Use of this content is subject to the Terms and Conditions
Yeo: Shackelford's Surgery of the Alimentary Tract, 6th
ed.Copyright 2007 Saunders, An Imprint of Elsevier
Chapter 78 Short-Bowel Syndrome Jon S. Thompson Alan N. Langnas
Intestinal failure refers to a condition that results in inadequate
digestion or absorption of nutrients, or both, so that an
individual becomes malnourished and requires specialized medical
and nutritional support.[1] Short-bowel syndrome is a type of
intestinal failure caused by a shortened remnant after intestinal
resection. The pathophysiologic changes that occur in short-bowel
syndrome relate primarily to the loss of intestinal absorptive
surface and more rapid intestinal transit ( Box 781 ). The
consequences of malabsorption of nutrients include malnutrition,
diarrhea, steatorrhea, specific nutrient deficiencies, and fluid
and electrolyte abnormalities. These patients are at risk for other
specific complications, including an increased incidence of
nephrolithiasis, cholelithiasis, and gastric hypersecretion. The
clinical manifestations of short-bowel syndrome vary greatly among
patients and depend on intestinal remnant length, location, and
function; the status of the remaining digestive organs; the
presence or absence of the ileocecal valve; and the adaptive
capacity of the intestinal remnant. Thus, short-bowel syndrome is
not entirely dependent on a given length of remaining intestine.
Box 78-1 Pathophysiologic Consequences of Massive Resection General
Malnutrition and weight loss
Diarrhea and steatorrhea
Vitamin and mineral deficiencies
Fluid and electrolyte abnormalities Specific Cholelithiasis
Gastric hypersecretion
Liver disease
Nephrolithiasis
The prevalence of short-bowel syndrome is 3 to 4 per million,
and thousands of patients are now surviving with short-bowel
syndrome.[1] This condition occurs in about 15% of adult patients
who undergo intestinal resection, with three fourths of these cases
resulting from massive intestinal resection and one fourth from
multiple sequential resections.[2] Massive intestinal resection
continues to be associated with significant morbidity and
mortality, primarily related to the underlying diseases
necessitating resection. [8] [9] About 70% of patients in whom
short-bowel syndrome develops are discharged from the hospital, and
a similar percentage are alive 1 year later.[4] This improved
survival rate has been achieved primarily by the ability to deliver
long-term nutritional support. The long-term outcome of these
patients is often determined not only by their age and underlying
disease but also by complications related to the management of
short-bowel syndrome. FACTORS INFLUENCING OUTCOME Intestinal
remnant length is the primary determinant of outcome in patients
with short-bowel syndrome. The length of the small intestine in
adults varies between 12 and 20 ft (360 to 600 cm), depending on
how it is measured and the height and sex of the individual. The
duodenum measures 10 to 12 inches (25 to 30 cm). The length of the
small intestine from the ligament of Treitz to the ileocecal
junction is about 16 ft (480 cm), with the proximal two fifths
being jejunum and the distal three fifths being ileum. Resection of
up to half of the small intestine is generally well tolerated.
Although short-bowel syndrome may develop in patients with less
than 180 cm of small intestine, or about a third the normal length,
permanent parenteral nutrition (PN) support is likely to be needed
in patients with less than 120 cm of intestine remaining without
colon in continuity and less than 60 cm remaining with colonic
continuity ( Table 78-1 ). [10] [11] Table 78-1 -- Intestinal
Length and Nutritional Prognosis Intestinal Anatomy Intestinal
Length to Avoid Permanent Parenteral Nutrition End-jejunostomy
(type 1) 100 cm
Intestinal Anatomy
Intestinal Length to Avoid Permanent Parenteral Nutrition
Jejunocolic anastomosis (type 2) 65 cm
Jejunoileocolic anastomosis 30 cm (type 3) Adapted from Messing
B, Crenn P, Beau P, et al: Long term survival and parenteral
nutrition dependence in adult patients with the short bowel
syndrome. Gastroenterology 117:1043, 1999.
The site of resection is also an important factor. Patients with
an ileal remnant generally fare better than those with a jejunal
remnant. The ileum has specialized absorptive properties for bile
salts and vitamin B12, unique motor properties, a hormone profile
different from that of the jejunum, and a greater capacity for
intestinal adaptation. [12] [13] The presence of the ileocecal
junction improves the functional capacity of the intestinal
remnant.[7] Although previously this had been attributed to a
barrier function and transit-prolonging property of the ileocecal
valve, this advantage may actually be related to the specialized
property of the terminal ileum itself. The status of the other
digestive organs also contributes to outcome. The stomach
influences oral intake, mixing of nutrients, transit time,
pancreatic secretion, and protein absorption. Pancreatic enzymes
are important in the digestive process and particularly influence
fat absorption. The colon absorbs fluid and electrolytes, slows
transit, and participates in the absorption of energy from
malabsorbed carbohydrates. When compared with an end-jejunostomy
(type 1 anatomy), a jejunoileal anastomosis with an intact colon
(type 3 anatomy) is equivalent to 60 cm of additional small
intestine, and a jejunocolic anastomosis (type 2 anatomy) is
equivalent to about 30 cm of small intestine.[5] A variety of
conditions requiring intestinal resection lead to short-bowel
syndrome ( Table 78-2 ).[8] Patients with underlying inflammatory
disease may have impaired intestinal function. The cause of
resection will also influence the outcome because of the effect on
other digestive organs. Long-term treatment and survival are
influenced by the patient's age and other morbid conditions.
Underlying disease will also influence these parameters. Table 78-2
-- Causes of Short-Bowel Syndrome Postoperative 52 (25%)
Irradiation/cancer 51 (24%)
Mesenteric vascular disease 46 (22%) Crohn's disease Other
benign causes 34 (16%) 27 (13%)
Total 210 From Thompson JS, DiBaise JK, Iver KR, et al: Short
bowel syndrome as a postoperative complication. J Am Coll Surg
201:85, 2005.
Copyright 2007 Elsevier Inc. All rights reserved. -
www.mdconsult.comBookmark URL: /das/book/0/view/1430/739.html
Use of this content is subject to the Terms and Conditions
Yeo: Shackelford's Surgery of the Alimentary Tract, 6th
ed.Copyright 2007 Saunders, An Imprint of Elsevier
INTESTINAL ADAPTATION The small intestine is able to adapt to
compensate for the reduction in absorptive surface area caused by
intestinal resection. [15] [16] [17] This process occurs within the
first year or two after resection and improves intestinal
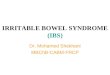
absorptive capacity ( Fig. 78-1 ). [11] Whether the adaptive
response can be significantly accelerated or augmented is not
clear. The overall intestinal adaptive response results from
changes in intestinal structure, function, and motility.
Figure 78-1 Schematic presentation of intestinal adaptation. AA,
accelerated adaptation; AHA, accelerated hyperadaptation; HA,
hyperadaptation; SA, spontaneous adaptation. (From Jeppesen PB:
Clinical significance of GLP-2 in short bowel syndrome. J Nutr
133:3721, 2003.)
Structural adaptation after intestinal resection involves all
layers of the intestine. [15] [16] Mucosal DNA and protein
synthesis and crypt cell proliferation are increased within hours
after resection. Both the total number of cells and the proportion
of proliferating cells are increased in the crypt. Enterocytes
migrate at a faster rate along the villus. Villus lengthening
occurs by an overall increased number of cells. Rates of apoptosis,
or programmed cell death, increase in both crypt and villus
enterocytes after resection. However, the proliferative stimulus
dominates, so adaptation occurs. The ratio of crypts to villi may
also increase. Microvilli along the epithelial surface increase as
well. Overall, mucosal weight increases. The thickness and length
of the muscle layers also increase after resection, primarily as a
result of hyperplasia rather than hypertrophy of the muscle
cells.[9] Muscle adaptation, however, occurs at a later time than
mucosal adaptation and only after more extensive resection. These
changes in the components of the intestinal wall
result in marked thickening of the intestinal wall, as well as
increased intestinal circumference and length. Thus, there is an
overall increase in mucosal surface area because of both villus
hypertrophy and the increases in length and circumference of the
remnant. Intestinal motor activity is also altered by intestinal
resection.[6] The canine small intestine demonstrates a biphasic
motor response to varying degrees of distal resection. There is
initial disruption of motor activity, followed by adaptation. In
the distal segment of the intestinal remnant after limited
resection and more generally after 75% resection, motility
recordings are initially dominated by recurring bursts of clustered
contractions.[12] With extensive resection, these clusters are
prolonged and associated with baseline tonic changes. With limited
resection, there is evidence of progressive motor adaptation with
eventual slowing of transit and return of migrating motor complex
(MMC) cycling. This adaptation is less apparent after massive
resection. Motor adaptation is more prominent in the jejunum than
in the ileum. These changes are accompanied by modest alterations
in smooth muscle contractility. Clinical reports also demonstrate a
biphasic adaptive motor response during the first year after
resection. There is disrupted motor activity in the first few
months after resection, but these changes occur only after
extensive resection (remnant shorter than 100 cm). Long-term human
studies demonstrate a shorter duration of the MMC cycle and fed
pattern after resection.[13] Functional adaptation has been well
documented after resection, [7] [11] [20] [21] and structural
adaptation increases intestinal absorptive surface area. Both
structural adaptation and motor adaptation lead to prolonged
transit time. Although the formerly accepted theory of improved
absorption by individual enterocytes was discounted, more recent
studies suggest that certain transport capabilities do improve.
Within months of resection, diarrhea diminishes and nutritional
status improves. The mechanism of intestinal adaptation has been
studied extensively but is still not entirely understood. The
degree of structural adaptation is related to the extent and site
of resection. [15] [16] Adaptation is greater with more extensive
resection, and the ileum has a greater adaptive capacity than the
jejunum does. Subsequent resection elicits a further adaptive
response. Luminal nutrients and secretions and growth factors are
important for achieving the maximal response but are not essential
for adaptation to occur ( Box 78-2 ). [15] [16] The early molecular
events associated with this hyperplastic response are being
investigated. [22] [23] Intestinal resection results in increased
levels of a variety of gene products in enterocytes within hours.
There is an immediate increase in genes that encode transcription
factors, not only genes that influence cell proliferation but also
those that augment nutrient trafficking, as well as heat shock
genes, which maintain normal cellular function. Many of these are
novel genes not normally present in intestinal epithelium. The
specific triggers for these events are not clear, and there are
obviously many candidates. Currently, there
is clinical interest in manipulating the adaptive response
pharmacologically. Box 78-2 Factors Influencing Intestinal
Adaptation
Gastrointestinal regulatory peptides
Luminal contents
Nutrients
Secretions
Systemic factors
Growth factors
Hormones
Cytokines
Tissue Factors
Immune system
Mesenchymal factors
Mesenteric blood flow
Neural influencesCopyright 2007 Elsevier Inc. All rights
reserved. - www.mdconsult.comBookmark URL:
/das/book/0/view/1430/740.html
Use of this content is subject to the Terms and Conditions
Yeo: Shackelford's Surgery of the Alimentary Tract, 6th
ed.Copyright 2007 Saunders, An Imprint of Elsevier
MEDICAL MANAGEMENT The early management of a patient with
short-bowel syndrome is that of a critically ill surgical patient
who has recently undergone intestinal resection and other
concomitant procedures. Thus, control of sepsis, maintenance of
fluid and electrolyte balance, and initiation of nutritional
support are important in the early management of these patients.
For patients who have survived this early phase, the primary goals
of management are to maintain adequate nutritional status, maximize
the absorptive capacity of the remaining intestine, and prevent the
development of complications related to both the underlying
pathophysiology and the nutritional therapy. Maintain Nutritional
Status The most important therapeutic objective in the management
of short-bowel syndrome is to maintain the patient's nutritional
status. This usually requires PN support in the early period after
surgery. Fluid and electrolyte losses from the gastrointestinal
tract may be great during the early postoperative period and must
be monitored and replaced as soon as possible. Enteral nutritional
support should be started as soon as possible when the ileus has
resolved. With time, an increasing amount of nutrients are absorbed
by the enteral route. This is important for maximizing intestinal
adaptation and preventing complications related to PN. As their
condition improves and intestinal adaptation occurs, many patients
can absorb the necessary nutrients entirely by the enteral route.
The length of the intestinal remnant and the status of the colon
have important prognostic implications in this regard (see Table
78-1 ). The ability of patients with short-bowel syndrome to
maintain adequate caloric intake enterally is determined by a
variety of factors, including intestinal remnant length and
location, any underlying intestinal disease, and the status of the
remaining digestive organs. [21] [24] Whether there is continuity
in the intestinal tract or
a stoma is also an important consideration. Diarrhea and
perianal complications may markedly diminish oral intake. Patients
with stomas are more likely to have a greater percentage of their
calories taken enterally. Hyperphagia develops in many patients
with short-bowel syndrome to overcome inefficient absorption.[19]
Many patients with short-bowel syndrome require long-term PN for
survival, and this therapy has considerable expense and morbidity.
Patients without malignancy have 1-, 3-, and 5-year survival rates
of about 90%, 70%, and 60%, respectively.[4] One third of deaths
are related to the underlying disease, 50% to other supervening
disease, and 10% to 15% to PN therapy. Sepsis and liver disease
related to PN are important factors in long-term survival. The
incidence of sepsis varies from 0.1 to 0.3 episodes per patient
year of PN. Sepsis may be associated with catheter thrombosis. The
need for prolonged therapy makes vascular access a long-term
problem, and catheters may eventually need to be placed in the
azygos, hepatic, or inferior vena cava veins. End-stage liver
disease develops in about 15% of long-term adult PN patients and is
associated with a survival time of about 1 year without liver
transplantation. [26] [27] Although the etiology of the liver
disease is not completely understood, it appears to be a
multifactorial process that is initially reversible but ultimately
leads to severe steatosis, cholestasis, and cirrhosis. Liver
disease occurs more frequently in children than adults. Provision
of enteral nutrients may prevent this problem, but overfeeding is a
predisposing factor. Control of sepsis and bacterial overgrowth is
important to minimize this liver disease. Patients with abnormal
liver function test results while receiving PN should undergo
abdominal ultrasound for evaluation of the gallbladder and bile
ducts and should have a liver biopsy performed as
appropriate.Copyright 2007 Elsevier Inc. All rights reserved. -
www.mdconsult.comBookmark URL: /das/book/0/view/1430/741.html
Use of this content is subject to the Terms and Conditions
Yeo: Shackelford's Surgery of the Alimentary Tract, 6th
ed.Copyright 2007 Saunders, An Imprint of Elsevier
Maximize Enteral Nutrient Absorption Because the morbidity
associated with nutritional support in patients with shortbowel
syndrome is related primarily to PN, maximizing enteral absorption
of nutrients is important for long-term survival. Furthermore,
diarrhea and stomal fluid losses can also be important clinical
problems that affect the patient's quality of life. Thus, it is
beneficial to ensure that the patient's intestinal remnant is
functioning optimally and absorbing nutrients and fluid. The
optimal diet for patients with short-bowel syndrome remains
controversial.
Provision of nutrients in their simplest form to minimize
digestion has been one strategic approach. Simple sugars and
dipeptides and tripeptides are rapidly absorbed from the intestinal
tract. However, partially hydrolyzed diets appear to be just as
effective and are less expensive. Complex carbohydrates reduce the
osmotic load, but concentrated sugars, such as fruit juices, should
be avoided because they generate a high osmotic load. Whether the
diet should have a high-fat or low-fat content is another issue.
There appears to be increasing agreement that patients with colon
should have a low-fat (20% to 30% of calories), high-carbohydrate
(50% to 60% of calories) diet but that patients with an
end-enterostomy do not require fat restriction (30% to 40% of
calories). Fat absorption obviously requires more digestion unless
the fat is supplied in the form of medium-chain triglycerides. The
ability to absorb these nutrients improves with time, so the diet
may need to be continually modified. Specific problems such as
lactase deficiency are often present, and the diet should be
altered appropriately. Ingestion of a glucose-electrolyte oral
rehydration solution with a sodium concentration of at least 90
mmol/L will optimize water and sodium absorption in the proximal
jejunum and prevent secretion into the lumen. Minimizing
gastrointestinal secretions and controlling diarrhea are also
important goals for maximizing absorption. Both histamine H2
receptor antagonists and proton pump inhibitors are effective in
controlling gastric hypersecretion, correcting malabsorption, and
improving nutritional status in patients with short-bowel syndrome.
Furthermore, cimetidine may also increase intestinal adaptation.
Somatostatin and its long-acting analogue octreotide have been
investigated for the management of severe refractory diarrhea in
short-bowel syndrome. They improve diarrhea by prolonging small
intestinal transit time and reducing salt and water excretion. Part
of the beneficial effect may also be related to a reduction in
gastric hypersecretion. Although these therapeutic agents are
beneficial in the short term, it is not clear whether they continue
to be effective after a few months, and they may have some
potential deleterious effects. Somatostatin may exacerbate
steatorrhea because of impaired pancreatic exocrine function. Other
potential adverse effects of octreotide are inhibition of
intestinal adaptation and the development of cholelithiasis. Recent
evidence supports the use of ox bile and cholylsarcosine, a
synthetic conjugated bile acid, as replacement therapy because they
improve fat absorption without exacerbating diarrhea. Another
important aspect of dietary management is to provide a diet that
will maximize the intestinal adaptive response. [15] [16] [24]
Provision of fat and dietary fiber may be particularly important in
this regard. Long-chain and short-chain fatty acids appear to have
a greater trophic effect on the intestine than medium-chain fatty
acids do. Although these nutrients directly stimulate intestinal
adaptation, nutrients also stimulate intestinal adaptation through
endocrine and paracrine effects. Pharmacologic therapy for
short-bowel syndrome is a rapidly expanding area of
investigation. Recent evidence suggests that provision of the
appropriate diet, nutritional supplements such as glutamine, and
growth factors such as growth hormone improves intestinal
absorption and perhaps modifies the adaptive response in patients
with established short-bowel syndrome.[22] However, which of these
components is actually responsible for improved absorption is
controversial. Growth hormone and glutamine do not have a
consistent beneficial effect. [29] [30] Currently, glucagon-like
peptide-2 appears to have the most promise for promoting absorption
and adaptation.[11] Epidermal growth factor also stimulates
intestinal adaptation and may soon be studied in clinical
trials.[25] An important clinical issue is whether to establish
intestinal continuity in patients who have a colonic remnant. There
are both advantages and disadvantages to restoring continuity ( Box
78-3 ). The colon may improve intestinal absorption by increasing
the absorptive surface area, deriving energy from short-chain fatty
acids, and prolonging transit time, particularly if the ileocecal
valve is intact. Avoiding a stoma also improves quality of life.
However, the response of the colon to luminal contents is somewhat
unpredictable. Bile acids may cause a secretory diarrhea. Perianal
problems can be quite disabling and decrease the patient's oral
intake. Oxalate is absorbed primarily in the colon, and restoring
continuity places the patient at increased risk for the formation
of calcium oxalate stones. Serum and intestinal fluid markers have
been investigated as a means of predicting the response of the
individual patient to restoring continuity, but none is generally
available and useful. Distal reinfusion of enteral contents into a
mucus fistula to assess the functional outcome has some usefulness,
but it is cumbersome. Not all patients who initially have a stoma
created eventually have continuity restored with a satisfactory
outcome.[26] This decision should be considered on an individual
basis and depends on the length of the intestinal remnant, the
status of the ileocecal valve and the colon, and the patient's
overall condition. Generally, at least 3 ft of small intestine is
required to prevent severe diarrhea and perianal complications.
Restoring continuity, however, should always be given strong
consideration because of possible improvement in absorption. Box
78-3 Restoration of Intestinal Continuity Advantages Absorptive
capacity increased
Energy absorbed from short-chain fatty acids
Infectious complications reduced
Transit time prolonged
Stoma avoided Disadvantages Bile acid diarrhea
Dietary restrictions
Nephrolithiasis increased
Perianal complications From Thompson JS: Intestinal resection
and the short bowel syndrome. In Quigley EMM, Sorrell MF (eds):
Medical Management of the Gastrointestinal Surgery Patient.
Baltimore, Williams & Wilkins, 1994, p 327.Copyright 2007
Elsevier Inc. All rights reserved. - www.mdconsult.comBookmark URL:
/das/book/0/view/1430/742.html
Use of this content is subject to the Terms and Conditions
Yeo: Shackelford's Surgery of the Alimentary Tract, 6th
ed.Copyright 2007 Saunders, An Imprint of Elsevier
Prevent Complications Metabolic complications are common in
patients with short-bowel syndrome because of their tremendous
fluid and electrolyte losses and the need to replace these losses
with specialized solutions. Intravascular volume has to be
maintained to prevent dehydration and renal dysfunction.
Hypocalcemia is a common problem related to poor absorption and
binding by intraluminal fat. Maintaining adequate calcium and
magnesium levels and vitamin D supplementation are important to
minimize bone disease. Hyperglycemia and hypoglycemia are
frequent
complications of patients receiving a large amount of their
calories parenterally. Both metabolic acidosis and metabolic
alkalosis can occur. A specific problem is dlactic acidosis, which
results from bacterial fermentation of unabsorbed nutrients,
particularly simple sugars. Lactate reduces colon pH, thereby
permitting the growth of acid-resistant anaerobes capable of
producing d-lactate. Impaired metabolism of d-lactic acid may also
contribute to elevated serum d-lactic acid levels. This diagnosis
is suggested by an unexplained metabolic acidosis and associated
neurologic symptoms, such as confusion and somnolence. d-Lactic
acid is not measured by standard laboratory techniques for lactic
acid determination. Thus, an increased anion gap but normal lactate
level in the appropriate clinical setting mandates measurement of
d-lactic acid. d-Lactic acidosis is treated by minimizing overall
caloric intake or by instituting a low-carbohydrate diet.
Administration of intestinal antibiotics may be appropriate, but
the optimal duration of such treatment is unclear, and recurrence
rates are significant. Specific nutrient deficiencies need to be
prevented and monitored closely, including iron and vitamin
deficiencies, as well as deficiencies in micronutrients such as
selenium, zinc, and copper. Because fat is poorly absorbed, fatty
acid deficiency can also occur. Although medium-chain fatty acids
can supplement the diet enterally, parenteral lipids are required
in patients who depend primarily on that route. Serum free fatty
acid levels and triene-to-tetraene ratios may need to be monitored
periodically to determine the need for supplementation and response
to treatment. In general, enteral intake must greatly exceed the
absorptive needs to ensure that these needs are being met.
Catheter-related sepsis is an important problem that often
necessitates rehospitalization and replacement of catheters.
Attention to technique and meticulous patient education are
important to prevent this complication. Most infections are due to
Staphylococcus species, but gram-negative bacteria and fungi are
also associated with line sepsis. An attempt at line sterilization
before removal is appropriate when infections are caused by
coagulase-negative staphylococci and gram-negative bacteria.
Repeated placement of catheters can lead to catheter thrombosis,
which is the other common problem. In patients who require PN
permanently, this may become an important factor in the patient's
survival because vascular access may not be achievable
indefinitely. PN-induced liver disease is another potential
long-term problem. [26] [27] It can be minimized by providing as
large a portion of the calories as possible enterally, avoiding
overfeeding, using mixed fuels (less than 30% fat), and preventing
specific nutrient deficiencies. Treating bacterial growth and
preventing recurrent sepsis are also important. Ursodeoxycholic
acid administration may likewise be beneficial. Bacterial
overgrowth is another long-term complication associated with both
intestinal disease and resection. It may result from impaired
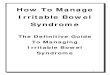
motility or stasis caused
by obstructive lesions ( Fig. 78-2 ). Achlorhydria is also a
contributing factor. Bacterial deconjugation of luminal bile salts
impairs bile salt reabsorption. Bacteria also metabolize
intraluminal vitamin B12. Depending on the bacterial species
present, secretory diarrhea may occur as well. Bacterial overgrowth
requires a high degree of suspicion to make the diagnosis. This
complication should be suspected when a patient's absorptive
capacity and stool habits change acutely. It may result from a
mechanical obstruction or a blind loop, which can be relieved by
surgery. However, it is often a primary motor abnormality and
requires intermittent therapy with antibiotics. Colonization of the
lumen with acidophilus or other nonpathogenic organisms is another
potential therapy.[27]
Figure 78-2 Contrast study of a patient with short-bowel
syndrome. The shortened remnant lies primarily in the
left side of the abdomen with a large dilated segment in the
pelvis. Contrast has passed into the right colon beyond this
area.
Cholelithiasis occurs in 30% to 40% of patients with intestinal
insufficiency. [34] [35] Factors that predispose these patients to
gallstone formation include altered hepatic bile metabolism and
secretion, gallbladder stasis, and malabsorption of bile acids.
Depending on the dominant mechanism, either mixed pigment stones or
cholesterol stones may occur. Long-term PN is an important
contributing factor causing altered hepatic bile metabolism and
gallbladder stasis. Patients receiving PN are susceptible to the
development of cholelithiasis and hepatocellular dysfunction and
thus require careful clinical evaluation. [34] [35] Biliary sludge
forms within a few weeks of initiating PN if there is no enteral
intake, but it rapidly disappears when enteral nutrition is
resumed. Intestinal mucosal disease and resection, particularly of
the ileum, cause bile acid malabsorption, which leads to lithogenic
bile and the formation of cholesterol stones. The risk for
cholelithiasis is significantly increased if less than 120 cm of
intestine remains after resection, the terminal ileum has been
resected, and PN is required. The incidence of cholelithiasis can
be minimized by providing nutrients enterally whenever possible.
Patients totally dependent on PN may be treated with intermittent
cholecystokinin injections to prevent stasis and the formation of
sludge. Administration of intravenous lipids also stimulates
gallbladder emptying. Cholelithiasis may lead to complications in a
higher number of patients with short-bowel syndrome than in the
general population and also requires more complicated surgical
treatment. Thus, several authors now recommend prophylactic
cholecystectomy in these patients when laparotomy is being
undertaken for other reasons.[29] Nephrolithiasis also occurs with
some frequency. Calcium oxalate stones form as a result of
increased oxalate absorption from the colon.[29] Oxalate is
normally bound to calcium in the intestinal lumen and is not
absorbed. Decreased availability of calcium secondary to reduced
intake or binding by intraluminal fat leaves free oxalate in the
lumen. Thus, the oxalate is absorbed in the colon and forms calcium
oxalate in the urine. Nephrolithiasis is unusual in patients after
intestinal resection and jejunostomy but occurred in a fourth of
such patients with an intact colon within 2 years of resection.
Nephrolithiasis can be prevented by maintaining a diet low in
oxalate, minimizing intraluminal fat, supplementing the diet with
calcium orally, and maintaining a high urinary volume. Foods with
high oxalate content include chocolate, tea, cola, spinach, celery,
carrots, and other fruits and vegetables. Cholestyramine, which
binds oxalic acid in the colon, is another potential treatment.
Gastric hypersecretion is a potential problem in patients with
short-bowel syndrome. Massive intestinal resection can cause
gastric hypersecretion as a result of parietal cell hyperplasia and
hypergastrinemia. This phenomenon is usually transient and
lasts several months. The etiology has not been elucidated but
may involve loss of an inhibitor from the resected intestine. The
associated hyperacidity exacerbates malabsorption and diarrhea.
Clinical development of peptic ulcer disease may also occur and is
seen in about a fourth of patients undergoing massive
resection.[26] Treatment of gastric acid secretion may improve
absorption but also prevents peptic ulcer disease. Control of acid
secretion by H2 receptor antagonists or proton pump inhibitors
should be initiated in the perioperative period after resection and
maintained until the increased acid production resolves. Some
patients, however, continue to have symptoms of peptic ulcer
disease that eventually require surgical intervention. Gastric
resection therapy should be avoided when possible. A highly
selective vagotomy may be the most desirable procedure if
feasible.Copyright 2007 Elsevier Inc. All rights reserved. -
www.mdconsult.comBookmark URL: /das/book/0/view/1430/743.html
Use of this content is subject to the Terms and Conditions
Yeo: Shackelford's Surgery of the Alimentary Tract, 6th
ed.Copyright 2007 Saunders, An Imprint of Elsevier
SURGICAL MANAGEMENT The primary goal of surgical therapy for
short-bowel syndrome is to increase intestinal absorptive capacity,
which can be achieved either by improving absorption by existing
intestine or by increasing the area of absorption ( Box 78-4 ).
Recruiting additional intestine into continuity, relieving
obstruction, or slowing intestinal transit will often improve
absorption. The intestinal lengthening procedure is feasible in
selected patients. The most significant increase in length,
however, is potentially achieved by intestinal transplantation. The
choice of surgical therapy for shortbowel syndrome is influenced by
intestinal remnant length and caliber and the clinical condition of
the patient ( Table 78-3 ).[3] Box 78-4 Surgical Strategies for
Short-Bowel Syndrome
Preserve and maximize remnant
Avoid resection
Restore continuity
Recruit additional intestine
Improve intestinal function
Relieve obstruction
Taper dilated bowel
Slow intestinal transit
Increase absorptive area
Intestinal lengthening
Intestinal transplantation
Table 78-3 -- Surgical Approach to Short-Bowel Syndrome
Intestinal Remnant Clinical Condition Surgical Options Adequate
length with Enteral nutrition (remnant Optimize intestinal
function, normal diameter >120 cm in adults, >60 recruit
additional length cm in children) Adequate length with dilated
bowel Bacterial overgrowth, stasis Treat obstruction, intestinal
tapering Recruit additional length, reversed intestinal segment,
artificial valve, colon interposition Optimize intestinal
function
Marginal length with normal Rapid transit, need for diameter
(remnant 60-120 parenteral nutrition cm in adults, 30-60 cm in
children) Short length with normal diameter (remnant