Embed Size (px)
Citation preview

6th GCC Primary Health Care Conference Riyadh
Kingdom of Saudi Arabia 05 June 2007
The Effectiveness of Primary Care
Elizabeth A. Dubois Associate Director of Public Health / Health Economist
Wandsworth Teaching PCT, London, UK

Content…
• Priorities for Primary Care • Effectiveness of Primary Care• Evaluation• Conclusion

3
Priorities for Primary Care
1. Prioritise Expenditure
2. Control Substitution
3. Responsiveness to Population & Accountability
4. Ability to Deliver
5. Roles of PC Team
6. Diversity & Quality
7. Demand Management
8. Education & Training in PC
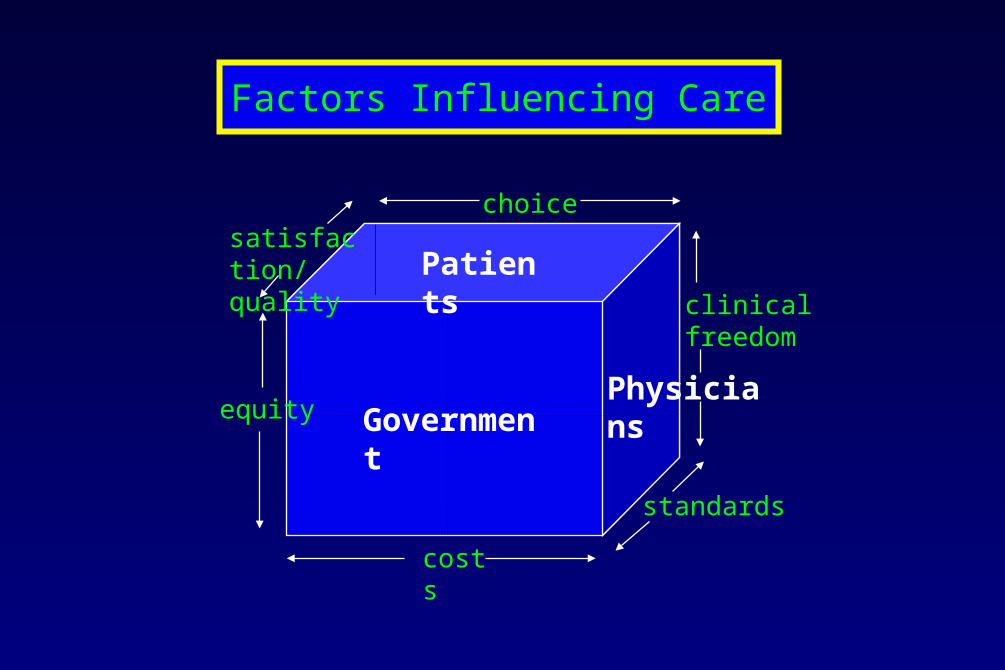
Factors Influencing Care
Government
Patients
Physicians
choicesatisfaction/quality
equity
costs
standards
clinical freedom
5
Prioritise Expenditure
• Agree responsibility for prioritising:
– Services
– Service spend
• Budget holding – powerful tool of change
• Professionals responsible for resource allocation
• Micro-level service development

6
Facts…..
Cost-Effectiveness (Intervention cost/case):
• Telephone Call £16
• Primary Care £15
• GP with Special Interest £55
• Outpatient £150
• Day Surgery £500
• Inpatient (2ndary Care) £5000
7
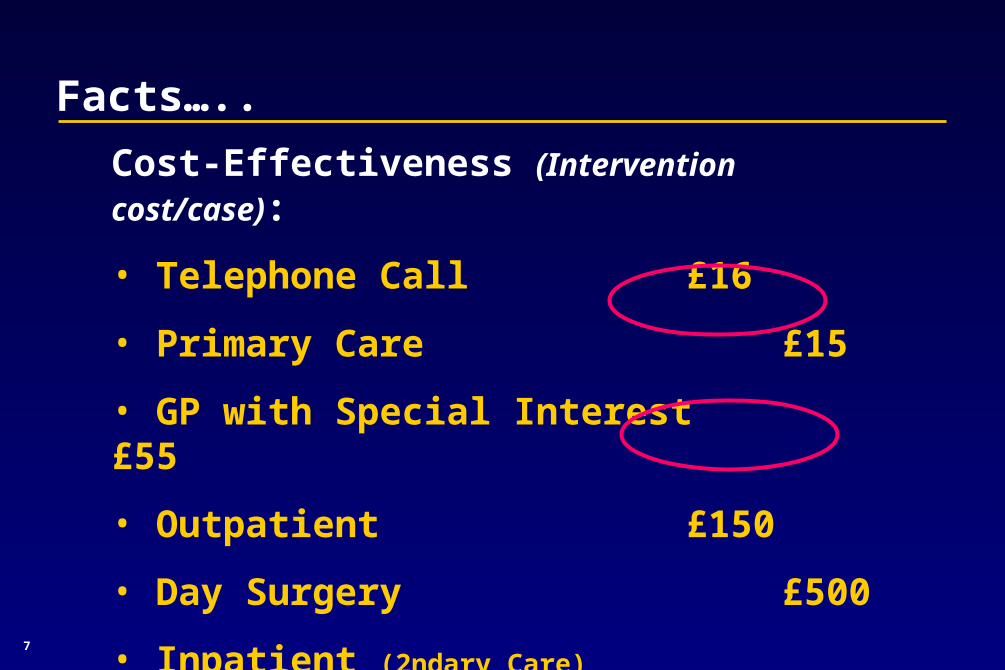
Facts…..
Cost-Effectiveness (Intervention cost/case):
• Telephone Call £16
• Primary Care £15
• GP with Special Interest £55
• Outpatient £150
• Day Surgery £500
• Inpatient (2ndary Care) £5000

8
Control Substitution
• Shift work from secondary care to primary care
• Define primary and community care in its own right, not a residual
• Vehicle of change rather than the receiver of it

9
Responsiveness to Population & Accountability
• Define core population need
– Health needs assessments
– Comparative audits
• Accountability to patients
• Accountability to the managers
• Accountability to the profession

10
Ability to Deliver
• Commitment of resources
• Development of leaders
• Teambuilding
• Training in resource management
• Training in public health tasks
• No hierarchy → matrix organisation
• Right people, right skills, right time

11
Roles of PC Team
• Re-examination of the role of the GP
• GPs cannot control and do all key tasks
• Re-examine the professional & clinical roles of:– Manager
– Nurse
– Pharmacist
– Psychologists
• Link public service values + private sector initiatives

12

13
Diversity & Quality
• Grow your own vision• Build upon skills and motivation• Develop new roles• Encourage innovative partnerships (voluntary sector, private
sector, community, academic departments)• Addressing poor quality; monitor through:
• Organisational development• Investment• Audit• Performance monitoring • Professional assessment• Retraining

14
Managing Demand
• One, if not the, most critical elements
• In the absence of DM, service development is irresponsible
• Increased demand due to:
– Consumer expectations
– Patient mobility
– Increasing complex problems
– Ageing population
– Advances in drugs & technology
• Address capacity issues innovatively & responsively
• Prevents service inadequacies

15
Suggestions for Demand Management
• Patient education initiatives
• Non-doctors doing medical role
• Training GPs in risk management
• Training in teamwork development
• Audit of referrals / consultations w/ peers
• Timely patient information (minorities, new patients)
• Use volunteers and/or carers
• Control through monitoring & policy

16
Education & Training in PC
What are we doing now? What do we want to be doing…and how shall we get there?
• Skilling
• Teambuilding
• Monitoring
• Training & development

Quality Integration
Choice
Costs
Change Organisational Behaviours
Change Physicians’ Behaviours
18
Evaluation of Effectiveness in Primary Care
• Explicit responsibility for decision making– Baseline measures specific to time and place
– Consider objectives of stakeholders
• Better partnerships with other organisations– Community
– Social services
– Psychiatry
– Geriatrics
– Voluntary
– Private

19
Evaluation of Effectiveness in Primary Care
• Value for money– *Key issue– Compare transaction costs– Measure need & patient outcome (but v. difficult)
• Responses to population need• Accountability to management & patient• Efficient provision of appropriate care• Evidence-based interventions• Management of demand• Equity of health care delivery• Sustainability and stability of systems• Staff retention & recruitment

20
Conclusion
• Colossal agenda but real opportunity• Focus on ‘appropriateness’ to estb. good practice
– Effectiveness of interventions– Efficiency– Patient acceptability– Clinical experience– Right people, right skills, right time
• Public Health skills crucial• Managerial experience crucial• User input crucial • Clear responsibilities, particularly budgetary• Clear objectives• Robust evaluation• Sense of mutual respect for all professions working in primary and community care

21

22
References
• Carruthers I. (1994) Total fundholding in the mainstream of the NHS. Primary Care Management. 4: 7-9.
• Fry J, Light D and Rodnick J. (1995) Reviving Primary Care: a US – UK comparison. 118-40. Radcliffe Medical Press, Oxford.
• Littlejohns P, Victor C. (1996) Making Sense of a Primary Care-led Health Service.14-28. Radcliffe Medical Press, Oxford.
• Starfield B. (1992) Primary Care: concept, evaluation and policy. Oxford University Press, New York.

23
Shukran JazeelanShukran Jazeelan
Elizabeth A. DuboisElizabeth A. DuboisWandsworth Teaching PCT, LondonWandsworth Teaching PCT, London





























