Embed Size (px)
Citation preview

8 April,2009
Planning a Community based Cancer Registry
Cancer Registration: Principles and Methods Edited by Jensen O. M. et al IARC
1991; pages 22 – 28.

8 April,2009
– The World Health Organization estimates that 7,6 million people died of Cancer in 2005 and 84 million people will die in the next 10 years if action is not taken.
– More than 70% of all Cancers Deaths occurs in Low and Medium Income Countries , where resources available for prevention, diagnosis and treatment of cancer are limited or non existent.
Cancer Control: Knowledge In Action: WHO,2006
Planning a Community based Cancer Registry

8 April,2009
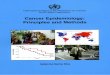
0 50 100 150 200
Developing
Developed
205020202000
PROJECTED CANCER CASES: 2000-2050

8 April,2009
2.1 2.3
5.56.7
0
2
4
6
8
10
2005 2015
tota
l dea
ths
(mill
ions
)
high income countries low-middle income countries
Cancer Deaths
9.07.6
WHO mortality database and projections

8 April,2009
Planning a Community based Cancer Registry
Estimated ASR(W) Gobocan,2002
314.1
158.7
158.7
228
128.8
156.7
0 50 100 150 200 250 300 350
More developed
Less developed
Eastern Africa
ASR(W)
Female
Male

8 April,2009
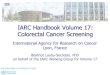
38 (710)86/105
45 (3700)48/83
Number of countries (total population in millions, 2000)Registries, populations in CI5 IX: accepted/submitted
10 (31)16/18
51 (800)4/16
28 (520)10/29
3 (310)119/136
GEOGRAPHICAL COVERAGE FOR- CI5IXPERIOD -1998-2002

8 April,2009
CI5 Volume IX 1998-2002CI5 Volume IX 1998-2002World population covered is 11%World population covered is 11%
(704.5 million) (704.5 million)
Cancer registries Included /submitted
% by
Continent
Population Coverage
million (%)
Africa (5/16) 31% 8.8 (1%)
Asia (44/77) 57% 152.3 (4%)
Europe (100/120) 83% 238.8 (33%)
North America (54/58) 93% 258.5 (80%)
Oceania (11/13) 85% 23.0 (73%)
South and Central America
(11/29) 38% 23.0 (4%)

8 April,2009
Cancer Incidence in Africa from the population based cancer registries
Ci5IX-1998-2002

8 April,2009
Cancer registry
•“The activity of a Population Cancer Registry is to collects information on all new cases cancer in a reference population, usually that of a defined geographical area.”
•“The minimal objectives are: incidence rates, planning and evaluation of cancer control program and survival.”
Jensen& Storm, 1991

8 April,2009
Cancer Registry
•Aims:
• To produce data on cancer INCIDENCE .
• Validate data on cancer MORTALITY.
• Time TRENDS
• Outcomes in Cancer SURVIVAL,
• Pathway to cancer RESEARCH .
• Instrument to support Cancer Control.

8 April,2009
Planning a Community based Cancer Registry
• Definition of cancer registry
• Advisory committee
• Population denominators
• Legal aspects on confidentiality
• Size of population and number of cases
• Physical Location of the registry
• Finance
• Personnel
• Equipment and office space

8 April,2009
Planning a Community based Cancer Registry
• Definition of cancer registry
• Cancer Registration is a process of continuing, systematic collection of data on the occurrence and characteristics of reportable malignant neoplasm with the purpose of helping to asses and control the impact of cancer in the
community.
Jensen& Whelan, 1991

8 April,2009
Planning a Community based Cancer Registry
• Cancer Registry
• Cancer Registry is an office or institution which attempts to collect, store, analyse and interpret data on persons with diagnosis of cancer .(or tumours )
–Ex urinary tract papilomas, brain tumours.Jensen& Whelan, 1991

8 April,2009
Planning a Community based Cancer Registry
• Population Based Cancer Registry
• The population based cancer registry collect information of all new cancer cases in defined population( most frequently in a geographical area )
–Data on cancer incidence has to be collected from all sources of information in the coverage area in starting from
Jensen& Whelan, 1991

8 April,2009
• New York State Cancer Registry, United States
• Registration area• The New York State Cancer Registry (NYSCR) contains reports on
all malignant tumors (except basal cell and squamous cell skin cancers), most in situ lesions, and certain benign tumors. The Registry, which is the second oldest state tumor registry in the United States, has had mandated cancer reporting since 1940. At the time of its founding, the registration area covered the entire state except New York City. Beginning in 1973, the reporting mandate was extended to include New York City. The Registry
is considered to be population-based since 1976.
GEOGRAPHICAL COVERAGE
CI5IX, Narratives www.dep.iarc

8 April,2009
Planning a Population Based Registry
• Advisory committee:
• It is board composed by cancer registry personnel, epidemiologist, pathologist, oncologist, and representing from the source of information and potential users of cancer registry data.
• They can be a link to establish cooperation and support with the local medical community and health care professionals.

8 April,2009
Planning a Population Based Registry
• Population denominators
• The availability of accurate and regularly published population data.
• Population figures by sex and five years age group. Except for Childhood cancer.
• The population cancer registry must use de definitions of populations groups, geographical areas as they are presented by the official vital statistics.

8 April,2009

8 April,2009
Population Based Cancer Registry Narrative and population

8 April,2009
Planning a Population Based Registry
• Legal aspects on confidentiality
• Reporting a cancer cases to a population based cancer registry can be:– Compulsory.– By Legislation.– Administrative order.

8 April,2009
Planning a Population Based Registry
• Size of a population and number of cases
• There is no ideal size for a population cancer registry.
• most of the cancer registry operates with a source of population from one to half a million

8 April,2009
Planning a Population Based Registry
• Size of a population and number of cases
• Large populations – difficult to maintain completeness and data quality.
• Small populations – takes time to get meaningful data.
• Intermediate population – linkage with vital statistics

8 April,2009
Korea National cancer Registry – population 48 million
Hiroshima 1,13milion
Large populations
Small populations
1999-2002-Number of casesMale =241.155Female=183.620
1996-2000-Number of casesMale=14.450Female=10.260

8 April,2009
Size of the population 5.340.000 million
Intermediate population
1998—2002Number of casesMale=61.586Female=66.532

8 April,2009
Planning a Population Based Registry
• Size of a population and number of cases
• It depends of the size of the country it is preferable to establish a intermediate cancer registries to ensure completeness and data quality

8 April,2009
Planning a Population Based Registry
• Physical Location of the registry• The location of the cancer registry
depends of the local situation – Universities – Associated hospital – Cancer centre – Pathology labs – Health statistics – Ministry of Health

8 April,2009
Planning a Population Based Registry
• Physical Location of the registry• • The location is intimately linked to the administrative
dependency of the cancer registry.
• Has to be able to request demographic data and to obtain detailed information from the medical sources in the region and to the governmental health services either professional groups.
• The cancer registry should be autonomous as possible to interact and collaborate nationally and internationally.

8 April,2009
Planning a Population Based Registry
•Finance• Funds to maintain a cancer registry
depends on:
• The size of the cancer registry.
• The number of data collected.
• The number and size of the different sources of information.
• If the registries do a regular follow up of the cases.
• The costs of the cancer registration increases over the time.– Increase the number of cases, sources of information, more
space, additional staff etc.

8 April,2009
Planning a Population Based Registry
• Personnel• The leadership of the coordinator is a key
for the success.• Technical Staff- Registrar.
– Training in cancer registration.– Collect data, Code, Check consistency– Software to input data.– The number of staff depends on the size of the
population coverage.– One staff to cover 1000 cases occurring annually in the
population.( Active data collection)

8 April,2009
Planning a Population Based Registry
• Personnel• Qualifications:
• Technical training and experience• Coordinator can be: Medically qualified with a background
in epidemiology, public heath or Oncology. • Consultants to advise on pathology, clinical oncology,
Epidemiology, and Statistics.• Technical staff:• Registrars responsible for cases findings, abstracting, code
with specific training course.• Data processors are needed depending on the size of the
cancer registry.

8 April,2009
Planning a Population Based Registry
• Personnel• Qualifications:
• Technical training and experience• Coordinator can be: Medically qualified with a background
in epidemiology, public heath or Oncology. • Consultants to advise on pathology, clinical oncology,
Epidemiology, and Statistics.• Technical staff:• Registrars responsible for cases findings, abstracting, code
with specific training course.• Data processors are needed depending on the size of the
cancer registry.

8 April,2009
Techniques of registration Population Surface area Latitude Year Year Cancer * % cases treated
outside registration area
% non-residents treated inside registration area
Africa
Algeria, Setif 1,365,488 6,504 35° N 1986 1986 A 60 20
Egypt, Gharbiah 3,665,524 1,943 31° N 1998 1999 A 8 10
Tunisia, Central Region 494,800 2,669 NS 1987 1989 A ~ 5 8
Case finding, abstracting and coding
Hospital in-patient recordsPublic hospital in-patient facilitiesPrivate hospital/clinic in-patient facilitiesPrivate hospital/clinic out-patient facilitiesRadiotherapy
Pathology labsHematology labs AutopsyDeath cert.
Screening programs% cases abstracted by registry personnel

8 April,2009
Classification and coding
MouthC03-C06 Malignant neoplasm of gum
Floor of mouth
Palate
Unspecified parts of mouth
C03
C04
C05
C06
Tongue Lip, Tongue
C01-C02 Malignant neoplasm of lip
Base of tongue
C00
C01
Short title Groupings Full titleSite

8 April,2009
Information recordedYes /Not
Basic Date of birth ID no
Incidence date
Ethnic group/race/colour
Stage of disease Nature of 1st treatment
Brain and nervous system
Follow-up for vital status: all/selected/none
Death certificates used to update vital status
Active follow-up of alive cases
Recoded to behaviour /3
Ca of Bladder, in situ Ca of bladder NOSBenign tumours of brain and nervous system
Borderline tumour, unc and unk behaviour of ovary Borderline tumour, unc and unk behaviour of endometrium Borderline tumour, unc and unk behaviour of brain
Ductal ca in situ of breastIntraduct ca NOS of breastLobular ca in situ of breast

8 April,2009
Planning a Population Based Registry
•Equipment and office space
• It depends of the size and activities of the cancer registry.
• Storage - secure space for case documents especially if the cancer registry is manually operating.
• If the cancer registry is connected to a sever it is necessary to do standards procedures to ensure data confidentiality.

8 April,2009

8 April,2009
CollaborationsCollaborationsOrganizations of registries
• International Association of Cancer Registries (IACR)
• European Network of Cancer Registries (ENCR)
(European Union - EU)

8 April,2009
Planning a Population Based Registry
• Conclusions
• To know the cancer incidence is should be stressed in a cancer control program
• The cancer registry is must be a continuous activity linked to cancer control and cancer research.