Embed Size (px)
Citation preview

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 1/104
GASTROINTESTINAL
SYSTEM
FUNCTION: DIGESTION, ABSORPTION,
ELIMINATION
COMPOSITION: ALIMENTARY CANAL,ACCESSORY ORGANS
PERISTALSIS ± wavelike motion that propels substances within the GIT
SPHINCTERS / VALVES: controls rate of
peristalsis / prevents regurgitation

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 2/104
D
I
G
E
S
T
I
V
E
T
R A
C
T

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 3/104
NURSING AND PATIENT CARECONSIDERATION:
Common practices are the following; for 3 days
before the test and during the stool collection period:
1. Diet should have a high fiber content.2. Avoid red meat in the diet.
Avoid food with a high peroxide content, such as
turnips,cauliflower,broccoli,horseradish,and melon.
Avoid enemas or laxatives before the stool specimencollection.
Avoid iron preparations,iodides,bromides,aspirin,no
steroidal anti-inflammatory drugs (NSAIDs), or
vitamin C supplements greater than 250 mg/day
DIAGNOSTIC TESTS:
�LABORATORY TESTS:
�A. HEMOCCULT GUAIAC TESTS:

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 4/104
B. HYDROGEN BREATH TEST
1. It is used to evaluate carbohydrate absorption.
2. A radioactive substance is ingested, and after acertain time period, exhaled gases are measured.
3.the test measures the amount of hydrogen
produced in the colon,absorbed in the blood,and
then exhaled in the breath.
4. This test is used as a diagnostic test for short
bowel syndrome,lactose intolerance, and bacterial
overgrowth of the intestine( blind loopsyndrome,Crohn's disease,distal ilea disease).

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 5/104
B. HYDROGEN BREATH TEST
NURSING CONSIDERATIONS:The patient should be NPO 12 hours before the
procedure.
The patient should not smoke after midnight
before the test.
Antibiotics and laxative/enemas should not be
used for 1 week before the test. These products
may alter the laboratory results.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 6/104
RADIOLOGY AND IMAGING STUDIES
UPPER GASTROINTESTINAL SERIES AND SMALLBOWEL SERIES
1. Upper GI series and small-bowel series arefluoroscopic x-ray examinations of theesophagus, stomach, and small intestine afterthe patient ingests barium sulfate.
2. As the barium passes through the GI tract,fluoroscopy outlines the GI mucus and organs.
3. Spot films record significant findings.
4. Double-contrast studies administer barium
first followed by a radio lucent substance, suchas air, to produce a thin layer of barium to coatthe mucusa.
This allows for better visualization of any type
of lesion..

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 7/104
UPPER GASTROINTESTINAL SERIES AND SMALL
BOWEL SERIES
NURSING AND PATIENT CARECONSIDERATIONS
1. Explain procedure to patient.
2. Instruct patient to maintain low-residue dietfor 2 to 3 days before test and a clear liquiddinner the night before the procedure.
3. Emphasize NPO after midnight before thetest.
4. Encourage patient to avoid smoking, alcohol,caffeine before the test.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 8/104
5. Explain that the health care provider mayprescribe all narcotics and anticholinergics to
be held 24 hours before the test.6. Tell the patient that he or she will beinstructed at various times throughout theprocedure to drink the barium (480 to 600 mL).
7. Explain that a cathartic will be prescribedafter the procedure.
8. Instruct the patient that stool will be light incolor for the next 2 to 3 days from the barium.
9. Instruct patient to notify health careprovider if he or she has not passed the bariumin 2 to 3 days
10. Note that water-soluble iodinated contrast

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 9/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 10/104
NURSING AND PATIENT CARE CONSIDERATIONS
1. Explain to the patient:
A. What the x-ray procedure involves.
B. That proper preparation provides a more accurate view
of the tract and that preparations may vary.
C. That it is important to retain the barium so all surfaces of
the tract are coated with opaque solution.
2. Instruct the patient on the objective of having the largeintestine as clear of fecal material as possible:
A. The patient may be given a low-residue, low-fat diet, 1 to
3 days before the examination.
B. The day before the examination, intake may be limited toclear liquids (no drinks with red dye).
C. The day before the examination, an oral laxative,
suppository, and/or cleansing enema may be prescribed

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 11/104
3. The patient will be NPO after midnight the day of procedure.
4. An enema or cathartic may be ordered after thebarium enema.
5. Inform the patient that barium may cause light-colored stools for several days after the procedure.
ULTRASONOGRAPHY1. A noninvasive test focuses high-frequency soundwaves over an abdominal organ to obtain an imageof the structure.
2. Ultrasound can detect small abdominal masses,fluid-filled cysts, gallstones, dilated bile ducts,ascites, and vascular abnormalities.
3. Ultrasound with Doppler may be ordered for
vascular assessment.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 12/104
NURSING AND PATIENT CARE CONSIDERATIONS
1. If indicated, prepare the patient before the procedure with
a special diet, laxative, or other medication to cleanse thebowel and decrease gas.
2. Abdominal ultrasound usually requires the patient to be
NPO for at least 6 hours before the procedure.
3. Change position of patient, as indicated, for bettervisualization of certain organs.
COMPUTED TOMOGRAPHY (CT) SCAN
1. This is an x-ray technique that provides excellent
anatomic definition and is used to detect tumors, cysts, andabscesses.
2. The CT can also detect dilated bile ducts, pancreatic
inflammation, and some gallstones.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 13/104
3. It identifies changes in intestinal wall
thickness and mesenteric abnormalities.
4. Ultrasound and CT can be used to perform
guided needle aspiration of fluid or cells from
lesions anywhere in the abdomen. The fluid or
cells are then sent for laboratory tests (such as
cytology or culture).
NURSING AND PATIENT CARE
CONSIDERATIONS
1. Instruct the patient that fasting for 4 hoursbefore the procedure and an enema or
cathartic may be necessary. This is to cleanse
the bowel for better visualization.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 14/104
2. Ask the patient if she is pregnant. If yes, do not
proceed with scan and notify health care provider.
3. Ask if there are known allergies to iodine or
contrast media. A contrast medium may be given
intravenously (IV) to provide better visualization of
body parts. If allergic, notify the technician and
health care provider immediately.
4. Instruct the patient to report symptoms of itching
or shortness of breath if receiving contrast media,
and observe patient closely.
ENDOSCOPIC PROCEDURESEndoscopy is the use of a flexible tube (the
fiberoptic endoscope) to visualize the GI tract and
to perform

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 15/104
certain diagnostic and therapeutic procedures.Images are produced through a video screen ortelescopic eyepiece. The tip of the endoscope moves
in four directions, allowing for wide-anglevisualization. The endoscope can be insertedthrough the rectum or mouth, depending on whichportion of the GI tract is to be viewed.
Endoscopes contain multipurpose channels thatallow for air insufflation, irrigation, fluidaspiration, and the passage of special instruments.These instruments include biopsy forceps, cytologybrushes, needles, wire baskets, laser probes, andelectrocautery snares.
Endoscopic functions other than visualizationinclude biopsy or cytology of lesions, removal of foreign objects or polyps, control of internal
bleeding, and opening of strictures.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 16/104
ESOPHAGOGASTRODUODENOSCOPY
(EGD)
1. This allows for visualization of the esophagus,stomach, and duodenum.
2. EGD can be used to diagnose acute or chronicupper GI bleeding, esophageal or gastric varices,polyps, malignancy, and gastroesophageal reflux.
3. Instruments passed through the scope can beused to perform a biopsy or cytologic study,
remove polyps or foreign bodies, control bleeding,or open strictures.
NURSING AND PATIENT CARECONSIDERATIONS
1. Explain the following to the patient:

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 17/104
A. The type of procedure to be performed on the patient. As
an outpatient, advise that someone must accompany the
patient to drive home due to the patient being sedated.
B. NPO for 8 to 12 hours before the procedure to preventaspiration and allow for complete visualization of the
stomach.
C. Remove dentures and partial plates to facilitate passing
the scope and preventing injury.
2. Inform the health care provider of any known allergies
and current medications. Medications may be held until the
test is completed.
3. Obtain prior x-rays, and send with the patient.
4. Describe what will occur during and after the procedure:
A. The throat will be anesthetized with a spray or gargle.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 18/104
B. An IV sedative will be administered.
C. The patient will be positioned on the left side with a towel
or basin at the mouth to catch secretions.
D. A plastic mouthpiece will be used to help relax the jaw
and protect the endoscope. Emphasize that this will not
interfere with breathing.
E. The patient may be asked to swallow once in a while asthe endoscope is being advanced. The patient should not
swallow, talk, or move tongue. Secretions should drain from
the side of the mouth, and the mouth may be suctioned.
F. Air is inserted during the procedure to permit better
visualization of the GI tract. Most of the air is removed at
the end of the procedure. The patient may feel bloated, burp,
or pass flatus from remaining air.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 19/104
G. Keep patient NPO according to protocol until patient isalert and gag reflex has returned.
H. May resume regular diet after gag reflex returns and
tolerating fluids.I. May experience a sore throat for 24 to 36 hours after theprocedure. When the gag reflex has returned, throatlozenges or warm saline gargles may be prescribed forcomfort.
5. Monitor vital signs every 30 minutes for 3 to 4 hours, andkeep the side rails up until the patient is fully alert.
6. Monitor the patient for abdominal or chest pain, cervicalpain, dyspnea, fever, hematemesis, melena, dysphagia,lightheadedness, or a firm distended abdomen. These mayindicate complications.
7. Instruct the patient on the above listed signs andsymptoms, and advise to report immediately should anyoccur, even after discharge.
8. Possible complications include perforation of the

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 20/104
esophagus or stomach, pulmonary aspiration,
hemorrhage, respiratory depression or arrest,
infection, cardiac arrhythmias or arrest.PROCTOSIGMOIDOSCOPY AND COLONOSCOPY
1. Proctosigmoidoscopy (rectosigmoidoscopy) is the
visualization of the anal canal, rectum, and sigmoid
colon through a fiberoptic sigmoidoscope.2. Colonoscopy is the visualization of the entire large
intestine, sigmoid colon, rectum, and anal canal.
3. Sigmoidoscopy or colonoscopy can be used to
diagnose malignancy, polyps, inflammation, or
strictures.
4. Colonoscopy is used for surveillance in patients with
a history of chronic ulcerative colitis, previous colon
cancer, or colon polyps.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 21/104
5. Lower GI endoscopy can be used to perform
biopsy, remove foreign objects, or obtain
specimen for culture or cytology.
6. Colonoscopy, a more extensive procedure
than proctosigmoidoscopy, requires several
days of bowel preparation and use of conscioussedation during the procedure. The bowel
preparation includes approximately 1 gallon or
less iso-osmolar electrolyte solution to consume
over a 3- to 4-hour period the day before theprocedure, clear liquid diet the day before the
procedure, and an oral laxative the night
before the procedure. Protocols may vary.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 22/104
NURSING CARE:
1. Verify the patient¶s compliance with the
pretest bowel preparation the day before theprocedure, usually an oral laxative (such as
magnesium citrate) and a clear liquid diet.
2. The patient must be NPO after midnight.3. Explain to the patient that a feeling of
fullness will occur when water is introduced
into the GI tract. This eliminates air space
and provides for high resolution.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 23/104
4. Observe the patient for a change in vital signs,
bleeding, pain, vomiting, abdominal distention or
rigidity.5. Ensure that patients who have had endoscopic
procedures requiring sedation have a caregiver to
drive home after the procedure.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 24/104
PURPOSES OF ENEMA ADMINISTRATION
1. Bowel preparation for diagnostic tests or surgery
to empty the bowel of fecal content.2. Delivery of medication into the colon ( such asenemas containing neomycin to decrease thebowel¶s bacteria count or a kayexalate enema to
decrease the serum potassium level)3. To soften the stool ( oil-retention enemas)
4. To relieve gas( tidal,milk and molasses,or fleetenemas)
5. Promote defecation and evacuate feces from thecolon for patients with constipation or animpaction.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 25/104
NASOGASTRIC AND NASOINTESTINAL
INTUBATION
Nasogastric intubation refers to the insertion of atube through the nasopharynx into the stomach.
Nasointestinal intubation is performed by insertinga small-bore tube, that is carried by way of peristalsis into the duodenum or jejunum. It isprimarily used for intestinal decompression,administering feedings and maintaining nutritionalintake.
PURPOSES OF NASOGASTRIC INTUBATION
Remove fluid and gas from the stomach(decompression).
Prevent or relieve nausea and vomiting aftersurgery or traumatic events by decompressing thestomach.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 26/104
Determine the amount of pressure and motor
activity in the GI tract (diagnostic studies).Irrigate the stomach (lavage) for active bleeding orpoisoning.
Treat mechanical obstruction.
Administer medications and feeding (gavage)directly into the GI tract.
Obtain a specimen of gastric contents for laboratorystudies when pyloric or intestinal obstruction is
suspected.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 27/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 28/104
Administer TPN at a constant rate, using an infusion pump.
The infusion should never be stopped abruptly. Administer
dextrose 10% in water if you must stop the infusion. During
the TPN administration, the pancreas secretes increasedinsulin; abrupt cessation can cause hypoglycemia.
Maintain strict asepsis. Use an occlusive dressing and change
the dressing,tubing and filter every 48 hours.
Monitor blood glucose levels or check urine for glucose every6 hours. Note that the client might need insulin.
Observe the client for headache,nausea,vomiting and fever.
These indicate an allergy to the protein.
Closely monitor intake and output.
Weigh the client daily. Expect a weight gain of ¼ lb per day.
Never use a filter with fat emulsions. Monitor for nausea
and fever, which are common adverse reactions.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 29/104
GASTRITISGASTRITIS is an inflammation of the gastric mucosa
(the stomach lining). It may be acute or chronic.
Acute gastritis produces mucosal reddening, edema,hemorrhage, and erosion. Chronic gastritis is
common among elderly people and people with
pernicious anemia. In chronic atrophic gastritis, all
stomach mucosal layers are inflamed.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 30/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 31/104
POSSIBLE CAUSES:
Acute gastritis
Chronic ingestion of irritating foods, spicy foods or
alcohol
Drugs, such as aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs)(in large doses),cytotoxic agents, caffeine, corticosteroids,
antimetabolites, phenylbutazone, and indomethacinIngestion of poisons, especiallydichlorodiphenyltrichloroethane (DDT), ammonia,mercury, carbon tetrachloride, and corrosive
substancesEndotoxins released from infecting bacteria, suchas staphylococci, Escherichia coli, and salmonella,viruses (gastroenteritis)

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 32/104
CHRONIC GASTRITIS:
1. Alcohol ingestion2. Cigarette smoke
3. Environmental irritants
4. Peptic ulcer diseaseASSESSMENT FINDINGS:
- Abdominal cramping
- Epigastric discomfort- Hematemesis
- Indigestion

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 33/104
DIAGNOSTIC EVALUATION:
1. Fecal occult blood test can detect occult
blood in vomitus and stools if the clienthas gastric bleeding.
2. Blood studies show low Hgb level andHct when significant bleeding hasoccurred.
3. Upper GI endoscopy with biopsyconfirms the diagnosis when performed
within 24hrs of bleeding.4. Upper GI series may be performed to
exclude serious lesions.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 34/104
TREATMENT:
-Blood transfusion
-I.V. fluid therapy-NG lavage to control bleeding
-Oxygen therapy, if necessary
-Partial or total gastrectomy (rare)-Vagotomy and pyloroplasty (limitedsuccess when conservative treatments havefailed)
IMPLEMENTATION:
1.If the client is vomiting, give antiemeticsand I.V. fluids to prevent dehydration and
electrolyte imbalance.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 35/104
2. Monitor fluid intake and output and electrolytelevels.
3. Provide a bland diet to prevent recurrence.
4. Offer smaller, more frequent meals to reduceirritating gastric secretions. Eliminate foods thatcause gastric upset.
5. If surgery is necessary, prepare the client
preoperatively and provide appropriatepostoperative care to decrease preoperative anxietyand prevent intraoperative and postoperativecomplications.
6. Administer antacids and other prescribedmedications
7. Urge the client to take prophylactic medications asprescribed to prevent recurring symptoms.
8. Provide emotional support.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 36/104
HIATAL HERNIA
A. ETIOLOGY
1. Portion of the stomach protruding througha hiatus (opening) in the diaphragm into the
thoracic cavity.
2. May result from a congenital weakness of the diaphragm or from injury, pregnancy, orobesity.
3. Function of the cardiac sphincter is lost,gastric juices enter the esophagus causinginflammation.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 37/104
Signs/symptoms

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 38/104
B. CLINICAL FINDINGS:
1. Subjective: substernal burning pain or
fullness after eating; dyspepsia in therecumbent position; nocturnal dyspnea.
2. Objective: GI series and endoscopy showprotrusion of the stomach through thediaphragm; regurgitation
C. THERAPEUTIC INTERVENTIONS:
1. Small, frequent, bland feedings.
2. Pharmacologic management: antacids,
antisecretory agents, antiemetics, especiallythose that promote gastric emptying
3. Surgical repair (done infrequently)
Fundoplication

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 39/104
PEPTIC ULCER DISEASE
(PUD)
A. ETIOLOGY:
1. Ulcerations of the gastrointestinal mucus
and underlying tissues caused by gastric
secretions that have a low pH (acid)
2. Causes include conditions that increase the
secretion of hydrochloric acid by the gastricmucosa or that decrease the tissue¶s resistance
to the acid.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 40/104
a. infection of the gastric and / or duodenal
mucusa by Campylobacter pylori or
Helicobacter pylori.
b. Zollinger ± Ellison syndrome: tumors
secreting gastrin, which will stimulate the
production of excessive hydrochloric acid.
c. certain drugs such as aspirin,steroids, andindomethacin will decrease tissue resistance.
d. smoking
3. Peptic ulcers may be present in the esophagus,
stomach, or duodenum ( most common site ).
4. Complication include pyloric or duodenal
obstruction, hemorrhage and or perforation.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 41/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 42/104
C. THERAPEUTIC INTERVENTIONS:
1. Bland foods, and restriction of irritating
substances.2. Antibiotic therapy if microorganism isidentified; tetracycline, metronidazole, andbismuth
3. Histamine H2 receptor antagonists orproton pump inhibitors, antacids
4. Sedatives, tranquilizers, anticholinergics,and analgesics
5. Antiemetics6. A nasogastric tube for decompression,
installation of vasocontrictors, and/or salinelavages when hemorrhage occurs.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 43/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 44/104
g. Common complications of total or partial
gastric resection:
(1) Dumping syndrome
(2) Hemorrhage
(3) Pneumonia
(4) Pernicious anemia
GASTRIC SURGERIES

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 45/104
GASTRIC SURGERIES

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 46/104
NURSING CARE:
1. Allow ample time for the client toexpress feelings and concerns.
2. Administer and assess effects of
sedatives, antacids, anticholinergics, H2
receptor antagonists, antibiotics, and
dietary modifications.
3. Encourage hydration to reduce
anticholinergic side effects and dilutethe hydrochloric acid in the stomach.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 47/104
4. Instruct client to:
a.Eat small to medium-sized meals becausethis helps prevent gastric distention;
encourage between-meal snacks to achieve
adequate calories when necessary.
b.Avoid foods that increase gastric acidsecretion or irrigate gastric mucosa.
c.Avoid foods that cause distress; varies for
individuals but common offenders are the
gas producers (legumes, carbonated
beverages, vegetables).

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 48/104
d. eat meals in pleasant, relaxing
surrounding to reduce acid secretions.
e. administer calcium and iron
supplements as ordered if client's
medication increases gastric pH.
5. Refrain from administering drugs such
as salicylates, NSAIDS, steroids,and
ACTH.
6. Observe for complications such asgastric hemorrhage,perforation and drug
toxicity.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 49/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 50/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 51/104
WOW!!! BEACH
BREAK MUNA ! ! !
MAG COCA COLA ! ! !

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 52/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 53/104
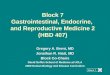
DIVERTICULAR DISEASE

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 54/104
DIVERTICULAR DISEASE
Diverticular disease has 2 clinical forms:
DIVERTICULOSIS andDIVERTICULITIS. Diverticulosisoccurs when the intestinal mucosaprotrudes through the muscular wall.
The common sites for diverticula are inthe descending and sigmoid colon, butthey may develop anywhere from theproximal end of the pharynx to the anus.
Diverticulitis is an inflammation of thediverticula that may lead to infection,
hemorrhage, or obstruction.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 55/104
POSSIBLE CAUSES:
Age (most common in people over age 40)
Chronic constipation, more common in
obese individuals
Congenital weakening of the intestinal wallLow intake of roughage and fiber
Straining during defecation
Stress
Men affected more than women
ASSESSMENT FINDINGS:

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 56/104
ASSESSMENT FINDINGS:
- Anorexia
- Stool with blood and mucus
- Change in bowel habits
- Constipation and diarrhea
- Fever
- Flatulence
- Intermittent left lower quadrant pain
or midabdominal pain that radiates to the
back - Nausea
- Rectal bleeding

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 57/104
DIAGNOSTIC EVALUATION:
1)Barium enema (contraindicated in clients with
acute diverticulitis) shows inflammation, narrowlumen of the bowel, and diverticula.
2)Hematologic study shows increased WBC count
and ESR.
3)Sigmoidoscopy (contraindicated in clients with
acute diverticulitis) shows a thickened wall in
the diverticula.
4)Computed tomography scan shows abscesses or
thickening of the bowel.
TREATMENT:

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 58/104
TREATMENT:
- Generally no treatment for asymptomaticdiverticulosis
- Colon resection (for diverticulitis refractory tomedical treatment)
- High residue diet with no seeds for diverticulosis
- Low residue diet with diverticulitis
- Bland diet, stool softeners, and occasional doses of mineral oil for diverticulosis with pain, mild GIdistress, constipation, or difficult defecation.
- Bland diet (for diverticulosis after pain subsides)
or liquid diet (for mild diverticulitis ordiverticulosis before pain subsides); low-fiber dietindicated following the liquid diet; when the client isasymptomatic, low-fat, high-fiber diet
recommended.
Temporary colostomy possible for perforation peritonitis

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 59/104
- Temporary colostomy possible for perforation, peritonitis,
obstruction, or fistula that accompanies diverticulitis.
� IMPLEMENTATION:1. Asses abdominal distention and bowel sounds to determine
baseline and detect changes in the clients condition.
2. Monitor and record vital signs, intake and output, and
laboratory studies to assess fluid status.3. Monitor stools for occult blood to detect bleeding.
4. Maintain the clients diet to improve nutritional status and
promote healing.
5. Maintain position, patency, and low suction of NG tube toprevent nausea and vomiting
6. Keep the client in semi-Fowler¶s position to promote
comfort and GI emptying.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 60/104
7. Prepare the client for surgery, if necessary
(administer cleansing enemas, osmoticpurgative, and oral and parenteral antibiotics),
to avoid wound contamination from bowel
contents during surgery.
8. Provide postoperative care (watch for signs of infection; perform meticulous wound care;
watch for signs of postoperative bleeding; assist
with turning, coughing, and deep breathing;
teach ostomy self-care) to promote healing andprevent complications.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 61/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 62/104
CROHN¶s DISEASE
(Regional Enteritis)
CROHN¶sDISEASE is a chronic inflammatorydisease of the small intestine, usually affectingthe terminal ileum. It also sometimes affectsthe large intestine, usually in the ascendingcolon. It¶s slowly progressive withexacerbations and remissions.
POSSIBLE CAUSES:
Emotional upsets
Fried foods
Milk and milk products
Unknown

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 63/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 64/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 65/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 66/104
Antidiarrheal: diphenoxylate (Lomotil)
Antiemetic: prochlorperazine (Compazine)
Anti-inflammatory: olsalazine (Dipentum)
Corticosteroid: prednisone (Deltasone)
Immunosupressant: mercaptopurine(Purinethol), azathioprine (Imuran)
Potassium supplement: potassium chloride (K-
Lor) administered with food, potassium
gluconate (Kaon)
IMPLEMENTATION:

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 67/104
IMPLEMENTATION:
Bedrest, weigh daily
NPO in acute stage, TPN as ordered.High CHON, calorie, bland, low residue diet.
Avoid gas-producers, irritating food, andmilk products.
Offer small frequent feedings.
Vitamin replacement ADEK.
IVF, I/O, tepid fluids up to 3L/day.
Perianal care with lubricants and ointments.
Hot sitz baths, monitor stools.
Emotional support esp. family members.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 68/104
Administer medications, as prescribed, tomaintain or improve the client¶s condition.
Maintain the client¶s diet; withhold food andfluid as necessary to minimize GI discomfort.
Minimize stress and encourage verbalization of feelings to allay the client¶s anxiety.
If surgery is necessary, provide postoperativecare (monitor vital signs; monitor dressings fordrainage; monitor ileostomy drainage andperform ileostomy care as needed; assessincision for signs of infection; assist withturning, coughing, and deep breathing; get theclient out of bed on the 1st postoperative day if stable) to promote healing and preventcomplications.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 69/104
Autoimmune disease

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 70/104
Emotional stress
Viral and bacterial infections
ASSESSMENT FINDINGS:
Abdominal cramping, distention, and tenderness
Anorexia
Bloody, purulent, mucoid, watery stools (15 to 20per day)
Dehydration
Fever
Hyperactive bowel soundsNausea and vomiting
Weakness
Weight loss

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 71/104
IMPLEMENTATION:

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 72/104
Assess GI status and fluid balance to determinedeficient fluid volume.
Monitor and record vital signs, intake andoutput, laboratory studies, daily weight, urinespecific gravity, calorie count, and fecal occultblood to determine deficient fluid volume.
Monitor the number, amount, and character of stools to determine status of nutrientabsorption.
Maintain the client¶s diet; withhold food and
fluid as necessary to prevent nausea andvomiting.
Administer I.V. fluids and TPN to maintainhydration and improve nutritional status.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 73/104
Maintain position, patency, and low suction of
NG tube to prevent nausea and vomiting.
Keep the client in semi-Fowler¶s position to
promote comfort.
Administer medications, as prescribed, to
maintain or improve the client¶s condition.Provide skin, mouth, nares, and perianal care
to promote comfort and prevent skin
breakdown.
OSTOMY CARE

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 74/104
OS O C
Referral to enterostomal therapist.
Encourage verbalization of fears/concerns.
Teach character of drainage: ileostomy ± liquid 4-6x/day,transverse colostomy ± mushy OD, descending/sigmoid ± soft
formed q 2-3 days
Skin care ± nystatin, karaya powder, soap/H2O pat dry
Odor control ± deodorant drops, bismuth tabs, mouthwashsolutions, spinach, parsley added to ostomy bag.
Odor ± avoid gas-formers (cabbage, beans, broccoli,
cauliflower, corn, onions, eggs, fish, condiments.
Diet ± ileostomy (clear liquids, strained fruits/veggiesprogress to regular diet, Na/K rich food, avoid fried,
seasoned food, nuts, raisins, raw fruits)
colostomy ± clear liquid, solid low-residue 1st 6 weeks
Ileostomy drainage q 4-6 hrs emptied, pouch 5-7 days max

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 75/104
OSTOMY IRRIGATION
Only colostomies are irrigated; ileostomy no need
Purposes ± stimulate emptying of colon to avoid use
of appliance
Started 5-7 days post-op in the bathroom preferably
Equipment: irrigating solution, catheter with stomatip, irrigating sleeve
Tepid water used 18-24 in above stoma (shoulder
height)
500-1000ml irrigated slowly
Done same time everyday / as preferred
Return flow expected within 15-45 mins
INTESTINAL OBSTRUCTIONS

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 76/104
INTESTINAL OBSTRUCTIONS
HEMORRHOIDS

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 77/104
HEMORRHOIDSA. GENERAL INFORMATION:
1. Congestion and dilation of the veins of therectum and anus; usually result from impairment of flow of blood through the venous plexus.
2. May be internal (above the anal sphincter) or
external (outside anal sphincter).3. Most commonly occur between ages 20-50.
4. Predisposing conditions include occupationsrequiring long periods of standing; increased intra-
abdominal pressure caused by prolongedconstipation, pregnancy, heavy lifting, obesity,straining at defecation; portal hypertension.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 78/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 79/104
2 Assess for rectal bleeding; inspect rectal

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 80/104
2. Assess for rectal bleeding; inspect rectalarea/dressings every 2-3hours and report significantincreases in bloody drainage.
3. Promote comfort.
a. Assist client to side-lying or prone position,provide flotation pad when sitting.
b. Administer analgesics as ordered
4. Promote elimination: administer stool softeners asordered and, if possible, administer analgesicsbefore first post-op bowel movement.
5. Provide client teaching and discharge planningconcerning
a. Dietary modification (low-residue, soft progressto high fiber/fresh fruits, force fluids 2.5-3L/day)

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 81/104
b. Defecate when urge is felt
c. Use of stool softeners as needed untilhealing occurs.
d. Sitz baths after each bowel movement.
e. Perineal care with antiseptic solutions.
f. Recognition and reporting immediately to
physician of the following signs and symptoms:
1. Rectal bleeding
2. Continued pain on defecation
3. Puslike drainage from rectal area
HEPATIC CIRRHOSIS

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 82/104
HEPATIC CIRRHOSIS
A. ETIOLOGY AND PATHOPHYSIOLOGY
1. Irreversible fibrosis and degeneration of the liver
2. Several types of cirrhosis; Laënnec¶s (alcoholic cirrhosis,
nutritional cirrhosis) most common
3. Incidence higher in alcoholics, who are often
malnourished, and in those who have had hepatitis4. As liver failure progresses, there is increased secretion of
aldosterone, decreased absorption and utilization of the
fat-soluble vitamins (A, D, E, K), and ineffective
detoxification of protein wastes5. Hepatic coma (hepatic encephalopathy) may result from
high blood ammonia levels when the liver is unable to
convert the ammonia to urea

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 83/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 84/104
7. Surgical intervention to decrease portal

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 85/104
g phypertension: a portacaval shunt
8. Esophageal varices management
Sengstaken-Blakemore tube:
9 P id h S t k Bl k

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 86/104
9. Provide care when a Sengstaken - Blakemore
tube is in place
a. Maintain traction once the tube is passedand the gastric balloon is inflated to ensure
proper placement, elevate bed 30-45 degrees
b. Maintain the esophageal balloon at
inflated level (30-35mm Hg) up to 48 hrs
c. Deflate gastric balloon for a few minutes
at specific intervals if ordered to prevent
necrosis
d. Gastric lavage as ordered
e. Suction orally as necessary because the
client is unable to swallow saliva
10 Dietary modification:

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 87/104
10. Dietary modification:
a. Cirrhosis:
1. Protein as tolerated (80-100g); withincreasing liver damage, protein metabolism ishindered
2. High carbohydrate, moderate fat;
provides for energy; vitamin, mineral, andelectrolyte supplements
3. Low sodium (500-1000mg daily); helpscontrol increasing ascites
4. Soft foods if esophageal varices arepresent; prevents danger of rupture andbleeding
5. Alcohol contraindicated to avoidirritation and malnutrition

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 88/104
b. Hepatic coma
1. Protein: reduced according totolerance; 15-30g
2. High calorie (1500-2000g) to
prevent catabolism and liberation of nitrogen
3. Fluid carefully controlled according
to output

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 89/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 90/104
CHOLELITHIASIS /

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 91/104
CHOLELITHIASIS /
CHOLECYSTITISA. ETIOLOGY AND PATHOPHYSIOLOGY:
1. Inflammation of the gallbladder; usuallycaused by the presence of stones(cholelithiasis), which are composed of
cholesterol, bile pigments, and calcium.2. Diseased gallbladder is unable to contract in
response to fatty foods entering the duodenumbecause of obstruction by calculi or edema.
3. When the common bile duct is completelyobstructed, the bile is unable to pass into theduodenum and is absorbed into the blood.
4. Incidence is highest in obese women
in the fourth decade.

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 92/104
C. THERAPEUTIC INTERVENTIONS:

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 93/104
C. THERAPEUTIC INTERVENTIONS:
1.Medical management
- Nasogastric suctioning to reduce nauseaand eliminate vomiting
- Narcotics to decrease pain
- Antispasmodics and anticholinergics toreduce spasms and contractions of the
gallbladder
- Antibiotic therapy if infection issuspected
- NURSING CARE:

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 94/104
NURSING CARE:
-Teach dietary modification to achieve a low-fat
intake because reduced bile flow will reduce fatabsorption; supplementation with water-miscible
forms of vitamins A and E may be prescribed.
-Relieve pain both preoperatively and
postoperativelyObserve for signs of bleeding (vitamin K is fat
soluble and is not absorbed in the absence of
bile); administer vitamin K preparations as
ordered
Provide care following a cholecystectomy:
surgical / laparoscopic laser
a. Monitor nasogastric tube attached to suction to
di i

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 95/104
prevent distention
1. Maintain patency of the tube
2. Assess and measure drainage
b. Provide fluids and electrolytes via intravenous
route
c. Keep the client in a low-Fowler¶s positiond. Have the client cough and deep breathe; splint the
incision (incision is high and midline, making
coughing extremely uncomfortable)
e. Provide care for the client with a T-tube (if thecommon bile duct has been explored, a T-tube is
inserted to maintain patency)
TREATMENT OF STONES:
CHOLESTEROL DISSOLVENT

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 96/104
� CHOLESTEROL DISSOLVENT:
Moctanin is administered through a nasal
biliary catheter to dissolve stones left in the bileduct after cholecystectomy. Dissolution maytake 1 to 3 weeks. Observe the client foranorexia, nausea, vomiting, and abdominalpain.
ORAL BILE ACIDS:
Chenodiol ( chenix ) and ursodiol ( actigall )are administered to dissolve small stones. Side
effects include diarrhea ( especially withchenodiol ), elevation of hepaticenzymes,gastritis, and gastric ulcers.Dissolution takes between 6 months and 2years, and the success rate is only about 30 %
Extracorporeal shockwave lithotripsy
E d i hi t t / t d h l i

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 97/104
Endoscopic sphincterotomy/retrograde cholangio-pancreatography
Percutaneous transhepatic dissolutionNasal biliary dissolution

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 98/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 99/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 100/104
6 Duodenal ulcer

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 101/104
6.Duodenal ulcer
7. Hyperlipidemia
ASSESSMENT FINDINGS:a. Abrupt onset of pain in the epigastric / LUQ area
that radiates to the shoulder, substernal area,
back, and flank
b. Abdominal tenderness and distention
c. Aching, burning, stabbing, pressing pain
d. Knee-chest position, fetal position, or leaning
forward for comfort d/t abdominal paine. Mental confusion, hypocalcemia ± mm irritability
f. Nausea and vomiting

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 102/104
g. Tachycardia, shock, hypotension
h. Dyspnea
i. Low grade fever
j. Elevated serum amylase / lipase / glucose
k. Grey Turner¶s, Cullens¶s sign
l. Chronic steatorrhea
m. Jaundiceo. Hyperglycemia

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 103/104

8/6/2019 7. Gastrointestinal
http://slidepdf.com/reader/full/7-gastrointestinal 104/104
9. Keep the client in semi-Fowler¶s position (if
his blood pressure allows) to promote
comfort and lung expansion.
11. Keep the client in bed and turn him every
2hrs, or utilize a specialty rotation bed to
prevent pressure ulcers.12. Provide a quiet, restful environment to
conserve energy and decrease metabolic
demands.