Embed Size (px)
Citation preview

Review Current thoughts on thepathogenesis of pre-eclampsiaAuthors Rebekah A Smith / Louise C Kenny
Pre-eclampsia remains a leading cause of maternal and perinatal
morbidity and mortality. In this review we examine the leading
hypotheses of the pathogenesis of this disorder and discuss recent
research in this area that has led to the exciting prospect of new
treatments for this devastating condition.
Keywords maternal mortality / pathogenesis / pre-eclampsia
Please cite this article as: Smith RA, Kenny LC. Current thoughts on the pathogenesis of pre-eclampsia. The Obstetrician & Gynaecologist 2006;8:7–13.
Author details
Rebekah A Smith MRCOG
Clinical Research Fellow
Maternal and Fetal Health Research Centre,
St Mary’s Hospital, Whitworth Park, Manchester
M13 0JH, UK
E-mail: [email protected] (corresponding
author)
Louise C Kenny PhD MRCOG
Senior Lecturer and Consultant Obstetrician
St Mary’s Hospital, Manchester, UK
The Obstetrician & Gynaecologist 10.1576/toag.8.1.007.27202 www.rcog.org.uk/togonline 2006;8:7–13 Review
’ 2006 Royal College of Obstetricians and Gynaecologists 7

IntroductionPre-eclampsia occurs in approximately 2% of
pregnancies and is associated with significant
maternal and perinatal mortality and morbidity.
Worldwide, 40 000 women die each year with pre-
eclampsia and eclampsia. In the 2004 report of the
Confidential Enquiries into Maternal Deaths in
the UK,1 hypertensive disorders of pregnancy were
second only to thromboembolism, accounting for
14 deaths. The Confidential Enquiry into
Stillbirths and Deaths in Infancy (CESDI) report
cites one in six stillbirths as occurring in
pregnancies complicated by maternal
hypertension.2 The condition is also responsible
for the occupancy of approximately 20% of special
care baby unit cots. Furthermore, pre-eclampsia
carries significant healthcare implications in adult
life, with offspring of affected pregnancies having
an increased risk of hypertension, heart disease
and diabetes.
Treatment of pre-eclampsia is now, as it has been
for the last 100 years, delivery of the fetus and
placenta. Consequently, part of the increased
perinatal mortality is due to iatrogenic
prematurity. It is estimated that 15% of preterm
births are secondary to delivery for pre-eclampsia.
The aetiology of this condition has remained
elusive for many centuries. However, there is now
a growing body of research in this area and in
recent years new insights into the pathogenesis of
this condition have provided the tantalising
prospect of the development of novel therapeutic
strategies.
Predisposing factors for pre-eclampsiaThere are many risk factors that increase a
woman’s chance of developing pre-eclampsia
(Box 1). A significant factor underlying the
condition is a genetic predisposition. The risk of
pre-eclampsia for women whose mother or sister
has had pre-eclampsia is increased 2–3 fold.
Further substantial risk factors for developing pre-
eclampsia are chronic medical conditions, such as
chronic hypertension, diabetes and collagen
vascular diseases. These conditions have an
underlying microvascular component that can be
associated with a reduction in placental blood
flow, which may precipitate pre-eclampsia.
Theories of pathogenesisThere is now a general consensus regarding the
individual stages in the pathogenesis of pre-
eclampsia. However, debate continues about the
primary precipitating factor. In recent years two
different theories have emerged.
(1) The two-stage process
In this theory it is suggested that the trigger in the
disease process is relative reduction in placental
blood flow secondary to either abnormal
placentation or maternal microvascular disease.
The poorly perfused placenta is thought to release
circulating factor(s) that target the maternal
vascular endothelium and lead to the clinical
syndrome (Figure 1).3 In this model, maternal
factors that antedate pregnancy lead to an
increased susceptibility to the disease and part of
the response to reduced placental perfusion is
thought to be a fetal adaptive response to attempt
to overcome the reduced delivery of nutrients.
This theory is supported by the observation that
not all babies born to mothers with pre-eclampsia
have intrauterine growth restriction and that there
is evidence of abnormal placentation in women
who do not have pre-eclampsia.
(2) Continuum theory
This theory proposes that pre-eclampsia is an
exaggerated form of the inflammatory response
characteristic of normal pregnancy. It is suggested
that this occurs in response to a relative increase in
trophoblastic debris, which is released from a
poorly perfused placenta or from a larger placental
mass; for example, in multiple pregnancies. The
exaggerated inflammatory reaction can also be
triggered by a normal amount of trophoblastic
debris in susceptible women (Figure 2).4
Reduced placental perfusionThe pivotal role of the placenta in the
pathogenesis of pre-eclampsia has been established
by several clinical observations. Firstly, it has long
been recognised that removal of the placenta leads
to resolution of the disease and indeed this
remains the mainstay of current clinical
management. Secondly, pre-eclampsia can occur
Box 1Risk factors for developingpre-eclampsia
Risk Factors Examples
Socio-demographicfactors
Extremes of reproductiveage, e.g. age .40 years
Socio-economic statusEthnic group: African–
AmericanGenetic factors Sister had pre-eclampsia
Mother had pre-eclampsiaPartner previously fathered
pregnancy complicatedby pre-eclampsia
Pregnancy factors Multiple pregnanciesPrimigravidaePrevious pre-eclampsia
Personal medical history ObesityChronic renal diseaseChronic hypertensionDiabetes mellitusThrombophilia
Review 2006;8:7–13 The Obstetrician & Gynaecologist
8 ’ 2006 Royal College of Obstetricians and Gynaecologists

in the absence of a fetus. Indeed hydatidiform
moles are associated with an increased incidence
of pre-eclampsia. Finally, the incidence of pre-
eclampsia is increased in pregnancies associated
with hyperplacentosis, such as multiple pregnancy
and diabetes.
Thirty years ago, morphological examination of
placental bed biopsies and caesarean hysterectomy
specimens from women with pre-eclampsia
demonstrated shallow invasion of trophoblasts
and failure of vascular remodelling.5 Applications
of contemporary bioscientific approaches have
provided detailed insight into deficient
mechanisms in this process.
Within the placenta in early gestation,
trophoblasts differentiate and give rise to
subpopulations of cells. One subpopulation, the
extravillous trophoblast, invades the uterine wall
(interstitial invasion) and its blood vessels
(endovascular invasion). During normal
pregnancy, the trophoblasts destined to be
endovascular adopt a more endothelial, cell-like
phenotype and invade the uterine spiral arteries
progressing back as far as the myometrial
segments. Immunohistochemical studies of
placental bed biopsies suggest that trophoblast
cells and endothelial cells transiently coexist on
walls of partially modified spiral arteries.6
Trophoblast cells migrate along the luminal
surfaces of vessels, invading them and partially
replacing the endothelial cells and most of the
musculoelastic tissue in the vessel walls (Figure 3).7
The vessels are subsequently restructured such that
they have little smooth muscle and become larger
in diameter. This creates a high flow, low
resistance circulation that maximises maternal
blood flow to the placental villi at the maternal–
fetal interface. There is contrasting evidence as to
whether trophoblasts themselves are important in
arterial remodelling. Although it has been
suggested that some changes in the decidual
vessels occur independently, as part of the
maternal response to pregnancy, there is also
strong evidence that invasive interstitial
trophoblasts prepare the decidual spiral arteries
for endovascular trophoblast migration.8 The
invasive trophoblast may play an important role in
inducing further changes either by interactions or
factors produced by the interstitial trophoblast or
by direct cellular interactions of the endovascular
trophoblast with the cells of the vessel that they
subsequently replace.
The pathogenesis of pre-eclampsia and
intrauterine growth restriction is associated with
trophoblasts failing to adopt an endothelial cell-
like phenotype and endovascular invasion failing
to proceed beyond the superficial portions of the
spiral arteries in early pregnancy.
The cause of this impaired placentation is not fully
understood but may in part be due to poor
invasive properties of the trophoblastic cells or
changes in the maternal decidual tissues, which
regulate trophoblast behaviour, perhaps mediated
via multifunctional cytokine pathways. The
cytotrophoblastic expression of adhesion
molecules, which influences invasion, is altered in
women with pre-eclampsia. In vitro studies have
shown that trophoblasts from placentas of women
with pre-eclampsia have lower attachment on
fibronectin and vitronectin compared with
normotensive controls, which may reflect
differences in expression of matrix receptors.9
Maternal factors leading to inhibition of
trophoblast invasion include reduced expression
of the histocompatibility antigen HLA-G, local
inflammatory cell behaviour and cytokine
regulation of integrin expression.
placentalperfusion
Small placenta Normal placentaLarge placenta
(eg twins)
trophoblastic debristrophoblastic debris Normal amount of
trophoblastic debris
Maternal susceptibilityMaternal response
Inflammatory reaction
Endothelial cell dysfunction
Maternal syndrome Fetal effects
First stage Second stage
Endothelialcelldamage
Release offactors intomaternalcirculation
Normal
Pre-eclampsia
Maternalsyndrome
Multisystemdisorder
Fetal effects
Reducedplacentalperfusion
Figure 1
Two-stage model of pre-eclampsia. Adapted
from Roberts et al.3
Figure 2
Continuum theory of inflammatory response to
trophoblastic debris. Adapted from Redman
et al.4
The Obstetrician & Gynaecologist 2006;8:7–13 Review
’ 2006 Royal College of Obstetricians and Gynaecologists 9

The end result of altered differentiation is
inadequate trophoblast invasion. The incomplete
remodelling of the maternal vasculature results in
inadequate uteroplacental perfusion, particularly
later in pregnancy. The subsequent hypoxia/
ischaemia is presumed to trigger the release of a
circulating factor(s) into the maternal circulation.
Release of circulating factorsThe link between deficient trophoblastic invasion
early in pregnancy and the widespread endothelial
dysfunction manifesting much later has eluded
researchers for many years. The observation that
terminating the pregnancy, and more specifically,
that delivery of the placenta results in resolution of
the disease suggest that the placenta is the focus of
production of the putative factor(s) that
influences the endothelial cell. This hypothesis,
and the nature of the circulating factor(s), has
been investigated in a wide variety of both in vivo
and ex vivo studies. One of the first studies10 to
investigate the potential of circulating factors was
reported over a decade ago and is widely credited
with reviving the concept of toxaemia. This much
cited study demonstrated that serum from women
with pre-eclampsia was cytotoxic to cultured
human umbilical vein endothelial cells (HUVECs)
when compared with control sera from normal
pregnant women. This landmark study has
subsequently been extended by other investigators
in a wide variety of cultured cell types and on
isolated small vessels. Pre-constricted vessels from
women with a normal pregnancy relax well when
exposed to the endothelium-dependent
vasodilator bradykinin. However, in the presence
of plasma from women with pre-eclampsia, the
response of these vessels is markedly impaired.
Under these conditions vessels from normal
pregnant women mimic the behaviour of vessels
isolated from women with pre-eclampsia.11
The nature of this circulating factor or factors has
been much debated. Putative candidates include
vascular endothelial growth factor (VEGF),
tumour necrosis factor, lipid peroxides and
syncytiotrophoblast microfragments.
Vascular endothelial growth factor
Serum levels of VEGF and its soluble receptor-1
(sFlt-1) are elevated in pre-eclampsia, even before
the onset of clinical symptoms.12 The source of
the elevated circulating levels of VEGF in
pregnancies complicated by pre-eclampsia is
unclear. VEGF is expressed in placental tissue and
when trophoblast cells are cultured in hypoxic
conditions, VEGF production is increased.
However, studies of placental tissue are equivocal;
some have demonstrated that the expression of
VEGF mRNA is decreased in pregnancies
complicated by pre-eclampsia, whereas others
using immunohistochemical analysis have
reported that staining for VEGF is increased in
pregnancies complicated by pre-eclampsia. In
addition, several alternative explanations have
been advanced to account for the increase in
circulating levels of VEGF observed in pre-
eclampsia. It has been postulated that VEGF can
increase secondary to impaired renal function and
diminished excretion. Alternatively, VEGF
production can increase in response to vascular
endothelial cell injury as it has recently been
demonstrated that VEGF produced in vascular
smooth muscle can contribute to the initiation of
endothelial repair. As endothelial cell damage is
widespread in pre-eclampsia, this would lead to an
Figure 3
Histology of the placental bed in the early first
trimester, with the enlarged portions
demonstrating a spiral artery undergoing
transformation. In (a) the spiral artery remains
thick walled and muscular. In (b) endovascular
trophoblast is now present and there has been a
complete loss of smooth muscle.7 Reproduced
with permission from John Wiley and Sons Ltd
on behalf of the Pathological Society.
Review 2006;8:7–13 The Obstetrician & Gynaecologist
10 ’ 2006 Royal College of Obstetricians and Gynaecologists

increase in both local and circulating
concentrations of VEGF.
VEGF has been demonstrated to induce a
functional change in the response of myometrial
resistance arteries to the endothelium-dependent
vasodilator bradykinin. Incubation with VEGF
induces a dose and time-dependent diminution in
endothelium-dependent relaxation in these
arteries, which mirrors that found following
incubation with plasma from women with pre-
eclampsia. Intriguingly, pre-treatment of both
VEGF and plasma from women with pre-
eclampsia with an antibody to VEGF protects
against loss of endothelium-dependent
relaxation.13 This suggests that the elevated levels
of VEGF observed in pre-eclampsia may play a
role in the pathogenesis of vascular damage, rather
than merely being an epiphenomenon.
Tumour necrosis factor
The plasma levels of tumour necrosis factor a
(TNF-a) are high in pre-eclampsia, and in vitro
placental production of TNF-a is greater in
placentas from women with pre-eclampsia.14
Microvascular filtration capacity can be measured
in vivo as a measure of microvascular permeability.
The microvascular filtration capacity is
significantly increased in pre-eclampsia and this is
correlated with plasma levels of TNF-a. TNF-a
increases endothelial cell activation and increases
microvascular protein leakage.15
Syncytiotrophoblast microfragments
Syncytiotrophoblast microfragments (STBMs) are
debris from syncytial apoptosis. Apoptosis is
programmed cell death and occurs in the normal
placenta. The rates of apoptosis are increased in
pre-eclampsia, and levels of STBMs are increased
in the plasma of women with pre-eclampsia.16 If
STBMs are cultured in vitro with endothelial cells
there is disruption of the endothelial cell
monolayer. When cultured with neutrophils,
STBMs isolated from the placentas of women with
pre-eclampsia cause activation of neutrophils and
an increased superoxide production.17 In contrast,
when STBMs were incubated with myometrial
vessels at the increased levels seen in women with
pre-eclampsia, there was no change in the
endothelial dependent relaxation of these
vessels.18 This would suggest that it is unlikely that
STBMs themselves induce the endothelial cell
dysfunction seen in pre-eclampsia, but STBMs
may interact with other factors such as leucocytes.
There are, therefore, several candidate circulating
factors in pre-eclampsia. The complex clinical
manifestations of the disease seem unlikely to be
related to one single factor and it seems much
more likely that these factors act in combination
to trigger the disease process.
Oxidative stressEvidence has emerged to support a role for
oxidative stress in linking reduced placental
perfusion with systemic maternal
pathophysiology.19
Oxidative stress is a pathological state, implicated
in the aetiology of many disorders, including
atherosclerosis, in which pro-oxidants dominate
over antioxidants. The resultant increase in the
formation of reactive oxygen species can damage
cell membranes, proteins and DNA.
Epidemiological studies have revealed that many
of the risk factors associated with the development
of pre-eclampsia such as obesity, black race, lipid
abnormalities, insulin resistance and raised serum
homocysteine are also associated with the risk of
developing atherosclerosis in later life. These
observations have led to the emerging hypothesis
that suggests reduced placental perfusion generates
oxidative stress and leads to widespread
endothelial dysfunction in pre-eclampsia.
One such factor involved in oxidative stress is
nitric oxide (NO). Within the circulation,
superoxide is formed by the reduction of oxygen.
Superoxide is normally broken down by
superoxide dismutase. However, NO competes
with superoxide dismutase and combines with
superoxide to form peroxynitrite. Therefore, high
concentrations of NO and superoxide, or a
reduction in superoxide dismutase, will lead to
increased peroxynitrite and its resulting toxic
effects.
Levels of superoxide dismutase in subcutaneous
fat vessels are lower in women with pre-eclampsia
compared with those from normotensive pregnant
women.20 Immunostaining of endothelial cells
from subcutaneous fat vessels showed
nitrotyrosine (as a marker of peroxynitrite and
therefore oxidative stress) to be present in 3% of
vessels in normal women, but present in 73% of
vessels in women with pre-eclampsia.20 Therefore,
in pre-eclampsia there is an increase in oxidative
stress in which NO plays a major role. The levels of
NO, cGMP and NO synthase may be increased in
pre-eclampsia; it is not known whether this is a
compensatory mechanism to produce more vessel
relaxation or a pathophysiological condition with
NO involved in oxidative stress. It may be for this
reason that efforts simply to increase total NO
production by the use of NO donors in pre-
eclampsia have not been shown to be clinically
beneficial, but that an increase in NO could
increase peryoxynitrite production and cause
endothelial dysfunction.
Further evidence supporting the role of oxidative
stress in pre-eclampsia has come from a
randomised placebo-controlled trial in which the
The Obstetrician & Gynaecologist 2006;8:7–13 Review
’ 2006 Royal College of Obstetricians and Gynaecologists 11

antioxidants vitamins C and E were given from
18–22 weeks of gestation to women who were
known to be at high risk of pre-eclampsia from
previous history or abnormal uterine artery
Doppler waveforms.21 The trial demonstrated a
significant reduction in the incidence of pre-
eclampsia in those taking vitamin
supplementation compared with those on a
placebo, and a significant fall in the biochemical
markers of endothelial cell activation. The possible
use of vitamin supplementation as prophylactic
agents in women at high risk of developing pre-
eclampsia is extremely encouraging. However, it is
important that vitamin supplementation is not
brought into routine clinical practice until the
results of larger multicentre vitamins in pregnancy
trials (currently continuing) are known.
Hypoxia–reoxygenationUntil recently the primary problem in pre-
eclampsia was thought to be a poorly perfused
placenta. Failure of the spiral arteries to remodel
in pre-eclampsia results in them retaining their
vasoreactivity. Therefore, it is now suggested that,
instead of a chronically hypoxic placental blood
supply, there is intermittent perfusion of the
intervillous space. This results in a fluctuating level
of oxygenation to the placenta and has been
termed a hypoxia–reoxygenation or ischaemia–
reperfusion injury. In vitro studies have
demonstrated an increase in oxidative stress in
placentas exposed to hypoxia–reoxygenation. In
contrast, placentas exposed to chronic hypoxia did
not show an increase in oxidative stress.22 The
effect of hypoxia–reoxygenation on the amount of
apoptosis has also been studied, with hypoxia–
reoxygenation being associated with an increase in
apoptosis.23
Endothelial cell activation andinjuryThe underlying pathophysiology in pre-eclampsia
is a loss of normal endothelial function with
leakage of protein and fluid from the intravascular
space. This is evident by the clinical signs of
proteinuria and oedema. The increased capillary
permeability in pre-eclampsia has also been
demonstrated using Evans blue dye.24
There are biochemical markers evident in the
blood of women with pre-eclampsia suggestive of
endothelial cell injury or activation. Levels of
cellular fibronectin (cFN, a marker of significant
endothelial cell injury), von Willebrand’s factor
(vWF, an activator of platelet adhesion), tissue
plasminogen activator (tPA, a fibrinolysis
promoter) and plasminogen activator inhibitor-1
(PAI-1, a fibrinolysis inhibitor) are higher in sera
of women with pre-eclampsia compared with
normotensive women.25
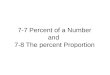
Further evidence of endothelial dysfunction in
pre-eclampsia can be seen in the relaxation of
myometrial vessels. The contractility and
relaxation of small myometrial vessels dissected
from myometrial biopsies taken at caesarean
sections can be measured in vitro. The relaxation
of myometrial vessels from women with pre-
eclampsia is reduced compared with normotensive
pregnant women (Figure 4).26 This relaxation was
shown to be endothelium dependent as the
difference in relaxation of vessels from women
with pre-eclampsia and normotensive pregnant
women is abolished when the endothelium is
removed. Endothelial dependent relaxation of
myometrial vessels in normal pregnancy is
through endothelium-derived hyperpolarising
factor (EDHF) and NO. However, in pre-
eclampsia endothelial dependent relaxation is
entirely through the NO pathway, and the activity
of this system is reduced.27 Any mechanism to
improve endothelial dependent relaxation of
myometrial vessels in women with pre-eclampsia
could have significant effects on the oxygenation
of the placenta and also the release of circulating
factors. One suggested avenue may be
phosphodiesterase inhibitors. Phosphodiesterase is
present within endothelial cells and degrades cyclic
GMP (the second messenger in the NO pathway).
Phosphodiesterase inhibitors will limit this step
and promote vasodilatation. This relaxant effect
has been demonstrated in myometrial vessels from
women with pre-eclampsia in vitro, so that the
response of these vessels is approaching that of
normal pregnancies.26
100
80
60
40
% A
VPm
ax
20
0P=0.0035 (ANOVA)
_11 _10 _9 _8
[Bradykinin]
Normal pregnant (N=12)Pre-eclampsia (N=18)
_7 _6
Figure 4
Bradykinin induced (mol/L) endothelium-
dependent relaxation of myometrial vessels in
normal pregnancy and pre-eclampsia. The y axis
demonstrates the relaxation as a percentage of
the maximal constriction to arginine vasopressin
(AVP).26 Reproduced with permission from
Elsevier.
Review 2006;8:7–13 The Obstetrician & Gynaecologist
12 ’ 2006 Royal College of Obstetricians and Gynaecologists

SummaryThere has been extensive research into the
pathogenesis of pre-eclampsia in recent years and
while a unifying hypothesis has not yet been
reached, there is general consensus regarding
many of the key steps in the disease process.
Deficient remodelling of the spiral arteries in early
pregnancy results in a reduced absolute placental
blood flow and fluctuations in oxygen
concentration. There is an increase in oxidative
stress within the placenta and throughout the
maternal circulation. This increase in placental
oxidative stress is likely to be related to the
increase in apoptosis seen in pre-eclampsia. The
placenta releases circulating factors that target the
maternal vascular endothelium and this in turn
causes the fetal and maternal effects seen in this
serious condition. Most importantly, a greater
understanding of this complex disease pathway
has led to new avenues for therapeutic strategies.
References1 Lewis G, editor. Why Mothers Die 2000–2002. The Sixth Report of the
Confidential Enquiries into Maternal Deaths in the United Kingdom.
London: RCOG; 2004.
2 Maternal and Child Health Research Consortium. Confidential Enquiry
into Stillbirths and Deaths in Infancy: 5th Annual Report. London: Maternal
and Child Health Research Consortium; 1998.
3 Roberts JM, Lain KY. Recent insights into the pathogenesis of pre-
eclampsia. Placenta 2002;23:359–72.
4 Redman CW, Sargent IL. Placental debris, oxidative stress and pre-
eclampsia. Placenta 2000;21:597–602.
5 Lyall F. Development of the utero-placental circulation: the role of carbon
monoxide and nitric oxide in trophoblast invasion and spiral artery
transformation. Microsc Res Tech 2003;60:402–11.
6 Pijnenborg R, Dixon G, Robertson WB, Brosens I. Trophoblastic invasion of
human decidua from 8 to 18 weeks of pregnancy. Placenta 1980;1:3–19.
7 Crocker IP, Wareing M, Ferris GR, Jones CJ, Cartwright JE, Baker PN, et al.
The effect of vascular origin, oxygen, and tumour necrosis factor alpha on
trophoblast invasion of maternal arteries in vitro. J Pathol
2005;206:476–85.
8 Kam EP, Gardner L, Loke YW, King A. The role of trophoblast in the
physiological change in decidual spiral arteries. Hum Reprod
1999;14:2131–8.
9 Pijnenborg R, Luyten C, Vercruysse L, Van Assche FA. Attachment and
differentiation in vitro of trophoblast from normal and preeclamptic
human placentas. Am J Obstet Gynecol 1996;175:30–6.
10 Rodgers GM, Taylor RN, Roberts JM. Preeclampsia is associated with a
serum factor cytotoxic to human endothelial cells. Am J Obstet Gynecol
1988;159:908–14.
11 Hayman R, Warren A, Johnson I, Baker P. Inducible change in the
behavior of resistance arteries from circulating factor in preeclampsia: an
effect specific to myometrial vessels from pregnant women. Am J Obstet
Gynecol 2001;184:420–6.
12 McKeeman GC, Ardill JE, Caldwell CM, Hunter AJ, McClure N. Soluble
vascular endothelial growth factor receptor-1 (sFlt-1) is increased
throughout gestation in patients who have preeclampsia develop.
Am J Obstet Gynecol 2004;191:1240–6.
13 Brockelsby J, Hayman R, Ahmed A, Warren A, Johnson I, Baker P.
VEGF via VEGF receptor-1 (Flt-1) mimics preeclamptic plasma in
inhibiting uterine blood vessel relaxation in pregnancy: implications
in the pathogenesis of preeclampsia. Lab Invest 1999;79:
1101–11.
14 Rinehart BK, Terrone DA, Lagoo-Deenadayalan S, Barber WH, Hale EA,
Martin JN Jr, et al. Expression of the placental cytokines tumour necrosis
factor alpha, interleukin 1beta, and interleukin 10 is increased in
preeclampsia. Am J Obstet Gynecol 1999;181:915–20.
15 Hung TH, Charnock-Jones DS, Skepper JN, Burton GJ. Secretion of
tumour necrosis factor-alpha from human placental tissues induced by
hypoxia-reoxygenation causes endothelial cell activation in vitro: a
potential mediator of the inflammatory response in preeclampsia.
Am J Pathol 2004;164:1049–61.
16 Redman CW, Sargent IL. Pre-eclampsia, the placenta and the maternal
systemic inflammatory response — a review. Placenta 2003;24:
S21–7.
17 Aly AS, Khandelwal M, Zhao J, Mehmet AH, Sammel MD, Parry S.
Neutrophils are stimulated be syncytiotrophoblast microvillous
membranes to generate superoxide radicals in women with
preeclampsia. Am J Obstet Gynecol 2004;190:252–8.
18 Van Wijk MJ, Boer K, Nisell H, Smarason AK, Van Bavel E, Kublickiene
KR. Endothelial function in myometrial resistance arteries of normal
pregnant women perfused with syncytiotrophoblast microvillous
membranes. BJOG 2001;108:967–72.
19 Roberts JM, Hubel CA. Is oxidative stress the link in the two-stage model
of pre-eclampsia? Lancet 1999;354:788–9.
20 Roggensack AM, Zhang Y, Davidge ST. Evidence for peroxynitrite
formation in the vasculature of women with preeclampsia. Hypertension
1999;33:83–9.
21 Chappell LC, Seed PT, Briley AL, Kelly FJ, Lee R, Hunt BJ, et al. Effect of
antioxidants on the occurrence of pre-eclampsia in women at increased
risk: a randomised trial. Lancet 1999;354:810–6.
22 Hung TH, Skepper JN, Burton GJ. In vitro ischaemia-reperfusion injury in
term human placenta as a model for oxidative stress in pathological
pregnancies. Am J Pathol 2001;159:1031–43.
23 Hung TH, Skepper JN, Charnock-Jones DS, Burton GJ. Hypoxia-
reoxygenation: a potent inducer of apoptotic changes in the human
placenta and possible etiological factor in preeclampsia. Circ Res
2002;90:1274–81.
24 Brown MA, Zammit VC, Lowe SA. Capillary permeability and extracellular
fluid volumes in pregnancy-induced hypertension. Clin Sci (Lond)
1989;77:599–604.
25 Friedman SA, Schiff E, Emeis JJ, Dekker GA, Sibai BM. Biochemical
corroboration of endothelial involvement in severe preeclampsia.
Am J Obstet Gynecol 1995;172:202–3.
26 Wareing M, Myers JE, O’Hara M, Kenny LC, Warren AY, Taggart MJ, et al.
Effects of a phosphodiesterase-5 (PDE5) inhibitor on endothelium-
dependent relaxation of myometrial small arteries. Am J Obstet Gynecol
2004;190:1283–90.
27 Kenny LC, Baker PN, Kendall DA, Randall MD, Dunn WR. Differential
mechanisms of endothelium-dependent vasodilator responses in human
myometrial small arteries in normal pregnancy and pre-eclampsia. Clin
Sci (Lond) 2002;103:67–73.
The Obstetrician & Gynaecologist 2006;8:7–13 Review
’ 2006 Royal College of Obstetricians and Gynaecologists 13



![December 21, 2015 - Wisconsin Supreme Court · RB-1 (2015) [?\^]`_ acbedgfhbeij[ ahik[ l 1. mon#p qsrHt`rvuxwnzye{E|}ux~)r 'p n#w )rv|}ux~x 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7 7](https://img.pdfslide.us/doc/110x75/5fb3422fccf05f68ab3a22e4/december-21-2015-wisconsin-supreme-court-rb-1-2015-acbedgfhbeij-ahik.jpg)