Embed Size (px)
Citation preview

8/3/2019 713neck After Total Laryngectomy
http://slidepdf.com/reader/full/713neck-after-total-laryngectomy 1/571 3
Dav id J. D iSan tis , M .D .
D enn is M . B alfe , M .D .
R icha rd E . H ayden , M .D .
S tuart S . Sag el, M .D .
D onald Session s, M .D .
Jo seph K . T . L ee , M .D .
The N eck a fte r To ta l La ryngec tom y:
C T S tudy1
Com pu ted tom ograph ic scan s in 23 pa-
tien ts who had undergone to ta l laryng ec-
tom y were analyzed retrosp ectiv ely to
d eterm ine norm al postoperativ e appea r-
ance and to eva luate th e ro le o f C T in as-
.5 sessing recurren t n eop la sm . N in e pa tien ts
w ithou t c lin ica l ev id ence o f recu rrence
illu stra ted th e no rm a l po stoperative
changes: a round or ovo id neopharynx
connecting th e base of th e tongue w ith
th e cerv ica l esophagu s and in tac t fa t
p lanes su rround ing th e neopharynx , n eu -
4. rovascu lar bund les , and sterno cle idom as-
to id m uscles. In th e 12 patien ts w ith re -
cu rren t n eop lasm , the C T m an ifesta tion s
in cluded m asses invo lv ing th e in terna l
jugu la r lym ph node cha in (ad jacen t to th e
neopharynx , n eurovascu lar bund les, o r
sternoc le idom asto id m uscles) , tra cheos -
tom y site , o r paratrachea l reg ion . R ecur-
ren ce wa s m im icked on CT in tw o pa -
tien ts , on e w ith an ab scess and one w ith
m etastases from an adenoca rc inom a of
unknow n pr im ary site. In e ight patien ts,
a d istended neopharyngea l lum en co rre -la ted w ith ben ign or m alignan t s tr ictu re.
CT supp lem en ted phy sica l exam ina tio n
-4 -V and ind irec t m irror exam ination , p rov id -
ing data regard ing presen ce and exten t of
recu rren t tum or and a id ing in p lann ing
th e m ode and scope of th erapy .
Index term s: L arynx , com puted tom og rap hy ,
271 .1211 #{149}arynx , n eo p lasm s, 27 1 .3 7 #{149}arynx ,
su rgery #{149} eck , com puted tom og raphy
Radiology 1984; 153: 713-717
* 1 F rom the M allinckro d t Inst itu te o f R adio log y
(D .J .D ., D .M .B ., S .S .S ., J .K .T .L .) and the D epartm en t o f
O tola ryn gology (R .E .H ., D .S .), W ash ing ton U niversity
S choo l o f M ed ic ine , S t. L ou is , M O . R ece ived M arch 22 ,
1 984 ; accep ted M ay 17 , 1984 .
#{176}RSNA ,1984 ht
C LIN ICA L eva lua tion of pa tien ts fo llow in g to ta l lary ngec tom y (TL )
frequen tly is d ifficu lt. Pa lpa tion is lim ited by po stsu rg ical
scar rin g an d rad ia tio n fib ro sis, w h ile ind irec t m irro r exam ina tion fa ils
to eva lua te the m ore caud al p ortions of the ph arynx . E ven esopha-
go scopy an d b iopsy m ay fa il to de tec t tum or recu rrence (1 ).
R ad iograph ic stud ies m ay prov ide h e lp in eva lua ting these pa tien ts .
B arium exam ina tion a ids in defin ing fis tu las , stric tu res, and tum or
recurren ce invo lv ing the ph arynx and esophagu s (2 ); it can no t,
how ever, ad equa tely assess lym ph node en largem en t on ex trano da l
tum or sp read . W hile no t focus ing on po stla ryngec tom y pa tien ts, re -
cen t rep orts h av e dem ons tra ted the u tility o f po stopera tive neck
com puted tom ograph y (CT ) fo r assessm en t o f tum or recurrence (3 -5 ),
sim ila r to its es tab lished ro le in p rim ary la ry ngea l m alignancy (6 , 7 ).
C onsequen tly , w e h ave correla ted pos tla ry ngec tom y CT find ings
w ith c lin ica l, su rg ica l, and p atho lo g ic da ta in 23 pa tien ts , in o rd er to
d iffe ren tia te the norm al from the pa tho log ic pos to pera tive C T ap-
pearance .
SURG ICAL CONSIDERAT IO NS
Tota l laryngec tom y is perfo rm ed for la ryng ea l neop lasm s tha t,
because of s ize on loca tion , a re no t am enab le to conserva tion surgery .
In g en eral, tho se tum ors th at invad e the laryngea l can tilages, ex tend
sub g lo ttica lly abou t the crico id cartilage , o r cause vo ca l co rd fixa tion
are best m an ag ed by th is typ e of su rgery . T um ors tha t recu r a fte rconserva tion su rgery or rad ia tion therapy a lso are trea ted by to ta l
la ryngec tomy.
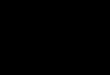
A fte r a low co lla r- ty pe inc ision and tn ach eo stom y, th e hy o id bo ne
is severed from th e sup nahyo id m u scu la tu re (F ig . la) . T he thyro id and
cn ico .id ca rtilages a re severed from the ir phary ngea l m uscu la r at-
tachm ents (F ig . ib ). T he inc ision is ex tended to encom pass the hyo id
bon e, ep ig lo ttis, anyep ig lo ttic fo ld s, pyn ifo rm fossae , thy ro id and
crico id cartilages, and true and fa lse vo ca l co rds . Th e resu ltan t an te rio r
phary ngea l defec t is c lo sed in lay ers: an inn er one of p haryng ea l
m ucosa ; a seco nd one com prising a v ariab le am ount o f cn icoph aryn-
g eu s and pharyng ea l co nstric to r m uscu la tu re ; an d an ou te rm os t layer
o f pen iphary ngea l co nnec tiv e tis su e. A con ical passagew ay ex tend ing
from the base of th e to ngue to the pro x im al esoph agus is fo rm ed , and
is te rm ed the n eo pharyn x (F ig . ic) (2 ) .
PAT IENTS AND M ETHODS
Review of the records from our institu tio n from 1980-1983 y ie ld ed 24 CT
stud ies o f the n eck in 23 pa tien ts w ho had undergon e to tal la ryngec tom y,
e ith er as prim a ry therapy for la ryn gea l c arcinom a or after fa i led rad iatio n
o r con servation surgery . T he popu lation inc lud ed 19 m en and fo ur w om en
w ith a m ean ag e of 6 4 yea rs. Tw enty p atie n ts had had rad iation th erapy as
w ell, and four had underg one u n ila te ra l rad ical neck d issec tion .
O f th e 23 pa tien ts , I 6 w ere re fe rred fo r C T eva lua tion because o f suspec ted
tum o r recu rrence , usu a lly because of sugg estive bu t incon c lu sive c lin ica l
eva lua tion s o n bec ause o f dysph agia . The exam ination w as requ ested to assess
ex ten t o f d is ease in tw o p atien ts w ith do cum en ted recurrenc e. F iv e asym p-
tom atic v o lu n teers w ere included a s a co ntro l g roup to def ine th e norm a l
pos to pera tive CT app earance .
8/3/2019 713neck After Total Laryngectomy
http://slidepdf.com/reader/full/713neck-after-total-laryngectomy 2/5
b.
‘4
I
-
Figu re 1
71 4 #{149}Radio logy Dec ember 1984
C.
///
II I
a and b . F ron tal (a) an d lateral (b ) dep ic tion s of the to tal lary ng ectom y procedure. Ii = hyo id b one ; m thy roh yo id m em brane; f = thyro id
car t i lage; c = c ric oid car tila ge; e ep ig lo t t is .
C. F orm a tion o f th e neo ph ary nx us ing m ucosal and m u scu lar la yers. ,i = neopharynx .
Genera lly , h ig h- reso lu t ion CT stu d ie s
w ere perfo rm ed w ith the pa tien t sup in e
and the neck ex tend ed ; scans w ere ob ta ined
from the ram i of the m andib le th rou gh the
upp er thorax to inc lude th e tracheos tom y
s ite . In tw o case s, the reg io n of th e tra ch e-
o stom y w as the a rea of clin ica l c onc ern , so
m ore cep halad lev els w ere n ot im aged .
Images w ere obtain ed using a 3-5 -secon dscan tim e , at 5 -m m inte rva ls w ith 5 -mm
collim a tion . In tra ven ou s con tra st m a ter ia l
w as adm in is tere d a t the d iscre tio n o f the
m on ito ring rad io log ist .
In the five n orm al vo lun tee rs, po sto per -
a tive fo llow -u p ran ged from 3.5 m onth s to
3 y ears w ith a m ean o f 1 8 m onth s. C lin ic al
fo llow -up after the C T scan in th is g rou p
averaged 4 m onth s. S ince gre ater than 9 0%
o f la ryn geal tum o r recu rren ces oc cur w ith in
2 years o f su rge ry or rad iat ion th erapy (8) ,
an d since the c lin ica l exam ina tio ns in these
asym ptom a tic pa tien ts rem ain ed u nre -
m ark ab le , they w ere th ought to define the
n orm al po sto pera tiv e ap pea ran ce. Th e re -
m ain ing 18 patien ts un derw en t op en bi-
opsy (12 c ase s), neck d issect ion (3 ca ses ),
p haryng oe sop hag oscop y (2 cases), o r en-
doscop ic b iopsy (1 case).
RESULTS
R etrosp ec tive ana lys is o f the po st-
la ryng ec tom y C T scans defined th ree
pa tien t g roup s: (I) those w ith n orm al
pos topera tive exam in a tion s; (II) pa -
tien ts w ith recu rren t tum or dem on-
s tra ted by CT ; (III ) p atien ts w ith CT
find ings m im ick ing tum or recur-
rence .
N orm al P ostoperativ e
Examina t ion s
In n ine pa tien ts th ere w as no s ig n
of tum or recu rrence ; th is g roup in -
c luded the f iv e asym ptom atic vo lun -
teens . In the vo lun tee rs , since no la -
ryn geal la ndm arks rem ained to act as
a gu ide , th ree leve ls hav e been chosen
to illu stra te the norm al pos to pera tive
appearance . T he m ost cep ha lad leve l is
a t the base of the ton gue , fo llow ed by
a m id neck leve l 2 -3 cm m ore caud a lly
and a low erm os t leve l a t the tracheos-
tom e, usua lly 3 -4 cm m ore caud a l.
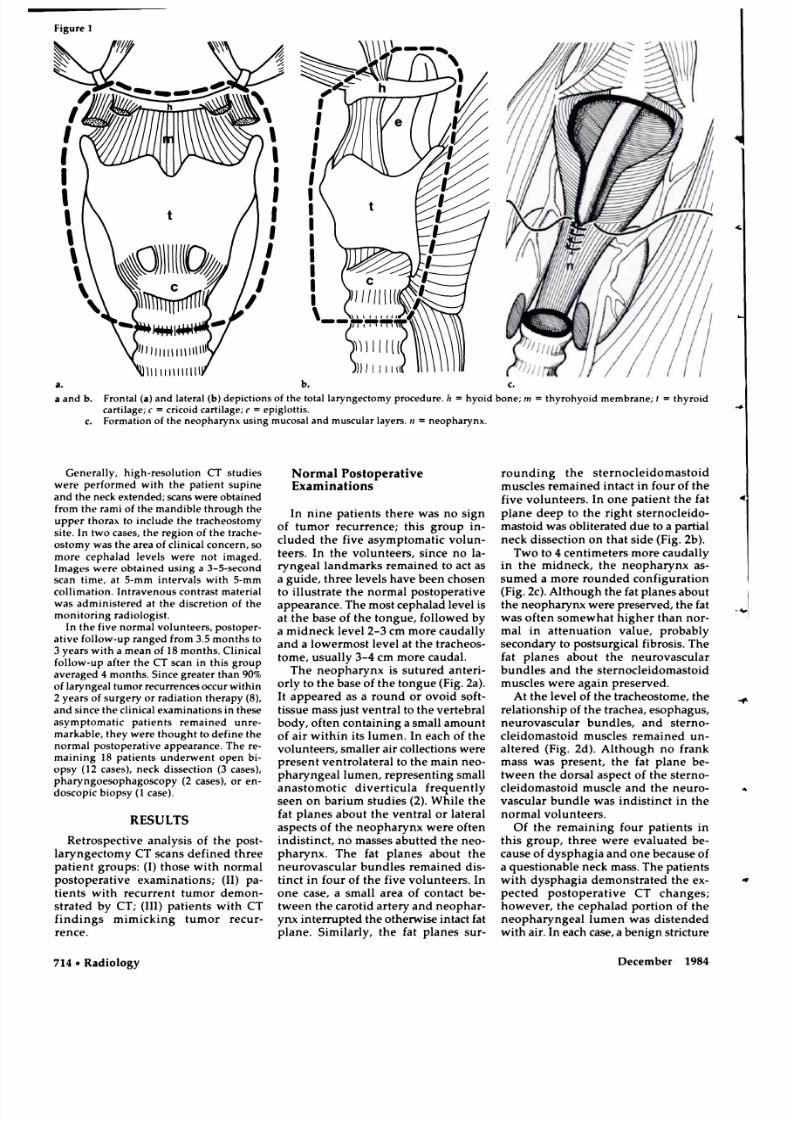
Th e neophary nx is su tu red an ten i-
o rly to the base of the tongu e (F ig . 2a ).
It ap peared as a roun d or o vo id so f t-
tis su e m ass jus t ven tra l to the verteb ra l
body , o ften con ta in ing a sm all am oun t
o f a ir w ith in its lum en . In each of the
vo lun tee rs , sm alle r a ir co llec tio ns w ere
presen t ven tro la te ra l to the m ain neo-pharyn gea l lum en , rep resen tin g sm all
anas tom otic d iv er ticu la frequen tly
seen o n barium stud ies (2 ). W h ile the
fa t p lanes abo u t the v en tral on la te ra l
asp ects o f the n eo pharyn x w ere often
ind istinc t, no m asses abu tted th e neo-
ph arynx . T he fa t p lanes abo u t the
neunovascu la r bu nd les rem ain ed d is -
tin ct in fou r o f the five vo lun tee rs . In
on e case , a sm all a rea of con tac t be -
tw een the caro tid a rte ry an d neoph ar-
yn x in te rrup ted th e o therw ise in tac t fat
p lane . S im ila rly , the fa t p lanes sun-
roun d ing the s ten noc le id om asto id
m uscles rem ained in tac t in fo ur o f the
five vo lun tee rs . In o ne pa tien t the fa t
p lane d eep to th e righ t s te rn oc leido -
m asto id w as ob lite ra ted due to a partia l
neck d issec tion on tha t side (F ig . 2b).
Tw o to 4 cen tim ete rs m ore cauda lly
in the m id neck , the n eo pharyn x as-
sum ed a m ore roun ded configu ra tion
(F ig . 2c ). A lth ough th e fa t p lan es abou t
the neoph arynx w ere prese rved , the fa t
w as often som ew hat h igh er than non-
m al in a ttenu ation va lu e , p robab ly
secon dary to pos tsu rg ica l fib rosis . T he
fa t p lanes abou t th e neunov ascu lan
bund les an d the s tenn oc le idom as to id
m usc les w ere again prese rved .
A t th e leve l o f the tracheos tom e, the
re la tio nsh ip o f the trachea , eso phagus ,
neun ovascu la r bund les , and s te rn o-
c le id om asto id m usc les rem ained un -
a ltered (F ig . 2d). A lth ough no fran k
m ass w as p resen t, th e fa t p lan e be-
tw een the dorsa l asp ec t o f the s terno-
c le id om asto id m uscle and the neuno-
vascu lar bun d le w as ind istinc t in the
no rm al vo lun tee rs .
O f th e rem ain ing fou r pa tien ts in
th is g ro up , th ree w ere eva lu ated be-
cause of d ysp hag ia and one b ecause of
a ques tion ab le n eck m ass . T he pa tien ts
w ith dysphag ia d em onstra ted the ex-
pec ted pos topera tive CT ch anges;
how ever, the cepha lad p ortio n of the
neoph ary ng eal lum en w as d iste nd ed
w ith a ir. In each case , a ben ign s tric tu re
8/3/2019 713neck After Total Laryngectomy
http://slidepdf.com/reader/full/713neck-after-total-laryngectomy 3/5
TABLE I: S ite o f R ecurren t T um or in 12
Patien ts
Site
N o. of
Patien ts
In tern al ju gu lar lym ph node s
(ad jac en t to neu rov ascu la r bun dle ,
neoph ary nx , or
ste rno cle idom asto id m usc le)
8
Pe ris tom al sof t t issue 3
Trachea 2
Mediast inum 2
N eck su bcutaneo us tis sue 2
b.
V olum e 153 N um ber 3 Rad io logy #{149} 15
o f the neo pha rynx w as d iagn osed b y
b arium exam in atio n and /on endoscop y
(F ig . 2e ). T h e pa tien t ev alu a ted fo r
question ab le neck m ass sh ow ed non -
m al pos topera tive ch an ges on CT , w ith
en dosco py and subseq uen t clin ica l
fo llow -up revealin g no tum o r recu r-
.1 rence.
Patien ts w ith R ecurren t Tum or
Tw elv e p atien ts had d ocum en ted
recu rren t on m eta sta tic neop la sm .
TA BLE I lis ts the site s in vo lved b y tum o r
and th e ir re la tive frequency . S eve ra l
pa tien ts h ad m ultip le site s o f invo lve -
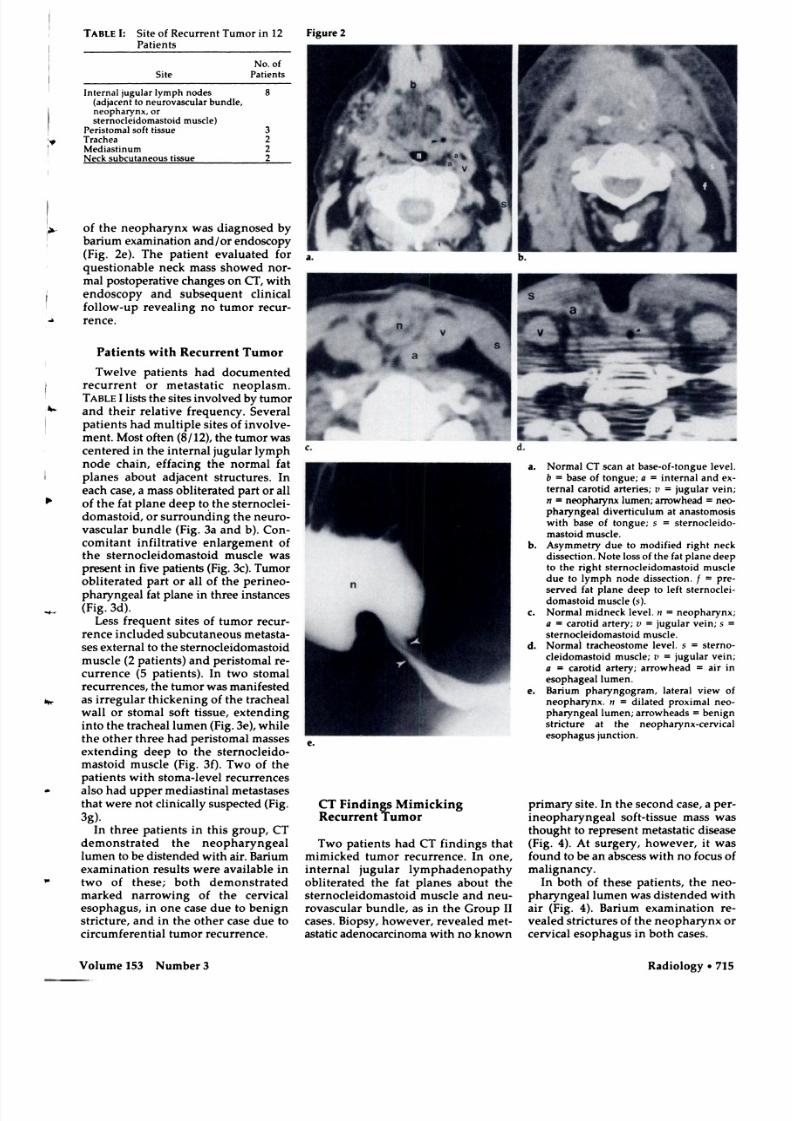
m en t. M ost o ften (8 /12 ) , the tum o r w as
cen tered in th e in terna l jug u la r lym ph
node ch ain , effac ing th e n orm a l fa t
p lan es abo u t ad jacen t struc tu re s . In
each case, a m ass ob lite ra ted p a rt on all
o f the fa t p lane d eep to the ste rn oc lei-
dom asto id , on su rrou nd in g the neuro -
v ascu lar bu nd le (F ig . 3a and b). C on-
com itan t in filtrativ e en largem en t o f
the ste rnoc le idom as to id m usc le w as
presen t in f ive pa tien ts (F ig . 3c ). T um o ro b lite ra ted pa rt o r all o f the pen ineo -
pharyngea l fa t p lane in th ree instances
-‘-V (F ig . 3d ).
L ess frequ en t sites o f tum o r recu r-
rence in clu ded sub cu tan eo us m e ta sta-
ses ex terna l to the stennoc le idom as to id
m usc le (2 p atien ts ) an d pen is tom a l re -
cun rence (5 pa tien ts). In tw o stom a l
recu rrences , the tum o r w as m an ifes ted
as irregu la r th icken in g of the trach ea l
w a ll o r stom a l so ft tissu e, ex tend in g
in to the trachea l lum en (F ig . 3 e) , w h ile
the o th e r th ree h ad pen is tom a l m asses
ex tend in g deep to th e ste rn oc le ido -
m asto id m u sc le (F ig . 3 f) . Tw o o f th e
pa tien ts w ith s tom a-lev el recu rrences
. a lso h ad upp er m ed iastin al m e ta sta se s
tha t w ere no t c lin ically su spec ted (F ig .
3g ) .
In th ree pa tien ts in th is g roup , C T
dem onstrated the n eo phanyngea l
lum en to b e d is ten ded w ith a ir . B arium
exam in atio n resu lts w ere ava ilab le in
tw o o f these ; bo th dem on stra ted
m arked n arrow in g of the ce rv ica l
e sop hagu s, in o ne case d ue to b en ign
str ic tu re , and in the o the r ca se du e to
c ircum fe ren tial tum or recu rrence .
Figure 2
CT F ind ings M im ick ing
R ecurren t Tum or
Tw o pa tien ts had CT fin d ing s th a t
m im icked tum o r recu rrence . In o ne ,
in terna l ju gu la r lym ph ad en opa thy
o b lite ra ted the fa t p lan es abou t the
s ten noc le idom asto id m usc le and n eu-
n ovascu la r bun d le , a s in the G roup II
ca se s. B iop sy , how eve r , revea led m et-
a sta tic adenocanc inom a w ith no know n
a . N o rm al C T scan at base-o f-to ng ue leve l.
b = base of tong ue ; a in te rna l and ex-
tenn al caro tid a rte r ie s; v = jugu la r ve in ;
n = neopharynx lum en ; a rrow head neo-
pha ry ng ea l d iv erticu lum a t an as tom o sis
w ith ba se o f tong ue; s sternocleido-
m as to id m usc le .
b . A symm etry d ue to m od ifie d r igh t ne ck
dissect ion . N o te lo ss of the fat p lan e deep
to the righ t s tern ocleid om asto id m u scledue to lym ph nod e d issec tion . f pre -
served fat p lane deep to lef t s te rnoc le i-
dom asto id m usc le ( s) .
C. N orm al m idneck leve l. n neopharynx ;
a c aro tid a rte ry ; v ju gu lar v ein ; s
ste rno cle idom as to id m uscle .
d . N orm a l trach eo stom e lev el. s = sterno-
c leidom as to id m usc le ; v = ju gu lar vein ;
a caro tid artery ; arrow head air in
esop hagea l lum en .
e. Bar ium ph ary ngogram , latera l v iew of
neopharynx . n dila ted prox im a l n eo-
ph ary ngeal lum en; a rrow head s ben ig n
stric tu re a t the neoph arynx-ce rv ica l
esop hagus junc tion .
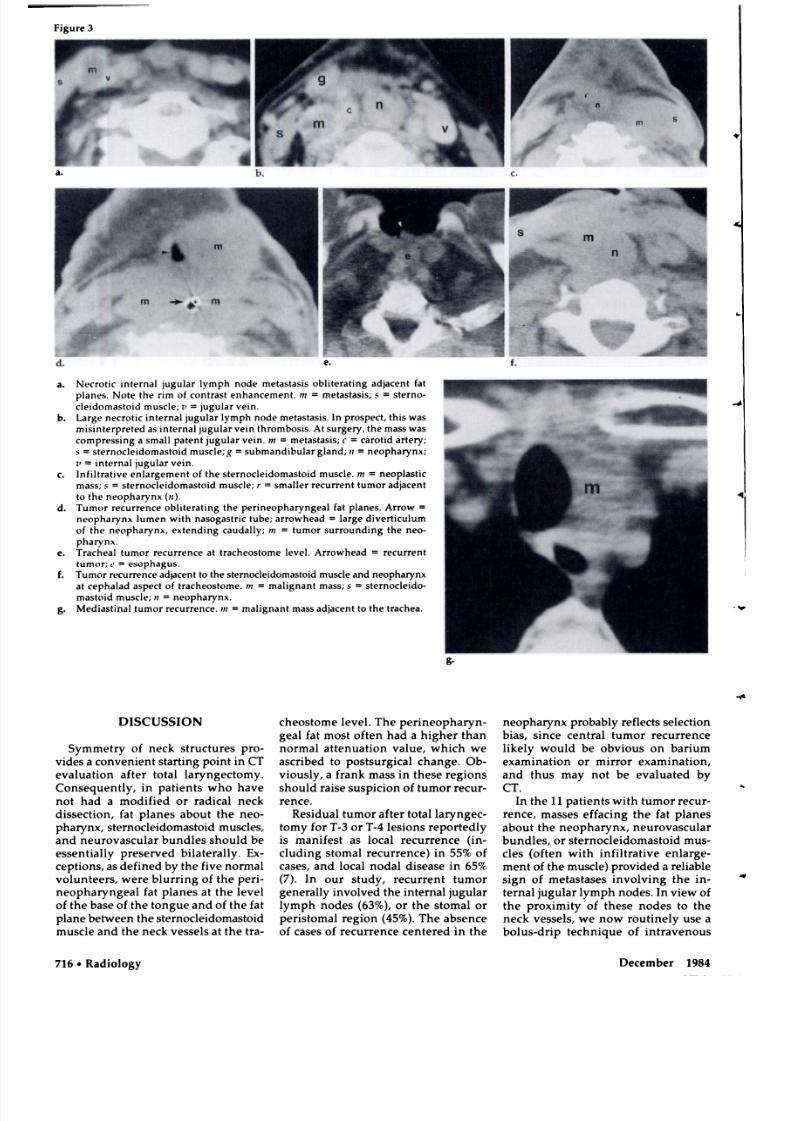
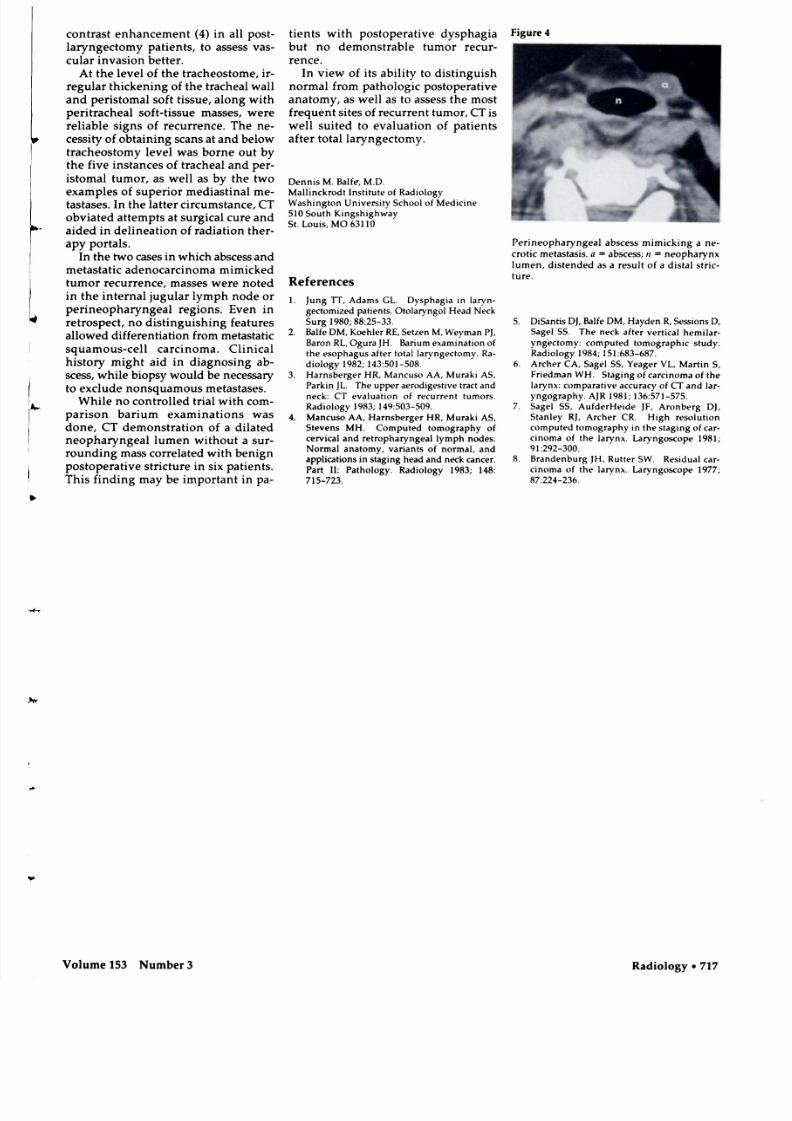
prim ary site . In the secon d case , a pe r-
ineophary ngea l so ft-tissue m ass w as
tho ugh t to rep re sen t m e ta sta tic d isea se
(F ig . 4 ). A t su rge ry , h ow ev er , it w as
fo un d to be an abscess w ith n o fo cu s o f
ma l i g n an cy .
In bo th o f these pa tien ts , the neo-
p ha ryn gea l lum en w as d istend ed w ith
a ir (F ig . 4 ). B arium exam in atio n re -
v ea led str ic tu res o f the n eo ph aryn x or
ce rv ica l e soph ag us in b o th cases.
8/3/2019 713neck After Total Laryngectomy
http://slidepdf.com/reader/full/713neck-after-total-laryngectomy 4/5
e.
g.
I
.4
Figure 3
71 6 #{149}Rad io logy D ecem ber 1984
a. N ecro tic in tern al ju gu lar lym ph nod e m eta stas is o b li tera tin g ad jac en t fa t
p lan es. N o te the rim o f con tra st enh an cem en t. in metastasis; s ste rno -
c leid om asto id m uscle ; z’ ju gu lar vein .
b. Large n ecro tic in tern al jugu lar lym ph nod e m e tastasis. In p ro spe ct, th is w as
m isin terpre ted as in te rna l ju gu lar vein throm bosis. A t surgery , the m ass w as
com pre ssin g a sm all pa ten t ju gu lar ve in . m me tastasis; c c aro tid ar tery ;
S = s ternoc leidom as to id m u scle; g su bm andib u la r g lan d ; neopharynx ;
1’ = in tern al ju gu lar v ein .
C. In filt ra tive en la rgem ent o f the sternoc leidom as to id m usc le . m neoplast ic
m a ss; s = sterno cleidom as to id m usc le; r sm alle r re cur ren t tum or ad jacen t
to th e neo ph ary nx (n ) .
d. T um or recurrence obliterating th e p erineo pha ryn geal fa t p lan es. A rrow
neoph ary nx lum en w ith n aso gas tric tub e; a rrow head la rge d ive rtic u lum
of the n eo pha ryn x , ex tend ing cau dally ; in tum o r surro un din g the neo-
pharynx .
e. T rach ea l tum or re cur ren ce a t tra cheostom e lev el. A rrow head re cu rren t
tum or ; = esophagus.
f. Tum o r recu rrence ad jacen t to the stern ocleid om asto id m usc le and n eo pha ryn x
at c eph alad a spe ct o f tracheo stom e . m m alig nan t m ass; s sternocleido-
m asto id m uscle ; z n eo pha ryn x .
g. M ed iast ina l tum or re cur ren ce. in = m alig nan t m a ss ad ja cen t to th e trachea .
DISCUSS ION
Symm etry of neck stru ctu res p ro -
v ides a co nven ien t sta r ting po in t in CTeva lua tio n afte r to ta l la ryn gec tom y .
C onsequ en tly , in pa tien ts w ho h av e
no t had a m odif ied o r rad ica l neck
d issec tion , fa t p lanes abo u t the neo-
pha ry nx , sterno cle idom asto id m usc les ,
and neurov ascu la r bu nd le s shou ld b e
essen tia lly p re se rved b ila tera lly . E x-
cep tion s, a s d efined by th e five no rm a l
v o lun tee rs , w e re b lu rrin g of the p en -
neo pha ryng ea l fa t p lanes a t the leve l
o f the base o f th e ton gue an d of th e fa t
p lan e be tw een th e ste rnoc le idom asto id
m u scle and th e neck v es sels a t the tra -
cheos tom e lev el. T he p en ineoph aryn -
g ea l fat m ost o ften had a h ighe r than
no rm al attenua tion v alue , w hich w e
asc r ibed to po stsu rg ica l ch an ge . O b -v io usly , a frank m ass in th ese reg ions
shou ld ra ise susp ic io n o f tum or recu r-
n en ce .
R es idua l tum or a fte r to tal la ryng ec -
tom y for T -3 on T -4 lesio ns reported ly
is m anifest as loca l recurren ce ( in -
c lud ing stom a l recu rrence ) in 55% of
cases, and loca l n oda l d isea se in 65%
(7 ). In ou r stu dy , recu rren t tum or
g en era lly in vo lv ed th e in te rna l jugu lar
lym ph nodes (63% ), on the s tom al o n
pen istom a l reg ion (45% ). Th e absen ce
of cases o f recu rrence cen tered in the
neopha ry nx p ro bab ly ref lects se lectio n
b ia s , s ince cen tra l tum o r recu rrence
like ly w ould be obv iou s on barium
exam ina tion or m irro r ex am ina tion ,and thu s m ay no t be eva lua ted by
CT .
In th e 1 1 p a tien ts w ith tum or recu r-
nence , m asses effac ing th e fa t p lan es
abo u t the neopha ry nx , neunovascu lan
bund les, on stenno cle idom asto id m us-
des (o ften w ith in filtrativ e en la rge -
m en t o f the m usc le ) p rov id ed a re liab le
sig n of m e ta stases in vo lv ing the in -
tenna l jug u la r lym ph nodes. In v iew o f
the p rox im ity o f th ese no des to th e
neck vesse ls , w e now ro u tine ly use a
bo lus-dn ip techn ique of in trav en ous
8/3/2019 713neck After Total Laryngectomy
http://slidepdf.com/reader/full/713neck-after-total-laryngectomy 5/5
Figu re 4
P erineo ph ary ngeal ab sces s m im ick ing a ne -
cro tic m e tastasis. a absc ess ; ii neopharynx
lum en , d is tend ed as a re su l t o f a d ista l stric-
tu re .
V olum e 153 N um ber 3 Radio logy #{149} 17
A t th e lev e l o f the tracheos tom e , in -
regu la r th icken in g o f the trach ea l w a ll
and pen istom a l so ft tissue , a lon g w ith
pe ritrach eal so ft-tissu e m asses, w e re
re liab le s igns of recurrence . The n e-
cess ity o f ob ta in in g scans a t an d be low
trach eostom y lev el w as bo rn e ou t b y
th e fiv e ins tan ces o f trachea l an d pe r-
is tom al tum o r, a s w e ll as b y the tw o
exam p les o f sup erio r m ed iastin al m e-
tas tases . In the la tte r c ircum stance , CT
obv ia ted attem p ts a t su rg ica l cu re an d
a ided in de linea tion o f rad iatio n th en -
apy porta ls .
In the tw o cases in w hich abscess and
m e ta sta tic adenoca rc inom a m im ick ed
tum or recu rrence , m asses w ere no ted
in the in te rn al jug u la r lym ph node or
p en ineop ha ry ngea l reg ions. E ven in
re tro spec t, n o d isting u ish in g fea tu re s
a llow ed d iffe ren tiatio n from m etasta tic
squam ou s-ce ll ca rc inom a . Clin ica l
h is to ry m ig h t a id in d iagn osing ab-
scess , w h ile b io psy w ou ld b e necessa ryto exc lude n onsq uam ous m eta sta se s.
W hile n o con tro lled tr ia l w ith com -
p an ison b arium exam ina tion s w as
don e, C T dem on stratio n of a d ilated
n eo ph aryn geal lum en w ithou t a sun -
rou nd in g m ass co rrela ted w ith b en ign
p osto pe ra tive str ic tu re in six pa tien ts .
This fin d ing m ay be im portan t in p a-
con trast enhan cem ent (4 ) in a ll pos t-
lary ngectom y p atie n ts , to as ses s vas-
cu lan in vasion be tter .
t ien ts w ith p ostop erative d ysp hag ia
bu t no dem onstrab le tum o r recu r-
rence.
In v iew of its ab ility to d is tin gu ish
norm al from patho lo g ic po stopera tive
ana tom y, as w ell as to assess the m ost
freq uen t site s o f recu rren t tum or, C T is
w e ll su ited to eva lua tion o f p atien ts
af te r to ta l la ryng ec tom y.
Dennis M . B alfe , M .D .
M a llin ck rod t Ins titu te of R adio log y
W ash ing ton U n ive rsity Sch ool o f M edicin e
51 0 South K ing sh ighw ay
S t. L ou is, M O 63110
References
1 . Ju ng T I , A dam s G L . D y sp hag ia in laryn-
ge ctom iz ed p atien ts . O to la ryn gol H ead N eck
Su rg 1980; 88 :25 -33 .
2 . B alfe DM , K oehle r RE , Se tzen M , W eym an PJ ,
B aron R L , O gura JH . B arium ex am ina tion of
the esoph ag us af ter to ta l laryng ectom y. R a -
d io lo gy 1982 ; 1 43 :50 1-5 08 .
3 . H arn sb erg er HR . M an cuso AA , M u rak i AS ,Park in JL . The u pp er a ero d ig estive trac t a nd
neck : C T ev alua tio n of re cu rren t tum o rs.
R ad io logy 1983; 1 49:503 -50 9 .
4 . M an cuso AA , H a rnsberger H R . M u rak i AS ,
S teven s MH . C om puted tom ograph y of
cerv ica l an d retro ph ary ngeal lym ph node s:
N orm al anatom y , var ian ts o f n orm al, and
ap plic ations in sta g in g head an d neck can cer .
Part I I: P a tho logy . R ad io log y 1983; 14 8:
715-723 .
5 . D iS an tis D J, B a lfe DM , H ayd en R , S ess ion s D ,
S age l 5 5 . T he neck a fte r ver tica l hem ilar-
y ngectom y : com puted tom ograph ic stu dy .
R adio lo gy 1984; 15 1:6 83 -68 7 .
6. A rcher CA , Sag el 55 , Y eager V L , M ar tin 5 ,
F riedm an W H . S tag ing of carc inom a o f the
la ryn x: com para tive accura cy of CT and lar-
y ng ograph y . A JR 1981; 1 36:571 -57 5 .
7 . S ag el 55 . A u fd erH eid e JF , A ronb erg D J,
S tan ley R J, A rche r C R . H igh reso lu tion
com pu ted tom ograph y in the stag ing o f ca r-
cin om a of the larynx . La ryn goscop e 1981;
91 :292-300 .
8. B randenbu rg JH , Ru tter SW . R esid ua l ca r-
cin om a of the larynx . L ary ngo sco pe 1977 ;
87 :224-236 .