Embed Size (px)
Citation preview
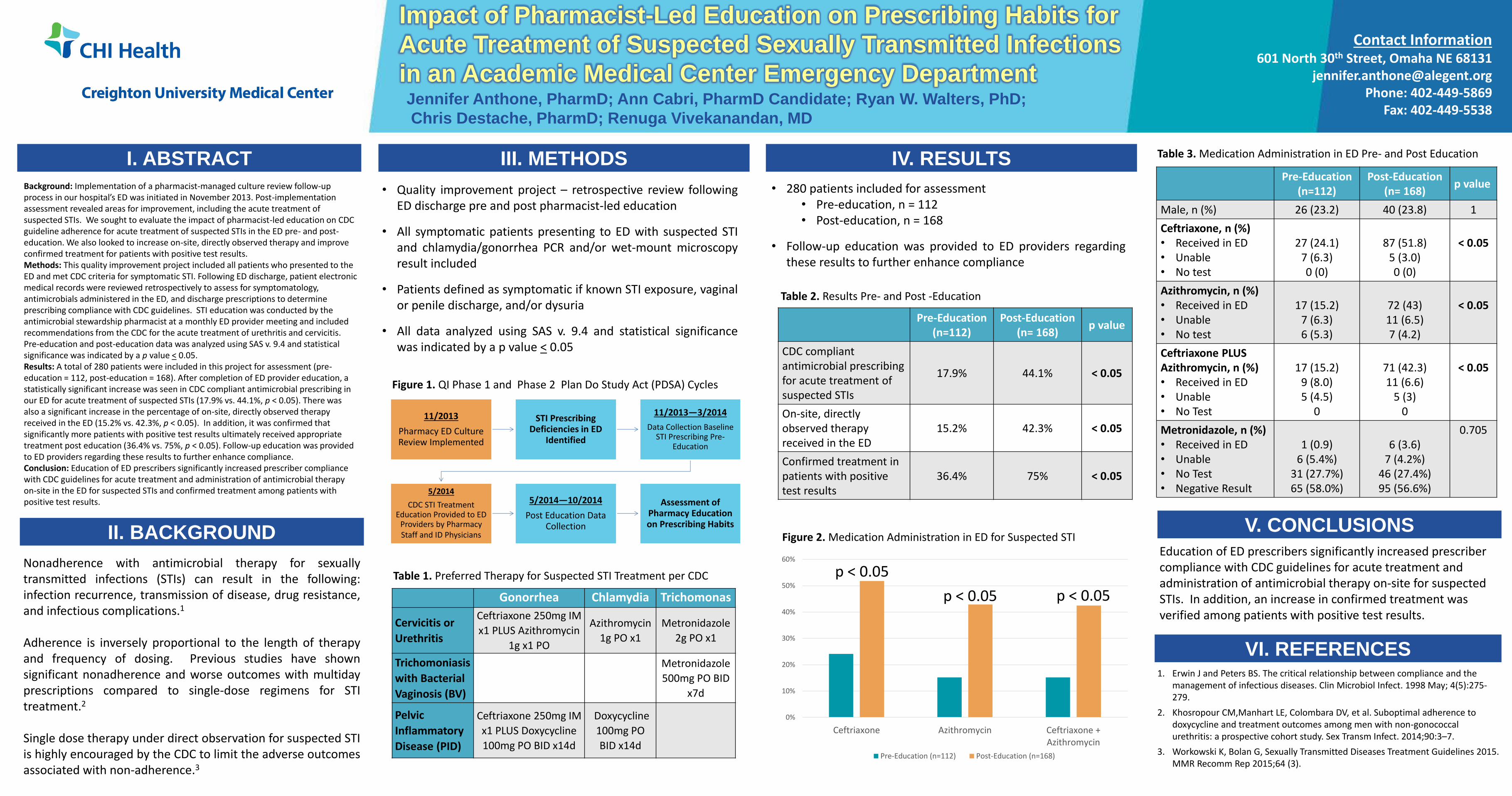
Impact of Pharmacist-Led Education on Prescribing Habits for
Acute Treatment of Suspected Sexually Transmitted Infections
in an Academic Medical Center Emergency Department
I. ABSTRACT
Jennifer Anthone, PharmD; Ann Cabri, PharmD Candidate; Ryan W. Walters, PhD;
Chris Destache, PharmD; Renuga Vivekanandan, MD
III. METHODS
V. CONCLUSIONS
Education of ED prescribers significantly increased prescriber compliance with CDC guidelines for acute treatment and administration of antimicrobial therapy on-site for suspected STIs. In addition, an increase in confirmed treatment was verified among patients with positive test results.
IV. RESULTS
• Quality improvement project – retrospective review following ED discharge pre and post pharmacist-led education
• All symptomatic patients presenting to ED with suspected STI and chlamydia/gonorrhea PCR and/or wet-mount microscopy result included
• Patients defined as symptomatic if known STI exposure, vaginal or penile discharge, and/or dysuria
• All data analyzed using SAS v. 9.4 and statistical significance was indicated by a p value < 0.05
Nonadherence with antimicrobial therapy for sexually transmitted infections (STIs) can result in the following: infection recurrence, transmission of disease, drug resistance, and infectious complications.1 Adherence is inversely proportional to the length of therapy and frequency of dosing. Previous studies have shown significant nonadherence and worse outcomes with multiday prescriptions compared to single-dose regimens for STI treatment.2 Single dose therapy under direct observation for suspected STI is highly encouraged by the CDC to limit the adverse outcomes associated with non-adherence.3
• 280 patients included for assessment • Pre-education, n = 112 • Post-education, n = 168
• Follow-up education was provided to ED providers regarding these results to further enhance compliance
0%
10%
20%
30%
40%
50%
60%
Ceftriaxone Azithromycin Ceftriaxone +Azithromycin
Pre-Education (n=112) Post-Education (n=168)
VI. REFERENCES 1. Erwin J and Peters BS. The critical relationship between compliance and the
management of infectious diseases. Clin Microbiol Infect. 1998 May; 4(5):275-279.
2. Khosropour CM,Manhart LE, Colombara DV, et al. Suboptimal adherence to doxycycline and treatment outcomes among men with non-gonococcal urethritis: a prospective cohort study. Sex Transm Infect. 2014;90:3–7.
3. Workowski K, Bolan G, Sexually Transmitted Diseases Treatment Guidelines 2015. MMR Recomm Rep 2015;64 (3).
Table 1. Preferred Therapy for Suspected STI Treatment per CDC
Figure 2. Medication Administration in ED for Suspected STI
Pre-Education (n=112)
Post-Education (n= 168)
p value
Male, n (%) 26 (23.2) 40 (23.8) 1
Ceftriaxone, n (%) • Received in ED • Unable • No test
27 (24.1)
7 (6.3) 0 (0)
87 (51.8)
5 (3.0) 0 (0)
< 0.05
Azithromycin, n (%) • Received in ED • Unable • No test
17 (15.2)
7 (6.3) 6 (5.3)
72 (43) 11 (6.5) 7 (4.2)
< 0.05
Ceftriaxone PLUS Azithromycin, n (%) • Received in ED • Unable • No Test
17 (15.2)
9 (8.0) 5 (4.5)
0
71 (42.3) 11 (6.6)
5 (3) 0
< 0.05
Metronidazole, n (%) • Received in ED • Unable • No Test • Negative Result
1 (0.9)
6 (5.4%) 31 (27.7%) 65 (58.0%)
6 (3.6)
7 (4.2%) 46 (27.4%) 95 (56.6%)
0.705
Table 3. Medication Administration in ED Pre- and Post Education
Gonorrhea Chlamydia Trichomonas
Cervicitis or
Urethritis
Ceftriaxone 250mg IM
x1 PLUS Azithromycin
1g x1 PO
Azithromycin
1g PO x1
Metronidazole
2g PO x1
Trichomoniasis
with Bacterial
Vaginosis (BV)
Metronidazole
500mg PO BID
x7d
Pelvic
Inflammatory
Disease (PID)
Ceftriaxone 250mg IM
x1 PLUS Doxycycline
100mg PO BID x14d
Doxycycline
100mg PO
BID x14d
II. BACKGROUND
Contact Information 601 North 30th Street, Omaha NE 68131
[email protected] Phone: 402-449-5869
Fax: 402-449-5538
Background: Implementation of a pharmacist-managed culture review follow-up process in our hospital’s ED was initiated in November 2013. Post-implementation assessment revealed areas for improvement, including the acute treatment of suspected STIs. We sought to evaluate the impact of pharmacist-led education on CDC guideline adherence for acute treatment of suspected STIs in the ED pre- and post-education. We also looked to increase on-site, directly observed therapy and improve confirmed treatment for patients with positive test results. Methods: This quality improvement project included all patients who presented to the ED and met CDC criteria for symptomatic STI. Following ED discharge, patient electronic medical records were reviewed retrospectively to assess for symptomatology, antimicrobials administered in the ED, and discharge prescriptions to determine prescribing compliance with CDC guidelines. STI education was conducted by the antimicrobial stewardship pharmacist at a monthly ED provider meeting and included recommendations from the CDC for the acute treatment of urethritis and cervicitis. Pre-education and post-education data was analyzed using SAS v. 9.4 and statistical significance was indicated by a p value < 0.05. Results: A total of 280 patients were included in this project for assessment (pre-education = 112, post-education = 168). After completion of ED provider education, a statistically significant increase was seen in CDC compliant antimicrobial prescribing in our ED for acute treatment of suspected STIs (17.9% vs. 44.1%, p < 0.05). There was also a significant increase in the percentage of on-site, directly observed therapy received in the ED (15.2% vs. 42.3%, p < 0.05). In addition, it was confirmed that significantly more patients with positive test results ultimately received appropriate treatment post education (36.4% vs. 75%, p < 0.05). Follow-up education was provided to ED providers regarding these results to further enhance compliance. Conclusion: Education of ED prescribers significantly increased prescriber compliance with CDC guidelines for acute treatment and administration of antimicrobial therapy on-site in the ED for suspected STIs and confirmed treatment among patients with positive test results.
p < 0.05
p < 0.05 p < 0.05
11/2013
Pharmacy ED Culture Review Implemented
STI Prescribing Deficiencies in ED
Identified
11/2013—3/2014
Data Collection Baseline STI Prescribing Pre-
Education
5/2014
CDC STI Treatment Education Provided to ED
Providers by Pharmacy Staff and ID Physicians
5/2014—10/2014
Post Education Data Collection
Assessment of Pharmacy Education on Prescribing Habits
Figure 1. QI Phase 1 and Phase 2 Plan Do Study Act (PDSA) Cycles
Pre-Education (n=112)
Post-Education (n= 168)
p value
CDC compliant antimicrobial prescribing for acute treatment of suspected STIs
17.9% 44.1% < 0.05
On-site, directly observed therapy received in the ED
15.2% 42.3% < 0.05
Confirmed treatment in patients with positive test results
36.4% 75% < 0.05
Table 2. Results Pre- and Post -Education
























![The Omaha Daily Bee. (Omaha, Nebraska) 1892-01-31 [p ]](https://img.pdfslide.us/doc/110x75/6194539d541cf57de7039baf/the-omaha-daily-bee-omaha-nebraska-1892-01-31-p-.jpg)


