Embed Size (px)
Citation preview

sompid/immunopath50
686-392 General Pathology“Immunopathology”
Dr. Sompid Kintarak D.D.S., Ph.D.Department of StomatologyFaculty of Dentistry, PSU

sompid/immunopath50
Content
• Immune cells• Cytokines• Major histocompatibility complex• Hypersensitivity reactions• Graft rejection• Immune tolerance• Autoimmune diseases• Amyloidosis

sompid/immunopath50
Immune system
• Innate immunity• Adaptive immunity
• Humoral immunity• Cellular immunity

sompid/immunopath50
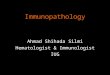
Blood cells
1
2
34
5
1 Neutrophil
2 Lymphocyte
3 Monocyte
4 Eosinophil
5 Basophil

sompid/immunopath50
T-lymphocyte• 60-70% of lymphocytes in
peripheral blood• TCR:CD3 complex• CD28 (binds costimulatory
molecules CD80 or CD86 on APC)
• CD4+ cell (MHC II)– Th1: IL-2, IFN- γ (cell-mediated
immunity)– Th2: IL-4, IL-5, IL-13 (B-cell
activation)
• CD8+ cell (MHC I)• CD4:CD8 ~ 2:1

sompid/immunopath50
CD40L:CD40
B-lymphocyte• 10-20% of lymphocytes in
peripheral blood• CD19, CD20• MHC II, FcR, CD21
(receptor for complement, EBV)
• Differentiation to plasma cell and produce IgG, IgA, IgE (requires help from CD4+ T-cell)

sompid/immunopath50

sompid/immunopath50
Macrophage
• Antigen-presenting cell
• MHC class II• Secrete IL-1, TNF-α
Dendritic cell

sompid/immunopath50
Natural killer cell • 10-15% of lymphocytes in
peripheral blood• TCR-, CD3-• Innate immune system• Destroy virus, some
tumor cells• CD16, CD56
– CD16 is FcR for IgG(ADCC)
• Produce IFN-γ (recruit T lymphocytes)

sompid/immunopath50
Immune response
CD40:CD40L

sompid/immunopath50
Cytokines• Mediate innate immunity: IL-1, TNF-α, IL-6, type 1 IFN • Regulate lymphocyte proliferation and differentiation:
IL-2, IL-4, IL-5, IL-12, IL-15IL-10, TGF-ß down regulate immune response
• Activate inflammatory cells (mostly produced from T cells): IFN-γ, TNF-α, TNF-ß, migration inhibition factor
• Affect leukocyte movements (chemotaxis): IL-8, eotaxin, macrophage inflammatory protein-1α
• Stimulate hematopoiesis: colony-stimulating factors, IL-3, IL-7 (affect growth of lymphocyte progenitor cells)

sompid/immunopath50
Major Histocompatibility Complex
• MHC class I: HLA-A, HLA-B, HLA-C– Presence on all nucleated cells and platelets
• MHC class II: HLA-DP, HLA-DQ, HLA-DR– Presence on APC, B cell
• MHC class III: C2, C3, Bf

sompid/immunopath50
Major Histocompatibility Complex
• Organ transplantation• Induction of immune response• Regulation of immune response• Disease association
– HLA-B27 – ankylosing spondylitis– HLA-DR4 – rheumatoid arthritis– HLA-B12, B51, Cw7 – recurrence aphthous stomatitis– HLA-B5, B12, B27 – Behçet’s syndrome

sompid/immunopath50
Immediate (Type I) hypersensitivity

sompid/immunopath50
Arachidonic acid metabolites
Aspirin, indomethacininhibit
Arachidonic acid
Phospholipases x Steroids inhibitCell membrane phospholipids
Cyclooxygenase x
Vasodilation, Potentiate edema
(causes vasoconstriction, promotes plt aggregation)
(cause vasodilation, inhibits plt aggregation)
Prostaglandin G2
Prostaglandin H2
Prostacyclin, PGI2 Thromboxane A2 ,TXA2
PGD2 , PGE2 , PGF2α
5-Lipoxygenase
5-HPETE
Leukotriene A4,LTA4
LTC4
LTD4
LTE4
Vasoconstriction BronchospasmIncreased permeability
LTB4
(chemotaxis)
5-HETE 12-Lipoxygenase
Lipoxin A4 Lipoxin B4
Vasodilation Inhibit neutrophil chemotaxisStimulate monocyte adhesion

sompid/immunopath50
Acute laryngeal edema caused by anaphylactic reaction to penicillin

sompid/immunopath50
Antibody-mediated (Type II) hypersensitivity

sompid/immunopath50
Complement activationAntigen-antibody (IgG or IgM)
complex
C1 Activated C1C4+C2
Classic pathway C3 convertase
Classic pathway C5 convertase
CLASSIC PATHWAY
ALTERNATIVE PATHWAY
C4b2a C4b2a3b
C3C3a
C5
C3 C3b C3bBb C3bBb3b
C5a
Microbial surfaces Polysaccharides Factor B
Factor DAlternative pathway
C3 convertasestabilized by
properdin
C5b C5-9C6 C7 C8 C9
Also generated via plasminor lysosomal proteases
Alternative pathway C5 convertase
C3b
C1 Activated C1
Mannose binding lectin

sompid/immunopath50
The membrane attack complex:
RBC
Intact E. coli After incubation with complement

sompid/immunopath50
Antibody-mediated (Type II) hypersensitivity

sompid/immunopath50
Goodpasture’s syndrome: this is the even linear pattern of immunofluorescence with antibody to IgG (autoantibody) which is directed against the entire glomerular basement membrane (linear pattern).
From: www-medlib.med.utah.edu/WebPath/ From: Robbins and Cotran Pathologic basis of disease. 7th ed.

sompid/immunopath50
Immune complex-mediated (Type III) hypersensitivity

sompid/immunopath50
Hageman factor (XII)Plasmin, Kallikrein Collagen, basement membrane, activated plt
Prekallikerein activator (XIIa)
Vasodilation, Pain Vasc. Permeability
Fibrin split products
Prekallikrein
Kallikrein
Kininogen
KininFibrinopeptidesFibrinogen Fibrin +
Plasminogen Plasmin
XI XIa
Prothrombin Thrombin (IIa)
X Xa Acute inflammation
Vasc. Permeability, Chemotactic
PARs
C3 C3a

sompid/immunopath50
Immune complex vasculitis
Vasculitis with fibrinoid necrosis

sompid/immunopath50
Cell-mediated (Type IV) hypersensitivity• Delayed type hypersensitivity
– Granulomatous inflammation– Type I DM, multiple sclerosis– Contact dermatitis

sompid/immunopath50
Delayed hypersensitivity in the skin
• Perivascularinfiltration by T cells and mononuclear phagocytes
• Anti-CD4 antibodies

sompid/immunopath50
Formation of granuloma in cell-mediated (type IV) hypersensitivity
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
Contact dermatitis: pre-sensitized lymphocytes led to this inflammatory reaction a couple of days after contact with the offending plant material (poison oak and poison ivy).
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
Graft rejection

sompid/immunopath50
Hyperacute rejection of renal allograft: Preformed antibodies in the recipient's blood have attacked the endothelium in this transplanted kidney, leading to thrombosis with consequent widespread infarction of the renal cortex (note the characteristic pale appearance). The renal pelvis shows hemorrhagic infarction.
From: Robbins and Cotran Pathologic basis of disease. 7th ed.

sompid/immunopath50
Acute rejection of renal allograft: The cortex is thickened and pale tan due to an intense infiltrate of predominantly mononuclear cells. Compare with the previous image. The mononuclear inflammatory infiltrate on the right of the image represents acute cellular rejection. The thrombosed vessel and consequent infarction with typical coagulative necrosis are manifestations of acute humoral rejection.
From: Robbins and Cotran Pathologic basis of disease. 7th ed.

sompid/immunopath50
Chronic rejection of renal allograft: The kidney is shrunken with a greyish irregular surface, indicating scarring. This is due predominantly to chronic vascular injury, resulting in atrophy and fibrosis of the renal parenchyma.
From: Robbins and Cotran Pathologic basis of disease. 7th ed.

sompid/immunopath50
Acute vascular rejection in heart transplant. The inflammatory reaction consists mostly of lymphocytes and is seen manly around small arteries, a vasculitis.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
By immunofluorescence, antibody to IgG is seen highlighting the vascular walls in this heart with acute vascular rejection.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
Chronic vascular rejection in renal transplant: a renal biopsy shows marked interstitial fibrosis.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
The renal arteries with chronic vascular rejection are markedly thickened and fibrotic.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
Acute cellular rejection in heart transplant: T-lymphocytes are identified by immunoperoxidase staining with antibody to CD3.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
GVHD: Besides the icterus in this skin there is a fine scaling rash in this patient following bone marrow transplantation with a 5 out of 6 antigen match. An example of GHVD in which donor lymphocytes attack host tissues.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
GVHD: There is vacuolization and dissolution of epidermal cells along the basal layer, along with lymphocytes. At the arrow is a rounded pink apoptotic body.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
GVHD: marked cholestasis in the liver, seen here as large collections of yellow-green bile pigment in the bile canaliculi.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
GVHD: there are yellow-brown collections of bile in the canaliculi, as well as chronic inflammatory cells within the liver parenchyma.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
Autoimmune disease
From: Robbins and Cotran Pathologic basis of disease. 7th ed.

sompid/immunopath50

sompid/immunopath50
Mechanisms of autoimmune diseases

sompid/immunopath50
Systemic lupus erythematosus (SLE)
• Causes: unknown– Genetic predisposition– Exogenous factors: drug (procainamide, hydralazine,
isoniazid, D-penicillamine), UV, hormone (estrogen)• Failure to maintain self tolerance with activation
of B cell• Tissue damage caused by immune complex
(type 3 hypersensitivity) and antibody-mediated injury (type 2 hypersensitivity)

sompid/immunopath50
SLE: malar/butterfly rash over the face, the rashes are made worse by sun exposure.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
LE cell test: the pink blobs are denatured nuclei (here are two). One is seen being phagocytozed in the center by a PMN. This test is not nearly as sensitive as the ANA which has supplanted the LE cell test. Therefore, NEVER order an LE cell test.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
ANA test: homogenous or diffuse, rim or peripheral, speckled, and nucleolar pattern.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
ANA test: double stranded DNA. These little Crithidiaorganisms have a small kinetoplast between the nucleus and the flagella which glows bright green under immuno-fluorescence microscopy, and is indicative of anti-native DNA antibody that is very specific for SLE.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
Skin biopsy: the region of rash reveals liquefactive necrosis of the basal layer at the dermal-epidermal junction along with dermal chronic inflammatory cell infiltrates (often perivascular) and extravasation of red blood cells (purpura) leading to the visible rash.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
Skin biopsy: the region of rash reveals liquefactivenecrosis of the basal layer at the dermal-epidermal junction along with edema.
Immunofluorescence: IgGdeposits along the dermal-epidermal junction.

sompid/immunopath50
Immunofluorescence of skin with antibody to IgG shows a band-like deposition of immune complexes that is bright green at the dermal epidermal junction in this skin biopsy taken from an area with a visible rash. With SLE such deposition can be found in skin uninvolved by a rash, whereas with DLE the immune complexes are found only in involved skin.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
SLE: Vasculitis with chronic inflammatory cells
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
SLE: shown here is Libman Sacks endocarditis in which there are many flat, reddish-tan vegetations spreading over the mitral valve and chordae.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
Lupus nephritis in SLE: a glomerulus with thickened pink capillary loops, the so-called “wire loops”. The surrounding renal tubules are unremarkable.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
A granular pattern of immunofluorescence in the glomerulus with antibody to IgG, indicative of deposition of immune complexes in the basement membranes of the glomerular capillary loops (lumpy-bumpy pattern).
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
Granular pattern of immunofluorescence in the glomeruluswith antibody to C1q complement, which is more specific for SLE
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
SLE: the thickened basement membrane (arrow) that results from immune complex deposition in the glomerularcapillary loop is prominent in this electron micrograph
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
Rheumatoid arthritis• Autoimmune disease• A chronic systemic inflammatory disorder that may affect
many tissues and organs, but principally attacks the joints, producing a nonsupurative proliferative and inflammatory synovitis that often progresses to destruction of the articular cartilage and ankylosis of the joints.

sompid/immunopath50
Immunopathogenesis of rheumatoid arthritis

sompid/immunopath50
• Associated with MHC Class II• HLA-DR4 (risk 4-6 times)• Rheumatoid factor (RF) – most IgM• Autoantibody to Fc portion of IgG• Positive 60-90% of RA, SLE, SS

sompid/immunopath50
Rheumatoid arthritis

sompid/immunopath50
Sjögren syndrome• Dry eyes and dry mouth
resulting from immune mediated lacrimal and salivary gland destruction (lymphocytic infiltration and fibrosis)
• 40% occur in isolation (primary form)
• 60% occur in association with other autoimmune diseases (secondary form)

sompid/immunopath50
Sjögren syndrome
• 75% of patients have RF• 50-80% of patients have ANAs
– Ribonucleoprotein antigens: SS-A and SS-B • HLA-B8, HLA-DR3, DRW52 related with primary
SS• Commonly in older women, ages 50-60 y• 40 times risk of developing lymphoid
malignancies esp. NHL (marginal zone lymphoma)

sompid/immunopath50
Sjögren syndrome: the mononuclear inflammatory infiltrates, interstitial fibrosis, and acinar atrophy of a minor salivary gland in a biopsy of lip is typical for long-standing Sjögren syndrome.
From: Neville Damm Allen Bouquot. Oral & Maxillofacial Pathology, 2nd ed.

sompid/immunopath50
Systemic sclerosis
• Abnormal accumulation of fibrous tissue in the skin and multiple organs
• Excessive fibrosis triggered from abnormal immune responses and vascular damage
• Diffuse vs Limited scleroderma• CREST syndrome (calcinosis, Raynaud
phenomenon, esophageal dysmotility, sclerodactyly, telangiectasia)– Anticentromere antibody

sompid/immunopath50

sompid/immunopath50
A patient demonstrating the taut and shiny skin typical of sclerodactyly. The skin becomes inelastic and it is hard to move the fingers.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
A higher magnification of the taut, shiny, inelastic skin with sclerodactyly. Note also the cheilosis at the corners of the mouth from riboflavin deficiency as a result of the malabsorption that can occur with scleroderma.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
A, Normal skin. B, Skin biopsy from a patient with systemic sclerosis. Note the extensive deposition of dense collagen in the dermis with virtual absence of appendages (e.g. hair follicles) and foci of inflammation (arrow).

sompid/immunopath50
At low magnification, the collagen of the dermis is increased. Chronic inflammatory cells are sparse with systemic sclerosis, unlike SLE.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
At high magnification, the dermis is expanded by dense collagenous fibrosis in a patient with systemic sclerosis. Immunofluorescence is not helpful with scleroderma.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
This trichrome stain of the stomach demonstrates intense blue staining in the submucosa from the collagen deposition. Such fibrosis can occur anywhere in the GI tract, but is most common in the lower esophagus, leading to the esophageal dysmotilitywith systemic sclerosis.
Epithelium
Muscle
Fibrosis
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
Renal disease suggests diffuse scleroderma in this patient with hyperplastic arteriolosclerosis and malignant hypertension (blood pressure 300/150 mm Hg)
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
Immunologic deficiency syndrome
• Primary immunodeficiencies– genetic

sompid/immunopath50
Immunologic deficiency syndrome
• Secondary immunodeficiencies – arise as complications of infections; malnutrition; aging; or side effects of immunosuppression, irradiation, or chemotherapy for cancer and other autoimmune diseases

sompid/immunopath50
Amyloidosis
• Primary amyloidosis – association with some immunocyte dyscrasia, multiple myeloma
• Secondary amyloidosis – occurs as a complication of an underlying chronic inflammatory or tissue destructive process
• Hereditary or familial amyloidosis

sompid/immunopath50
Amyloidosis is characterized by slow deposition over years of increasing amounts of an amorphous proteinaceousmaterial in one or more tissues. Seen here in the heart between the darker red myofibers are pale pink amyloiddeposits.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
With conge red stain and observed under polarized light, the amyloid has a characteristic “apple green’ birefringence as seen here in a deposit around an artery in the heart.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
By electron micrograph, amyloid is composed of a “beta-pleated sheet” of fibrils, seen here as irregular grey material. When the amyloid protein is made up of immunoglobulin light chains, then it is “AL amyloid” and when it is derived from serum amyloid-associated protein, then it is “AA amylod.” in terms of the effect upon the organs, “amyloid is amyloid”.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
This is the immunofluorescent appearance of the myocardium with antibody to lambda light chain. Thus, this is “AL amyloid”.
From: www-medlib.med.utah.edu/WebPath.html

sompid/immunopath50
References• Abbas AK, Chapter 6: Diseases of immunity. In: Kumar V, Abbas
AK, Fausto N (eds). Robbins and Cotran pathologic basis of disease. 7th ed. Philadelphia: WB Saunders Co. 2005. p. 193-267. and p. 1305-1309.
• Kumar V, Cotran RS, Robbins SL (eds). Basic pathology. 6th ed. Philadelphia: WB Saunders Co. 1997. p. 81-131.
• Peakman M, Vergani D (eds). Basic and clinical immunology. New York: Churchill Livingstone. 1997.
• Cotran RS, Kumar V, Robbins SL (eds). Robbins pathologic basis of disease. 5th ed. Philadelphia: WB Saunders Co. 1994. p. 171-240.
• www-medlib.med.utah.edu/WebPath/ TUTORIAL/TUTORIAL.html

sompid/immunopath50