechanism is mediated through both Fc dependent and independent mechanisms.
2. BOB.1 INDUCES COSTIMULATORY CAPACITY OF B CELLS DURING T CELL-
DEPENDENT ACTIVATION
Levels M.J1,2,3, Fehres C.M1,2,3, Germar K1,2,3, van Uden N. O. P1,2,3, Blijdorp I.C.J1,2,3, Bakker A.Q4,
O'Toole T.G5, Spits H,4,6, Baeten D1,2,3, Yeremenko N.G1,2,3
1Academic Medical Center/University of Amsterdam, 2Agendia BV, Clinical Immunology and
Rheumatology, Academic Medical Center/University of Amsterdam, Amsterdam, Netherlands,
2Amsterdam Rheumatology and immunology Center, Amsterdam, Netherlands, 3Experimental
Immunology, Academic Medical Center/University of Amsterdam, Amsterdam, Netherlands, 4AIMM
Therapeutics, Amsterdam, Netherlands, 5 Department of Molecular Cell Biology and Immunology,
Vrije Universiteit Medical Center, Amsterdam, The Netherlands, 6Department of Cell Biology and
Histology, Academic Medical Centre/University of Amsterdam, Amsterdam, Netherlands
Background: B cells play an important pathogenic role in RA. Although it remains unclear what
molecular mechanisms guide or control pathogenic B cells during joint inflammation, the production

of autoantibodies and the presence of ectopic lymphoid structures in the RA synovium suggest that
local players in the synovial tissue may contribute to autoimmune tissue inflammation. Recently we
identified the transcriptional co-activator BOB.1 as specifically overexpressed in RA synovium, where
its levels strongly correlated with the presence of germinal centers (GCs). In accordance with human
data, mice lacking functional BOB.1 failed to mount GC response and were resistant to the
experimental model of RA. In this study we investigated whether increased levels of BOB.1 impact the
phenotype and function of B cells in a GC-like environment.
Methods: cDNA encoding BOB.1 was introduced into B cells isolated from peripheral blood or tonsils
by retrovirus-mediated gene transfer. The phenotype, activation, survival, proliferation and BCR
signaling were analyzed by FACS.
Results: Human B cells cultured with CD40L and IL-21 rapidly differentiate to antibody-producing
plasma cells, a process that is accompanied by decreased expression of CD20 and CD22 and an
increased expression of CD38 and CD27. In contrast, cells transduced with BOB.1 retained CD20 and
CD22 expression and were CD27intermediateCD38intermediate. Accordingly, the percentage of plasma cells
was significantly lower in BOB.1-overexpressing cells confirming that high levels of BOB.1 suppress
plasma cell differentiation. Further analysis revealed that BOB.1-transduced memory B cells showed
more rapid Ca2+ mobilization following BCR stimulation and expressed higher levels of CD40, CD80
and PD-L2 costimulatory receptors involved in B-T cell interactions and critical for the development of
T cell-mediated antibody responses. To address the role of BOB.1 on BCR-mediated antigen binding
and processing we made use of an influenza‐specific B cell clone capable of binding and internalizing
H1 antigen. Remarkably, overexpression of BOB.1 in these cells resulted not only in the elevated
expression of MHC class II, CD40 and CD86 molecules, but also in a faster binding of H1 antigen
suggesting that BOB.1 can control antigen presentation strength.
Conclusions: These data suggest that increased levels of BOB.1 in B cells during T cell-dependent
responses suppress plasma cell differentiation and impact BCR signaling strength, BCR-mediated
antigen processing and expression of costimulatory molecules. Whether it results in the broadening
and maturation of the autoimmune response and in survival of autoreactive B cells in RA joint is
currently under investigation.
3. High-throughput sequencing of auto-antigen specific antibodies in RA patients
Yan Wang, Katy Lloyd, Uta Hardt, Vivianne Malmström, Karin Lundberg, Lars Klareskog and Caroline Grönwall
Dept. of Medicine, Rheumatology Unit, Karolinska Institutet, Karolinska University Hospital, Stockholm, Sweden
The presence of autoantibodies is a hallmark for many autoimmune diseases, yet exactly how autoreactive B cells are first generated is still unclear. Single-cell sequencing techniques have been previously used to analyse ACPA-secreting B cells, however higher-throughput analysis is required to

explore how autoreactivities against citrullinated antigens first originate in ACPA seropositive RA. Next-generation sequencing enables a comprehensive view of the human B cell repertoire for the first time. The high error-rate of this technology limited its application for the accurate analysis of mutations within antibody repertoires, however this has recently been resolved by attaching molecular barcodes to individual mRNA. ACPA-positive B cells isolated from RA patients can be too many in number for single-cell sequencing techniques, but too few for currently described molecular barcoding methods. To overcome this issue, we have developed a method to generate cDNA library featuring molecular barcodes from a hundred to a few thousand B cells. The heavy chain and light chain antibody gene will be amplified from this molecular-barcoded library and will be sequenced using Illumina MiSeq sequencing. The sequencing results will allow us to analyse the isotype, mutation rate and antigen-selection of autoreactive B cells in an error-free manner, owing to the use of molecular barcodes. This high-throughput method is a powerful tool to study B cell repertoires, and we hope that analysing somatic hypermutations within the antibody variable genes will allow us to track the maturation of autoreactive B cells.
4. Number and type of ACPA fine specificities are correlated to High resolution computed tomography parenchymal lungs changes in patients with early untreated rheumatoid arthritis.
Vijay Joshua1, Aase Haj Hensvold1, Gudrun Reynisdottir1, Monika Hansson1, Martin Cornillet2, Leonor Nogueira2, Guy Serre2, Sven Nyren3, Reza Karimi4, Anders Eklund4, Carl Magnus Sköld4, Johan Grunewald4, Katerina Chatzidionysiou1* and Anca I. Catrina1*
1 Rheumatology Unit, Department of Medicine, Solna, Karolinska Institute, Karolinska University Hospital, Stockholm, Sweden
2 Unité Différenciation Épithéliale et Autoimmunité Rhumatoïde, Unité Mixte de Recherche 1056, INSERM – Université de Toulouse, Toulouse, France
3 Department of Radiology, Karolinska University Hospital, Stockholm, Sweden.
4 Division of Respiratory Medicine, Department of Medicine, Solna, Karolinska Institutet, Stockholm, Sweden
Background
Airways abnormalities that are consistent with inflammation are common in anti-CCP2 positive subjects without inflammatory arthritis. Anti-CCP2 antibodies are associated with HRCT parenchymal lung abnormalities in patients with early RA. This study aims to examine the association between ACPA fine specificities and HRCT lung changes in an early RA cohort and to asses these changes after 6 months.
Methods
Patients (n=106) with newly diagnosed RA according to the ACR 1987 criteria and naïve to treatment with oral glucocorticoids or DMARDs were included. HRCT was performed in order to assess the presence parenchymal (nodules, ground-glass opacities, opacities, fibrosis, emphysema) and airway abnormalities (bronchiectasis, air trapping, air wall thickening). EliA system (Phadia) was used to detect RF IgA and IgM, anti-CCP2 IgA and IgG, and peptide microarray (Phadia) was used to detect antibodies against 10 citrullinated (Cit) peptidic antigens: CCP-1 (Filaggrin), CEP-1 (α-enolase), Vim 2-17, Vim 60-75 (Vimentin), Fib α 36-50, Fib α 573, Fib α 591, Fib α 621-635, Fib β 36-52, Fib β 60-74 (Fibrinogen). Most of the patients (n=93) were followed up after 6 months. Logistic regression analysis

was performed to examine associations between HRCT lung changes at the time of RA diagnosis and autoantibodies.
Results
HRCT parenchymal and airway changes was present in 58 (54.7%) and 68 (64.2%) patients, respectively. The forced vital capacity (FVC) was significantly lower in the presence of airway abnormalities, while the ratio FEV1/FVC was significantly lower in patients with parenchymal lung changes. Higher age, RF IgA, CCP2 IgG, ever smoking and pack-years above 24 were significant predictors of parenchymal lung changes. Some ACPA fine specificities, especially against Cit Fib and Vim peptides, were associated to parenchymal lung changes in ever smokers. The risk of having parenchymal changes increased parallel to the increase in number of ACPA specificities. Having more than 5 ACPA specificities at the time of diagnosis increased the risk of having parenchymal lung abnormalities in current smokers (OR=13.8, 95% CI=1.0-196.2, p=0.05). Of the patients that were followed up after 6 months 4 had progression of fibrosis and 3 had new fibrosis. No difference in airway changes were observed at follow-up. There was a significant decrease in DAS28 at follow-up (Mean±SD: 5.5 ± 1.1 vs 3.2±1.3 P value < 0.001). The titers of some but not all of the ACPA fine specificity was significantly decreased after 6 months of treatment CCP-1 (Mean±SD 46.6±289.7 vs 101.6±235.3), CEP-1 (59.1±120.1 vs 35.9±76.3), Vim 60-75 (338±488.1 vs 220.3±327.2), Vim 2-17 (25.7±59.3 vs 17±37.8), Fib β 60-74 (237.3±411 vs 136.4±241.5), Fib α 621-635 (187.3±306.3 vs 115.9±203.2).
Conclusions:
The presence of RF IgA, anti-CCP2 IgG and antibodies to Cit Fib and Vim peptides were associated with parenchymal lung changes in early-untreated RA. The more ACPA fine specificities, the higher the risk of having parenchymal lung changes already at the time of RA diagnosis. Treatment with DMARDs significantly reduces the disease activity and titers of some of the ACPA fine specificities.
5. Season of Birth and Cigarette Smoking as Modifiers of the Effect of HLA DRB1 Shared
Epitope on the Development of ACPA Positive RA. Results from a Swedish Population
Based Case-Control Study.
Patrik Stolt¹, Lars Klareskog², Leonid Padyukov², Camilla Bengtsson¹, Lars Alfredsson¹
1: Institute of Environmental Medicine, Unit of Cardiovascular Epidemiology, Karolinska Institutet,
171 77 Stockholm, Sweden. 2: Department of Medicine, Rheumatology Unit, Center for Molecular
Medicine, Karolinska University Hospital Solna, 171 76 Stockholm, Sweden
Abstract
Background: Shared epitope (SE) alleles, cigarette smoking and antibodies to citrullinated peptide
antigens (ACPA) are well recognized components in the development of Rheumatoid Arthritis (RA) (1).
More recently, the effect of early life exposures on this process has become a topic of interest (2). The
objective of this study was to analyse the combined effect of season of birth, used as a marker of
prenatal to early childhood exposures, SE alleles and cigarette smoking on the development of RA of
different ACPA phenotype.

Method: In a Swedish study of RA, 1726 cases and 3683 controls included October 2005 – September
2014 were investigated by analysing the effect of different combinations of season of birth, SE
genotype and cigarette smoking status on the risk of RA of different ACPA phenotype. The analyses
were based on comparisons of single SE (SSE) carriers and double SE (DSE) carriers with SE-non
carriers, of ever-smokers with never-smokers and of persons having different season of birth. Risk was
estimated by calculating odds ratio (OR) with 95% confidence interval (95% CI).
Results: Comparing persons having different month of birth, a tendency towards a comparably lower
risk of ACPA positive RA among persons born in July was observed, however inconclusively due to
wide and overlapping CI:s. Adding SE genotype as explanatory variable by analysing the variation of
the effect of carrying DSE, compared with not carrying SE, over different seasons of birth, a lower risk
estimate of ACPA positive RA was observed among persons born in the period of June – August than
among persons born in the other quarters of the year. Repeating these analyses among the ever-
smokers separately, a clearly lower risk estimate of ACPA positive RA was observed among persons
born in the period of June-August, the OR = 2.81, 95% CI 1.16-6.77, than among persons born at any
time of the year except June – August, the OR = 21.02, 95% CI 11.00-40.15, or at any time of the year,
OR = 11.44, 95% CI 6.96-18.82. An analogous variation was not observed among the never-smokers,
the corresponding OR being 7.12, 95% CI 2.33-21.76, 7.62, 95% CI 4.10-14.17 and 7.54, 95% CI 4.39-
12.96, respectively. The corresponding analyses in which SSE replaced DSE remained inconclusive due
to overlapping CI:s.
Conclusion: These results indicate that the effect of SE on the development of ACPA positive RA may
be modified by season of birth when combined with cigarette smoking in adulthood. This is suggestive
of some seasonal factor in the prenatal to early childhood period modifying the risk of developing RA
by interacting with gene polymorphisms and exposures later in life.
References:
1. Klareskog L et al. A new model for an etiology of rheumatoid arthritis: smoking may trigger
HLA-DR (shared epitope)-restricted immune reactions to autoantigens modified by
citrullination. Arthritis Rheum. 2006;54:38-46.
2. Disanto G et al. Month of birth, vitamin D and risk of immune- mediated disease: a case
control study. BMC Medicine 2012;10:69.
6. Cloning of Gingival Tissue B Cells From an ACPA+ RA Patient with Periodontitis
Natalia Sherina1, Khaled Amara1, Natalie Sippl1, Daniel Ramsköld1, Johanna Steen1, Lena Israelsson1, Monika Hansson1, Annika van Vollenhoven1, Kaja Eriksson2, Tulay Yucel-Lindberg2, Vivianne Malmström1, Karin Lundberg1
1. Rheumatology Unit, Department of Medicine, Karolinska University Hospital, Karolinska Institutet, Solna, Stockholm, Sweden

2. Division of Periodontology, Department of Dental Medicine, Karolinska Institutet, Huddinge, Sweden
Background and objectives
Rheumatoid arthritis (RA) is characterized by autoantibodies to citrullinated proteins (ACPA). Recently Porphyromonas gingivalis, a major cause of periodontitis (PD), has been linked to ACPA+ RA. Our ambition with this study is to clone ACPA-specific B cells from gingival tissue (GT) of patients suffering from both PD and RA, in order to demonstrate that citrulline-specific B cells, previously only detected in RA joints and circulation, may also reside in gingival tissue.
Materials and Methods
Gingival tissue-derived single CD19+ B cells from an ACPA+ RA patient with PD (RA/GT) were sorted by flow cytometry. Immunoglobulin (Ig) variable region genes were sequenced and expressed to generate recombinant monoclonal antibodies (mAbs).
Results
We have isolated 480 CD19+ B cells from the gingival tissue, and analyzed 110 variable heavy chain Ig genes (IGHV). Ig gene sequence analysis demonstrated that the B cell repertoire was predominantly polyclonal, although two clonally related B cell populations (approximately 2%) were detected. Compared to B cells from peripheral blood of healthy controls, RA/GT B cells showed decrease in usage of VH3 and increase in VH4. By individual VH gene segments, IGHV4–31 was overrepresented compared to controls. Conversely, IGHV1-2, IGHV3-23, and IGHV4-34 were under-represented. Interestingly, antibodies with positively charged IGHV CDR3 regions, a feature associated with autoreactivity, were enriched in GT. By contrast, antibodies with negatively charged CDR3 regions were enriched in controls. Alignment of VH sequences to their closest germline counterparts revealed that RA/GT B cells exhibited extensive mutations in the IGH CDR regions and higher levels of somatic mutations in the V gene segments compared to controls, suggesting an antigen-driven B cell response. We have so far expressed 60 mAbs that we are currently screening for reactivity with citrullinated epitopes and bacterial antigens.
Conclusions
We have been able to successfully isolate and clone a number of gingival tissue-derived B cells. Based on the hypothesis that the ACPA-response may be initiated at mucosal surfaces such as gingival tissue, we now have the tools available to more directly address this etiological question.
7. A novel candidate for genetic control of Collagen Induced Arthritis is involved in transcriptional regulation of B-cell proliferation Samra Sardara, Alish Kerra,b, Daniëlle Vaartjesa,c, Mathilde Emilie Voetmanna,d, Emilie Riis Moltveda,e,
Åsa Anderssona,f
a Section for Molecular and Cellular Pharmacology, Department of Drug Design and Pharmacology,
University of Copenhagen, Copenhagen, Denmark
b Present address: Pfizer pharmaceuticals, Dublin, Ireland
c Present address: Division of Medical Inflammation Research, Department of Medical Biochemistry
and Biophysics, Karolinska Institutet, Stockholm, Sweden
d Present address: Biogen Denmark A/S, Hillerød, Denmark
e Present address: QuintilesIMS, North Carolina, United States of America
f School of Business, Engineering, and Science, Halmstad University, Halmstad, Sweden
Introduction: Rheumatoid Arthritis (RA) is a common autoimmune disease, caused by a complex
interplay of genetic and environmental factors. This project aims to investigate the role for the
transcriptional regulator TBX3 in the development of experimental arthritis. TBX3 was identified in
functional genetic studies of Collagen Induced Arthritis (CIA), an experimental model for RA.
Methods: CIA is induced in mice by immunization with collagen type II. The studies were performed
in mice congenic for a 1.4 Mbp genetic fragment on mouse chromosome 5 (Eae39r2). The whole
genomes of the parental mouse strains were sequenced by NGS. Congenic and control mice were
characterized by flow cytometry, in vitro lymphocyte activation assays, and transcript level studies in
order to identify the candidate gene. A time-course CIA experiment was performed to study protein
expression kinetics in relation to arthritis. CRISPR/Cas9 knock-out of the candidate gene in murine B
lymphocytes is currently underway.
Results: CIA experiments in Eae39r congenic, sub-congenic, and control mice have shown that a 1.4
Mbp sub-locus, within the Eae39r fragment, is controlling the severity of arthritis, in addition to anti-
collagen antibody titers. Within this sub-locus, a candidate gene, Tbx3, has been identified based on
its: (-) differential expression in the spleens and specifically in B cells of naïve congenic and control
mice; (-) various regulatory variations identified by NGS; (-) genetic conservation between mouse and
human; (-) a documented role in bone signaling pathways. In vitro lymphocyte activation and protein
activity experiments have demonstrated that the activity of TBX3 decreases in primary B-lymphocytes
upon stimulation through the B cell receptor. The protein activity also varies in B-lymphocytes at
different stages of CIA, hinting towards the importance in disease pathogenesis/progression.

Conclusion: We suggest that TBX3 is a novel candidate contributing to arthritis development by
controlling B lymphocyte activation. Studies of associated pathways will provide new insights into
disease pathogenesis and potential drug targets.
8. Identifying novel drug targets of inflammation by customized CRISPR/Cas9 approach
Authors: Sudeepta Kumar Panda, Zsolt Kasza, Sanjaykumar Boddul, Yanek Jiménez, Gustaf
Wigerblad, Long Jiang and Fredrik Wermeling
Affiliations: SKP, ZK, SB, YJ, GW, LJ, FW: Rheumatology Unit, Department of Medicine Solna,
Karolinska Institutet, Stockholm, Sweden.
Background: - Inflammation is a protective body response towards foreign invaders and ultimately
helps to restore body homeostasis. However, excessive and misdirected inflammation can result in
allergy and autoimmune disorders. Therefore, there is a huge demand to discover potent anti-
inflammatory drugs. In the clinic, high dose intravenous immunoglobulin (IVIG) administration is
used in severe inflammatory diseases such as Idiopathic thrombocytopenic purpura, and Kawasaki
disease, but also occasionally in Myositis and Rheumatoid Arthritis. On note, effectiveness of IVIG
depends on the minute expression of the IL-4Rα in myeloid effector cells. Interestingly, mice injected
with any inflammatory stimuli results in myeloid IL-4Rα expression, mediated by a soluble proteinase-
k sensitive factor that is secreted from bone marrow-derived cells found in fat pads and lung
(Wermeling et al., PNAS 2013). That we have referred to as the IL-4Rα regulating factor (IRF). In
general, neutrophils have low IL-4Rα expression, whereas during inflammation there is a massive
upregulation of this receptor, which has been a great paradox for us.
Aim: - Here we aim to investigate this soluble factor, possibly a novel biomarker of inflammation, in
myeloid cells using a CRISPR/Cas9 screening approach.
Methods and Results: - First, we established an in vitro model system in which in which
supernatant from LPS challenged mouse alveolar macrophages (MH-S) and conditional Hoxb8
macrophage cell line selectively upregulated IL-4Rα expression in bone marrow-derived neutrophils.
Secondly, different MH-S clones (good and poor IRF producers) were challenged by LPS and gene
expression was determined by microarray. Thirty-four different candidate genes for the IRF were
identified comparing the good and poor IRF producers with control. Among 34 candidates list, seven
top most genes that are highly upregulated IL-4Rα expression in good clones were used in the CRISPR
screen purpose. To simplify the generation of such custom CRISPR screens we have furthermore
developed a software called Green Listed (Panda et al., Bioinformatics 2016). Thirdly, we established a
stable Cas9 expressing Hoxb8 macrophage cell line (Hoxb8 macrophageCas9) that serve as a host for a
lenti viral guide RNA library. This Hoxb8 macrophageCas9 cells were infected with the lenti viral library
at a very low MOI (MOI < 0.03) to integrate one guide RNA per one cell. To this, we established 132
different single cell clones. Consecutively, we repeated the in vitro bone marrow assay in neutrophils
by priming the supernatant of these LPS challenged clones.

Conclusion: We are currently screening these clones to identify the gene, as an IL-4Rα regulating
factor (IRF), responsible for the myeloid IL-4Rα expression. This study will delineate the novel
regulatory pathways that targets STAT6 signaling to myeloid cells that could have implications for
several inflammatory and autoimmune diseases.
9. Machine learning using rheumiatoid arthritis synovial gene expression data defines
histologic features that correlate with systemic inflammation and autoantibodies
Dana Orange
Rockefeller University
Objective: We sought to refine histologic scoring of rheumatoid arthritis synovial tissue by training
scoring metrics with transcriptome-wide expression data and machine learning.
Methods: Twenty histologic features were assessed on 140 synovial tissue samples. Consensus
clustering of gene expression data from a subset of 45 synovial samples identified three unbiased and
robust subtypes. Support vector machine (SVM) learning was then used to predict gene expression
subtypes using histology data as the descriptive features. Corresponding clinical and laboratory data
were compared across subtypes.
Results: Consensus clustering of RNA-seq data revealed three distinct synovial subtypes of RA,
including [i] a highly inflammatory subtype characterized by extensive infiltration of leukocytes, [ii] a
low-inflammatory, or fibroid subtype characterized by enrichment in pathways including TGF-β,
neuronal genes and mucin deposition, and [iii] a mixed subtype. Patients with highly inflammatory
synovial subtypes exhibited higher levels of markers of systemic inflammation and autoantibodies, but
not increased joint counts or pain relative to other subtypes. Though CRP and ESR correlated with
pain in the highly inflammatory patients, there was no evident relationship for the fibroid samples.
Machine learning algorithms applied to histology features using RNA-seq subtypes as data labels
yielded good predictive scores, particularly for the high and low inflammatory subtypes, revealing good
synchrony between RNA-seq data and the histology features selected for this study.
Conclusion: Careful analysis of RNAseq data revealed three distinct synovial subtypes that associate
with levels of ESR, CRP and autoantibodies, and a learning algorithm using histology scores and
subtype labels distinguished the subtypes successfully. Comparison of gene expression patterns to
clinical features revealed a potentially clinically important distinction: mechanisms of pain may differ
in patients with high ESR and a synovial inflammatory expression pattern from those with low ESR
and a fibroid synovial expression pattern.
10. NEW MUTATED PEPTIDYLARGININE DEIMINASE FROM PORPHYROMONAS GINGIVALIS A TARGET IN EARLY RA CITRULLINATES MAJOR RA-AUTOANTIGENS
M. Jenning1, B. Marklein1, J. Yetterberg2, G. Burmester1, K. Skriner1,*
1Department of Rheumatology and Clinical Immunology, CHARITÉ UNIVERSITY MEDICINE, Berlin, 2Department of Rheumatology and Clinical Immunology, Karolinska Institutet, Stockholm, Germany
Objectives: Previous reports showed that peptidylarginine deiminase (PPAD) form Porphyromonas gingivalis (P.g.) is not able to citrullinate proteins internaly. New mutated PPAD (mPPAD) from P.g. involved in periodontal disease (PD) cloned out of P.g. strain was characterized and analyzed for its reactivity in sera from patients with systemic autoimmune diseases
Methods: We cloned a new enzymatically active recombinant mutated PPAD from P.g. mPPAD mutations and citrullination sites were analyzed by DNA sequencing and/or protein mass spectrometry. Autocitrullination activity it´s enzymatic-activity and human autoantigen protein citrullination was investigated by 2D-Elektrophoresis, MS, immunoblot analysis and ELISA. Furthermore we tested anti-mPPAD/cit-mPPAD with human sera (n=93) from early RA before and after onset of RA (n=30), established RA (n=32), SLE (n=16) and healthy blood donors (n=15) in ELISA assays. To study a potential impact on the RA mouse model (CAIA), mPPAD-containing vesicles from P.g. were injected by intraperitoneal injection (IP).
Results: Recombinant mPPAD lacks 43 amino acids at the N-terminus and exhibits so far two new amino acid mutations (amino acid position 73 (F>L) and 447 (E>V). We were able to demonstrate, mPPAD is enzymatically active over a huge pH-range (3-10) and autocitrullinates at amino acid position 63 the arginine to citrulline. Moreover mPPAd citrullinates major autoantigens in RA (Fibrinogen, Vimentin and hnRNP-A2/B1) which are detectable by RA patient sera and specific anti-citrulline monoclonal antibodies. mPPAD citrullinates HeLa-protein extracts and these specific citrullinated proteins are recognized by RA patient sera. Anti-citrullinated mPPAD antibodies were detected in 41% (n=32) of patients with RA but not in SLE (n=16) and control sera (n=15). In a RA follow-up study (n=30), we detected nearly similar antibody-sensitivities for citrullinated mPPAD before and after onset of RA (13/20%). Only a minority (7%) of RA patients show higher mPPAD antibody levels after RA diagnosis. In the Collagen antibody-induced arthritis (CAIA) RA mouse model mPPAD containing P.g. vesicles when injected IP showed a TLR2-dependent protective anti- inflammatory effect like P.g. LPS and Lipomannan.
Conclusions: Pg. infection and RA disease diagnosis occurs on different timepoints and Pg. infection induces a TLR2-dependent protective anti-inflammatory effect.We show the first time that mPPAD can citrullinate major human autoantigens internally and their immunologically and diagnostic relevance.
11. A long non-coding RNA in the rheumatoid arthritis risk locus at chromosome 18 is involved in T cell activities M. Houtman, K. Shchetynsky, L. Padyukov. Rheumatology Unit, Department of Medicine Solna, Karolinska Institute and Karolinska University Hospital, Stockholm, Sweden. Rheumatoid arthritis (RA) is a relatively common autoimmune disorder that is characterized by joint inflammation and destruction. Genome-wide association studies have enabled the discovery of common genetic variations in over 100 loci contributing to RA, but the precise targets of the majority of these associations are unknown. We aimed to identify the molecular mechanisms that connect variations in the protein tyrosine phosphatase non-receptor type 2 (PTPN2) locus with RA. We have found that previously identified RA-susceptibility variants in the PTPN2 locus are associated with the expression of a long non-coding RNA LINC01882 located 30kb downstream of PTPN2 (whole blood, GTEx). To identify the function of this long non-coding RNA, we suppressed the expression of LINC01882 using antisense oligonucleotides and RNA interference in Jurkat T cells. Twenty-four and 48 hours after knockdown, total RNA was extracted and ribosomal RNA was depleted. Sequencing libraries were generated using the Illumina TruSeq Stranded Total RNA kit and sequenced on an Illumina HiSeq 2500 platform, yielding about 25 million paired-end reads per sample. Differential expression analyses were conducted using DESeq2. We identified 12 deregulated genes after LINC01882 knockdown (6 upregulated and 6 downregulated; FDR < 0.05). One of the downregulated genes is the zinc finger E-box-binding protein 1 (ZEB1), a repressor of interleukin-2 (IL-2) gene transcription. This points towards the involvement of LINC01882 in T cell differentiation. Our data suggest that LINC01882 might contribute to the molecular mechanism underlying RA. Overall, these findings suggest that previous annotation of the associated locus to PTPN2 is potentially incorrect and that the long non-coding RNA LINC01882 might be the causal gene. Overall, these findings point towards the potential role of LINC01882 in the RA susceptibility association attributed to the PTPN2 locus.

12. Elevated serum IL-25 in rheumatoid arthritis patients with bone erosion and
interstitial lung disease
LU Jinyue1,DA Minglian1,FENG Yuchen1, LIU Yuanyuan2,ZHANG Sigong2,SHEN Haili*
1Second Clinical Medical College, Lanzhou University ,Lanzhou 730000;2Department of
Rheumatology, Lanzhou University Second hospital, Lanzhou 730000,China
*Corresponding author, E-mail:[email protected]
Objective To detect the serum levels of IL-25 and IL-17 in rheumatoid arthritis (RA) patients and
investigate the potential relationship with bone erosion and concomitant interstitial lung disease
(ILD). Methods The study enrolled a total of 117 RA patients and 56 healthy subjects as control. The
serum levels of IL-25 and IL-17 were determined by ELISA, and RF was detected by turbidimetric
immunoassay, anti-CCP antibody as well as erythrocyte sedimentation rate (ESR) and C-reactive
protein (CRP)were also tested. ILD was identified on high-resolution computed tomography (HR-CT),
the degree of bone erosion was inspected by musculoskeletal ultrasoum examination, and radiographic
grade was graded by Sharp-van der Heijde Score (SHS), Disease activity in RA was scored with the
DAS28 and visual analogue scale(VAS). correlation analysis was used to evaluate the correlations of
IL-25 and IL-17 in different groups. Results Compared with heathy control group, the serum levels
of IL-25 and IL-17 were increased significantly in patients with RA(graph A,B). Compared with bone
erosion negative group, the serum level of IL-25 was higher significantly in bone erosion group(graph
C,D). The level of IL-25 was higher in the ILD group of RA patients than the non-ILD group(graph
E,F). In addition, there were positive correlation between the serum level of IL-25 and RF-
IgG(r=0.367), RF-IgA(r=0.319), RF-IgM(r=0.436)( graph G). Meanwhile, the serum level of IL-17 had
the positive correlation with RF-IgG(r=0.216), RF-IgM(r=0.271) . both of them have no correlation
with anti-CCP antibody. Conclusion The serum level of IL-25 is raised in RA patients with bone
erosion and ILD.
[Key words] rheumatoid arthtitis;cytokines;bone erosion;intersititial lung disease ;inflammatory
13. ALTERED LYMPH NODE STROMAL CELLS DURING THE EARLIEST PHASES OF RHEUMATOID ARTHRITIS
C. Ospelt1, E. Karouzakis1, J. Hähnlein2, J.F. Semmelink2, R.E. Gay1, P.P. Tak2, 3, D.M. Gerlag2, 4, S. Gay1, L.G.M. van Baarsen2
1Center of Experimental Rheumatology, University Hospital of Zurich, Zurich, Switzerland, 2Academic Medical Center, Amsterdam, Netherlands, 3Cambridge and GlaxoSmithKline, University of Cambridge, Stevenage, 4R&D Projects Clinical Platforms & Sciences, GSK Clinical Unit Cambridge, Cambridge, United Kingdom
Background: Rheumatoid arthritis (RA) is an autoimmune disease with unknown etiopathogenesis where systemic autoimmunity precedes clinical disease onset. Adaptive immunity is initiated in lymphoid tissue where lymph node stromal cells (LNSC) play a crucial role in shaping the immune response and maintaining peripheral tolerance. We developed an experimental model for studying the functional capacities of human LNSC during the earliest phases of RA and compared their cellular and molecular characteristics to LNSC from healthy volunteers.
Methods: ACPA+ RA patients (n=24), ACPA+ RA-risk individuals (n=23) and seronegative healthy controls (n=14;HC) underwent ultrasound-guided inguinal lymph node biopsy. Human LNSCs were isolated and expanded in vitro for cellular (flow cytometry), molecular (methylome, transcriptome and microRNA) and functional analyses.
Results: Key LN chemokines CCL19, CCL21 and CXCL13 were induced in LNSCs upon stimulation with TNFα and lymphotoxin α1β2, but to a lesser extent in LNSCs from RA patients. RNA sequencing was performed on LNSC of HC (n=5), ACPA+ RA-risk individuals (n=6) and ACPA+ RA patients (n=4). Of interest, LNSC from ACPA+ RA-risk individuals and ACPA+ RA patients revealed a common significantly differential expressed gene signature compared with HC LNSC. Pathway analysis of this common signature showed, among others, significant enrichment of pathways affecting actin cytoskeleton, focal adhesion and cell junction. Accordingly, in a gel contraction assay LNSC from ACPA+ RA-risk individuals and RA patients showed impaired collagen contraction compared to healthy LNSC. In RA LNSC a significant enrichment was observed for genes involved in TGFb signalling while in RA-risk LNSC cell cycle genes were differentially expressed compared with HC. DNA methylation analyses revealed common differentially methylated CpG sites (DMS) in LNSC from ACPA+ RA patients (n=5) and ACPA+ RA-risk individuals (n=3) compared with HC (n=4). These DMS were significantly hypomethylated and associated with antigen processing and presentation (HLA-DRB1).
Conclusions: This data point towards alterations in the cytoskeleton and antigen-processing and presentation in LNSC from ACPA+ RA-risk individuals and RA patients. Further studies are required to investigate the influence of this LNSC abnormality on immune responses.
14. Receptor activator of nuclear factor kappa-B ligand (RANKL) and
Marginal jawbone loss predates the onset of rheumatoid arthritis.
Johansson L3, Kindstedt E1, Palmqvist P1, Koskinen-Holm C1, Kokkonen H3, Johansson I2, Rantapää
Dahlqvist S3*, Lundberg P1*
INTRODUCTION: Previous studies have shown a higher incidence of alveolar bone loss in patients with rheumatoid arthritis (RA) and that patients with periodontitis are at a greater risk for developing RA. Periodontitis, displayed as marginal jawbone loss was analysed in individuals prior to symptom onset of RA and related to plasma levels of receptor activator of nuclear factor kappa-B (RANKL), a cytokine crucial for bone resorption.
METHODS: A case-control study performed within the Medical Biobank of Northern Sweden included 232 pre-symptomatic individuals with blood samples donated before symptom onset and 194 controls. A questionnaire on self-assed dental status and smoking status was retrieved. Dental radiographs to evaluate marginal jawbone levels were available from 93 pre-symptomatic individuals (mean age; 56.8 95%CI55.9, 57.7 years and pre-dating time; -5.3 95%CI -12.2, -0.2, 74.2% females) and 83 controls (mean age; 55.5 95%CI54.6, 56.5, 73.5% females) . Of these individuals 45 had radiograph documentations prior to development of RA symptoms and to whom sex, age and smoking status could be matched among the controls. Plasma were analysed for RANKL (BioVendor, Karasek, Czech Republic), and anti-citrullinated peptide antibodies (ACPA) (anti-CCP2 test, Eurodiagnostics, Sweden) from similar time points.
RESULTS: Compared to matched controls, total bone loss was significantly higher in never-smokers who developed RA but not in smokers and increasing levels on total jawbone loss was associated with a significantly higher odds to be diagnosed with RA later (OR=1.06, 95%CI 1.01, 1.11). Regardless of smoking status, the number of unaffected teeth did not differ significantly between those who were subsequently diagnosed with RA and their matched controls. In the pre-symptomatic individuals RANKL positive individuals had significantly higher extent of marginal jawbone loss, which was further increased in ACPA positive individuals. Previously documented association between smoking and ageing and marginal jawbone loss was verified.
CONCLUSIONS: Marginal jawbone loss preceded onset of symptoms of RA but the difference was only manifested in non-smokers. Moreover, marginal jawbone loss and plasma RANKL levels were related in the pre-symptomatic individuals particularly in ACPA positive individuals.
15. The association between HLA-DRB1 alleles and risk of rheumatoid arthritis is
influenced by massive gene-gene interactions.
Lina-Marcela Diaz-Gallo,1* Daniel Ramsköld,1,7 Lasse Folkersen,2,7 Klementy Shchetynsky,1,7 Karine
Chemin,1 Boel Brynedal,3 Steffen Uebe,4 Yukinori Okada,5,6 Lars Alfredsson,3 Lars Klareskog,1 Leonid
Padyukov1**
1. Rheumatology Unit, Department of Medicine Solna, Karolinska Institutet, Karolinska
University Hospital, Stockholm, 171 76 Sweden.
2. Department of Bioinformatics, Technical University of Denmark, DK-2800 Lyngby,
Denmark
3. Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden.
4. Human Genetics Institute, Universitätsklinikum Erlangen, Erlangren, Germany.
5. Division of Rheumatology, Immunology, and Allergy, Brigham and Women’s Hospital.
Harvard Medical School, Boston, Massachusetts, USA.
6. Laboratory of Statistical Immunology, Immunology Frontier Research Center (WPI-
IFReC), Osaka University, Suita, Japan.
Correspondence: * [email protected], @LinMarDiaz ** [email protected]
In rheumatoid arthritis (RA) a particular subset of HLA-DRB1 gene variants provide a higher risk
factor. A common way of describing these subsets has been by naming them the “shared epitope (SE)”
refereeing to amino acid sequences known to be coded by the susceptibility gene variants. Here, we
aimed to investigate how gene-gene interactions influence this major HLA-DRB1 related disease risk
and more specifically we set out to investigate whether a large number of non-HLA SNPs with
individually low risk to develop RA modulate the HLA-DRB1 effect to develop RA.
In order to address this question, we measured additive interaction at GWAS level for two independent
RA cohorts, the Swedish EIRA and the North American NARAC. We computed the attributable
proportion (AP) due to interaction between HLA-DRB1 SE and a set of SNPs associated with disease or
not-associated with disease in these cohorts (in total more than 5 million SNPs). The distributions of
the observed AP p-values were compared by the Kolmogorov-Smirnov test. We found a strong
enrichment of significant interactions (AP p-value <0.05) between HLA-DRB1 SE alleles and a group
of SNPs associated with RA in both cohorts, evidenced by the distribution test (KS-test D=0.35 for
EIRA and D=0.25 for NARAC, p<2.2e-16 for both).
Our data indicate that the strong association between HLA-DRB1 SE alleles and risk of anti-
citrullinated protein antibody (ACPA) positive RA is modulated in a major way by massive interactions
with non-HLA genetic variants.
16. Characterisation of the antibody response to a citrullinated peptide derived from Porphyromonas gingivalis PAD in RA Nastya Kharlamova1, Boel Brynedal2, Xia Jiang2, Natalia Sherina1, Kaja Eriksson3, Tulay Lindberg3, Monika Hansson1, Lena Israelsson1, Johanna Steen1, Vivianne Malmström1, Lars Alfredsson2, Khaled Amara1, Karin Lundberg1
1 Rheumatology Unit, Department of Medicine Solna, Karolinska Institutet, Stockholm, Sweden 2 Cardiovascular Epidemiology, Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden 3 Division of Periodontology, Department of Dental Medicine, Karolinska Institutet, Stockholm, Sweden
Objectives: Anti-citrullinated protein antibodies (ACPA) - a hallmark of rheumatoid arthritis - can be detected years before clinical signs of joint inflammation. Since citrullination and expression of peptidyl arginine deiminase (PAD) (i.e. the enzyme responsible for citrullination) is an inflammation-dependent process, and generally not present in healthy joints, it has been suggested that break of immune tolerance to citrullinated proteins occurs at an extra-articular site. The possible involvement of the gum mucosa has been discussed, primarily based on the unique feature of Porphyromonas gingivalis (P.g) - a keystone pathogen in periodontitis (PD) - to express a bacterial version of the PAD enzyme (denoted P.PAD), capable of autocitrullination. In the present study, we have investigated the antibody response against CPP3, a citrullinated peptide derived from P.PAD, in order to address the hypothesis that P.g may drive ACPA-production. Methods: This study includes: 2,859 RA cases and 4,864 controls from the Epidemiological Investigation of RA (EIRA) cohort; 65 PD patients and 59 periodontally healthy individuals; and 218 monoclonal antibodies, derived from RA B cells. Reactivity with citrullinated P.g and human antigens was assayed by ELISA and/or multiplex. Associations with genetic risk factors and smoking were determined by logistic regression. ACPA co-occurrence was analysed by pairwise Pearson correlation. Monoclonal antibody mutations were analysed by IgBLAST comparison. Results: Anti-CPP3 IgG was detected in 11% of RA, 10% of PD and <2% of controls, with higher levels in RA compared to PD. These antibodies clustered outside the classical ACPA response, associated with smoking, but not with major genetic risk factors. Two CPP3-reactive monoclonal antibodies were identified; one which cross-reacted with citrullinated human vimentin and had extensive mutations, indicating antigen-driven clonal selection and affinity maturation. Conclusion: Based on our data, we propose that P.g infection triggers an antibody response to CPP3, which cross-reacts with citrullinated human proteins by mechanisms of molecular mimicry. Future studies should address whether anti-CPP3 IgG could serve as a biomarker to identify individuals with PD at increased risk for RA.
17. PTPN22 - novel gene to function data for T cells in Rheumatoid Arthritis
Karine Chemin1, Daniel Ramsköld1, Lina-Marcela Diaz-Gallo1, Jessica Herrath1, Karolina Tandre2, Lars Rönnblom2, Anca Catrina1, Vivianne Malmström1
The presence of the PTPN22 risk allele (1858T) is associated with several autoimmune diseases including rheumatoid arthritis (RA). Despite a number of studies exploring the function of PTPN22 in T cells, the exact impact of the PTPN22 risk allele on T-cell function in humans is still unclear. In this study, using RNA sequencing, we show that, upon TCR-activation, naïve CD4+ T cells homozygous for the PTPN22 risk allele overexpress a limited number of genes including CFLAR and 4-1BB, which are important for cytotoxic T-cell differentiation. Moreover, the protein expression of the T-box transcription factor Eomesodermin (EOMES) was increased in T cells from healthy donors homozygous for the PTPN22 risk allele. No difference in the frequency of other CD4+ T cell subsets (Th1, Th17, Tfh, Treg) was observed in healthy donors homozygous for the PTPN22 risk allele and suppressive capacity of Treg cells was not altered. Finally, an accumulation of EOMES+CD4+ T cells was observed in synovial fluid of RA patients with a more pronounced production of Perforin-1 in PTPN22 risk allele carriers. Altogether, we propose a novel mechanism of action of PTPN22 risk allele through the generation of cytotoxic CD4+ T cells and identify EOMES+ CD4+ T cells as a relevant T-cell subset in RA pathogenesis.
1Rheumatology Unit, Department of Medicine, Karolinska University Hospital Solna, Karolinska Institute, Stockholm, Sweden

2Department of Medical Sciences, Rheumatology, Science for Life Laboratory, Uppsala University, Uppsala, Sweden
18. Monoclonal ACPA-IgG feature extensive Fab glycosylation
Katy A Lloyd1, Johanna Steen1, Phillip J Titcombe1,2, Khaled Amara1, Diana Zhou1, Lena Israelsson1, Susanna L Lundström1,3, Daniel L Mueller2,4, Lars Klareskog1, Vivianne Malmström1, Caroline Grönwall1
1Department of Medicine, Rheumatology Unit, Karolinska Institutet, Karolinska University Hospital, Stockholm, Sweden; 2Department of Medicine, University of Minnesota Medical School, Minneapolis, Minnesota, USA; 3The Center for Immunology, University of Minnesota Medical School, Minneapolis, Minnesota, USA.
4. Division of Physiological Chemistry, Department of Medical Biochemistry and Biophysics, Karolinska Institutet, Stockholm, Sweden
Background
Fab-glycosylation is found in ~15-25% serum IgG and while its exact consequence remains unknown, it may alter IgG functionality. Recent data revealed elevated Fab-glycosylation in polyclonal anti-citrullinated protein autoantibodies (ACPA) from rheumatoid arthritis (RA) patients. Herein, we characterize the Fab-glycan profile of monoclonal ACPA.
Methods
A total of 14 recombinant human ACPA, derived from RA synovial plasma cells or circulating memory, were evaluated for predicted N-linked glycosylation sites using the NetNGlyc server. Fab-glycosylation was verified with enzymatic digestion, Western blot, lectin-ELISA, and mass spectrometry. Antigen binding was investigated by CCP3 ELISA. VH-VL structure models were generated using the PIGS tool and the GlyProt server. The frequency of predicted VH-VL sites was compared to single-cell paired heavy and light chains from extensively mutated mAbs (>15 mutation in VH or VL): 51 expressed non-ACPA synovial B cells from seropos. RA, and 27 from seroneg. RA, and 198 bone marrow (BM) plasma cells, and 27 clones from healthy control circulating memory. These were compared to 19 highly-mutated broadly-neutralizing (bn) HIV mAbs and 103 plasmodium faciparium (PF) specific mAbs from the literature. Fisher’s exact test or Kruskal-Wallis test was used in statistical analysis.
Results
The majority of ACPA exhibited variable region N-linked motifs (85.7%), compared to 18.5% in control (p<0.0001), 21.2% in RA BM plasma cells (p<0.0001), 31.4% non-ACPA synovial RA mAbs (p=0.0005), 7.4% of clones from seroneg. RA (p<0.0001), 25.2% in PF mAbs (p<0.0001), and 63.2% of HIV bnAbs (p=0.24), featured in both framework and CDRs generated by somatic hypermutation (SHM). Indeed, ACPA displayed high level of SHM (average 30 VL and 52 VH), yet when adjusted for SHM, N-linked motifs were significantly elevated in ACPA compared to all groups including bnAbs. IgG mAb characterization revealed that N-linked motifs were indeed glycosylated, although preliminary data suggested that glycans had no striking effect on antigen-binding. Homology-based structures predicted glycans to be primarily positioned outside of the potential antigen-binding site. Lectin analysis and mass spectrometry suggested that ACPA mAb Fab-glycan composition was distinctly different from Fc-glycans, and could have high sialic acid content.
Conclusions
The results support that Fab glycosylation is a key feature of ACPA. Significant increases in N-linked motifs in ACPA compared to other highly-mutated antibodies signifies that this is not solely associated to mutation frequency. Future studies are merited to further investigate the selection mechanisms and functional role of Fab-glycosylated autoantibodies.
19. Autoantibodies to post-translational modifications in Rheumatoid Arthritis are highly diverse in characteristics and functionality.
Johanna Steen1, Peter Sahlström1, Victoria Odowd2, Akilan Krishnamurthy1, Lena Israelsson1, Monika Hansson1, Linda Mathsson Alm3, Karl Skriner4, Stephen Rapecki2, Holger Bang5, Anca Catrina1, Daniel Lightwood2, Lars Klareskog1, and Vivianne Malmström1
1 Karolinska Institutet, Stockholm, Sweden
2 UCB, Slough, England
3 Thermo Fisher, Uppsala, Sweden
4 Charité Univeristätsmedizin, Berlin, Germany
5 Orgentec Diagnostika, Mainz, Germany
Rheumatoid Arthritis (RA) is a common inflammatory autoimmune disease that is characterized by a sub-population harboring autoantibodies to citrullinated antigens (ACPA). Patients that are ACPA positive suffer from a more severe disease and this set of autoantibodies have been postulated to be involved in the RA pathogenesis. However, ACPA appear years before disease onset, and thus have this notion been questioned.
We have expressed monoclonal plasma cell derived IgG antibodies from an RA patient’s joint. We showed that ACPA were highly mutated as compared to the nonACPA antibodies and were not phylogenetically related, and thus originated from separate immune responses. One of the four identified ACPA were clonally expanded.
The four ACPAs were all highly cross-reactive with different citrullinated targets, both peptides and proteins, however did they never target any non-modified antigens. None of the ACPA had identical citrulline recognition pattern. One of the autoantibodies also detected carbamylated antigens, another post-translational modification related to RA autoimmunity.
We made chimeric antibodies where we removed the hypermutations in either the heavy or the light chain, to dissect their contribution. We concluded that mutations could be restricted to one of the chains (either the light or the heavy), with retained citulline reactivity.
To investigate if the ACPA could have effect on bone destruction in RA, we tested the ACPAs in in vitro assays. Two of the ACPA had effect – one had a promoting effect, and one had an inhibitory effect in vitro. This highlights the importance of monoclonal investigations of ACPA functions.
20. Occupational Exposure to Asbestos and Risk of Rheumatoid Arthritis Authors: Anna Ilar1, Per Gustavsson1,2, Pernilla Wiebert1,2, Camilla Bengtsson1, Lars Klareskog3, Lars Alfredsson1,2 1. The Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden

2. Centre for Occupational and Environmental Medicine, Stockholm County Council, Stockholm, Sweden 3. Rheumatology Unit, Department of Medicine, Karolinska Institutet, Stockholm, Sweden Background Due to the known association between silica dust and rheumatoid arthritis (RA), we wanted to study the association between RA and another silicate mineral; asbestos. The aim was to estimate the risk of seropositive or seronegative RA from ever occupational asbestos exposure as well as years with exposure. Methods The study base consisted of men and women living in Sweden between 2006 and 2013. RA patients were identified from the Swedish Rheumatology Quality Register (SRQ). We matched ten controls from the national population register per case on age, county and sex. Data on occupational histories were collected from the national population and housing censuses carried out in 1960, 1970, 1975, 1980 and 1990. A job-exposure matrix (JEM) containing historical exposure estimates from 1955-1995 to asbestos was applied to the study participants’ occupational histories. We used conditional logistic regression to assess the odds ratios (ORs) and 95 % confidence intervals (CIs) of RA associated with ever exposure and years of exposure to asbestos. ORs were adjusted for ever exposure to silica dust and household disposable income divided into quartiles. Results 9 704 cases and 90 271 controls were included in the analysis. Ever vs. never asbestos exposure resulted in an OR of 1.35 (95 % CI: 1.22-1.48) among men and 1.10 (95 % CI: 0.94-1.29) among women for seropositive RA. The ORs decreased to 1.12 (95 % CI: 1.01-1.25) and 1.02 (95 % CI: 0.86-1.22) for men and women respectively after adjusting for silica exposure and household disposable income. Asbestos exposed men were more likely than women to have worked with asbestos for a longer period of time and their risk of seropositive RA increased with years with the exposure. Male participants with more than 20 years of asbestos exposure at work had an adjusted OR of 1.27 (1.06-1.53, p for trend: 0.008). Conclusions Asbestos exposure is associated with seropositive RA among men. The increased risk remained after adjustments for potential confounding from silica exposure and household disposable income.
21. Assay comparison for measurement of drug level and immunogenicity in rheumatoid arthritis patients.
Christina Hermanrud1, Karen Hambardzumyan2, Malin Ryner1, Per Marits2, Saedis Saevarsdottir2 and Anna Fogdell-Hahn1.
1Clinical Neuroimmunology, Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden. 2Rheumatology Unit, Department of Medicine, Solna, Karolinska Institutet, Stockholm, Sweden.
Infliximab and adalimumab are tumor necrosis factor-alpha (TNF-α) inhibitors used for treatment of rheumatoid arthritis (RA). Low drug levels often correlate with anti-drug antibodies (ADA) and are
likely to result in poor clinical outcome. Serum anti-TNF-α drug levels and ADA are screened with an
in-house validated ELISA used in clinical routine at Karolinska University hospital. However, samples with a drug level above 0.2µg/mL cannot be screened for ADA due to the assay´s drug tolerance.
Moreover, immune complexes could occur, thus making ADA undetectable yielding false negative
results. We determined the correlation of drug levels and ADA between the ELISA with measurement
of neutralizing ADA (bioassay, iLite) and immune complexes (PandA with acid dissociation). For 84 RA serum samples, there were a 100% correlation of infliximab and adalimumab levels
between ELISA and iLite. All infliximab treated patients (n=17) with low drug levels
were identified as ADA positive with ELISA, but only seven were characterized with neutralizing ADA with iLite. This lack of neutralizing capacity was not in agreement with
the low drug level. RA patients treated with infliximab (n=101) were analyzed with ELISA and
PandA. After 21 months post treatment initiation, 28 patients had no measurable drug levels and 19 were ADA positive. Only 20 patients had optimal drug levels. Serum samples with a drug level above
0.2µg/mL were screened for ADA with PandA and up to 62% were positive. The clinical relevance of
screening for immunogenicity of drugs and potential possibilities to aide optimization of treatment will
be evaluated.
22. Risk Factors for Cardiovascular Disease Predate the Onset of Symptoms of Rheumatoid Arthritis
Heidi Kokkonen1, Hans Stenlund2, and Solbritt Rantapää Dahlqvist1
1Department of Public Health and Clinical Medicine, Rheumatology, Umeå University, Umeå, Sweden, 2Department of Public Health and Clinical Medicine, Epidemiology and Global Health, Umeå University, Umeå, Sweden
Background: Patients with rheumatoid arthritis (RA) are at increased risk of developing cardiovascular (CV) comorbidity compared with the general population. Contradictory results concerning CV disease prior to onset of RA have been reported. Of the known CVD risk factors, a more atherogenic lipid profile and smoking have been presented prior to RA onset.
In this study, lifestyle factors, lipid levels, presence of hypertension and diabetes were evaluated in individuals prior to onset of symptoms of RA and matched population controls from northern Sweden.
Methods: A nested case-control study was based on population surveys from The Västerbotten Intervention Programme (VIP) and the WHO Multinational Monitoring of Trends and Determinants in Cardiovascular Disease (MONICA). Data were collected by a questionnaire (socioeconomic and lifestyle factors), assessments by a nurse (body mass index; BMI, waist and blood pressure), and blood sampling. The registers of patients with RA (ARA criteria) attending the Department of Rheumatology, Umeå was co-analysed with the registers from VIP and MONICA. This study included 547 pre-symptomatic individuals (median age 50.2 years; 372f/175m, median (IQR) predating time 5.0 (7.0) years), and 1641 controls (median age 50.3 years; 1116f/525m). CVD risk factors were defined as: hypertension (systolic ≥140 mmHg and/or diastolic ≥90 mmHg including hypertensive treatment), elevated ApoB/ApoA1 ratio (females ≥0.7, males ≥0.8, including lipid lowering treatment), BMI ≥25, diabetes, and ever smoker.
Results: In conditional logistic regression models elevated ApoB/ApoA1 ratio (OR 1.3 (95% CI 1.0,1.6)), smoking (OR 2.0 (95% CI 1.6,2.5)), BMI≥ 25 (OR 1.3 (95% CI 1.1,1.6)) and diabetes (OR 2.0 (95% CI 1.1,3.7)) were associated with individuals who subsequently developed RA. In women elevated ApoB/ApoA1 (OR 1.4 (95% CI 1.1-1.8)), smoking (OR 1.9 (95% CI 1.1-1.8)), and BMI ≥25 (OR 1.3 (95% CI 1.1-1.7)) were significant for being pre-symptomatic for RA, in men the risk factors were smoking (OR 2.2 (95% CI 1.5-2.5), and diabetes (OR 4.7 (95% CI 1.71-13.1)). Stratifying on the median age, the factor remaining significant for the future RA group in older individuals was smoking (OR 1.7 (95% CI 1.2,2.5)), whereas in the individuals ≤50.2 years the factors were: elevated ApoB/ApoA1 ratio (OR 1.4 (95% CI 1.0,1.9)), BMI ≥25.0 (OR 1.5 (95% CI 1.0-2.0)), and smoking (OR 2.1 (95% CI 1.5,3.0). The pre-symptomatic individuals had significantly higher frequency of risk factors, 42% had ≥3 of these compared with 30% of the matched controls (OR 2.8 (95% CI 1.8, 4.5)). Especially, ACPA positive pre-symptomatic individuals had a high OR for future RA when having ≥3 of the CV risk factors (OR 5.7 (95% CI 2.1-15.3)).
Conclusion: Several of the CV risk factors were present in individuals already years before onset of symptoms of RA. One third of the pre-symptomatic individuals had at least 3 of these factors present. The risk factors for CVD associated with future RA differ between women and men. In younger individuals as well as ACPA positive individuals the CVD risk factors have a greater impact. These results urge an early CV prevention in patients with RA.
23. Autoreactivity to malondialdehyde-modifications in rheumatoid arthritis is linked to disease activity and synovial pathogenesis
Authors:
Caroline Grönwalla,b*, Khaled Amaraa, Uta Hardta, Akilan Krishnamurthya, Johanna Steena, Marianne Engströma, Meng Suna, A. Jimmy Ytterberga,c, Roman A. Zubarevc, Dagmar Scheel-Toellnerd, Jeffrey D. Greenbergb, Lars Klareskoga, Anca I. Catrina a, Vivianne Malmströma and Gregg J. Silvermanb
a) Rheumatology Unit, Department of Medicine, Karolinska Institutet and Karolinska University Hospital, Stockholm, Sweden
b) Division of Rheumatology, Department of Medicine, NYU School of Medicine, New York, NY, USA
c) Department of Medical Biochemistry and Biophysics, Karolinska Institutet, Stockholm, Sweden
d) Rheumatology Research Group, Centre for Translational Inflammation Research, College of Medical and Dental Sciences, University of Birmingham, Birmingham, United Kingdom
Oxidation-associated malondialdehyde (MDA) modification of proteins can generate immunogenic neo-epitopes that are recognized by autoantibodies. In health, IgM antibodies to MDA-adducts are part of the natural antibody pool, while elevated levels of IgG anti-MDA antibodies are associated with inflammatory and autoimmune conditions. Yet, in human autoimmune disease IgG anti-MDA responses have not been well characterized and their potential contribution to disease pathogenesis is not known. Here, we investigate MDA-modifications and anti-MDA-modified protein autoreactivity in rheumatoid arthritis (RA). While RA is primarily associated with autoreactivity to citrullinated antigens, we also observed increases in serum IgG anti-MDA in RA patients compared to controls. IgG anti-MDA levels significantly correlated with disease activity by DAS28-ESR and serum TNF-alpha, IL-6, and CRP. Mass spectrometry analysis of RA synovial tissue identified MDA-modified proteins and revealed shared peptides between MDA-modified and citrullinated actin and vimentin. Furthermore, relatively high frequency of anti-MDA autoreactivity among synovial B cells (3.5 % of memory B cells and 2.3% of plasma cells) was discovered when investigating recombinant monoclonal antibodies (mAbs) cloned from single B cells. Several clones were highly specific for MDA-modification with no cross-reactivity to other antigen modifications such as citrullination, carbamylation or 4-HNE-carbonylation. The mAbs recognized MDA-adducts in a variety of proteins including albumin, histone 2B, fibrinogen and vimentin. Interestingly, the most reactive clone, originated from an IgG1-bearing memory B cell, was encoded by near germline variable genes, and showed similarity to previously reported natural IgM. Other anti-MDA clones display somatic hypermutations and lower reactivity. Importantly, these anti-MDA antibodies had significant in vitro functional properties and induced enhanced osteoclastogenesis, while the natural antibody related high-reactivity clone did not. We postulate that these may represent distinctly different facets of anti-MDA autoreactive responses.
24. The prognostic value of IgA autoantibodies (rheumatoid factor and ACPA) for prediction of therapeutic responses to anti-TNF therapy in patients with rheumatoid arthritis
Daniela Sieghart1, Farideh Alasti1, Paul Studenic1, Thomas Horn2, Thomas Perkmann3, Daniel Aletaha1, Josef Smolen1, Günter Steiner1 1Division of Rheumatology, Department of Internal Medicine III, Medical University of Vienna, Vienna, Austria; 2Phadia Austria GmbH, Thermo Fisher Scientific, Vienna, Austria; 3Department of Laboratory Medicine, Medical University of Vienna, Vienna, Austria.
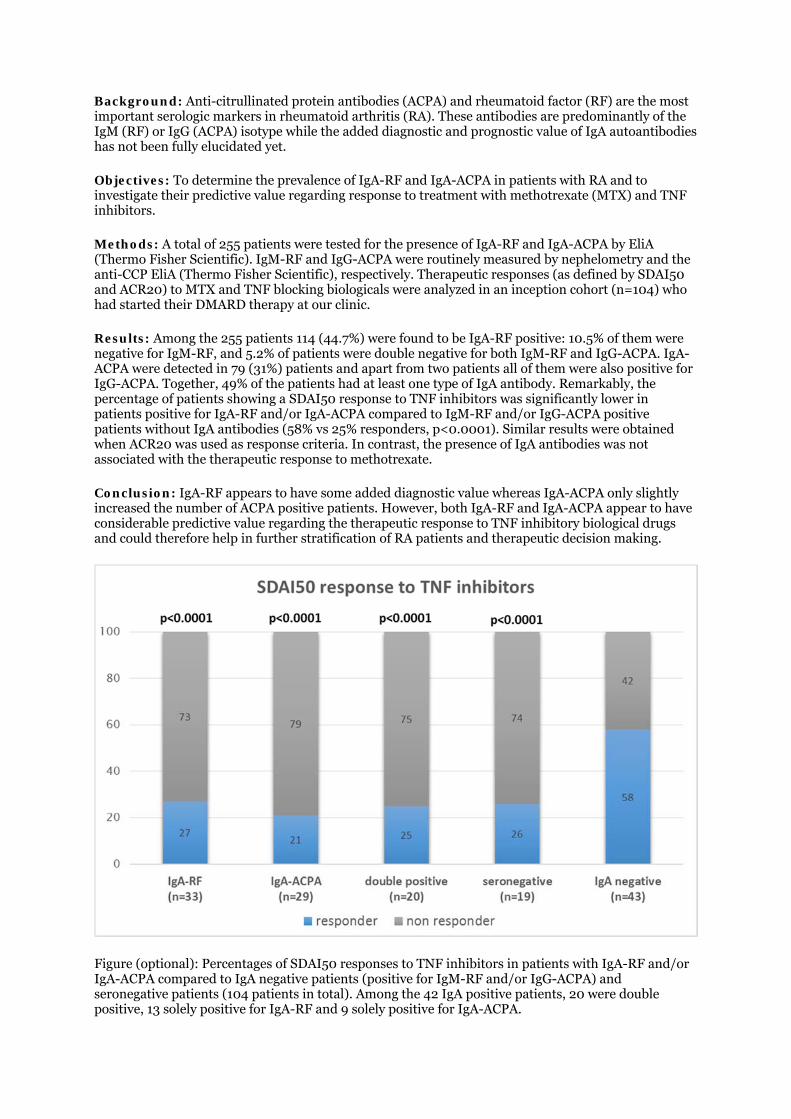
Background: Anti-citrullinated protein antibodies (ACPA) and rheumatoid factor (RF) are the most important serologic markers in rheumatoid arthritis (RA). These antibodies are predominantly of the IgM (RF) or IgG (ACPA) isotype while the added diagnostic and prognostic value of IgA autoantibodies has not been fully elucidated yet.
Objectives: To determine the prevalence of IgA-RF and IgA-ACPA in patients with RA and to investigate their predictive value regarding response to treatment with methotrexate (MTX) and TNF inhibitors.
Methods: A total of 255 patients were tested for the presence of IgA-RF and IgA-ACPA by EliA (Thermo Fisher Scientific). IgM-RF and IgG-ACPA were routinely measured by nephelometry and the anti-CCP EliA (Thermo Fisher Scientific), respectively. Therapeutic responses (as defined by SDAI50 and ACR20) to MTX and TNF blocking biologicals were analyzed in an inception cohort (n=104) who had started their DMARD therapy at our clinic.
Results: Among the 255 patients 114 (44.7%) were found to be IgA-RF positive: 10.5% of them were negative for IgM-RF, and 5.2% of patients were double negative for both IgM-RF and IgG-ACPA. IgA-ACPA were detected in 79 (31%) patients and apart from two patients all of them were also positive for IgG-ACPA. Together, 49% of the patients had at least one type of IgA antibody. Remarkably, the percentage of patients showing a SDAI50 response to TNF inhibitors was significantly lower in patients positive for IgA-RF and/or IgA-ACPA compared to IgM-RF and/or IgG-ACPA positive patients without IgA antibodies (58% vs 25% responders, p<0.0001). Similar results were obtained when ACR20 was used as response criteria. In contrast, the presence of IgA antibodies was not associated with the therapeutic response to methotrexate.
Conclusion: IgA-RF appears to have some added diagnostic value whereas IgA-ACPA only slightly increased the number of ACPA positive patients. However, both IgA-RF and IgA-ACPA appear to have considerable predictive value regarding the therapeutic response to TNF inhibitory biological drugs and could therefore help in further stratification of RA patients and therapeutic decision making.
Figure (optional): Percentages of SDAI50 responses to TNF inhibitors in patients with IgA-RF and/or IgA-ACPA compared to IgA negative patients (positive for IgM-RF and/or IgG-ACPA) and seronegative patients (104 patients in total). Among the 42 IgA positive patients, 20 were double positive, 13 solely positive for IgA-RF and 9 solely positive for IgA-ACPA.

25. Structural studies of citrullinated T-cell epitopes in rheumatoid arthritis
Anatoly Dubnovitsky1, Genadiy Kozhukh1, Tatiana Sandalova2, Adnane Achour2, Lars Klareskog1,
Vivianne Malmström1
1 Rheumatology Unit, Department of Medicine, Karolinska University Hospital in Solna, Karolinska Institutet, Stockholm, Sweden
2 Science for Life Laboratory, Department of Medicine Solna, Karolinska Institutet, and Department of Infectious Diseases, Karolinska University Hospital, Solna, Stockholm, Sweden
Citrullinated proteins can be found in humans in the setting of both health and disease. Immune
tolerance to citrullinated proteins is lost in ACPA-positive RA patients. The strong genetic association
of ACPA-positive RA with certain HLA-DR alleles suggests an important role of MHC II-mediated
antigen presentation to CD4+ T cells in RA pathology. The conversion of arginine to citrulline leads to
a significant change in physicochemical properties of the amino acid side chain by removal of a
positive charge present on arginine residue. This can affect both interaction of the modified peptides
with HLA-DR as well as interaction of peptide-MHC complex with T-cell receptors. In the latter case, a
neo-epitope is created by citrullination. In order to provide better understanding of how citrullination
alters the above-mentioned interactions we have determined several crystal structures of peptide-
MHC complexes with arginine/citrulline residues located at different positions in the MHC peptide
binding cleft. The peptides we used in this study originate from the candidate autoantigens alpha-
enolase (amino acids 26-40 or 326-340) and cartilage intermediate layer protein (amino acids 297-
311).
Our crystal structures demonstrate that the arginine/citrulline residues, which were found in positions
P-1, P2 or P3 are all solvent exposed and can therefore interact with TCR. Moreover, the citrullination
did not alter the binding register of the peptide in the MHC cleft compared to arginine version of the
same peptide. Our data thus demonstrate that citrulline can occupy different positions in the MHC
binding cleft and how citrullination in these positions creates neo-antigens that can select for new
repertoire of T-cell receptors. Hereby the T cell reactivity to citrullinated peptides in RA is broader
than previously recognised.
26. Ex vivo analysis of autoantigen-specific T cell responses using a multi HLA-class II tetramer approach
Christina Gerstner1, Hannes Uchtenhagen1,2, Jennifer Pieper1, Anatoly Dubnovitsky3,4, Karolina Tandré5, Lars Rönnblom5, William Kwok2, Eddie A James6, Vivianne Malmström1
1 Rheumatology Unit, Department of Medicine Solna, Karolinska Institutet, Stockholm, Sweden
2 Translational Research Program, BRI at Virginia Mason, Seattle (WA), USA
3 Department of Clinical Neurosciences, Karolinska Institutet, Stockholm, Sweden
4 Science for Life Laboratory, Department of Medicine Solna, Karolinska Institutet, Stockholm, Sweden

5 Department of Medical Sciences, Rheumatology, Science for Life Laboratory, Uppsala, Sweden
6 Tetramer Core Facility, BRI at Virginia Mason, Seattle (WA), USA
HLA class II tetramers allow direct ex vivo enumeration and phenotypic characterization of antigen-specific T cells and have proven useful in different settings, e.g. allergy and vaccination.
Based on flow cytometry we developed a multi HLA-class II tetramer approach that renders it possible to look at numerous specificities simultaneously and is sufficiently sensitive at the same time as auto-reactive T cells are likely to be rare. We focused on validated citrullinated T cell epitopes previously studied in RA from �-enolase, fibrinogen and CILP.
To test robustness and sensitivity of our multi-tetramer assay, we performed repeated experiments on PBMCs of HLA-DRB1*04:01-positive healthy controls (HCs) as well as RA patients.
First, we examined the sensitivity of the panel by assessing PBMC from HCs where we could detect low frequencies of auto-reactive T cells (1-10 per million CD4), mostly displaying a naïve phenotype. This was in sharp contrast to the numbers of influenza-specific T cells in the same donors that were 10-20 fold higher in numbers and of memory phenotype. Next, we tested the robustness of the panel by running technical repeats of all HC samples, which yielded similar frequencies. Thereafter, we focused on RA patient PBMC obtained from repeated blood draws (2-4 weeks apart). Also in these samples, frequencies ranged between 1-10 tetramer-positive cells per million CD4+ T cells. Moreover, not all T cell specificities were present in all patients. Still, frequencies were found to be stable in the repeated blood draws in approximately half of the individuals, implicating that frequencies close to 1 cell per million CD4+ T cells is borderline of what we can stably detect. Importantly, the patient samples utilized were not taken from time points of active disease, where we hypothesize frequencies to be elevated.
In conclusion, we developed a sensitive tetramer panel allowing simultaneous enumeration and phenotypic characterization of antigen-specific T cells in ex vivo samples from RA patients that can be used for monitoring and in-depth studying of these cells during the course of disease and treatment in individual patients.
27. Comprehensive Spatial Transcriptomics analysis of inflammatory cell infiltrates in RA and SpA synovial tissue biopsies
Konstantin Carlberg1,2, Marina Korotkova2, Anca I. Catrina2, Joakim Lundeberg1, Vivianne Malmström2
1Science for Life Laboratory, Division of Gene Technology, KTH Royal Institute of Technology
2Karolinska Institute, Department of Medicine, Rheumatology Unit, Karolinska University Hospital
Background:
Rheumatoid Arthritis (RA) and Spondyloarthropathy (SpA) are two common chronic inflammatory joint diseases where recruitment of macrophages and T cells are commonly observed in the affected synovia. Current treatment regimes for the two disorders points to both common and unique features of disease, e.g. TNF blockade being widely used for both, while IL-17 targeting can be beneficial in SpA but less so for RA. Moreover, the genetic predisposition differs between RA and SpA with certain HLA-DR class II alleles associating to RA while SpA is genetically associated to the class I allele HLA-B27 and ER aminopeptidases.
In this study we profile the whole transcriptome of synovial tissue from RA and SpA samples while at the same time capture the spatial context of the gene expression patterns on each tissue section [1]. With this spatial transcriptomic (ST) method we retrieve higher granularity and can query the differences and commonalities of gene expression in the inflammatory infiltrates of affected joint tissue in RA and SpA.
Materials and methods:
Snap frozen synovial biopsies from three ACPA+ RA patients and three SpA patients undergoing joint replacement surgery was included. Sections of 7 μm representing a single layer of cells were placed on a barcoded ST slide and prepared as previously described [1]. Library preparation, sequencing and data processing were performed according to standard ST methodology [1][2][3].
Results:
Extracted RNA from the synovial biopsies had RIN values between 6.4 and 9.2. The complexity of the samples was mirrored by the numbers of detected genes which were 16-20,000 per tissue section. The number of barcoded spots covered by tissue was 300-500 while the number of unique genes per spot varied from 300 to 2,300. Hierarchical clustering based on data from the entire sections and the top 100 differentially expressed genes showed distinctive patterns for the two diseases. The platform allowed us to next re-analyze the data focusing only on the barcoded spots covered by inflammatory cell infiltrates and hereby zoom into the local cellular crosstalk e.g. between B and T cells.
Conclusion:
By using the spatial transcriptomic method, we have generated and analyzed unprecedented transcriptomic data on immunological tissue and compared two diseases revealing gene expression patterns that could not be inherited from homogenized RNA-seq samples.
28. Macrophages drive chronic active arthritis without involvement of T cells
Cecilia Hagert1,2, Outi Sareila1, Tiina Kelkka1,3, Kutty Selva Nandakumar4,5, Sirpa Jalkanen1, Rikard Holmdahl1,5
1.Medicity, University of Turku, Turku, Finland 2. The National Doctoral Programme in Informational and Structural Biology (ISB), Turku, Finland 3. The Turku Doctoral Programme of Biomedical Sciences (TuBS), Turku, Finland 4. School of Pharmaceutical Sciences, Southern Medical University, Guangzhou, China, 5. Division of Medical Inflammation Research, Department of Medical Biochemistry and Biophysics, Karolinska Institutet, Stockholm, Sweden.
Abstract To analyze and evaluate chronic arthritis independently from the adaptive immunity we developed a novel, chronic, innate driven collagen antibody induced arthritis (CAIA) model. A four-monoclonal cocktail of anti-collagen type II antibodies initiate an active chronic arthritis, facilitated by mannan (Saccharomyces cerevisiae) injected on day five and sixty. Our model corresponds to the human rheumatoid arthritis both in its relapsing nature of the chronic phase and the inflammation caused by the infiltrating cells. This relapsing disease is driven by the complement pathway and ROS deficient macrophages. It is a model independent of FcγRIII, B- and T-cells, but a role for the innate immune system as driver of the chronic autoimmunity in this model is being suggested. In fact, our data illustrates an essential role for macrophage produced ROS to protect against the disease. On the other hand, the complement cascade seems to be promoting the disease, initiated via classical and/or alternate pathway but not through the lectin pathway. Our results, pinpoint macrophages and the

complement cascade as important drivers of active chronic arthritis, which is in contrast to the current dogma that arthritis is primarily driven by autoantibodies and T cells. Instead, this novel model specifies a role for the adaptive immunity in the beginning of arthritis, but at later stages of disease it will have less importance in driving the chronicity of the disease. This could suggest a need for an alternate approach while exploring new drug targets to attenuate arthritis.
29. THE MUTATED RNA SPLICING PROTEIN HNRNP-A3 IS A NOVEL AUTOANTIGEN IN SYSTEMIC RHEUMATIC DISEASES A LINK TO WARBURG EFFECT IN RA
B. Marklein1, M. Hansson2, G. Steiner3, G. Burmester1, K. Skriner1,*
1Department of Rheumatology and Clinical Immunology, CHARITÉ UNIVERSITY MEDICINE, Berlin, Germany, 26 Rheumatology Unit, Department of Medicine, Karolinska Institutet, Stockhom, Sweden, 32Division of Rheumatology, Department of Internal Medicine III, Medical University of Vienna, Vienna, Austria
Background: The present study was undertaken to investigate novel anti-hnRNPs autoantibodies in rheumatic diseases.
Objectives: Novel mutated hnRNP A3 was cloned out of RA synovial tissue linking it directly to Warburg effect and lactate production in RA. Increased lactate production in RA synovia and tumors is klinked to alternative splicing process from PKM1 to PKM2 hnRNPs dependent
Methods: After immunobloting and 2D-gel-eletrophoresis of a semipurified hnRNP fraction two protein spots were sequenced and identified to be highly similar to hnRNPA3. The hnRNP A3 variants were cloned from RA synovial tissue, which identified the isoforms found on protein level. 3700 RA sera were screened for the presence of mutated anti-hnRNP A3 autoantibodies using recombinant proteins and peptides thereof. Binding of RNA to hnRNP A3 (MA3) and mutated citrullinated A3 peptides (MCA3) the epitope recognition was investigated. Expression of hnRNP A3 in synovial tissue was analysed by
Results: Autoantibodies to MA3 protein were detected in 13 % of RA (n=215) patients, in 9% SLE(n=154), in 27 % of MCTD patients (n=44/10) and in less than 5% of 129 patients with other rheumatic disorders but not at all in healthy controls on immunoblot. When using renaturated MA3 on ELISA 22% of RA patients were detected and 87 % of these patients had erosive arthritis. Same modification as in cancer cells were identified in synovial tissue and verified by MS and DNA sequencing. Using 2-3 citrullinated MCA3 peptides up to 81% of patients (n=150) with established and 67% (n=2926) of patients with an early RA with a specificity of 97% were detected. In early RA 27% and 25% in established RA of CCP2 negative and 93% of CCP2 positive patients were identified. By combining with the already established CCP2 and the new MCA3, 72% of early patients are positive. MCA3 autoantibodies predominantly occur (p <0.001) in an erosive, severe course of disease and approximately 60% of these patients receive a TNF alpha blocker within a year. MRL Lpr/lpr sera were hnRNP-A3 reactive and the antibody generation is Toll 7 and 9 dependent. Anti-hnRNP-A3-antibodies are directed to conformational RNA binding epitopes. Expression of hnRNP-A3 revealed the antigen to be overexpressed in RA synovial tissue.
Conclusions: Mutated hnRNP-A3 is as a novel Toll7/9 dependent autoantigen in systemic rheumatic diseases. These mutated proteins are major components of RNA and DNA containing alternative splicing complexes leading to the Warburg effect and and autoantibodies predominantly occurre in an erosive, and severe courses of RA.
30. NEW AUTOANTIGEN (JKTBP) PART OF STRESS GRANULES CLOSES THE SENSITIVITY GAP IN RHEUMATOID ARTHRITIS
B. Marklein1, M. Jenning1, K. Muenzer1, G. Burmester1, K. Skriner1,*
1Department of Rheumatology and Clinical Immunology, CHARITÉ UNIVERSITY MEDICINE, Berlin, Germany
Background: Rheumatoid arthritis triggers the formation of prion-like stress granules. To investigate which members of the heterogeneous nuclear ribonucleoprotein (hnRNP)-family, components of functionally important subcellular particles are targeted by autoantibodies from RA and other systemic rheumatic diseases.
Methods: Using a protein macroarray we identified JKTBP in humans and animal models of inflammatory rheumatic diseases. Bacterially expressed recombinant JKDBP proteins were used to confirm the obtained data. Epitope, TLR7/9 and MyD88 dependency was determined by ELISA. JKTBP expression in cultivated cells and synovial tissue was analysed by indirect immunofluorescence, immunoblot and immunohistochemistry.
Results: Anti-JKTBP autoantibodies were detected in 46% of the patients with systemic lupus erythematosus (n=103), in 20-30% of the patients with rheumatoid arthritis (n=286), in 10% of the patients with mixed connective tissue disease (n=20) or spondyloathropathy (n=20) , and in <10% of patients with other autoimmune disorders (n=382). Sera positive to JKTBP as well as hnRNP-B1, revealed nearly two thirds of the RF IgM/ CCP2-seronegative patients as early RA patients. Combining sensitivities to all autoantigens tested (JKTBP, AUF1, hnRNP-B1), it was possible to identify 92% of the early RA patients (n=91). In the MRL/lpr mouse model of SLE, mice deficient of MyD88 or TLR7/9 lacked anti-JKTBP autoantibodies, whereas mice deficient of SIGIRR/TIR8 showed enhanced anti-JKTBP autoantibody production. These results show that autoantibody generation against JKTBP, AUF1, hnRNP-B1 is dependent on TLR 7 and TLR9 like rheumatoid factor different to TLR 7 dependent generation of snRNPs. For all tested autoantigens either their titter or generation are dependent on the activation of innate immunity genes MyD88 and SIGIRR/TIR8 gene.
In localization, experiments anti-JKTBP autoantibodies specifically stained stress granules (SG) in the cytoplasm. Immunohistochemical studies revealed JKTBP to be highly expressed in SG in the cytoplasm of RA synovial tissue different from OA and normal control tissue
Conclusions: These data identify SG as targeted particle in RA and JKTBP as a novel autoantigen in RA, SLE patients and mouse models of inflammatory rheumatic diseases. In combination with the hnRNPs AUF1 and hnRNP-B1, JKTBP autoantibodies close the sensitivity gap in RA left by rheumatoid factor and anti-CCP2 antibodie
31. Impact of Toll-like receptor 9 in inflammatory arthritis and osteoclastogenesis
Anita Fischer*, Christina Böhm*, Marije Koenders†, Wim van den Berg†, Tobias Rothe‡, Gerhard Krönke‡, Diana Dudziak# and Günter Steiner*.
*Department of Rheumatology, Medical University of Vienna, Austria. †Department of Rheumatology, Radboud University Nijmegen Medical Centre, Netherlands. ‡Internal Medicine III and #Department of Dermatology, University of Erlangen-Nuremberg, Germany.
Background and Objectives. Release and insufficient removal of endogenous nucleic acids may be involved in triggering autoimmune reactions important in the initiation of systemic autoimmune diseases including rheumatoid arthritis (RA). Nucleic acid sensing molecules, such as the endosomal Toll-like receptors (TLRs) 7 and 9, have been linked to pathogenic autoimmune processes, but their role in RA is less clear. To gain more insight into the role of TLR9 in autoimmune arthritis, TLR9 inhibition was investigated in rats with pristane-induced arthritis (PIA). To further investigate TLR9 involvement, serum transfer arthritis was induced in TLR9 knock-out mice. Materials and Methods. Arthritis was induced in mice with arthritogenic K/BxN serum and in rats with the mineral oil pristane. Rats were treated with a TLR9 antagonist, starting before disease
induction. Arthritis was scored using established scoring systems, inflammation and bone erosion were quantified by histological analysis. The role of TLR9 in osteoclast differentiation and activation was investigated in vitro. Results. In the serum transfer model, which is independent of the adaptive immune system, arthritis severity was not changed in mice lacking a functional tlr9 gene. In PIA, which is T cell-dependent, the TLR9 antagonist reduced arthritis severity by ~50%. TLR9 inhibition led to reduced inflammation, bone erosion and cartilage degradation. However, when treatment was started after the onset of arthritis TLR9 inhibition did not influence disease severity. Treatment with the TLR9 antagonist influenced downstream signaling, mainly via NFκBp65, in lymph nodes. Remarkably, mRNA levels of TLR7 and TLR9 strongly differed in the course of in vitro osteoclastogenesis. Whereas TLR7 expression did not change throughout osteoclastogenesis, expression of TLR9 was higher in precursor cells than in mature osteoclasts and stimulation with a TLR9 agonist (CpG) completely inhibited osteoclastogenesis. Conclusions. Taken together, the results suggest a role for TLR9 in the T cell-dependent initiation phase of PIA and thus an important involvement of the DNA (CpG) recognizing TLR9 in the initiation of autoimmune arthritis and during osteoclastogenesis. The precise role(s) of TLR9 in the different stages of arthritis needs to be further elucidated in future experiments.
32. Expression and clinical significance of glutamate in the serum of patients with rheumatoid arthritis
LIANG Li-Jun1; DENG Zhao-Da2; ZAHO Qin1; SHEN Hai-Li3
Objective: To analyze the expression levels of glutamate(Glu), IL-17 and TNF-α in serum of
patients with rheumatoid arthritis(RA) and investigate the clinical significance of Glu in RA.
Method: A total of 34 RA patients were enrolled and 20 healthy subjects were enrolled as healthy
control group. Glu,IL-17and TNF-a levels were determined by enzyme-linked immunosorbent
assay(ELISA), serum Glu levels
were detected in 20 cases healthy controls by the same way. Pearson correlation analysis were used to
define the correlation of Glu,IL-17andTNF-α.RA patients were divided into bone erosion group and
non-bone erosion group and compare the differences of Glu,IL-17 and TNF-α in the two groups.
Results: The levels of Glu were significantly higher in RA group than healthy control
group[(14.16±7.76)μmol/L vs(11.31±1.08)μmol/L,P=0.003],and were positively correlated to IL-
17,TNF-a,visual analogue scale(VAS) scores,disease
activity score in 28 joints(DAS28) and tender joint count,however no correlation with ESR,CRP ,anti-
CCP antibody and swollen joint count. The levels of Glu, IL-17,TNF-a in serum were higher in the
bone-erosion group than the no bone-erosion group[(16.53±10.35)μmol/L,(273.44±114.31)pg/mL,
(169.95±92.58)pg/mL vs (14.79±4.90)μmol/L,(203.62±62.18)pg/mL,(107.49±56.42)pg/mL].
Conclusion: The levels of glutamate may be involved in the occurrence of RA inflammatory
pain,and has potential significance in predicting RA bone erosion.
1.Second School of Clinical Medicine, Lanzhou University,China;
2.Department of clinical medicine, Lanzhou University,China;
3.Department of Rheumatoid Immunology, Second Hospital of Lanzhou University, China

33. Stromal inflammatory memory mediates chronification of arthritis Christiane Reinwald1, Adela Rauschenberg1, Benjamin Wirth1, Vladimir Trajkovic2, Rabinder Prinhja3, Christopher D Buckley4, Andrew Filer4, Georg Schett1, and Markus H Hoffmann1
1Friedrich-Alexander University Erlangen-Nürnberg, Department of Internal Medicine 3, Universitätsklinikum Erlangen, Germany; 2Institute of Microbiology and Immunology, School of Medicine, University of Belgrade, Serbia; 3Epigenetics DPU, Immuno-Inflammation Therapy Area Unit, GlaxoSmithKline, Medicines Research Centre, Stevenage, UK; 4Rheumatology Research Group, Institute of Inflammation and Ageing (IIA), University of Birmingham, UK.
Chronic inflammation causes severe collateral damage to the tissue that can be debilitating or life-threatening. The arthritic disorders Rheumatoid arthritis and gout are chronic, destructive inflammatory diseases often preceded by recurring, but spurious inflammatory attacks. In this project we aimed to characterize the mechanisms of the transition from acute inflammatory bouts to chronic inflammatory arthritis. Since local memory is likely mediated by stromal cells in the joint, we focused on the impact of synovial fibroblasts (SF) on chronification in arthritis in mice and humans. To model the early stages and the transition to the chronic phase in arthritis, we developed an animal model that relies on repeated injection of an inflammatory trigger into the paw, such as zymosan or monosodium urate crystals (MSU). In this model, a single exposure to zymosan/MSU led to acute but self-limiting arthritis in the respective paw. In contrast, arthritis exhibited a chronic course upon reinjection of the trigger into the same paw after resolution of the initial inflammation. Morphologically and functional comparison of SF isolated from paws that were exposed to the inflammatory trigger once or twice, respectively, revealed an elongated cell shape and higher interconnectivity in SF that had repeatedly been exposed (“trained” SF). This SF phenotype went along with increased invasiveness and higher cytokine production after exposure to the inflammatory trigger and seems to be epigenetically regulated. RNA-seq showed upregulation of the complement system and of integrins in trained SF. Blockade of integrins or complement abrogated interconnectivity and the development of inflammatory memory in vitro and in in vivo, respectively. We hypothesize that during the course of arthritis acute inflammation is gradually turned into a chronic state characterized by enhanced adhesion and higher interconnectivity between local SF. Another hallmark of chronic inflammation is the higher and prolonged reactivity upon re-exposure to an inflammatory trigger. We hypothesize that this effect is due to epigenetically regulated autoimmune memory formation, includes upregulation of integrins and the complement system, and is connected to the morphologic changes we observed and the interactions of different cells within an inflamed joint.
34.The short-term application of etanercept in the elderly in a follow-up trial in real world
WANG Xin1, XI Haipeng2, SU Jinhu3, LIANG Lijun1, WANG Xiaoyuan1, SHEN Haili1
Objective:Our aim was to compare therapeutic effects and safety of biological disease
modifying antirheumatic drugs (bDMARDs)amd conventional synthetic DMARD (csDMARD) in
elderly rheumatoid arthritis(RA) in a short-term follow-up investigation in Gansu area.
1 Department of Rheumatology,Lanzhou University Second Hospital,China 2 School of Information Science and Engineering, Lanzhou University,China 3 Department of Health Care ,Lanzhou Military Area Command of the Chinese People's Lliberation Army
Methods :100 patients were included and divided into 3 parts, elderly-onset RA(EORA, age at
disease onset>60)、non-elderly-onset RA(NEORA,age at disease onset<60,current age>60) and
younger-onset RA (YORA current age<60 ). 5 groups were named after the protocols,EORA-
bDMARDs(E-bD),NEORA-bDMARDs(NE-bD),EORA-csDMARDs(E-cD),NEORA-csDMARDs(NE-
cD),YORA-bDMARDs(Y-bD), each with 20 patients. Effectiveness and safety of the therapy were
compared among 5 groups.
Results:After 4 weeks following-up,there was a decrease in joint pain counts(E-bD9.30±7.09
,NE-bD7.15±6.68,Y-bD8.00±4.35, P<0.05),ESR(E-bD24.90±22.34,NE-bD26.15±22.33,Y-
bD29.00±17.88, P<0.05) and disease activity, in E-bD,NE-bD,Y-bD groups, especially in Y-bD(E-
bD1.87±1.34,E-cD1.42±0.76,NE-bD1.98±1.32,NE-cD1.06±0.81,Y-bD2.13±1.10, P>0.05),
however, the difference was not statistically significant. Data followed for 4 weeks showed a
larger drop of disease activity in E-bD and NE-bD groups than in E-cD and NE-cD groups,
P<0.05.After a median follow-up period of 8 weeks, the indicators of E-cD and NE-cD groups declined
compared with the baseline, but it was not statistically significant between these 2 groups
(P>0.05).The use of biological agents and csDMARDs carried a similar infection risk between EORA
and NEORA(P>0.05).It seemed Y-bD group had fewer adverse reactions than E-bD,NE-bD, but
differences were no significant(P>0.05).The adverse reactions had not statistical difference
between EORA and NEORA whatever the treatments was.
Conclusion :It would be a longer time for E-bD,NE-bD to get remissions than Y-bD groups,
meanwhile more untoward reaction might be found in E-bD,NE-bD groups. Biological agents had
a similar therapeutic effect on E-bD and NE-bD regardless of the age at disease onset and course.
Biologics has faster and better efficacy than csDMARDs in the same group, but there was
no statistics significant of adverse reactions bwtween them.The incidence of adverse events was not
associatedwith age at disease onset between E-cD and NE-cD groups.
35. Occupational Physical Workload and Development of Anti-Collagen Type II Antibodies in Rheumatoid Arthritis Patients
Pingling Zeng1 , Lars Alfredsson,1,2 Lars Klareskog,3 Mohammed Mullazehi4,
Saedis Saevarsdottir3, Camilla Bengtsson1, Johan Rönnelid4
1Institute of Environmental Medicine, Karolinska Institute, Stockholm, Sweden
2Center for Occupational and Environmental Medicine, Stockholm County Council, Stockholm, Sweden
3Rheumatology Unit, Department of Medicine at Karolinska University Hospital, Karolinska Institute, Stockholm, Sweden
4Department of Immunology, Genetics and Pathology, Uppsala University, Uppsala, Sweden
Background/Purpose: We have previously observed an association between exposure to occupational physical workload (PW) and risk of developing rheumatoid arthritis (RA)[1].We posit that PW could impose mechanical stress on the joints leading to neo-epitope formation and immune activation. The major solid component of the articular cartilage is collagen type II (CII). Elevated level of anti-CII antibodies do not predate RA development, but are transiently found in 6-9% early RA patients. These antibodies are associated with acute RA onset and HLA-DRB1*01 and *03, yet predict good long-term prognosis[2]. We hypothesized that exposure to PW especially in the period closely predating RA diagnosis would associate with anti-CII positive RA but not anti-CII negative RA.
Methods: Data involving 1396 incident RA cases and 5935 controls from the Swedish population-based case-control study, Epidemiological Investigation of Rheumatoid Arthritis (EIRA), were analyzed. Information on self-reported exposure to occupational PW was collected through questionnaire. Anti-CII was measured using ELISA. The odds ratio (OR) with 95% confidence interval (CI) of developing anti-CII positive RA or anti-CII negative RA associated with PW exposure was calculated using logistic regression. Adjustment for sex, age, residential area, educational level, alcohol consumption, body mass index, cigarette smoking, silica exposure and occupational class did not substantially change the estimates.
Results: The ORs observed for the association between anti-CII positive RA and different types of PW ranged from 1.0 (95% CI, 0.4-2.4) to 2.3 (95% CI, 1.3-4.0). There was no difference in the ORs for PW exposure at diagnosis or five years earlier (table1). The ORs for the association between anti-CII negative RA and PW ranged from 1.0(95% CI, 0.8-1.3) to 1.8(95% CI, 1.5-2.1). No statistically significant difference was observed between the ORs for anti-CII positive RA and the ORs for anti-CII negative RA (all p-values > 0.2).Stratification for HLA-DRB1*01/*03 or symptom duration did not change the results.
Conclusion: Since physical workload is associated with rheumatoid arthritis irrespective of anti-CII status or the presence of anti-CII associated HLA alleles, and regardless of whether the timing of PW exposure was close to the appearance of anti-CII. We found no evidence suggesting an association between PW and development of anti-CII in RA.
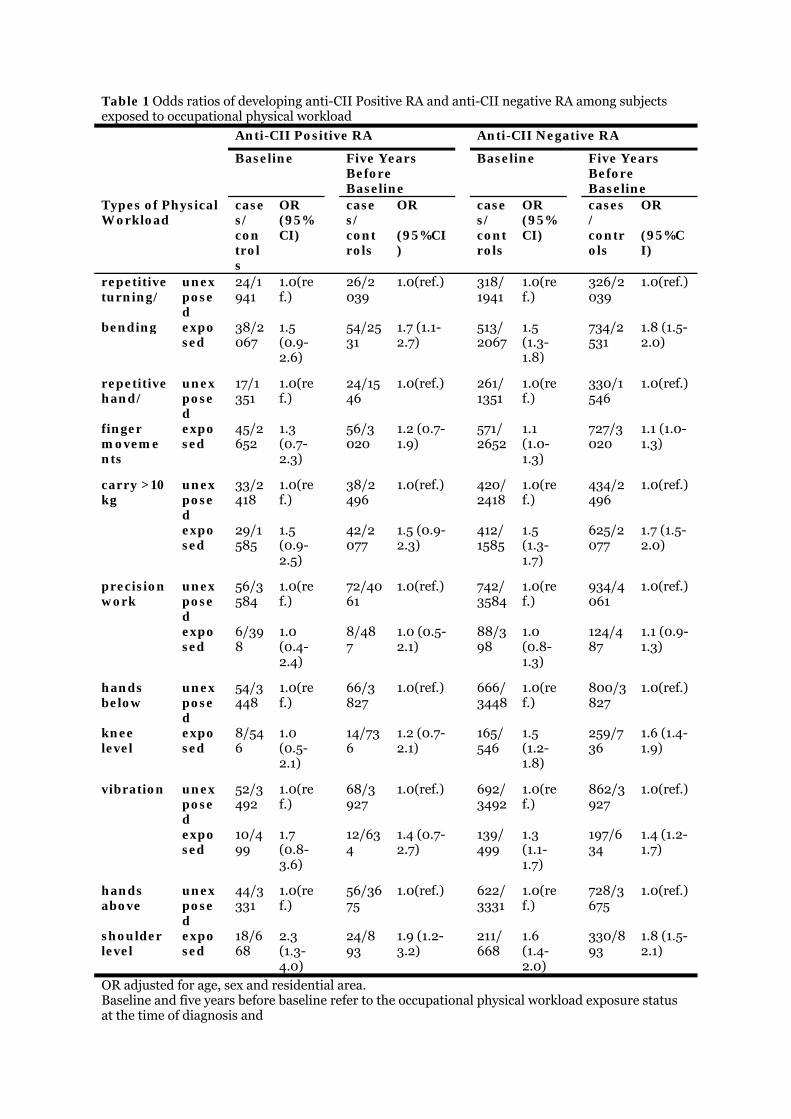
Table 1 Odds ratios of developing anti-CII Positive RA and anti-CII negative RA among subjects exposed to occupational physical workload
Anti-CII Positive RA Anti-CII Negative RA
Baseline
Five Years Before Baseline
Baseline
Five Years Before Baseline
Types of Physical Workload
cases/ controls
OR (95%CI)
cases/ controls
OR (95%CI)
cases/ controls
OR (95%CI)
cases/ controls
OR (95%CI)
repetitive turning/
unexposed
24/1941
1.0(ref.)
26/2039
1.0(ref.)
318/1941
1.0(ref.)
326/2039
1.0(ref.)
bending exposed
38/2067
1.5 (0.9-2.6)
54/2531
1.7 (1.1-2.7)
513/2067
1.5 (1.3-1.8)
734/2531
1.8 (1.5-2.0)
repetitive hand/
unexposed
17/1351
1.0(ref.)
24/1546
1.0(ref.)
261/1351
1.0(ref.)
330/1546
1.0(ref.)
finger movements
exposed
45/2652
1.3 (0.7-2.3)
56/3020
1.2 (0.7-1.9)
571/2652
1.1 (1.0-1.3)
727/3020
1.1 (1.0-1.3)
carry >10kg
unexposed
33/2418
1.0(ref.)
38/2496
1.0(ref.)
420/2418
1.0(ref.)
434/2496
1.0(ref.)
exposed
29/1585
1.5 (0.9-2.5)
42/2077
1.5 (0.9-2.3)
412/1585
1.5 (1.3-1.7)
625/2077
1.7 (1.5-2.0)
precision work
unexposed
56/3584
1.0(ref.)
72/4061
1.0(ref.)
742/3584
1.0(ref.)
934/4061
1.0(ref.)
exposed
6/398
1.0 (0.4-2.4)
8/487
1.0 (0.5-2.1)
88/398
1.0 (0.8-1.3)
124/487
1.1 (0.9-1.3)
hands below
unexposed
54/3448
1.0(ref.)
66/3827
1.0(ref.)
666/3448
1.0(ref.)
800/3827
1.0(ref.)
knee level
exposed
8/546
1.0 (0.5-2.1)
14/736
1.2 (0.7-2.1)
165/546
1.5 (1.2-1.8)
259/736
1.6 (1.4-1.9)
vibration unexposed
52/3492
1.0(ref.)
68/3927
1.0(ref.)
692/3492
1.0(ref.)
862/3927
1.0(ref.)
exposed
10/499
1.7 (0.8-3.6)
12/634
1.4 (0.7-2.7)
139/499
1.3 (1.1-1.7)
197/634
1.4 (1.2-1.7)
hands above
unexposed
44/3331
1.0(ref.)
56/3675
1.0(ref.)
622/3331
1.0(ref.)
728/3675
1.0(ref.)
shoulder level
exposed
18/668
2.3 (1.3-4.0)
24/893
1.9 (1.2-3.2)
211/668
1.6 (1.4-2.0)
330/893
1.8 (1.5-2.1)
OR adjusted for age, sex and residential area. Baseline and five years before baseline refer to the occupational physical workload exposure status at the time of diagnosis and

at 5 years prior to diagnosis respectively. OR, odds ratio; anti-CII, anti-collagen type II anti-bodies ; RA , rheumatoid arthritis; 95% CI, 95% confidence interval
36. Association between Occupational Physical Workloads and Development of Anti-Collagen Type II Antibodies in Rheumatoid Arthritis Patients
Pingling Zeng1 , Lars Alfredsson,1,2 Lars Klareskog,3 Saedis Saevarsdottir3 ,Camilla Bengtsson1, Johan Rönnelid4
1Institute of Environmental Medicine, Karolinska Institute, Stockholm, Sweden
2Center for Occupational and Environmental Medicine, Stockholm County Council, Stockholm, Sweden
3Rheumatology Unit, Department of Medicine at Karolinska University Hospital, Karolinska Institute, Stockholm, Sweden
4Department of Immunology, Genetics and Pathology, Uppsala University, Uppsala Sweden
Background/ Purpose: We have previously observed an association between exposure to occupational physical workloads (PW) and risk of developing rheumatoid arthritis (RA)[1].We posit that PW could impose excessive mechanical stress on the proteins of the joints which may lead to the formation of neo-epitopes that activate the immune system. Mechanical stress loaded on the joints is facilitated by the articular cartilage. The major solid component of the articular cartilage is collagen type II (CII). Elevated level of antibodies against CII is found in around 3-27% of RA patients[2]. Given this background, we hypothesized that the development of anti-CII antibodies in RA patients may be associated with exposure to physical workload at work.
Methods: Data involving 1396 incident RA cases and 5935 controls from the Swedish population case-control study, Epidemiological Investigation of Rheumatoid Arthritis (EIRA), were analyzed. Information on self-reported exposure to occupational PW was collected through questionnaire. The level of anti-CII antibody in the serum samples was measured. The odds ratio (OR) with 95% confidence interval (95% CI) of developing anti-CII positive RA or anti-CII negative RA associated with the exposure to PW was calculated using logistic regression. Adjustment for sex, age, residential area, educational level, alcohol consumption, body mass index, cigarette smoking, silica exposure, symptom duration and occupational class did not substantially change the estimates.
Results: The ORs observed for the association between anti-CII positive RA and different types of physical workload ranged from 1.0 (95%CI, 0.4-2.4) to 2.3 (95%CI, 1.3-4.0) (table 1). The ORs for the association between anti-CII negative RA and physical workloads ranged from 1.0(95%CI, 0.8-1.3) to 1.8(95%CI, 1.5-2.1). No statistically significant difference between the ORs for anti-CII positive RA and the ORs for anti-CII negative RA was observed (all p-values > 0.2).
Conclusion: Since physical workload is associated with rheumatoid arthritis regardless of whether anti-collagen type II antibodies are present, we found no evidence suggesting an association between occupational physical workload exposure and development of anti-collagen type II antibodies in rheumatoid arthritis patients.
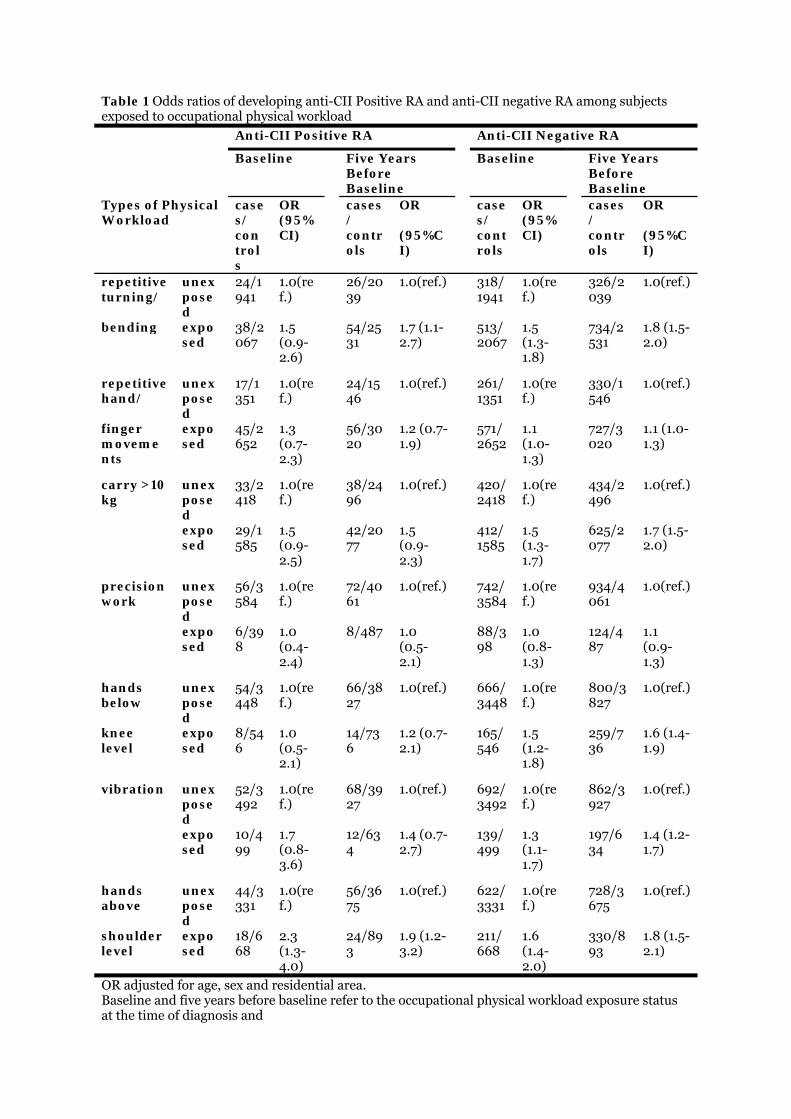
Table 1 Odds ratios of developing anti-CII Positive RA and anti-CII negative RA among subjects exposed to occupational physical workload
Anti-CII Positive RA Anti-CII Negative RA
Baseline
Five Years Before Baseline
Baseline
Five Years Before Baseline
Types of Physical Workload
cases/ controls
OR (95%CI)
cases/ controls
OR (95%CI)
cases/ controls
OR (95%CI)
cases/ controls
OR (95%CI)
repetitive turning/
unexposed
24/1941
1.0(ref.)
26/2039
1.0(ref.)
318/1941
1.0(ref.)
326/2039
1.0(ref.)
bending exposed
38/2067
1.5 (0.9-2.6)
54/2531
1.7 (1.1-2.7)
513/2067
1.5 (1.3-1.8)
734/2531
1.8 (1.5-2.0)
repetitive hand/
unexposed
17/1351
1.0(ref.)
24/1546
1.0(ref.)
261/1351
1.0(ref.)
330/1546
1.0(ref.)
finger movements
exposed
45/2652
1.3 (0.7-2.3)
56/3020
1.2 (0.7-1.9)
571/2652
1.1 (1.0-1.3)
727/3020
1.1 (1.0-1.3)
carry >10kg
unexposed
33/2418
1.0(ref.)
38/2496
1.0(ref.)
420/2418
1.0(ref.)
434/2496
1.0(ref.)
exposed
29/1585
1.5 (0.9-2.5)
42/2077
1.5 (0.9-2.3)
412/1585
1.5 (1.3-1.7)
625/2077
1.7 (1.5-2.0)
precision work
unexposed
56/3584
1.0(ref.)
72/4061
1.0(ref.)
742/3584
1.0(ref.)
934/4061
1.0(ref.)
exposed
6/398
1.0 (0.4-2.4)
8/487 1.0
(0.5-2.1)
88/398
1.0 (0.8-1.3)
124/487
1.1 (0.9-1.3)
hands below
unexposed
54/3448
1.0(ref.)
66/3827
1.0(ref.)
666/3448
1.0(ref.)
800/3827
1.0(ref.)
knee level
exposed
8/546
1.0 (0.5-2.1)
14/736
1.2 (0.7-2.1)
165/546
1.5 (1.2-1.8)
259/736
1.6 (1.4-1.9)
vibration unexposed
52/3492
1.0(ref.)
68/3927
1.0(ref.)
692/3492
1.0(ref.)
862/3927
1.0(ref.)
exposed
10/499
1.7 (0.8-3.6)
12/634
1.4 (0.7-2.7)
139/499
1.3 (1.1-1.7)
197/634
1.4 (1.2-1.7)
hands above
unexposed
44/3331
1.0(ref.)
56/3675
1.0(ref.)
622/3331
1.0(ref.)
728/3675
1.0(ref.)
shoulder level
exposed
18/668
2.3 (1.3-4.0)
24/893
1.9 (1.2-3.2)
211/668
1.6 (1.4-2.0)
330/893
1.8 (1.5-2.1)
OR adjusted for age, sex and residential area. Baseline and five years before baseline refer to the occupational physical workload exposure status at the time of diagnosis and
at 5 years prior to diagnosis respectively. OR, odds ratio; anti-CII, anti-collagen type II ; RA , rheumatoid arthritis; 95% CI, 95% confidence interval
37. Is Leukotoxin A produced by Aggregatibacter Actynomycetemcomitans Important For Initiating Autoimmune Responses Underlying Rheumatoid Arthritis?
Mikhail Volkov1, Jacqueline Dekkers1, Bruno G. Loos2, Sergio Bizzarro2, Thomas W.J. Huizinga1, Helle A. Praetorius3, René E.M. Toes1, Diane van der Woude1
1. Department of Rheumatology, Leiden University Medical Center, Leiden, the Netherlands
2. Department of Periodontology, Academic Centre for Dentistry Amsterdam (ACTA), University of Amsterdam and Vrije Universiteit, Amsterdam, the Netherlands
3. Department of Biomedicine, Aarhus University, Aarhus, Denmark
Background: In a recent publication in Science Translational Medicine, Konig et al. (2016) describe a potential explanation for the link between periodontal infection and RA. They identify a specific periodontitis-associated bacterium: Aggregatibacter actinomycetemcomitans (Aa), which via its pore-forming toxin (leukotoxin A: LtxA) can dysregulate the activity of citrullinating enzymes in neutrophils. Furthermore, the authors report that the risk conferred by the most important genetic risk factor for RA: the HLA-DRB1 shared epitope (HLA SE) alleles, was limited to RA patients who had been exposed to Aa as determined by seropositivity to LtxA. Aiming to replicate their findings, we focused on two main questions: 1) is the increased exposure to Aa as measured by the presence of anti-LtxA-antibodies specific for RA, or also present in other forms of inflammatory arthritis? 2) can we replicate the finding that the association between HLA SE alleles and ACPA-positive RA is limited to the anti-LtxA-positive subset?
Methods: We established an ELISA against purified LtxA (acquired from the same source as in the original article) and tested sera from 594 patients from the Leiden Early Arthritis Clinic with various diagnoses, including RA, OA, SpA, PsA, sarcoidosis, and gout. Serial dilutions of a mix of 3 strongly positive RA patients were used as a standard, and the lowest point of the linear part of the standard curve (2000 AU/ml) was defined as the cut-off.
Results: Anti-LtxA antibodies could be found in a substantial proportion of RA patients, but also in patients with other forms of arthritis. Within RA patients, there was no association with the presence of HLA SE alleles and/or ACPA, in contrast to the previous findings.
Conclusion: Although microbial influences may well be important in the development of RA, our results do not support a key role of exposure to LtxA originating from the periodontal pathogen Aa in linking the effect of the HLA SE alleles and periodontal disease to anti-citrullinated protein autoimmunity in RA.
38. Free secretory component among patients with recent-onset RA and patients with ACPA-positive musculo-sceletal pain
Klara Martinsson, Michael Ziegelasch, Jan Cedergren, Per Eriksson, Vladimir Klimovich*, Åsa Reckner-Olsson, Marina Samoylovich*, Christopher Sjöwall, Thomas Skogh, Jonas Wetterö & Alf Kastbom.

Department of Clinical and Experimental Medicine, Faculty of Medicine and Health Sciences, Linköping University, Linköping, Sweden, *Russian Research Center for Radiology and Surgical Technologies, St. Petersburg, Russia
Background: Emerging evidence suggests that mucosal immunity is important for development of rheumatoid arthritis (RA). Secretory component (SC) is expressed on mucosal epithelial cells and involved in formation of secretory IgA (sIgA). During this process, SC may be shed, forming free SC. This project aimed to determine if free circulating SC is elevated in RA or during its development. We also addressed the prognostic value of circulating SC levels among patients with recent-onset RA.
Materials & Methods: Two inception cohorts were studied, i.e. TIRA2 (timely intervention in RA) comprising 498 recent-onset RA patients (symptom duration <12 months) with clinical and radiological follow-up during 3 years, and the TIRx cohort (Xtra timely RA follow-up) including 110 patients with circulating IgG anti-citrullinated peptide antibodies (IgG-ACPA) and musculo-skeletal pain, but ≤1 joint with palpable synovitis (the majority having none). Free SC was analysed in serum using a sandwich ELISA. Controls comprised of blood donors (n=100) and patients with ankylosing spondylitis (AS), ANCA-associated vasculitis (AAV) or systemic lupus erythematosus (SLE) (total n=169).
Results: Free SC was elevated in TIRA2 patients compared to all controls (p<0.01). The proportion of patients testing positive was higher among IgG-ACPA positive patients compared to IgG-ACPA negative patients (p<0.001). Free SC levels correlated with sIgA-ACPA in serum (r=0.55; p<0.001), IgG-ACPA (r=0.38; P<0.001) and smoking. 3 months after inclusion, the levels of free SC had declined slightly, and the change in SC level correlated with change in disease activity score (DAS28; r=0.12; p=0.006). Free SC levels were increased among TIRx patients compared to blood donors, AAV patients, and SLE patients, but not to AS patients. No significant difference in free SC levels was detected in those who had palpable synovitis at baseline, or developed RA within 1 year.
Conclusion: Free SC levels are higher among recent-onset RA patients compared to other inflammatory diseases and associate with presence and levels of ACPA. Furthermore, free SC was elevated among IgG-ACPA positive patients prior to arthritis development. These findings provide yet another link between ACPA production and mucosal surfaces early in RA development.
39. LILRA3 contributes to osteoclastogenesis independently or synergy with RANKL
Jianping Guo, Mengru Liu, Yan Du, Yuxuan Wang, Yundong Zou, Fanlei Hu, Zhanguo Li
Department of Rheumatology and Immunology, Peking University People's Hospital,
Beijing, China
Objective Leukocyte immunoglobulin-like receptor A3 (LILRA3) is a secreted protein belongs to
LILR family. Our research group previously reported that the functional LILRA3 is a novel genetic risk
for multiple autoimmune diseases including rheumatoid arthritis (RA). LILRA3 had an impact on joint
destruction, especially in early ACPA-positive RA. In present study, we aimed to investigate the effect
of the variant on osteoclast differentiation.
Methods Expression of LILRA3 in serum and synovial fluid (SF) from patients with RA, OA, and
healthy controls were measured by ELISA. RAW264.7 cells or PBMCs from RA, OA patients and
healthy controls were cultured or transfected with recombinant LILRA3 protein in presence or absence
of RANKL and M-CSF. Expression of osteoclast-related markers, including TRAP, CTSK, MMP-9 were
measured by q-PCR, IHC and western blotting method. Bone resorption activity of osteoclasts was
determined by bone slices stained with toluidine blue. Three MAPK family signaling members
including ERK, JNK and p38, and NF-B signaling pathway activities were assessed by western
blotting.
Results Compared to healthy controls, the levels of serum LILRA3 were increased in patients with RA
and OA (p<0. 01). LILRA3 was specifically expressed in SF from RA but not OA patients (p<0.001).
The serum LILRA3 level was positively correlated with Sharp-vander Heijde scores in RA patients
(r=0.36, p=0.003). LILRA3 promoted osteoclast differentiation independently or synergy with
RANKL in RAW264.7 cells or human PBMCs through ERK, JNK and NF-B, but not p38 signaling
pathways.
Conclusion Our data indicate that LILRA3 may serve a potent pro-inflammatory factor participated
in osteoclast differentiation through MAPK family and NF-B signaling pathways in RA development.
40. LOW RATES OF RADIOGRAPHIC PROGRESSION OF STRUCTURAL JOINT
DAMAGE OVER 2 YEARS OF BARICITINIB TREATMENT IN PATIENTS WITH
RHEUMATOID ARTHRITIS
Authors: D. van der Heijde1, M. Schiff2, Y. Tanaka3, R. Klar4, L. Xie5, G. Meszaros5, T. Ishii5, M.
Casillas5, R. Ortmann5, P. Emery6, E. Larsson7 (Non-Author Presenter)
Affiliations: 1Leiden University Medical Center, Leiden, Netherlands, 2University of Colorado,
Denver, United States, 3School of Medicine, Kitakyushu, Japan, 4Quintiles IMS Holdings, Inc,
Durham, 5Eli Lilly and Company, Indianapolis, United States, 6University of Leeds, Leeds, United
Kingdom,7Eli Lilly Sweden AB, Solna, Sweden
Background: In a ph3 study, baricitinib (bari) inhibited progression of radiographic joint damage for
up to 1 year in patients (pts) with active rheumatoid arthritis (RA) who were DMARD-naïve or who
had an inadequate response to conventional synthetic DMARDs (csDMARD-IR).
Objectives: To evaluate radiographic progression of structural joint damage in pts with RA over 2
years of treatment.
Methods: Upon completion of a bari ph 3 study, pts could enter a long-term extension (LTE) study, in
which they continued to receive the same bari dose as in the original ph3 study. At 52 wks, DMARD-
naïve pts receiving methotrexate (MTX) or combination therapy (bari 4mg + MTX) were switched to
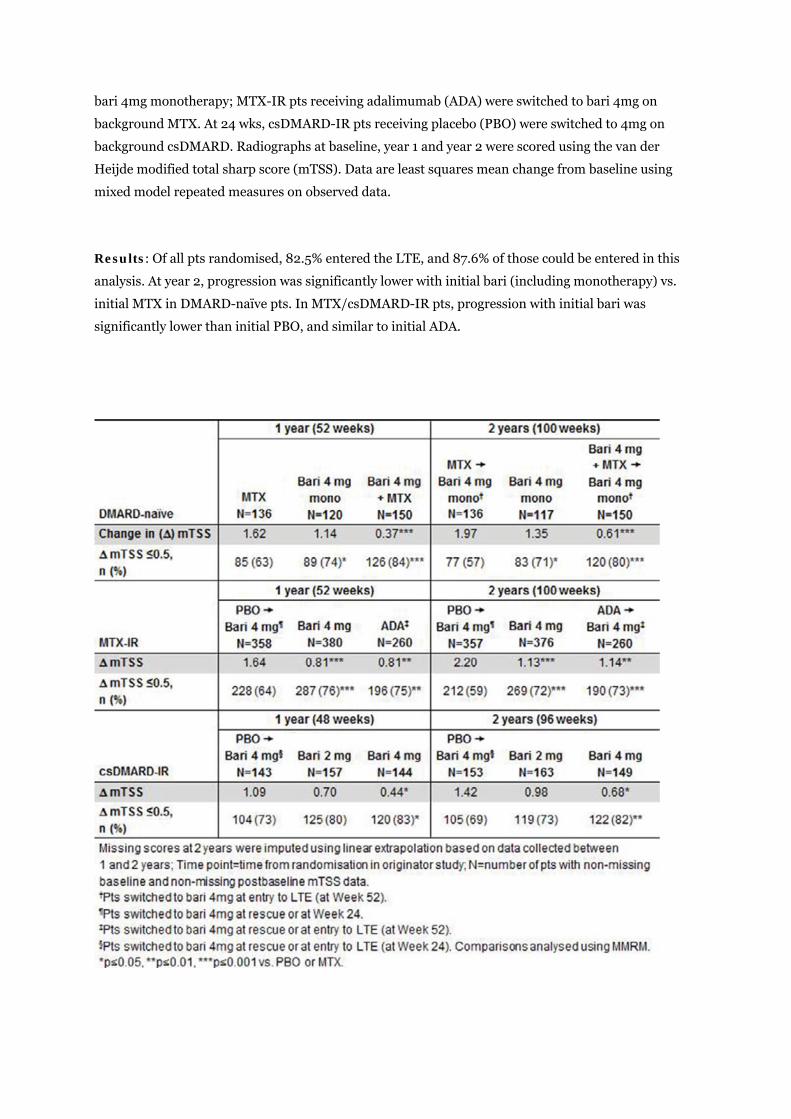
bari 4mg monotherapy; MTX-IR pts receiving adalimumab (ADA) were switched to bari 4mg on
background MTX. At 24 wks, csDMARD-IR pts receiving placebo (PBO) were switched to 4mg on
background csDMARD. Radiographs at baseline, year 1 and year 2 were scored using the van der
Heijde modified total sharp score (mTSS). Data are least squares mean change from baseline using
mixed model repeated measures on observed data.
Results: Of all pts randomised, 82.5% entered the LTE, and 87.6% of those could be entered in this
analysis. At year 2, progression was significantly lower with initial bari (including monotherapy) vs.
initial MTX in DMARD-naïve pts. In MTX/csDMARD-IR pts, progression with initial bari was
significantly lower than initial PBO, and similar to initial ADA.
Conclusions: Treatment with once-daily oral bari resulted in low rates of radiographic progression
for up to 2 years. Pts starting with bari showed progression that was significantly less than those
starting with PBO or MTX, and comparable to those starting with ADA. The most robust benefit was
seen with the 4mg dose.
This abstract was previously presented at EULAR 2017, Madrid, 14th-17th June and published in the
Annals of the Rheumatic Diseases, June 2017, Volume 76 (Supplement 2), page 510-511.
Disclosure of Interest: D. van der Heijde Consultant for: AbbVie, Amgen, Astellas, AstraZeneca,
BMS, Boeringer Ingelheim, Celgene, Daiichi Sankyo, Eli Lilly and Company, Galapagos, Gilead,
Janssen, Merck, Novartis, Pfizer, Regeneron, Roche, Sanofi-Aventis, UCB, Employee of: Director of
Imaging Rheumatology bv, M. Schiff Consultant for: Abbvie, BMS, Eli Lilly and Company, Johnson &
Johnson, Speakers bureau: Abbvie, Y. Tanaka Grant/research support from: Mitsubishi-Tanabe,
Takeda, Daiichi-Sankyo, Chugai, BMS, MSD, Astellas, Abbvie, Eisai, Speakers bureau: Abbvie, Chugai,
Daiichi-Sankyo, BMS, Mitsubishi-Tanabe, Astellas, Takeda, Pfizer, Teijin, Asahi-kasei, YL Biologics,
Sanofi, Janssen, Eli Lilly and Company, GlaxoSmithKline, R. Klar Employee of: Quintiles IMS
Holdings, Inc., L. Xie Employee of: Eli Lilly and Company, G. Meszaros Employee of: Eli Lilly and
Company, T. Ishii Employee of: Eli Lilly and Company, M. Casillas Employee of: Eli Lilly and
Company, R. Ortmann Employee of: Eli Lilly and Company, P. Emery Consultant for: Pfizer, MSD,
Abbvie, BMS, UCB, Roche, Novartis, Samsung, Sandoz, Eli Lilly and Company.