Embed Size (px)
Citation preview

A Computer Model of the Human
Cardio-Respiratory Control System
including Acid-Base Equilibrium
L. Chiari, G. Avanzolini, M. Ursino
D. E. L S. University of Bologna,
Viale Risorgimento 2, 40136 Bologna, Italy
E-Mail: lchiari@deis. unibo. it
Abstract
A non-linear dynamical model of the human cardio-respiratory control and of acid-baseregulation oriented to clinical applications is presented. The model incorporates therespiratory, cardiovascular and body fluids buffer systems. The respiratory system inte-grates three controlled compartments, i.e., the lung, body tissue and brain tissue, anda controller which adjusts alveolar ventilation in response to chemical perturbations de-tected by two groups of chemoreceptors: the central ones, which are sensitive to CO%pressure changes in the medulla, and the peripheral ones, which respond to changesin arterial C02 and 02 pressure. The cardiovascular system includes a simple bicorn-partmental model of the systemic circulation that allows systemic arterial pressure andvenous return to be computed. Cardiac output depends on heart rate and on rightat rial pressure according to the Starling law. Two different mechanisms act on cardio-vascular dynamics: the barorefiex control system which modulates heart rate, systemicarterial resistance and venous unstressed volume in response to pressure perturbationsand a local chemical control which adjusts blood flow in presence of changes in arterialblood O] and CO% The body fluids buffer system is described by a new realistic CO2dissociation curve, based on a two-buffer model of acid-base equilibrium. In addition,other relevant physiological factors are incorporated, such as buffer base, the Haldaneeffect on blood C02 saturation, and the Bohr effect on blood oxygen saturation. Inthis work, the model is validated simulating the ventilatory, cardiovascular and chemicalresponses to acute hypoxia during normocapnia. The results obtained agree with thosefound in the clinical and physiological literature rather well regarding the patterns of themain cardio-respiratory quantities. The model can be used as a support for the analysisof many clinical problems associated with acid-base perturbations, such as metabolicdisorders, lung diseases, hemodialysis, and post-cardiosurgical care.
Transactions on Biomedicine and Health vol 4, © 1997 WIT Press, www.witpress.com, ISSN 1743-3525

58 Simulations in Biomedicine IV
1 Introduction
The cardiovascular and respiratory control systems interact in complexways in the organism. Changes in ventilation affect the cardiovascular re-sponse by changing the composition of body fluids. It is well known thathypoxia and hypercapnia are powerful vasodilators of many peripheral va-scular beds, including those of the brain, of the heart and muscles. Massivevasodilation in these organs may induce arterial hypotension, triggeringthe regulatory response of the baroreflex control system and activating thechcmoreccptor system, which may induce additional reflex vasoconstric-tion and increases in heart rate.
On the other hand, cardiovascular alterations significantly modulatethe control of ventilation through changes in cardiac output and cere-bral blood flow, which influence C02 washout and oxygen supply to tis-sues. Ultimately, the controls of ventilation, blood flow and pressure mustwork concurrently with coordinated adjustments to fulfil metabolic requi-rements and ensure acid-base equilibrium and cardio-respiratory stability.Several clinical and/or pathophysiological conditions are seriously concer-ned with a dysfunction in such a complex regulatory system. Amongthe others, mention can be made to asphyxia, metabolic disorders, lungdiseases, and to metabolic and hemodynamic changes occurring duringhemodialysis or in cardio-surgical Intensive Care.
A broad understanding of the entire control system previously descri-bed should take into account at least three differently organized sub-systems, i.e., the respiratory, cardiovascular and body fluids buffer systems,together with their complex relationships. Nevertheless, these systems arefrequently treated separately in the literature, arid insufficient emphasis isgiven to their mutual links. Even though several models of each of themhave been presented in previous years, incorporating different levels ofphysiological detail, to our knowledge a comprehensive quantitative studywhich combine all these aspects together is still lacking.
Aim of this work is to present the main features of a mathematical mo-del which includes control of ventilation, cardiovascular regulation (bothchemical arid baroreflex-rnecliated) arid acid-base equilibrium. The paperis structured as follows. First, the characteristics of the model are brieflyoutlined in qualitative terms, laying particular emphasis on the relation-ships between hemo dynamic, chemical and respiratory quantities. Then,the model is used to simulate the ventilatory and cardiovascular responseto acute hypoxia, and the consequent recovery when normoxia is restored.Finally, the main results are commented, and lines for future investigationspointed out.
2 Model formulation
The block diagram of Fig.l sketches out the general set-up of the modelwhich is proposed as an integrated approach to cardio-respiratory control.
Transactions on Biomedicine and Health vol 4, © 1997 WIT Press, www.witpress.com, ISSN 1743-3525

Simulations in Biomedicine IV 59
|y
e
fin~
^ /Cardiovascular *y
n /,.,.. "riam n^ ja
Pr«
RespiratoryPlant
/~» » • iCardiovascular/~i 11Controller
n
/
/
^^^
^
)a, )2
^
RespiratoryController
Psa
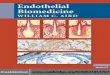
Figure 1. Block diagram describing the relationships between the respirespra-
Respiratory system - The respiratory plant incorporates three compar-tments involved in gas (62 and CO 2) exchange and storage: lung, bodytissue and brain tissue. Each compartment is described through the massbalance equations for both 82 and CC>2, while algebraic relations definethe mixing law in the venous blood and the effect of the pulmonary shunt.Moreover, the plant description is completed with the gas dissociationcurves in tissues and blood, so as to define the relations between concen-trations and partial pressures [2].
With regard to oxygen we used the formulation proposed by Sharan[9], in which a sigmoiclal dissociation curve, incorporating the Bohr ef-fect, gives a reasonable analytical fit of experimental data. As to carbondioxide, the dissociation curve was derived through the model of acid-baseregulation in body fluids mentioned below.
Gas transport arid distribution through the compartments is carriedout by circulation. Cardiac output, Q, and cerebral blood flow, QB, areprovided by the circulatory model. The alveolar ventilation, y, is con-tinuously adjusted by the action of the respiratory controller, which at-tempts to keep the arterial and medullary gas levels close to their basalvalues in spite of changes in external conditions. The functionally relevantaction of the controller depends, as a first instance, on the contribution ofthe peripheral and central chemoreceptors. Assuming that the individualfeedback mechanisms interact linearly, alveolar ventilation was computedas the sum of a basal value and the ventilation changes due to the perip-heral and central components. We adopted a first order dynamics for eachcontributions.
The peripheral receptors arc assumed to respond very rapidly to chaii-ges in arterial CC>2 tension, &,co2, and arterial 82 concentration, C%,O2,
Transactions on Biomedicine and Health vol 4, © 1997 WIT Press, www.witpress.com, ISSN 1743-3525

60 Simulations in Biomedicine IV
-2020
40
\ 20
3_j^ o
-20
Pi,co2 ImmHg]0.73 0.2 0.23
Figure 2. Steady state characteristics of the ventilatory controller, a:peripheral (solid thin line) and central (solid thick line) components of ven-Lilatory response to arterial and medullary CO-2 pressure changes. Dashdotlines represent the response of peripheral chemoreceptors to a ±12% va-riation in Ga,O2- t>: Ventilatory response of peripheral chemoreceptors toarterial 0*2 concentration changes (solid line). Dashdot lines represent theresponse of peripheral chemoreceptors to a ±25% variation in Pa,co2-
with a short delay inversely proportional to blood flow (basal value 5s).The central ones arc sensitive to the medullary CO% tension, Pm,cO2, andhave a slower time constant due to C02 diffusion across the CSF mem-brane.The steady-state characteristics are shown in Fig.2. Here panel adescribes the linear relation between V and Pa,002 due to peripheral che-moreceptors and the piecewise relation between V and Pm,co2 relative tocentral chemoreceptors. Panel b reports the linear relation between V andPa,02 due to the peripheral component only. The model considers that C>2and CO<2 interact non-linearly within the peripheral chemoreceptors, sothat the sensitivity of the peripheral chemoreceptors to Pa,co2 increasesduring hypoxia, and the sensitivity of the peripheral chemoreceptors toCa,02 increases during hypercapnia. This is shown by the dashclot lines inFig.2.
Acid-base buffer system - Although the literature on respiratory physio-logy emphasizes the relevance of acid-base regulation, previous respiratorysystem models either neglect this aspect [3] or use complex numerical de-scriptions [4]. We overcame such limitation, by developing an originalapproach in which a carbonic arid a non-carbonic buffer are assumed toexhaustively describe the buffer action of body fluids [1]. The relationshipwas detailed by including its dependence on the level of oxygen at ion (theHaldane effect) [2].
The chemical control constituted by the acid-base buffer systems inthe body fluids acts, within a fraction of a second, to prevent excessivechanges in hydrogen ion concentrations. Such a subsystem provides theconcentrations of total carbonic buffer, bicarbonate and hydrogen ions, a,tany time, both in blood and in the compartments.
Transactions on Biomedicine and Health vol 4, © 1997 WIT Press, www.witpress.com, ISSN 1743-3525

Simulations in Biomedicine IV 61
Figure 3. Electric analog of the systemic emulation. Q: cardiac output;Psa &W Cga/ si/s^emzc arZerW pregg^re a/zo! gi/s^e/Tizc a/icrzi ( comp/m%ce;RC and R^: portions of the systemic arterial resistance regulated by local
pressurecz'rcwWzcm; P,
atrial compliance.
Cardiovascular system - According to the electric analog of Fig. 3,the model of the cardiovascular system includes the systemic circulationin series with a flow generator. The latter is representative of the heartand pulmonary vessels together. The systemic circulation comprises thearterial and venous compartments: each of them is described by meansof a hydraulic resistance, which reproduces pressure energy losses, anda hydraulic capacity, which simulates blood volume storage. Moreover,the systemic resistance is subdivided into the parallel arrangement of twodistinct resistances, R<. arid R^. The first represents the microcirculatioiiin the organs with intense metabolism, which crucially depend on oxygensupply and on concentration of metabolites. The second is representativeof those peripheral vascular beds (like the splanchnic circulation) whichexhibit only minor local autoregulation and are mainly involved in the ba-rorefiex control. Finally, the systemic circulation terminates into the rightatrium, described as a constant capacity. Both the arterial and venous, aswell as the atrial capacity consist of an unstressed volume (defined as thevolume at zero transmural pressure) and a linear compliance.
The flow generation capacity of the heart-lung compartment is repro-duced assuming that stroke volume depends linearly on pressure in theright atrium, in order to mimic the Starling mechanism. Cardiac outputis then computed as the product of stroke volume and heart rate. It isremarkable that cardiac output in the model is not pulsatile, i.e., only thetemporal mean value of the herno dynamic quantities is reproduced. Seve-ral regulatory mechanisms work on the cardiovascular system in responseto pressure and chemical perturbations to maintain adequate values ofperfusion pressure and organ blood flows. In this model, we have included
Transactions on Biomedicine and Health vol 4, © 1997 WIT Press, www.witpress.com, ISSN 1743-3525

62 Simulations in Biomedicine IV
0
Figure 4. Block diagram describing the baroreflex action on the generice cc or 0 f0 ma?/ 6e e^/ter resWtmcc ^ veno?^ ?/,??,,s resse o /nc or /teorfperiod). G^& and GC&: central gains of the arterial and cardiopulmonary
Pra' systemic arterial pressure and right atrial pressure, respectively. Thesigrnoidal static characteristic (last block in the figure) is negative monotonicas to the control of resistance (as shown here) but is positive monotonic asto the controls of unstressed volume and heart period.
two main regulatory actions, i.e., the baroreflex system and the chemicalregulation. A specific description of each of them is provided below.
The baroreflex control system - The baroreflex system works in responseto pressure perturbations to maintain cardiovascular homeostasis. Affe-rent information to the central neural system is provided by two maingroups of receptors: the high-pressure or arterial baroreceptors, which aresensitive to systemic arterial pressure, and the low-pressure or cardiopul-monary baroreceptors. We assumed that the latter are sensitive to pres-sure in the right atrium. The afferent information from these two groupsof receptors is used to modify three parameters in the cardiovascular plant,which are the effectors of the regulation: the systemic venous unstressedvolume, \4, heart rate, /, and the portion of systemic arterial resistancenot directly controlled by chemical stimuli. Each effector responds to alinear combination of systemic and right atrial pressure changes. Accor-ding to Fig. 4, the response is simulated by means of a, siginoidal staticrelationship and a low-pass linear transfer function with a real pole.
The chemical regulation - We assumed that changes in C>2 and COzblood content have a strong vasodilatory effect on the resistance R^ inFig. 3. This simulates the circulation to those organs (like the brain, theheart and the kidney) which are strongly regulated by local metabolic andchemical stimuli. We assume that the effects of Pa,o2 and l\ coi on theperipheral conductance G,, — I /Re are additive, and that both of themcomplete their action with a first order dynamics characterized by a timeconstant TC — 10s. The steady state relationships relating the conductanceGC to Pa,O2 and Pa,coi during normocapnia arid riorrnoxia are presented
Transactions on Biomedicine and Health vol 4, © 1997 WIT Press, www.witpress.com, ISSN 1743-3525

Simulations in Biomedicine IV 63
b
5
Figure 5. Steady state characteristics describing the chemical control of. a: egW o/ 0(2 Gr^cnaZ press %7'e
m. b: ej ec o/ C>norrnocapnia. The conductance is normalized to its basal level.
in Fig. 5. It is worth noting that deep hypoxia may cause a three-foldincrease in local blood flow (see Fig. 5.b), while hypercapiiia can increaseblood flow up to twice the normal (see Fig. 5.a). Finally, cerebral bloodflow, which is an input for the ventilatory control system (see Fig. 1) iscomputed as a constant fraction (about 33%) of blood flow entering theconductance GC-
3 Results
The above system is described by a 15th order non-linear model whosesolution needs a numerical integration algorithm. For this purpose, asoftware package, SIMULINK (The Mathworks Inc.), mainly oriented tothe development of non-linear numerical simulators, was used.
Figs. 6 and 7 show the time patterns of the main ventilatory, acid-base and cardiovascular quantities predicted by the model in response to10 minutes of acute hypoxia and subsequent recovery. The experimentwas designed by lowering the fraction of inspired 62 from the normal level(21%) to 8%. The sudden decrease in f%,o2 (see Fig. G.b) heavily in-fluences the controlling variables \/ and Q, which increase to support theoxygen request by tissues (see Figs. 6.d and 7.d). This induces a signifi-cant decrease of both P coi and Pm,co2 thus driving a delayed depressionof ventilation. In the recovery phase, the abrupt rise in 62 joined with thecontemporary low value of CO2 lead to a total depression of ventilationthat introduces a slow recovery with an initial phase of apneic oscillationfollowed by a rioii-apiieic one. This is a manifestation of the so calledCheyne-Stokes breathing and is well documented in physiological litera-ture. This pattern propagates to all the cardiovascular quantities, as well(see Fig. 7). The pHa correctly reveals the moderate alkalosis that takesplace during hypoxia (see Fig. 6.c).
Transactions on Biomedicine and Health vol 4, © 1997 WIT Press, www.witpress.com, ISSN 1743-3525

64 Simulations in Biomedicine IV
45
'wl 40ffi
fl 35
30
7.5
7.4
Pa,C020 70 20 JO
-TV-pHa
70 20 JO 40[min]
700
ffl
3, 50
250 70 20 JO 40
70 20 JO 40[mill]
Figure 6. Ventilatory and acid-base quantities in the simulated hypoxiaexperiment, a: arterial C0<2 tension; b: arterial 0-2 tension; c: arterialpH; d: alveolar ventilation.
700
70 20 30 40[min]
70 20 30 40[min]
Figure 7. Cardiovascular quantities in the simulated hypoxia experiment.a: systemic arterial pressure; b: systemic arterial resistance; c: heart rate;d: nor
; ear rae;rmalized cardiac output (thick line) and cerebral blood flow (thin line).
Transactions on Biomedicine and Health vol 4, © 1997 WIT Press, www.witpress.com, ISSN 1743-3525

Simulations in Biomedicine IV 65
4 Discussion
The present model constitutes a first attempt to investigate the relation-ships between the cardiovascular and ventilatory control systems duringchemical perturbations in quantitative terms. The use of such a modelmay be of importance both to improve the physiological knowledge oncardio-respiratory regulation, and, in perspective, to help medical doctorsin the analysis and management of pathological conditions associated withmetabolic and cardio-respiratory alterations. The present model improvesand extends previous works [3,4] in several important aspects. In particu-lar, various authors developed models of the ventilatory control system, inwhich the role of cardiac output and cerebral blood flow is taken into ac-count. However, in these models the dependence of blood flow on 0% andCO2 is provided by empirical relationships, without details on cardiova-scular system dynamics. Hence, they cannot be used to analyze the effectof clinical maneuvers (such as hemodialysis) or pathological conditions(such as heart failure) associated with alterations in circulatory parame-ters. On the other hand, previous models which are explicitly focusedon cardiovascular system regulation [5] do not incorporate a ventilatorycontrol explicitly.
The preliminary simulation results presented in the previous sectionshow reasonable agreement with clinical and physiological data, even ifsome limitations and aspects requiring further improvements are also ap-parent. In particular, the time pattern of the main quantities in the respi-ratory model (ventilation, 0] and €0% arterial pressure, p//«) agree withthe data reported in the literature following acute hypoxia [7]. Similarly,the increase in heart rate, cardiac output and cerebral blood flow, and thedecrease in total systemic resistance replicate the well-known hemodyna-mic adjustments (both local and reflex-mediated) induced by hypoxemia.
The main present difference between model response and real dataconcerns systemic arterial pressure (see Fig. 7.a). In the model, systemicarterial pressure decreases significantly during hypoxia, as a consequenceof peripheral vasodilatiori. The decrease in arterial pressure is antagonisedby the baroreflex response, which induces vasoconstriction of the remai-ning portion of the systemic arterial vascular bed, venous vasoconstrictionand tachycardia. Owing to the baroreflex control, the fall in systemic ar-terial pressure is moderate (from 100 mmHg to about 85 mmHg). Clinicaland physiological results, however, suggest that arterial pressure remainunchanged or may even increase slightly following hypoxemia [8,10]. Apossible reason for these differences is that the present model does notincorporate a rieurally-mediated chemoreflex response, but only local au-toregulation to changes in blood gas content. The expected effect of thechemoreceptors during hypoxia is that of causing further vasoconstriction,contributing to a better maintenance of the systemic arterial pressure level.In support of this hypothesis, Lugliani et al. [6] found that during hypoxia,
Transactions on Biomedicine and Health vol 4, © 1997 WIT Press, www.witpress.com, ISSN 1743-3525

66 Simulations in Biomedicine IV
subjects with intact chemoreceptors show minor increases in systemic ar-terial pressure, whereas subjects with carotid body clenervation (whichaffect the chemoreceptor but not the baroreceptor system) exhibit arterialpressure reduction. Inclusion of the chemoreflex response may constitutea future, necessary improvement of the present model.
In conclusion, the proposed model may represent a new tool for theanalysis of the overall cardio-respiratory control system, able to deal withchemical and cardiovascular perturbations together. It can be used asa support for the analysis of many clinical problems, such as metabolicdisorders, lung diseases, hemodialysis and post-car diosurgical care.
References
[1] Chiari, L., Avanzolini, G., Grandi, F. & Gnudi, G. A simple model ofthe chemical regulation of acid-base balance in blood, Proc. XVI Int.CW/. /Egg-gMRS, pp. 1025-1026, Baltimore, Maryland, 1994.
[2] Chiari, L., Avanzolini, G. & Ursino, M. A comprehensive simulatorof the human respiratory system: validation with experimental andsimulated data. Ann. Biomed. Eng., (submitted).
[3] Finch am, W.F. & Tchrani, F.T. A mathematical model of the humanrespiratory system. J. Biomed. Hng., 1983, 5, 125-133.
[4] Grodins, F.S., Buell, J. & Bart, A.J. Mathematical analysis and digitalsimulation of the respiratory control system. J'. Appl. PhysioL, 1967,22, 260-276.
[5] Guy ton, A.C., Coleman, T.G. & Granger, H.J. Circulation: overallregulation. /Irnm. #e%. P/ti/sW., 1972, 34, 13-46.
[6] Lugliaiii, R., Whipp, B.J. & Wassermaii, K. A role of the carotid bodyiri the cardiovascular control in man. Cliest, 1973, 63, 744-750.
[7] Reynolds, W.J. & Milhorn, H.T. Transient vcntilatory response tohypoxia with and without controlled alveolar Pco-2- •/• Appl. PhysioL,1973, 35, 187-196.
[8] Richardson, D.W., Kontos, H.A., Raper, A.J. & Patterson, J.L. Mo-dification by beta-adrenergic blockade of the circulatory responses toacute hypoxia in man. J. Clin. Invest., 1967, 46, 77-85.
[9] Sharan, M., Singh, M.P. & Aminataei, A. A mathematical model forthe computation of the oxygen dissociation curve in human blood.Bmsi/sfcms, 1989, 22, 249-260.
[10] Sylvester, J.T., Scharf, S.M., Gilbert, R.D., Fitzgerald, R.S. & Trayst-man, R.J. Hypoxic and CO hypoxia in dogs: hcmodynamics, carotidreflexes, and catecholamiiies. Am. J. Physiol, 1979, 236, H22-H28.
Transactions on Biomedicine and Health vol 4, © 1997 WIT Press, www.witpress.com, ISSN 1743-3525