Embed Size (px)
Citation preview

Environmental ScanHealth Supports for Consumers with Chronic Conditions
Funded through a grant from Kaiser Permanente with additionalsupport from The Robert Wood Johnson Foundation.
www.chcs.org
Center for Health Care Strategies, Inc.CHCS
By Melanie Bella, Elizabeth Cobb, and Joanie Rothstein Center for Health Care Strategies
Claudia WilliamsAZA Consulting
November 2005
7508 11/17/05 10:55 AM Page 1

The Center for Health Care Strategies (CHCS), founded in 1995, is a nonprofit health
policy resource center seeking to advance the quality and value of health care services
for low-income populations and people with chronic illnesses and disabilities. CHCS
works with state agencies, health plans, providers, and consumer groups to develop
cost-effective solutions that deliver measurable improvements in consumer health.
CHCS believes that Medicaid, as the nation’s largest health care purchaser and the
most sophisticated purchaser of managed care services, is uniquely positioned to
demonstrate the long-term value — for people, for health plans and providers, for
government, and for society as a whole — of investing in the improvement of health
care quality.
This report was produced under the Medicaid Value Program: Health Supports for
Consumers with Chronic Conditions, a collaborative of 10 diverse organizations — four
health plans, two state Medicaid agencies, one clinical research organization, one
academic medical center, one safety net provider, and one disease management
organization — to develop and test models of care management for Medicaid
consumers with co-morbidities. This CHCS initiative is funded by Kaiser Permanente
Community Benefit, with additional support from The Robert Wood Johnson
Foundation.
For more information about the Medicaid Value Program and other CHCS initiatives,
visit www.chcs.org.
© 2005 Center for Health Care Strategies
7508 11/17/05 10:55 AM Page 2

Foreword 3Background 4Introduction 6Identification of Target Populations 7Guidelines and Measures 9Information Technology 12Care Management 15Consumer Role 21Financing and Incentives 24Organizing Entity 27Conclusion 29Appendix A: Interview List 30Appendix B: Expert Panel 31
1
Table of Contents
Environmental ScanHealth Supports for Consumers with Chronic Conditions
Center for Health Care Strategies, Inc.CHCS
7508 11/17/05 10:55 AM Page 3

Health Supports for Consumers with Chronic Conditions
2
Acknowledgements
The authors thank the numerous individuals who helped distill the components for a compre-hensive chronic care infrastructure detailed herein. In particular, we are grateful to the insightsof our expert panel members as well as the on-the-ground perspectives from experts across thecountry. We recognize Ray Baxter, PhD, Maureen Hanrahan and Paul Wallace, MD from KaiserPermanente for their inspirational guidance. In addition, we thank Stephen Somers, PhD,President of CHCS, for keen direction and leadership; and Lorie Martin, of CHCS, for editorialcontributions.
Finally, and most importantly, we are grateful to the generous support and foresight of KaiserPermanente Community Benefit, which is providing not only funding, but a wealth of knowl-edge, data-rich experience, and innovative tools to significantly advance care management practices to improve the health and quality of life of people with multiple chronic conditions.
7508 11/17/05 10:55 AM Page 4

3
Health Supports for Consumers with Chronic Conditions
Foreword
or years, we have been hearing from our stakeholders that existing approaches to identifying,delivering services to, and assessing the quality of care for Medicaid consumers with co-mor-
bid chronic conditions were, for the most part, not meeting the needs of this most high-risk andhigh-cost population. That is why we at the Center for Health Care Strategies (CHCS) embracedthe opportunity when Kaiser Permanente asked us to consider a major initiative to advance ourcollective understanding of the nature and scope of the complex co-morbidities in a Medicaidpopulation. The intent of the proposed initiative was to promote the development of new modelsof care that could take us beyond management of single diseases and even beyond the bifurcationof physical and behavioral health care and some of the other social supports needed by so manyconsumers with multiple chronic conditions who are served by Medicaid as well as those who aredually eligible for Medicaid and Medicare. With significant backing from Kaiser PermanenteCommunity Benefit and additional support from The Robert Wood Johnson Foundation, CHCSlaunched the Medicaid Value Program: Health Supports for Consumers with Chronic Conditions. Tenearly innovator teams were chosen to participate in this two-year collaborative to expand,enhance, and assess new models of care for Medicaid consumers with different combinations ofserious illness and disability. The collaborative will run through December 2006.
As a first step to guide the efforts of the 10 participating teams, CHCS conducted an environmen-tal scan of existing programs across the country to unearth state-of-the-art approaches and impor-tant future directions. The nationwide scan revealed six key components that we believe areessential for a comprehensive, sustainable chronic care infrastructure. The key components are:
1. Identification of target populations2. Guidelines and measures3. Information technology4. Care management5. Consumer role6. Financing and incentives
This report, which details considerations for each of these components and defines the need foran “organizing entity” to oversee these functions, is our first installment in what we hope will be aseries of valuable insights and lessons for our stakeholders — the state Medicaid agencies, man-aged care organizations, providers, and consumer groups — to improve the quality of care for theirbeneficiaries, particularly those with intense, chronic health care needs.
F
7508 11/17/05 10:55 AM Page 5

4
Health Supports for Consumers with Chronic Conditions
Background
tatistics paint a compelling picture ofthe impact of chronic illnesses in the
United States today. More than 90 millionAmericans live with chronic illnesses,accounting for greater than 75 percent of thenation’s $1.4 trillion medical care costs andone-third of the years of potential life lostbefore age 65.1 Chronic disabling conditionscause major limitations in activity for morethan one of every 10 Americans, or 25 mil-lion people.
The impact of chronic illness on Medicaidprograms is even more staggering. Almosttwo thirds (61 percent) of adult Medicaidenrollees have a chronic or disabling condi-tion, most frequently diabetes, hypertension,asthma, psychoses, and chronic depression.2
S
1 National Center for Chronic Disease Prevention and Health Promotion, “Chronic Disease Overview,” http://www.cdc.gov/nccdphp/overview.htm (26 September 2005).
2 S. Allen and A. Croke, The Faces of Medicaid: The Complexities of Caring for People with Chronic Illnesses and Disabilities, Center for Health Care Strategies (2000).
3 Partnership for Solutions, “Chronic Conditions: Making the Case for Ongoing Care,” December 2002, http://www.partnershipforsolutions.com/dms/files/chronicbook2002.pdf (26 September 2005).
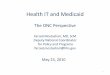
Figure 1: Average Annual Per Capita Health Care Spending and Number ofDoctors of Chronic Conditions for Medicaid Enrollees
Hea
lth C
are
Spen
din
g*
Number of Chronic Conditions
$8,000
$6,000
$4,000
$2,000
0
10
8
6
4
2
0
Num
ber of D
octors**
Zero One Two Three Four
Source: C. Williams, “Medicaid Disease Management: Promises and Pitfalls,” Kaiser Family Foundation, 2004.Data Source: Medical Expenditure Panel Survey, 1998. Data for all Medicaid enrollees.
*Mean cost per capita **Average number of unique physicians
$737 1.4
4
5.2
6.5
8.2
$2,307
$3,817
$6,002
$6,942
Eighty percent of Medicaid resources arespent on this population.3
Almost half (46 percent) of Medicaidenrollees with one chronic or disablingcondition have another, often a mentalhealth condition. As the number of condi-tions increases, so too does the cost andcomplexity of health care. Annual healthcare costs are nearly tenfold higher forMedicaid enrollees with four chronic con-ditions ($6,942) compared to enrollees withno chronic conditions ($737), and theaverage number of physicians treating aMedicaid enrollee rises from 1.4 forenrollees with no chronic conditions to 8.2for enrollees with four conditions (Figure 1).
7508 11/17/05 10:55 AM Page 6

5
Health Supports for Consumers with Chronic Conditions
4 E. A. McGlynn et al., “The Quality of Health Care Delivered to Adults in the United States.” New England Journal of Medicine 348, no. 26 (2003).
Despite the high cost of care and involve-ment of multiple providers among this popu-lation, there is considerable evidence thatpeople with chronic conditions do notreceive the health care they need. A study ofadults with medical conditions showed thatonly 45 percent of people with diabetes getthe care they need and only 25 percentreceive recommended testing to monitortheir condition.4 The data would likely besignificantly worse for people with diabetesand one or more other chronic conditions.
In recent years many Medicaid programshave implemented traditional disease man-agement programs to address problems relat-ed to chronic care. Programs typically cover
a handful of conditions — often diabetes,asthma, and congestive heart failure — butuse care management approaches that “silo”patients into single-disease focused inter-ventions. These programs fall short of theideal for enrollees with more than onechronic condition for a number of reasons:they offer no strategies for assessing and pri-oritizing enrollees’ multiple problems; theyleave in place a fragmented and non-inte-grated delivery system; and they fail toincorporate the behavioral and non-med-ical (wrap-around) services needed by thispopulation but not typically included indisease management programs.
7508 11/17/05 10:55 AM Page 7

Health Supports for Consumers with Chronic Conditions
6
• Input and debate with the Expert Panelconvened for this initiative (seeAppendix B); and
• Surveys of state Medicaid directors andhealth plan representatives.
As anticipated, the interviews provided therichest and most interesting information forthe environmental scan. While there aremany documents and articles focusedbroadly on chronic disease and chroniccare, few address the specific issues ofchronic care for low-income consumerswith co-morbidities.
The environmental scan revealed six keycomponents that we believe are essentialfor a comprehensive, sustainable chroniccare infrastructure. The report outlinesconsiderations for each of the componentsas well as discussions about larger issuesthat impact our ability to serve consumerswith multiple chronic conditions. Thecomponents are:
1. Identification of target populations2. Guidelines and measures3. Information technology4. Care management5. Consumer role6. Financing and incentives
Following the discussion of these key com-ponents, we present the need for an “organ-izing entity” to provide an infrastructure forsetting priorities of chronic care improve-ment, bringing together stakeholders,determining how to improve communica-tion and data sharing among these groups,and potentially realigning reimbursementand incentives.
Introduction
he Medicaid Value Program: HealthSupports for Consumers with Chronic
Conditions (MVP: HSCCC) is supporting10 innovation teams that will develop andtest groundbreaking approaches to addressthe needs of Medicaid enrollees with multi-ple chronic conditions. This environmentalscan is the first product of this initiative.The report synthesizes literature, expertviews, and on-the-ground experience todescribe the issues and problems associatedwith improving the care and health ofMedicaid consumers with multiple chronicconditions and to outline potential bestpractices in key areas.
MVP: HSCCC Innovation Teams
CareOregon
Comprehensive NeuroScience, Inc.
District of Columbia Department ofHealth Medical Assistance Administration
Johns Hopkins Healthcare, LLC
Managed Health Services, Inc.
McKesson Health Solutions
Memorial Healthcare System
Partnership HealthPlan of California
University of California at San Diego
Washington State Department ofSocial and Health Services
Information and insights for the environ-mental scan were gathered through:
• Literature and document review;• Interviews and site visits with experts
and leaders of on-the-ground initiatives(see Appendix A);
T
7508 11/17/05 10:55 AM Page 8

he first essential step in designing anychronic care management program is
to define and identify the target population.The identification methodology will varygreatly depending on the goals and expect-ed outcomes of the program. Identification
methodologies are typicallystructured to target specificconditions, high-cost individu-als, or high-risk individuals.
Traditional disease manage-ment programs use a disease-specific approach to identifyenrollees and organize care
management. Programs identify individualswith a given chronic disease (asthma, dia-betes, CHF, COPD) using ICD-9 diagnosiscodes from inpatient, outpatient, and phar-macy claims data. Identifying eligible indi-viduals through administrative data is sim-ple and inexpensive, but has potentialdrawbacks due to variations in physiciancoding, incomplete data, inability to iden-tify co-morbidities, and data lags.5
Other chronic care programs are designedto target and provide interventions tohigh-cost individuals. High-cost enrolleesare identified through claims data andassigned to programs designed to managecare and control utilization. This methodof identification has been subject to criti-cism because it fails to catch at-risk members
before they become high utilizers.Additionally, program evaluation is diffi-cult due to “regression to the mean.” Thatis, individuals identified as high-cost oneyear are likely to use fewer services the fol-lowing year even absent an intervention.
Many disease management programs arenow identifying target populations throughpredictive modeling. Predictive modelinguses historical claims data to forecast futureadverse events and high utilization. Thismethod can identify individuals who are atrisk of becoming high utilizers, allowing apreventive rather than reactive approach.But there are also potential drawbacks tothis approach. Because these are propri-etary tools, vendors may not be eager toshare the individual-level details or specifi-cations that might allow program managersto use the results not just to identify mem-bers but also to shape interventions.6
Once the population has been identified, itis often stratified into groups by risk level.High-risk groups will typically require amore aggressive intervention, such as high-touch nurse case managers. Low-risk groupsmay receive telephonic interventions orsome other type of less intense strategy.7
Like identification, risk stratification can bedone in many different ways including bycost and by actual or predicted utilization.8
Health Supports for Consumers with Chronic Conditions
7
5 V. Villagra, “Strategies to Control Costs and Quality: A Focus on Outcomes Research for Disease Management,” Medical Care 42, no. 4 supp (April 2004): 24-30.
6 M. Cousins, L. Shickle, J. Bander, “An Introduction to Predictive Modeling for Disease Management Risk Stratification,” Disease Management 5, no. 3 (3 September 2002): 157-167.
7 M. Schatz, R. Nakahiro, C. Jones, R. Roth, A. Joshua, D. Petitti, “Asthma Population Management: Development and Validation of a Practical 3-Level Risk Stratification Scheme,” The American Journal of Managed Care 10, no. 1 (January 2004): 25-32.
8 J. Rosenzweig, K. Weinger, L. Poirier-Soloman, M. Rushton, “Use of a Disease Severity Index for Evaluation of Healthcare Costs and Management of Comorbidities of Patients with Diabetes Mellitus,” The American Journal of Managed Care 8, no. 11 (November 2002): 950-958.
Identification of Target Populations
T
The first essential
step in designing
any chronic care
management program
is to define and
identify the target
population
7508 11/17/05 10:55 AM Page 9

• Even if a single disease is the “ticket in”to the program, the identification processneeds to examine the whole patient,his/her risks, and co-morbidities. An ini-tial approach would be to conduct a com-prehensive risk assessment of each personscreened into a program as a result of hisor her chronic condition. The risk assess-ment could identify co-morbidities andlifestyle risk factors (including diet, phys-ical activity, and smoking) as well associal and family risk factors, which con-tribute to medical problems and mightinfluence care management strategies.Ultimately, this could progress to a moreambitious population-based screening onall members to identify “pre-members”who do not yet have a chronic condition,but are candidates for lifestyle change andprevention interventions. CareOregon, anon-profit, Medicaid-only health planserving more than 100,000 membersunder the Oregon Health Plan, is anearly adopter in this area — screening allnew members to identify those in need ofcomplex care management.
Health Supports for Consumers with Chronic Conditions
8
Future Direction
• Regardless of the identification methodchosen, from a data, cost, and efficiencystandpoint, it will make sense to central-ize the identification process for mostchronic care initiatives. In many cases,the state Medicaid agency will be thesource of data and will conduct the iden-tification process. In other cases, aMedicaid health plan or vendor maycomplete the identification process usingidentification criteria that they haveeither developed or that has been pro-vided by the state.
• For the foreseeable future, individual dis-ease states will still drive identificationand treatment. Although there is wide-spread interest in developing a “person-centered” rather than a “disease-cen-tered” approach to chronic care, theprocess will still likely start with theidentification of enrollees with particulardiseases or clusters of conditions.Identifying clusters of conditions is anemerging approach that warrants furtherinvestigation because it holds greatpromise for more effectively looking atthe whole person and taking intoaccount the presence of multiple chronicconditions.
7508 11/17/05 10:55 AM Page 10

here are many sources for clinicalpractice guidelines in the United
States today. Organizations like theNational Heart Lung and Blood Instituteand the American Diabetes Associationproduce guidelines for specific diseases orconditions. Health plans such as KaiserPermanente and GroupHealth Cooperativehave produced evidence-based guidelines ina variety of areas. Finally, states (e.g., NewYork, Indiana) and other localities haveproduced guidelines for use in a specificregion. The Agency for HealthcareResearch and Quality’s National GuidelineClearinghouse™ is a comprehensive data-base of evidence-based clinical practiceguidelines and related documents.9
A recent article in Health Affairs outlinedsome of the barriers to the use of guidelinesand the practice of evidence-based medi-cine.10 These barriers include:
• The physician-patient relationship:There is a strong desire, on the part ofboth patients and physicians, to preservethe primacy of the physician-patient rela-tionship, and the notion that care shouldbe tailored to an individual.
• Lack of automation: It may be difficultfor physicians to reference multiple andvaried guidelines during a routine visit.Although not yet widely available, espe-cially among Medicaid providers, clinicaldecision support systems, such as elec-tronic medical records, may hold the keyto making guidelines and other evidence-based practice tools more accessible.
Just as there are many sources of guidelines,there are a multitude of quality measures,many of them based on the evidence-basedguidelines. Measurement is a fundamentalcomponent of quality improvement. Measuresare typically categorized as process or outcomeoriented. Process measures tend to beadapted from evidence-based guidelines andare designed to track and measure the actu-al care delivered as opposed to the overallhealth outcome or status. Examples includepercentage of children with asthma oninhaled steroids, and percentage of diabeticswith an annual foot exam. Outcome meas-ures report the end result of the care deliv-ered or overall health status, such as mortal-ity rates, functional status, or total permember per month expenditures. There arebenefits and drawbacks to using eitherprocess or outcome measures in health care,and they are most effective when used inconjunction with one another.
One challenge to measure-ment of care for peoplewith co-morbidities is theearly stage of developmentof the evidence base. Thatevidence base and, there-fore, the decision supporttools, necessary for the pro-vision of standardized and clinically appro-priate care, are not structured to guide careand care management for people with mul-tiple chronic conditions. Indeed, many ofthe randomized trials that have led to dis-ease-specific guidelines excluded patientswith co-morbidities, the elderly, and people
Health Supports for Consumers with Chronic Conditions
9
One challenge to
measurement of care for
people with co-morbidities
is the early stage of
development of the
evidence base.
Guidelines and Measures
T
9 National Guideline Clearinghouse, an initiative of the Agency for Healthcare Research and Quality, U.S. Department of Health and Human Services, http://www.guideline.gov (26 September 2005).
10D. Mendelson and T. Carino, “Evidence Based Medicine in the United States – De Rigueur or Dream Deferred,” Health Affairs 24, no. 1 (January/February 2005): 133-136.
7508 11/17/05 10:55 AM Page 11

with disabilities. In some cases, the evi-dence for high-risk Medicaid consumerswith complex clinical needs and physicaldisabilities is simply non-existent.
Understandably, guidelines and measurestend to be disease specific and do not takeinto account the interactive nature of mul-tiple health care problems or provide direc-tion for caring for patients with co-morbidconditions. However, there is increasingrecognition that this needs to change —especially with the aging of the population.The interplay of multiple health issues cre-ates an effect of “cascading conditions.”Each health issue interacts with and mustbe examined through the lens of the others.For example, a provider treating someonewith diabetes, congestive heart failure, anddepression cannot just follow the specificguidelines for each standalone disease; theprovider must adapt her care to take intoaccount the interplay of the three condi-tions affecting that specific patient.Similarly, measuring the quality of thatindividual’s care will have to take intoaccount the multiple conditions. Thismakes it even more important to have amix of process and outcome measures thatcan provide a comprehensive and holisticmeasure of the patient’s health status andthat reflect a causal relationship to thequality/care management intervention.
Future Direction
• New, flexible treatment protocols andinterventions are needed, as well as waysof measuring progress for people withmultiple chronic conditions that are notsimply additive, but that take intoaccount the interplay between conditions.Because disease states provide an impor-tant organizing structure and way to
measure progress, the single disease willlikely remain the fundamental way wethink about health and treatment. Yet amore integrated approach to both treat-ment and measurement is needed. Thiswill be a significant challenge for thefuture as we do not yet have the scientificevidence base to develop these protocols.They will need to be derived from med-ical “best judgment” as the evidence baseis being developed. Medicaid, given itsposition as payer for consumers witharguably the most complex and multipleconditions, is uniquely positioned to be asignificant driver of the efforts to expandthe evidence base.
• A first step could be to rethink careguidelines and “change concepts” forpatients with co-morbidities to prioritizethe most important pieces of the inter-vention. This may not be as overwhelm-ing a task as it first appears. While thereare many patterns of co-morbidity, a smallnumber account for most of the peoplewith more than one condition. A work-able approach, therefore, would be toidentify one or several common clusters ofconditions or key co-morbidity patternsand gather relevant practitioners to talkabout how guidelines can be combinedand modified for these clusters. Possibleclusterings could include diabetes withcardiovascular disease and asthma withCOPD, with thought given to whetherdepression should be taken into accountin all clusters.11 Consideration would needto be given to how the three to fourimportant care recommendations for eachof the conditions interplay, i.e., the priori-tization of treatment, which trumps whichand what single disease recommendations,if any, need to change.
Health Supports for Consumers with Chronic Conditions
10
11Interview with Tom Bodenheimer, MD, Professor, University of California San Francisco, April 18, 2005.
7508 11/17/05 10:55 AM Page 12

• A next step could be to develop compos-ite measures focusing on the most com-mon and important disease clusters iden-tified. A composite measure would com-bine disease specific measures (e.g.,HbA1c, blood pressure, cholesterol), out-come measures (e.g., functional status,patient satisfaction), and a financialmeasure (e.g., per member per monthexpenditures). Composite measures couldcapture disease cluster recommendations,assess consumer indicators (satisfactionwith care, ability to manage care, healthstatus and functioning), and assist in pro-jections of overall health care costs, serv-ing as a progress “dashboard” for groups ofconsumers.
• A final step would be to align reimburse-ment and incentives to support high qual-ity care as measured by a “snapshot” ofthe patient’s health status and improve-ment as a whole as opposed to by a singlecondition or episode of care.
• Advances in medical technology and newdecision support tools, such as predictivemodeling and risk assessment methodolo-gies, may someday allow physicians toefficiently access care recommendationsbased on a variety of factors and condi-tions, enhancing their ability to practiceevidence-based medicine tailored to theindividual.
Health Supports for Consumers with Chronic Conditions
11
7508 11/17/05 10:55 AM Page 13

ealth information technology (HIT)tools hold great promise for improving
chronic care delivery across all spectrums ofthe system — from payers and providers toemployers and consumers. Remarks fromDavid Brailer, MD, PhD, NationalCoordinator for Health InformationTechnology, highlight the potential:
“Health IT will transform the way Americansregard their health and the way they participatein health care. The important aspect of healthIT is not software and computers – it is physi-cians making better treatment decisions, nurs-es and pharmacists delivering safer care, andconsumers making better choices among treat-ment options. It is the way people connecttogether across a fragmented delivery system –from physician offices to hospitals to skillednursing facilities and even to the consumer'shome. It is putting consumers in control oftheir health status, and customizing care deliv-ery to meet their needs.”12
Many efforts are underway to develop anational health infrastructure built on inter-operable standards that will link health care
information nationwide— across payers, servicedelivery settings, andclinical conditions. TheHIT infrastructure envi-sioned would be a pow-erful tool for improving
quality and reducing costs. As local, state,and national efforts unfold, it is critical thatsafety net providers, especially those insmall one or two physician practices, not be
forgotten. Efforts to support and financeHIT initiatives on the Medicare side shouldbe explored for Medicaid as well.
Future Direction
• Provider demand for health care technol-ogy could be fostered by providing basicdata that are in electronic formats andmight have immediate clinical value.Data might include lab, pharmacy, emer-gency department alerts, and utilizationmeasures from claims and could be col-lected (through some sort of automaticinterface) in a centralized data warehouse.Lab data (standardized and electronicallyreported) could provide a rich startingplace. Several initiatives have focused onthis area. A clinical messaging initiativein central Indiana currently provides labresults electronically to 1,000 providersand will be expanding to all 2,700providers in that region by the end of2005. The California HealthCareFoundation has spearheaded the develop-ment and adoption of lab reporting stan-dards in California. It is expected thatCalifornia will have standardized lab datawithin the next year.
• A widely discussed tool with great poten-tial opportunity is the electronic medicalrecord. President Bush has called forevery person to have an electronic med-ical record (EMR) in 10 years.13 An elec-tronic medical record will make it mucheasier to identify consumers with co-mor-bidities or allow the care team to look
Health Supports for Consumers with Chronic Conditions
12
12 Remarks by David Brailer, National Coordinator for Health Information Technology, at the HIMSS 2005 Conference, http://www.himss.org/content/files/DavidBrailerRemarksHIMSS2005.pdf (26 September 2005).
13 White House Press Release, “President discusses health care, information technology benefits,” Intercontinental Cleveland Clinic Suite Hotel, Cleveland, Ohio, 27 January 2005, http://whitehouse.gov/news/releases/ 2005/ 01/ 20050127-7.html (26 September 2005).
The HIT infrastructure
envisioned would be a
powerful tool for
improving quality and
reducing costs.
Information Technology
H
7508 11/17/05 10:55 AM Page 14

across members and diseases to identifyclusters of consumers with particular pat-terns of conditions. But as is the case forhealth care technology more generally,the EMR can only support better chroniccare if it is part of an overall care redesignprocess that introduces a more integratedand less “disease siloed” approach. Wecan only be partially successful if weinsert an electronic medical record in afragmented and disorganized delivery sys-tem without giving thought to the overalldesign of the processes and structure.
• While many small provider practicesseem a long way from implementingEMRs, a handful have already taken the
technological plunge (see box below).Their experiences are instructive. One ofthe initial challenges they face is the dis-ruption caused by implementation of theEMR. This disruption — to care process-es, office relationships, practice structure,and reimbursement — needs to be antici-pated and managed. As some continuousquality improvement experts have sug-gested, “disruptive technology” can beproductive and should, for that reason, beembraced. By disturbing existing process-es and clinical care approaches, the EMRmight spur needed changes, helping todisorganize, and then constructively reor-ganize chronic care.
Health Supports for Consumers with Chronic Conditions
13
14 Interview with Richard Baron, MD, Greenhouse Internists, April 5, 2005. 15 R.J. Baron, E.L. Fabens, M. Schiffman, E. Wolf, “Electronic Health Records: Just around the Corner? Or over the
Cliff?” Annals of Internal Medicine 143, no. 3 (August 2005): 223-225. 16 Ibid.
Implementing an EMR in a Small Physician Practice
One physician shared his experience implementing an EMR in a four-person pri-mary care practice. As expected, the start-up costs were significant. The hard-ware, software, training, and support costs for the first year of implementation atthis small practice were approximately $140,000, in line with the published esti-mates of per physician costs ($12 to $24 thousand per physician) in the first yearof implementation.14,15 While in time the practice “broke even” financially, itunderestimated other implementation demands. Every employee, from physiciansto file clerks, had to re-learn their jobs and how to work within the newlyredesigned office system. This process was stressful to all and required a signifi-cant adjustment period. The practice also increasingly relied on outside technolo-gy support, which proved difficult to finance given its size. The practice alsofound that a great deal of information is difficult to automatically upload anddoes not flow easily into the EMR due to the absence of national standards thatlink data systems. For example, while the practice has an interface for laboratorydata, the majority of the information they “receive (such as radiology reports,consultations, and procedure reports) does not come in a format that the systemcan recognize electronically.”16 Small physician practices, like this one highlight-ed, form the backbone of the U.S. health care system and their adoption of auto-mated records is critical for national movement in this direction. The arduous trialof this pioneering practice demonstrates the need for substantial financial andadministrative support for these small practices to invest in information technology.
7508 11/17/05 10:55 AM Page 15

• Identifying innovative ways to financethe upfront investment required for pur-chasing and deploying HIT will be key toincreasing the adoption and spread ofHIT, particularly for small provider groupsand/or individual practitioners. This is anarea of opportunity for health plans. Planscould provide the HIT hardware/softwaredirectly, provide it indirectly through atargeted financial incentive or grant, orstructure a revolving loan program forproviders. There are several Medicaidplans that are seeking partnerships withothers in their geographic service areas tospur the adoption of HIT among theirproviders. States could play this role too;although, states are more likely to be in aposition to provide low cost loans asopposed to directly funding HIT forproviders. Lastly, the Centers forMedicare and Medicaid Services (CMS)could be a partner in this effort. HIT is aquality improvement tool supported byCMS in the newly launched MedicareHealth Support demonstration forapproximately 160,000 Medicare benefici-aries with diabetes and congestive heartfailure.17 CMS could assist states throughenhanced federal financial participationfor HIT investments and/or by helpingleverage other sources of federal funding(e.g., Agency for Healthcare Researchand Quality, Department of Health andHuman Services, etc.) for HIT infrastruc-ture development.
Health Supports for Consumers with Chronic Conditions
14
17 Centers for Medicare and Medicaid Services Press Release, “CMS Acts to Improve Quality Care for Chronically Ill Beneficiaries,” 2 August 2005, http://www.cms.hhs.gov/media/press/release.asp?Counter=1521 (26 September 2005).
18 Johns Hopkins HealthCare/ Priority Partners Phase I Report, Improving Care for Adults with Chronic Illnesses andDisabilities BCAP Workgroup, submitted to Center for Health Care Strategies (16 April 2003).
• Another tool with potential, particularlyin rural areas, is remote monitoring.Home technology can be used to monitorconsumers with chronic conditions andmight be an effective means to addressrural health access issues, but would needto be paired with strategies to increaseaccess to the required technology. It isunclear how it might best be used amongthe Medicaid population. However, homemonitoring is expected to be used in theMedicare Health Support demonstrationprogram and may provide valuable lessonsand replicable practices for Medicaid pro-grams addressing similar patient popula-tions and conditions.
Using Home Technology in Rural Areas
Johns Hopkins HealthCare implemented atelemedicine program to address disparities inhealth care access and health outcomes amongits rural Medicaid consumers with heart failure,diabetes, and co-morbid conditions. TheTeleWatch program enables patients to be mon-itored remotely by Johns Hopkins specialistsand disease management nurses, thus bringingspecialized expertise to the care of patients inrural areas. The program decreased hospitaliza-tions, inpatient days, and total costs as well asimproved clinical indicators.18
7508 11/17/05 10:55 AM Page 16

Health Supports for Consumers with Chronic Conditions
15
o date, care for Medicaid consumerswith multiple chronic conditions,
especially for those with both physical andbehavioral co-morbidities,has been fragmented andpoorly organized. Themajority of Medicaid con-sumers with multiplechronic conditions are notpart of a single system thathelps them organize, makesense of, and navigate theoverall health care system.They may have multiplephysicians, case managers,
and/or ancillary providers, but often there isno care plan and/or no person in charge ofoverseeing the care plan that could unitethe components of care. This is an issue alsofaced by consumers with single chronic con-ditions, of course, but the challenge is moreacute and complex for people with multiplechronic conditions. Our research and dis-cussions identified four closely linked con-cepts — the care team, the “go to” person, themedical home, and the care intervention —that could, in varying combinations, providestructure for organizing care for people withmultiple chronic conditions.
Future Direction
The Care TeamRethinking the care team for this popula-tion and how it should be organized (seebox on next page), is a first step. The careteam, in most cases, needs to include PCPs,specialists, behavioral health professionals,and, perhaps, pharmacists. It also needs toinclude the other care resources workingwith the consumer. For consumers with substance abuse or mental health problems,social workers, psychiatric nurses, and sub-stance abuse counselors could be importantmembers of the team. Health educators, psy-chologists, and behavioral health practition-ers might be key resources for addressingbehavior change and mental health issues.
• The consumer should have a lead role indeciding who is on the care team, whichmight also include family, friends, andneighbors. Cash and counseling programs,which provide consumers with a monthlyallotment and give them control over hir-ing their own personal care providers, areearly demonstrations of consumer-directedcare in the arena of long-term supportsand services.
Care Management
T
The majority of
Medicaid consumers
with multiple chronic
conditions are not part
of a single system that
helps them organize,
make sense of, and
navigate the overall
health care system.
7508 11/17/05 10:55 AM Page 17

Health Supports for Consumers with Chronic Conditions
16
19 Interview with Laureen Gray, Planned Care Project Director, Cambridge Health Alliance, June 14, 2005.
Examples of Care Team Design
Commonwealth Care Alliance (CCA), a Massachusetts health plan, uses an inte-grated care team approach in which the care manager is a clinician, who can treatthe patient and authorize services, e.g., physical therapy, etc. The concept for thiscare team was developed out of the discovery that the needs of most complexpatients are not met during the standard three to four office visits per year. CCAenvisioned the care manager as someone who could intervene between visits toassist patients in meeting their goals. Each patient is evaluated and assigned to atype of care team based on need. The core care team is composed of the caremanager (typically a nurse practitioner and the team lead), a medical assistant(helps patients to make appointments, arrange transportation, and fill prescrip-tions), a primary care practitioner, and a behavioral health practitioner. This teamworks with the patient to ensure needs are met by accompanying patients tooffice visits, offering on-site behavioral health treatment, conducting home visits,referring patients to specialists, and linking patients and their families to valuablecommunity resources.
Cambridge Health Alliance (CHA), an integrated health system in Massachusetts,uses a planned care model led by the care coordinator who plays a “navigator”role, rather than a clinical role. The care team is composed of a physician, a nurse,a medical assistant, a nutritionist, a social worker, and the planned care coordina-tor. The care coordinator uses a registry to identify patient needs or gaps in careand will follow up with each individual patient to check in on health status, sched-ule an appointment, or send a reminder for a test, etc. Using this system of aplanned care team, CHA reports an increase in the eye appointment rate for dia-betics from 54 percent to 74 percent. Similarly, in one year CHA reports a reduc-tion in asthma-related emergency room admission from seven percent to undertwo (1.78) percent.19
• Experts and practitioners in the field dif-fer over the best model for organizing thecare team and responsibilities of its mem-bers. Some argue that each member ofthe care team needs to be engaged indeveloping the care plan and coordinat-ing with others on the care team. Otherssay there can be more of a hub and spokemodel — with a “go to” person leadingmuch of the development and coordina-tion of the care plan with input from theother parties.
“Go To” PersonOne of the biggest problems in the currentsystem is the lack of coordination of healthcare resources around the consumer. This isin large part due to a reimbursement systemthat generally pays providers for singleepisodes of sick care, defined by traditionaloffice visit codes. A “go to” person shouldbe matched with each consumer with mul-tiple chronic conditions (and reimbursedaccordingly) to help consumers connect,navigate, and interact with the delivery sys-tem.
7508 11/17/05 10:55 AM Page 18

Health Supports for Consumers with Chronic Conditions
17
20 Interview with Robert Master, MD, President, Commonwealth Care Alliance, June 14, 2005. 21 Interview with Laureen Gray, Planned Care Project Director, Cambridge Health Alliance, June 14, 2005.
• The “go to” person might be a care man-ager, patient advocate, health care buddy,medical assistant, social worker, or anoth-er player in the health care system (seebox below). The physician will have akey role, but will probably not be the “goto” person responsible for care manage-ment. Nurses are well-suited to the role,but might need additional training in keyareas, such as behavior change tech-niques, motivational interviewing, andassessing patient activation.
• The “go to” person would help consumerssolve a variety of problems, whether clini-cal, behavioral, or even social, in somecases, not in the standard benefit pack-age. Two major responsibilities of the “goto” person would be working with con-sumers to develop the care plan andorganizing and directing the care manage-ment process. The “go to” person woulddevelop a shared care plan, coordinateproviders, and identify consumer needsspanning beyond the traditional medicalmodel.
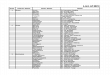
• The specific skills and background of the“go to” person will depend on the needsof the consumer. For example, two pro-gram models (see Figure 2), one devel-oped by the Cambridge Health Allianceand the other by the CommonwealthCare Alliance in Massachusetts, havestratified the “go to” person profile basedon the complexity or risk level of thepatient.20,21
Examples of the “Go To” Person
Whatcom County. Clinical specialists who arenurses or social workers help consumers draft acare plan and coordinate with providers.
Cambridge Health Alliance. Planned care sitecoordinators act as buddies for patients and areinstrumental in getting patients to appointmentsand helping them deal with a range of issues.
MaineHealth. Non-nurse care managers areassigned to practices. They work across dis-eases, but tend to focus on diabetes since it isthe focus of current quality initiatives.
Partners. Health coaches (provided through acontract with a vendor, Health Dialog) work withup to 1,000 Medicaid consumers with chronicconditions. Coaches provide self-managementsupport, make social service referrals, and helpconsumers navigate the health care system.
7508 11/17/05 10:55 AM Page 19

Health Supports for Consumers with Chronic Conditions
18
• The approach taken by the “go to” per-son needs to be adapted to the culture,lifestyle, and preferences of the specificconsumer. The importance of identifyingand addressing racial and ethnic dispari-ties as well as building cultural competen-cy into care management cannot beunderstated.
Medical HomeA “medical home” for all Medicaid con-sumers is critical, but the definition of themedical home may need to be rethought inlight of consumers with multiple chronicconditions to ensure that it is flexible andadaptive enough to meet their needs. The“go to” person will complement but notreplace the medical home. Purchasers,health plans, and policymakers should care-fully consider the following:
• The medical home for consumers withmultiple chronic conditions needs to bevery different from the traditional physi-cian’s office. Ideally, it will adopt a moreholistic approach to chronic care —
including components such as a sharedcare plan, planned care visits, informa-tion systems to support alerts andreminders, and better referral systems.
• The practice specialty of the coordinat-ing physician, the skills and backgroundof the “go to” person, and the composi-tion of the care team will vary dependingon the needs and severity of the patient.While a primary care provider will be themedical home for many Medicaid con-sumers, a specialist may be better suitedto serve some, especially those with com-plex conditions.
• Some have suggested that a new kind ofspecialist — an “outpatient intensivist”— may be needed to serve as the medicalhome for consumers with especially com-plex chronic conditions. This providerwould be a “specialist” in a new way, hav-ing expertise in health behavior changeand extensive training across specialtiesrather than deep knowledge of one prac-tice area.
Figure 2: Care Management Program Models
Organization Type of Patient Type of “Go-To” Person
Cambridge Health Alliance
Less complex patients Buddy or coach
Psycho-socially complex Social worker
Medically complex Physician and nurse care manager
Commonwealth Care Alliance
Low-risk Monitored through ongoing data surveillance
Moderate-risk Nurse with physician consultation
High-risk Nurse practitioner providing care at home
7508 11/17/05 10:55 AM Page 20

Health Supports for Consumers with Chronic Conditions
19
22 B. Reigel, B. Carlson, Z. Kopp, B. LePetri, D. Glaser, A. Unger, “Effect of a Standardized Nurse Case-Management Telephone Intervention on Resource Use in Patients With Chronic Health Failure, “ Archives of Internal Medicine 162 (March 2002): 705-712.
23 C.B. Taylor, N. Houston Miller, K. Reilly, G. Greenwald, D. Cunning, A. Deeter, L. Abascal, “Evaluation of a Nurse-Care Management System to Improve Outcomes in Patients with Complicated Diabetes,” Diabetes Care 26, no. 4 (April 2003): 1058-1063.
24 Missouri Medicaid Pharmacy Program, http://www.heritage-info.com/mocaidrx/dm/index.htm (26 September 2005).
Care InterventionCare intervention is a central componentof any successful chronic care managementprogram. Successful care interventionsshould be focused on addressing medical,social, and behavioral issues. Interventionscan vary in intensity and length and oftendepend on the severity and complexity ofthe conditions. Patients can be stratified byrisk and assigned interventions accordingly.
• Telephonic care management is mostoften used in managing care for lower riskindividuals. Calls from lay care managersare used to provide basic health educationinformation, monitor adherence to med-ications, support behavior change, assesschanges in health status, and answer anyquestions. Some studies have shown thatthis method of care management reduceshospitalizations and improves health out-comes (please note these studies did notinclude Medicaid consumers).22 Comparedto the most intensive care managementmethods, telephonic outreach is relativelyinexpensive to maintain on an ongoing basis(although it requires an upfront investmentin the infrastructure/technology).
• Nurse care management is an effectiveway to manage health care for the high-risk chronically ill population. Nurse caremanagers might combine home visitswith face-to-face meetings at theprovider’s office and telephone calls.These sessions are used to discuss careplans, develop self-management goals,
and assist the patient in coordinating hercare. While this high-touch method issignificantly more resource intensive thantelephonic intervention alone, the twomethods combined have proven to besuccessful in improving health status forindividuals with multiple chronic condi-tions (as noted previously, these studiesdid not include Medicaid consumers).23
• Pharmacy management will be criticallyimportant for consumers with multiplechronic conditions. States have tended topursue pharmacy utilization managementand care management approaches sepa-rately. Good models for integrating thetwo are needed. Properly managed, muchof this population may see a substantialincrease in medication usage. Accordingly,the clinical pharmacist will play an impor-tant role on the care team and in ensur-ing that patients are on the appropriatemedications. Kaiser Permanente willsoon implement such a model for patientsat high-risk for cardiovascular disease.Identified at-risk patients will be auto-matically placed on a set of drugs per aclinical protocol agreed to by physicians,pharmacists, and patients. A program inMissouri, which pairs primary careproviders and clinical pharmacists tojointly develop pharmacy managementplans for chronically ill patients, hasshown good initial results in terms of costsavings.24 The state plans to blend thispharmaceutical approach with a multi-component program that will include
7508 11/17/05 10:55 AM Page 21

nurse care management. On January 1,2006, the Medicare Part D drug benefitwill take effect and Medicaid consumersthat are dually eligible for Medicaid andMedicare will no longer receive theirpharmacy coverage through Medicaid.States are concerned that they will nolonger have access to pharmacy claimsdata, which will significantly underminetheir ability to manage the aspects of careof the dual eligibles for which Medicaidwill retain responsibility. It will be criti-cal to preserve access to these data, espe-cially for those with multiple chronicconditions, which is the majority of dualeligibles.
• An essential element for an interventioninvolving a complex population is thesuccessful integration of physical andbehavioral health. In many health caresystems, these two pieces are siloedresulting in data fragmentation and poorcommunication between physical andbehavioral health providers. However,there are systems that have recognizedthe division between the two systems andhave created innovative models for inte-gration (see box at right).
Health Supports for Consumers with Chronic Conditions
20
CareSouth’s Integration of Physical andBehavioral Health
CareSouth, a community health center in SouthCarolina, successfully integrated primary careand behavioral health. Every patient is screenedby the primary care physician, and if a behav-ioral health need is identified, that patient isimmediately referred to a behavioral health clini-cian. This model allows the care team toaddress the needs of the patient on the spotwithout having to schedule a future appoint-ment. The primary care physicians are support-ive of this practice because it allows them tofocus their time with the patient on physicalhealth needs alone.
7508 11/17/05 10:55 AM Page 22

Health Supports for Consumers with Chronic Conditions
21
more activated and engaged con-sumer should be at the heart of
chronic disease improvement efforts. Theprevalence of chronic disease has, inrecent years, prompted researchers andpractitioners to rethink the roles of con-sumers, physicians, and other health pro-fessionals in treating these conditions.25
Because chronic conditions are not reme-died by a quick trip to the doctor’s office,but require ongoing management andbehavior change, consumers can play amuch larger role in their own care.
Recently, practice change models empha-sizing the role of consumers in managinghealth have received widespread attentionfrom both academicians and clinicians.Enabling consumers to take control oftheir own health through changes in “diet,exercise, self-measurement, and medica-tion use”26 is seen as an effective way toimprove health outcomes, reduce pressureson the health care system, and meet con-sumer needs. An environmental scan con-ducted by RAND’s Evidence-BasedPractice Center for people with hyperten-sion or diabetes showed that self-manage-ment interventions could have a signifi-cant positive effect on health outcomes.27
Consumer direction has gotten the atten-tion of several states, e.g., Florida, SouthCarolina, and West Virginia. As part oftheir broader reform efforts, these statesseek to expand consumer direction andresponsibility and are requesting CMSapproval to create vehicles such as health
investment accounts for Medicaid con-sumers that reward them for healthy choic-es, such as accessing preventive services.While it is important totest greater consumerinvolvement in health caredecisions, it is also impor-tant to move cautiously toensure that consumershave the information theyneed to make the bestdecisions. It is one thingto ask people with frailtiesand disabilities (who out ofnecessity tend to be veryengaged in managing their care) to makedecisions about selecting personal careworkers in the Cash and Counseling pro-grams; it is considerably more complex toask them to navigate the health care sys-tem to make informed choices about theirmedical care.
Overall, lack of patient-centeredness inexisting chronic care initiatives was men-tioned by a broad spectrum of experts inour interviews. The issue manifests itself inat least two ways. First, most initiativesfocus on a single disease and do notaddress multiple conditions. Second, thepatient voice and perspective are oftenmissing in the care management process. Itis also worth noting that some feel that theconsumer must be the one to initiate tak-ing more responsibility in managing his orher health rather than relying on the systemto reorganize itself around the consumer.
Consumer Role
A
25 H. Holman, K. Lorig, “Patient Self-Management: A Key to Effectiveness and Efficiency in Care of Chronic Disease,” Public Health Reports 119, no. 3 (May-June 2004).
26 T. Bodenheimer, E.H. Wagner, K. Grumbach, “Improving Primary Care for Patients with Chronic Illness,” Journal of the American Medical Association 288, no. 14 (9 October 2002): 1775-9.
27 The Center for Advancement in Health, “Essential Elements of Self-Management Interventions,” http://www.cfah.org/pdfs/Essential_Elements_Report.pdf (11 March 2005).
While it is important to
test greater consumer
involvement in health
care decisions, it is also
important to move
cautiously to ensure that
consumers have the
information they need to
make the best decisions.
7508 11/17/05 10:55 AM Page 23

Health Supports for Consumers with Chronic Conditions
22
Future Direction
• Solutions must address the need for afocus on multiple conditions. The organiz-ing entity (e.g., health plan, provider net-work, health system etc.), the medicalhome, and “go to” person must devise amore integrated approach to care manage-ment. One possible approach is to identi-fy patients with particular “improvable”diseases, but design a care managementprocess that works “upstream” and “down-stream” to address co-morbid conditions,lifestyle issues, and underlying behavioralissues. Another is to design interventionsfor patients with a given cluster of chronicconditions. Both approaches will requiregreater fluidity, adaptability, and respon-siveness in care management approaches.
• Solutions must include the patient per-spective. New strategies to engage con-sumers about their own goals, needs, andpreferences are needed. This will requirecarefully testing different consumer-drivenapproaches as there has been only mini-mal work in this area to date and there islittle evidence about what works best.However, many experts believe that thereis considerable potential for incorporating
consumer preferences and priorities toguide the composition of the care team(including the role and involvement ofthe patient’s family), the care manage-ment approaches used, and, most impor-tantly, what health issues and problemstake priority.
• That said, it is unrealistic to expect theconsumer to drive the whole process. Thehealth care system is so complicated andthis population has such complex needsthat it may not be realistic to view con-sumers as the “drivers” of all aspects oftheir care. Even assuming consumers dowant to play this role, it is unfair to askthem to do so until clinical, quality, andcost information that is transparent,robust, and free flowing exists to allowthem to make informed decisions andactively drive their health care. There areinitiatives underway that are building thisinformation base, particularly in the areaof electronic patient health records (seebox on next page).
7508 11/17/05 10:55 AM Page 24

Health Supports for Consumers with Chronic Conditions
23
• A patient health record can motivatemore patient-centered care management.Many people use the term “patient cen-tered care,” but care management struc-tures do not necessarily reflect this phi-losophy. Whatcom County, Washingtontook this concept literally and decided toinclude consumers as consultants in allphases of project planning for its chroniccare initiative. Patients involved in thisplanning process felt that the standardmedical record was missing importantinformation about the consumer’s envi-ronment, the consumer’s goals, how theconsumer likes to learn, and who theconsumer views as essential to the careteam. Whatcom County decided todevelop an alternative model (see boxbelow).
• Improving consumer self-managementwill require a flexible and skilledapproach. Many Medicaid consumerswith multiple chronic conditions, as wellas fundamental social and economicchallenges, may not be ready to be “acti-vated.” Patient engagement and empow-erment will require trust building overtime and a flexible, not rules bound,approach. Training for care managers andothers promoting self-management skillswill be key and should draw from emerg-ing findings and techniques on behaviormodification and readiness to change.
• Another good way to ensure that caremanagement is patient-centered isthrough home visits. By seeing con-sumers in their own homes, the “go to”person or care manager can appreciatethe consumer’s environment and con-text, as well as their values.
Whatcom County’s Patient Health Record
Whatcom County developed a new patient-gen-erated health record including patient-generatedinformation describing the care team, listing pre-scription drugs, and outlining preferred ways oflearning as well as short- and long-term goals.Patients can create the patient health record ontheir own or with the help of a care manager. Itsuse has changed the dynamic between physicianand patient. Armed with documentation of theirpreferences and goals, patients find that doctorsare more willing to listen to, learn about, andincorporate the patient perspective. A demon-stration of the patient record can be viewed atwww.sharedcareplan.org.
7508 11/17/05 10:55 AM Page 25

different from the commercial population,so goals and benchmarks should be adjust-ed to reflect those differences.
Through the national Rewarding Resultsprogram, seven Medicaid managed careplans in California are working to developfinancial and non-financial incentives forproviders and members to improve thequality of and access to pediatric preven-tive care services. The primary incentivestarget well-baby visits and adolescent wellcare visits. A complementary measurerewards medical groups based on the vol-ume, timeliness, and quality of electronicencounter data. Although not targeted tochronic illness care, the publication of theexternal evaluation of this project, avail-able in 2006, will contribute to the ongo-ing discourse about incentives in Medicaidmanaged care.
Meanwhile, providers are being asked to dodifferent things and develop differentresources for each purchaser — an unwork-able situation. There are several potentialstrategies Medicaid can use to enhance col-laboration among purchasers, and therebylessen the burden on providers. One is toadopt protocols and quality strategies inMedicaid chronic care initiatives that havebeen embraced by other purchasers. Maine,for instance, is trying to build on the payfor performance approaches developed by acollective of the state’s purchasers.
For several years, Medicaid programs havebeen looking for ways to use incentives to
Health Supports for Consumers with Chronic Conditions
24
ny redesign of the health care deliv-ery system needs to consider better
ways to align incentives with quality ofcare. One alignment strategy is through“pay for performance,” which is gainingpopularity in health systems across thecountry. As of March 2005, there were 104pay-for-performance programs being devel-oped or implemented across the country.28
These programs are generally sponsored byhealth plans or employer purchasing coali-tions. They compensate physicians andother members of the care team with bothfinancial and non-financial rewards forboth process (annual foot exam for diabet-ics) and outcome (improving hemoglobinA1c values for diabetic members) measures.Financial incentives include performance-based reimbursement, bonuses, and pay-ment for specific achievements or outcomeson quality measures.29 Non-financial incen-tives can range from simple recognition toencouraging consumers to switch to higherperforming providers. Although a few stateMedicaid agencies and health plans areexperimenting with these approaches, mostof the current pay for performance initia-tives around the country reside in the com-mercial realm.
One critical issue for Medicaid managedcare organizations is how to gain leveragefor chronic care improvement withproviders. For a health plan that is institut-ing a new incentive program it may be verydifficult to get buy-in from enoughproviders to make the program effective.Additionally, the Medicaid population is
Financing and Incentives
A
28 G. Baker and B. Carter, “Provider Pay-for-Performance Incentive Programs: 2004 National Study Results,” (Med-Vantage, Inc.: 2005).
29 Bailit Health Purchasing, LLC, “Ensuring Quality Providers: A Purchaser’s Toolkit for Using Incentives,” National Health Care Purchasing Institute, May 2002, http://www.bailit-health.com/articles/index/shtml (26 September 2005).
7508 11/17/05 10:55 AM Page 26

align payment and quality. States are usingdirect financial incentives to rewardMedicaid managed care plans for superiorperformance on standardized measures ofquality and satisfaction. New York distrib-uted close to $13 million to health plansfrom September 2004-August 2005 as apart of its Quality Incentive Program, whichallows for performance payments of up toone percent (increasing to three percent infuture years) of each plans’ Medicaid managed care capitation rate. In the nextyear, incentive payments will be nearly $40 million.30
One of the New York plans, Health Now,has, in turn, developed an internal systemto reward physicians for their performanceon a variety of measures, including HbA1cresults, nephropathy testing, and eye examsfor diabetics, and preventive screenings.31
Another example, though not for chronicillness care per se, is Rhode Island. For thepast six years, the state has linked financialincentives to a series of 21 measures andjust recently expanded to 31 indicators ofquality including both HEDIS and CAHPSmeasures.
Some states are also rewarding high per-forming plans through the auto assignmentof new members. This strategy directsenrollment of Medicaid members (whohave failed to select a health plan on theirown) to these high performing plans. Forexample, Michigan, New Mexico, and NewYork are testing this form of incentive. InMichigan, there are two auto-assignmenttiers based on network/access capacity andquality of care as determined by HEDISscores (immunization, well child visits,timeliness of prenatal and postnatal care,and HbA1c testing for diabetes), with the
average auto-assignment rate around 40percent. It is worth noting that auto-assignment will only be an attractiveincentive to managed care plans if the cap-itated rates are properly risk adjusted. Theimportance of accurate risk adjustment inrate setting and program design cannot beunderestimated and is a particularly criticalcomponent in the design of any care man-agement program for Medicaid consumerswith multiple chronic conditions and/ordisabilities.
Future Direction
A systematic approach to chronic care isthe right thing to do, but there is not ashort-run business case for it in the currentfinancing environment.Because chronic careinitiatives are more like-ly to result in long-term,rather than short-term,savings, champions willoften have more successadvancing them as quali-ty initiatives than ascost-saving approaches. This is a tough sellin today’s cost-cutting environment.Organizations are encouraged to focusinstead on the long-term investmentpotential of these initiatives, and theintrinsic social and economic value ofimproving the health status of consumerswith chronic needs.
• Moreover, even if efforts do result in costsavings, there will likely be winners andlosers, at least in the short term, until wefind a better way to pool resources andpotential savings and to reallocate thedollars to reward quality.
Health Supports for Consumers with Chronic Conditions
25
A systematic approach to
chronic care is the right
thing to do, but there is
not a short-run business
case for it in the current
financing environment.
30 Joseph Anarella, Assistant Director, New York State Bureau of Quality Management and Outcomes Research (November 8, 2005 e-mail correspondence).
31 J. Verdier, L. Felland, S. Felt-Lisk, F. Smieliauskas, J. Wong, Quality-Related Provider and Member Incentives in Medicaid Managed Care Organizations, Center for Health Care Strategies (July 2004).
7508 11/17/05 10:55 AM Page 27

• In parallel, the business case analysismust be expanded beyond health carecosts to include a broader economic andsocial case that assesses the impacts onworker/student absenteeism, productivity,and progression of disability. Shifting themindset to consider enrollees (who mayor may not be part of the target popula-tion) as “pre-members” whose high-riskbehaviors or conditions put them at riskfor chronic conditions and who may bepart of any payer’s system at any giventime reinforces the importance ofexpanding the business case analysis.
• Resources are needed to build the infra-structure and organizing function. Newfinancing strategies might still be direct-ed at providers, but must also motivatebehaviors and interventions for thewhole care team, not just the physician.This will require finding a way to “collec-tivize” small care sites. North Carolinahas done this by paying regional physi-cian collaboratives (rather than individ-ual doctors), a strategy that is also beingtried in British Columbia. Anotherapproach, which Maine hopes to try,involves paying providers a monthly caremanagement fee (larger than the typicalprimary care case management [PCCM]payment) if they are willing to play the“organizer” function.
• Providers need to get paid more for doingmore comprehensive chronic care, partic-ularly as it relates to consumers with mul-tiple chronic conditions. Disease manage-ment vendors are realizing that they needto use financial incentives for providersto foster collaboration and to recognizethe provider’s role in improving chronicillness care. In Washington, one of itsvendors, Renaissance Health Care, Inc.,is offering incentives to physicians whoprovide lab values related to end stagerenal disease. In another example,
Indiana Medicaid implemented a newcode to reimburse for non-provider groupvisits.
• Lack of integration of Medicare andMedicaid financing streams (and otherpurchasers) poses multiple challenges.Many Medicaid enrollees with multiplechronic conditions are either dual eligi-bles or are in the two-year transition toMedicare, heightening the importance offinding some way for Medicare andMedicaid to work together. States areconcerned that implementation ofMedicare’s Part D (and other parts of theMedicare Modernization Act) will fur-ther fragment care, potentially create abudget drain on Medicaid because of theclawback provisions, and make identifi-cation of the target population more dif-ficult if Medicaid no longer receives realtime, accessible pharmacy utilizationdata.
• In the end, not much can be accom-plished without substantially aligning theunderlying financial incentives.Obviously, this is a big, unwieldy issue,but we must start paying providers forkeeping people well. Financing and reim-bursement innovations have tended tolag behind programmatic innovation.Policymakers and, potentially, founda-tions should underwrite the design offinancing innovations in this area as theprogrammatic models for better caremanagement processes are being devel-oped. Such innovations might includepaying chronic care providers for keepingpatients out of the hospital, investing ineffective behavior change strategies forso-called “pre-members,” integratingMedicaid and Medicare services andfinancing, and adopting similar incen-tives and reimbursement approachesacross purchasers.
Health Supports for Consumers with Chronic Conditions
26
7508 11/17/05 10:55 AM Page 28

n an ideal world, some type of “organ-izing entity” would serve to synchro-
nize stakeholders and coordinate all of thecomponents of care. Questions remain,however, about what type of entity can bestfill this role in different environments. It
does seem clear, however,that the more the organiz-ing entity bears the riskand can pool the resourcesfor patients with multiplechronic conditions, thebetter chance the entityhas to break through barri-
ers and achieve meaningful integration.The fully capitated managed care organiza-tion remains the most obvious structure forachieving this level of financial integrationand leverage. This will likely require newfinancing mechanisms.
Specific functions of the organizing entitywould include setting priorities for chroniccare improvement, bringing together stake-holders; aligning incentives and financing(and, ideally, holding risk); designing andmanaging IT and data systems; synthesizingand communicating important informationabout a consumer to all relevant providers(or making it possible for providers to talkto each other in a streamlined and straight-forward manner); working to educate andengage consumers in their care; and hiringand managing “go to” people (e.g. nurses orsocial workers).
Health Supports for Consumers with Chronic Conditions
27
Organizing Entity
I Examples of Organizing Entities
Regional Physician Networks – Payments fromMedicaid support North Carolina’s regional physiciannetworks that hire care managers and initiate qualityimprovement efforts. Monthly payments of $2.50 permember are made to the network as well as to theparticipating primary care provider.
Large Safety Net Provider – The Cambridge HealthAlliance — a safety net system composed of hospi-tals, ambulatory care sites, and local public health —hires care managers and is launching an electronicmedical record to link ambulatory care components.
Health Care System – A community hospital or sys-tem can act as a leader in the community to bringtogether stakeholders and build a care managementinfrastructure. Two examples of this are BellinghamHospital (Washington) and Maine Health (Maine).
Medicaid – In Indiana, the Medicaid program acts asthe organizing entity by bringing together healthinformation technology, provider collaboratives, nursecare management, and telephonic care support. InWashington, Medicaid plays this role by contractingwith two commercial disease management vendors tooperate a program including telephonic and nursecare management.
Health Plan – Managed care plans often have theorganizational, informational, and coordination capa-bilities required of an organizing entity. They alsohave the strongest incentives for improving healthstatus and preventing costly exacerbations of chronicdisease. An intriguing variation would involve ahealth plan “leasing” care management and organi-zation functions to a state for the PCCM or fee-for-service Medicaid population.
The fully capitated
managed care organization
remains the most obvious
structure for achieving
financial integration and
leverage.
7508 11/17/05 10:55 AM Page 29

Future Direction
• Several types of organizations mightserve as the organizing entity. Thesecould include health plans (many ofwhich already perform these functions),provider networks, Medicaid agencies, orhealth systems.
• Flexible approaches will work best.Some providers see the organizing func-tion as their role and have some of theneeded resources already in place. If pur-chasers determine that this is the case,reimbursement mechanisms should berealigned to support those providers inperforming this organizing function.Needed first, however, is a mechanism forassessing which strategy is workable indifferent locations and how multiplestrategies can be combined. In one exam-ple, Maine is considering allowingprovider sites that already have nursecare managers to bill Medicaid for theseservices under new care managementcodes. The state would then provide caremanagers (under contract with a vendor)to work with sites that do not have theseresources.
• Other providers may not be able to fillthese new roles but should be integratedinto the process. Many care sites do nothave the needed capabilities (or desire to
develop them) and are already stretchedtoo thin. For these providers, the caremanagement and other support functionsshould be organized externally and inte-grated back with primary care. Even ifthe organizing entity and “go to” personare external to the primary care provider,these providers will still play an impor-tant role in introducing the chronic caremodel, contributing to the care plan,facilitating linkages to outside servicesand supports, providing referrals to spe-cialty care, and initiating discussionsabout behavior change.
• New mechanisms are needed to financethe “go to” function. The traditionallynominal PCCM payments will not besufficient to cover coordination and inte-gration functions. Some states might con-sider increasing payments within aPCCM-type system for providers servingmore complex patients and who have aninterest in developing the “go to” func-tion. In other cases, the “go to” personsmight be deployed from another base,possibly community hospitals, plans, ordisease management organizations (anyof which might also be an organizingentity). In a given state or community,both practice-based and non practice-based models might exist side-by-sidedepending on providers’ patient volume,interest, and capabilities.
Health Supports for Consumers with Chronic Conditions
28
7508 11/17/05 10:55 AM Page 30

his environmental scan is just thefirst step in CHCS’ efforts with its
partners at Kaiser Permanente, The RobertWood Johnson Foundation, and the 10MVP: HSCCC teams to foster dramaticimprovement in the care of people withmultiple chronic conditions. It is clear thattoo little is known about the make-up ofthis comorbid population within Medicaid.What are their primary medical problems,but also their underlying behavioral health,social, and supportive service challenges?What is the scope and severity of the vari-ous combinations — or clinical clusters —of these conditions? That is only the firstset of questions, to which we have tried tosupply some initial answers. Next come thequestions of where and how are they get-ting what care? It is increasingly evidentthat more needs to be done.
We have probed the states, managed careplans, disease management organizations,integrated delivery systems, and providerswho have begun to wrestle with this prob-lem. Early innovators are developing methods to better identify and stratify theirhigh-risk populations with multiple chronicconditions and are implementing outreachand treatment interventions that put thepatient and his or her particular needs atthe center of care design. Building uponthese early lessons and those from theChronic Care Model32 and various diseasemanagement approaches that have beenadapted by Kaiser Permanente and otherinnovative health care organizations across
the country, we hope that the 10 MVP:HSCCC teams will take us another steptoward delivering the right care to thesepatients at the right time. We believe thatrapid cycle quality improvement approach-es — such as those developed and usedwith providers by the Institute forHealthcare Improvement and ImprovingChronic Illness Care and with health plansin Medicaid by CHCS with its BestClinical and Administrative Practicesmodel33 — will be the vehicles for helpingthese 10 early innovator teams lead thenation toward better systems of care for itsmost complex and chronically ill citizens.
Addressing this major root cause ofMedicaid’s burgeoning growth will result ina program that deliversincreased value throughimproved health care qual-ity and more effective tar-geting of resources for ournation’s most vulnerableindividuals, today and forfuture generations. Theseadvancements will benefitnot only those inMedicaid, but also those inMedicare and the commer-cially insured. Americanswill be living longer withmore chronic illnesses,frailties, and disabilities — it is incumbentupon the nation’s health care system tofocus on getting their care right.
Health Supports for Consumers with Chronic Conditions
29
Conclusion
T
32 E.H. Wagner, “Chronic Disease Management: What Will it Take to Improve Care for Chronic Illness?” Effective Clinical Practice 1 (1998): 2-4.
33 K.L. Brodsky and R.J. Baron. “A ‘Best Practices’ Strategy to Improve Quality in Medicaid Managed Care Plans,” Journal of Urban Health 77 (December 2000): 592-602.
Addressing this major root
cause of Medicaid’s
burgeoning growth will
result in a program that
delivers increased value
through improved health
care quality and more
effective targeting of
resources for our nation’s
most vulnerable
individuals, today and
for future generations.
7508 11/17/05 10:55 AM Page 31

Health Supports for Consumers with Chronic Conditions
30
NAME TITLE ORGANIZATIONGerry Anderson, PhD Director Partnership for Solutions
Richard Baron, MD Physician Greenhouse Internists
Ray Baxter, PhD Senior Vice President Community Benefit, Kaiser Permanente
John Benz Strategic Business and Development Officer Memorial Healthcare System
Bob Berenson, MD Senior Fellow Urban Institute
Laureen Biczak, DO Medical Director MaineCare (Maine Medicaid)
Kate Bones Senior Project Manager Institute for Healthcare Improvement
Tom Bodenheimer, MD Professor University of California at San Francisco
Sophia Chang, MD Director of Chronic Disease Care California HealthCare Foundation
Allen Dobson, MD President and CEO Cabarrus Family Medicine
Tim Ferris, MD Director, Pediatric Quality Improvement Partners Healthcare System, Inc
Michael Garrett Vice President, Business Development Qualis Health (QIO)
Laureen Gray Planned Care Project Director Cambridge Health Alliance
Jimmy Hara, MD Family Practice Residency Director Kaiser Los Angeles Medical Center
Denise Levis Hewson Director of Quality Improvement Community Care of North Carolina (North
Carolina Medicaid)
Bob Hurley, PhD Associate Professor Virginia Commonwealth University
Tom Inui, MD President and CEO Regenstrief Institute
Andrea Kabcenell Executive Director for Pursuing Perfection Institute for Healthcare Improvement
David Labby, MD Vice President CareOregon
Lisa Letourneau, MD Director of Clinical Integration MaineHealth
Marty Levine, MD Chief of Geriatric Services GroupHealth Cooperative
Anne Lewis CEO CareSouth Carolina
Doug Libby Executive Director Maine Health Management Coalition, Inc.
Alice Lind Care Coordination Manager Washington State Department of Social and
Health Services
Bob Master, MD President Commonwealth Care Alliance
Kathy Moses Chronic Disease Director Indiana Office of Medicaid Policy and Planning
George Oestreich, PharmD Director, Pharmacy Program Missouri Division of Medical Services
Marc Pierson, MD Executive Director Whatcom County's Pursuing Perfection Project
Marc Rosenman, MD Research Scientist Regenstrief Institute
Michael Rothman Senior Consultant University of Mississippi Medical Center
Pat Rutherford Vice President Institute for Healthcare Improvement
Christobel Selecky Executive Chairman LifeMasters Supported SelfCare, Inc.
Lois Simon Chief Operating Officer Commonwealth Care Alliance
David Stevens, MD Quality Improvement (Commission Corps) Agency for Healthcare Research and Quality
Warren Taylor, MD Director of Chronic Conditions Management Kaiser Permanente Northern California
Diana Verrilli Director, Strategic Marketing McKesson Health Solutions
Sandeep Wadhwa, MD Vice President of Government Programs McKesson Health Solutions
Ed Wagner, MD Director Improving Chronic Illness Care
Paul Wallace, MD Executive Director Care Management Institute, Kaiser Permanente
Wendy Wolf Executive Director Maine Health Access Foundation
Dawn Wood, MD Vice President, Corporate Medical Director WellPoint
Appendix A: Interview List
7508 11/17/05 10:55 AM Page 32

Health Supports for Consumers with Chronic Conditions
31
NAME TITLE ORGANIZATIONSophia Chang, MD Director, Chronic Disease Care Programs California HealthCare Foundation
Donna Checkett Senior Vice President, Medicare & Medicaid Schaller Anderson, Incorporated
Programs
Stephanie DeKemper President Centene Foundation
Sandra Foote Senior Advisor, Chronic Care Improvement Centers for Medicare and Medicaid Services
Mark Gibson Deputy Director Center for Evidence Based Policy, OHSU
Bob Hurley, PhD Associate Professor Virginia Commonwealth University
Warren Jones, MD Distinguished Professor of Health Policy University of Mississippi Medical Center
Doriane Miller, MD Program Director, Co-Management Learning Rush University/Stroger Hospital of Cook County
Network
George Rust, MD Interim Director National Center for Primary Care at Morehouse
School of Medicine
Karen Scott Collins, MD Deputy Chief Medical Officer NYC Health and Hospitals Corporation
Chris Selecky Executive Chairman Disease Management Association of America
Richard Sheola President, Public Sector Division Value Options
Sandra Shewry Director California Department of Health Services
Marshall Thomas, MD Vice President, Medical Services Colorado Access
Ed Wagner, MD Director Improving Chronic Illness Care
Andrew Webber President and Chief Executive Officer National Business Coalition on Health
Morris Weinberger, PhD Professor UNC School of Public Health
Dawn Wood Vice President, Corporate Medical Director WellPoint State Sponsored Business
Appendix B: Expert Panel
7508 11/17/05 10:55 AM Page 33

7508 11/17/05 10:55 AM Page 34

7508 11/17/05 10:55 AM Page 35

Center for Health Care Strategies, Inc.CHCSP.O. Box 3469Princeton, NJ 08543-3469(609) 895-8101(609) 895-9648 fax
www.chcs.org
7508 11/17/05 10:55 AM Page 36