Embed Size (px)
Citation preview

Poster Session IV Operative Obstetrics, Clinical Obstetrics, Intrapartum, Medical-Surgical www.AJOG.org
CONCLUSION: Counselling to women prior to ECV should address thelikelihood of success based on the predicting factors described above,as well as the increased risk for operative vaginal delivery in the caseof successful ECV.
584
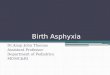
Prediction of birth asphyxia in term neonatesSabine Ensing1, Anita Ravelli2, Ben Willem Mol1,Ameen Abu-Hanna21Academic Medical Center, Obstetrics & Gynecology, Amsterdam,Netherlands, 2Academic Medical Center, Medical Informatics, Amsterdam,NetherlandsOBJECTIVE: To develop and internally validate a prognostic model forpredicting perinatal asphyxia at birth among term infants.STUDY DESIGN: We studied 1,606,493 women with a living fetus atstart of labor who attempted vaginal delivery with singleton termpregnancies in cephalic presentation without congenital anomalies.Data for the years between 1999 and 2010 were extracted from thenationwide perinatal registry in the Netherlands. To assess the risk ofbirth asphyxia (5 minute Apgar score < 7) we developed a multiplelogistic regression model for nulliparous (model 1) and multiparous(model 2) women. We used bootstrapping techniques to internallyvalidate our models. Predictive performance was assessed bydiscrimination (area under the receiver operating characteristic(AUC)) and calibration (calibration graphs).RESULTS: Birth asphyxia occurred in 1.2% among nulliparous and0.59% among multiparous women. Major antepartum predictors ofa 5 minute Apgar score < 7 were increased maternal age, non-Western ethnicity, low socio-economic status, hypertensive disease,increased gestational age, birth weight below 5th percentile and birthweight above 95th percentile. For multiparous women previous ce-sarean section was also considered. Intrapartum predictors wereinduction of labor, prolonged rupture of membranes, meconiumstained amniotic fluid and epidural anaesthesia. The AUC of thenulliparous and multiparous models were 0.64 (95%CI .0.63 - 0.65)and 0.66 (95%CI 0.65- 0.68). Calibration was reasonable for bothmodels, but showed structural overprediction at higher values ofpredicted probabilities.CONCLUSION: In Dutch women with a singleton term pregnancy weidentified antepartum and intrapartum characteristics that can assistin predicting birth asphyxia in attempted vaginal deliveries. Thismodel is a first step towards early prediction of birth asphyxia andrequires external validation before possible use in obstetric clinicalmanagement.
S288 American Journal of Obstetrics & Gynecology Supplement to JANUARY
Multivariable associations for model 1(nulliparous) and model 2 (multiparous)
*SES: socio-economic status.
585
Pregnancy complications for di-chorionic tri-amniotictriplets: markedly increased over tri-chorionic and reducedcasesSuzanne Peeters1, Mark Evans2, Femke Slaghekke1,Frans Klumper1, Johanna Middeldorp1, Enrico Lopriore3,Dick Oepkes11Leiden University Medical Center, Obstetrics, Leiden, Netherlands, 2MountSinai School of Medicine, Comprehensive Genetics, New York, NY, 3LeidenUniversity Medical Center, Pediatrics, Leiden, NetherlandsOBJECTIVE: To evaluate perinatal outcome by chorionicity in tripletpregnancies evaluated before the onset of pathophysiology.STUDY DESIGN: Retrospective analysis of prospectively collected dataon triplet pregnancies initially evaluated before 16 weeks in singleexperienced fetal therapy center from 2002 - 2012. Excluding mono-amniotic pairs, we evaluated prenatal interventions, pregnancycomplications, and perinatal outcome by chorionicity (mono-chorionic triamniotic (MCTA), dichorionic triamniotic (DCTA),trichorionic triamniotic (TCTA)) in Leiden, The Netherlands.RESULTS: Pregnancy outcomes by chorionicity are presented in Table 1.CONCLUSION: The 55% TTTS, 23% selective IUGR, and 14% IUFDrates demonstrate DCTA twins are at much higher risk than TCTA.Our data suggest that the MC pair in DCTA significantly increasesthe risks far beyond those of TCTA, and optimal statistics (New Yorkdata not shown) are achieved with FR to singletons.
2014



![Resp Failure in Neonates 072916 [Read-Only] Resp...• Etiology/physiology – Chronic asphyxia – Surfactant dysfunction –toxic pneumonitis – Air trapping • Treatment](https://img.pdfslide.us/doc/110x75/5b1f0c387f8b9a901f8c4976/resp-failure-in-neonates-072916-read-only-resp-etiologyphysiology-chronic.jpg)

![Acute Kidney Injury in Asphyxiated neonates admitted into a ......with perinatal asphyxia. Perinatal Asphyxia ranks as the second most important cause of neonatal death[1]. Major risk](https://img.pdfslide.us/doc/110x75/61110be6b93f5b0fcd11cc91/acute-kidney-injury-in-asphyxiated-neonates-admitted-into-a-with-perinatal.jpg)