Embed Size (px)
DESCRIPTION
ref
Citation preview
![Page 1: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/1.jpg)
Numerical Simulation of Cardiovascular DynamicsWith Left Heart Failure and In-series Pulsatile
Ventricular Assist Device
Yubing Shi and Theodosios Korakianitis
Department of Engineering, Queen Mary University of London, London, UK
Abstract: This article presents a numerical model forinvestigations of the human cardiovascular circulationsystem response, where the function of the impaired leftventricle is augmented by the pumping action of a pulsatileventricular assist device (VAD) connected in series to thenative heart. The numerical model includes a module fordetailed heart valve dynamics, which helps to improve theaccuracy of simulation in studying the pulsatile type VADdesigns. Simulation results show that, for the case with leftventricular (LV) failure, the VAD support successfullycompensates the impaired cardiovascular response, andgreatly reduces the after-load of the diseased ventricle, thusassisting possible recovery of the ventricle from the dis-eased condition. The effects of these conditions on pulmo-nary circulation are also shown. To investigate the effect of
different pumping-activation functions (VAD motion pro-files) on the cardiovascular response, three different VADmotion profiles are investigated. The numerical resultssuggest that Hermitian type motion profiles (smoothcurves skewed toward early systole) have the advantage ofrequiring minimum power to the VAD, and producing theminimum after-load to the left ventricle, minimum ven-tricular wall stress, and minimum ventricular work to thediseased ventricle; while sawtooth type motions needslightly more power input, and induce slightly increasedaortic pressure in diastole, thus improving coronaryperfusion. Key Words: Numerical simulation—Cardio-vascular dynamics—Heart failure—Ventricular dysfunc-tion—Pulsatile—Ventricular assist device—Heart valvedynamics.
Since their first surgical implantation in the 1960s,ventricular assist devices (VADs) have greatlyhelped in the treatment of heart failure, either as abridge to transplantation, or as a bridge to recovery,while lately there is also mention of permanentimplantation (destination therapy) (1). Two kinds ofVADs are available for clinical usage now: the impel-ler pump types (which usually provide continuousblood flow); and the displacement pump types (whichusually provide pulsatile blood flow). The impellerpump type VADs have the advantage of producingrelatively larger volume rate of flows with lower pres-sures, while for relatively lower volume rate of flowsand higher-pressure applications the displacementpump type of VADs are generally more suitable (1).
Additionally, the impeller pumps operate at higherrevolutions per minute and are thus limited by thecavitation threshold and the maximum allowableshear rates (1), while the displacement pumps arelarger, operate at lower reciprocations per minute,and need relatively more complex control systems forproper function. In recent years some researchersalso proposed the application of pulsatile impellerpumps, producing the pulsatile flow by varying eitherthe rotating speed of the pump or the axial placementof the impeller in its casing in a heart cycle (2,3). Theadvantages and the disadvantages of the pulsatile andnonpulsatile effects have been intensively discussed.In supporting nonpulsatile perfusion, Saito et al. (4)investigated the hepatic and renal function andplasma renin levels in 15 healthy sheep under chronicnonpulsatile circulation support, concluded thatneither functional nor histologic changes wereobserved in major end organs, and stated that thenonpulsatile devices can be used safely for long-termsupport. Also Chow et al. (5) used near-infrared
Received March 2006; revised April 2006.Address correspondence and reprint requests to Dr. Theodosios
Korakianitis (a.k.a. Theodosios Alexander), Department of Engi-neering, Queen Mary University of London, London E14NS, UK.E-mail: [email protected]
Artificial Organs30(12):929–948, Blackwell Publishing, Inc.© 2006, Copyright the AuthorsJournal compilation © 2006, International Center for Artificial Organs and Transplantation
929
![Page 2: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/2.jpg)
spectroscopy to examine the relationship betweenpump flow rate and cerebral hemodynamics duringpulsatile and nonpulsatile cardiopulmonary bypass in40 patients, and concluded that pulsatile flow doesnot increase cerebral blood flow or alter hemoglobinconcentration during cardiopulmonary bypass inchildren. Recently, more pro-pulsatile perfusion evi-dence has been published. Sezai et al. (6) examinedthe major organ function under the pulsatile andnonpulsatile support by observing various physi-ological changes during 3-hour biventricular-assistedcirculation after acute myocardial infarction model inpigs. They concluded that pulsatile pumping pro-duced superior circulation in the kidney and liver,and microcirculation at the cell level was superior aswell in early treatment of acute heart failure. Resultsof other researchers also support similar conclusions(7). In an invited editorial (8), Ündar reviewed thevarious aspects of this dispute, confirmed the advan-tages of pulsatile over nonpulsatile perfusion, andalso revealed that pulsatile roller pumps can not beguaranteed to generate more “hemodynamic energy”when compared with nonpulsatile pumps, concludingthat in order to achieve the full advantages of pulsa-tile perfusion “physiological pulsatile pumps” arenecessary.
In the past decades enormous numerical andexperimental investigations have been carried outto improve VAD designs. As an economical and ver-satile tool in scientific research, numerical simula-tion has been extensively applied in the design andanalysis of VADs. The published articles on thesenumerical simulation works can be classified intotwo groups: those concentrated on developing thenumerical models, and those on the application ofthe developed model to investigate the hemody-namic response in the cardiovascular system underthe support of various VADs. The current researchstudies the interaction between the native cardio-vascular system and pulsatile VADs. This article pre-sents a detailed numerical model for the systemdynamics and belongs to the first group of studies.Future articles will use these models to studyvarious cases of system response under physiologi-cal and pathological conditions with various VADdesigns, and these articles will belong to the secondgroup of studies.
Previous numerical studies of cardiovasculardynamics under VAD assist concentrated on analyz-ing the system response and optimization of theVAD design, so that most of these studies used rela-tively simple cardiovascular system models. In ahierarchical series of articles Verkerke et al. (9)coupled a cardiovascular system model, including
the systemic circulation and the coronary circula-tion, and a pulsatile catheter pump type VADmodel, to study the influence of the VAD on thenative cardiovascular system. Other researchers(2,10) simplified the cardiovascular system into aWindkessel model or a Westkessel model combinedwith the left heart, while some researchers devel-oped complete cardiovascular system modelsincluding both the systemic and pulmonary circula-tion (3,7,11–13). From the point of view of accuracy,the complete cardiovascular system model as wellas the complete VAD model are necessary in thenumerical simulation.
Among the above numerical models, somestudied the interaction between the native cardio-vascular system and the nonpulsatile, impeller-typeVADs (3,13), some studied the impeller-type VADsbut changed the rotating speed of the impeller inthe heart cycle to produce pulsatile type VADaction (2,3), and some investigated the assistingaction of the intra-aortic balloon pump or of dis-placement type pulsatile VADs (7,9–12). Ündar (8)suggested that “physiological pulsatile pumps”provide the best hemodynamic VAD supportmechanism. To date the dynamic interaction of pul-satile and nonpulsatile rotary-type VADs with thecardiovascular system has been systematically inves-tigated with both numerical and experimentalstudies, while for the physiological pulsatile typeVADs, only the traditional intra-aortic balloonpump has been extensively studied with numericalinvestigations (10,12) as well as experimental study(14). Numerical study of other displacement typeVADs involve complex dynamic characteristics(7,9,11) and thus received less attention, but due totheir special hemodynamic advantage they still needfurther investigation.
The present article presents numerical models ofthe cardiovascular system and of physiological typepulsatile VADs, and investigates the interaction ofreciprocating valve pulsatile VADs with the nativecardiovascular system. Atrial contraction and heartvalve dynamics, which affect and contribute to thepulsatility of the physiological flow, are specially con-sidered in the model. Various types of prototypemodels for reciprocating valve VADs can be found inthe literature (e.g., [15,16]). In these designs any typeof prosthetic heart valve (monoleaflet, bileaflet,PTFE membrane, bioprosthetic, etc.) is mounted onan annular magnet, and it is moved in a reciprocatingmotion along the length of the VAD. The prostheticvalve is closed and acts as a piston pump in onedirection of motion along the length of the VAD,while it opens to let flow through the valve in the
Y. SHI AND T. KORAKIANITIS930
Artif Organs, Vol. 30, No. 12, 2006
![Page 3: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/3.jpg)
reverse direction of motion along the length ofthe VAD. Although both devices can be installed inthe traditional in-parallel configuration (in which theVAD inlet is in the left ventricular (LV) apex, and theVAD outlet is in the aorta), the designers of theVADs mentioned above recommend the in-seriesconfiguration (in which the VAD replaces a smallportion of the ascending aorta, as shown in Fig. 1a,b).This in-series pulsatile VAD application closelycouples the VAD’s pumping action with the remain-ing contractile ability of the diseased ventricle, thus
achieving improved pumping efficiency, and may alsoassist the recovery of the diseased ventricle. Thus, thein-series configuration takes advantage of the workof the native diseased ventricle, and in this way thepower consumption of the VAD is minimized. Alsothe aiding function of the VAD can be increased ifnecessary, decreased in the case of partial recovery ofthe native ventricle, or stopped in case of full recov-ery (16). With these advantages in-series applicationof these reciprocating valve types of VAD are goodprospects for clinical applications.
(a)
(b)
(c)
FIG. 1. Illustration of the simulation model. (a) Schematic of the native circulation system; (b) schematic of the reciprocating valve pumptype VAD; (c) illustration of typical forces acting on a heart valve leaflet.
CARDIAC DYNAMICS WITH PULSATILE VAD 931
Artif Organs, Vol. 30, No. 12, 2006
![Page 4: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/4.jpg)
MATERIALS AND METHODS
Model of the native cardiovascular systemA schematic of the native circulation system is
illustrated in Fig. 1a. The system is modeled in threemain parts: heart, systemic circulation loop, and pul-monary circulation loop. The heart is modeled as afour-chamber pump with variable elastance andfour heart valves that control the blood flow direc-tion. The systemic and pulmonary circulation loopsare each separated into aortic sinus/pulmonaryartery sinus, artery, arteriole, capillary and vein seg-ments. In every segment the individual componentis modeled by considering the local resistance toblood flow, elasticity of blood vessels, and inertia ofblood. The combined effect of venule, vein and venacava is modeled as the vein segment. The arterysegment represents the general characteristics ofboth the main and smaller arteries. The aorticsinus is separated from the artery to facilitate esti-mation of pressure response in the aortic arch. Thefollowing models, figures, and equations includerepeating symbols. Definitions of all the symbols areincluded in the nomenclature, while the values anddimensions of the variables are included in thetables.
Heart chambersIn modeling the heart, basic chamber characteris-
tics are described with the pressure-volume relationwith the widely used Suga et al.’s variable elastancemodel (17), in which the chamber pressure isdescribed as a linear function of the chamber volumeand the chamber elastance. The chamber volume isdecided by the flow-rate difference between the inletand the outlet of the chamber, while the chamberelastance varies in a heart cycle representing theaction of the heart muscle.
Take the left ventricle for example. The instanta-neous volume change in the left ventricle is equal tothe flow-rate difference between mitral and aorticvalves:
dVdt
Q Qlvmi ao= − (1)
The time-varying ventricle elastance is a functionof the characteristic elastance (Elv,s and Elv,d) and anactivation function elv(t):
e t EE E
e tlv lv,dlv,s lv,d
lv2
( ) = +−
⋅ ( ) (2)
The activation function elv(t) describes the contrac-tion and the relaxation changes in the ventricularmuscle. A commonly used activation function isadopted:
e t
tT
t T
t TT T
Tlv
s1s1
s1
s2 s1s( ) =
− ⎛⎝⎜
⎞⎠⎟ ≤ <
+−−
⎛⎝⎜
⎞⎠⎟
1 0
1
cos :
cos :
π
π 11 s2
s20
≤ <
≤ <
⎧
⎨
⎪⎪⎪
⎩
⎪⎪⎪
t T
T t T:
(3)
The pressure in the left ventricle is then derivedfrom the instantaneous volume and elastance valuesin the ventricle:
P P e V Vlv lv,0 lv lv lv,0= + −( ) (4)
The model for the right ventricle is similar to thatfor the left side, except the values of parameters aredifferent. Modeling of the left and right atria aresimilar to that for the ventricles, but with differentmaximum and minimum chamber elastances and dif-ferent activation function for the elastance change.The activation functions for the left and right atria,era(t) = ela(t), are set as:
e t
t T
t T
TT t T Tla
pwb
pwb
pwwpwb pwb pww
0
( ) =
≤ <
−−⎛
⎝⎜⎞⎠⎟
≤ < +
0 0
1 2
:
cos :π
:: T T t Tpwb pww+ ≤ <
⎧
⎨⎪⎪
⎩⎪⎪
(5)
Blood circulation loopsIn modeling the various components of systemic cir-culation, depending on detailed local flow conditions,the frictional loss, elastance, and blood inertia aremodeled as resistance, compliance, and inductanceeffects, following the classical idea of electric-fluidanalog. The native systemic circulation loop isdivided into five parts: aortic sinus, artery, arterioles,capillary, and vein. The artery is quite elastic, and theflow is pulsatile in this segment, so that all the resis-tance, compliance, and inductance effects must beconsidered.The aortic sinus has the similar character-istics as the artery segment, but in the simulation thissegment is greatly affected by the VAD, and thus, theinertial and resistance effects is combined into theconsideration of the VAD dynamics. The arteriolesand capillaries are dominated by the resistance effect.Veins function to collect and store blood, thus resis-tance and compliance effects are considered in thevein model.
Y. SHI AND T. KORAKIANITIS932
Artif Organs, Vol. 30, No. 12, 2006
![Page 5: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/5.jpg)
Pressure and flow-rate oscillations are experiencedin the aortic sinus due to the local tissue elastanceand result in important flow features related to coro-nary flow. The pressure is governed by:
dPdt
Q QC
sas ao sas
sas
=−
(6)
The pressure and flow-rate changes in the arteryare similar to that in the aortic sinus. As arteriolesand capillaries are both considered as pure resistanceunits, their effects are integrated with the artery asresistance units. Thus, the pressure equation is:
dPdt
Q QC
sat sas sat
sat
=−
(7)
and the flow-rate equation is:
dQdt
P P R R R Q
Lsat sas svn sat sar scp sat
sat
=− − + +( )
(8)
The systemic vein is modeled as a compliance com-bined with a resistance. In the vein the pressure is:
dPdt
Q QC
svn sat svn
svn
=−
(9)
and the flow rate is governed by:
QP P
Rsvn
svn ra
svn
=−
(10)
The pulmonary loop model is similar to that of thesystemic loop, with different values for systemparameters. Also as in the segment of the pulmonaryartery sinus all the resistance, compliance, and iner-tial effects are considered.
Heart valveIn the native heart there are four heart valves:
mitral, aortic, tricuspid, and pulmonary. In the recip-rocating valve type of pulsatile VAD described abovethe additional prosthetic-valve assists in the pumpingaction and becomes part of the dynamic system.Although the native and the prosthetic valves havedifferent geometries, their dynamic mechanisms ofoperation are similar, so their basic heart valve modelis identical, but different values are adopted in theparameters of the model to reflect the differencesamong the individual valves.
In the physical system heart valve dynamics aredominated by the blood–leaflet interaction effect(18,19). Full description of this effect needs detailed
three-dimensional distributed-parameter modeling ofthe pulsatile flow field around the valve and the valve-leaflet deformation/motion (such as with computa-tional fluid dynamics (CFD) studies).Previous studieson the blood–leaflet interaction effect (18,19) aremostly case specific, and cannot be used for overalldynamic modeling of the whole cardiovascular systemas illustrated in Fig. 1a. As a novel contribution, thisarticle makes a compromise between the detailedthree-dimensional study and the simplified diode-likedescription of the valve, using a concentrated-parameter method to describe the blood–leaflet inter-action effect. For this modeling purpose, the heartvalve is simplified as follows:a nominal leaflet openingangle is used as an average of the variation of angularposition in the different parts of the elastic leaflet; thedetailed pressure and velocity distributions in thevalve are rounded and replaced with the averagedpressure and flow rate before and after the valve.Thenominal leaflet opening angle is calculated by solvingthe governing differential equation for the leafletdynamics, which takes into account the contributionof the blood flow, while the corresponding leafletmotion also drives the local pressure and flow-ratechanges around the valve. This concentrated-parameter model of the blood–leaflet interactioneffect is less detailed than three-dimensional distrib-uted parameter studies, but is an advancement overthe diode models, and it satisfies the need of thepresent article to model the overall cardiovascularsystem.
In the current model the basic pressure-flow rela-tion in the aortic valve is described with an orificemodel:
QCQ AR P P P P
CQ AR P P P Pao
ao ao lv sas lv sas
ao ao sas lv lv sas
=⋅ ⋅ − ≥
⋅ ⋅ − ≤
:
:
⎧⎧⎨⎪
⎩⎪(11)
while the valve opening ARao is a function of theangular position of the valve leaflets, as illustrated inFig. 1c:
ARr
rao
ao
ao max
=−( )[ ]
−( )[ ]=
−( )−(
π θπ θ
θθ
1
1
1
1
2
2
2cos
cos
cos
cos max ))2 (12)
In Eq. 12, q is the leaflet opening angle. Zero (0degrees) for q corresponds to the fully closed leafletposition, and the maximum opening angle corre-sponds to the fully open leaflet position. q is com-puted by considering the various factors that affectthe leaflet motion. These include: the moment due tothe pressure difference across the valve; the momentgenerated by the shear stress on the leaflet due to
CARDIAC DYNAMICS WITH PULSATILE VAD 933
Artif Organs, Vol. 30, No. 12, 2006
![Page 6: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/6.jpg)
fluid flow; the moment produced by the frictionalforce; and the moment generated by the vortexnear the valve leaflet surface, as shown in Fig. 1c.Based on the CFD results of Hart et al. (18) and Shiet al. (19), the shear stress force is much smaller thanthe pressure force acting on the leaflet, so the shearstress acted on the valve is neglected. The effect ofthe vortex in the heart valve is an open question andits contribution is still under investigation. Someresearchers proposed that the vortices influence thevalve closing process (20), but this argument needsfurther validation, and it is the subject of futureinvestigations. Thus, in this article the vortex effect isalso neglected. Based on these considerations the fol-lowing governing equation for the aortic leafletmotion is derived:
Iddt
k P P A kddt
ao p,ao lv sas ao f,ao⋅ = ⋅ −( ) − ⋅2
2
θθ
θcos (13)
The number of coefficients is minimized by substi-tuting Kp,ao = kp,ao·Aao/Iao and Kf,ao = kf,ao/Iao:
ddt
K P P Kddt
2
2
θθ
θ= ⋅ −( ) − ⋅p,ao lv sas f,aocos (14)
The consideration of valve dynamics helps todescribe the regurgitant flow in the valve, thusimproving the accuracy of the simulation. Modelingof the remaining three native heart valves, and of theprosthetic valve in the VAD is implemented in thesame way, except the values of model parameters aredifferent.
Model of Pulsatile VAD pumping actionand motion
Traditional pulsatile VADs such as the aorticballoon pump and in-parallel installations of pneu-matic diaphragm pumps have been applied in clinicalpractice for many years, and numerous analyses havebeen carried out to study their performance. Themodel in this article concentrates on the in-seriesaction of reciprocating valve pulsatile-type VADs.These have various different implementations asillustrated by Larson et al. (15) and Korakianitis andGrandia (16). These different implementations havedifferent driving mechanisms and control strategies,which are beyond the scope of this article. As theemphasis of the present article is on the fluid–dynamic interaction of the VAD and the nativecardiovascular system, the motion profile of thepumping action is directly used in the current study.
Figure 1b illustrates the schematic of the recipro-cating pump. Any type of prosthetic heart valve
(leaflet, membrane, bioprosthetic, or other) ismounted on an annular magnet inside a cylinder. Inthe in-series configuration the length of the cylinderreplaces a portion of the length of the ascendingaorta. The annular magnet and valve assembly ismoved in a reciprocal fashion along the length of thecylinder (via external electromagnetic coils [15] andvia an external magnet [16]). In either case the flowthrough the prosthetic valve of the VAD can bemodeled by:
Q
Adxdt
CQ AR
P P
P P
Adxdt
CQvad
vad vad vad
sas sat
sas sat
vad
=
⋅ + ⋅ ⋅
−≥
⋅ +
:
vvad vad
sat sas
sas sat
⋅ ⋅
−<
⎧
⎨
⎪⎪⎪
⎩
⎪⎪⎪
AR
P P
P P:
(15)
When the VAD motion is properly designed flowin the VAD chamber is continuous, so that:
Q Qvad sas= (16)
Motion of the pumping action is specified by theVAD control algorithm. To have maximum VADworking efficiency and minimum impact to the physi-ological function of the native cardiovascular system,the pumping motion must be carefully designed. Inthe current research, three pumping motion profiles,illustrated in Fig. 2a, are examined, and their effectson the native cardiovascular response are evaluated.Figure 2b shows the three corresponding velocityprofiles. For easy comparison the electrocardiograph(ECG) signal is shown in Fig. 2 and the characteristicinstances of 0, Ttwe, and T are specially marked withdash-dot lines. (Comparisons of timing of thesemotion profiles with later system-response figurescan be made with the ECG trace.)
The first motion profile is the sawtooth profileadopted by Larson et al. (15):
x t
X tT
t T
XX t T
T TT t T
( ) =
⋅≤ ≤
−⋅ −( )−
< <
⎧ vad
twetwe
vadvad twe
twetwe
: 0
:⎨⎨⎪⎪
⎩⎪⎪
(17)
This motion profile is quite straightforward andeasy to implement in both the numerical model andmotion control algorithm. The general motion trendalso conforms to the ventricular motion, thus it helpsto reach a reasonable efficiency. However, in thismotion profile the VAD motion is not smooth (dis-continuity in velocity and acceleration) at instants 0
Y. SHI AND T. KORAKIANITIS934
Artif Organs, Vol. 30, No. 12, 2006
![Page 7: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/7.jpg)
and Ttwe. This affects the system response, and alsoincreases the instantaneous system power require-ment around these points. To improve the situation,we propose two further motion profiles. First, wepropose the use of two segments of sine wave toreplace the sawtooth function (as shown in Fig. 2a).With the sinusoidal profiles the slope of the motionprofile (the velocity) at instances 0 and Ttwe is speci-fied to be 0 m/s:
x t
X tT
t T
X t T( ) =
⋅ −⋅⎛
⎝⎜⎞⎠⎟ ≤ ≤
⋅ +⋅ −(
vad
twetwe
vad twe
2:
2
1 0
1
cos
cos
π
π ))−
⎛⎝⎜
⎞⎠⎟ < <
⎧
⎨⎪⎪
⎩⎪⎪ T T
T t Ttwe
twe:
(18)
The sine wave motion profile smooths the VADmotion, and thus helps to lower the power require-ment in the VAD specification. However, in the earlysystole part of ventricular contraction of the nativehealthy system the ventricular pressure increasesalmost exponentially. In order to produce a similarpressure response from the combined action of thediseased heart and VAD pumping motion, wepropose a displacement profile that increases fasterthan the sine wave in the early part of time betweent = 0 and t = Ttwe. In order to achieve this we proposefor the motion profile the Hermitian functiondescribed below (and illustrated in Fig. 2a).There aremany types of Hermitian profiles that could be used,but for the purposes of this article the displacementand velocity in the motion of the VAD are specifiedat time instants t = 0 s and t = Ttwe s. In addition, wespecify the position and slope of the motion profile atan intermediate instant between t = 0 s and t = Ttwe s,so that at t = Tr s the displacement is Xr m and the
velocity is Sr m/s. The return (nonpumping) motionprofile from Ttwe s to T s is the same as the sine wave.Thus, the proposed two-segment Hermitian motionof the pumping part of the profile for the VADbecomes:
x t
Xt T
TS t T
tT
t T
X
( ) =
⋅ −−⎛
⎝⎜⎞⎠⎟ + ⋅ −( )⎡
⎣⎢⎤⎦⎥
⋅
⎛⎝⎜
⎞⎠⎟ ≤ ≤
rr
rr r
rr
r
1 2
02
⋅⋅ −−−
⎛⎝⎜
⎞⎠⎟
+⎡⎣⎢
⋅ −( ) ⎤⎦⎥
⋅−−
⎛⎝⎜
⎞⎠⎟
1 2t T
T T
S t Tt T
T T
r
r twe
r rtwe
r twe
22
2
1 2
+ ⋅
−−
−⎛⎝⎜
⎞⎠⎟
⋅−
−⎛⎝⎜
⎞⎠⎟
< ≤
X
t TT T
t TT T
T t T
vad
twe
twe r
r
twe rr twe
XX t TT T
T t Tvad twe
twetwe
2⋅ +
⋅ −( )−
⎛⎝⎜
⎞⎠⎟ < <
⎧
⎨
⎪⎪⎪⎪⎪⎪⎪⎪
⎩
⎪⎪⎪⎪⎪
1 cosπ
⎪⎪⎪⎪
(19)
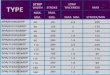
System parametersIn this work, most of hemodynamic variables used inthe numerical model of the cardiovascular system areassigned values by referring to published materials.Most researchers used variable elastance model todescribe the heart dynamics. By referring to param-eter selection in Ursino (21) and Lu et al. (22) in thecurrent research, chamber elastance values areassigned as shown in Table 1. Parameter settings asshown in Table 2 for systemic and pulmonary loopsare based on the works of Ursino (21) and Lu et al.(22). In modeling heart valve dynamics, coefficientsfor valve motion equations are selected through
(a) (b)
FIG. 2. Pumping action profiles of the left ventricular assist device (LVAD). (a) Motion profiles of the LVAD; (b) velocity profiles of theLVAD.
CARDIAC DYNAMICS WITH PULSATILE VAD 935
Artif Organs, Vol. 30, No. 12, 2006
![Page 8: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/8.jpg)
numerical experiments to find the optimal parametercombinations that produce near physiological valvemotion process as described in literature of De Hartet al. (18) and of Shi et al. (19), as shown in Table 3.Other parameters such as systolic duration, beginninginstance and duration of the P wave in the ECG signal,and the time step of simulation, etc., were chosenbased on general knowledge in physiological text-books (23).Table 4 shows values for these parameters.In assigning values to the VAD motion, the sectionalarea of the cylinder is decided based on the humanaortic geometry and the VAD design, and themaximum piston displacement is chosen based on thenormal stroke volume and the piston head area.
RESULTS
Based on the mathematical models describedabove, a program is developed in C language to simu-
late the dynamic changes in the cardiovascularsystem under various healthy, diseased, and VAD-supported conditions. In the study, first, the normalvalues are assigned to the cardiovascular variables toreveal the physiological response in healthy condi-tion; next, the LV characteristics are changed to simu-late the pathological condition of LV failure. Basedon the LV failure condition, the reciprocating valvepump as VAD with three kinds of motion profiles isindividually coupled with the diseased cardiovascularmodel to study the dynamic response of the nativediseased cardiovascular system under VAD support.Based on these results, important physiological vari-ables such as pressure in the left atrium and the pul-monary vein, and some characteristic variables, suchas the power requirement for the VAD, and LV wallstress, etc., are compared, to investigate the effect ofdifferent motion profile design on the cardiovascular
TABLE 1. Parameters for the heart
Parameter Value Parameter Value Unit
CQao 350 CQpo 350 mL/(s mm Hg0.5)CQmi 400 CQti 400 mL/(s mm Hg0.5)Elv,s 2.5 Erv,s 1.15 mm Hg/mLElv,d 0.1 Erv,d 0.1 mm Hg/mLPlv,0 1. Prv,0 1. mm HgVlv,0 5. Vrv,0 10 mLEla,max 0.25 Era,max 0.25 mm Hg/mLEla,min 0.15 Era,min 0.15 mm Hg/mLPla,0 1. Pra,0 1. mm HgVla,0 4. Vra,0 4. mL
TABLE 2. Parameters for the blood vessels
Parameter Value Parameter Value Unit
Csas 0.08 Cpas 0.18 mL/mm HgRsas 0.003 Rpas 0.002 mm Hg s/mLLsas 0.000062 Lpas 0.000052 mm Hg s2/mLCsat 1.6 Cpat 3.8 mL/mm HgRsat 0.05 Rpat 0.01 mm Hg s/mLLsat 0.0017 Lpat 0.0017 mm Hg s2/mLRsar 0.5 Rpar 0.05 mm Hg s/mLRscp 0.52 Rpcp 0.25 mm Hg s/mLRsvn 0.075 Rpvn 0.006 mm Hg s/mLCsvn 20.5 Cpvn 20.5 mL/mm HgVlv0 800 Vrv0 500 mL
TABLE 3. Parameters for variable valve opening model
Parameter Value Parameter Value Unit
Kp,ao 5500 Kp,po 5000 rad/(s2 mm Hg)Kf,ao 50 Kf,po 60 L/sKp,mi 6000 Kp,ti 5800 rad/(s2 mm Hg)Kf,mi 40 Kf,ti 45 L/sKp,vad 3500 rad/(s2 mm Hg)Kf,vad 25 L/s
Y. SHI AND T. KORAKIANITIS936
Artif Organs, Vol. 30, No. 12, 2006
![Page 9: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/9.jpg)
response. The heart period is chosen to be 1 s in thesimulation (60 beats per minute). In the simulation,the system often reaches periodic solution after fourto five heart cycles of calculation. The convergedsolution in the period from 10 to 11 s is chosen inevery simulated case for comparison of results. Forreference, the ECG signal is shown in some of thefigures, to facilitate comparison and illustration of thetiming in the cardiac cycle, and with the pumpingmotion profiles in Fig. 2.
This article introduces the numerical model devel-oped and presents some elementary results on thehemodynamic response in the cardiovascular systemin the healthy, diseased, and assisted conditions. Onlyrepresentative baseline healthy and diseased condi-tions, with and without VAD support, are presentedin this article. The in-depth exploration of the effectof each type of VAD on the cardiovascular system isthe topic of future works.
Response in healthy conditionsFirst, the simulation is carried out to simulate the
cardiovascular response under healthy conditions.For this purpose the normal physiological values areadopted in the model, and the VAD model is deacti-vated in the global model. Figure 3 shows the simu-lation results for pressure, flow rate, and volumechanges in the systemic and pulmonary circulationloops under the healthy condition. In Fig. 3 it isobserved that these simulation results agree well withthe typical drawings for cardiovascular responseshown in textbooks such as Textbook of MedicalPhysiology (23). The LV pressure is in the range of0–120 mm Hg, and the aortic pressure changesbetween 80 and 120 mm Hg. Periodic peak flows existin the mitral and aortic flows, with average flow rateof about 5 L/min. The LV volume change is approxi-
mately from 50 mL to 120 mL, with a stroke volumeof 70 mL. In the pulmonary circulation the cardiovas-cular response also matches the description in thephysiological textbooks. Accompanying the heartvalve closing motion in end systolic and diastolicphases, there are reverse flows in the four valves,which suggests the advantage of the current valvedynamics model over previous simpler models.
Response with LV failureTo simulate the pathological condition of LV
failure, the value of the maximum elastance in theleft ventricle is changed from the normal valueof 2.5 mm Hg/mL to the much impaired value of0.5 mm Hg/mL. Figure 4 illustrates the simulationresults for pressure, flow rate, and volume changes inthe systemic and pulmonary circulations under theLV failure condition, which agrees with representa-tive diseased heart results described by Guyton (23).(Comparison between healthy response, diseasedresponse, and diseased response aided with three dif-ferent VAD pumping profiles is also shown in Fig. 8.)
Generally, the cardiovascular response in the LVfailure condition follows the same trend as that in thehealthy condition, but the values for the physiologicalvariables change greatly. In Fig. 4a it is observedthat, under the LV failure condition, the aortic pres-sure range is reduced from the normal value of80–120 mm Hg to the current 46–68 mm Hg, and thepeak systolic LV pressure is reduced from the nor-mal value of 120 mm Hg to the current value of68 mm Hg. This greatly impaired perfusion conditionwill adversely affect the function of important organsin the cerebral, renal, and hepatic subsystems.Also inFig. 4a,d, it is observed that pressures in the leftatrium and the pulmonary vein are elevated to about14 mm Hg, almost increased 50% from the normalvalue of about 9 mm Hg. The LV failure situationsimulated here is a mild case. When the LV failuredevelops further, and the pressure of the pulmonaryvein is elevated to above 18 mm Hg, pulmonaryedema will manifest itself and serious consequence ofpulmonary failure will follow (23). In the flow-rateresponse of Fig. 4b,e it is illustrated that peak flowrates across the mitral and aortic valves are reducedto about 60% of the normal healthy values. At thesame time, although there is no great change in thepeak flow rates in the tricuspid and pulmonary valves,the flow rates drop faster from the peak. In thevolume response of Fig. 4c,f, it is observed that thereare prominent changes to all four chamber volumesin the heart. (The computed volumes of the heartchambers in the model are affected by the combinedeffect of the equations in the numerical model, Eqs.
TABLE 4. Additional parameters
Parameter Value Unit
Avad 0.0008 m2
DT 0.0001 sElvf 0.5 mm Hg/mLT 1. sTs 0.3 sTpwb 0.92 sTpww 0.09 sTr 0.28 sTs1 0.3 sTs2 0.45 sTtwb 0.22 sTtwe 0.42 sTtww 0.2 sXvad 0.11 mXr 0.0605 m
CARDIAC DYNAMICS WITH PULSATILE VAD 937
Artif Organs, Vol. 30, No. 12, 2006
![Page 10: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/10.jpg)
1–14, and particularly by Eqs. 1–4.) The LV volumevaries between 139 mL and 192 mL, greatly elevatedfrom the normal healthy range of 50–130 mL in thehealthy condition, and with a corresponding decreasein the difference between the minimum andmaximum volumes. (The ventricular maximum tominimum volume difference is slightly larger than theejected blood volume per heart beat, due to regur-
gitant flows in the valves. In the physiological casewith heart failure, the heart rate would increaseaccordingly to make up for lost volume pumped perbeat to maintain the total cardiac output required.)The left atrial volume is also increased, from thenormal range of 40–68 mL in the healthy condition,to the current range of 57–87 mL. These changessuggest that the ventricular volume difference has
(a)
(b)
(c)
(d)
(e)
(f)
FIG. 3. System response with cardiovascular model in healthy conditions. (a) Pressure, left heart; (b) flow rate, left heart; (c) volume, leftheart; (d) pressure, right heart; (e) flow rate, right heart; (f) volume, right heart.
Y. SHI AND T. KORAKIANITIS938
Artif Organs, Vol. 30, No. 12, 2006
![Page 11: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/11.jpg)
been reduced from the normal 80 mL to the currentvalue of 53 mL, with corresponding decrease incardiac output, while at the same time prominent leftheart dilation has developed.Accompanying the dila-tion in the left heart, there is great volume reductionin the right ventricle and atrium. These pathologicalchanges in the cardiovascular response need to beremedied by medical intervention.
Response with pulsatile left ventricular assist device(LVAD) support
To simulate the cardiovascular response in LVfailure condition with VAD support, the three VADmotion profiles described by Eqs. 17–19 are appliedto activate the reciprocating valve pump (LVAD) inthe numerical model. Figure 2a shows the threemotion profiles with the ECG signal as timing refer-
(a) (d)
(b) (e)
(c) (f)
FIG. 4. System response of cardiovascular model with left ventricular failure. (a) Pressure, left heart; (b) flow rate, left heart; (c) volume,left heart; (d) pressure, right heart; (e) flow rate, right heart; (f) volume, right heart.
CARDIAC DYNAMICS WITH PULSATILE VAD 939
Artif Organs, Vol. 30, No. 12, 2006
![Page 12: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/12.jpg)
ence, and Fig. 2b shows the corresponding velocitychanges associated with the three motion profiles.Figures 5–7 show the corresponding changes of pres-sure, flow rate, and volume with LV failure conditionassisted by the LVAD pumping action, operatedunder these three motion profiles. Figure 8 comparessome important physiological variables, including
pressures in the left atrium, left ventricle, systemicartery, pulmonary vein, etc., and the pressure-volumeloop under the conditions of healthy, LV failure, andLV failure assisted by LVAD. Figure 9a compares theideal power requirement of LVAD with differentmotion profiles, and Fig. 9b illustrates the corre-sponding estimated LV wall stress changes.
(a) (d)
(b) (e)
(c) (f)
FIG. 5. System response with left ventricular failure and sawtooth type left ventricular assist device motion. (a) Pressure, left heart; (b)flow rate, left heart; (c) volume, left heart; (d) pressure, right heart; (e) flow rate, right heart; (f) volume, right heart.
Y. SHI AND T. KORAKIANITIS940
Artif Organs, Vol. 30, No. 12, 2006
![Page 13: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/13.jpg)
Comparing Figs. 5–7 with Figs. 3 and 4 illustratesthat LVAD assistance greatly improves the cardiacfunction, and compensates the impaired cardiovas-cular response to almost match that in the normalhealthy condition. As shown in Figs. 5–7 parts (a)and (d), the systemic arterial pressure under LVADsupport with the three different motion profilesreturns to the normal range of 80–120 mm Hg, and
the pressures in the left atrium and the pulmonaryvein drop back to the normal value of about9 mm Hg. The greatly dilated left heart chambers inthe LV failure situation are satisfactorily remedied,as shown in part (c) of Figs. 5–7, and the compen-sated volume responses in the VAD assistance con-dition match that in the normal healthy condition ofFig. 3c. (Here, the computed volumes of the heart
(a) (d)
(b) (e)
(c) (f)
FIG. 6. System response with left ventricular failure and sine type left ventricular assist device motion. (a) Pressure, left heart; (b) flowrate, left heart; (c) volume, left heart; (d) pressure, right heart; (e) flow rate, right heart; (f) volume, right heart.
CARDIAC DYNAMICS WITH PULSATILE VAD 941
Artif Organs, Vol. 30, No. 12, 2006
![Page 14: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/14.jpg)
chambers in the model are affected by the com-bined effect of the equations in the numericalmodel, Eqs. 1–19, and particularly by Eqs. 1–4.) Theshape of the aortic flow-rate response in the LVADassist condition, as shown in parts (b) of Figs. 5–7,becomes smoother and is different from that ofFig. 3b in the healthy condition. Nevertheless, thevolume changes as discussed above suggest that thecardiac output is not impaired by the change in
aortic flow. Besides successful compensation ofpressure and volume response discussed above,other aspects of pressure, flow rate, and volumeresponse almost duplicate the native response in thehealthy condition. This suggests that under the threemotion profiles studied, from the theoretical pointof view, the reciprocating valve pump is a suitablechoice for LVAD support under the LV failurecondition.
(a)
(b)
(d)
(e)
(c) (f)
FIG. 7. System response with left ventricular failure and Hermitian type ventricular assist device motion. (a) Pressure, left heart; (b) flowrate, left heart; (c) volume, left heart; (d) pressure, right heart; (e) flow rate, right heart; (f) volume, right heart.
Y. SHI AND T. KORAKIANITIS942
Artif Organs, Vol. 30, No. 12, 2006
![Page 15: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/15.jpg)
To investigate the effect of different pumpingmotion profiles on the cardiovascular response, thecharacteristic variables of LVAD function are com-pared, as illustrated in Figs. 8 and 9. From Fig. 8a,e, itis observed that LVAD assistance with any of thethree motion profiles can bring the elevated left atrialand pulmonary vein pressures in LV failure back to
normal value of below 10 mm Hg. In terms of flowrates and volumes in the cardiovascular system, thedifference among the three LVAD motion profiles isminor. Among the three motion profiles, the Hermi-tian type motion induces the lowest peak LV pressure(Fig. 8b). LV failure causes the peak LV pressure todrop from the normal value of about 120 mm Hg to
(a) (d)
(b) (e)
(c) (f)
FIG. 8. Comparison of cardiovascular system response under various conditions. (a) Left atrial pressure; (b) left ventricular pressure; (c)pressure in ventricular assist device inlet; (d) pressure in systemic artery; (e) pressure in pulmonary vein; (f) pressure-volume loops.
CARDIAC DYNAMICS WITH PULSATILE VAD 943
Artif Organs, Vol. 30, No. 12, 2006
![Page 16: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/16.jpg)
68 mm Hg in the diseased condition. With LVADsupport the cardiac output is increased to normallevels, while the left ventricle is working at a reducedrate. Figure 8b illustrates that LV pressure canremain lower while the LVAD support maintainsarterial pressure to normal levels (Fig. 8d). Someclinical studies suggest that this opportunity to restmay assist the diseased ventricle to regenerate.Figure 8c illustrates that the pressure in the aorticroot (ventricular after-load), which is the same as thepressure at the inlet to the LVAD, is greatly reducedin the systolic phase, while it returns to normal levelsin the diastolic phase (the after-load in diastole helpscoronary perfusion). Among the three motion pro-files, the Hermitian type motion produces the lowestafter-load to the diseased ventricle in the systolicphase, and the after-load is reduced to about one-fourth of that in the healthy condition and about onehalf of that in the diseased condition. In terms ofventricular after-load, the Hermitian type motion ismore beneficial for the recovery of the diseasedventricle. The after-load returns to the normal valuein different stages of the diastolic phase, with thesawtooth type motion restoring the after-load theearliest, in early diastole. Thus, the sawtooth typeVAD motion is more helpful in promoting coronaryperfusion. From Fig. 8d it is observed that the appli-cation of LVAD generally restores the systemicartery pressure, from the much impaired value in theLV failure case, back to the normal range.Among thethree motion profiles, the Hermitian type motionproduced the smoothest pressure variation, and thesawtooth type motion causes the highest systemicartery pressure among the three. Figure 8f illustratesthe pressure-volume loops of the left ventricle underthe various conditions. The area enclosed inside the
pressure-volume loop is the work performed by theventricle. From this it is estimated that ventriclework, from maximum to minimum value, is for thehealthy state, diseased state, sawtooth, sine, and Her-mitian profiles, respectively. Figure 9 compares theLVAD ideal power requirement and the LV wallstress changes in a heart cycle under the differentconditions. The ideal LVAD power requirement isestimated from the power difference downstreamand upstream of the LVAD:
P P Q P Q= ⋅ − ⋅sas sas sat sat (20)
Figure 9a shows that generally the three motionprofiles require similar power input, and the meanpower requirements in all the three cases are esti-mated to be below 2 W. For most of the heart cyclethe instantaneous power requirement is below 1 Wfor all three motion profiles, while the sawtooth typemotion produces a peak power requirement of about4 W. The peak power requirement occurs immedi-ately before the QRS complex in the ECG wave; andoscillations in instantaneous power requirementoccur soon after the end of the T wave in the ECGsignal, both of which correspond to changes in thedirection of motion of the VAD. The Hermitian typemotion produces two peak power requirements inthe heart cycle, one (of about 1.6 W in amplitude)during the QRS complex, corresponding to thepumping phase of the VAD; and a second (of aboutthe same amplitude) corresponding to the retreatingmotion of the VAD. The sine type motion producesthe smoothest power requirement. Of course thispower requirement estimation is based purely onhemodynamic response, and this does not include the
(a) (b)
FIG. 9. Estimation of ventricular assist device (LVAD) characteristic variables. (a) Estimation of LVAD ideal power requirement; (b)estimation of left ventricular wall stress.
Y. SHI AND T. KORAKIANITIS944
Artif Organs, Vol. 30, No. 12, 2006
![Page 17: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/17.jpg)
effects of other important factors such as electromag-netic LVAD efficiency, driving mechanism efficiency,etc.
In Fig. 9b the LV wall stress is estimated based onLaplace’s theory for thin-wall shell structure (24).The left ventricle is assumed to be a near sphericalshell, thus, the wall stress is approximately:
θ =⋅
⋅ +( )P D
w w Dlv lv
2
lv4(21)
with the wall thickness to be w = 10 mm at peaksystole (2). The LV wall stress generally follows thesame trend as that of the LV pressure shown inFig. 8b. VAD assistance greatly reduces the wallstress in the diseased ventricle, thus is beneficial forthe ventricle recovery from the diseased condition.The Hermitian type motion produces the lowest wallstress, and the sine type motion the highest.
DISCUSSION
This article presents numerical models for thehuman cardiovascular system and for physiologicallypulsatile type VADs, and studies and compares thepredicted dynamic response of the human cardiovas-cular system under three conditions: healthy, LVfailure, and LV failure assisted by an LVAD. Thefocus of the article is on presenting the numericalmodel developed and predicting the hemodynamiccharacteristics of the interaction between the nativecardiovascular system and the VAD under represen-tative baseline conditions of healthy, diseased, anddiseased with VAD support. The cardiovascularmodel includes the four heart chambers and theiractivation, the systemic and pulmonary circulationloops, and improved models for the four native heartvalves (predicting regurgitant valve flow). The VADmodel includes a realistic description of the pulsatilepumping action and regurgitant flow generated by aprosthetic valve, which acts as a pumping piston, butis generic to all such pumping devices present in theliterature, as the model does not depend on the pow-ering or control mechanism for the VAD. Detailedconsideration of the VAD control and driving mecha-nism varies with different implementations, such asin the design of Larson et al. (15) (which uses anelectric-coil driving mechanism), and the designof Korakianitis and Grandia (16) (which uses amagnetic-hydraulic driving mechanism driven in turnby an electric coil in order to fit within the constraintsof the human body). In either case, the detailed VADpowering and control system are beyond the scope ofthe current work.
As shown in Fig. 3 the healthy cardiovascularsystem model accurately predicts left and right heartpressures, heart chamber volumes, and flow rates.For instance the LV pressure is between 80 and120 mm Hg, the mean flow rates through the mitralvalve is 5 L/min, corresponding to 0.17 m/s for valvesize of 25 mm. The improved valve model predictsregurgitant calve flows and pressure fluctuationsafter aortic and pulmonary valve closure. (The pres-sure fluctuations are present in both aortic and pul-monary valve closure, but they are more prominentlyshown on the pulmonary-side pressure plot as theoverall pressure is lower on the right heart.) Thevolumes of the four chambers of the heart are alsoaccurately predicted.
The diseased system response under the conditionof LV failure is shown in Fig. 4. This condition issimulated by a reduction in the maximum elastanceof the left ventricle. The numerical model again accu-rately predicts the reduction in pressures on theleft side of the heart, the increase in left heartvolumes, and the increased after-load on pulmonarycirculation.
Three different LVAD motion profiles (and corre-sponding pumping action profiles) are studied in thisarticle.The pumping action is effected by a prostheticvalve which is placed to replace a portion of theascending aorta. The fluid dynamic model for thisvalve is similar to the model used for the native heartvalves, and thus includes the effects of regurgitantflows. The displacement and velocity profiles of thepumping action are shown in Fig. 2. The response ofthe diseased system (LV failure) as aided by theLVAD is shown in Figs. 5–9.The results show that thereciprocating valve VAD satisfactorily supports thefailing heart by restoring important physiologicalvariables to their values under healthy normal con-ditions, such as pressures in the pulmonary vein andthe aorta, the volume of the diseased ventriclechamber, etc. This preliminary study shows that thereciprocating valve VAD needs an ideal power con-sumption of about 1 W, with peak values in the regionof 2–4 W. Although this power estimation did notconsider the VAD pumping efficiency, the prelimi-nary result is promising. Even if one takes intoconsideration electromagnetic and fluid dynamiclosses in the operation of the VAD, these levels ofpower consumption indicate that the reciprocatingprosthetic-valve type of pump has great potential inenergy conservation when compared with othermainstream pulsatile VADs currently in the market.
By comparing the results for the three motion pro-files, it is observed that Hermitian type VAD motionas proposed in the current article helps to reach mini-
CARDIAC DYNAMICS WITH PULSATILE VAD 945
Artif Organs, Vol. 30, No. 12, 2006
![Page 18: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/18.jpg)
mized ventricular wall stress, while the sine typeVAD motion helps to minimize the VAD powerrequirement. These two types of VAD motion alsohelp to minimize the ventricular work. Minimizingthe ventricular work in the diseased ventricle helpsto unload the chamber and promote its recoveryprocess in “bridge to recovery” applications.The saw-tooth type VAD motion produces slightly higherventricular wall stress and requires slightly more ven-tricular work, but at the same time it induces slightlyincreased arterial pressure in diastole, thus aidingcoronary perfusion. In this sense the sawtooth typeVAD motion assists the ventricular recovery processfrom another aspect. From these preliminary resultsit is hard to judge which motion profile is superior.There is evidence from the group of Papaioannouet al. (25) that the lower the aortic compliance, thegreater the performance of the intra-aortic balloonpumping. Also the detailed VAD driving and controlmechanism (electromagnetic, hydroelectromagnetic,etc.) will affect the VAD efficiency and VAD powerrequirement, thus the efficiencies of these differentimplementations of the reciprocating valve VADneed to be compared. For in-depth comparisons,further investigation of the system response undervarious conditions must be conducted, including dif-ferent pathological situations like heart rate changes,variation of aortic compliance and different serious-ness of heart failure. These are the subject of futureinvestigations.
The ongoing discussion of pulsatile/nonpulsatileperfusion has an enormous impact on VADdevelopment. Ündar (8) reviewed the publishedworks and concluded that pulsatile perfusion is indis-pensable for normal function of the end organs.Thus,in this article the action of a new design of prosthetic-valve type VAD on an improved cardiovascularmodel is presented and studied. This preliminarywork indicates that the powering requirement of theprosthetic-valve type of pulsatile VAD is promising,and that further research on these designs iswarranted. Several other researchers also worked onnumerical studies of the effect of pulsatile VADs onthe native cardiovascular system. Drzewiecki et al.(7) studied the effect of an atrio-aortic pneumaticallydriven VAD on the native cardiovascular system.Both the systemic and the pulmonary loops wereincluded in the cardiovascular model, which was usedto evaluate the system response of mean aortic pres-sure, LV oxygen consumption, and stroke volumechanges with different time delay in VAD motiontiming. Barnea et al. (12) analyzed the effect of theintra-aortic balloon pump VAD on a complete car-diovascular model, and studied the changing of infla-
tion and deflation times on the various cardiovascularparameters of cardiac oxygen availability and con-sumption, mean diastolic pressure, peak systolic pres-sure, etc. Verkerke et al. (9) presented a combinedmodel of the cardiovascular system that includes thesystemic circulation, coronary circulation, and a pul-satile catheter type VAD. The model was used tosimulate the changes of LV and aortic pressures, andcoronary flow under three conditions of healthy,heart infarction, and heart infarction with VADassist. De Lazzari et al. (11) constructed a combinedmodel of a pneumatic LVAD and an open-loopcircuit description of the systemic circulation, andevaluated the changes of cardiac flow, pressure-volume area and cardiac mechanical efficiency withdifferent atrial and arterial pressures in the open-loop circuit. These previous studies concentrated onthe analysis of the VAD effect and optimization ofVAD motion, and the numerical models used werenot the focus of the work presented. As a contrast inthe present article the emphasis is on the presenta-tion of the improved cardiovascular model and theintroduction of the model for the new type of VAD.In-depth analysis of VAD performance and VADmotion optimization will be the topic of the nextstage of the work presented in this article.
Previous experimental studies of pulsatile VADperformance (such as [14]) have revealed that thetiming in the pulsatile VAD motion has direct influ-ence on VAD efficiency. In these studies the heartvalve opening and closure were often used as refer-ence instances for VAD motion design. Nevertheless,even in those studies with complete cardiovascularsystem models (3,7,11–13), the important feature ofdetailed heart valve dynamics was not considered. Inthese earlier studies the heart valves were mostlydescribed as an on/off diode combined with a resis-tance component. Such heart valve models neglectthe valve motion processes and therefore produceinaccurate valve motion sequences. For pulsatile typeVADs, the valve motion is crucial to the effectivenessof the motion profile designs, and thus to the VADoptimization process. The current article presents animproved numerical model, which includes the com-plete cardiovascular model and also detailed descrip-tion of the heart valve dynamics, providing a betterplatform for numerical study of pulsatile type VADperformance. In addition, the present model can becoupled with more-elaborate models of local circula-tions (renal, cerebral, etc.).
CONCLUSIONS
This article introduces numerical models for thehuman cardiovascular system and for prosthetic-
Y. SHI AND T. KORAKIANITIS946
Artif Organs, Vol. 30, No. 12, 2006
![Page 19: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/19.jpg)
valve pulsatile type VADs. Detailed heart valvedynamics were considered in the modeling process,which helps to improve the accuracy of simulation instudying the pulsatile type VAD designs. The articlealso compares the predicted dynamic response of thehuman cardiovascular system under three conditions:healthy, LV failure, and LV failure assisted by aprosthetic-valve pulsatile LVAD, under three differ-ent motion profiles.The three motion profiles studiedare sawtooth, sine, and Hermitian. With the LVADsupport, the impaired cardiovascular response in theLV failure condition is successfully compensated, andthe after-load of the diseased ventricle and of thepulmonary-side circulation are greatly reduced, thushelping the recovery of the ventricle from the dis-eased condition. It is found that the Hermitian typepumping motion has the advantage of requiringminimum power, and produces the minimum after-load, ventricular wall stress, and ventricular work tothe diseased ventricle. The sawtooth type pumpingmotion needs slightly more power input, but inducesslightly increased artery pressure in diastole, thusimproving coronary perfusion.
NomenclatureA = sectional areaC = complianceCQ = flow coefficientDT = time stepE, e = elastanceI = inertial moment of rotatingK, k = coefficientL = inertanceM = massP = pressureQ = flow rateR = resistanceT = time; heart periodV = volume, velocityX = stroke, displacementw = wall thicknessq = rotating angle of valve leaflet, ventricular wallstress
Subscripts0 = initial value; offset value; value for unstressedconditionao = aortic valved = diastolic phasee = elastance actionea = elastance of atriumev = elastance of ventriclef = frictional actionla = left atrium
lv = left ventriclelvf = left ventricular failuremax = maximum valuemin = minimum valuemi = mitral valvep = effect of pressure forcepar = pulmonary arteriolespas = pulmonary artery sinuspat = pulmonary arterypcp = pulmonary capillarypo = pulmonary valvepvn = pulmonary veinpwb = beginning of P wavepww = duration of P waver = a specified intermediate instant in early systolera = right atriumrv = right ventricles = systolic phases1 = peak of systolic phases2 = end of systolic phasesar = systemic arteriolessas = systemic aortic sinussat = systemic arteryscp = systemic capillarysvn = systemic veinti = tricuspid valvetwb = beginning of T wavetwe = end of T wavetww = duration of T wavevad = ventricular assist device
REFERENCES
1. Reul HM, Akdis M. Blood pumps for circulation support.Perfusion 2000;15:295–311.
2. Vandenberghe S, Segers P, Meyns B, Verdonck P. Unloadingeffect of a rotary blood pump assessed by mathematicalmodeling. Artif Organs 2003;27:1094–101.
3. Pekkan K, Frakes D, de Zelicourt D, Lucas CW, Parks WJ,Yoganathan AP. Coupling pediatric ventricle assist devices tothe fontan circulation: simulation with a lumped-parametermodel. ASAIO J 2005;51:618–28.
4. Saito S, Westaby S, Piggot D, et al. End-organ function duringchronic nonpulsatile circulation. Ann Thorac Surg 2002;74:1080–5.
5. Chow G, Roberts IG, Edwards AD, et al. The relation betweenpump flow rate and pulsatility on cerebral hemodynamicsduring pediatric cardiopulmonary bypass. J Thorac CardiovascSurg 1997;114:568–77.
6. Sezai A, Shiono M, Orime Y, et al. Major organ function undermechanical support: comparative studies of pulsatile and non-pulsatile circulation. Artif Organs 1999;23:280–5.
7. Drzewiecki GM, Pilla J, Welkowitz W. Design and controlof the atrio-aortic left ventricular assist device based on o2
consumption. IEEE Trans Biomed Eng 1990;37:128–37.8. Ündar A. Myths and truths of pulsatile and nonpulsatile per-
fusion during acute and chronic cardisc support. Artif Organs2004;28:439–43.
9. Verkerke GJ, Geertsema AA, Mihaylov D, Blanksma PK,Rakhorst G. Numerical simulation of the influence of a left
CARDIAC DYNAMICS WITH PULSATILE VAD 947
Artif Organs, Vol. 30, No. 12, 2006
![Page 20: [60]](https://reader034.pdfslide.us/reader034/viewer/2022051821/55cf8582550346484b8ec805/html5/thumbnails/20.jpg)
ventricular assist device on the cardiovascular system. Int JArtif Organs 2000;23:765–73.
10. Nitta S, Yoshizawa M, Yambe T, Tanaka M, Takeda H. A lessinvasive emax estimation method for weaning from cardiacassistance. IEEE Trans Biomed Eng 1995;42:1165–73.
11. De Lazzari C, Mimmo FR, Tosti G, Ambrosi D. A desk-topcomputer model of the circulatory system for heart assistancesimulation: effect of an LVAD on energetic relationshipsinside the left ventricle. Med Eng Phys 1994;16:97–103.
12. Barnea O, Moore TW, Dubin S, Jaron D. Cardiac energy con-siderations during intraaortic balloon pumping. IEEE TransBiomed Eng 1990;17:170–81.
13. Vollkron M, Shima H, Huber L, Wieselthaler G. Interaction ofthe cardiovascular system with an implanted rotary assistdevice: simulation study with a refined computer model. ArtifOrgans 2002;26:349–59.
14. Barnea O, Smith BT, Dubin S, Moore TW, Jaron D. Optimalcontroller for intraaortic balloon pumping. IEEE TransBiomed Eng 1992;39:629–34.
15. Larson CO, Smith JS, Chapman JH, et al. Reciprocatingpumps and linear motor arrangement. Patent No.: US5,879,375, United States Patent, March 9 1999.
16. Korakianitis T, Grandia L. Optimized pulsatile flow ventricu-lar assistance device and total artificial heart. Patent No.: US6,632,169, United States Patent, October 14, 2003.
17. Suga H, Sagawa K, Shoukas AA. Load independence of theinstantaneous pressure-volume ratio of the canine left ven-
tricle and effects of epinephrine and heart rate on the ratio.Circ Res 1973;XXXII:314–22.
18. De Hart J, Paters GWM, Schreurs PJG, Baaijens FPT. Athree-dimensional computational analysis of fluid–structureinteraction in the aortic valve. J Biomech 2003;36:103–12.
19. Shi YB, Zhao Y, Yeo JH, Hwang NHC. Numerical simulationof opening process in a bileaflet mechanical heart valve underpulsatile flow condition. J Heart Valve Dis 2003;12:245–56.
20. Bellhouse BJ. The fluid mechanics of heart valves. In: BergelDH, eds, Cardiovascular Fluid Dynamics, Vol. 1, Chapter 8.London: Academic Press, 1972;261–85.
21. Ursino M. A mathematical model of the carotid baroregula-tion in pulsating conditions. IEEE Trans Biomed Eng 1999;46:382–92.
22. Lu K, Clark JW, GhorBel FH, Ware DL, Bidani A. A humancardiopulmonary system model applied to the analysis of thevalsalva maneuver. Am J Physiol (Heart Circ Physiol) 2001;281:H2661–79.
23. Guyton AC. Textbook of Medical Physiology. Philadelphia:W.B. Saunders Company, 1986.
24. Fung YC. Biodynamics: Circulation. New York: Springer-Verlag, 1984.
25. Papaioannou TG, Mathioulakis DS, Stamatelopoulos KS, et al.New aspects on the role of blood pressure and arterial stiffnessin mechanical assistance by intra-aortic balloon pump: in-vitrodata and their application in clinical practice. Artif Organs2004;28:717–27.
Y. SHI AND T. KORAKIANITIS948
Artif Organs, Vol. 30, No. 12, 2006