Embed Size (px)
Citation preview
6/5/2010
1
• ICD-10HIPAA 5010• HIPAA 5010
• General Hot Topics– Physician Signatures & CERT Audits– PECOS & Ordering/Referring Physician– PPACA & Timely Filing Changesy g g– CMS & 72h Rule– OIG Outpatient Charge Audit Algorithm
6/5/2010
2
• The many failures of ICD-9…Intended in its original adoption to collect information– Intended in its original adoption to collect informationon mortality starting in 1979
– 31 years later, the code set is being used for a variety of clinical and administrative activities for which it was never meant to be used.
– The structure of the system is inflexible and has d t it l bilitmaxed out on its scalability
6/5/2010
3
• The many failures of ICD-9…Many chapters are full and cannot handle new codes– Many chapters are full and cannot handle new codes,making the placement of some new codes arbitrary and senseless at best
– Procedure codes in particular are no where near the required level of technical description to match with clinical technology and approachesDi i d ft l l ki i– Diagnosis codes are often grossly lacking inappropriate nomenclature (i.e., bacteremia = UTI)
16,000 diagnosis and procedure codes exist, but you can easily say on a daily basisyou can easily say on a daily basis
yes, there’s an yes, there’s an app for that…app for that…
But no, there isn’t a code.But no, there isn’t a code.
6/5/2010
4
• The October 1, 2013 implementation date will be pushed backpushed back
• Non-covered entities (Worker’s Comp, auto insurers, etc. will not have to covert to ICD-10
• State Medicaid plans will not be required to update their systems in order to use I-10
• There will not be any I-10 codebooks• ICD-10 superbills will be far too complex to use easily• CPT is being replaced by I-10• GEMS will be used to facilitate coding
CMS Medicare Learning Network ICD-10-CM/PCS Myths & Facts,
6/5/2010
5
• General Equivalence Mappings• Bi directional translational dictionary model comprised• Bi-directional translational dictionary model comprised
of four (4) conversions:• ICD-9-CM to ICD-10-CM• ICD-10-CM to ICD-9-CM (initial conversion)• ICD-9-PCS to ICD-10-PCS• ICD-10-PCS to ICD-9-PCS
• Facilitates consistent conversion of equivalent codes from one standard to the other for the purposes of claimfrom one standard to the other for the purposes of claimformatting, reimbursement analysis, quality measures, risk calculations, etc.
• GEMS are also being used to convert MS-DRGs from ICD-9 to ICD-10ICD 9 to ICD 10
• Plan is to keep MS-DRGs in current format and logic, so extensive translation and testing exercises are being completed to validate the conversions in terms of accuracy
• Errors and issues identified in the GEMS testing processes are incorporated as corrections when theprocesses are incorporated as corrections when themapping is update every January (or sooner for critical issues)
6/5/2010
6
• ICD-10 create two completely separate and distinct systems for diagnosis and procedure coding:systems for diagnosis and procedure coding:– ICD-10-CM: Diagnoses– ICD-10-PCS: Procedures
• >69,000 ICD-10-PCS codes in 21 chapters• Updated annually in January
To facilitate conversion proposed last update to ICD 9• To facilitate conversion, proposed last update to ICD-9and ICD-10 systems will be October 1, 2011 (FY2012)
• ICD-10 goes live October 1, 2013 (FY2014)
• ICD-10-CM codes are 3-7 CHARACTERS• Character definitions:• Character definitions:
– Char 1 (alphabetic) + Char 2-3 (numeric) = CATEGORY – Char 4-6 (primarily numeric except for “x” placeholder in
positions 5 or 6) = ETIOLOGY, ANATOMICAL SITE, SEVERITY– Char 7 = EXTENSION (in some chapters)
• E Codes now have a first character V through YE Codes now have a first character V through Y• V Codes now have a first character of Z
6/5/2010
7
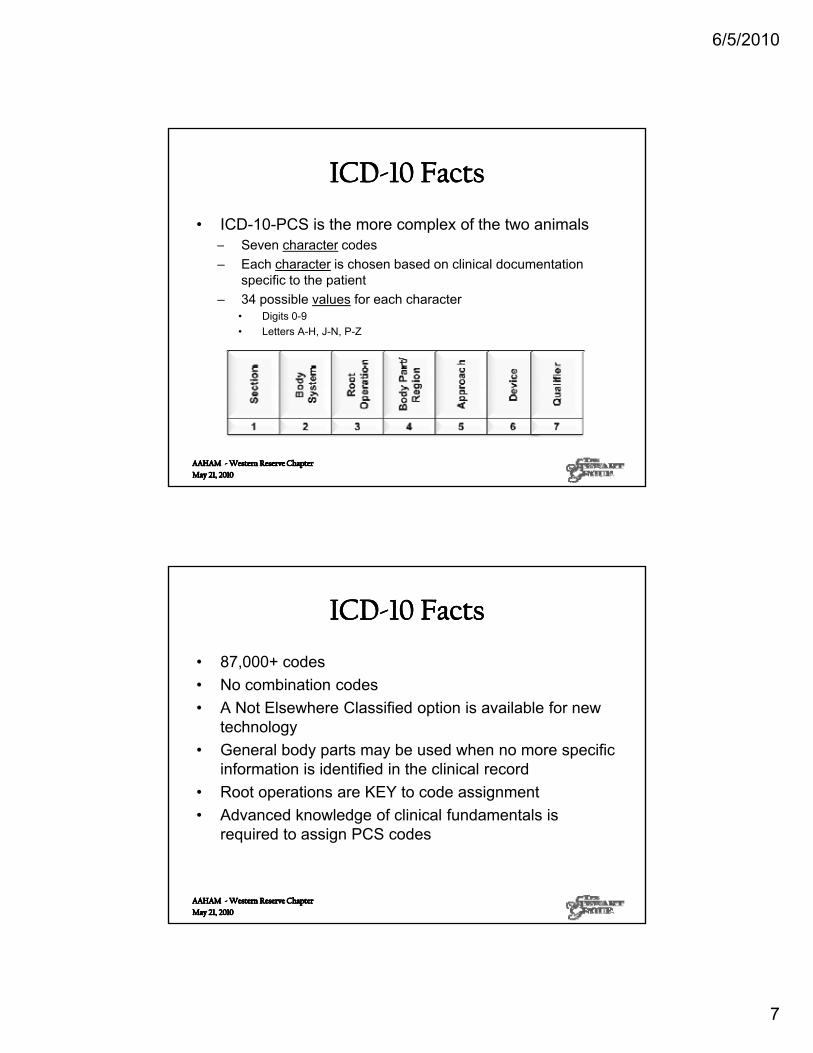
• ICD-10-PCS is the more complex of the two animals– Seven character codesSeven character codes– Each character is chosen based on clinical documentation
specific to the patient– 34 possible values for each character
• Digits 0-9• Letters A-H, J-N, P-Z
• 87,000+ codes• No combination codes• No combination codes• A Not Elsewhere Classified option is available for new
technology• General body parts may be used when no more specific
information is identified in the clinical record• Root operations are KEY to code assignment• Advanced knowledge of clinical fundamentals is
required to assign PCS codes
6/5/2010
8
• CMS estimates it will take approximately 50 hours of training to learn ICD-10-CM & PCS:training to learn ICD 10 CM & PCS:– 16 hours for ICD-10-CM– 24 hours for ICD-10-PCS– 10 hours for hands-on coding “practicum” using both systems
• Unfortunately, what was NOT factored in was the significant amount of clinical foundation reinforcementsignificant amount of clinical foundation reinforcementthat will be required in anatomy, physiology, disease pathology, etc.
• PFS and PAS professionals have long learned to use ICD-9-CM and PCS in their daily work not as coders,ICD 9 CM and PCS in their daily work not as coders,but from the front-end and back-end revenue cycle operation perspective.
• Unfortunately, ICD-10 will require SOME level of training for staff to understand the system since they will be working with it regularly.
• However the PCS portion of ICS-10 will absolutely• However, the PCS portion of ICS-10 will absolutelyrequire a very good relationship with HIM because there isn’t a book of ICD-10 procedures codes (and software will NOT solve the issue)
6/5/2010
9
• (ASC) X12 005010 Technical Report Type 3s (TR3s) for healthcare transactionshealthcare transactions
• National Council for Prescription Drug Programs (NCPDP) Version D.0 for pharmacy transactions (ASC X12 5010/D.0.)
• Standard for Medicaid pharmacy subrogation transactions (V3.0) for State Medicaid agencies to recoup payments for pharmacy services where third-recoup payments for pharmacy services where third-party payor has primary financial responsibility
6/5/2010
10
• 270/271 - Health Care Eligibility Benefit Inquiry• 270/271 - Health Care Eligibility Benefit Inquiryand Response
• 276/277 - Health Care Claim Status Request and Response
• 278 - Health Care Services - Request for Review and Response; Health Care Servicesand Response; Health Care ServicesNotification and Acknowledgment
• 835 - Health Care Claim Payment/Advice• 835 - Health Care Claim Payment/Advice• 837 - Health Care Claim: Professional ,
Institutional, and Dental, including coordination of benefits (COB) and subrogation claims
• NCPDP D.0 - Pharmacy Claim
*There are also changes in 5010 for the 834 (enroll. disenroll from health plans ) and 820 (health plan premium payment)
6/5/2010
11
• Front matterFront matter– Standardized implementation guides (TR3s)
• Technical improvements– Consistent terms across all guides– Separation of multi-functional segments
• StructuralAddition deletion modification &– Addition, deletion, modification &repositioning of loops, segments and data elements
• Data content
• Elimination of data that was rarely usedy• Decreased redundancy of data collected• Improved compliance with Minimum Necessary
requirements of privacy rule• Clarification of the definition of previously ill-
defined/described data elements so that only one element goes in a field with clearer definitions of theelement goes in a field with clearer definitions of theelement
6/5/2010
12
• Enhanced transactions to improve operating and financial p p gperformance for front-end and back-end functions
• Updated standards to reflect current processing environment and business needs– Present on Admission– ICD-10
• Additionally, CMS indicates they are also makingy y gtheir own systemic changes where possible:– Implementing standard acknowledgement and rejection
transactions across all jurisdictions (TA1, 999 and 277CA transactions);
– Improving claims receipt, control, and balancing procedures; – Increasing consistency of claims editing and error handling;
R t i l i di ti li i th d– Returning claims needing correction earlier in the process; and– Assigning claim numbers closer to the time of receipt.
6/5/2010
13
• Anesthesia will be billed in MINUTES• Billing providers must use same subpart schema in
billing across trading partners• Providers should start following 5010 content rules on
situational data and only send required data according to the HIPAA 5010 Guide and as needed for specific payer requirements (situational v. required rules)q ( q )
• PINS should no longer be submitted per 5010 rules
• I-10-CM diagnosis coding is very learnable, but PFS staff will need basic training for their everyday interaction withwill need basic training for their everyday interaction withthe codes.
• HOWEVER, ICD-10-PCS is a beast of EPIC proportions– Significant amount of clinical foundation and coding education to
take it onDoes not actually have formed codes but tables and tables of– Does not actually have formed codes, but tables and tables ofsegments and values that are always different based on the exact scenario in the book.
6/5/2010
14
• Get to know what you need to know• Get to know what you need to know– Identify a senior-management champion (CIO, CFO)– Convene an ICD-10/HIPAA 5010 Steering Committee
• PFS, PAS, HIM, IT, Quality, Administration
– Review CMS Transition Checklist (Addenda)– Complete comprehensive gap analysis:
• Systems inventory• 5010/ICD-10 data flow and manipulation (into and out of organization)• Report sources and distribution
• Get to know what you need to know• Get to know what you need to know– Develop implementation plan to address gap analysis findings
and ensure all stakeholders are included in the process – Include tracking of all contracted payors, as the HIPAA 5010
mandates applies to ALL insurers, not just fee-for-service providers
Fun fact: MMO is reporting they are an “early adopter” of the 5010, soas you work through your Level I & Level 2 testing, they should beavailable to readily test with your trading partners if you have an MMOcontract.
6/5/2010
15
• Level 1 Compliance: December 31 2010• Level 1 Compliance: December 31, 2010
• Level 2 Compliance: December 31, 2011
• Production
Strategic (Total Adoption)v.
Hybrid (Function Centric Adoption)v.
Tactical ComplianceTactical Compliance(Interface Level Adoption)
6/5/2010
16
• CMS Transmittal 327, Change Request 6698 (2010-Mar-16)
• Issue: CERT auditors have started issuingfull denials for chart reviews whereprovider signatures are MISSING orILLEGIBLE, even when remainder ofencounter meets all criteria
• Patient Protection and Affordable Care Act (2010-Mar-23)
• Issue: The PPACA signed into law in Marchchanged the timely filing requirement to 12MONTHS after the date of service effective withMONTHS after the date of service effective withDOS on/after October 1, 2009.
6/5/2010
17
• Medicare Change Requests 6417, 6421, 6696 • Issue: All Ordering and Referring Physicians
reported on Medicare Part B Claims effective January 3, 2011 MUST have a current PECOS record on file with CMS WITH their NPI numberrecord on file with CMS WITH their NPI number
• Different scenarios will cause for pause & requireDifferent scenarios will cause for pause & requireevaluation of your providers’ current PECOS record status– Providers enrolled AFTER Nov 2003– Providers enrolled BEFORE Nov 2003 who have submitted an
855R since that date– Providers enrolled BEFORE Nov 2003 who have NOT
submitted an 855R since that date– Providers who work for the DVA, DOD/Tricare, or PHS, as well
as Dentists who may refer or order Medicare services– Clinics & groups to whom a provider reassigns Part B payments
6/5/2010
18
Current PECOS Enrollment Look-Up:
http://www.cms.gov/MedicareProviderSupEnroll/06 MedicareOrderingandRefeupEnroll/06_MedicareOrderingandRefe
rring.asp#TopOfPage
6/5/2010
19
• Medicare overpayments for outpatient services• Medicare overpayments for outpatient services(primarily drugs) for DOS 01/01/2006 –06/30/2009
• Trigger criteria:(1) The amount paid for a line item was greater than the billed
charge by $500/$1000 or more, and(2) The number of units billed for the line item was more than two.
Elizabeth Stewart, RHIA, CCS, CRCA, CPMBVice President & Managing PartnerThe Stewart Group [email protected]@sc.rr.com803 530 4397803.530.4397