Embed Size (px)
Citation preview

COPYRIGHT © 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING
OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-OUT WRITTEN PERMISSION FROM THE PUBLISHER.
71
AAlingually inclined maxillary incisor presents a com-mon problem for the orthodontist, in both treated
and untreated cases. In untreated cases, linguallyinclined incisors are generally combined with maxil-lary crowding, deep bite, and gingival impingement. Inboth treated and untreated cases, the upright incisorsmay lead to TMJ symptoms since mandibular move-ments are restrained and anterior disc displacementand/or compression of the joint may be present.1
These patients are generally classified as a Class II,Division 2, but lingually inclined maxillary incisorsmay be present in both skeletal Class II and Class Ipatients; in the latter, the mandibular incisors willalso be upright and crowded.
The correction of lingually inclined incisors is closelydependent upon the developmental stage of the pa-tient. In the child, the easiest correction is performedthrough simple proclination of the incisors. This will, onthe other hand, lead to an increase in the overjet that,in the case of a growing individual, can be corrected bystimulation of the forward growth of the mandible.
Correction of lingually inclined maxillary incisors inadult patients is often more problematic. Sagittalexpansion can be allowed only if a Class I relation-ship prevails in the buccal segments and the uprightincisors are combined with the presence of crowdingin both arches. In cases where sagittal expansion isundesirable for various reasons, the correction of theincisor inclination can be obtained only through lin-gual movement of the incisor roots. To obtain thistooth movement, the requirements of the necessaryforce system cannot be met with a continuous arch,since the direction of the needed force has to belocalized apically to the center of resistance of theanterior teeth. In these patients, the lingually inclinedincisors constitute a serious problem that is oftensolved by orthognathic surgery.
Patients who have already received orthodontictreatment and still present with upright incisors arefrequently extraction cases that have been finishedwithout sufficient lingual root torque during spaceclosure. These patients may suffer from symptomsrelated to a posteriorly forced mandible, and theretroclined incisors will frequently interfere with theestablishment of a perfect intercuspation of the buc-cal segments.
The aim of this article is to discuss the correctionof lingually inclined incisors in various categories ofpatients and to demonstrate how the use of a com-puter can facilitate the mechanical design for thesecorrections. In addition, the efficiency of properlydesigned mechanics is demonstrated by review ofthe treatment records of 9 cases.
Lingually Inclined IncisorsLingually Inclined IncisorsBirte Melsen, DDS, DO, PhD1/Giorgio Fiorelli, DDS2
Aim: To survey the different possibilities available for the correction of lingually inclinedincisors. Material and Methods: The use of computers for the definition of the correct forcesystem has been developed and the results are demonstrated. A computer program, basedon vectorial calculations, is useful in the appliance design. Discussion: The necessity for dif-ferentiated diagnosis and definition of the treatment goal is underlined. Conclusions: Theefficiency of these force-based appliances is illustrated in case reports. World J Orthod;2000;1:71–78.
1 Professor, Department of Orthodontics, Royal Dental College,Aarhus University, Aarhus, Denmark.
2 Clinical Assistant Professor, Orthodontic Department, Universityof Siena, Siena, Italy.
REPRINT REQUESTS/CORRESPONDENCE
Prof Birte Melsen, Department of Orthodontics, Royal Dental Col-lege, Aarhus University, Vennelyst Boulevard, DK-8000 Aarhus C,Denmark. Tel: +45 89 42 40 00. Fax: +45 86 19 60 29. E-mail:[email protected]

COPYRIGHT © 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING
OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-OUT WRITTEN PERMISSION FROM THE PUBLISHER.
72
Melsen/Fiorelli WORLD JOURNAL OF ORTHODONTICS
THEORETICAL BACKGROUNDTHEORETICAL BACKGROUND
Any well-defined tooth movement can only beachieved with 1 particular force system, which can bedefined by the line of action of the force in relation tothe center of resistance of the tooth to be displaced.The desirable movement in patients with linguallyinclined incisors is often a combination of a changein incisor inclination and a displacement in anotherplane of space. The necessary force system will thenbe defined according to the desired combination.
Some of these displacements are consideredeasy, eg, the proclination of incisors as often under-taken during pretreatment for functional appliancewear. Other displacement combinations, such asintrusion and lingual root movement, are consideredcomplicated movements. Given a valid estimate ofthe localization of the center of resistance, the nec-essary force can be defined mathematically and,therefore, also by means of a computer. Softwarethat would define the necessary force, with respectto the estimated center of resistance, for any specificdental movement has been developed.2 Once thedesired tooth movement is indicated, this softwaredescribes the force resultant by drawing a vector oneither the head film or the cephalometric tracing (Fig1). The clinician can then determine whether theforce’s line of action is directly accessible or whethera replacement system has to be generated.3 The lat-ter can be done either through a combination of 2cantilevers or by the insertion of a loop designed forthis purpose. This computer program can also beuseful when designing statically determinate appli-ances comprising 2 cantilevers.4 The appliancedesign is based on vectorial calculations, resulting inits correct configuration. The activation of the can-tilevers can, given the alloy and the length of the can-tilever, be calculated by software designed specifi-cally for this purpose.
THE DIFFERENT COMBINATHE DIFFERENT COMBINATIONSTIONSOF TOOTH MOVEMENTSOF TOOTH MOVEMENTS
The change in inclination necessary for the correc-tion of lingually inclined incisors can be obtained invarious ways, and can be roughly classified accord-ing to the schematically produced drawing (Fig 1),which will be discussed below.
Pure rotation around CR
This kind of movement (see Figs 1e, 3, and 4) takesplaces only if a couple is applied to the teeth. In case
of a pure change in inclination, the center of rotationwill coincide with the center of resistance of theincisors. A suitable appliance for the production of apure couple would be a centered V-bend5,6 or a torquearch composed of stainless steel and superelasticwires.7 The clinical result of a pure couple would beanterior displacement of the crown and lingual dis-placement of the root. The prerequisite of such amovement would, however, be the total absence offriction and the equal resistance to movement of theanterior and the posterior unit. This would maintainthe force system identical to a pure couple. As this israrely the case, it is crucial to carefully monitor themovement. An alternative appliance delivering thesame force system, but independent of friction, wouldbe to apply 2 cantilevers (Fig 2). One of the 2 can-tilevers is represented by a torque arch, inserted in theanterior tooth slots and ligated to the posterior unitwith a single point of contact. The torque arch deliversboth a moment and an extrusive force to the anteriorteeth. To neutralize the vertical extrusive force, a sec-ond cantilever should be applied. This cantileverwould be inserted into the bracket or tube of the pos-terior unit and ligated with a single point of contact tothe anterior segments, generating intrusive force thatacts on the incisor group. If a pure couple is desired,the degree of activation of the 2 cantilevers should beequal. The influence of friction is minimized in thisdesign, allowing free sliding of the cantilevers. A differ-ent mechanical design would be the combination ofthe labial and lingual appliances, as seen in Fig 3.
Proclination of the crown
Proclination by sagittal expansion. This is prob-ably the simplest way to improve the inclination oflingually inclined anterior teeth (see Figs 1f and 5).Any anteriorly directed force applied at the level ofthe incisor brackets will produce a moment, withrespect to the center of resistance, equal to the dis-tance between brackets and centric relation (CR; cal-culated perpendicularly to the occlusal plane). Thesemoments generate an improvement of the inclina-tion of the incisors. A great variety of fixed andremovable appliances can successfully achieve thistask. This kind of movement is one of the most fre-quently encountered movements in orthodontictreatment. It can be, therefore, part of the treatmentfor Class II, Division 2 malocclusions, where themandible is expected to be displaced forwardthrough repositioning, growth, or surgical interven-tions (Fig 4). In patients where the reactive, distallydirected forces are not acceptable, a face mask maybe recommended (Fig 5).
COPYRIGHT © 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING
OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-OUT WRITTEN PERMISSION FROM THE PUBLISHER.
73
VOLUME 1, NUMBER 1, 2000 Melsen/Fiorelli
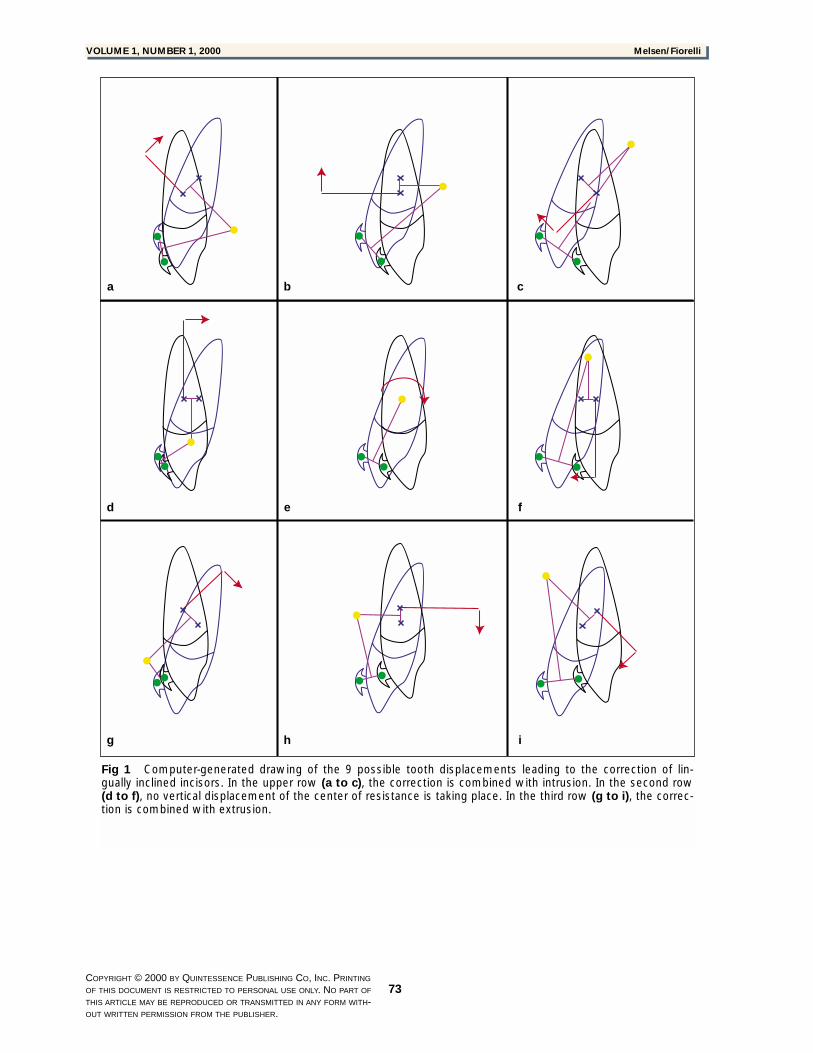
Fig 1 Computer-generated drawing of the 9 possible tooth displacements leading to the correction of lin-gually inclined incisors. In the upper row (a to c), the correction is combined with intrusion. In the second row(d to f), no vertical displacement of the center of resistance is taking place. In the third row (g to i), the correc-tion is combined with extrusion.
a b c
d e f
g h i
COPYRIGHT © 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING
OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-OUT WRITTEN PERMISSION FROM THE PUBLISHER.
74
Melsen/Fiorelli WORLD JOURNAL OF ORTHODONTICS
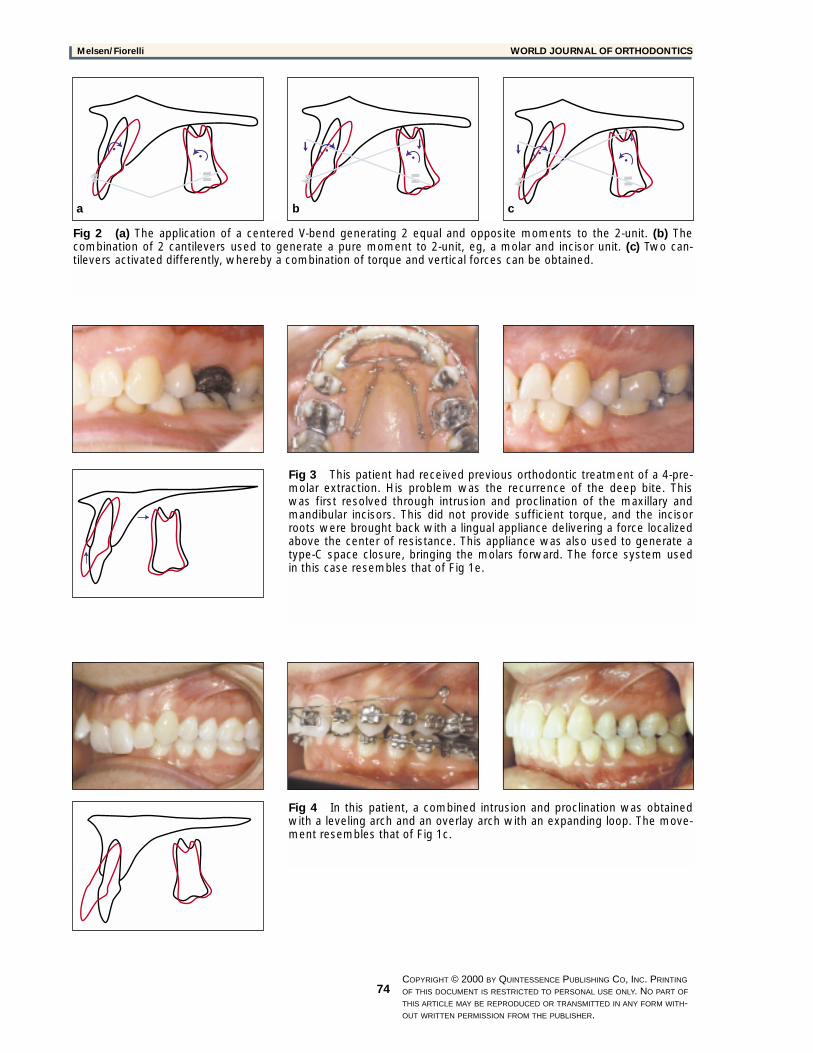
Fig 2 (a) The application of a centered V-bend generating 2 equal and opposite moments to the 2-unit. (b) Thecombination of 2 cantilevers used to generate a pure moment to 2-unit, eg, a molar and incisor unit. (c) Two can-tilevers activated differently, whereby a combination of torque and vertical forces can be obtained.
Fig 3 This patient had received previous orthodontic treatment of a 4-pre-molar extraction. His problem was the recurrence of the deep bite. Thiswas first resolved through intrusion and proclination of the maxillary andmandibular incisors. This did not provide sufficient torque, and the incisorroots were brought back with a lingual appliance delivering a force localizedabove the center of resistance. This appliance was also used to generate atype-C space closure, bringing the molars forward. The force system usedin this case resembles that of Fig 1e.
Fig 4 In this patient, a combined intrusion and proclination was obtainedwith a leveling arch and an overlay arch with an expanding loop. The move-ment resembles that of Fig 1c.
a b c
COPYRIGHT © 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING
OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-OUT WRITTEN PERMISSION FROM THE PUBLISHER.
75
VOLUME 1, NUMBER 1, 2000 Melsen/Fiorelli
Proclination and intrusion. This displacement iseasily generated, since it only requires a line of actionof a force with an intrusive component applied to theanterior brackets (Figs 1b, 1c, 5, and 6). An intrusiveforce applied to the incisors will generate a change ininclination (Figs 5 and 6). The moment delivered tothe incisors depends on the perpendicular distancefrom the CR to the line of action of the force. This dis-tance is small in the case of lingually inclined incisors,even when the most anterior position of the point offorce application is chosen. The distance will increase,however, once the proclination and the intrusion has
started. Intrusion mechanics, such as a base arch ora cantilever, will not always result in a sufficientlylarge moment with respect to CR. In that case, a com-bination of 2 cantilevers or a statically indeterminatesystem, as described in the section on pure rotation,would be indicated (see Fig 2c). The only difference isthat there must be a difference between the 2 verticalactivations equal to the net intrusive force that isneeded for the anterior intrusion. The line of action ofthe resultant force will pass anteriorly to the bracketof the incisors at a distance equal to the moment-to-force ratio generated by the system.
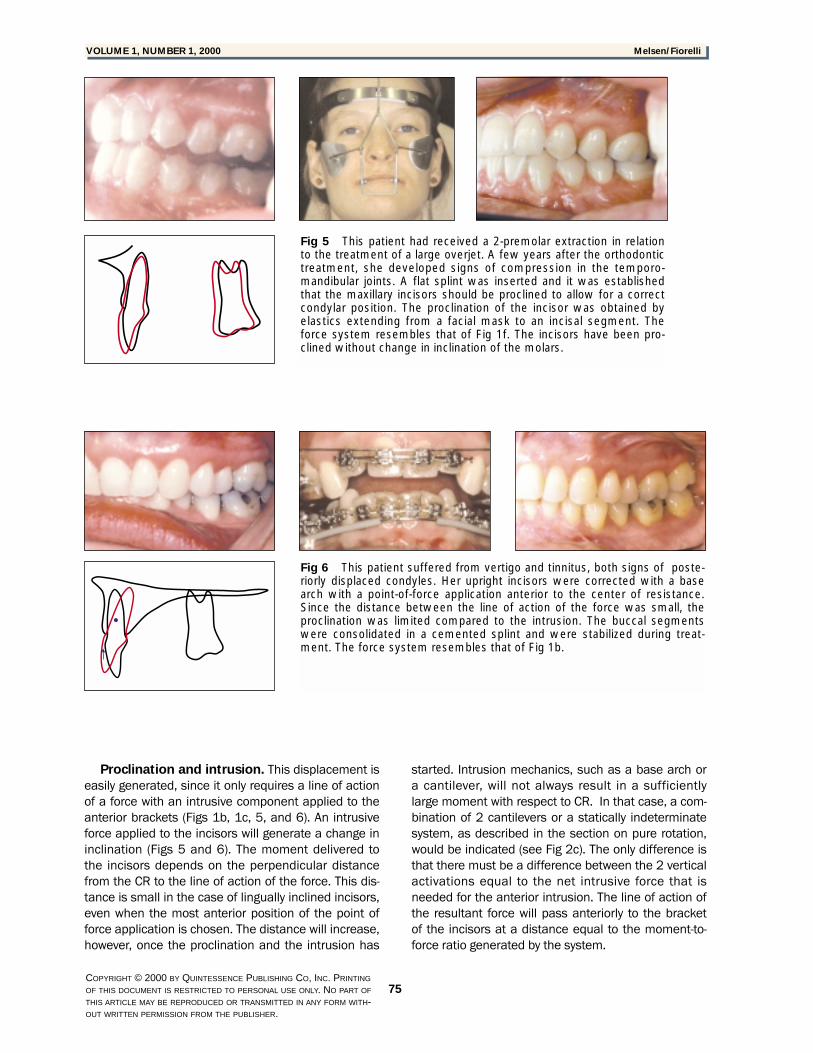
Fig 6 This patient suffered from vertigo and tinnitus, both signs of poste-riorly displaced condyles. Her upright incisors were corrected with a basearch with a point-of-force application anterior to the center of resistance.Since the distance between the line of action of the force was small, theproclination was limited compared to the intrusion. The buccal segmentswere consolidated in a cemented splint and were stabilized during treat-ment. The force system resembles that of Fig 1b.
Fig 5 This patient had received a 2-premolar extraction in relationto the treatment of a large overjet. A few years after the orthodontictreatment, she developed signs of compression in the temporo-mandibular joints. A flat splint was inserted and it was establishedthat the maxillary incisors should be proclined to allow for a correctcondylar position. The proclination of the incisor was obtained byelastics extending from a facial mask to an incisal segment. Theforce system resembles that of Fig 1f. The incisors have been pro-clined without change in inclination of the molars.
76
Melsen/Fiorelli WORLD JOURNAL OF ORTHODONTICS
COPYRIGHT © 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING
OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-OUT WRITTEN PERMISSION FROM THE PUBLISHER.
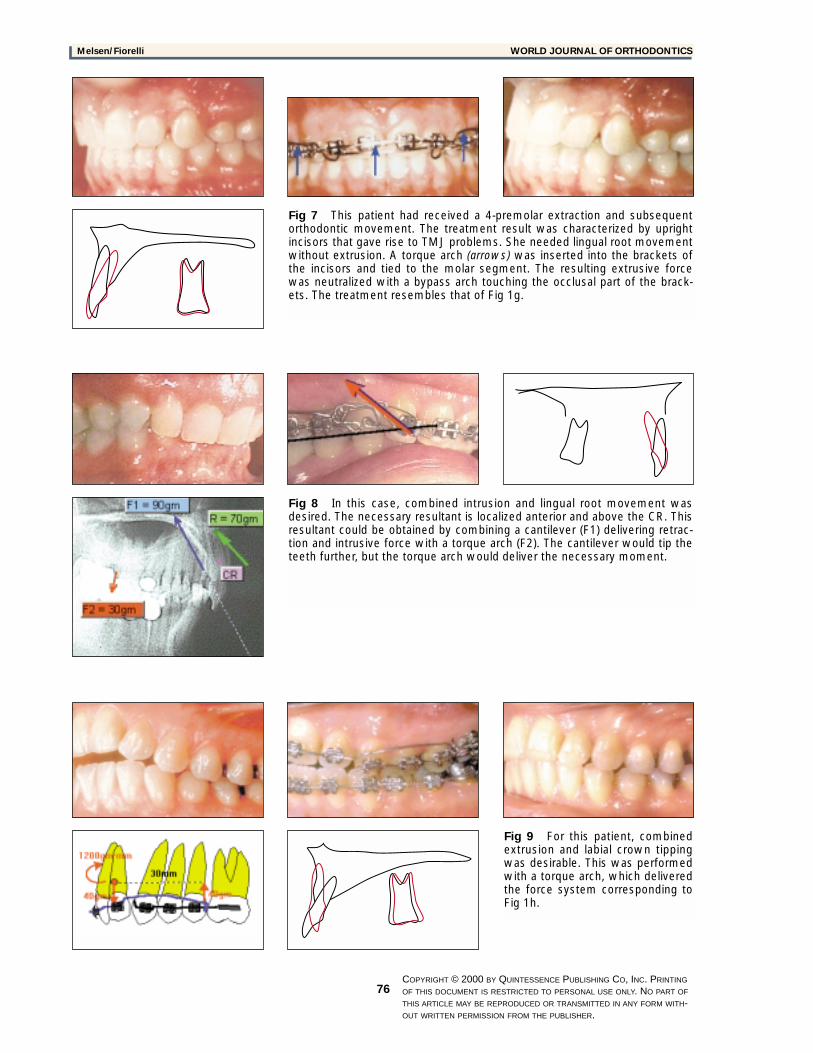
Fig 7 This patient had received a 4-premolar extraction and subsequentorthodontic movement. The treatment result was characterized by uprightincisors that gave rise to TMJ problems. She needed lingual root movementwithout extrusion. A torque arch (arrows) was inserted into the brackets ofthe incisors and tied to the molar segment. The resulting extrusive forcewas neutralized with a bypass arch touching the occlusal part of the brack-ets. The treatment resembles that of Fig 1g.
Fig 9 For this patient, combinedextrusion and labial crown tippingwas desirable. This was performedwith a torque arch, which deliveredthe force system corresponding toFig 1h.
Fig 8 In this case, combined intrusion and lingual root movement wasdesired. The necessary resultant is localized anterior and above the CR. Thisresultant could be obtained by combining a cantilever (F1) delivering retrac-tion and intrusive force with a torque arch (F2). The cantilever would tip theteeth further, but the torque arch would deliver the necessary moment.

COPYRIGHT © 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING
OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-OUT WRITTEN PERMISSION FROM THE PUBLISHER.
77
VOLUME 1, NUMBER 1, 2000 Melsen/Fiorelli
The relationship between the proclination and theintrusion depends on the force direction, whereas themoment delivered depends on the perpendicular dis-tance from the CR to the resultant. Proclination com-bined with intrusion can, depending on the relativequantity of the 2 displacements, be produced by anumber of different appliances. The parameters deter-mining the displacement are the point of force applica-tion and the force direction. Any point of force applica-tion anterior to the CR will produce a forward tippingmoment that will increase as the perpendicular dis-tance from the CR to the line of action increases. Thedirection of the force can be varied with use of a differ-ent cantilever configuration for intrusion.8 Thus, a util-ity-shaped arch would result in a more anteriorlydirected force than a regular tip-back bend.
Proclination and extrusion. This dental move-ment may be needed in the correction of invertedincisors, where the extrusive component can be use-ful for the generation of sufficient overbite for resultstability. The same movement may also be desirablein patients with a slight overbite or slight open bite. Atorque arch can generate the necessary force sys-tem, including a moment and an extrusive force. Thelength of the torque arch, inserted into the bracketsof the incisors and tied to the buccal segments, willdetermine the relationship between the moment andthe force. The configuration of the torque arch con-trolling the direction of the deactivation force will, onthe other hand, determine the relative amount of for-ward displacement of the crown (Figs 1g to 1i and 7).
Lingual root movement
Retroclination of roots. The incisor torque control,lingual root movement, has often been left to thelast stage of treatment, and the suggested torquedevices combine the lingual root torque with extru-sion (see Fig 1d). The deepening of the bite is gener-ally undesirable, and the possibility of this sideeffect is the likely reason why insufficient torque is acommon finding when observing posttreatmentextraction cases.
The difficulties in obtaining the combined intru-sion torque and retraction is well illustrated by theinfluence a minor change in the resultant force local-ization will have on the type of displacement.6
The combination of a torque arch delivering thedesired moment and a bypass arch extending fromthe reactive units to the buccal segments will pre-vent undesirable incisor extrusion. Tie-back of thebypass arch will also prevent forward displacementof the crown and thus displace the center of rotationto the crown (Fig 7).
Lingual root movement and intrusion. Lin-gual root movement combined with intrusion isdesirable in patients with lingually inclined incisorsand deep bite, and when increasing the overjet isunacceptable. This tooth movement is consideredthe most difficult, since it requires a line of action ofthe force localized above and anterior to the incisorsegment (see Fig 1a). A replacement force system,generated by a loop delivering the necessarymoment-to-force ratio, can be applied to the bracket.This solution has been presented3 and is based onclosing loop mechanics. Theoretically, it is possibleto activate a T-loop for this force direction with thecorrect moment-to-force ratio. The precision requiredfor such activation is, however, out of reach in dailyclinical practice. Therefore, we have used a com-puter program for the design of an appliance con-sisting of 2 cantilevers that can be tested by the clin-ician and which, when left in place for sufficienttime, will produce the desired movement.
The 2-cantilever mechanic represents a staticallydeterminate system, is easy to monitor, and has ahigh degree of constancy. On the other hand, stati-cally indeterminate systems, such as the T-loops, aredifficult to correctly activate and are characterized bya significant change of the force system developedat the 2 extremes of the spring during its deactiva-tion. This disadvantage applies to all statically inde-terminate appliances and makes their monitoringdifficult. Prediction of the force system deliveredfrom the loops activated for simultaneous intrusionand retraction is, therefore, of the utmost difficulty.
The correct combination of 2 cantilevers can bedefined through simple vectorial calculations. Thesecan be facilitated by computer software that is ableto define the second cantilever once given the resul-tant and a suggestion for the first cantilever (Fig 8).For example, if a torque arch delivering the desirablemoment is inserted, the arch will displace thecrowns forward and generate an extrusive force. Thisside effect can be counteracted by the addition of asecond cantilever that is designed so that, combinedwith the torque arch, it will generate the desiredresultant. Through an iterative process, the lengthand the point of force applications can be varied sothat the final result is feasible.2
The advantage of such a system is that it is stati-cally determinate, indicating that the clinician cancontrol the length and the force delivered by eachcantilever independently. Thus, the monitoring of theappliance is simple.
Lingual root movement and extrusion. Lin-gual root movement and extrusion is generally pro-duced when a tie-back is added to the torque arch.The moment delivered from the torque arch will

COPYRIGHT © 2000 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING
OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF
THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITH-OUT WRITTEN PERMISSION FROM THE PUBLISHER.
78
Melsen/Fiorelli WORLD JOURNAL OF ORTHODONTICS
attempt to procline the incisor crowns, whereby aretraction force is generated between the tie-backand the front segment. This results in a direction offorce that will generate lingual root movement com-bined with extrusion. This appliance is especiallyuseful in cases of open bite caused by underdevel-opment of the maxillary anterior segment (Fig 9).
CONCLUSIONCONCLUSION
This article provided the clinician with a discussionof treatment possibilities for lingually inclinedincisors, starting with the pure moment and alsoincluding the possible combinations with verticaland horizontal forces. Based on the one-to-one rela-tionship between tooth movement and necessaryforce directions, all the appliances were selected onthe basis of the resultant defined by special com-puter software.
Variation of the resultant force will generate com-pletely different methods of changing the inclinationof the incisor. The use of standard appliances forincisor torque should therefore be abandoned. Thedefinition of the desired movement—in other words,the treatment goal—should always precede theselection of the appliance. This is especially so in
cases where the line of action of the required forcecannot be generated by conventional appliancesand preadjusted brackets. The use of computers forappliance design is recommended if round-trippingis to be avoided.
REFERENCESREFERENCES
1. Nilner M. Relationships between oral parafunctions and func-tional disturbances in the stomatognathic system among 15-to 18-year-olds. Acta Odontol Scand 1983;41:197–201.
2. Fiorelli G, Melsen B. Biomechanics in orthodontics. CD-Rom,Rel. 2.0. Copenhagen, Denmark: Medi-Dent, 2000.
3. Burstone CJ. The segmented arch approach to space closure.Am J Orthod. 1982;82:361–378.
4. Melsen B, Fiorelli G. Computer Aided Orthodontic TreatmentPlanning. Orthodontics for the next millennium. Dallas: RohitC.L. Sachdeva, 1998.
5. Burstone CJ, Koenig HA. Creative wire bending—The force sys-tem from step and V bends. Am J Orthod Dentofacial Orthop1988;93:59–67.
6. Isaacson RJ, Lindauer SJ, Rubenstein LK. Moments with theedgewise appliance: Incisor torque control. Am J OrthodDentofacial Orthop 1993;103:428–438.
7. Wichelhaus A, Sander FG. Biomechanical testing of the newtorque-segmented arch. Fortschr Kieferorthop 1995;56:224–235.
8. Dalstra M, Melsen B. Force systems developed by six differ-ent cantilever configurations. Clin Orth Res 1999;2:3–9.





























