Embed Size (px)
Citation preview

Saving Newborn Lives Initiative
SAVING NEWBORN LIVES TOOLS FOR NEWBORN HEALTH
QUALITATIVE RESEARCH TO IMPROVE NEWBORN CARE PRACTICESRonald P. Parlato, Gary L. Darmstadt,and Anne Tinker
310496.Cover.qxd 7/9/2004 8:26 PM Page 1

All rights reserved. Publications of Saving Newborn Lives initiativeof Save the Children can be obtained from Saving Newborn Lives,Save the Children US, 2000 M Street NW, Suite 500,Washington,DC 20036 (tel: 202-293-4170; fax: 202-637-9362). Requests for permission to reproduce or translate SNL publications for non-commercial distribution should be addressed to SNL Public Affairs Department at the above address.
Save the Children does not warrant that the information con-tained in this publication is complete and correct and shall not beliable for any damages incurred as a result of its use.
Printed in the United States of America.
Editor: Robin BellEditorial and design assistance: Julia RubenCover design: Kinetik CommunicationsFront cover photo: Brian MoodyBack cover photo:Thomas Kelly
SAVING NEWBORN LIVES INITIATIVE, supported by theBill & Melinda Gates Foundation, is a global initiative to improvethe health and survival of newborns in the developing world. Sav-ing Newborn Lives works with governments, local communitiesand partner agencies in developing countries to make progresstoward real and lasting change in newborn health.
SAVE THE CHILDREN is a leading international nonprofitchild-assistance organization working in over 40 countries world-wide, including the United States. Our mission is to make lastingpositive change in the lives of children in need. Save the Childrenis a member of the international Save the Children Alliance, aworldwide network of 30 independent Save the Children organi-zations working in more than 100 countries to ensure the well-being and protect the rights of children everywhere.
© Save the Children 2004
310496.Cover.qxd 7/9/2004 8:26 PM Page 2
SAVING NEWBORN LIVES TOOLS FOR NEWBORN HEALTH
Saving Newborn Lives InitiativeWashington, DC
QUALITATIVE RESEARCH TO IMPROVE NEWBORN CARE PRACTICES
Ronald P. Parlato, Gary L. Darmstadt,and Anne Tinker
310496.Text.qxd 7/9/2004 8:29 PM Page A

B
310496.Text.qxd 7/9/2004 8:29 PM Page B

ii
Many people put their thoughts, time, and effort into the shape and content of this publication. Theauthors wish to thank Nancy Nachbar and Annette Bongiovanni of the Academy for EducationalDevelopment, who made valuable contributions to early drafts of the document. La Rue Seims ofSaving Newborn Lives, Save the Children, prepared parts of Chapter 4. Our thanks also go toClaudia Fishman of CDC, Peter Winch of Johns Hopkins University, Jose Martines of WHO, NitaBhandari of AIIMS, Alessandra Bazzano of the London School of Hygiene, and Steven Wall, DavidMarsh, Frances Ganges, Malia Boggs, and Nabeela Ali of Save the Children, all of whom helped withtheir technical review. The authors are also grateful to David Oot, Director of the Office of Health,Save the Children, for his continued support and advice. Sarah Holland, Julia Ruben, Michael Foley,and Megan Renner deserve acknowledgment for for their assistance in the preparation of the docu-ment. Finally, the authors wish to thank all SNL staff who field-tested this guide and offered timelyand useful comments throughout the development process.
Without the generousity of the Bill & Melinda Gates Foundation, Saving Newborn Lives would notbe able to adapt qualitative research tools to the urgent goal of reducing newborn deaths. Our thanksto the Gates Foundation for its support and guidance.
ACKNOWLEDGMENTS
310496.Text.qxd 7/9/2004 8:29 PM Page i

blank
310496.Text.qxd 7/9/2004 8:29 PM Page ii

iii
Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .ii
Table of Contents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .iii
How to Use this Guide . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Chapter 1: Antenatal Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11
Chapter 2: Intrapartum Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .17
Chapter 3: Postnatal Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21
Chapter 4: Research Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29
Chapter 5: Applying Data Analysis to BCC Planning and Programming . . . . . . . . . . . . . . . . . . . .33
Appendix: Qualitative Research Resources . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .40
Notes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .41
TABLES AND FIGURES
Figure 1. Essential Newborn Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Table 1. All ENC Periods: Constraints and Lines of Inquiry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6
Table 2. Antenatal Period: Lines of Inquiry about Current Practices . . . . . . . . . . . . . . . . . . . . . . .13
Table 3. Antenatal Period: Constraints and Lines of Inquiry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .15
Table 4. Intrapartum Care: Lines of Inquiry about Current Practices . . . . . . . . . . . . . . . . . . . . . .18
Table 5. Intrapartum Care: Lines of Inquiry about Constraints . . . . . . . . . . . . . . . . . . . . . . . . . . .20
Table 6. Immediate Newborn Care: Lines of Inquiry about Current Practices . . . . . . . . . . . . . . .22
Table 7. Immediate Newborn Care: Lines of Inquiry about Constraints . . . . . . . . . . . . . . . . . . . .24
Table 8. Neonatal Care: Lines of Inquiry about Current Practices . . . . . . . . . . . . . . . . . . . . . . . . .26
Table 9. Neonatal Care: Lines of Inquiry about Constraints . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .28
Table 10. Qualitative Research: Methods and Examples of Newborn Care Applications . . . . . . . .30
Table 11. Analyzing Qualitative Data and Developing a BCC Strategy . . . . . . . . . . . . . . . . . . . . . . .35
CONTENTS
310496.Text.qxd 7/9/2004 8:29 PM Page iii

blank
310496.Text.qxd 7/9/2004 8:29 PM Page iv

How to Use this Guide 1
The purpose of this guide is to provide a readyreference tool for conducting qualitative researchand planning a behavior change communicationsstrategy to improve newborn care practices. Inthis guide, we label this research ‘qualitative,’ butit is important to note that the term ‘formative’can be used to describe it as well. The guide hasbeen designed with the understanding that thequalitative research and analysis could be carriedout by subcontracted technical agencies or indi-viduals who would supply the information toprogram managers. The program manager willnot design, develop, or execute field studies, butrather will provide terms of reference andinformed technical supervision and manage-ment.
No matter how well-qualified, the researcher maybe new to the subjects of Essential NewbornCare (ENC) and Behavior Change Communication(BCC). In this regard, this guide will help orientthe program manager and the researcher to thesetechnical areas and help to ensure that theresearch remains focused to generate informationthat will inform the design of BCC programs.
This guide provides:
• Evidence-based practices that have beenshown to have the most significant and directimplications for newborn health, mortalityand morbidity.1 These are the target practicesfrom which to choose while designing thequalitative research. It is strongly recom-mended that only practices from this list beselected to ensure consistency and maintain afocus on evidence-based practices.
• Methods to identify the current practices oflocal communities and lists of constraints—informational, social, cultural, economic, or
supply factors shown in prior qualitativeresearch studies to limit or discourage theadoption of evidence-based ENC practices.This guide also provides sample lines ofinquiry that correspond to each currentpractice and constraint. These lines ofinquiry are designed to suggest where andhow to look for answers; however, they willneed to be adapted for direct use in qualita-tive research questionnaires.
• Guidelines for identifying target audiencesand assessing the decision-makingprocesses of their members. This caninclude assessing family decision-making.This can also include eliciting informationabout those members of the community,other than the extended family, who areinfluential in ENC decision-making—such astraditional practitioners and facility-basedhealth workers. Not only is it important toidentify who is exerting influence overimportant ENC decisions, but it is alsoimperative to understand the beliefs of thoseinfluential individuals themselves.
• Procedures involved in qualitative researchmethods, such as in-depth interviews andfocus group discussions.
• Practical guidance on how to move to the nextsteps after qualitative research—the all-impor-tant phases of data analysis and BCC plan-ning and programming.
Introduction to Chapter Structure
Each of the ENC chapters (Chapters 1 – 3) ofthe guide includes matrices (Tables 1-9) present-ing comprehensive lines of inquiry for both cur-rent practices and constraints.
HOW TO USE THIS GUIDE
310496.Text.qxd 7/9/2004 8:29 PM Page 1

2 Qualitative Research to Improve Newborn Care Practices
Each of these chapters is divided into the follow-ing sections:
1. Presentation of evidence-based ENC practicesand sub-practices and a discussion of theirimportance, answering the question: “Whatproven, evidence-based interventions lead tolower neonatal mortality and morbidity?”
2. Presentation of lines of inquiry to determinecurrent ENC practices, answering the ques-tions: “What are the current practices, and towhat degree or under what circumstancesmight they be changed?”
3. Presentation of lines of inquiry to determinethose constraints pertaining to each evidence-based practice, answering the question:“What factors inhibit or discourage people’sability and willingness to practice evidence-based ENC?”
These chapters address the three temporal peri-ods of care: antenatal, intrapartum, and postna-tal. Within each period there are major evidence-based practices and sub-practices, and for each ofthese there may be a variety of informational,social, cultural, economic, and supply constraintsthat limit or discourage behavior change.
Nevertheless, it is unlikely that program man-agers will have to deal with all practices or allquestions.
Various factors might allow the researcher tofocus and simplify inquiries:
• In some cases, a particular evidence-basedpractice is already common in the country. InMalawi, for example, antenatal care is alreadyunderstood and practiced. Similarly, in manyareas of Bangladesh, exclusive breastfeedingis the norm rather than the exception. Underthese circumstances there is no need foradditional research, for these practices willprobably not require further attention.
• Another consideration is whether otheragencies are already addressing certain ENCpractices. Another international organization,for example, may be implementing or haverecently implemented a program to promotebetter maternal nutrition, exclusive breast-feeding, or tetanus toxoid immunization,thus obviating the need for additionalresearch or programming.
• In other cases, although no current or priorprograms exist, there may be a sufficientbody of existing knowledge on the subject.Others may have done exploratory researchthat is sufficient to form the basis for BCCplanning in particular subject areas. In SNLfocus countries, for instance, the baselinesurvey may supply enough relevant informa-tion to reduce the need for further invest-ment in certain qualitative research topics.
310496.Text.qxd 7/9/2004 8:29 PM Page 2
Introduction 3
Newborn mortality is one of the world’s mostneglected health problems. It is estimated thatglobally, four million newborns die before theyreach one month of age and another four mil-lion are stillborn each year. Deaths during theneonatal period (the first 28 days of life) accountfor almost two-thirds of all deaths in the first yearof life and 40 percent of deaths before the ageof five.
Most of these deaths could be preventedthrough proven, cost-effective interventions,such as tetanus toxoid immunization or exclusivebreastfeeding. The Saving Newborn Lives (SNL)initiative is designed to reduce neonatal mortalityand morbidity by strengthening and expandingthese and other interventions in Africa, Asia, andLatin America.
Behavior Change Communications (BCC) isa process that provides timely, relevant, anduseful information to local communitiesthat can be used to encourage families toimprove newborn care practices. Successfulbehavior change requires a thorough under-standing of the target audience. Qualitativeresearch provides essential informationabout what could motivate this audience toimprove its newborn care practices.
This guide is intended to discuss behaviorchange within the context of EssentialNewborn Care (ENC) and to provide guide-lines on how to plan, manage, and use qual-itative research and design a BCC strategy.
Essential Newborn Care Practices
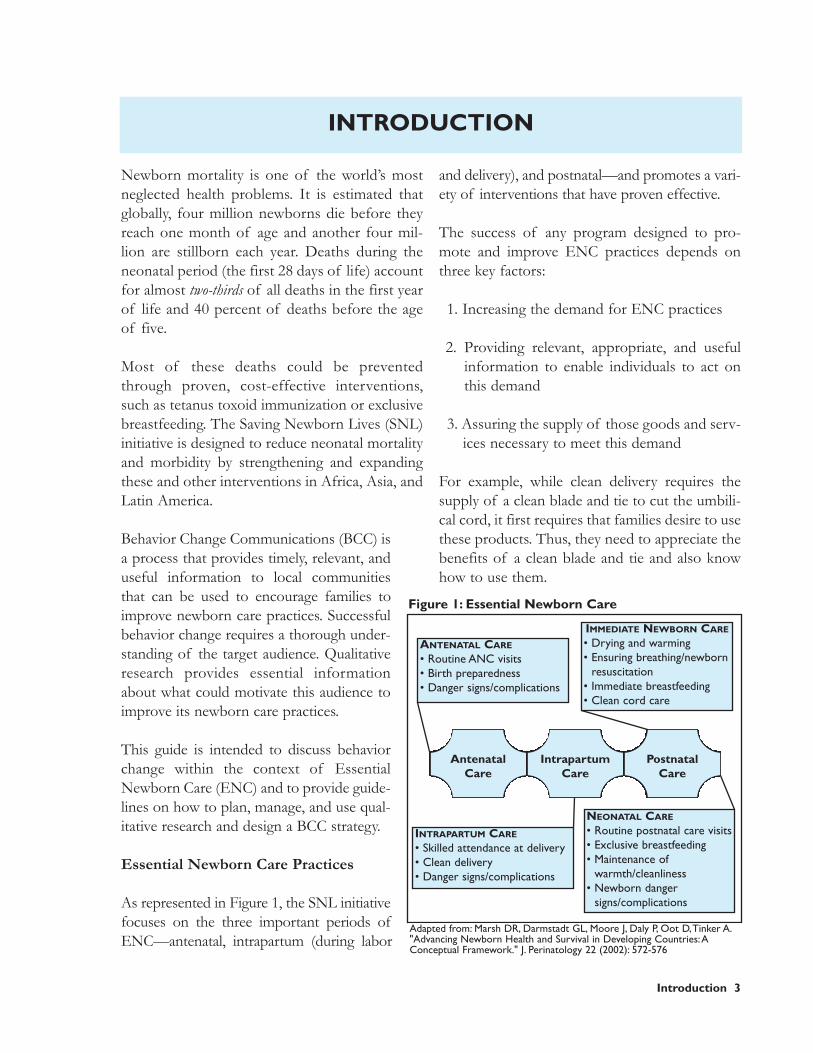
As represented in Figure 1, the SNL initiativefocuses on the three important periods ofENC—antenatal, intrapartum (during labor
and delivery), and postnatal—and promotes a vari-ety of interventions that have proven effective.
The success of any program designed to pro-mote and improve ENC practices depends onthree key factors:
1. Increasing the demand for ENC practices
2. Providing relevant, appropriate, and usefulinformation to enable individuals to act onthis demand
3. Assuring the supply of those goods and serv-ices necessary to meet this demand
For example, while clean delivery requires thesupply of a clean blade and tie to cut the umbili-cal cord, it first requires that families desire to usethese products. Thus, they need to appreciate thebenefits of a clean blade and tie and also knowhow to use them.
Adapted from: Marsh DR, Darmstadt GL, Moore J, Daly P, Oot D,Tinker A."Advancing Newborn Health and Survival in Developing Countries:AConceptual Framework." J. Perinatology 22 (2002): 572-576
Figure 1: Essential Newborn Care
INTRODUCTION
ANTENATAL CARE
• Routine ANC visits• Birth preparedness• Danger signs/complications
IMMEDIATE NEWBORN CARE
• Drying and warming• Ensuring breathing/newborn
resuscitation• Immediate breastfeeding• Clean cord care
INTRAPARTUM CARE
• Skilled attendance at delivery• Clean delivery• Danger signs/complications
NEONATAL CARE
• Routine postnatal care visits• Exclusive breastfeeding• Maintenance of
warmth/cleanliness• Newborn danger
signs/complications
AntenatalCare
IntrapartumCare
PostnatalCare
310496.Text.qxd 7/9/2004 8:29 PM Page 3

4 Qualitative Research to Improve Newborn Care Practices
Similarly, while birth preparedness requires iden-tifying available transportation and upgradedreferral facilities, it also requires a demand forthese services as well as the ability to pay forthem. On the informational side, families mustfirst be able to recognize danger signs and com-plications, be confident that referral care will helpensure the survival of mother and newborn, andbe motivated to act on this knowledge.
Some practices, such as immediate and exclusivebreastfeeding or drying and warming the new-born, require little in the way of supplies orproducts, but a great deal in the way of convic-tion. A new mother and her family must under-stand the value of immediate and exclusivebreastfeeding, must value it enough to give upthe traditional feeding habits for newborns andinfants, and must be convinced that regardless ofthe practices of other women and their families,this practice will be beneficial for their child.
Promoting evidence-based practices for new-born caregivers and modifying practices that areharmful will improve newborn health and reducemortality and morbidity. However, for numerousreasons, demand for evidence-based newborncare practices is often quite low. First, many fam-ilies do not receive the information required tounderstand the relationship between improvedpractices and better health outcomes. Second,the presentation of this information may nottake into account existing social, cultural, andeconomic constraints to behavior change. Third,well-established and traditional newborn carepractices may be strongly reinforced by familyand community structures that tend to favorthem over innovation.
Economic constraints are perhaps the most sig-nificant of these barriers to demand for healthservices. Cost—whether a simple lack of fundsor opportunity cost—is a formidable deterrentto behavior change.2
Social, cultural, and economic constraints are notinsurmountable barriers to change. Under-standing them can assist communications plan-ners to customize the crafting of messages andmedia. In reality, improvements in newborn carepractices have been seen throughout the world.Immediate and exclusive breastfeeding rates haveincreased dramatically in many countries due tosuccessful BCC programs. Social mobilizationcampaigns have increased demand for tetanustoxoid coverage and thus reduced the incidenceof death from a disease for which prevention isabsolutely paramount. BCC initiatives have beenequally successful in increasing rates of antenatalcare and skilled care at birth.
Qualitative Research
Qualitative research offers specialized techniquesfor obtaining and understanding in-depth infor-mation about what people know, think, and do.Qualitative research analyzes social patterns andtraditions that influence decision-making. It con-siders cultural beliefs and convictions that give areligious and philosophical significance to new-born care. It looks at economic constraints thatlimit the ability of families and communities topractice positive behaviors even when they mayhave the knowledge and conviction to do so.
Qualitative research, however, is not merelydescriptive; it is practical, useful, and dynamic. Itinvestigates not only why people do what theydo, but more importantly, what can help them tochange. It provides the BCC planner with ade-quate information to identify the most effectiveentry point for behavior change negotiation, andthe most acceptable and feasible degree ofchange within existing constraints.
An example of how qualitative research data canbe used to design appropriate and persuasivemessages comes from the Hausa population inrural Nigeria. Qualitative research showed thatimmediately after birth, families commonly give
310496.Text.qxd 7/9/2004 8:29 PM Page 4

Introduction 5
newborns water that has been poured over paperon which verses from the Koran have beeninscribed—a practice rooted in a centuries-oldtradition. According to Hausa beliefs, this prac-tice provides the vulnerable newborn the protec-tion of Allah. At the same time, the Hausabelieve that breast milk is good for the newbornand that through drinking breast milk, the new-born eats and drinks what the mother does. ABCC campaign promoting exclusive breastfeed-ing among the Hausa combined these two beliefsinto a communication strategy. If the motherdrinks Koranic verses, it was argued, the benefitswould pass on to the newborn through her breastmilk. Respecting both medical judgment (avoid-ing giving water to the newborn) and the local tra-ditions and beliefs of the Hausa population, thecampaign was a success.
In this case and many others, qualitative researchhas provided BCC planners with the client-baseddata on which to ground the development ofcommunication strategies—suggesting creativeapproaches to balancing demands of a tradition-al society with the value of modern health con-cepts. In short, qualitative research leads to anunderstanding of what people are currentlydoing, why they are doing it, what changes mightbe feasible within the context of existing con-straints, and how communicators might effec-tively address these changes.
At the same time, qualitative research can helpthe BCC planner rule out those ENC practicesthat might not be the most practical or viable pri-orities. Changing certain practices may simplyrepresent too great a social, cultural, or econom-ic risk to justify an investment of limited BCCresources. The practice of ritual prelacteal feeds, forexample, is common in many parts of theworld—often tied to long-standing cultural tradi-tion, social practice, or religious belief.3 Althoughthe Hausa were generally open to modifying theirpractice in favor of exclusive breastfeeding, othercommunities might consider discontinuing their
practice as a major breach in tradition. Prelactealfeeds often fulfill important sociocultural func-tions—uniting families, reaffirming family roles,sanctifying the life of the newborn, and demon-strating religious respect and homage. It mayonly be possible to modify the practice gradually,over the longer term. In general, the potentialhealth impact of a behavior change should beassessed in relation to its feasibility and socialacceptability—a judgment best made with theparticipation of the target community.
Qualitative research, then, can provide answersto the following questions:
• Which practices are likely to remain unchangeddespite even the best BCC programs?
• Which practices have the fewest social, eco-nomic, or cultural constraints and thus aremost amenable to change and most likely tolead to improved health outcomes?
• Which practices are amenable to change, butmay not significantly impact health status andthus may not be valuable, cost-effective tar-gets for BCC programs?
• For practices that appear amenable to changeand are known to have a significant impacton health, what might convince families toimprove them?
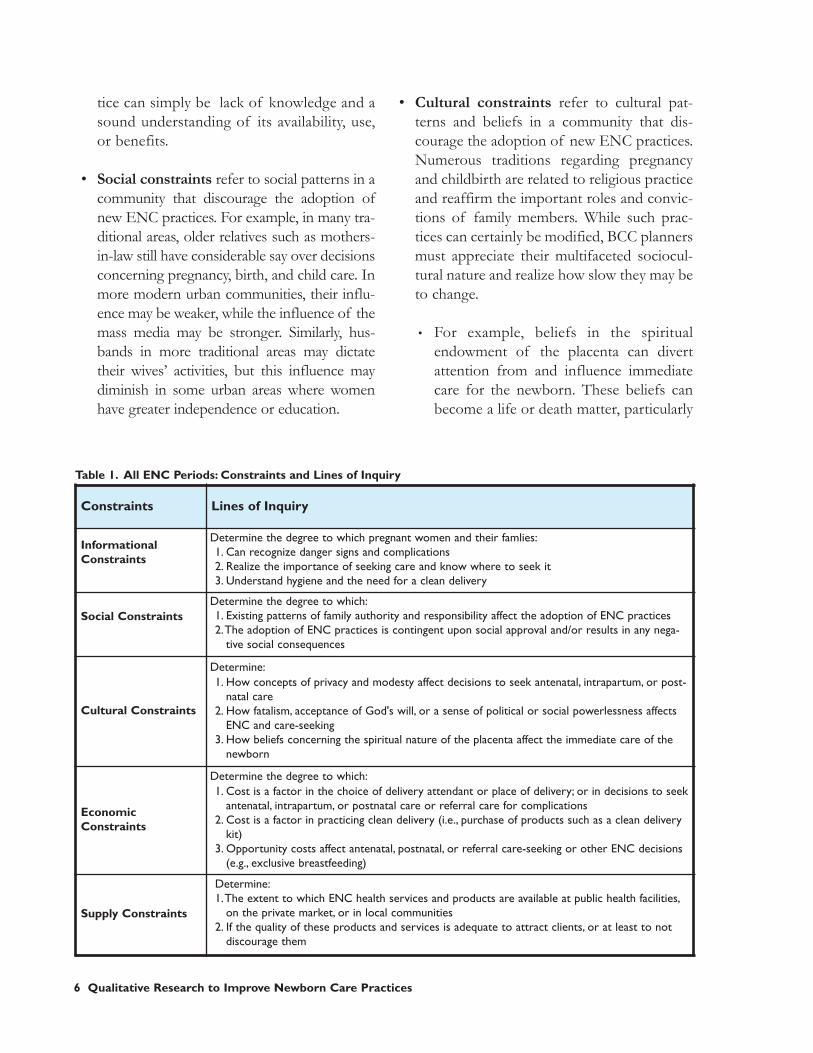
Constraints4
A constraint is defined as any factor that limitsbehavior change. Several types of constraints aredetailed below:
• Informational constraints refer to theclient’s lack of information regarding cur-rent or recommended ENC practices andtheir health outcomes. That is, aside fromsocial, cultural, and economic constraints, amajor reason for not adopting a new prac-
310496.Text.qxd 7/9/2004 8:29 PM Page 5
6 Qualitative Research to Improve Newborn Care Practices
tice can simply be lack of knowledge and asound understanding of its availability, use,or benefits.
• Social constraints refer to social patterns in acommunity that discourage the adoption ofnew ENC practices. For example, in many tra-ditional areas, older relatives such as mothers-in-law still have considerable say over decisionsconcerning pregnancy, birth, and child care. Inmore modern urban communities, their influ-ence may be weaker, while the influence of themass media may be stronger. Similarly, hus-bands in more traditional areas may dictatetheir wives’ activities, but this influence maydiminish in some urban areas where womenhave greater independence or education.
• Cultural constraints refer to cultural pat-terns and beliefs in a community that dis-courage the adoption of new ENC practices.Numerous traditions regarding pregnancyand childbirth are related to religious practiceand reaffirm the important roles and convic-tions of family members. While such prac-tices can certainly be modified, BCC plannersmust appreciate their multifaceted sociocul-tural nature and realize how slow they may beto change.
• For example, beliefs in the spiritualendowment of the placenta can divertattention from and influence immediatecare for the newborn. These beliefs canbecome a life or death matter, particularly
Constraints Lines of Inquiry
InformationalConstraints
Determine the degree to which pregnant women and their famlies:1. Can recognize danger signs and complications2. Realize the importance of seeking care and know where to seek it3. Understand hygiene and the need for a clean delivery
Social ConstraintsDetermine the degree to which:1. Existing patterns of family authority and responsibility affect the adoption of ENC practices2.The adoption of ENC practices is contingent upon social approval and/or results in any nega-
tive social consequences
Cultural Constraints
Determine:1. How concepts of privacy and modesty affect decisions to seek antenatal, intrapartum, or post-
natal care2. How fatalism, acceptance of God's will, or a sense of political or social powerlessness affects
ENC and care-seeking3. How beliefs concerning the spiritual nature of the placenta affect the immediate care of the
newborn
EconomicConstraints
Determine the degree to which:1. Cost is a factor in the choice of delivery attendant or place of delivery; or in decisions to seek
antenatal, intrapartum, or postnatal care or referral care for complications2. Cost is a factor in practicing clean delivery (i.e., purchase of products such as a clean delivery
kit)3. Opportunity costs affect antenatal, postnatal, or referral care-seeking or other ENC decisions
(e.g., exclusive breastfeeding)
Supply Constraints
Determine:1.The extent to which ENC health services and products are available at public health facilities,
on the private market, or in local communities2. If the quality of these products and services is adequate to attract clients, or at least to not
discourage them
Table 1. All ENC Periods: Constraints and Lines of Inquiry
310496.Text.qxd 7/9/2004 8:29 PM Page 6

Introduction 7
in the first critical moments after birthwhen the newborn’s risk of asphyxia andhypothermia are greatest.
• Concepts of ‘hot’ and ‘cold’ are oftenrelated less to temperature than philo-sophical systems. Similarly, attitudestoward hygiene and cleanliness are oftenmore a function of environmental realitythan lack of understanding. The conceptof hygiene in a community without run-ning water, sanitation, fly screens, dustcovers, etc., is quite different from that incommunities with the resources to exer-cise such protective measures.
• Economic constraints refer to either unavail-ability of cash or credit to pay for ENCgoods and services, or opportunity cost situ-ations wherein the adoption of a new ENCpractice reduces productivity in other areas.
Lines of Inquiry
Lines of inquiry are simply guidelines for theresearcher—not questions to be inserted into aqualitative research questionnaire. They areintended to suggest areas of investigation thatprevious research efforts have found productive.For example, although there may be only one lineof inquiry in the matrix that concerns hygieneand cleanliness (see Table 1), a field investigatorwould be expected to ask a number of questionsabout the issue and would need to probe further:What is the current concept of cleanliness? Howis it affected by environmental conditions? Is theconcept of antisepsis understood?
All lines of inquiry indicated in this guide are evi-dence-based. That is, research has shown theycan elicit information about behavior, knowl-edge, attitudes, and beliefs that are relevant toENC behavior change. Table 1 includes an amal-gam of many constraints and lines of inquiry forall ENC periods.
Progressive Behavior Change
Perhaps the most important aspect of qualitativeresearch is the concept of progressive change.That is, given the constraints that make behaviorchange difficult, to what degree and under whatcircumstances might individuals change?
For example, a family may be severely limitedfinancially and living on the margin in terms ofeconomic productivity. If, as a result, the familyis unable to spare the time or resources for apregnant woman to make the four prescribedantenatal care visits, encouraging her to attendat least one or two visits may be a viable short-term alternative.
Qualitative researchers need to evaluate whetherthe existing constraints are so severe that changeis not possible, or more commonly, whetherincremental, progressive change may be morefeasible. The question repeated many timesthroughout this guide—“To what degree andunder what circumstances might current prac-tices be changed?”—goes to the heart of thisissue, and should be explored for each line ofinquiry presented in the various matrices.
For example, if a pregnant woman states thatafter her last delivery she had not breastfed exclu-sively, the researcher would pose the question,“What would make it easier for you to adopt thispractice?” before asking more probing questions,such as, “Do you think you could at least not givewater to your newborn?” or “Would you consid-er increasing the number of times you breastfeedin a day?” In short, lines of inquiry should leadto deeper, core questions regarding ability andwillingness to change.
Behavioral trials, conducted with members of atarget audience in their own community, are par-ticularly effective for assessing the feasibility ofadopting new practices. As extensions of thequalitative research process, behavioral trials
310496.Text.qxd 7/9/2004 8:29 PM Page 7

negotiate possible changes with families (previ-ously identified through in-depth interviews,group discussions, focus groups, etc.) in a real lifesetting. This process can help validate theassumptions made from qualitative research andin the strategic planning process.
In one study in Bangladesh, qualitative researchdetermined that bathing the newborn on the firstday of life was almost universal. This practicewas based on the conviction that an infant isborn unclean and therefore must be cleansedbefore being handled. This perceived “uncleanli-ness” has more to do with ritual, tradition, andceremony than with practical, common desires tocleanse the newborn of blood and afterbirth.BCC planners wondered whether families mightcompromise between current practice and nobathing at all. In a series of behavioral trials usinga doll to simulate possible practices, the plannersidentified a set of new practices that were closerto the ideal and acceptable to trial families. Oneof the most successful compromise practices wasgiving a brief sponge bath with warm water, in awarmed room, followed by immediate dryingand wrapping with clean, dry cloths.
Target Audiences
In addition to addressing factors that determinebehavior, qualitative research is also essential foridentifying those individuals who exert the great-est influence on newborn care decisions becausemothers rarely make these decisions on theirown. Although mothers-in-law and husbands areoften cited as the key influentials in ENC familydecision-making, their influence varies accordingto local practice, and they are not the sole sourceof authority.
For example, husbands often have the strongestinfluence on economic decisions regarding bothfinancial outlay (e.g., funds for emergency trans-port, purchase of clean delivery equipment) andopportunity cost. A husband, who may be
required by social custom to accompany his wifeon trips outside the family compound or com-munity (e.g., to the health center for ANC), maybe unwilling to give up what he considers to bemore productive labor time.
Traditional healers are another common influ-ence. Though losing authority and respect insome communities as modern media and ideasmake inroads, they remain powerful and influen-tial in more isolated communities.
Overall, an accurate identification of key influen-tials in a community is best made on the basis ofqualitative research.
Research Methods
Qualitative research is usually conducted usingstandard methodological tools. The two mostcommon are in-depth interviews and focusgroups.
These and other useful methodological tools forqualitative research are discussed in some detailin Chapter 4.
Strategic Planning
An understanding of the informational, social,cultural, and economic constraints that deter-mine family and community behavior opensthe door to communicating with target popu-lations. Research data are valued most whenthey are used to guide the BCC planner in thedevelopment of BCC campaigns using elec-tronic, print, and other mass media, and/orinterpersonal communication.
As mentioned above, qualitative research canenable the BCC planner to select priority prac-tices—those leading to the greatest improve-ments in newborn health and survival and whichare amenable to change. As evident in Figure 1(page 3), several ENC practices are recommend-
8 Qualitative Research to Improve Newborn Care Practices
310496.Text.qxd 7/9/2004 8:29 PM Page 8

Introduction 9
ed, and each one of these practices can be brokendown into sub-practices. For example, interven-tions to promote breastfeeding include: a)encouraging a mother to put her newborn to thebreast immediately, b) encouraging her to avoidprelacteal or interlacteal feeds, c) encouraging herto feed colostrum, d) helping her to appropriate-ly position the infant at the breast, and e) encour-aging her to continue feeding exclusively through-out the first six months of her infant’s life.
Based on the data generated from clients, a BCCplanner can make critical decisions concerningwhich of the major ENC practices and sub-prac-tices should be considered the highest priorities.
Qualitative research can also enable the BCCplanner to determine the appropriate communi-cation strategy for each selected priority practice.If drying and warming are selected as prioritypractices, how should one work with the commu-nity to promote these practices? To what beliefs,expectations, and hopes should one appeal?Some communities, such as those in the alti-plano of Bolivia, already warm a room before
birth. That is, they understand the importanceof receiving a newborn in a warm environment.A possible communication strategy to promotedrying, wrapping, or skin-to-skin contact mightbegin with ambient temperature and the con-cept of warmth as they experience it as adults,and then advance to more thorough practicesfor their newborns.
Qualitative research data can be used to identifyspecific target audiences: influential members ofthe family and community, newborn caregiversand health providers, and pregnant womenthemselves. Importantly, qualitative researchcan help program managers design informationand media specifically tailored to these audi-ences, given their particular roles and responsi-bilities within the family and community. Thestrategies noted above are provided as examplesto illustrate how qualitative research data can betransformed into a BCC strategy. These andother issues relating to the application of quali-tative research data are explored in some depthin Chapter 5.
310496.Text.qxd 7/9/2004 8:29 PM Page 9

blank
310496.Text.qxd 7/9/2004 8:29 PM Page 10
1.1 What proven, evidence-basedinterventions lead to lower neona-tal mortality and morbidity?
Routine ANC visits: Antenatal care is impor-tant, not only for the clinical appraisal of preg-nancy and remedial clinical interventions per-formed by trained professionals, but also for thecounseling and educational services provided forthe benefit of both mother and newborn.Ensuring proper tetanus toxoid immunization,educating women on the danger signs and com-plications of pregnancy, and preparing them forimmediate, exclusive breastfeeding are particular-ly important. Although their significance variesgeographically, maternal malnutrition, malaria,and reproductive tract infections may adverselyaffect newborn health outcomes;5 thus theyshould also be addressed in the context of ANC.Professional counseling by trained staff (and insome cases, trained peer counselors) regarding
issues such as nutrition, hygiene, family plan-ning, preparation for breastfeeding, child devel-opment, minor discomfort during pregnancy,and danger signs and complications, can also bean effective method for encouraging healthyhousehold practices.
The World Health Organization (WHO) recom-mends at least four ANC visits. However, it is notonly the number of ANC visits that is important;the quality of service and counseling received iseven more important. As mentioned previouslyin the introduction, both demand and supplymust be assured.
Recognition of danger signs and complica-tions of pregnancy: Regardless of whether awoman seeks ANC, it is important that she, herfamily, and her health providers know when,how, and where to seek care from an appropri-ately skilled professional. Below is a list of pri-ority danger signs and complications duringpregnancy of which everyone should be aware:
• Vaginal bleeding• Convulsions (fits)• Loss of consciousness• Severe headaches with or without dizziness• Fever• Difficulty breathing (especially with dizziness
and/or very pale skin)• Contractions/labor pains or water breaking
before 37 weeks gestation
If the mother experiences any of the above,she should know to seek professional careimmediately, day or night, as these signs couldindicate a life-threatening condition for herand/or the fetus.
Antenatal Care 11
CHAPTER 1: ANTENATAL CARE
EVIDENCE-BASED PRACTICES
1. Pregnant women should make at leastfour ANC visits to a health providertrained in midwifery skills.
2. Pregnant women and their families, aswell as health providers, should be ableto recognize danger signs and compli-cations of pregnancy, and knowwhen/how to seek appropriate referralcare if needed.
3. Pregnant women, families, and commu-nities should prepare for birth, includ-ing their responses to potential mater-nal and newborn emergencies.
310496.Text.qxd 7/9/2004 8:29 PM Page 11

12 Qualitative Research to Improve Newborn Care Practices
The mother should also be aware of less seri-ous danger signs that require consultation assoon as possible:
• Pale skin• Cloudy urine• Foul smelling vaginal discharge• Swelling of the face, hands, feet, or legs
Birth preparedness: The third important ante-natal practice for a pregnant woman, her family,and her community is preparation for the birthand any potential referral care needs. Birth pre-paredness may affect newborn survival by ensur-ing that in the event of serious danger signs andcomplications, not only will they be recognized,but the mother and newborn will be able to reachan appropriate medical facility in a timely fash-ion, and the family will be able to access andafford quality emergency care. Thus, “preparing”for birth consists of several practices:
• Selecting a skilled birth attendant6• Selecting a health facility to go to if the moth-
er or newborn experience complications• Identifying and assuring emergency trans-
portation to a health facility• Setting aside sufficient money to pay for
emergency transportation and medical care
1.2 What are the current prac-tices, and to what degree or underwhat circumstances might they bechanged?
Identifying current newborn care practices is thefirst step in preparing a foundation for the designand development of a BCC program. Under-standing the degree to which women and theirfamilies would be willing to accept new practicesand change their current behavior—that is, whatchanges they would make and under what condi-tions they would make them—is essential to craft-ing realistic, relevant behavior change messages.
Qualitative research should first investigate prac-tices currently performed during pregnancy rela-tive to the evidence-based practices listed above:Do women go for ANC? When and how fre-quently? What is the content of these visits? Canthey and their families recognize danger signsand complications during pregnancy? Do fami-lies adequately prepare for birth and anticipatethe possibility of an emergency?
Recognizing danger signs and complications canbe a problematic line of inquiry for the qualita-tive researcher, due to the subjective nature ofmany symptoms. For example, in communitieswhere diarrhea, malaria, or upper respiratoryinfections are common and frequent, a fever maybe overlooked or disregarded and its significanceinaccurately gauged. Difficulty breathing is alsosubject to local interpretation, particularly in thepreterm infant or in the presence of frequentrespiratory infections or environmental pollutionand dust. Therefore, it is important not only tofind out what people claim to know and recog-nize, but also to ascertain the depth and accuracyof their knowledge. Identifying and using thelocal terms for commonly recognized dangersigns can also be essential for eliciting andrecording accurate responses.
The second step for qualitative research shouldbe to determine what it would take for families toadopt more positive behaviors—how and towhat degree could the current practices be mod-ified? Based on an understanding of the informa-tional, social, cultural, economic, and supply con-straints, good researchers may be able to inferwhat changes are feasible. However, it is only byprobing prospective behavior that one can deter-mine the real degree of change that might beacceptable and achievable.
For example, if a woman states that she does notseek ANC because of economic constraints, shemight reconsider attending just one antenatal
310496.Text.qxd 7/9/2004 8:29 PM Page 12

Antenatal Care 13
visit instead of four. Similarly, another womanmight be unwilling to seek ANC more than oncebecause of cost, but she might agree if the visitcould be made at home. She might also agree topay for ANC visits if she perceived the quality ofservice to be better. Overall, although familiesmay not be willing or able to take all recommend-ed birth preparedness measures, they might bewilling to take some of them. An understanding ofthe positive potential for progressive behaviorchange, in addition to an understanding of thenegative constraints on behavior change, isessential to the crafting of effective BCC strate-gies and messages.
Table 2 lists priority practices of the antenatalperiod and several corresponding lines of inquirythat researchers may want to address to deter-mine the current level of compliance with evi-dence-based practices.
1.3 What factors limit or discour-age people’s ability and willingnessto practice evidence-based ENC?
There are four major categories of demandconstraints that affect ability and willingness tomove from existing newborn care practices tothe evidence-based ENC practices recom-mended by SNL:
• Informational constraints: a simple lack ofinformation, knowledge, or experience need-ed to make informed ENC choices
• Social constraints: patterns of family andcommunity authority, roles, and responsibilities
• Cultural constraints: religious beliefs or tra-ditional rituals and other practices
Current Practices Lines of Inquiry
Routine ANC Visits
Determine:1.Whether pregnant women currently receive any ANC2. If they do, where and from whom they receive it3.The timing and frequency of these visits4.The procedures performed and counseling provided during these visits5.What would facilitate an increased number of visits
Recognition of DangerSigns and Complications ofPregnancy
Determine:1.When respondents feel that mother or newborn are in danger during pregnancy, and the
local terms for these symptoms of illness2.What their responses would be to these symptoms3.The health provider or facility to which they would go to seek care for these symptoms4.Which danger signs/complications are generally perceived or recognized as such; and
which ones are not recognized, misperceived, or misinterpreted
Birth Preparedness
Determine if pregnant women and their families:1. Select a skilled birth attendant to assist at delivery2. Prepare for emergencies that might occur during pregnancy, labor, or delivery3. Identify a particular health facility to go to in case of an emergency4. Identify emergency transportation5. Set aside funds for emergency care and transportation6.What would facilitate 2-5, above
Determine:1. If there is a community fund for use in maternal or newborn emergences2. If so, how families gain access to this fund
Table 2. Antenatal Period: Lines of Inquiry about Current Practices
310496.Text.qxd 7/9/2004 8:29 PM Page 13

14 Qualitative Research to Improve Newborn Care Practices
• Economic constraints: deficiency of indi-vidual, family, or community resources,translating into lack of access to healthgoods and services
Some of the issues meriting particular attentionin the antenatal period include:
ANC visits and economic constraints:Although the concept of financial cost will beeasily understandable to families and field inter-viewers, the concept of opportunity cost may notbe. In fact, it is likely to be far greater than anycash outlay. Field investigators must be aware ofthis factor and probe for relevance. Male familymembers, for example, may not wish to accom-pany their wives to the clinic simply because theydo not feel they can lose a valuable morning orday of work.
Knowledge and understanding of dangersigns and complications: Assessing familymembers’ knowledge on this topic is not astraightforward task. It is complicated by the sub-jectivity of many of the symptoms—includingtheir context—and the various local terms usedto describe them. Bleeding, for example, may beconsidered natural and normal during pregnancy,as some spotting is quite common. Similarly, theexpression “difficulty breathing” may simply beapplied to a bad cold or congestion during a verydusty, windy time of year. Therefore, interview-ers must be trained to probe carefully to ensure
that local terms are identified, the local context isunderstood, and the respondents answer as clear-ly as possible. Interviewers should determine onlywhether people’s knowledge conforms to the clin-ical definitions used by the researcher. Finally, it isimportant to explore prospective responses tosymptoms; specifically, from whom and underwhat circumstances help is sought.
Birth preparedness: While health professionalsunderstand implicitly the need for emergencypreparation, many local residents may not appre-ciate its importance. This is due not only to infor-mational constraints, but also to cultural percep-tions of risk, destiny, or fate, and economic per-ceptions of power. That is, the cost of preparingfor an emergency for middle class urban familiesmay be considered relatively small compared withthe benefits. This is not likely to be true for poorrural families living on the economic margins.Similarly, middle class urban audiences may havegained a certain confidence in public and privatehealth facilities, believing that they can in factimprove health outcomes, while poorer familiesmay believe that they are better off caring for themother and newborn at home. In short, while theconcept of birth preparedness seems simple andstraightforward, current practices may be inti-mately linked to subtle informational, social, cul-tural, and economic factors.
Table 3 provides lines of inquiry that have provenfruitful in research on antenatal care practices.
310496.Text.qxd 7/9/2004 8:29 PM Page 14

Antenatal Care 15
Consraints Lines of Inquiry
Informational Constraints
Determine whether pregnant women and their families:1. Know the benefits of seeking ANC2. Understand the importance of attending ANC more than once3. Understand the importance of proper home care during pregnancy4. Understand the importance of preparing for a maternal or newborn emergency5. Understand the relationship between danger signs and complications during
pregnancy and maternal and neonatal mortality and morbidity6. Understand the relationship between proper care during pregnancy and positive
birth outcomes
Social and CulturalConstraints
Determine:1.The necessity of having an accompanying male relative2. Privacy or modesty concerns about disrobing in the presence of a health
provider3. Other religious or cultural rituals or beliefs 4. Perceptions of service quality
Economic Constraints
Determine if cost is a factor in:1. Selection of health providers2.ANC attendance3. Setting aside of emergency funds for transportation and care
Transportation ConstraintsDetermine if the availability of transportation affects ANC attendance or emer-gency care planning
Time Constraints Determine how other obligations (e.g., work, childcare) affect ANC attendance.
Influence of Decision-Makers
Determine:1.The most influential family or community members for each major antenatal
practice2.Whether their influence is positive or negative (i.e., how or to what extent the
influential party encourages or discourages evidence-based practices)3.What influence pregnant women have, if any, over decisions concerning care dur-
ing pregnancy
Table 3. Antenatal Period: Lines of Inquiry about Constraints
310496.Text.qxd 7/9/2004 8:29 PM Page 15

blank
310496.Text.qxd 7/9/2004 8:29 PM Page 16
Intrapartum Care 17
2.1 What proven, evidence-basedinterventions lead to lower neona-tal mortality and morbidity?
Skilled attendance at delivery: The impor-tance of this aspect of intrapartum care has beenwell documented historically. However, at pres-ent only about half of all women in developingcountries deliver with a skilled attendant. Whena skilled attendant is not yet available, trainedcommunity-based birth attendants can helpimprove newborn health and survival.Incorporating community-based health providersin maternal and neonatal health programs shouldbe accompanied by strengthening the links alongthe household to the hospital continuum of care,including a long-term plan for training and pro-viding sufficient skilled attendants. All SNL pro-grams focus on strengthening the midwiferyskills of birth attendants, whether at health facil-ities or in the community, to provide counseling,conduct clean and safe deliveries, recognize dan-ger signs, take appropriate action to help bothmother and newborn survive, and refer compli-cated cases to a higher level of care as needed.
Recognition of danger signs and complica-tions of labor and delivery: As with antena-tal care, the second aspect of intrapartum carecritical to the survival and well-being of moth-er and newborn is the ability to recognize whento seek referral or emergency care from anappropriately trained professional. Below is alist of priority danger signs and complicationsof the intrapartum period of which everyoneshould be aware:
• Bleeding• Convulsions (fits)• Loss of consciousness• Prolonged labor >12 hours• Preterm labor• Prolapsed cord or noncephalic presenting part• Meconium discharge during labor• Fever
Because a woman in labor may not be able toassess her own risk, it is important that the birthattendant immediately recognize and appropri-ately manage or arrange referral care for dangersigns and complications. Therefore, qualitativeresearch should be designed to assess the knowl-edge and understanding of mothers, their fami-lies, and birth attendants.
The birth preparations recommended in theantenatal period (identifying a referral facility,securing emergency transport, and setting asideemergency funds) play their most critical role inthe intrapartum period. These measures canexpedite transfer of the mother and newborn inan emergency, thereby saving lives.
Clean delivery: Newborns are also more likelyto survive if the delivery is clean—that is, if
CHAPTER 2: INTRAPARTUM CARE
EVIDENCE-BASED PRACTICES
1. A skilled birth attendant shouldassist at the delivery.
2. Pregnant women and their families, aswell as birth attendants, should be ableto recognize danger signs and compli-cations of labor and delivery, andknow when/how to manage or seekappropriate referral care if needed.
3. All deliveries should be “clean” to pre-vent infection.
310496.Text.qxd 7/9/2004 8:29 PM Page 17

18 Qualitative Research to Improve Newborn Care Practices
actions are taken to help prevent infection. Just as“preparing for birth” consists of several practices,ensuring a clean delivery also is comprised of aset of sub-practices. A “clean delivery” means:
• All those attending to the mother or new-born wash their hands with soap and waterbefore, during, and after delivery
• Perineal area is washed before each examina-tion and before delivery, and nothing foreignis put into the vagina (i.e., nothing but theexaminer’s hand, and only when necessary)
• Delivery surface is clean or, at a minimum,the birth does not occur on the bare flooror ground
2.2 What are the current prac-tices, and to what degree or underwhat circumstances might they bechanged?
Again, the first step for qualitative research is toinvestigate the practices currently followed duringthe intrapartum period in relation to the evidence-based practices listed above. Second, the researchmust determine the degree to which and underwhat conditions behavior change would be accept-able and feasible. This helps to ensure the design ofa BCC program that is both realistic and relevant.
Thus, qualitative research should first obtaininformation about the practices and procedurescurrently followed during labor and delivery:Who is present at what times during labor anddelivery? What do they do to assist the birth?Can they recognize danger signs and complica-
Current Practices Lines of Inquiry
Skilled Attendance atDelivery
Determine:1.Whether pregnant women use a skilled attendant for delivery2.Where pregnant women deliver, whether at home or at a health facility3.Who attends to the needs of mother and newborn during labor and delivery4. If a family would consider using a skilled birth attendant for delivery, and what would
make this decision easier and/or the practice more acceptable or feasible
Recognition of Danger Signsand Complications of Laborand Delivery
Determine:1.When respondents feel that mother or newborn are in danger during labor and deliv-
ery, and the local terms for these symptoms of illness2.What their responses would be to these symptoms3.The health provider or facility to which they would go to seek care for these symp-
toms4.Which danger signs/complications are generally perceived or recognized as such; and
which ones are not recognized, misperceived, or misinterpreted
Clean Delivery
Determine:1.Whether those attending to mother or newborn wash their hands with soap and
water before, during, and after delivery2. On what surface women deliver, whether it is cleansed with soap and water or other
traditional materials, and whether it is cleansed more than once during labor anddelivery
3.Whether the perineal area is cleansed before vaginal examinations and delivery4.What would make these decisions about cleansing easier and the practices more
acceptable or feasible5.Whether anything foreign is put into the vagina, and under what conditions this prac-
tice might be discontinued
Table 4. Intrapartum Care: Lines of Inquiry about Current Practices
310496.Text.qxd 7/9/2004 8:29 PM Page 18

Intrapartum Care 19
tions during delivery, and what are theirresponses to these? Are clean delivery proce-dures followed?
With regard to recognizing danger signs andcomplications, it is again important to find outnot only which symptoms are known and recog-nized, but also the depth and accuracy of thisknowledge and what actions they would promptin response. It is also important to understandhow birth attendants respond to danger signs orcomplications during delivery.
After identifying current practices, qualitativeresearch should then determine what it wouldtake for the adoption of evidence-based prac-tices. If a pregnant woman does not practiceclean delivery, what might make such changesmore acceptable or feasible? Under the currentcircumstances, what would be the most appropri-ate degree of change to promote? For example,although families might consider it awkward orcumbersome to have the birth attendant washher hands during delivery, they might accept themore important practice of washing immediatelybefore. If they feel that physical cleaning of thedelivery surface is all that is required (i.e., no spe-cial birthing cloth or plastic) and are unwilling tochange, they might consider the more importantuse of a clean blade and tie for cord care.
Table 4 (page 20) lists priority practices of theintrapartum period and several correspondinglines of inquiry that researchers may want toaddress to determine the current level of compli-ance with evidence-based practices.
2.3 What factors limit or discour-age people’s ability and willingnessto practice evidence-based ENC?
As with antenatal care, a variety of informational,social, cultural, economic, and other factors con-
dition people’s ability and willingness to changeintrapartum care practices. When investigatingthese constraints, there are a number of impor-tant issues that must be addressed for the intra-partum period. Some which merit particularattention include:
Birth attendants: While the advantages ofskilled birth attendants may be obvious to pro-fessionals, families, influenced by norms of tradi-tion, trust, friendship, and privacy, often have adifferent perspective. They may also be suspi-cious of letting “outsiders” into personal mat-ters, and may rightly conclude that a skilled birthattendant will cost more. Qualitative research,therefore, must probe the depths of these con-victions, and determine whether and under whatconditions the use of birth attendants mightbecome more acceptable or realistic.
Concepts of privacy and modesty: In soci-eties where these concepts are highly valued forwomen, families may not choose birth attendantswho require that they undress (as may berequired by many doctors and nurses) or mayavoid facilities where they would be in the pres-ence of strangers.
Knowledge and understanding of dangersigns and complications: Determining knowl-edge of danger signs and complications is com-plicated by the local terms and context, as well asby the subjectivity of many of the symptoms.Interviewers must probe carefully to ensure thatresponses are clear and accurately interpreted;they must be trained to assess only whetherknowledge conforms to the clinical definitions ofthe symptoms.
Clean delivery: This is a complex subjectbecause it is comprised of several sub-practices;researchers will have to explore each one careful-ly. For example, hand washing before delivery mayseem logical and immediately understandable to
310496.Text.qxd 7/9/2004 8:29 PM Page 19
20 Qualitative Research to Improve Newborn Care Practices
skilled health providers, but may not be so totrained birth attendants and families who areoften used to hand washing after delivery.Similarly, while there may be many families whowould consider hand washing before delivery, theymay find it awkward or inconvenient to wash fre-quently during delivery.
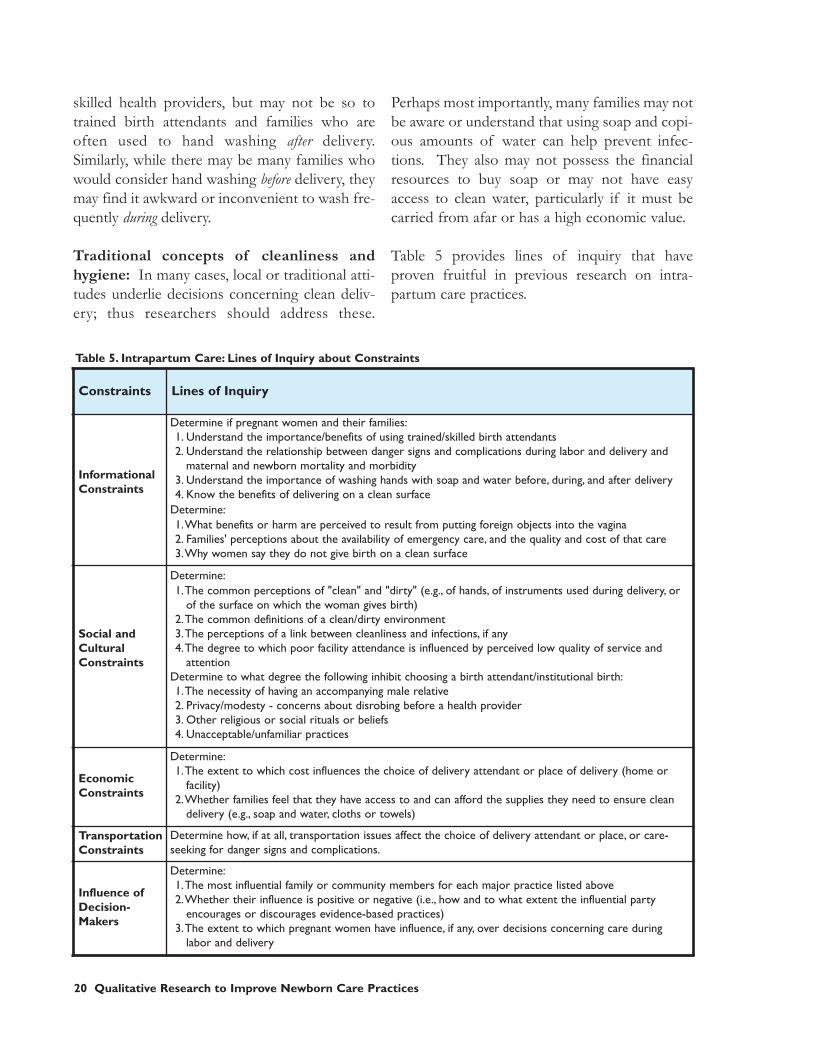
Traditional concepts of cleanliness andhygiene: In many cases, local or traditional atti-tudes underlie decisions concerning clean deliv-ery; thus researchers should address these.
Perhaps most importantly, many families may notbe aware or understand that using soap and copi-ous amounts of water can help prevent infec-tions. They also may not possess the financialresources to buy soap or may not have easyaccess to clean water, particularly if it must becarried from afar or has a high economic value.
Table 5 provides lines of inquiry that haveproven fruitful in previous research on intra-partum care practices.
Constraints Lines of Inquiry
InformationalConstraints
Determine if pregnant women and their families:1. Understand the importance/benefits of using trained/skilled birth attendants2. Understand the relationship between danger signs and complications during labor and delivery and
maternal and newborn mortality and morbidity3. Understand the importance of washing hands with soap and water before, during, and after delivery4. Know the benefits of delivering on a clean surface
Determine:1.What benefits or harm are perceived to result from putting foreign objects into the vagina2. Families' perceptions about the availability of emergency care, and the quality and cost of that care3.Why women say they do not give birth on a clean surface
Social andCulturalConstraints
Determine:1.The common perceptions of "clean" and "dirty" (e.g., of hands, of instruments used during delivery, or
of the surface on which the woman gives birth) 2.The common definitions of a clean/dirty environment3.The perceptions of a link between cleanliness and infections, if any4.The degree to which poor facility attendance is influenced by perceived low quality of service and
attentionDetermine to what degree the following inhibit choosing a birth attendant/institutional birth:1.The necessity of having an accompanying male relative2. Privacy/modesty - concerns about disrobing before a health provider3. Other religious or social rituals or beliefs4. Unacceptable/unfamiliar practices
EconomicConstraints
Determine:1.The extent to which cost influences the choice of delivery attendant or place of delivery (home or
facility)2.Whether families feel that they have access to and can afford the supplies they need to ensure clean
delivery (e.g., soap and water, cloths or towels)
TransportationConstraints
Determine how, if at all, transportation issues affect the choice of delivery attendant or place, or care-seeking for danger signs and complications.
Influence ofDecision-Makers
Determine:1.The most influential family or community members for each major practice listed above2.Whether their influence is positive or negative (i.e., how and to what extent the influential party
encourages or discourages evidence-based practices)3.The extent to which pregnant women have influence, if any, over decisions concerning care during
labor and delivery
Table 5. Intrapartum Care: Lines of Inquiry about Constraints
310496.Text.qxd 7/9/2004 8:29 PM Page 20
Postnatal Care 21
3.1 IMMEDIATE NEWBORN CARE
3.1.1 What proven, evidence-basedinterventions lead to lower neona-tal mortality and morbidity?
Drying and warming: A newborn regulates hisor her body temperature much less efficientlythan an adult, and loses heat more easily, espe-cially from the head. To prevent hypothermia,the newborn should be thoroughly dried with aclean cloth or towel as soon as the head and bodyare fully delivered and before the placenta is deliv-ered. Besides limiting loss of body heat, the stim-ulation this provides can promote breathing andaid an asphyxiated newborn.
The newborn should then be wrapped, includingthe head, with a clean and dry cloth or towel. Inaddition to immediate wrapping, the newborn’swarmth should be ensured after delivery throughcontact with the mother, especially for infantswith a low birth weight.
There are two possible practices in this regard:
• Lay the newborn on the mother’s abdomen,with the mother’s skin touching the new-born’s skin (skin-to-skin contact, alsoreferred to as Kangaroo Mother Care). Coverboth newborn and mother with a clean anddry cloth, towel, or blanket.
• If skin-to-skin contact is not possible, lay thewrapped newborn on the mother’s abdomenor next to the mother on a clean and drycloth, towel, or blanket. Cover the newbornand keep him or her covered with anotherclean and dry cloth, towel, or blanket.
Bathing the newborn is generally not necessaryon the first day, and should be postponed untilthe infant is stable—at least six hours, butpreferably no earlier than 24 hours after birth.The bathwater and the room should be heatedwhen bathing.
Ensuring breathing: The newborn that, despitethe stimulation provided by vigorous drying, hasnot cried, is not breathing regularly, or is gaspingone minute after birth, needs immediate inter-vention. The skilled birth attendant should beequipped and prepared to perform resuscitation,preferably by bag-and-mask.
Immediate breastfeeding: The newborn shouldbe breastfed within one hour after birth, andshould be fed only breast milk (see section 3.2).
Clean cord care: Clean cord care practices arecrucial to prevent infection. The umbilical cordshould be cut with a clean (boiled) blade and tiedwith clean (boiled) materials. No substancesshould be put on the stump.
CHAPTER 3: POSTNATAL CARE
EVIDENCE-BASED PRACTICES
1. Newborns should be thoroughly driedimmediately after delivery and kept warm.
2. Newborns should be observed for cryingand breathing immediately after delivery;asphyxiated newborns should be recognizedand resuscitated.
3. Newborns should be immediately breastfed.
4. Cord care procedures should be clean.
310496.Text.qxd 7/9/2004 8:29 PM Page 21

22 Qualitative Research to Improve Newborn Care Practices
3.1.2 What are the current prac-tices, and to what degree or underwhat circumstances might they bechanged?
As in the first two chapters, the first task for qual-itative research is to elicit information about whatpeople currently do to care for the newbornimmediately after delivery. Specifically, thesequence of immediate newborn care should beexplored: What is done to dry and warm the new-born, and when is this done in relation to deliveryof the placenta? When and how is breathingassessed and ensured? How is the cord cut and
cared for? When is the newborn first breastfed?Second, the researcher must determine what itwould take for the adoption of evidence-basedENC practices. For instance, although keepingwarm is a natural human instinct, the newborn’shigh risk of hypothermia and the consequentneed for special attention to his or her warmthmay not be well understood. Probing questionsshould be asked to determine what steps familiesmight take to give their newborns added thermalprotection. Might they consider drying the new-born before delivery of the placenta, providing atleast a light covering, and keeping the infant incontact with the mother or another caregiver?
Current Practices Lines of Inquiry
Drying andWarming
Determine:1.Whether newborns are dried and wrapped immediately after birth, and before delivery of the
placenta2. If so, how and with what materials3. If not, whether families would consider drying/wrapping the baby immediately after delivery, and
what might facilitate this4.Where the newborn is placed immediately after delivery; before and after delivery of the
placenta and after drying, and for how long5.Whether the newborn has skin-to-skin contact with the mother6. If not, whether families would consider it possible to put the newborn immediately against
mother's skin/body7.What would make this practice (or modifications of it) more acceptable or feasible8.Whether the newborn remains with the mother immediately after delivery, and if separated, how
soon after birth and for how long9. How soon after delivery the newborn is first bathed and by whom (e.g., family member, birth
attendant, etc.)10. If it would be acceptable to delay bathing until the second day of life, if not longer11.The temperature of the bath water and the room during bathing
Ensuring Breathing
Determine:1.Whether and when attention is given to assessing the newborn's cry and breathing, and who
makes this assessment2.What signs of breathing are assessed3.What is done for the non-breathing newborn, by whom, and for how long4. If breathing is not assessed (and assisted, if necessary) immediately after birth, what might
facilitate this
Clean Cord Care
Determine:1.What instruments/materials are used to cut and tie the cord2.What measures, if any, are taken to clean these instruments (e.g., if they are boiled)3.What might facilitate the use of clean instruments for cord care 4.What substances, if any, are applied to the cord stump and by whom5.The frequency and duration of this treatment6.Whether it would be acceptable to simply keep cord stump clean and dry, and apply nothing
Table 6. Immediate Newborn Care: Lines of Inquiry about Current Practices
310496.Text.qxd 7/9/2004 8:29 PM Page 22

Postnatal Care 23
Table 6 lists priority practices of the immediatepostnatal period and several corresponding linesof inquiry that researchers may want to pursue todetermine the current level of compliance withevidence-based practices.
3.1.3 Which factors limit or dis-courage people’s ability and will-ingness to practice evidence-based ENC?
When investigating constraints on immediatenewborn care, there are a number of importantissues that must be addressed. Those warrantingparticular attention include:
Concept of warmth: While warmth appears tobe a basic human concept, in reality there can bemany subjective versions of warmth. Membersof the same household often disagree on themost comfortable temperature. The elderlyoften feel cold more intensely than the young.On the subject of ENC, many women whoexperience a “shiver reflex” immediately afterbirth draw the conclusion that their bodies andskin are colder than those of the newborn, andthus refuse skin-to-skin contact. It is critical forinvestigators to gauge indigenous perceptions ofwarm and cold to create accurate and effectiveBCC messages of drying and warming.
Concept of the spiritual endowment of theplacenta: While most Western cultures view theplacenta as essential to the growth and survivalof the fetus while in the womb, but of no valueafter birth, many other societies believe it isendowed with a spirit. Because of this separatespiritual identity, and also because of fears insome societies that the undelivered placenta maymove upwards in the chest and choke thewoman, the “delivery” of the placenta is oftenconsidered as important as that of the newborn,
and of even greater urgency. Consequently, moreattention is often paid to the delivery of the pla-centa than to the newborn. At the same time,because spiritual identity also means that thenewborn and the placenta are equal beings atbirth, mothers and caregivers should be able toaddress the immediate needs of the newborn. Inany case, this subtle and often profound beliefhas important ramifications for ENC behaviorchange and must be carefully explored.
Concepts of hygiene and cleanliness:Hygiene and aseptic conditions may be unknownor very difficult to achieve in many poor commu-nities. People may be unaware of the environ-mental dangers of infection, and may be unableto do much to combat them. This pervasiveacceptance of unhygienic conditions may extendto cord care, newborn drying and wrapping,materials, etc.
A related issue may arise in those cultures wherebirth is considered polluting; in this situation,laying the newborn against the mother’s skin ordelaying bathing may be considered dangerous.Moreover, these practices may be a violation ofreligious beliefs, perceived as compromising thereligious standing of those who have contactwith the “polluted” infant. There may also besociocultural reasons why families do not prac-tice clean cord care; they may believe that apply-ing certain substances on the cord helps it toheal, when in fact, this practice increases therisk of infection. Often there is a religious orcultural significance to the application of cer-tain substances.
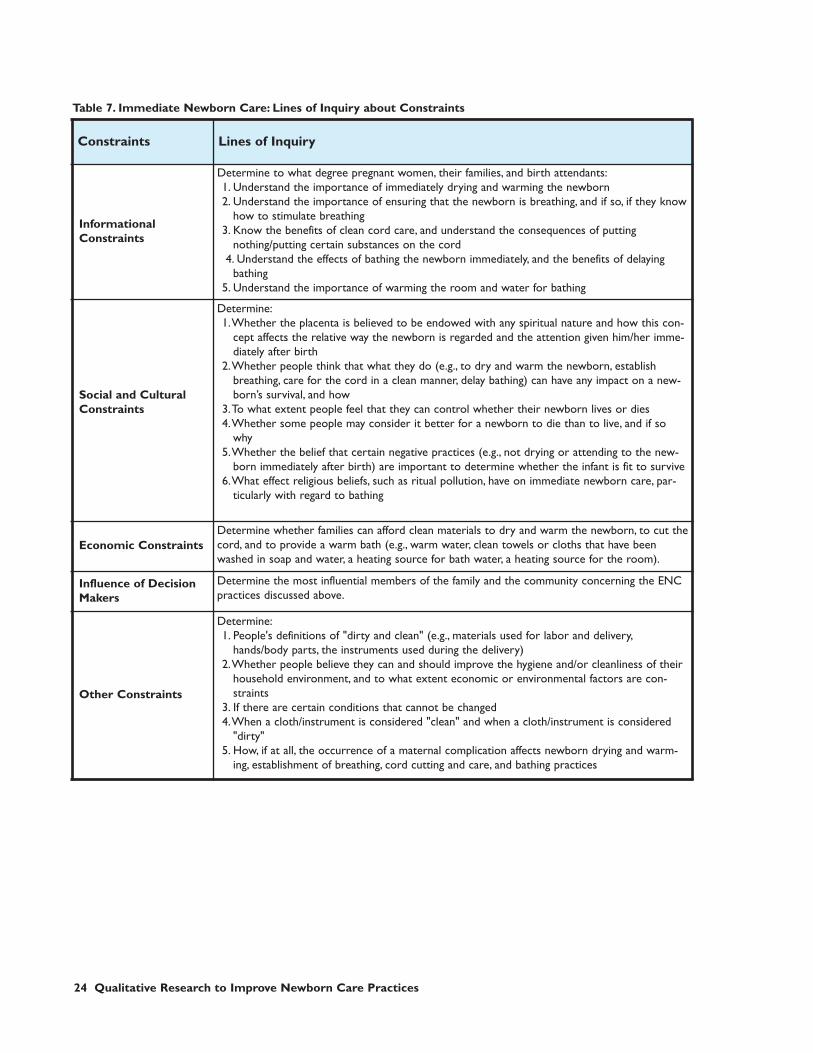
Table 7 lists priority practices of the immediatepostnatal period and several corresponding linesof inquiry that researchers may follow to deter-mine the current level of compliance with evi-dence-based practices.
310496.Text.qxd 7/9/2004 8:29 PM Page 23
24 Qualitative Research to Improve Newborn Care Practices
Constraints Lines of Inquiry
InformationalConstraints
Determine to what degree pregnant women, their families, and birth attendants:1. Understand the importance of immediately drying and warming the newborn2. Understand the importance of ensuring that the newborn is breathing, and if so, if they know
how to stimulate breathing3. Know the benefits of clean cord care, and understand the consequences of putting
nothing/putting certain substances on the cord4. Understand the effects of bathing the newborn immediately, and the benefits of delaying
bathing5. Understand the importance of warming the room and water for bathing
Social and CulturalConstraints
Determine:1.Whether the placenta is believed to be endowed with any spiritual nature and how this con-
cept affects the relative way the newborn is regarded and the attention given him/her imme-diately after birth
2.Whether people think that what they do (e.g., to dry and warm the newborn, establishbreathing, care for the cord in a clean manner, delay bathing) can have any impact on a new-born’s survival, and how
3.To what extent people feel that they can control whether their newborn lives or dies4.Whether some people may consider it better for a newborn to die than to live, and if so
why5.Whether the belief that certain negative practices (e.g., not drying or attending to the new-
born immediately after birth) are important to determine whether the infant is fit to survive6.What effect religious beliefs, such as ritual pollution, have on immediate newborn care, par-
ticularly with regard to bathing
Economic ConstraintsDetermine whether families can afford clean materials to dry and warm the newborn, to cut thecord, and to provide a warm bath (e.g., warm water, clean towels or cloths that have beenwashed in soap and water, a heating source for bath water, a heating source for the room).
Influence of DecisionMakers
Determine the most influential members of the family and the community concerning the ENCpractices discussed above.
Other Constraints
Determine:1. People's definitions of "dirty and clean" (e.g., materials used for labor and delivery,
hands/body parts, the instruments used during the delivery)2.Whether people believe they can and should improve the hygiene and/or cleanliness of their
household environment, and to what extent economic or environmental factors are con-straints
3. If there are certain conditions that cannot be changed4.When a cloth/instrument is considered "clean" and when a cloth/instrument is considered
"dirty"5. How, if at all, the occurrence of a maternal complication affects newborn drying and warm-
ing, establishment of breathing, cord cutting and care, and bathing practices
Table 7. Immediate Newborn Care: Lines of Inquiry about Constraints
310496.Text.qxd 7/9/2004 8:29 PM Page 24

Postnatal Care 25
3.2 NEONATAL CARE
3.2.1 Which proven, evidence-based interventions lead to lowerneonatal mortality and morbidity?
Routine postnatal care visits: While the opti-mal timings of postnatal visits for healthy new-borns have not yet been adequately tested indeveloping countries to allow an evidence-basedrecommendation, research suggests that keyintervention times to prevent neonatal deathsare: immediately after delivery, on day 2 – 3, andon day 6 – 7, at a minimum.
Exclusive breastfeeding: In the postnatal peri-od, the most important practice is to establishimmediate and exclusive breastfeeding. This ben-efits both the mother and the newborn. For themother, immediate breastfeeding stimulates uter-ine contractions and delivery of the placenta, andthus may reduce the risk of postpartum hemor-rhage. For the newborn, early breastfeeding pro-vides nutrition and warmth, and colostrum(mother’s “first milk”) contains substances thathelp prevent infection.
In addition, it is very important that the infant isexclusively breastfed; that is, not given water orany other substances. Immediate and exclusivebreastfeeding are of particular importance forpreterm and low birth weight newborns.
Maintenance of warmth and clean environ-ment: The principles of keeping the newbornwarm and maintaining cleanliness (particularlyhand-washing when handling the newborn),remain priorities for preventing hypothermia andinfection in the postnatal period. Special atten-tion should be given to warming and hygiene forpreterm and low birth weight newborns.
Recognition of newborn danger signs andcomplications: As in the antenatal and intra-partum periods, the practice of complicationpreparedness is critical. The mother and her fam-ily, as well as health providers, should be aware ofthe following common danger signs and compli-cations during the neonatal period:
• Inability to feed adequately or cessation of sucking
• Weak or abnormal cry or cessation of crying• Lethargy or loss of consciousness• Redness of the umbilicus extending to the
skin of the abdomen• Discharge (pus) from the umbilicus• Localized skin infection (pustules)• Discharge from or redness of the eyes• Persistent vomiting and/or abdominal distention• Difficulty breathing (including chest in-draw-
ing on inspiration or grunting on exhalation)• Fast breathing (> 60 breaths per minute)• Fever or unusually cold body temperature• Convulsions, seizures, or fits • Yellow discoloration (jaundice) of the skin—
the further “down” the body (i.e., hands andfeet) the worse the jaundice
EVIDENCE-BASED PRACTICES
1. Mother and newborn should have routinepostnatal care visits with a health provider,particularly during the first week after birth.
2. Newborns should be exclusively breastfed.
3. Warmth and clean environment should bemaintained.
4. Mothers and their families should be ableto recognize newborn danger signs andcomplications, and know when/how tomanage or seek appropriate referral care ifneeded.
310496.Text.qxd 7/9/2004 8:29 PM Page 25
26 Qualitative Research to Improve Newborn Care Practices
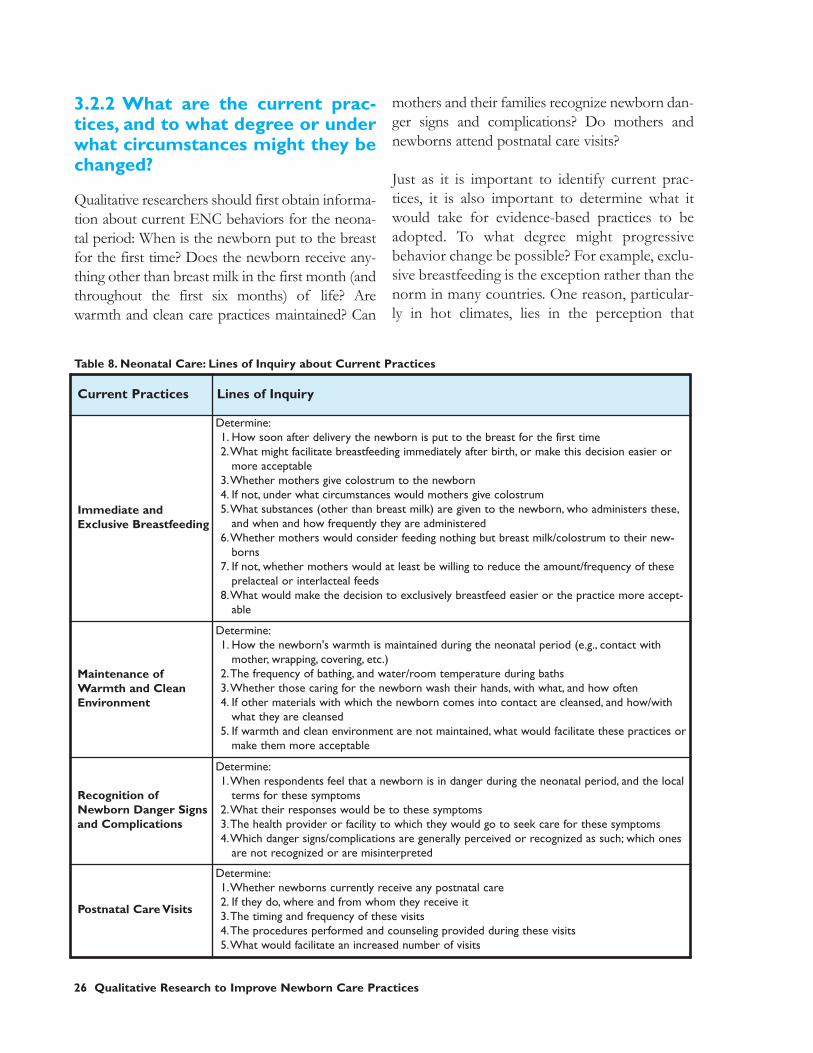
3.2.2 What are the current prac-tices, and to what degree or underwhat circumstances might they bechanged?
Qualitative researchers should first obtain informa-tion about current ENC behaviors for the neona-tal period: When is the newborn put to the breastfor the first time? Does the newborn receive any-thing other than breast milk in the first month (andthroughout the first six months) of life? Arewarmth and clean care practices maintained? Can
mothers and their families recognize newborn dan-ger signs and complications? Do mothers andnewborns attend postnatal care visits?
Just as it is important to identify current prac-tices, it is also important to determine what itwould take for evidence-based practices to beadopted. To what degree might progressivebehavior change be possible? For example, exclu-sive breastfeeding is the exception rather than thenorm in many countries. One reason, particular-ly in hot climates, lies in the perception that
Table 8. Neonatal Care: Lines of Inquiry about Current Practices
Current Practices Lines of Inquiry
Immediate andExclusive Breastfeeding
Determine:1. How soon after delivery the newborn is put to the breast for the first time2.What might facilitate breastfeeding immediately after birth, or make this decision easier or
more acceptable3.Whether mothers give colostrum to the newborn4. If not, under what circumstances would mothers give colostrum5.What substances (other than breast milk) are given to the newborn, who administers these,
and when and how frequently they are administered6.Whether mothers would consider feeding nothing but breast milk/colostrum to their new-
borns7. If not, whether mothers would at least be willing to reduce the amount/frequency of these
prelacteal or interlacteal feeds8.What would make the decision to exclusively breastfeed easier or the practice more accept-
able
Maintenance ofWarmth and CleanEnvironment
Determine:1. How the newborn's warmth is maintained during the neonatal period (e.g., contact with
mother, wrapping, covering, etc.)2.The frequency of bathing, and water/room temperature during baths3.Whether those caring for the newborn wash their hands, with what, and how often4. If other materials with which the newborn comes into contact are cleansed, and how/with
what they are cleansed5. If warmth and clean environment are not maintained, what would facilitate these practices or
make them more acceptable
Recognition ofNewborn Danger Signsand Complications
Determine:1.When respondents feel that a newborn is in danger during the neonatal period, and the local
terms for these symptoms2.What their responses would be to these symptoms3.The health provider or facility to which they would go to seek care for these symptoms4.Which danger signs/complications are generally perceived or recognized as such; which ones
are not recognized or are misinterpreted
Postnatal Care Visits
Determine:1.Whether newborns currently receive any postnatal care2. If they do, where and from whom they receive it3.The timing and frequency of these visits4.The procedures performed and counseling provided during these visits5.What would facilitate an increased number of visits
310496.Text.qxd 7/9/2004 8:29 PM Page 26

Postnatal Care 27
breastfeeding does not provide adequate fluid.However, a number of breastfeeding promotionprojects have been successful in encouragingmothers to discontinue the practice of givingwater to newborns, at least during cooler times ofthe year.
Qualitative research should also explore possibil-ities for behavior change negotiation on the issueof prelacteal feeding. Prelacteal feeds, such ashoney, tea, ghutti, or sugar water, can be harmful,as they may cause infections and diarrhea. Therisks of this ritual are even more serious if sub-stances (like honey) are routinely given a numberof times as an interlacteal feed. The goal of qualita-tive research in these situations is to determine ifthere are conditions under which a family mightagree to reduce the amount and frequency ofprelacteal feeds. Limiting the practice to theanointing of the newborn’s lips, rather than actu-ally introducing the food itself, might also be afeasible compromise in some cultures.
Table 8 lists priority practices of the neonatalperiod and several corresponding lines of inquirythat researchers may want to address to deter-mine the current level of compliance with evi-dence-based practices.
3.2.3 What factors limit or discour-age people’s ability and willingnessto practice evidence-based ENC?
For neonatal care, as with the previous ENCperiods, a variety of informational, social, cultur-al, economic, and other factors can affect peo-ple’s ability and willingness to change to evi-dence-based practices. When investigating theseconstraints on neonatal care, there are a numberof important issues that must be addressed.Those meriting particular attention include:
Colostrum: Many societies reject feeding thenewborn a mother’s colostrum, despite the nutri-
tional and immunological properties that it pos-sesses. In many cultures, colostrum is consideredan unclean substance that must be extruded (dis-carded) before the milk can be fed. Others con-sider it a purgative, and still others believe it to bea neutral, but non-nutritive cleansing substance.It is important for the researcher to determinethe convictions that families have regardingcolostrum’s negative properties, as well as thedepth of these beliefs. In other words, in societiesthat believe colostrum to be simply a neutral, non-nutritive substance, changing practices may bemuch easier than in those societies that think it isa purgative. In areas where immunization pro-grams are already well accepted,likening colostrum to the infant’s first immuniza-tion may be an effective behavior change message.
Prelacteal feeds: Prelacteal feeds are consideredan important social and cultural custom that, likemarriage, confirmation, and circumcision, conferspecial importance on certain family membersand confirm their role and responsibilities withinthe family. In some cultures, prelacteal feeds arereligiously significant, the practice seen asbestowing God’s protection upon the newborn.While it is is, consequently, particularly difficultto eliminate, it may be possible to modify thepractice, retaining its traditional ritual valueswhile reducing the adverse health risks (see forinstance, the Hausa ritual, described on p. 4-5).
Breastfeeding and economic factors/oppor-tunity costs: One of the greatest obstacles toexclusive breastfeeding can be the opportunitycost of the practice. While some BCC programshave portrayed breastfeeding as a no-cost option,in reality that is far from the case. Breastfeedinga newborn 8 to 10 times a day, which is usual inon-demand feeding cycles, represents a distincteconomic cost whether a woman works within oroutside the home. In modernizing urban soci-eties where women work in the organized sector,exclusive breastfeeding may represent an oppor-tunity cost that is simply too great to bear.
310496.Text.qxd 7/9/2004 8:29 PM Page 27

28 Qualitative Research to Improve Newborn Care Practices
Similarly, in more traditional societies wherewomen’s domestic labor is arduous and continu-ous, time taken for breastfeeding reduces otherproductive work. Therefore, the decision not tobreastfeed is a logical one when the perceivedeconomic benefits of labor exceed the perceivedadvantages of breastfeeding. Qualitative researchersshould investigate the economic ramifications ofbreastfeeding and determine whether economi-cally productive women could increase the fre-quency of breastfeeds.
Knowledge and understanding of dangersigns and complications: Although the new-
born danger signs and complications listed previ-ously may appear obvious to the experiencedhealth professional, they are, in fact, somewhatsubjective and open to local interpretation. It iscritical that when performing qualitativeresearch, interviewers define local terms andcontext for various illnesses and signs of illness,and agree upon minimum criteria to accept asrecognition of each danger sign.
Table 9 suggests areas of investigation that havebeen productive in former research on neonatalcare practices.
Constraints Lines of Inquiry
InformationalConstraints
Determine the perceived positive or negative effects of:1. Giving colostrum to the newborn2. Giving only breast milk3. Putting the newborn to breast within an hour of delivery
Determine whether mothers believes:4.Their breast milk provides sufficient food and liquid5.Their breast milk supply is adequate in the first month
Social and CulturalConstraints
Determine:1. Common perceptions of colostrum: whether it is considered dirty, a purgative, a non-nutri-
tive precursor to breast milk, etc.2.Whether there are any rituals in which substances are given to the newborn, and for what
reasons3.Whether keeping the newborn with the mother is perceived as important, and if not, why 4. How belief in the spiritual endowment of the placenta affects the timing of first breastfeed-
ing (i.e., do women wait for the placenta to be delivered)5.Whether families realize that breastfeeding helps stimulate delivery of the placenta and
limit the risk of postpartum hemorrhage6.Whether the mother’s age or the newborn’s birth order or sex is a factor in breastfeeding
Economic Constraints
Determine:1.Whether women's economic opportunities, at home or outside the home, interfere with
exclusive breastfeeding2.Whether women believe that their diet or inadequate food availability influence the quanti-
ty/quality of breast milk
Time ConstraintsDetermine whether mothers perceive exclusive breastfeeding in the first month to be moreor less time consuming than other feeding alternatives, and what effect, if any, this may have onfeeding behavior
Table 9. Neonatal Care: Lines of Inquiry about Constraints
310496.Text.qxd 7/9/2004 8:29 PM Page 28
Research Methods 29
4.1 Overview
The previous chapters of this guide provide linesof inquiry to investigate current ENC practicesand the various constraints limiting ENC behaviorchange. Actual field research may be designed andimplemented on the basis of these lines of inquiry.
There are many different qualitative researchmethods available, ranging from those that arewidely applicable, such as focus groups, to morespecific, but equally useful techniques, such asmapping. The choice of methods depends onmany factors. The two most commonly usedqualitative research methods follow:
Focus groups are best used to probe a com-plex, narrowly focused issue. A topic thatinvolves cultural and religious beliefs and prac-tices, for example, may require the patient, delib-erate, participatory techniques that characterizefocus groups. A topic such as exclusive breast-feeding, which is conditioned by a number ofsocial, cultural, and economic factors, also lendsitself to focus group discussions.
Focus groups are usually comprised of 8 to 12persons of similar background. A skilled facilita-tor guides the discussion—probing beliefs andattitudes underlying the topic of interest—whilemembers of a study team may record answers.
Individual or group interviews are often usedwhen factual information needs to be collected,such as the current practices of health personnel.It may be more efficient to collect this informa-tion from a number of workers gathered in oneplace than to interview them individually. Agroup of health workers may be asked, for exam-ple, “Why did you want to become a communityhealth worker?”
In a group interview, all respondents are inter-viewed and urged to respond. No attempt ismade to record the answers for each respondentseparately. A group interview can be done usinga structured or semi-structured questionnairewith closed or open-ended questions.
Individual interviews may be more effective forexploring sensitive topics that the intervieweewould not feel comfortable discussing in a groupsetting, such as the relative value of a female child.
Table 10 presents these and other common qual-itative research methods and gives the salientfeatures of each, with examples of newborncare applications.
For those program managers who desire moredetailed and technical information about theseand other qualitative research methods, a list ofresources has been provided in Appendix 1.Included are in-depth guides to both focusgroups and group interviews and a general guideto qualitative methods, with detailed instructionson their use.
4.2 Selection of Respondents, DataAnalysis, and Reporting
Selection of Respondents
Techniques for the selection of respondents forqualitative studies are not random, but ratherbased upon the researchers’ judgment of whichrespondents would generate the best-quality data.In some cases, respondents may be selected whoare especially vocal, for example. Respondents areusually selected based on similarities in terms ofcriteria such as age, sex, and socioeconomic status.
CHAPTER 4: RESEARCH METHODS
310496.Text.qxd 7/9/2004 8:29 PM Page 29

30 Qualitative Research to Improve Newborn Care Practices
Table 10. Qualitative Research: Methods and Examples of Newborn Care Applications
Method Description Features Examples of Newborn CareApplications
IndividualIn-depth Interview
• Uses a structuredquestionnaire withopen-ended ques-tions to probe prac-tices and beliefs indetail
• Generates detailedinformation regardingpractices and con-straints
• Elicits information onsensitive topics
• Home care practices during preg-nancy
• Steps taken to prepare for delivery
Group Interview
• Uses a structured orsemi-structuredinstrument to probepractices and beliefs,but anyone in thegroup can respond
• Allows for efficientlycollecting informationfrom several respon-dents at the sametime
• The degree to which pregnantwomen and their families recognizedanger signs and complications ofthe antenatal, intrapartum, and post-natal periods
• The degree to which cost is a factorin the choice of delivery attendant orplace of delivery
Focus GroupDiscussion (FGD)
• Explores centralthemes or issues;allows for free andopen discussion withdebate
• Allows for in-depthexploration of focusedtopics
• Practices surrounding initiation ofbreastfeeding
DirectObservation
• A trained observer ispresent to observepractices firsthand
• The most accurateway of recording prac-tices, but requireshighly skilledobservers and is timeconsuming
• Sanitation in the home, includingavailability and use of soap andwater
• Where the newborn is placeddirectly after birth
• How the newborn is dried andwrapped
Narratives orScenarios
• Uses actual or recre-ated stories about aparticular topic toexplore practicesand beliefs orprompt discussion
• Enables participants tofocus on a real-lifeENC situation
• Often situates partici-pants within a familiarsociocultural context
• Quality of care received duringantenatal, intrapartum, and postnatalperiods
• Process of birth and emergencypreparation
MappingTechniques
• Community• Social• Body
• The first two typesof mapping ask par-ticipants to visualizecommunity or socialsystems; body map-ping asks partici-pants, for example,to visualize theirreproductive systems
• Encourages partici-pants to identify anddescribe systems orpatterns with whichthey are so familiarthat they rarely definethem
• Community mapping of a villagewith health post, health providers,and TBAs to explore sources ofhelp for newborn problems
• Social mapping of organizations,such as occupational, social, or reli-gious groups
• Body mapping of reproductiveorgans, fetal growth, or bodilychanges of pregnancy
GroupingTechniques
• Asks participants toorganize and rankvarious elements ofthe ENC system
• Indicates how respon-dents prioritize itemsaccording to particularcharacteristic(s)
• Newborn or maternal danger signsand complications grouped by type,severity, cause, frequency of occur-rence, and/or treatment
310496.Text.qxd 7/9/2004 8:29 PM Page 30

Research Methods 31
Data Analysis
Qualitative data are most often analyzed by hand.The basic data analysis steps include reviewing,coding, summarizing, and interpreting the datacollected. Community members may actively par-ticipate in the analysis either individually, in smallgroups, or in a workshop setting. Examples ofhow analyses for focus groups or interviews canbe conducted include:
• Individually or in small groups: Researchersgo through their interview notes and for eachrespondent (e.g., mother), put the answer toeach question on a separate index card. Thenthe index cards are reviewed, commonthemes are identified, and the cards are sort-ed according to each theme. Each theme canthen be summarized in a few words and theresults interpreted.
• In a workshop: All researchers go throughtheir interview notes together in a workshop.One question at a time is written on a flipchart,and interviewers read out all the responses theyobtained for each question, while someonerecords them. The group next identifies themost common responses. Then, group discus-sion can focus on interpreting these commonresponses and deciding upon the appropriateactions to improve health interventions.
There are several computer programs that per-form analyses of qualitative data, and reader-friendly guides are available to aid in their usage.7
Chapter 5 explains how to set up an analyticalframework for qualitative research.
Reporting
Qualitative research methods answer questionssuch as “who,” “what,” “when,” “where,” “why,”and “how.” Questions such as “how often” and“how many” are more appropriately answered byquantitative research methods. Reports of quali-tative research, therefore, should state trends butshould not attempt to quantify results using num-bers or percentages. Examples of the types ofstatements that could be made on the basis ofqualitative methods follow:
• There was a general perception in the com-munities where group interviews were con-ducted that health care staff had improvedtheir treatment of newborns and their moth-ers since ENC training was introduced.
• Of those young mothers (< 20) who partici-pated in focus groups in peri-urban commu-nities, most mentioned the importance ofantenatal care in improving safe delivery aftercommunity health workers began makinghouse-to-house visits. Very few mentionedthe importance of antenatal care in focusgroups held before this intervention.
Including direct quotations from participantswithin the report can sometimes capture the rich-ness of the data collected.
310496.Text.qxd 7/9/2004 8:29 PM Page 31

blank
310496.Text.qxd 7/9/2004 8:29 PM Page 32
After the Research 33
Once qualitative research has been completed,the program manager will 1) analyze the infor-mation and 2) based upon this data analysis,make appropriate decisions concerning programdesign. BCC strategic planning will address bothmedia programming—selection of outlets,design of messages, format, and presentation—and interpersonal communication (IPC) trainingand implementation programs.
5.1 Using Qualitative Research Data
The design of BCC programs will use theresults of qualitative research in the followingprinciple ways:
1. Identification of priority practices: Ifqualitative research has been conductedproperly, considerable effort will have beeninvested in determining which current prac-tices are amenable to change given informa-tional, social, cultural, economic, and supply con-straints. Qualitative research can also be usedto offer insights into how and why currentpositive ENC behaviors are practiced orhave come about.
If certain practices, such as prelacteal feeds,are strongly embedded within traditionalsocial patterns and cultural and religiousbeliefs, changing them may not be feasible—at least within the lifetime of most BCC pro-grams. On the other hand, practices forwhich there are few prevailing socioculturalconstraints may be relatively easy to change.For example, mothers who already under-stand the importance of ANC visits mayquite readily agree to increase attendancefrom two visits to three.
Certain practices are conditioned by eco-nomic necessity. For example, additionalANC visits represent opportunity costs,and the purchase of clean delivery kits orproducts may be inhibited by limited finan-cial resources.
Other practices are limited by access to orsupply of goods and services. If emergencyreferral services are not available in a partic-ular area, then it is programmaticallyunsound and ethically dubious to promotethe immediate evacuation of mothers andnewborns in distress to a health facility.Similarly, if emergency funds for birth pre-paredness are promoted but no communityloan or transport systems have been created,the message may be quickly discredited.
Therefore, program managers and researchersmust recognize these limitations and identifysound priority practices. As has been shownin the tables throughout this document, linesof inquiry have been designed to answer thequestions “Would you consider adopting Xbehavior?” and “To what degree or underwhat circumstances would you change yourcurrent practice?” Other lines of inquiryassess the nature and quality of existing prac-tices; how deeply rooted, integral to socialand cultural patterns, and strictly governed byexisting networks of authority they are. Ananalysis of these lines of inquiry will answer:
• When given sound ENC informationfrom a trustworthy source, are people atall willing to change?
• What are the easiest or first things theywould change about their current practice?
CHAPTER 5: APPLYING DATA ANALYSIS TO BCCPLANNING AND PROGRAMMING
310496.Text.qxd 7/9/2004 8:29 PM Page 33
34 Qualitative Research to Improve Newborn Care Practices
• Even if people indicate a willingness tochange, is the change feasible withinexisting social, cultural, economic, andsupply realities?
It should be noted that the final selection of pri-ority practices will be a function of two otherimportant factors:
• Epidemiology and tipping points: Aparticular practice may be considered fea-sible, given an analysis of constraints, butmay not be cost-effective as a priority. Forexample, many countries have alreadyachieved considerable success in increas-ing the rates of ANC attendance. Giventhe evolution of social norms, practicesthat have achieved 50% coverage tend toaccelerate geometrically in acceptance pastthis “tipping point.” Thus, it will be fareasier to achieve change from 50% to 60%than from 10% to 20%. Usually, as a prac-tice becomes increasingly common andclose to evolving into a social norm, socialdynamics are such that little additionalinvestment is required to move the popu-lation to near-complete compliance.
• Parallel programs and investments:Most Safe Motherhood projects focus onANC, recognition of danger signs andcomplications during pregnancy, skilledattendance at birth, and responsible andprompt referral. Therefore, although thequalitative research may show that theseareas are particularly promising as priori-ties, other programs may already be ade-quately addressing them. BCC invest-ments within the context of an ENC pro-gram, therefore, may focus on other pri-orities, such as postnatal care.
2. Selection of a progressive change strate-gy: The research results will provide the BCCprogrammer with valuable information con-
cerning possible strategies for progressivechange—that is, the most acceptable and fea-sible degree of behavior change to promotefor a particular audience at a particular time.
Women in a recent BCC breastfeeding pro-gram in India were encouraged, as a first stepto exclusive breastfeeding, to eliminate “topmilk” (a water-based liquid thought to sup-plement or “top off ” breast milk). In manyother countries, a similar focus in exclusivebreastfeeding campaigns was placed on elim-inating water from the newborn’s breastfeed-ing regimen. Because giving the newbornwater has no particular religious or tradition-al significance, and because it is has such apernicious effect on newborn health, this wasan ideal place to begin the progressive behav-ior change process.
Qualitative research inquiries will also pointthe researcher towards possible areas fornegotiated behavior change. For example,some potentially harmful practices, such asbathing the newborn immediately after birth,may be modified or replaced by more positivepractices, such as delaying bathing or cleaningthe newborn instead with a warm, damp cloth.
3. Identification of behavioral entry points:Qualitative research data will provide valu-able insights regarding entry points forbehavior change—that is, common practicesor beliefs on which one can build a case forimproved ENC. For example, in many cul-tures there is a common practice of heating aroom before the delivery of a child.Certainly, if there is already this belief aboutwarmth, it could be built upon to encouragefamilies to increase that warmth and alsoapply it in new circumstances. Similarly, ifthere is a strong cultural belief about theequivalent souls of newborn and placenta, thisbelief could be developed to stress the impor-tance of caring for both simultaneously.
310496.Text.qxd 7/9/2004 8:29 PM Page 34

After the Research 35
All people are aware to some degree of thesigns and symptoms of disease. A sore throat,runny nose, and sneezing may presage theonset of a cold. A queasy stomach often pre-cedes diarrhea. BCC strategies should also beable to build on these common perceptionsto increase the recognition and appreciationof danger signs and complications during theantenatal, intrapartum, and postnatal periods.
5.2 Setting Up an Analytical Framework
It is extremely important for program managersand researchers to develop an analytical frame-work for the qualitative research before theresearch begins. That is, the purpose and applica-tions of the data generated and the manner inwhich it will be organized should be determinedahead of time.
Table 11 is a suggested matrix for organizing thedata gathered in qualitative research, which shouldbe completed following the data collection:
• Evidence-based practices: Before begin-ning qualitative research, select those prac-tices that have the greatest potential impacton newborn health. Consider the relativeanticipated health impact of the practicesbased on available evidence and rank theimpact of each as high, medium, or low.
• Current practices: After qualitative researchhas been completed, list the current practicesof women, family members, or caregiversthat correspond to each of the potentialhigh-impact practices. For exclusive breast-feeding, for example, indicate what women
actually do—prelacteal feeds, early administra-tion of water, supplemental feeding, etc.
• Informational, social, cultural, and eco-nomic constraints: List those constraintsthat have emerged from the research and aremost likely to interfere with behavior change.That is, what factors limit or discourage thepractice of evidence-based ENC?
• Supply constraints: The strategic planningprocess must also consider elements ofENC—such as service delivery, essentialdrugs, clean delivery supplies, etc.—from theperspective of supply. That is, although qual-itative research will have identified families’perceptions of the supply of these elements,the actual situation in terms of the availabilityof supplies and services must also beassessed. No responsible BCC program canpromote the increased use of health facilities,their services, and supplies unless they are infact already available and accessible or theENC program has assured their availability.
• Feasibility of change: Based on the infor-mation on constraints and underlying ENCpractices, determine which of the currentpractices are the most likely to be modified.That is, for which of the high-impact prac-tices are there a minimum of social, cultural,economic, and supply constraints? Rank thefeasibility of change for each as high, medi-um, or low.
• Behavioral trials of improved practices:Once high feasibility, high impact practiceshave been identified, additional explorationmay be necessary to determine what women,
Evidence-BasedPractices
CurrentPractices
Informational, Social,Cultural, Economic,and SupplyConstraints
Feasibilityof Change
BehavioralTrials ofImprovedPractices
FinalPriorityPractices
CommunicationStrategies
Table 11. Proposed Matrix for Analyzing Qualitative Data and Developing a BCC Strategy
310496.Text.qxd 7/9/2004 8:29 PM Page 35

36 Qualitative Research to Improve Newborn Care Practices
families, birth attendants, and communitieswould be willing to do to change them. Trialsof improved practices can be a useful way todo this. They provide feedback on the prob-ability of getting people to adopt a particularnew behavior. These trials are a technique toelicit and negotiate those solutions that arethe most appropriate, acceptable, and realis-tic from the client’s perspective.
• Final priority practices: Given the effortrequired to change behavior, particularlypractices rooted in ritual or tradition, it isimportant to select no more than 4 to 5 prioritypractices on which to focus in any BCC cam-paign or program. These priority practicesshould be taken from among those identifiedas both high impact and high feasibility.
• Communication strategies: Finally, basedon the behavioral information derived fromqualitative research, determine the best com-munication methods for encouraging clientsto change from current practices to prioritypractices. Qualitative research should answerthe questions: “What information do clientsneed to help them move along the path to pri-ority practices?” and “What might be themost persuasive and effective ways to presentthis information?” Communication strategiesmay also be derived from learning why andhow families that have adopted positive ENCpractices came to make these decisions.8
5.3 BCC Planning andProgramming
The planning and programming steps to be takenafter completion of data analysis are explainedbelow. In addition to the planning of the BCCprogram, a monitoring and evaluation strategyshould be developed for performance assess-ment and impact evaluation.
BCC Strategic Planning
The BCC Strategic Plan is the formal documentto be used by executing agencies, be they NGOs,research institutions, or governments, whenselecting, designing, and developing media andmaterials, and when designing and implementingIPC training. It summarizes the results of thequalitative research and defines: a) the prioritypractices considered the most amenable tochange and most likely to have the greatestimpact on neonatal health and survival, and b)the communication strategies most appropriatefor each priority practice. In other words, theplan identifies the most acceptable and effectiveways to encourage people to progress towardadoption of evidence-based ENC priority prac-tices. A communication strategy is derived bothfrom responses to the question “What changemight you consider in your current behavior?”and from an analysis of those factors that con-tribute to existing positive behavior.
The BCC Strategic Plan is based on qualitativeresearch data that have been subjected to a rigor-ous analytical process. Therefore, the plan offersconclusions and recommendations that havebeen derived directly from real-life experience.The priority practices presented in the plan arethose meeting the criteria of high impact andhigh feasibility. The communication strategiespresented should have been selected from manyoptions, and should be those most likely toappeal to client communities.
The BCC Strategic Plan, therefore, can beused as a guide for:
1. Developing media
2. Developing IPC training materials
The plan will assist the program manager todevelop media and IPC training materials in thefollowing ways:
310496.Text.qxd 7/9/2004 8:29 PM Page 36

After the Research 37
• It will indicate which priority practices should beaddressed. Given constraints of time and budg-et, the chances of behavior change increasewhen investments of time, effort andresources are focused on a few, key practices.
• It will suggest the behavioral approach most likely tosucceed for each priority practice within the particu-lar social, cultural, and economic context. Forexample, in some countries an initial focuson immediate breastfeeding may be morelikely to yield significant results than a focuson exclusive breastfeeding. Similarly, a pro-gram emphasizing that immediate breast-feeding eases placental delivery may be moreeffective in bringing about behavior changethan the more common nutritional orimmunological arguments.
Media Selection, Design and Production
The following are suggested guidelines for creat-ing effective media:
• The selection of media should be based oncoverage, audience, and cost. Unlike theircommercial cousins, most BCC campaignshave limited finances; therefore the selectionof media becomes all the more important. Ifa particular medium has limited coverage, ifits per-beneficiary cost is high relative to theexpected impact on behavior change, or if itis of limited interest to clients, then it shouldnot be programmed. For example, there hasbeen a tendency on the part of BCC plannersover the last three decades to use programposters, despite the fact that they are oftenexpensive to produce, work best only insophisticated multimedia campaigns, andprovide only reminder information. A com-mitment to community-based, participatoryprogramming has at times led other BCCplanners to overprogram community dramas,puppetry, and folk media. These media, while
certainly of interest to individual communi-ties, are expensive and difficult to manage ona large scale. The point is not to excludeeither posters or community-based media,but to ensure that if used they are cost-effec-tive; that is, relative to the investments in cashand management costs, they will have a sig-nificant impact on behavior change.
• The design of all media should reflect thestrategic principles articulated in the BCCStrategic Plan. There should be a focus onlyon priority messages, and each mediumshould respect only one unique selling prin-ciple—the communication strategy recom-mended in the plan. Of course, every medi-um is different in terms of nature and utility:A poster is simple and declaratory with strik-ing graphics and text, a brochure providesmore textual materials and some illustrations,and a community drama incorporates localfolklore and traditions. Nevertheless, allmedia should promote the same prioritypractices and use the same communicationstrategies as presented in the plan.
If a program manager, based on qualitativeresearch and strategic planning, decides topromote immediate breastfeeding by focus-ing on its role in easing/hastening delivery ofthe placenta, this focus should be retainedthroughout the campaign. Although otheradvantages of breastfeeding may supplementthis unique selling principle, the emphasis onthis initial message must be maintained.Similarly, if another program chooses tofocus on the nutritive qualities of breastmilk, that message should be the focusthroughout the BCC campaign.
• The design of individual media should bebased on creative thinking. Once the BCCStrategic Plan has established the prioritypractices to be stressed, the communication
310496.Text.qxd 7/9/2004 8:29 PM Page 37

38 Qualitative Research to Improve Newborn Care Practices
strategies to be applied, and the types ofmedia to be programmed, program managersmust then design each medium. While thequalitative research will in some cases pro-vide useful data to guide this process (i.e.,information on hopes, aspirations, expecta-tions, concerns, fears, etc.—the staples ofcommercial advertising), in most cases it willnot. Therefore, the program manager shouldrecruit those communication agencies withthe most creative and innovative personnel.A creative professional is one who: a) under-stands the audience from previous salesexperience, b) can easily review, understand,and assimilate qualitative research data toglean insights about product/service appeal,and c) can follow instincts and suggest cre-ative designs that still remain within prevail-ing sociocultural norms.
While not every country has a highly devel-oped advertising or marketing industry, mosthave professionals with at least some relevantcommercial or social experience. During thecompetitive bidding process that characterizesmost subcontracting, the program managersshould be particularly attentive to the creativeexperience of proposed staff; this experienceshould be documented and available.
• Media production should be as professionalas possible, within cost constraints. The mostcreative media designs can be wasted by infe-rior production. Although production isoften expensive, once cost-effective mediahave been selected, sufficient investmentshould be made to assure quality, attractive-ness, and appeal.
IPC Training
The development of IPC training materials issimilar to the design and development ofmedia, for every training course should incor-porate the strategic principles generated from
qualitative research and included in the BCCStrategic Plan.
IPC agents are those community-based and facil-ity-based personnel responsible for the dissemi-nation of information about ENC. They may bedoctors and nurses at a health care facility. Theymay be midwives or TBAs. They may be villagevolunteers with no health training, but with expe-rience in health promotion.
These IPC agents should be trained in the following:
• Priority practices: IPC agents should fullyunderstand which practices are to be pro-moted, why they are important, and how theycontribute to newborn health.
• Current practices: It is important for IPCagents to fully understand the current prac-tices they are dealing with—the point ofdeparture for behavior change.
• Constraints: IPC agents must know whyclients have not yet changed their behavior,and why it may be difficult to change.
• Communication strategy: Community IPCagents should be trained in the communica-tion strategies enunciated in the StrategicPlan, for it is on the basis of these strategiesthat they will develop individualized familybehavior change programs.9
• Case histories and negotiated behaviorchange planning: In order to be effective inthe field, every IPC worker should be trainedin the essentials of taking reliable case histo-ries—eliciting and recording informationabout how mothers and families have prac-ticed ENC in the past—and in developingnegotiated behavior change plans. These plansidentify the degree to which a family is willingto change over a given time period; they areessential for establishing the IPC workplan.
310496.Text.qxd 7/9/2004 8:29 PM Page 38

After the Research 39
• Work planning and management: Althoughan IPC worker may be well trained, an essen-tial key to ultimate behavior change is man-agement—how to develop a reasonable andrealistic workplan, and how to work effec-tively and efficiently within this supervisoryand management plan.
Conclusion
Qualitative research assists program managersand researchers in developing effective, feasible,and acceptable BCC strategies to improve new-born care practices. It allows for the commonor "normal" practice to be identified and thegap between that practice and the evidence-based or "best" practice to be recognized. Oncethe causes of this gap have been identified, therelevant constraints can be probed, understood,and finally modified.
In Nepal, SNL used in-depth qualitativeresearch findings to create a BCC strategyfocusing on priority behaviors - such asdelayed bathing for prevention of hypother-mia- and disseminated these messages throughradio vignettes, community dramas, and indi-vidual and group counseling. The midtermresults of Nepal's program in the KailaliDistrict, showing an increase in delayedbathing (for at least 24 hrs) from 7% to 68%in less than 2 years, provides an example ofthe insight that qualitative research can give tochanging behavior, even with those practicesmost resistant to change. Similar success indelaying bathing has been reported in theSylhet District of Bangladesh, after researchersundertook a well-designed formative researcheffort, as outlined in this guide.
Pakistan's maternal and neonatal tetanus elimi-nation program - involving the extremelyeffective tetanus toxoid immunization - was
not successfully implemented or utilized untilthe focus was taken off the campaign's logis-tics and put on demand creation.10 SNL's qual-itative research found that the demand prob-lem was due not only to restrictions onwomen's mobility, but also to lack of supportby fathers, husbands, mothers-in-law, and com-munity leaders, whose involvement turned outto be absolutely essential for the campaign.
After conducting qualitative research throughfocus groups in two randomly selected dis-tricts, SNL took the lessons learned to design ademand-generating program where, instead ofbeing administered by male service providers,the three doses were administered by ladyhealth workers, door-to-door. The campaignbegan by raising awareness among the numer-ous decision-makers, and also respected thecultural norms of privacy. As a result, nationalcoverage increased dramatically in just twoyears- exceeding the 80 percent target.
Not every practice will, even after thoroughqualitative research, be amenable to change tomatch the evidence-based practice, but themore aspects of essential newborn care thatcan be successfully integrated into thewoman's and her family's decisions andactions - through the antenatal, intrapartum,or postnatal periods - the more likely that thehealth of the newborn and mother willimprove. Moreover, change is likely to occurincrementally from current to best practices.Admittedly, qualitative research and a success-ful BCC strategy are only a small part ofimproving newborn health. Families overcom-ing economic, social, and informational barri-ers to embrace new ENC practices, thoughnecessary, must also be complemented byknowledgeable health workers, accessible serv-ices, and adequate supplies.
310496.Text.qxd 7/9/2004 8:29 PM Page 39

Directory of Qualitative Research Manuals
Winch, Peter, Jennifer Wagman, Rebecca Malouin, and Garrett Mehl. January 2000. QualitativeResearch for Improved Health Programs: A Guide to Manuals for Qualitative and Participatory Research onChild Health, Nutrition, and Reproductive Health. Support for Analysis and Research in Africa (SARA)project, USAID, Bureau for Africa, Office of Sustainable Development. Available from Website:<http://webdrive.jhsph.edu/pwinch/PWinch_Qual_manuals.pdf>.
Qualitative Research Manuals
Aubel, Judi. 1993. Qualitative Research for Improved Health Program Design: Guidelines for Studies for Usingthe Group Interview Technique. Development Policy Department, International Labor Office, Geneva,Switzerland. Available in English, Spanish, and French. Email: [email protected] or Fax: (41) 227996111.
Debus, Mary. 1988. The Handbook for Excellence in Focus Group Research. Academy for EducationalDevelopment/HEALTHCOM. Available in English, Spanish, and French. BASICS InformationCenter, 1600 Wilson Boulevard, Suite 300, Arlington, VA 22209. Phone: (703) 312 6800, Fax: (703)312 6900, or Email: [email protected]; or Academy for Educational Development, 1825Connecticut Avenue NW, Washington, DC 20009, Phone: (202) 884 8118, Fax: (202) 884 8491, orEmail: [email protected] or [email protected].
Nachbar, Nancy, et al. Assessing Safe Motherhood in the Community: A Guide for Formative Research. 1998.MotherCare/John Snow, Inc. 1616 N. Fort Myer Drive, 11th Floor, Arlington, VA 22209, Phone:(703) 528 7474, Fax: (703) 528 7480, Email: [email protected], or Website:<http://www.jsi.com/intl/mothercare/PUBS/Assessment/cd_manual/index.htm>.
Weiss, William, and Paul Bolton. Training in Qualitative Research Methods for PVOs and NGOs (andCounterparts). 2000. Center for Refugee and Disaster Studies, The Johns Hopkins University Schoolof Public Health. 615 N. Wolfe Street, Baltimore, MD 21205. Phone: (443) 287-7277.Available from Website: <http://www.jhsph.edu/refugee/resources.html>.
APPENDIX: QUALITATIVE RESEARCH RESOURCES
40 Qualitative Research to Improve Newborn Care Practices
310496.Text.qxd 7/9/2004 8:29 PM Page 40

Notes 41
1. Bhutta ZA, Darmstadt GL, and Hassan B. Community-Based Interventions for Improving Perinatal andNeonatal Outcomes in Developing Countries: A Review of the Evidence. Submitted to Pediatrics (suppl.); in press.
2. Opportunity cost is the value of productive labor lost due to behavior change.3. A prelacteal feed is a substance that is given before breastfeeding is initiated.4. The focus of this guide is on demand. It does not address in detail the various supply factors
that influence behavior change, such as the availability and accessibility of quality services, drugs,or other health products.
5. Marsh DR, Darmstadt GL, Moore J, Daly P, Oot D, and Tinker A. “Advancing NewbornHealth and Survival in Developing Countries: A Conceptual Framework.” J. Perinatology 22 (2002):572-576.
6. A skilled birth attendant is a person with midwifery skills (for example, a doctor, midwife, ornurse) who has been trained in the skills necessary to provide competent care during pregnancyand childbirth. If a woman does not have access to a skilled attendant, at a minimum she shouldseek an attendant trained in the evidence-based practices recommended in this guide. Based onReduction of maternal mortality, A Joint WHO/UNFPA/UNICEF/World Bank Statement (Geneva:WHO, 1999).
7. See the Directory of Qualitative Research Manuals, in the Appendix.8. Communication approach developed by Save the Children – is based on the assumption that
negative behavior can be changed through a better understanding of the determinants of positivebehavior and the translation of that understanding into BCC messages.
9. Community IPC agents should also be trained in a number of practical aspects of BCC pro-grams such as workplanning, monitoring and evaluation, etc.
10. Ramussen, B and Ali, N. “Moblizing Demand for Maternal and Neonatal TetanusImmunization: Reaching Women in Pakistan.” Shaping Policy for Maternal and Newborn Health: ACompendium of Case Studies (Baltimore: JHPIEGO: 2003) 23-28.
NOTES
310496.Text.qxd 7/9/2004 8:29 PM Page 41

blank
310496.Text.qxd 7/9/2004 8:29 PM Page 42
Ronald P. Parlato
Ron Parlato has over 30 years of experience in international
development, specializing in behavior change communica-
tions.At CARE India, he designed and implemented one of
the first behavior change campaigns to address health and
social issues through social marketing. He has been a film
producer for youth media, designed and implemented forma-
tive research, and done both training and impact evaluation.
He was a staff member for the World Bank in the United
Nations Water and Sanitation Decade program; a Senior
Development Advisor for PATH in Ukraine; and from 2001
to 2003 was the Behavior Change Advisor for Saving New-
born Lives.
Gary L. Darmstadt
Dr. Gary L. Darmstadt is the Senior Research Advisor for
the Saving Newborn Lives initiative of Save the Children and
Assistant Professor in the Department of International
Health at Johns Hopkins University in Baltimore. He trained
in Pediatrics at Johns Hopkins and in dermatology at Stan-
ford University. He also completed training in pediatric infec-
tious diseases at the University of Washington, where he
was formally Assistant Professor in the Departments of
Pediatrics and Medicine. His research expertise includes
developing improved strategies for prevention, detection,
and management of bacterial neonatal infections, and pro-
moting healthy newborn care practices and management of
illness at the community level in developing countries.
Anne Tinker
Anne Tinker is the Director of the Saving Newborn Lives
initiative at Save the Children. She has over 25 years of
experience in health and population in over 35 countries,
with an emphasis on reproductive and child health. She is
on leave from the World Bank, where she has been a Lead
Health Specialist in the South Asia Region and the global
Human Development Network, and was previously a Global
Advisor on women's health and safe motherhood. She was
also Division Chief in the Office of Health, USAID. She holds
graduate degrees in international studies (Georgetown U.)
and public health (Johns Hopkins U.). She has authored many
articles and publications on women’s and children’s health.
ABOUT THE AUTHORS
310496.Cover.qxd 7/7/2004 11:19 PM Page 3
About Saving Newborn Lives Tools for Newborn Health Series
Newborn health care poses unique problems for health profes-sionals and program managers in developing countries, wheremost women deliver at home, and where health care for new-borns is virtually non-existent. Improving household practices,introducing newborn health into pre- and in-service training forhealth workers at every level, and integrating newborn healthcare in the home and community with care in the facility require“fine-tuning” of established methodologies. In shaping solutionsfor the context of newborn health, Saving Newborn Lives hascome up with innovative approaches to qualitative research, eval-uation methods, behavior change communication, and trainingtechniques that are precisely tailored to meet the challenges ofinstitutionalizing newborn health care.
The SNL Tools for Newborn Health Series is designed to sharethe innovative techniques used by SNL with policymakers, healthprofessionals, and others who are working to improve newbornhealth care in developing countries.
Volumes in the SNL Tools for Newborn Health series include:• Care for the Newborn:A Reference Manual• Qualitative Research to Improve Newborn Care Practices• Social Mobilization for MNT: Guidelines for
Immunization Campaigns
SAVING NEWBORN LIVESSave the Children/US2000 M Street NWSuite 500Washington, DC 20036www.savethechildren.org
310496.Cover.qxd 7/9/2004 8:26 PM Page 4