-
8/8/2019 665 Fridman Blood
1/6
-
8/8/2019 665 Fridman Blood
2/6
This plasma technology can find many applications in the medical
field. Within thehospital setting, this technology may prove useful
in the operating room for patientssuffering from bleeding not
amenable to other methods of coagulation. Because of thepotential
for simultaneous sterilization, our device could also help prevent
intra-
operative infections. Sterilization effects of non-thermal
plasma are well-known [10-13] and were confirmed, for example, in
our research with NASA Jet Propulsion Lab[14]. In the future, we
intend to develop a significantly smaller version of our
powersupply to create a portable, possibly battery-operated blood
coagulator and woundsterilizer (Fig. 4). In addition, due to its
ability to promote coagulation, the non-thermal plasma discharge
device can be used for hemophiliac patients who haveclotting
difficulties or those who are on anti-coagulants.
2. Experimental Setup
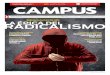
Schematics of our experimental setup of the varying and fixed
(Fig. 4) frequency,voltage, and power Floating Electrode DBD setups
are presented. Power of bothsystems is approximately 1 W/cm 2 and
the treatment surface varies from less than
1cm 2 to 10cm 2 depending on the attached electrode (Fig. 6).
Utilizing the variable frequency, voltage, and powersetup we are
able to tune the setup for treatment dose appropriate for a
specific application. I.e. for tissuesterilization we might want
lower power with longer treatment time; while for blood coagulation
we might wanthigh power with low treatment time to stop gushers
large flow of blood; or lower power to coagulate bloodin small
cuts.
Fig. 4. Floating Electrode DBD schematic.
We started a fundamental study of mechanism of blood coagulation
with the help of electrical discharge plasma.Fig. 5 presents our
setup for treatment of small blood volumes 500l. While not wasting
too much blood pertest, this volume is a minimum required for
standardized hematological tests we perform at the Drexel
UniversityHahnemann Hospital hematology lab: PT (Prothrombin time),
aPTT (activated partial thromboplastin time), andSTA-Thrombin
(Diagnostica Stago proprietary Thrombin formation time test). In
this setup we are able toprecisely control the distance of Floating
Electrode DBD to the treated blood sample for the purpose of
Fig. 3. Quartz-coatedTreatment Electrode
-
8/8/2019 665 Fridman Blood
3/6
determining correct dose required for clot formation and to get
reproducible results necessary for thefundamental study.
Fig. 5. Blood treatment experimental setup schematic.
Schematic representations of the three treatment electrode types
used for this research are shown in Fig. 6.
Round electrode is used for treatment of small areas and when
distance between electrode and the treatedsurface is closely
monitored (0.1mm). Wand electrode is used in hand-held operation
where distance andtreated area are not precisely monitored. Roller
is used for treatment of large flat areas.
Fig. 6. Treatment electrodes. Top: 3D models; bottom: schematic
representations;left to right: round, wand, roller.
During treatment, tissue samples are placed directly on a
grounded stainless steel plate. Blood samples aredispensed into 0.1
or 0.5 ml grounded stainless steel, aluminum, brass, or titanium
containers (Fig. 5). For bloodtreatment we found titanium to be the
best material where control blood sample coagulates the
slowest.
3. Safety considerations
-
8/8/2019 665 Fridman Blood
4/6
Safety of Floating Electrode DBD plasma electrode for humans
needs to be considered for application in woundhealing. Here we
consider a simplified electric scheme to estimate conditions
required for electrical safety. Oncehuman approaches Floating
Electrode, plasma ignites and at that point we can consider DBD
plasma as capacitorand resistor in series and human as a resistor
andcapacitor in series (Fig. 7).
Total plasma resistance can then be estimated as a sum of
capacitive and active resistances:
( )2
21
p p p
p p p
i R R
C
R RC
= +
= +
Where p R
is total plasma resistance, pC is plasma
capacitance, p R is plasma active resistance, and is the
signal frequency. Similarly, total resistance of a human can be
estimated as:
( )2
21h h
h
R RC
= +
Where h R
is total resistance of a human, hC is human capacitance, and h R
is active resistance of a human. Forthe Floating Electrode DBD
plasma device to be safe, total plasma resistance needs to be
greater than totalresistance of a human:
( ) ( )2 2
2 21 1 p h
p h
R R
C C
+ >> +
Active resistance of a human is ~1 MOhm [15-17]and human
capacitance is ~50 pF (though it rangesfrom 20 pF to 90 pF,
depending on the surfacehuman is standing on, thickness of his/her
soles,and distance to nearest grounded object) [15,17].For our
frequency range, Floating Electrode DBDplasma active resistance can
be estimated to 5 to 10MOhm and its capacitance to ~50pF [18,19].
Thusat the operating frequency of 12 kHz we see thattotal
resistance of a human (1.9 MOhm) is far
smaller than total plasma resistance (5.3 MOhm), assuming hC =50
pF, h R =1 MOhm, pC =50 pF, p R =5MOhm. Even in the case where
human total resistance will increase for some reason, total current
passingthrough the human will be very low because of a massive
total resistance of the system. From this estimation wecan conclude
that even in the worst case where resistance of a human is
approaching that of plasma, the overallsystem will still be
completely safe from the electrical standpoint (Fig. 8).
4. Results
In our tests we have successfully accomplished the
following:
Fig. 7. Plasma/human interface principal schematic.
Fig. 8. Floating Electrode DBD: safe to touch.
-
8/8/2019 665 Fridman Blood
5/6
Designed and built a Dielectric Barrier Discharge (DBD) system
capable of delivering 1 W/cm 2 of plasmapower at operating
frequencies of 10-30 KHz. While the system employs a power supply
delivering voltage of up to 10 KV, it is perfectly safe as the high
frequency plasma current is limited to below a milli-ampere.
Developed treatment electrodes (Fig. 3-6) for treatment of blood
and tissue samples. Performed blood coagulation tests on blood from
cadaver organs (Fig. 9). The results consistently show faster
coagulation when exposed to DBD plasma: for example, blood
treated for 15 seconds completely coagulates in2 minutes while
untreated sample coagulates in 13 minutes.
Performed blood coagulation tests on cadaver organs with
subsequent gross and microscopic evaluation of tissue to test for
damage. Our analysis demonstrates blood clotting within 15 seconds
without gross ormicroscopic evidence of tissue damage (Fig.
10,11).
Performed skin sterilization tests on cadaver skin with
subsequent microbiologic culture. The resultsdemonstrate complete
sterilization of skin flora after 6 seconds of treatment by the
plasma.
Examined skin histology to find existence and/or extent of
microscopic damage. No tissue damage was foundafter as much as 5
minutes of plasma treatment (Fig. 11).
Fig. 9. Plasma-assisted blood coagulation with
15-secondtreatment (left) and 1-minute treatment (right);control
drop on the bottom, treated drop on top.
Fig. 10. 1-minute plasma treatment shows no visible
tissuedamage. Left: before treatment; right: after treatment.
Fig. 11. Skin histology (left to right): control, 1 minute, and
5 minute treatment times show no detectable tissue damage.
5. Conclusion
This device can find many applications in the medical field,
ranging from replacing high-power, high-temperature thermal plasma
coagulators in the operating rooms to personal portable wound
sterilizing andhealing instruments. The scope of the presented
research included only initial studies of plasma influence onblood
coagulation and simultaneous tissue sterilization. However, these
studies are essential in providing us withknowledge and expertise
on the underlying processes.
At the present, we are actively working on developing a kinetic
model of DBD plasma influence on Bloodplasma coagulation cascade as
well as DBD plasma role in the tissue sterilization process. We
have interestingmodeling results (that agree with experimental
evidence) involving DBD plasma influence on Calcium ion
-
8/8/2019 665 Fridman Blood
6/6
concentration and in turn on blood coagulation cascade. These
results will be presented at the ISPC-17conference.
Bibliography
[1] Hydrogen peroxide as a topical hemostatic agent, Clin Ortop.
1984 Jun; (186):244-8. Hankin FM,Campbell SE, Goldstein SA,
Matthews LS.
[2] Clinical usefulness of 3% hydrogen peroxide in acute upper
GI bleeding: a pilot study. GastrointestEndos. 1999 Apr; 49(4 Pt
l):518-21. Kalloo AN, Canto MI, Wadwa KS, Smith CL, Gislason GT,
Okolo PI3rd, Pasricha PJ.
[3] Hydrogen peroxide is involved in collagen- induced platelet
activation. Blood.I998 Jan 15;91(2):484-90. Pignatelli P,
Pulcinelli FM, Lenti L, Gazzangia PP, Violi F.
[4] Role of hydroxyl radicals in the activation of human
platelets. Eur J Biochem. 1994 Apr l5; 221(2):695-704. Iuliano L,
Pederson JZ, Pratico D, Rotilio G, Violi F.
[5] H 2O2 activity on platelet adhesion to fibrinogen and
protein tyrosinephosphorylation. Biochim BiophysActa. 2000 Feb 2;
1495(2): 1 83-93.
[6] Free radicals contribute to platelet aggregation and cyclic
flow variations in stenosed and endothelium-injured canine
arteries. J Am Coil Cardiol. l994 Dec; 24(7):1749-56.
[7] A plasma scalpel: comparison of tissue damage and wound
healing with electrosurgical and steelscalpels. Archives of Surgery
Vol 11 l No 4, Apr 1976. W.J. Link, F.P. Incropera, J.L.
Glover.
[8] The plasma scalpel: a new thermal knife. Lasers Surg Med.
1982; 2(1):I01-6. Glover JL, Bendick PJ,Link WJ, Plunkett RJ.
[9] Evaluation of the plasma scalpel for intracranial surgery: a
pilot study. Surg Neurol. I 979 Sep;12(3):247-50. Payne NS, Tindall
GT, Fleischer AS, Mirra SS.
[10] Biological decontamination by non-thermal plasmas. IEEE
Trans. Plasma. Sci., Vol. 28, No. 1, pp. 184-188, 2000. M.
Laroussi, I. Alexeff, W. Kang.
[11] A Remote Exposure Reactor (RER) for plasma processing and
sterilization by plasma active species atone atmosphere. IEEE
Trans. Plasma Sci., Vol. 28, No. 1, Feb 2000. J.R. Roth, D.M.
Sherman, R.B.Gadri, F. Karakaya, Z. Chen, T.C. Montie, K.
Kelly-Wintenberg, P.P.-Y. Tsai.
[12] Use of one atmosphere uniform glow discharge plasma to kill
a broad spectrum on microorganisms. J.Vac. Sci. Technol. A., Vol.
17, No. 4, Jul/Aug 1999. K. Kelly-Wintenberg, A. Hodge, T.C.
Montie, L.
Deleanu, D. Sherman, J.R. Roth.[13] Demonstration of a Hermetic
Airborne Ozone Disinfection System: Studies on E. coli. AIHA J 64
no2
Mr/Ap 2003. W.J. Kowalski, W.P. Bahnfleth, B.A. Striebig, T.S.
Whittam.[14] Final Technical Report - NASA Contract NAS3-01068 Use
of Non Thermal Plasma for Sterilization of
Material Handling Devices[15] MARBLE, A. E., MACDONALD, A. C.,
MCVICAR, D., and ROBERTS, A., 1977, Phys. Med. Biol., 22,
365.[16] "Bioelectrical impedance measurements in patients with
gastrointestinal disease: validation of the
spectrum approach and a comparison of different methods for
screening for nutritional depletion",Petronella LM Cox-Reijven,
Bernard van Kreel and Peter B Soeters, American Journal of
ClinicalNutrition, Vol. 78, No. 6, 1111-1119, December 2003
[17] "Fusion Pore Conductance: Experimental Approaches and
Theoretical Algorithms", Vladimir Ratinov, Ilya
Plonsky, and Joshua Zimmerberg, Biophys J, May 1998, p.
2374-2387, Vol. 74, No. 5[18] Electrical Characterization of a
Corona Discharge for Surface Treatment, LA Rosenthal, DA Davis,
IEEE Trans. on Ind. Apps., Vol. IA-11, No. 3, May/June 1975.[19]
Microdischarge behaviour in the silent discharge of nitrogen-oxygen
and water-air mixtures, Z
Falkenstein, JJ Coogan, J. Phys. D: Appl. Phys., 30 (1997)
817-825.