Embed Size (px)
Citation preview

Welcome tothe team25 years offrontline careSEE PAGE 10
Ebola: A raceagainst timeSEE PAGE 6
No. 90

Support us now at msf.org.uk
Your support
About DispatchesDispatches is written by peopleworking for MSF and sent outevery three months to oursupporters and to staff in thefield. It is edited by MarcusDunk. It costs 15.6p to produce,3.3p to package and 34.5p tosend, using Mailmark, thecheapest form of post. We sendit to keep you informed aboutour activities and about howyour money is spent. Dispatchesgives our patients and staff aplatform to speak out about theconflicts, emergencies andepidemics in which MSF works.We welcome your feedback.Please contact us by themethods listed, or email:[email protected]
Sign up to emailGet the latest MSF newsdelivered to your inbox. Signup at msf.org.uk/signup
Make a donationYou can donate by phone,online or by post. If possibleplease quote your supporternumber (located on the topleft-hand side of the letter)and name and address.
Leaving a gift in your willHave you thought ofremembering MSF in yourwill? Any gift is welcome,however large or small. Formore information, contactElisabeth Stodel at: [email protected] or callus on 0207 404 6600.
Changing your addressPlease call 0207 404 6600 oremail: [email protected]
Changing a regular giftTo increase or decreaseyour regular gift, please callus on 0207 404 6600 or email:[email protected] your request. Please alsoget in touch if your bank detailshave changed.
If you would like to stopreceiving communicationsfrom us please contact ourSupporter Care team on020 7404 6600 or by [email protected] we’ll be happy to help.Thank you for all your support.
Médecins Sans Frontières/DoctorsWithout Borders (MSF) is a leadingindependent humanitarian organisationfor emergency medical aid. In more than70 countries worldwide, MSF providesrelief to the victims of war, naturaldisasters and epidemics irrespective ofrace, religion, gender or politicalaffiliation. MSF was awarded the 1999Nobel Peace Prize.
Tel 0207 404 6600Address Médecins Sans Frontières,Chancery Exchange, 10 Furnival Street,London EC4A 1AB
@msf_uk
msf.englishEng Charity Reg No.1026588
REGULARS
2SITUATION REPORT
Mali: Vaccinating 10,000children in the desert
Yemen: Malnutrition ina conflict zone
Ethiopia: How one girlfound a family
South Sudan: Juba’sfemale mechanic
Tajikistan: CelebratingWorld TB Day
Jordan: Rebuilding lives
FEATURES
6DEMOCRATIC REPUBLIC OF CONGO
Ebola: A raceagainst timeRepairing bridges, comforting the dyingand fighting the fear: A nurse and a waterand sanitation specialist report from thelatest outbreak of this deadly disease.
10IRAQ
“A call came throughthe radio: a suicide vesthad been detonated...”
12COVER FEATURE
25 years of frontline careLandmines, gunshot wounds, genocideand hope: Four MSF staff look back on thehighs and lows of life in the field.
14SOUTH SUDAN
“Five minutesto port!”As a woman struggles in labouron a speedboat, the teamprepare for her arrival.
16DEMOCRATIC REPUBLIC OF CONGO
A Saturday likeno otherA football match turns into amedical crisis.
Contents
Christmas cardsPurchasing Christmas cards is a greatway to support our emergency medicalwork and spread the word about MSF.We have a varied selection of designs,including photos from our work inZimbabwe and Democratic Republicof Congo. We also have two imagesdonated by Royal Institute Artist DeliaCardnell. Cards come with envelopesin packs of ten and cost £6.00;MSF will receive 66% of the pack price.You can view the selection and placeyour order at msf.org.uk/cards. If yourequire further information, please callus on 020 7404 6600 and speak to ourSupporter Care team.
Autumn 2018 DISPATCHES 3
Support us now at msf.org.uk
SOUTH SUDANETHIOPIA
YEMEN
JORDAN
TAJIKISTAN
MALI
MALI
Being vaccinatedagainst diseases suchas diphtheria, measlesand whooping cough isa commonplace event formany children. But in thevast desert of northernMali, where insecurity,isolation and limitedhealth infrastructuremean many can’t accesshealthcare, it can provealmost impossible toprotect children againstthese illnesses.Almost impossible, that is, untilnow. Late last year, MSF and theMali Ministry of Health set outto vaccinate 10,000 children agedfive-years and under from 11 potentiallife-threatening diseases includingtuberculosis, measles, yellow fever,meningitis and diphtheria.
“A large proportion of the inhabitantsin this region are nomadic, movingfrom one place to the next with their
cattle,” says Patrick Irenge, MSF’smedical coordinator in Mali. “Thisposed an additional challenge, assome of these vaccines had to beadministered in three separate dosesover a number of weeks.
“We had to use motorcycles and othervehicles adapted to the arid terrain.The vaccines had to be kept betweentwo and eight degrees in the middleof a desert, where temperatures werereaching 50 degrees.”
Despite these obstacles, the teamssuccessfully carried out the campaignin three stages over four months,travelling over 37,000 miles; theequivalent of driving around theglobe one and a half times.
“These vaccinations mean that fewerchildren will become ill over time,”says Irenge, “which will have a bigimpact on the finances of familieswho won’t have to spend money onhealthcare. In a region like this,that really matters.”
msf.org.uk/mali
Eleven illnesses, eightvaccinations, four months:Vaccinating 10,000 children over37,000 miles of desert
11Illnesses: tuberculosis,measles, yellow fever,meningitis, diptheria, polio,Haemophilus influenzae typeB, tetanus, pneumococcus,hepatitis B and rotavirus
10,000children vaccinated
37,280 milescovered in northern Mali
The distance covered is1.5 times the circumferenceof the Earth

DISPATCHES Autumn 2018SITUATION REPORT4
Support us now at msf.org.uk
Left: A youngboy withburnsreceives aphysiotherapysessionduringsurgery tohelp himrecovermobility in hisright arm atthe Al-Salamhospital inKhamer, northYemen.Photograph© AgnesVarraine-Leca/MSF
MSF teams in west Yemen continue to treat significantnumbers of children suffering from malnutrition.Although the security situation in the areais now more stable, with fewer airstrikesthan in the northern and coastal regions,malnutrition and difficulties in accessinghealthcare remain serious problems.
“People often think malnutrition is theresult of food not being available,” saysDr Vinh Kim Nguyen. “But here, it’smore an economical problem wherepeople can’t afford the food availablein the markets.
“Living conditions in the country havebeen difficult for a long time. There wasalready a high level of malnutrition, butthe war has clearly made the situationworse. Some areas are more affected thanothers, particularly remote valleys withvery isolated communities.”
In Amran governorate, Yemenis can nowtravel more safely to access healthcare,but they can’t always afford the cost oftransportation to reach a health facility.Since March 2015, the national averageprices of fuel commodities have morethan doubled, and Amran governorateis still suffering from scarcity of fuel.
To help address the problem, MSFteams have been running outreachclinics in some of the more isolatedregions, providing basic health services,treating malnutrition and referring morecritical patients to the MSF-supportedAl-Salam hospital in Khamer.
msf.org.uk/yemen
YEMEN
Cut offfrom care
TAJIKISTAN
The MSF team celebrate WorldChildren’s Day with patientssuffering from drug-resistanttuberculosis, inside Machitonhospital, Dushanbe, Tajikistan.
msf.org.uk/tuberculosis
JORDAN
Sixteen-year-old Yousef receivesintensive physiotherapy at MSF’sreconstructive surgical hospital inAmman, Jordan. He sufferedthird-degree burns which left himunable to move his upper body,after being robbed and set on firein Baghdad, Iraq.
msf.org.uk/jordan
Photograph © Alpamis Babaniyazov/MSF
Photograph © Faris Al-Jawad/MSF
Autumn 2018 DISPATCHES 5
Support us now at msf.org.uk
Top left: Abang and baby JoyPhotograph © MSF
Above: Poni Betty workinginside MSF’s workshopin Juba Photograph ©Jason Rizzo/MSF
One morning in early February, a baby girl was foundon a pile of rubbish in a side street next to SaintMichael’s Church in Gambella town, Ethiopia.
The baby was naked, sufferingfrom severe hypothermia and verylow blood sugar levels. She wasrushed to the Gambella generalhospital where the MSF paediatricteam took charge of her care.
“We think that her mother mighthave given birth to the baby in thestreet, and can only assume thatthere was some sort of family orsocial problem,” says MSF’s DrCésar Pérez Herrero. “The babywas in a very bad condition, butour neonatal intensive care teamwere able to stabilise her condition.
“We were all touched by her plightand did our best to ensure thatshe was well cared for. One of ourcolleagues, Abang Ochudo Gilo,a translator in the maternity ward,was especially taken with her.”
The hospital’s medical directorbrought the case to the attentionof the child and women’s affairsdepartment in Gambella, as is the
standard procedure. By this time,Abang had made a very importantdecision. She decided that shewould like to adopt the child.Abang immediately filed arequest with the authorities, andpermission was granted after asearch for the baby’s family provedunsuccessful.
“I fell in love with the baby andwanted to protect her,” says Abang.
“I felt huge happiness when I sawher and that’s why, from that firstmoment, I decided to call her Joy.Joy is always smiling at everybody.We are all so happy with the newarrival who has changed our lives.”
MSF’s neonatal intensive care unitin Gambella hospital treats prematurebabies, neonatal infection, meningitisand malformations through pregnancy.In March 2018, more than 270 mothersgave birth and over 40 babies wereadmitted to the neonatal unit.
msf.org.uk/ethiopia
ETHIOPIA
How baby Joy found a familySOUTH SUDAN
The mechanicof Juba
MSF’s workshop in Juba, SouthSudan, services vehicles, trucks,and generators for MSF projectsacross the country. Poni Betty isone of the workshop’s mechanics.
“My name is Poni Betty and I’m a mechanicworking for MSF. I love this work. There are somany things to do, like repairing the steeringsystem, the AC system. There are so manydifferent things to work on in the car.”
“What a man can do, a woman can do. So, I’mencouraging ladies to join the mechanics. Youshould not see this as a man’s work. But wewomen can also do it.”
“I’m married and I have two children. Myyoungest child is five-years-old. When he seesme driving and working, he tells me he feelsgood. There was a day he told me he wants tostudy, so that he can also become a mechanicand he can drive as well.”
“When I go home in my overalls and see myMum she says, ‘Okay, this is our engineer.This is our girl and she is an engineer.’ Theyfeel proud of me, and that makes me proud.”
msf.org.uk/southsudan
EbolaA race against time
DISPATCHES Autumn 2018EBOLA: A RACE AGAINST TIME6
Support us now at msf.org.uk
7
Support us now at msf.org.uk
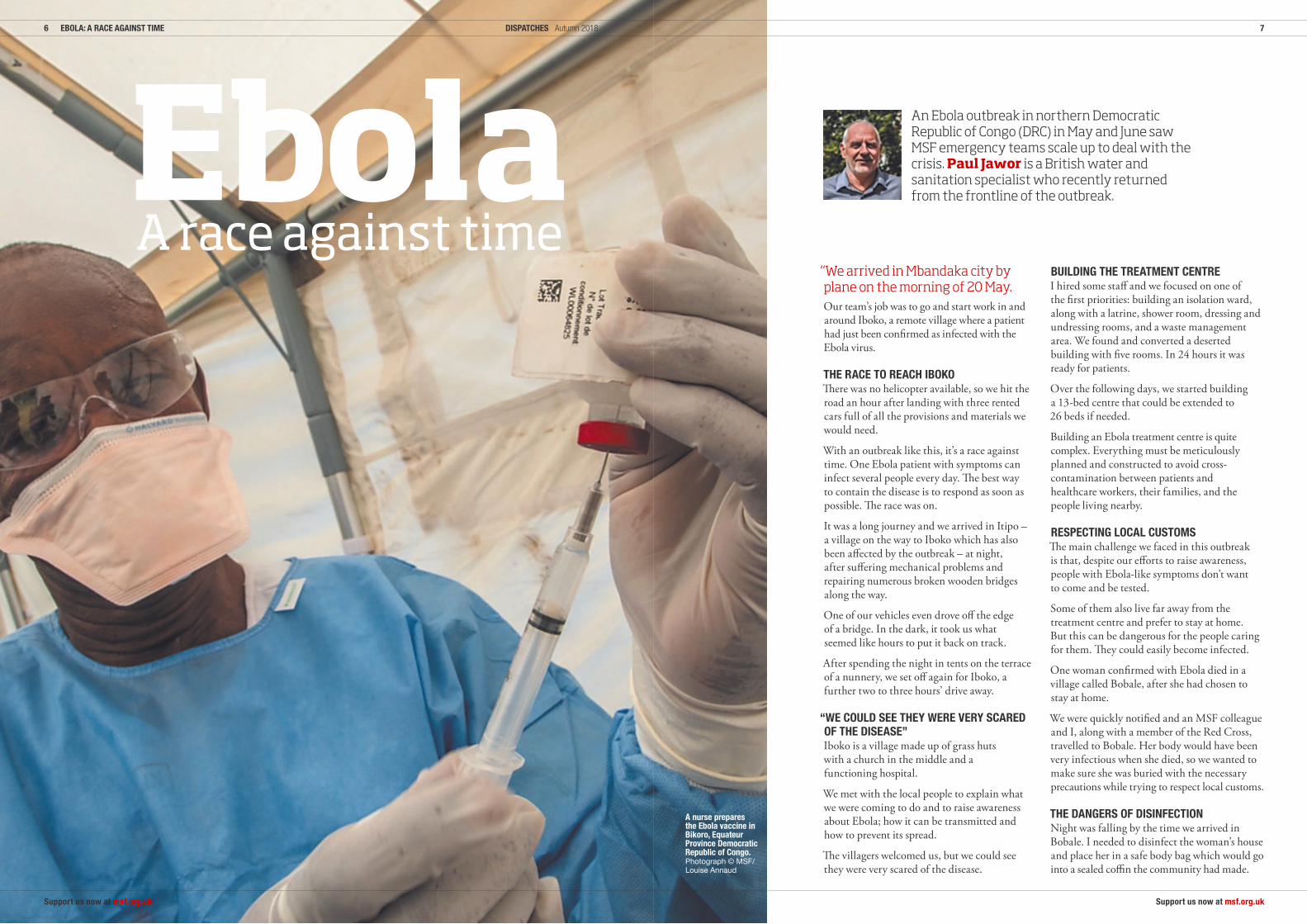
“We arrived in Mbandaka city byplane on the morning of 20 May.Our team’s job was to go and start work in andaround Iboko, a remote village where a patienthad just been confirmed as infected with theEbola virus.
THE RACE TO REACH IBOKOThere was no helicopter available, so we hit theroad an hour after landing with three rentedcars full of all the provisions and materials wewould need.
With an outbreak like this, it’s a race againsttime. One Ebola patient with symptoms caninfect several people every day. The best wayto contain the disease is to respond as soon aspossible. The race was on.
It was a long journey and we arrived in Itipo –a village on the way to Iboko which has alsobeen affected by the outbreak – at night,after suffering mechanical problems andrepairing numerous broken wooden bridgesalong the way.
One of our vehicles even drove off the edgeof a bridge. In the dark, it took us whatseemed like hours to put it back on track.
After spending the night in tents on the terraceof a nunnery, we set off again for Iboko, afurther two to three hours’ drive away.
“WE COULD SEE THEY WERE VERY SCAREDOF THE DISEASE”Iboko is a village made up of grass hutswith a church in the middle and afunctioning hospital.
We met with the local people to explain whatwe were coming to do and to raise awarenessabout Ebola; how it can be transmitted andhow to prevent its spread.
The villagers welcomed us, but we could seethey were very scared of the disease.
An Ebola outbreak in northern DemocraticRepublic of Congo (DRC) in May and June sawMSF emergency teams scale up to deal with thecrisis. Paul Jawor is a British water andsanitation specialist who recently returnedfrom the frontline of the outbreak.
BUILDING THE TREATMENT CENTREI hired some staff and we focused on one ofthe first priorities: building an isolation ward,along with a latrine, shower room, dressing andundressing rooms, and a waste managementarea. We found and converted a desertedbuilding with five rooms. In 24 hours it wasready for patients.
Over the following days, we started buildinga 13-bed centre that could be extended to26 beds if needed.
Building an Ebola treatment centre is quitecomplex. Everything must be meticulouslyplanned and constructed to avoid cross-contamination between patients andhealthcare workers, their families, and thepeople living nearby.
RESPECTING LOCAL CUSTOMSThe main challenge we faced in this outbreakis that, despite our efforts to raise awareness,people with Ebola-like symptoms don’t wantto come and be tested.
Some of them also live far away from thetreatment centre and prefer to stay at home.But this can be dangerous for the people caringfor them. They could easily become infected.
One woman confirmed with Ebola died in avillage called Bobale, after she had chosen tostay at home.
We were quickly notified and an MSF colleagueand I, along with a member of the Red Cross,travelled to Bobale. Her body would have beenvery infectious when she died, so we wanted tomake sure she was buried with the necessaryprecautions while trying to respect local customs.
THE DANGERS OF DISINFECTIONNight was falling by the time we arrived inBobale. I needed to disinfect the woman’s houseand place her in a safe body bag which would gointo a sealed coffin the community had made.
A nurse preparesthe Ebola vaccine inBikoro, EquateurProvince DemocraticRepublic of Congo.Photograph © MSF/Louise Annaud

DISPATCHES Autumn 2018EBOLA: A RACE AGAINST TIME8
Support us now at msf.org.uk
But it was dark and there wasn’t enough lightto enter the house without the risk of tearingmy protection suit on sharp objects. We decidedto postpone until the next morning.
It took an hour, sweating in my protection suit,to spray the house and disinfect the woman’sbody in a respectful way. Her husband stoodclose by, watching as I collected all the clothes,sheets and other potentially contaminatedmaterials into a bag that I sprayed with chlorine.That was, in turn, put into another bag, sprayedagain, and put into another bag. It was thentaken back to our treatment centre and burnt.
We are taking the maximum number ofprecautions to avoid spreading the disease.”
Luis Encinas, anurse from Spain,spent several weeksworking in MSF’s Ebolatreatment centres innorthern DRC.
“Tonight, I accompany two nurses inside the Ebolatreatment centre. I ask if there are any children inhospital. There aren’t. Since becoming a dad, theimage of a dying child puts a knot in my stomach.
I’m wearing my canary yellow suit. XL this timeas I’m 6”4. I can breathe. But the boots are anotherstory. The biggest size they have is 43. I sink myfeet inside as best I can but my toes are scrunched.
I finish dressing in the protective suit and checkthe suits of my colleagues: Patrick and Héritier.Their fear transmits to me. One of the patientsinside the centre is a colleague of theirs. We headinto the high-risk area.
THE WORDS ARE TOO MUCHWe enter the first room: four beds and twopatients wandering around, complaining ofjoint pain. They are waiting for their medicationand the evening meal. We exchange somewords with them and help them.
There is a nurse in the process of recovery. Hegives me his hand. I rest mine on top. We lookat each other without talking much, the wordsare too much. I give him all my energy and wishhim courage. ‘It will be fine!’ he says with ahalf-smile. It’s poignant.
THE SMELL OF CHLORINEBefore arriving at the second room, we mustgo through a long passageway. Two patients arelying on the floor: a priest and another nurse.They have trouble getting up.
They sit up with difficulty, and have troublespeaking. We try to help them inside the room,but they refuse. It’s the smell of the omnipresentchlorine that disturbs them.
Then I arrive in room two. There are fourpatients inside. We help a woman up on to herbed. Her strength has gone and we struggle toconnect her IV bag.
My colleagues are with me. Our eyes meet andwe check how each other is doing. We attend tothe other patients. Time is running at incrediblespeed. Here we are in the last room: theantechamber of death.
I CROUCH DOWN AND TAKE HER HANDA woman is lying here with swollen lips. Salivafoams from her nose. She’s barely breathing andthe breaths she takes are fast and shallow.
“Itwasdarkand therewasn’t enoughlight toenterthehousesafelywithoutthe riskoftearingmyprotectionsuit.”
Autumn 2018 DISPATCHES 9
Support us now at msf.org.uk
Find out more: msf.org.uk/ebola
Find out more
The Ebolaoutbreak in DRCwas officiallydeclared overon 22 July. *From8 May to thatdate, MSF teamsand the CongoleseMinistry of Healthprovided care to:
38confirmedpatients
24of who survived
120+other patientswere treatedafter presentingwith symptomsconsistentwith Ebola
*As we went to press, it wasannounced that a newoutbreak of the disease hadbroken out in the Beniregion of North Kivu. MSFteams are currently on theground establishingtreatment centres.msf.org.uk/ebola
Here, too, the desire to be with her and comforther as she makes the journey to the hereafteroverwhelms me. I crouch down and take herhand. A few seconds, maybe a little more. Aminute or two. I stroke her hair. I feel my throatknotting, to the point where I can’t feel anything.
I get up, wash my gloved hands in chlorinatedwater, and head for the exit. On my return tobase, I still have enough energy to take a shower.
ENOUGH IS ENOUGH!At three in the morning, I wake with a start.I realise that the sheets are soaked. It’s sweat.My heart races.
What happened? Where am I? Where do thesecries come from?
“Help me Lord! Help!”
It’s the voice of Madeleine*, a patient who wasadmitted to the Ebola treatment centre twodays ago. But where is she?
I open the zip of my mosquito net and go out.There’s no one there.
I realise I’m having a nightmare. I take theopportunity to go outside and get some fresh air.I sit on the edge of the small wall and look at thesky and the stars. I see the faces of the patientsscroll by, one by one, slowly. Why them?
I take my head in my hands and cry silently.I feel so small, so helpless in the face of this.Then I’m filled with an incredible energy.I make a promise to fight for them.
Enough is enough!”
EBOLA VACCINE3,199 people were vaccinatedagainst Ebola with theinvestigational Ebola vaccinerVSVDG-ZEBOV-GP by teamsfrom MSF, the World HealthOrganization (WHO) and theCongolese Ministry of Health.This investigational vaccine hasnot yet been licensed and wasimplemented through a studyprotocol, which was acceptedby national authorities andMSF’s Ethical Review Board.
“The results of the trial suggestthat the vaccine will present areal benefit to people at highrisk of contracting Ebola,” saidMicaela Serafini, MSF’s medicaldirector, “protecting themagainst the infection. However,vaccination remains just oneadditional tool in the fightagainst the disease.”Participants receivedinformation on the vaccinebefore consenting, and continueto be carefully monitored.Participation was voluntaryand the vaccination is free.
Above left:Luis and hiscolleagueJosuéassess ayoung boywho hasbeen incontact withan Ebolapatient,during avaccinationcampaignfor the virusin IkokoImpenge.Photograph© LouiseAnnaud/MSF
Above: TheMSF healthpromotionteamreceivestrainingin Bikoro.Photograph© LouiseAnnaud/MSF
Right:A doctorcheckson peoplerecentlyvaccinatedagainst theEbola virusto monitorany sideeffects inIkokoImpenge.Photograph© LouiseAnnaud/MSF
*Name has been changed.

DISPATCHES Autumn 2018FRONTLINE CARE10
Support us now at msf.org.uk
ChrisPeskettjoined MSFas a nursein 2002.
“I’ve been on 19 missions with MSF.What always strikes me about theorganisation is how seriously theytake our security. I’ve always feltsafe, although, of course, we cannever predict what’s going tohappen. But if you’re going to bewith anybody, MSF is the one tobe with if you’re in an insecureenvironment.
I worked in a very basic clinicduring my first mission in SouthSudan. The building was made of
Over the past 25 yearsMSF UK has sent 4,329experienced medical andlogistical staff from theUK to work in countriesaround the world.
To celebrate this milestone,we asked long-standingMSFers to reflect on someof their most memorableexperiences workingon the frontline. Fromrunning mass vaccinationcampaigns in Zambia tofacing deadly landminesin Angola, no day is thesame when you workfor MSF.
stone with a straw roof and dirtfloor. We had an improvised littleoperating theatre to conductsimple surgeries. That experienceshowed me what MSF is capableof doing in the most basic, mostisolated locations. You don’t neednice facilities, you don’t need nicebuildings. What you need is adedicated team following veryprofessional, simple guidelines.Everybody who works for MSF istrying to deliver the best possiblecare to the people most in need.
I’ve worked a lot in HIV and TBprojects around the world. In manycountries these diseases are stillemergencies, because people do notalways have access to the care theyneed and patients can also face alot of stigma from theircommunities. A lot of people don’trealise that TB is an emergency,because it’s ever-evolving intodrug-resistant forms and normalmedications don’t work.
In Zambia I was also involvedin one the biggest choleravaccination campaigns in history.We vaccinated about 423,000people of all ages and genders injust three weeks. It was incrediblychallenging – we got up at quarterpast four every morning andfinished late at night. But it wasworth it in the end because ofwhat we managed to achieve.
Earlier this year I spent severalmonths working in a remote partof South Sudan, where we arerunning mobile clinics fordisplaced people living in thebush. On one occasion I remembera nine-year-old boy was brought tous with a gunshot wound to the leg.Someone had tried to patch himup, but by the time he arrived hisleg was really infected and puffy.Luckily he reached us in time and
4,329UK staff departures to thefield since 1993
70+countries worldwide
£52 millionraised from our UKsupporters in 2017
“People are alivebecause MSFwas there”
Autumn 2018 DISPATCHES 11
Support us now at msf.org.uk
we managed to treat his infection.If he hadn’t been to the clinic, hecould have died.
I’ve been working as a nurse forMSF for many years. I’ve been toa lot of different countries, but Ikeep returning to South Sudan.The challenges are great, but theneeds are even greater. Thesatisfaction of working in thecountry, bringing much neededhealthcare to very vulnerablepeople, is one of the driving forcesfor me and my colleagues. I couldsee myself going back again.”
PaulForemanspent 16 yearsworking forMSF as a
project coordinator andHead of mission.
“Working in a country withlandmines really scared me. Myfirst proper mission with MSF wasin Angola, which was just comingout of a very long civil war. Therewere landmines everywhere, andwe lost a Land Cruiser ambulancewith 13 people in it, six of whomwere killed.
They’d gone out with five or sixpeople in the vehicle, had pickedup a load of patients so therewere 13 in the car, which is themaximum you could take. Thatwas the difference between drivingover the sandy road earlier in theday and not setting the mine off,and driving back on the same roadlater in the day with a load of extraweight, and setting it off.
You can’t negotiate with alandmine. You can’t see them andnobody will tell you that they’recoming. Having people arrest youor frequently facing guys armed tothe teeth is scary, but you can look
“It’s thesourceofmygreatestpleasureandpride toknowthatmenandwomenarealive,lookingafter theirchildrenandwalkingtheearth, becauseofsomethingyou’vebeeninvolved in.”
Left:Zambia,April 2016:A childreceivesa single-dose oralvaccinationagainstcholeraduringan MSFcampaignin Lusaka.Photograph© LaurenceHoenig/MSF
Below:Chad,January2004:A teamfrom MSFdelivers aidto Sudaneserefugees.Photograph© PeterCasaer
Right:Angola,January1998: Amine-clearanceexpert atwork.Photograph© MSF
them in the eye, find somehumanity and appeal to it. Butworking in a country that washeavily mined, making decisionsevery single day about where peopleshould go with the knowledgethat they could be blown to bitsbecause of those decisions; thatwas incredibly stressful and scary.I’ve worked in Ebola outbreaks andin areas where kidnappings werecommon and would do so again.But I’d think long and hard aboutgoing back to a country where landmines are prevalent.
The best thing about workingfor MSF is knowing that there arepeople who are alive who would bedead if MSF hadn’t been there. It’sdepressingly easy to count gravesand corpses, and we do that all thetime. But to go somewhere, workas a team to bring the mortalityrate down and improve the healthof people – there’s nothing betterthan that. It’s the source of mygreatest pleasure and pride to knowthat men and women are alive,looking after their children andwalking the earth, because ofsomething you’ve been involved in.
It’s a huge privilege to do what wedo. Stuff goes wrong all the timeand things fall apart; it’s the natureof our work. Catastrophe anddisaster are our stock in trade.But you go anywhere in the worldand ask people what they want,it’s always the same. They wanthealth and education so that theirchildren can grow up in a betterworld than they grew up in. If youcan help in providing half of thatequation, it makes everythingelse worthwhile.”

DISPATCHES Autumn 2018FRONTLINE CARE12
Support us now at msf.org.uk
Tish Shahjoined MSFas a doctorin 1999.
“A patient I’ll neverforget was a little nine-month-oldboy called Ali. He was very sickand I was not sure he wouldsurvive even one day. He stayedwith us for two months and nearthe end he gave me a smile, for thefirst time. While it was one of themost rewarding moments of mycareer, I realised that we weresending him back to an awfulsituation where there was limitedclean water, no nutritious foodand practically no healthcare provision.
My second mission was as projectcoordinator. It was not just abouttreating the people who cameto our facilities, but also thepossibility of reaching those thatcould not make the journey. Nextto medical engagement this alsorequired negotiating with themilitary for security reasons andensuring a positive team spirit.
I feel a lot of affection for somany colleagues and patients Ihave met along the way, who havebeen determined, humbling andinspiring. It’s been a privilege towork with MSF.”
Jacqui Tongjoined MSFin 1994 as anurse beforetaking on
numerous seniorroles in the field andat headquarters.
“How do you feel about Rwanda?’was the first thing MSF said to mein my interview. It was the time ofthe genocide and I had never fora moment imagined I would gothere. But I got on a cargo planein Belgium and flew into Goma, inthe now DRC. I was sent to whatwas at the time the world’s largestrefugee camp. I remember lookingaround and… it was so awful. Isaw some terrible things. I think itwas my innocence that saved me.
My second mission was Somalia.It was a really tough mission andI almost fell apart there.Psychologically it was really heavygoing. This was in the mid-90s andat that stage, Chechnya, Liberia,Somalia, and then of course,Bosnia, were considered to be themost toughest missions to go to.
My highlights are all those smallmiracles of patient survival, thosethat bring you back to your senseof purpose.”
Jacqui sadly passed away onSaturday 14 July at home in Geneva.She will be sincerely missed by herMSF family.
Above:Angola,September1999: AnMSF healthworkernegotiateswith anarmedsoldier.Photograph© Hans-JüergenBurkard
Below:Rwanda,January1993:Burundianrefugees fleeinter-ethnicviolence.Photograph© MSF
Join our 25-yearcelebrationInstead of buying a gift,dedicate your birthday,anniversary, Christmas orother special occasion to MSFby asking friends and familyto donate to our medical work.
How it worksLet us know if you arecelebrating with us by
calling Meera Patel on020 7067 4245 or registeronline at www.msf.uk/celebration.
We will then send you allthe information you need
to get started.
Ask your friends andfamily to donate to MSF’s
medical work in celebrationof your special day. Thank youso much for your support.
“Myhighlightsareallthosesmallmiraclesofpatient survival, thosethatbringyouback toyour senseofpurpose.”
Autumn 2018 DISPATCHES
Support us now at msf.org.uk
Respondingto an influxof patientsinjured bya suicidebomber late
last year in Iraq, Australiandoctor GeorgieWoolveridge wasconfronted with injuriesshe had never seen before.She recalls the moment aseverely wounded toddlerwas wheeled into MSF’semergency room…
“I’ve never wanted to forgetsomething so desperately as thefirst time I saw you. As I finishedtreating my sixth patient in onehour, I watched them wheel youin. You were one of two tiny bodieslaid out on a steel bed meant forbroken adults. Your baby brotherwas next to you.
I choked back tears as my worldhurtled away from the one I wasused to, where babies cried whenthey were immunised, hungry onlyin the minutes it took to prepare abottle, hurt only when learning towalk. Here in Tal Maraq, northIraq, children are brought tohospitals bloodied and lifeless.
An hour before, a call came overthe radio: a suicide vest had beendetonated at a checkpoint and afew ambulances carrying survivors
were on the way to us. Mechanismswere in place to accommodate thearrivals, but nothing could prepareme for the flood of human debristhat was to arrive.
Chaos descended and by the timeyour stretcher was wheeled in wewere engaged in a morbid game ofTetris with all the extra beds. Wehunkered down for the worst.
“I STOOD AT YOUR BEDSIDEAND LOST IT”I was dubious about you, little one.Limp, verging on lifeless and withinjuries that could potentiallyprove fatal, we worked as hard andfast as possible to stabilise you andyour brother, while our colleaguespetitioned authorities to grant uspassage through checkpoints soyou could be referred for moredefinitive care.
Medicine can make us hard,detached and emotionallydisengaged. But in a moment ofuncharacteristic calm betweenarrivals, I stood at your bedsidewith my hand on the side of yourhead and lost it just a little.
Implying you were lucky thatday is overstating things. Beinginvolved in a blast that killedyour mother and another sibling,leaving you and your brotherseverely injured doesn’t seemall that lucky.
But it was fortunate whenpermission was granted to send
a single ambulance through thecheckpoints. We stabilised you thebest we could and squeezed threetiny, war-ravaged bodies – you,your brother and an 11-year-oldboy – into the back of theambulance and sent you off.
MUSTERING HOPEVague reports filtered back to usabout your prognosis: alive, severebrain injuries, no family.
Two weeks later, I tracked youdown in a hospital two hours’ away.I walked with quiet apprehensioninto your room to find yousprawled in childish sleep – onehand instinctively flung over youryounger sibling, your ally. Andthen seeing you playing andcuddling for hours when youwoke is the most precious memoryI could take from an experiencethat overwhelmed me.
The day we met, I struggled todream of a future for you. Now,I can muster hope. My hope is thatone day, your biggest concern willbe which grassy hill to roll down,how to kick a ball past yourbrother, and how to negotiatea later bedtime. My hope is thatyou will thrive.”
Read more from Georgie atblogs.msf.org
Find out more
“A call camethrough theradio: a suicidevest had beendetonated...”
Above: Georgieholds a newbornbaby in Tal-Maraqhospital.Photograph © MSF
13

DISPATCHES Summer 2018SOUTH SUDAN14
Support us now at msf.org.uk
Photos byFrederic Noyin Old Fangak,South Sudan
“We’ll be at port infive minutes. She’sgiving birth now!”
OLD FANGAK 4:22PMThe radio is calling.
Alex: “ER for Camille...”
Camille: “We’ll be arriving at theport in five minutes. The womanis giving birth right now, we needa stretcher!”
Alex: “The emergency team willbe there to meet you!”
Camille, an MSF midwife, puts herhand on the belly of 36-year-oldMartha to check her labour, as theboat speeds down the river.
Martha lays at the bottom of theboat and clings to a bench. She isexperiencing contractions and isin a lot of pain.
Her sister, Nyajine, accompaniesher for support.
Just a few hours earlier the boat wasurgently called to retrieve Marthafrom the nearby village of Wanglel.She had gone into labour the daybefore and received support fromfriends and family. If there are nocomplications, giving birth at homecan often go well. But this time thedelivery has been going on too long,and Martha is also bleeding heavily.
The family have been trying to seekour help since yesterday, but thehospital is far away and the journeyis difficult.
Camille opens the paper case of acompress to help stop the bleeding,as Martha goes into the final stagesof labour on the floor of the boat.
An MSF translator leans in tocomfort Martha, over the roarof the boat’s engine.
In a remote hospital in South Sudan, acall crackles through the radio. An MSFboat is speeding towards port. Onboard,a woman is going into labour and isbleeding heavily. Emergency Room (ER)doctor Alexander Nyman and theteam are ready to meet them…
Summer 2018 DISPATCHES 15
Support us now at msf.org.uk
Her pain and contractions arenow more intense.
Martha already has five children athome: one girl and four boys. Sadly,she has lost two children.
The boat is approaching theriverbank at full speed. It slowsdown as it hits the sand. Theemergency team is already in place.
The whole crew is seated right onthe deck of the boat. I’m overseeingCamille, the midwife who’s helpingMartha to deliver her baby.
The child is in a cephalic position(head first). The head is alreadyout. The umbilical cord is wrappedaround the baby’s neck; Camilleputs two forceps on it, cuts thecord with scissors and releases itas she continues the delivery.
The baby is quickly wrapped up ina cloth and placed in the arms of theER nurse. We all run the 30 metresto the ER. Martha is put onto a
stretcher and rushed into thehospital. The infant isn’t crying orbreathing. The situation is critical.
The MSF emergency teamgathers to treat Martha’s baby.Nurse Delphine Jacquet and doctorMustafa Alajeeli join the efforts.
Martha is also in a seriouscondition. She’s lost a lot of bloodand is in shock. Here in OldFangak, there is no blood bank. Ifyou need a transfusion, it’s usuallya family member who will be thedonor – if their blood group is theright match, that is.
Luckily her sister had the rightblood group. We rapidly startedthe transfusion, and four hourslater her condition was stable.
Sadly, the baby did not survive.By the time they arrived at thehospital, it was already too late.It’s terrible that we couldn’t savethe child. But we did save Martha.
MSF’s UK VolunteersAfghanistan Suzanne Thorpe, Nurse; DilettaSalviati, Advocacy manager
Bangladesh Sophie Sabatier, Head of mission;Amy Garrett, Midwife; Sunny La Valle, Nurse;Emi Alicia Bensusan, Epidemiologist; John Phillips,Water and sanitation manager; Alexander Hunter,Water and sanitation manager; Elisabeth GanterRestrepo, Pharmacist; Mary Flanagan, Doctor
Cambodia Wendell Junia, Lab manager
Central African Republic Katherine Tomlinson,Nurse; Claire Simpson, Pharmacist
Chad Zuzanna Kucharska, Humanitarian affairsofficer; Jillienne Powis, HR manager; Jean MarieVianney, Logistician
Democratic Republic of Congo Mark Blackford,Finance coordinator; Marsha Mattis, HR manager
Ethiopia Christine Tasnier, Midwife; KennethLamden, Health promoter; Emma Turner,Deputy head of mission; Harriet Zych, Nurse
European migrant and refugee missionDeclan Barry, Doctor (Greece); Faris Al-Jawad,Communications manager (Greece); SophieMcCann, Advocacy manager (Greece); ElizabethAshford, Doctor (Greece); Clare Brigid Atterton,Nurse (Greece); Ben Du Preez, Advocacymanager (Greece)
Guinea Mohammed Sesay, Advocacy manager
Haiti Aglaia Manesi, HR manager
Honduras Samuel Thame de Toledo Almeida,Advocacy manager
India Fadumo Omar Mohamed, Psychologist;Sakib Burza, Head of mission
Iran Nicole Claire Nyu Hart, Medical team leader
Iraq Aimen Sattar, Logistician; Ismail Inan,Logistician; Peter Garrett, Doctor
Jordan Vittorio Oppizzi, Head of mission;Eve Bruce, Medical coordinator
Kenya Michael McGovern, Doctor;Ian Cross, Doctor
Lebanon Laura Gregoire Rinchey, Doctor;Luz Macarena Gomez Saavedra, Projectcoordinator; James Kelly, Logistician
Malawi Brian Davies, Advocacy manager
Mauritania Mohamed Camara, Pharmacist
Myanmar Bryony Lau, Deputy head of mission;Marielle Connan, Project coordinator
Nigeria Andrew Mews, Head of mission;Christopher Hook, Doctor
Pakistan Alexis Mackleworth, Doctor;Justin Healy, Doctor; Laura Holland,Water and sanitation expert
Palestinian Territories Jacob Burns,Communications manager; Alva White,Communications manager
Papua New Guinea Claire Mason, Doctor
Sierra Leone Lara Flatters, Nurse
Somalia Ruth Zwizwai, Epidemiologist
South Africa Amir Shroufi, Doctor
South Sudan Danila Luraschi, Doctor;Timothy Hull Bailey, Logistician; Jennifer Benson,HR manager; Tereza Kaplanova, Epidemiologist;Melissa Buxton, Nurse; Joan Hargan, Medicalteam leader; Isla Gow, Midwife
Sudan Alexandra Malet, Nurse
Syria Padraic McCluskey, Humanitarian affairsofficer; Duncan Stokoe, Logistician; BenjaminHargreaves, Logistician; Joshua Rosenstein,Project coordinator
Turkey Hayley Morgan, HR coordinator
Uganda Ryan Bellingham, Water and sanitationexpert; Julianna Smith, Research coordinator
Uzbekistan Ffion Carlin, Doctor; Yuhui Sha,Head of mission
Yemen Marissa Gripenberg, Epidemiologist;Cristina Ceroli, Midwife; Rachel Jane Fletcher,Hospital director; Alex Dunne, Humanitarianaffairs officer

DISPATCHES Autumn 2018DEMOCRATIC REPUBLIC OF CONGO16
Support us now at msf.org.uk
A Saturdaylike no other
ReemBouarroujis a Tunisiandoctor onassignmentin the
remote town of Walikale,Democratic Republic ofCongo (DRC). Here sherecounts how a footballmatch suddenly turnedinto a medical emergency...
“It was a Saturday like any other.In the morning I went to thehospital. My patients were stable.I went home, had lunch, andthought about taking a nap. Exceptthis is Walikale, in the heart of theDemocratic Republic of Congo.As my project coordinator toldme when I first arrived: ‘You neverknow what will happen here. Youmust always be ready for anything.’
He was right. This Saturday wasgoing to be unlike any other…
“THERE ARE PATIENTS WITHBULLET WOUNDS IN THE HOSPITAL”Suddenly we received an emergencycall. “There are patients with bulletwounds,” said the voice on theother end. “There was shooting atthe nearby stadium and injuredpeople are arriving.”
With the shooting ongoing, I wasnot allowed to move about untilour project coordinator couldconfirm it was safe. After a few,endless minutes, he called: “Doyou feel able to go?”
His question made me realise, onceagain, a reality about MSF: I willnever be forced to do somethingagainst my will.
Of course my answer was, “Yes,I’m ready!” As far as I’m concerned,my role is to be present, do my verybest and give everything I can.
MASTERING THE SITUATIONI went by motorbike with ourmidwife to the hospital. The peoplewe greeted along the way were calm.
While I was getting off the bike,I saw traces of blood. The hospitalwas full of people. I immediatelywent to the emergency room andfound two children. One had asuperficial injury and the otherwas suffering from anaphylacticshock – a severe and dangerousallergic reaction – caused whenhe was stung by something whilehiding from the gunshots.
After examining and treating thetwo children, I went to the surgerydepartment and then to the wardto examine the gunshot wounds.
It took us about three hours to masterthe situation, with everyone focusedon doing the best for our patients.
That afternoon there was anexceptional mobilisation ofpersonnel, even those who werenot supposed to be at the hospital.They heard the shots and didn’thesitate to rush in and help theircolleagues. I was proud to be partof this team.
WILL THE CALM RETURN?Returning to base after thisextraordinary Saturday, I feltconflicted. I was excited, havingbeen at the heart of the action,but scared that Walikale would nolonger be as calm as it was before.
The next day going to the hospital,I did not know what to expect or
how people were going to be.But Walikale was the same. Peoplesmiled as if nothing had happened.
Most Congolese people I meethave a wonderful temperamentand a rich kindness. Despite thecountry’s traumatic history anduncertain present, people seemjoyful. Meeting new people everyday has been pure happiness for me.
“I LAUGHED SO MUCH MYJAW HURT”One day we had a party in a smallimprovised shed that was coveredin tarpaulins. Suddenly it began torain and the earth under our feetturned to mud. Do you think itstopped us from dancing andsinging? Oh no! We were wet,had mud up to the knees and wecontinued to dance. I laughed somuch my jaw hurt!
Each day I’m learning to develop ataste for simplicity and spontaneity.We don’t know what tomorrowwill bring, but if it’s somethingunexpected like a shooting at afootball match, we’ll be readyand willing to give our all.”
Above:February16, 2017: Aplane bringssupplies tothe WalikaleHospital andthe 4 healthcentressupportedby MSF inthis regionof NorthKivuprovince.Photograph© GwennDubourth-oumieu
650256_UK_M
Read MSF blogs at blogs.msf.org
Find out more
Spread the word about MSF! Pass your copy of Dispatches on.